Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Migraine Duration as a Potential Amplifier of Obesity
Authors Fan XX ![]() , Ye L, Yang YH, Huang WJ
, Ye L, Yang YH, Huang WJ ![]() , Ko CY
, Ko CY ![]()
Received 1 November 2023
Accepted for publication 15 February 2024
Published 29 February 2024 Volume 2024:17 Pages 1025—1037
DOI https://doi.org/10.2147/DMSO.S447781
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Xi-Xin Fan,1,2,* Lichao Ye,3,* Ya-Hui Yang,1,2 Wen-Jian Huang,2,4 Chih-Yuan Ko2
1The School of Public Health, Fujian Medical University, Fuzhou, People’s Republic of China; 2Department of Clinical Nutrition, the Second Affiliated Hospital of Fujian Medical University, Quanzhou, People’s Republic of China; 3Department of Neurology, the Second Affiliated Hospital of Fujian Medical University, Quanzhou, People’s Republic of China; 4Huidong Center for Chronic Disease Control, Huizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chih-Yuan Ko, Department of Clinical Nutrition, The Second Affiliated Hospital of Fujian Medical University, No. 34, Zhongshanbei Road, Licheng District, Quanzhou, Fujian Province, 362000, People’s Republic of China, Tel +86 0595-26655200, Email [email protected]
Purpose: Migraine is a complex neurovascular disorder with obesity as a notable risk factor. This study aimed to investigate an under-researched area of the association between migraine duration and body composition.
Patients and Methods: Patients with migraine from a neurology outpatient department were enrolled and were categorized into four groups based on illness duration: 1 year, 1– 5 years, 5– 10 years, and > 10 years. Patient demographics, blood biochemistry, and body composition data were collected and analyzed statistically.
Results: Patients with migraine were predominantly female, with lower education levels, significant work stress, poor sleep, and limited exercise. Longer migraine duration corresponded to increased obesity metrics. Notably, those patients with under 1 year of illness showed elevated blood lipid and liver function levels, whereas those with > 10 years showed increased weight, waist circumference, body mass index, and fat content, despite higher physical activity. Significant positive correlation between obesity metrics and migraine duration was seen in patients who had migraine for > 1 year.
Conclusion: Our findings indicate that protracted episodes of migraine could amplify obesity tendencies, underscoring the imperative of weight regulation in migraine intervention to diminish ensuing adiposity-associated hazards.
Keywords: migraine, illness duration, obesity, body composition
Introduction
Migraine is a globally prevalent chronic disease marked by intense pulsating headaches and symptoms such as nausea and photophobia.1,2 Studies from China indicate its predominance in middle-aged urban women aged >30 years.3,4 Lower socioeconomic status and limited education increase adverse outcomes, possibly due to insufficient awareness, medical access barriers, and treatment noncompliance.5,6 Over-reliance on readily available over-The-counter analgesics can exacerbate symptoms, potentially transitioning episodic migraines to chronic forms.7 Frequent analgesic use might deter patients from seeking formal medical advice. Moreover, the extended consequences of migraine, including anxiety, depression, and diminished activity, can affect the overall well-being of patients.
Obesity increases the risk of migraine. Individuals with a body mass index (BMI) ≥30 kg/m2 show a markedly higher migraine prevalence than those with normal weight, and obese individuals are twice at risk than of their normal-weight counterparts [odds ratio (OR) 2.10 (1.39–3.12)].8 This could be due to chronic inflammation and endocrine dysfunction observed in obese individuals.9 Obese women had elevated levels of the pain-transmitting protein, calcitonin gene-related peptide (CGRP), compared with those having normal weight.10 Rats with obesity and high CGRP levels also demonstrated more frequent events of cortical spreading depression (CSD), a slow neural and glial wave in the brain linked to ion imbalances.11 Thus, the influence of obesity on migraine may arise from modulation of mechanisms, including endocrine pathways. However, CGRP is not considered as the gold standard for diagnosing migraines.
Body composition offers a more precise measure of obesity than body weight alone. Although BMI measures weight relative to height, the actual fat and muscle distribution is overlooked. With progressing of age, body fat percentage and muscle mass can shift without change in weight, leading to varied degrees of obesity for individuals with identical BMIs. Body composition analysis visually presents muscle, fat, water, and mineral proportions, indicating overall health. Major parameters, such as body fat percentage, visceral fat area, and waist-to-hip ratio, can precisely determine fat distribution and obesity assessment.12 Techniques such as bioelectrical impedance analysis (BIA), dual-energy X-ray absorptiometry, and magnetic resonance imaging can measure body composition. Of these, BIA is highlighted for its simplicity, cost-effectiveness, and absence of radiation exposure.
Although obesity can elevate migraine risk, the influence of migraine duration on obesity levels or body composition variations among patients with different illness durations has not been elucidated yet. This study used the BIA technique to evaluate body composition, capturing metrics, such as BMI, waist circumference, fat-free mass (FFM), fat, protein, and minerals. This study aimed to discern lifestyle and body composition differences in patients with migraine based on their illness duration and to measure the effect of this duration on their degree of obesity.
Materials and Methods
Participants
The study complies with the Declaration of Helsinki, having been approved by the Independent Ethics Committee of the Second Affiliated Hospital of Fujian Medical University (IRB No. 2022–117) and involved the recruitment of adult migraine patients from the neurology outpatient department. Data collection encompassed sociodemographic details, exposure history, medical records, blood biochemistry, and body composition. Migraine-type evaluations were also conducted. They were categorized based on illness duration into four groups: Group 1 (G1, under 1 year), Group 2 (G2, 1 to 5 years), Group 3 (G3, 5 to 10 years), and Group 4 (G4, over 10 years). Exclusions were made for individuals under 18, those with physical conditions like diabetes or cardiovascular diseases, those pregnant or lactating, and those with mental disorders.
Medical history data provided insights into the demographic characteristics of participants, such as age, educational duration, and marital status. Details on exposure history, including occupational exposures and tobacco and alcohol consumption, and triggers like specific preceding events were also collected.
Migraine Diagnosis
Migraine types were determined by specialists, adhering to the International Classification of Headache Disorders, 3rd edition guidelines. Diagnosis relied on current medical history. During subsequent outpatient visits, ambiguous cases were advised to maintain a headache diary for a clearer diagnosis. This study included only primary migraine patients with or without aura and secondary migraine cases arising from substance or medication withdrawal.2
Blood Biochemistry Analysis
Participants provided a 2 mL venous blood sample, collected using standard procedures. The biochemical assessment was conducted using the Mindray BS-280 Fully Automated Chemical Analyzer (NMT, Shenzhen, China), which analyzed various parameters.
