Back to Journals » Journal of Pain Research » Volume 12
Microvascular decompression and radiofrequency for the treatment of trigeminal neuralgia: a meta-analysis
Authors Li Y ![]() , Yang L, Ni J, Dou Z
, Yang L, Ni J, Dou Z ![]()
Received 30 January 2019
Accepted for publication 28 May 2019
Published 28 June 2019 Volume 2019:12 Pages 1937—1945
DOI https://doi.org/10.2147/JPR.S203141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Yan Li,1–3 Liqiang Yang,1,2 Jiaxiang Ni,1,2 Zhi Dou1,2
1Department of Pain Management, Xuanwu Hospital, Capital Medical University, Beijing 100053, People’s Republic of China; 2National Center for Clinical Medicine of Geriatric Diseases, Beijing 100053, People’s Republic of China; 3Center for Anesthesiology, Beijing Anzhen Hospital, Capital Medical University, Beijing 100029, People’s Republic of China
Purpose: Surgical treatments are used for trigeminal neuralgia (TN) when drug treatment fails. Surgical options can be divided into two categories: ablation (destructive) or non-ablation. Microvascular decompression (MVD) is primarily a non-ablation option, while radiofrequency thermocoagulation/rhizotomy (RF) is an ablation option. The aim of this study was to compare outcomes of MVD versus RF in the treatment of TN.
Materials and methods: This article evaluates the clinical results and economic effectiveness of trigeminal nerve RF and MVD for the treatment of TN. This review was conducted according to the methodological standards described in the Cochrane Handbook for Systematic Reviews of Interventions and the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement. The PubMed, Embase and Cochrane libraries were searched in January 2018. We have registered our review at the Review Registry.
Results: Nine studies were included in this review. The sample size was 2163 participants. The results showed that compared with RF, MVD had a lower risk of requiring a secondary procedure. The MVD group also had a lower risk of facial numbness. There was no significant difference in postoperative medication use between the two groups. Compared to RF, MVD was more likely to increase the risk of hypacusis and hypesthesia and to decrease the risk of facial pain and dysesthesia. The total cost of MVD, including the operation, hospital stay and additional procedures, was much higher than that of RF.
Conclusion: MVD had a lower risk of requiring a secondary procedure and facial numbness after surgery. RF could be considered in patients who are unfit for MVD or refused invasive treatment.
Keywords: meta-analysis, facial pain, surgical treatment
Plain language summary
Microvascular decompression (MVD) and radiofrequency thermocoagulation/rhizotomy (RF) are the two main surgical treatments for trigeminal neuralgia. In this article, we compared the efficacy and safety of these two methods. We found that MVD was associated with better efficacy, but greater postoperative complications and total costs compared to RF.
Introduction
Trigeminal neuralgia (TN) is defined as “sudden, usually unilateral, severe, brief, stabbing recurrent pains in the distribution of one or more branches of the fifth cranial nerve” by the International Association for the Study of Pain (IASP).1 Although drug therapy is the first-line treatment for TN, surgical intervention is an important alternative treatment in patients with refractory TN or intolerable side effects. Surgical intervention for the treatment of TN falls into two categories: non-ablation and ablation.2
The classic non-ablation technique for the treatment of TN is microvascular decompression (MVD), which is based on the neurovascular compression hypothesis first described by Dandy. MVD was first performed by Gardner in 1959 and then popularized by Janetta, and it has been considered the gold standard for TN treatment for nearly 60 years.3 MVD requires the separation of the trigeminal nerve from the adjacent vessels through a craniotomy under general anesthesia. Although MVD is considered a classic procedure for the treatment of TN, complications such as postoperative facial numbness, intracranial hemorrhage, cerebrospinal fluid leakage, and deafness may occur due