Body Composition Measurement
The body composition data were obtained and assessed by multifrequency tetrapolar Inbody S10 equipment (Biospace Co, Ltd., Seoul, Korea), the procedures were conducted in our prior research.13 Pre-measurement protocols required fasting, bladder and bowel emptying, removal of metal jewelry, and lightweight clothing. Measurements were taken in seated or supine positions, ensuring proper contact with device electrodes. Evaluated indicators encompassed body weight, waist circumference, total body water (TBW), intracellular water (ICW), extracellular water (ECW), ECW/TBW ratio, body mass index (BMI), body fat mass (BFM), percent body fat (PBF), visceral fat area (VFA), fat mass (FFM), protein, skeletal muscle mass (SMM), lean balance, minerals, and phase angle (PhA).
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software. The normality of the data was assessed using the Kolmogorov–Smirnov test, while the homogeneity of variances was assessed using the Levene test. Normally distributed continuous data was described using mean ± standard deviation (X ± SD). The independent two-sample t-test was used to compare means between two groups (assuming homogeneity of variances), to determine if there were statistically significant differences in the measured variables between the groups. For non-normally distributed continuous data, variables were transformed to achieve normality or described using the median and interquartile range (P50, P75-P25). The Mann–Whitney U-test was used for comparison. Count data was expressed as percentages (%), and the chi-square test was used for comparisons. The relationship between disease duration and body composition was analyzed using Spearman’s rank correlation. A p-value of < 0.05 was considered statistically significant.
Results
Characteristics of Patients
In this study, the final participants, were 10 men and 79 women, with an average age of 42.2±10.9 years. The participants were divided into four groups: G1 (15 participants), G2 (27 participants), G3 (19 participants), and G4 (28 participants). There were more female participants, aged between 34 and 51. No significant differences were found in age (p = 0.155) and height (p = 0.595) among the groups. Around 62.9% of the participants did not complete 9 years of compulsory education, and there were no significant differences in educational attainment among the groups (p = 0.492) (Table 1). The majority of patients (80.9%) reported engaging in light-intensity household chores as their primary occupation. Participants in G3 and G4 had a higher prevalence of individuals experiencing stress (p < 0.001), with 41.6% perceiving mild to severe work-related stress (Table 1). Most patients in all groups reported no work-related stress. However, some patients, especially who had been suffering from migraines for over five years, expressed in the questionnaire the pressure caused by chronic migraines leading to inadequate sleep and decreased work efficiency, which is also a contributing factor to the perception of work-related stress the subjects in this study, even when engaged in light labor.
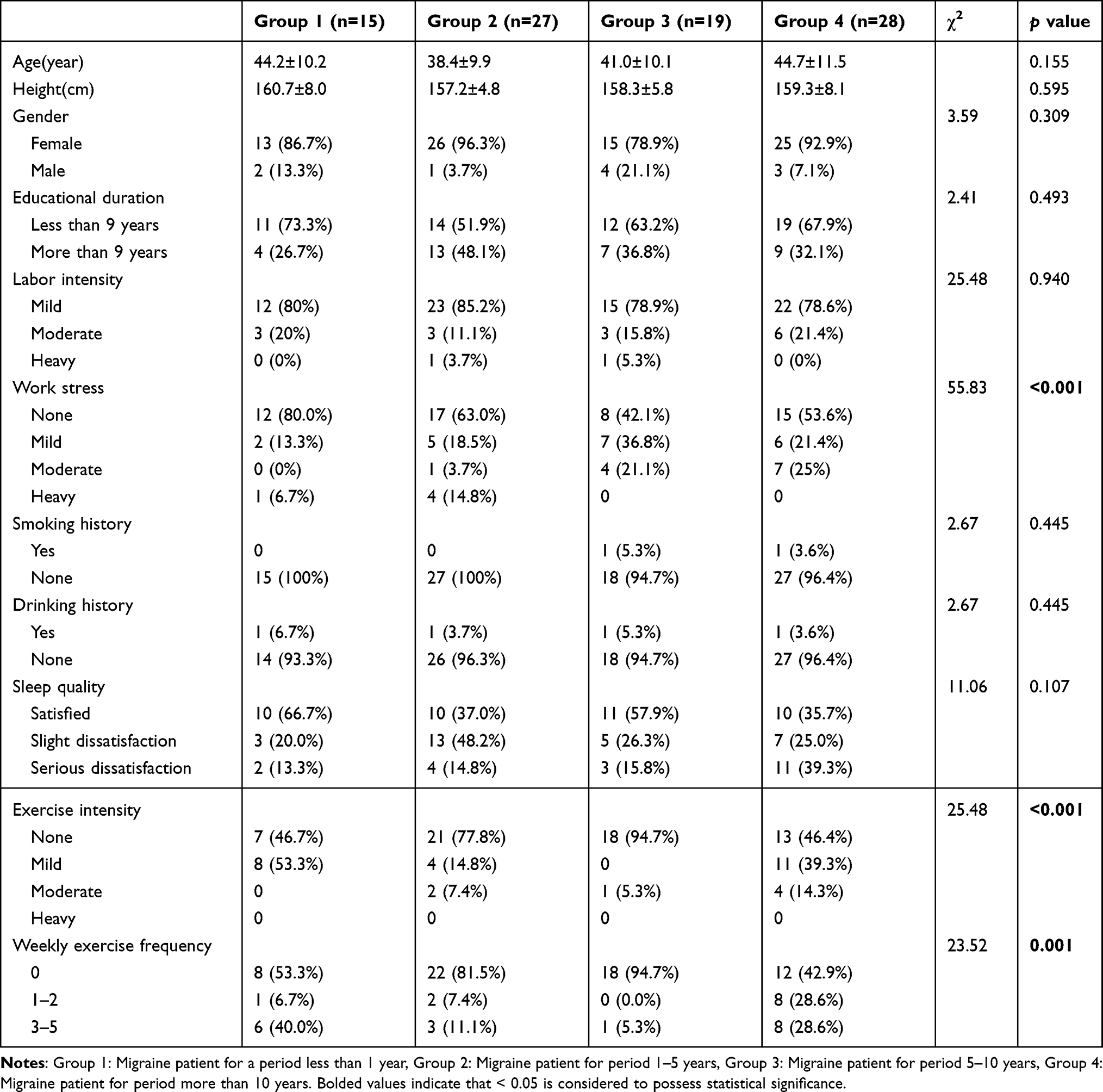 |
Table 1 Characteristics of the Participants |
Only 12.4% of the participants reported experiencing menstrual-related headaches, and there were no significant differences in the prevalence of menstrual-related headaches among the groups (p = 0.187). A small percentage of participants had a history of smoking (2.2%) and alcohol consumption (4.4%). More than half of the participants (53.9%) expressed dissatisfaction with their sleep quality, with the highest level observed in the G4 group, indicating the poorest sleep quality. However, there were no significant differences in sleep problems among the groups (p = 0.107). The majority of patients (66.3%) do not have a regular exercise habit, and those who engage in exercise mainly participate in light-intensity activities such as walking. G2 and G3 had the lowest levels of physical activity (p < 0.001) and exercise frequency (p = 0.001) (Table 1).
Blood Biochemistry
Table 2 shows significant differences in blood biochemistry results among the different groups. The following parameters exhibited significant differences: total protein (p = 0.009), alanine aminotransferase (ALT) (p = 0.001), aspartate aminotransferase (AST) (p = 0.014), AST/ALT (p = 0.046), alkaline phosphatase (ALP) (p = 0.024), γ-glutamyl transpeptidase (γ-GT) (p < 0.001), cholesterol (p = 0.005), low-density lipoprotein-cholesterol (LDL-c) (p = 0.001), apolipoprotein-B (APB) (p = 0.007), and APB: APA (p = 0.04).
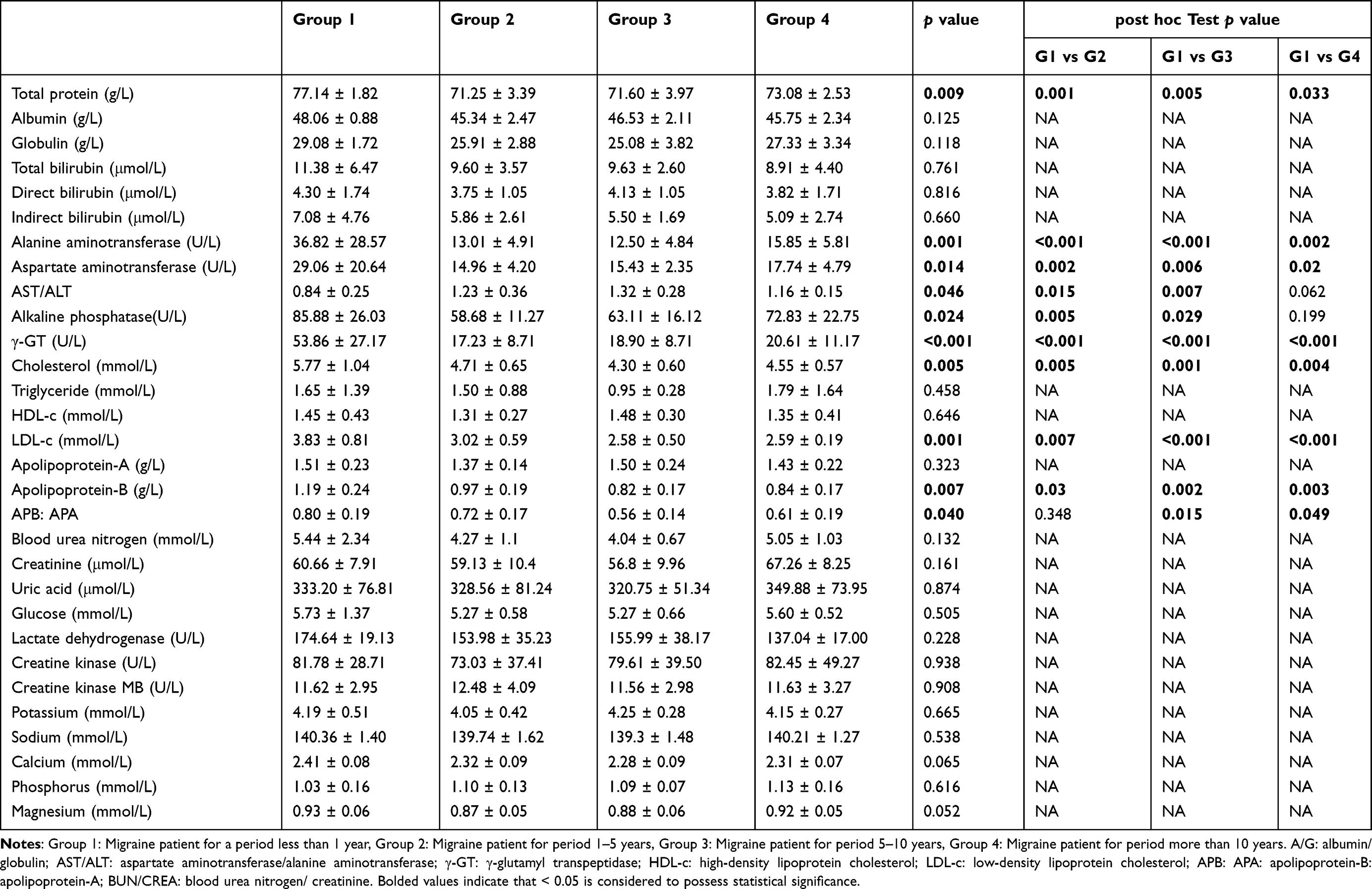 |
Table 2 Analysis of Blood Profiles Across Different Periods Cohort Migraine Patients |
G1 had the highest values in total protein, ALT, AST, γ-GT, cholesterol, LDL-c, and APB, which were significantly higher than those of the other three groups. However, no significant differences were observed among the other three groups. ALP levels were significantly higher in G1 compared to G2 (p = 0.005) and G3 (p = 0.029) but did not differ significantly from G4. The APB: APA ratio in G1 was higher than that of G3 (p =0.015) and G4 (p = 0.049). The AST/ALT ratio in G1 was the lowest and significantly lower than G2 and G3 (p = 0.015, 0.007), but did not differ significantly from G4 (Table 2).
Body Composition
The results demonstrate significant differences in body weight (p = 0.041) and waist circumference (p = 0.043) among the groups. Both G1 and G4 had higher values compared to G2 and G3 in terms of weight and waist circumference. Specifically, G4 displayed the highest values for waist circumference (p = 0.012) and weight (p = 0.006) compared to G2 (Table 3, Figure 1). However, no significant differences were observed in other body composition indicators such as TBW, ICW, ECW, ECW/TBW, PBF, VFA, FFM, protein, SMM, mineral, and PhA (Table 3).
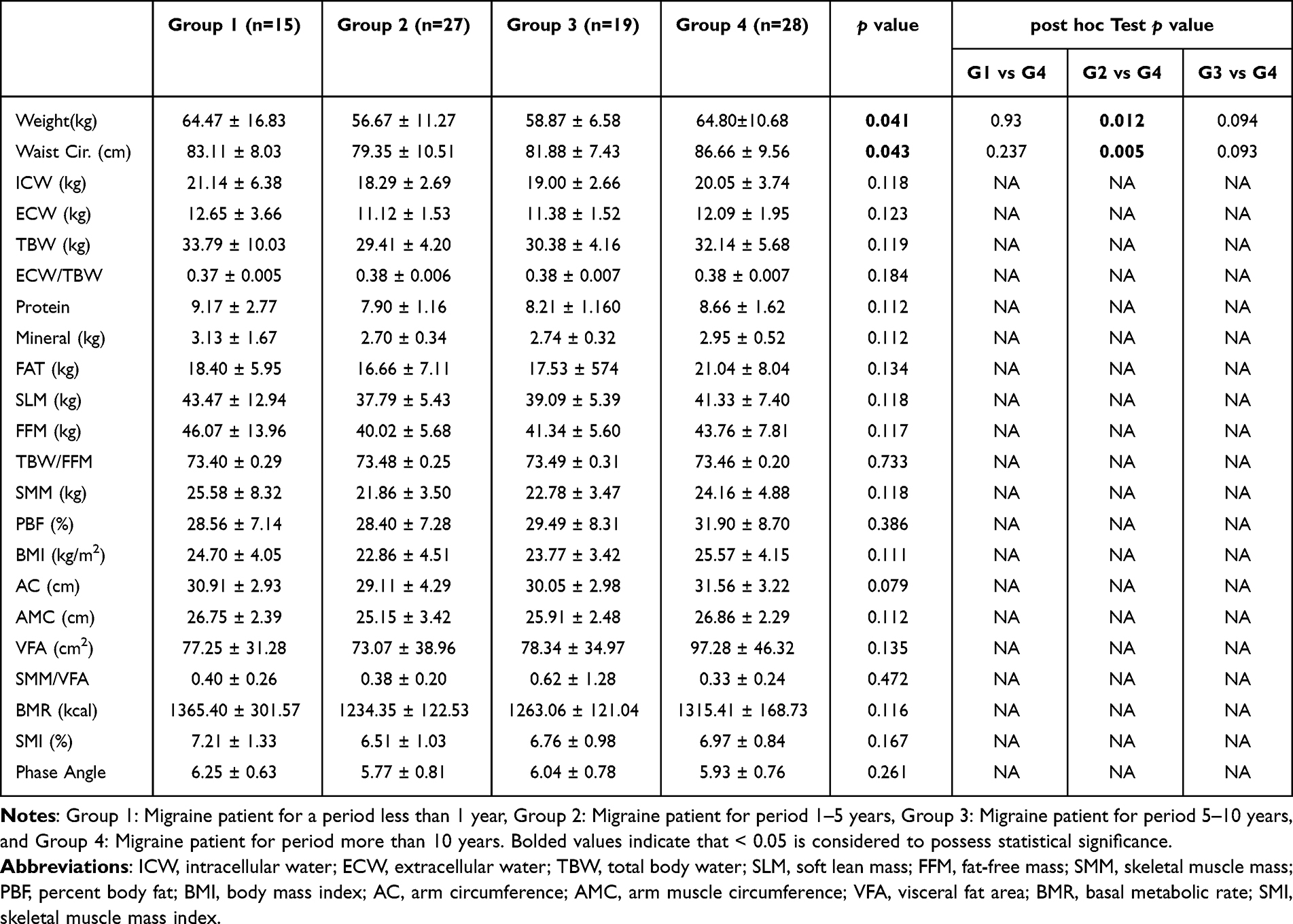 |
Table 3 Analysis of Body Composition Across Different Periods Cohort Migraine Patients |
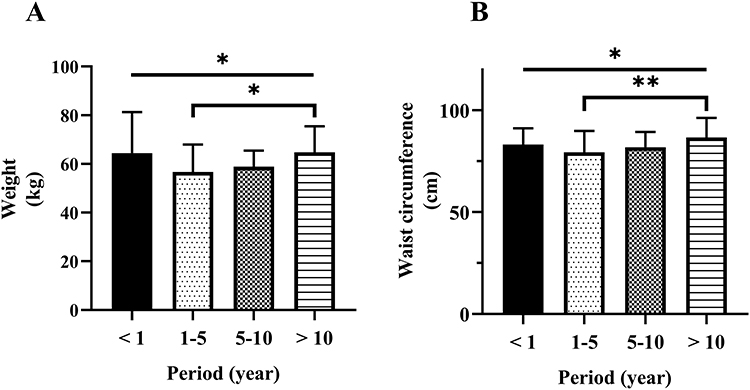 |
Figure 1 Body weight (A) and waist circumference (B) of cohort migraine patients. *p <0.05, **p <0.01. |
Figure 2 shows an increasing trend in body weight, waist circumference, fat, and BMI among the three groups, except for Group 1. Group 4 has significantly higher body weight (p = 0.012), waist circumference (p = 0.005), fat (p = 0.025), and BMI (p = 0.019) compared to Group 2. Figure 3 shows the correlations between weight, waist circumference, BMI, and fat of migraine patients for more than 1 year. The other three groups showed significant differences in weight (r = 0.509, p < 0.0001), waist circumference (r = 0.479, p < 0.0001), BMI (r = 0.467, p < 0.0001), and fat (r = 0.366, p = 0.0017), indicating a gradual increasing trend. Furthermore, a positive correlation was observed between the increase in these indicators and the duration of the disease in these three groups. Considering the potential impact of work-related stress and exercise on body weight, comparable data were grouped and contrasted based on similar levels of work-related stress and exercise habits. Similar results were observed in the subgroup with no work-related stress and no exercise habits, as in the ungrouped data.
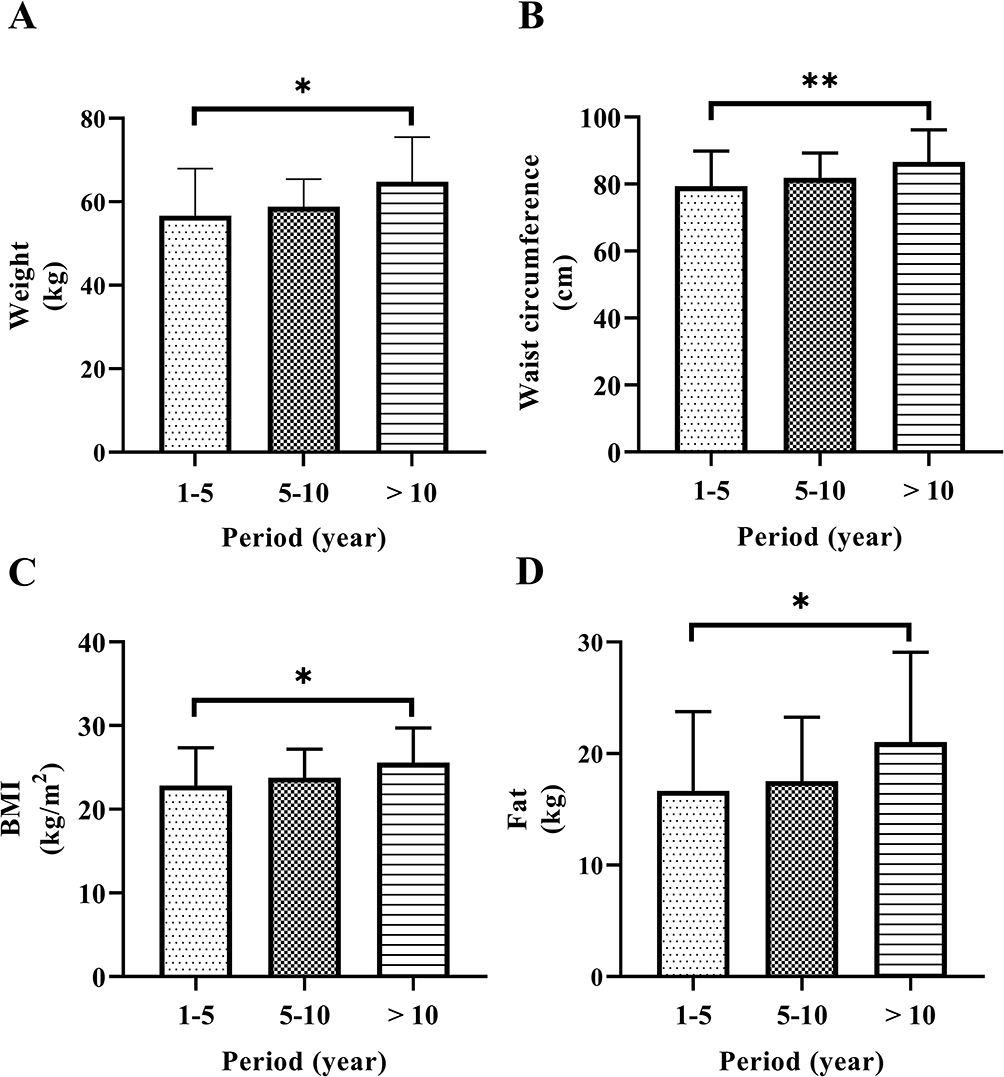 |
Figure 2 Body weight (A), waist circumference (B), body mass index (BMI) (C), and fat (D) of cohort migraine patients. *p<0.05, **p<0.01. |
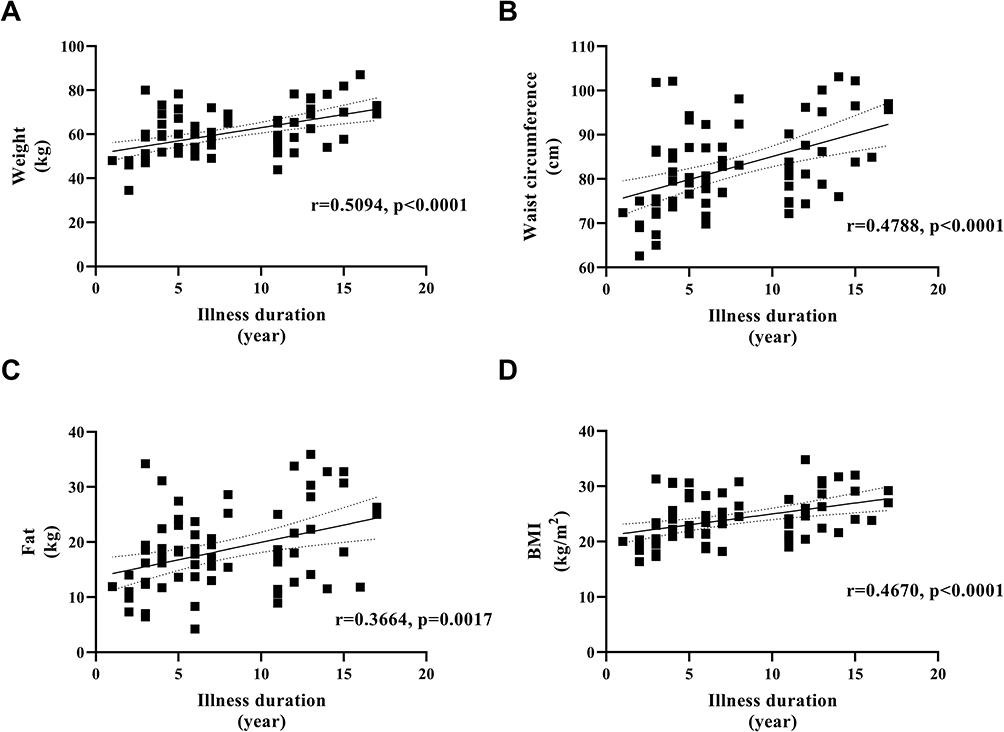 |
Figure 3 The correlation between the duration of illness and weight (A), waist circumference (B), fat (C), body mass index (BMI) (D) of migraine patients for a period of more than 1 year. |
Discussion
Present study mainly identified patients seeking outpatient care for migraines, predominantly middle-aged women, with approximately 50% being overweight or obese, with education levels up to elementary or junior high school, and mostly homemaker individuals. Life stress, sleep disturbances, and a sedentary lifestyle were commonly reported by the patients. Notably, a significant increase in weight, waist circumference, BMI, and body fat correlated with disease duration, even after adjusting for height and age.
This study primarily included female participants aged 34–51 years, consistent with a previous study.3 The increased occurrence of migraines in women has been linked to ovarian sex hormone secretion, leading to a heightened migraine frequency in women of childbearing age compared with men. Conversely, the migraine rates of postmenopausal and prepubescent women were similar to men.14 Lower estrogen levels reduce migraine symptoms, possibly due to the effect of sex hormones on cerebral circulation, reducing vascular tone and increasing cerebral blood volume.15 Women experience longer migraines durations and more frequent recurrences,16 along with extended periods of activity limitation due to migraines compared with men, leading to greater prevalence of headache-related disability among women.17,18
Our findings revealed that chronic migraine adversely affects sleep quality. Sleep disturbances, including trouble initiating sleep and premature awakenings were reported by majority of patients, resulting in overall dissatisfaction in sleep quality. Notably, those with migraine durations >10 years experienced poor sleep quality, underscoring the negative impact of long-term headaches on sleep. Lack of sleep triggers migraine by disrupting biological rhythms, hormonal balance, and increasing inflammatory factors.19 Additionally, poor sleep quality in patients with migraine is frequently linked with adverse emotional states, such as anxiety and depression.19 Migraine attacks prolong sleep onset and shorten sleep duration, which reduces sleep quality and exacerbates anxiety and depression, that can cause migraines, complicate treatment, and lead to relapses.20 Sleep deprivation and anxiety are also recognized risk factors for obesity.21 Although neither is a major cause of migraines, it can further exacerbate the frequency and severity of migraine headaches.22
A few patients in this study reported work-related stress. Different results have been observed in previous studies of psychosocial factors and body weight in the workplace, but a slight correlation was found in men with long working hours.23 The patients in this study did not report long working hours, and thus work-related stress was not a cause of obesity in migraine patients.
Notably, the study population exhibited a lack of exercise, primarily due to migraine-related discomfort deterring physical activity, resulting in inadequate exercise and aggravated obesity. Exercise plays a crucial role in migraine treatment and prevention. Individuals lacking physical activity are at a higher risk of migraines, whereas regular exercise diminishes migraine risk and occurrence frequency.24 Interestingly, it was found that patients with >10 years of illness demonstrated a significantly increased exercise intensity and frequency, indicating that prolonged headache experience might increase disease awareness and motivate beneficial physical engagement.
Currently, most migraine medications, such as sodium valproate and flunarizine, except for topiramate, are associated with weight gain. The participants in our study often resorted to irregular migraine treatments, especially using over-The-counter pain relievers, such as aspirin, ibuprofen, and acetaminophen, during headaches. Notably, these medications did not significantly affect body weight. However, our findings revealed that approximately 50% of patients had a BMI ≥24, classifying them as overweight or obese, which is consistent with existing research indicating a correlation between increased body weight and a higher migraine risk.8 Significant differences were seen in the weight and waist circumference among patients with migraine and varying illness durations. Specifically, weight, waist circumference, BMI, and body fat percentage showed positive correlations with illness duration among those with migraine >1 year. International population surveys validate that obesity can increase the risk of chronic migraines25–27 or intensify headache frequency and severity,28 possibly due to obesity-related chronic inflammation and metabolic dysregulation.29 Chronic inflammation in obesity might affect the trigeminal nerve and meninges.30 Obese rats exhibited heightened CGRP release from the trigeminal nerve under harmful stimuli, reducing the headache threshold.31 The trigeminal nerve is central to pain perception in the anterior two-thirds of the head and plays a crucial role during headache.32 Concurrently, CSD between the meninges and cortex is a key mechanism in migraine with aura, and it can also be affected by inflammation.33 Inflammation-induced alterations in K+ channels may also explain the increased CSD production in obese rats.34 Furthermore, the unhealthy lifestyles of obese patients, such as a high-fat diet, sedentary habits, and irregular sleep, combined with cumulative daily stress from work and social pressures, have been linked to migraine onset and progression. These daily stressors can also worsen symptoms and influence migraine frequency and severity via neural regulation, inflammatory responses, and blood rheology.35
Although our study did not show significant differences in the inflammatory markers in the patient’s blood tests, a previous study has confirmed a close association between migraines and inflammation. The pathophysiology of migraines involves proinflammatory cytokines, including interleukin-6 (IL-6), interleukin-1β (IL-1β), and tumor necrosis factor-α (TNF-α). These markers undergo changes at serum levels of patients with migraine,36 with alterations in TNF-α levels observed in the serum and/or urine samples of some patients with migraine during and between attacks.36,37 However, these data are controversial. Furthermore, migraines were speculated to be the result of neurogenic inflammation.36 Dural neurogenic inflammation is considered a driving factor for migraine attacks. Studies reveal that neurogenic inflammation contributes to increased blood–brain barrier permeability, leukocyte infiltration, glial cell activation, and inflammatory cytokines secretion.36 On the other hand, increased adipose tissue mass and adipocyte hypertrophy are closely associated with the secretion of inflammatory mediators, such as cytokines, chemokines, and acute-phase proteins.38 The plasma levels of TNF-α, IL-6, and C-reactive protein (CRP) are elevated in overweight individuals.39 Therefore, in migraine patients with an inflammation history, increased inflammatory cytokine levels may be a contributing factor to their obesity, whereas the exacerbation of inflammatory conditions may also be related to more frequent and severe migraine attacks, eventually transitioning to chronic migraines.40
The patients enrolled in this study were not diagnosed with any metabolic disorders, such as insulin resistance. However, the presence of abnormal biochemical markers indicated underlying metabolic disturbances. In the subgroup experiencing migraines <1 year, blood biochemical tests revealed lipid-associated markers including elevated levels of cholesterol, LDL-C, APB, and the APB:APA ratio. Notably, LDL-C showed a positive correlation with body adiposity index, indicating its association with obesity.41 The surge in cholesterol and APB indicates compromised adipocyte functionality and enlargement, implying severe obesity and disrupted lipid metabolism in this particular group.42 Additionally, liver function markers including ALT, AST, γ-GT, and alkaline phosphatase, were significantly elevated. Moreover, elevated alanine aminotransferase and aspartate aminotransferase levels indicated liver cell damage and cholestasis-related injury.43 These outcomes indicated that the subgroup with migraine <1 year showed more pronounced liver damage than the other groups, further underlining severe obesity and metabolic disturbances. The common characteristics of G1 were higher age, weight, BMI, and waist circumference, indicating severe obesity in G1. This explains the higher values in their biochemical test results, which indicated the presence of obesity before headache onset, potentially influencing migraine severity and occurrence.28,44
Notably, the severity of obesity and duration of illness showed a clear positive correlation after removing G1. The degree of obesity in the G1 group was comparable to that of the G4 group, and no significant age difference was observed between the two groups, with the age distribution relatively close to that of the other groups. Although female aging coupled with reduced menstruation and decreased hormone levels may lead to weight gain and increased body fat, age was not an influential factor for obesity in migraine patients in this study.45 This result may be related to the severity of the headache at the time the patient seeks medical attention. Blood test results indicated that patients with migraine <1 year may have been obese and had more severe headaches before their migraine attacks. In contrast, patients with a longer duration of illness did not seek medical attention in a timely manner because their previous migraine symptoms were mild and did not significantly affect their work and daily life, and sought medical help only after their symptoms worsened, thus prolonged migraines led to the development of obesity in the patients.
The shared mechanism underlying migraine and obesity may involve interactions at the central and peripheral levels. The hypothalamus, which stimulates and inhibits feeding, also regulates gastrointestinal function. Hypothalamic-related symptoms, such as food cravings, emotional disturbances, and sleep issues are often experienced by patients with migraine.46 Imaging studies have shown hypothalamic activation during migraine attacks may contribute to hyperphagia and subsequent weight gain.47 Additionally, the hypothalamic release of feeding-related peptides and proteins, including serotonin, orexin, and leptin, play role in migraine pathophysiology, potentially increasing the migraines incidences in individuals with obesity.48 Peripherally, the association between migraine and obesity is linked to the release of inflammatory factors from the adipose tissue in obesity cases.
This study has few limitations. First, the cross-sectional design hindered our ability to track body composition changes before and after illness onset. A longitudinal approach in future studies could provide more insight into the migraine–obesity connection. Second, the limited sample size raises concerns regarding potential bias in the results, indicating the requirement for larger-scale research with more participants to support the validity of the study. The gender ratio and age range of the participants in this study were similar to those in previous relevant surveys, indicating generalizability to the migraine population. However, the cases were limited to the Quanzhou region, which may limit the generalizability to populations in other areas. Thus, more external data collection through multicenter research in the future could validate our study results. Our findings support clinical guidelines for migraine prevention, emphasizing behavioral interventions and reasonable medication use for preventing the progression from episodic to chronic migraines. Third, the lack of headache severity quantification in this study restricted our understanding of variations in disease severity across different groups. Future research should consider including headache severity, frequency, and duration for a more comprehensive evaluation of patients with migraine.
Conclusion
Present study identified that the key characteristics in patients with migraine were female sex, lower education, high work stress, poor sleep, and little exercise. A clear correlation was seen between migraine duration of >1 year and increased body metrics, such as weight and BMI. Shorter migraine history was linked to altered lipid and liver function, indicating the potential role of obesity in the worsening of migraine severity, indicating a possible selection bias because less obese individuals may seek less medical care. Despite existing research, the precise relationship between chronic migraine and obesity requires further high-quality, prospective studies for a clearer understanding and improved patient care.
Data Sharing Statement
The data used to support the findings of this study have been included in this article.
Ethics Approval and Consent to Participate
This study was performed in according with the Declaration of Helsinki and was approved by the Research Ethics Committee of the Second Affiliated Hospital of Fujian Medical University (IRB No. 2022-117). Participants provided written informed consent before initiating the study.
Acknowledgments
We extend our heartfelt thanks to all participants and their families involved in this study. Their assistance was crucial in facilitating communication and elucidating certain aspects of the information collection process. This support was especially invaluable considering the educational background of many participants and their exclusive use of local dialects.
Funding
This study was supported by a grant from the Second Affiliated Hospital of Fujian Medical University (serial No. YJ202301).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders, 3rd edition. Cephalalgia. 2013;33(9):629–808. doi:10.1177/0333102413485658
3. Yu S, Liu R, Zhao G, et al. The prevalence and burden of primary headaches in China: a population-based door-to-door survey. HeadacheApr. 2012;52(4):582–591. doi:10.1111/j.1526-4610.2011.02061.x
4. Yu S, He M, Liu R, et al. Headache yesterday in China: a new approach to estimating the burden of headache, applied in a general-population survey in China. Cephalalgia. 2013;33(15):1211–1217. doi:10.1177/0333102413490347
5. Lipton RB, Bigal ME, Diamond M, Freitag F, Reed ML, Stewart WF. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):343–349. doi:10.1212/01.wnl.0000252808.97649.21
6. Hagen K, Vatten L, Stovner LJ, Zwart JA, Krokstad S, Bovim G. Low socio-economic status is associated with increased risk of frequent headache: a prospective study of 22718 adults in Norway. Cephalalgia. 2002;22(8):672–679. doi:10.1046/j.1468-2982.2002.00413.x
7. Bahra A, Walsh M, Menon S, Goadsby PJ. Does chronic daily headache arise de novo in association with regular use of analgesics? Headache. 2003;43(3):179–190. doi:10.1046/j.1526-4610.2003.03041.x
8. Yu S, Liu R, Yang X, et al. Body mass index and migraine: a survey of the Chinese adult population. J Headache Pain. 2012;13(7):531–536. doi:10.1007/s10194-012-0470-5
9. Dandona P, Aljada A, Bandyopadhyay A. Inflammation: the link between insulin resistance, obesity and diabetes. Trends Immunol. 2004;25(1):4–7. doi:10.1016/j.it.2003.10.013
10. Zelissen PM, Koppeschaar HP, Lips CJ, Hackeng WH. Calcitonin gene-related peptide in human obesity. Peptides. 1991;12(4):861–863. doi:10.1016/0196-9781(91)90147-H
11. Marics B, Peitl B, Varga A, et al. Diet-induced obesity alters dural CGRP release and potentiates TRPA1-mediated trigeminovascular responses. Cephalalgia. 2017;37(6):581–591. doi:10.1177/0333102416654883
12. Kyle UG, Bosaeus I, De Lorenzo AD, et al. Bioelectrical impedance analysis--part I: review of principles and methods. Clin Nutr. 2004;23(5):1226–1243. doi:10.1016/j.clnu.2004.06.004
13. Huang WJ, Ko CY. A trend of high-fat and low-carbohydrate oral nutritional supplements on body composition and handgrip strength in individuals with chronic obstructive pulmonary disease. Current Topics Nutraceutical Res. 2023;22(1):39–44. doi:10.37290/ctnr2641-452X.22:39-44
14. Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76–87. doi:10.1016/S1474-4422(16)30293-9
15. Pavlović JM, Allshouse AA, Santoro NF, et al. Sex hormones in women with and without migraine: evidence of migraine-specific hormone profiles. Neurology. 2016;87(1):49–56. doi:10.1212/WNL.0000000000002798
16. Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41(7):646–657. doi:10.1046/j.1526-4610.2001.041007646.x
17. Radtke A, Neuhauser H. Prevalence and burden of headache and migraine in Germany. Headache. 2009;49(1):79–89. doi:10.1111/j.1526-4610.2008.01263.x
18. Franconi F, Finocchi C, Allais G, et al. Gender and triptan efficacy: a pooled analysis of three double-blind, randomized, crossover, multicenter, Italian studies comparing frovatriptan vs. other triptans. Neurol Sci. 2014;35(Suppl 1):99–105. doi:10.1007/s10072-014-1750-4
19. Irwin MR, Witarama T, Caudill M, Olmstead R, Breen EC. Sleep loss activates cellular inflammation and signal transducer and activator of transcription (STAT) family proteins in humans. Brain Behav Immun. 2015;47:86–92. doi:10.1016/j.bbi.2014.09.017
20. Victor TW, Hu X, Campbell J, White RE, Buse DC, Lipton RB. Association between migraine, anxiety and depression. Cephalalgia. 2010;30(5):567–575. doi:10.1111/j.1468-2982.2009.01944.x
21. Cappuccio FP, Taggart FM, Kandala NB, et al. Meta-analysis of short sleep duration and obesity in children and adults. Sleep. 2008;31(5):619–626. doi:10.1093/sleep/31.5.619
22. Palacios-Ceña M, Fernández-Muñoz JJ, Castaldo M, et al. The association of headache frequency with pain interference and the burden of disease is mediated by depression and sleep quality, but not anxiety, in chronic tension type headache. J Headache Pain. 2017;18(1):19. doi:10.1186/s10194-017-0730-5
23. Solovieva S, Lallukka T, Virtanen M, Viikari-Juntura E. Psychosocial factors at work, long work hours, and obesity: a systematic review. Scand J Work Environ Health. 2013;39(3):241–258. doi:10.5271/sjweh.3364
24. Amin FM, Aristeidou S, Baraldi C, et al. The association between migraine and physical exercise. J Headache Pain. 2018;19(1):83. doi:10.1186/s10194-018-0902-y
25. Kristoffersen ES, Børte S, Hagen K, Zwart JA, Winsvold BS. Migraine, obesity and body fat distribution - A population-based study. J Headache Pain. 2020;21(1):97. doi:10.1186/s10194-020-01163-w
26. Santos IS, Goulart AC, Passos VM, Molina Mdel C, Lotufo PA, Bensenor IM. Obesity, abdominal obesity and migraine: a cross-sectional analysis of ELSA-Brasil baseline data. Cephalalgia. 2015;35(5):426–436. doi:10.1177/0333102414544978
27. Peterlin BL, Rosso AL, Rapoport AM, Scher AI. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50(1):52–62. doi:10.1111/j.1526-4610.2009.01459.x
28. Bigal ME, Liberman JN, Lipton RB. Obesity and migraine: a population study. Neurology. 2006;66(4):545–550. doi:10.1212/01.wnl.0000197218.05284.82
29. Ramachandran R. Neurogenic inflammation and its role in migraine. Semin Immunopathol. 2018;40(3):301–314. doi:10.1007/s00281-018-0676-y
30. Eftekhari S, Salvatore CA, Johansson S, Chen TB, Zeng Z, Edvinsson L. Localization of CGRP, CGRP receptor, PACAP and glutamate in trigeminal ganglion. Relation to the blood-brain barrier. Brain Res. 2015;1600:93–109. doi:10.1016/j.brainres.2014.11.031
31. Kitamura E, Kanazawa N, Hamada J. Hyperleptinemia increases the susceptibility of the cortex to generate cortical spreading depression. Cephalalgia. 2015;35(4):327–334. doi:10.1177/0333102414540813
32. Thuraiaiyah J, Erritzøe-Jervild M, Al-Khazali HM, Schytz HW, Younis S. The role of cytokines in migraine: a systematic review. Cephalalgia. 2022;42(14):1565–1588. doi:10.1177/03331024221118924
33. Chen SP, Qin T, Seidel JL, et al. Inhibition of the P2X7-PANX1 complex suppresses spreading depolarization and neuroinflammation. Brain. 2017;140(6):1643–1656. doi:10.1093/brain/awx085
34. Takeda M, Tanimoto T, Kadoi J, et al. Enhanced excitability of nociceptive trigeminal ganglion neurons by satellite glial cytokine following peripheral inflammation. Pain. 2007;129(1–2):155–166. doi:10.1016/j.pain.2006.10.007
35. Bigal ME, Lipton RB. Modifiable risk factors for migraine progression. Headache. 2006;46(9):1334–1343. doi:10.1111/j.1526-4610.2006.00577.x
36. Edvinsson L, Haanes KA, Warfvinge K. Does inflammation have a role in migraine? Nat Rev Neurol. 2019;15(8):483–490. doi:10.1038/s41582-019-0216-y
37. Perini F, D’Andrea G, Galloni E, et al. Plasma cytokine levels in migraineurs and controls. Headache. 2005;45(7):926–931. doi:10.1111/j.1526-4610.2005.05135.x
38. Hauner H. Secretory factors from human adipose tissue and their functional role. Proc Nutr Soc. 2005;64(2):163–169. doi:10.1079/PNS2005428
39. Park HS, Park JY, Yu R. Relationship of obesity and visceral adiposity with serum concentrations of CRP, TNF-alpha and IL-6. Diabet Res Clin Pract. 2005;69(1):29–35. doi:10.1016/j.diabres.2004.11.007
40. Peterlin BL. The role of the adipocytokines adiponectin and leptin in migraine. J Am Osteopath Assoc. 2009;109(6):314–317.
41. Jabłonowska-Lietz B, Wrzosek M, Włodarczyk M, Nowicka G. New indexes of body fat distribution, visceral adiposity index, body adiposity index, waist-to-height ratio, and metabolic disturbances in the obese. Kardiol Pol. 2017;75(11):1185–1191. doi:10.5603/KP.a2017.0149
42. Yu BL, Zhao SP, Hu JR. Cholesterol imbalance in adipocytes: a possible mechanism of adipocytes dysfunction in obesity. Obes Rev. 2010;11(8):560–567.
43. Kwo PY, Cohen SM, Lim JK. ACG clinical guideline: evaluation of abnormal liver chemistries. Am J Gastroenterol. 2017;112(1):18–35. doi:10.1038/ajg.2016.517
44. Westgate CSJ, Israelsen IME, Jensen RH, Eftekhari S. Understanding the link between obesity and headache- with focus on migraine and idiopathic intracranial hypertension. J Headache Pain. 2021;22(1):123. doi:10.1186/s10194-021-01337-0
45. Batsis JA, Mackenzie TA, Bartels SJ, Sahakyan KR, Somers VK, Lopez-Jimenez F. Diagnostic accuracy of body mass index to identify obesity in older adults: NHANES 1999–2004. Int J Obes. 2016;40(5):761–767. doi:10.1038/ijo.2015.243
46. Blau JN. Migraine prodromes separated from the aura: complete migraine. Br Med J. 1980;281(6241):658–660. doi:10.1136/bmj.281.6241.658
47. Denuelle M, Fabre N, Payoux P, Chollet F, Geraud G. Hypothalamic activation in spontaneous migraine attacks. Headache. 2007;47(10):1418–1426. doi:10.1111/j.1526-4610.2007.00776.x
48. Puledda F, Silva EM, Suwanlaong K, Goadsby PJ. Migraine: from pathophysiology to treatment. J Neurol. 2023;270(7):3654–3666. doi:10.1007/s00415-023-11706-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Liraglutide on Fat Mass Percentage Among Overweight and Obese Adults with Type 2 Diabetes: A Systematic Review
Aladel A, Aljaouni J, Basaad R
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3381-3391
Published Date: 27 October 2023
Effect of Weight Loss on the Apnea Hypopnea Index is Related to Waist Circumference in Chinese Adults with Overweight and Obesity
Ren Y, Cui X, Zhu X, Guo H, Zhou Q, Yuan P, Cheng H, Wu W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:453-463
Published Date: 27 January 2024
Effect of SophorOx® on Oxidative Stress and Body Composition in Individuals with High BMI: A Randomized Controlled Trial
Roza JM, Srivastava S
Diabetes, Metabolic Syndrome and Obesity 2024, 17:2221-2234
Published Date: 5 June 2024
Progressive Weight Loss-Induced Remission of Insulin Resistance/Hyperinsulinemia and Improvements in Cardiovascular Risk Factors
Leng M, Guo X, Wei C, Zhang Y, Li Z, Gao X, Hou D, Li C
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1099-1110
Published Date: 15 April 2025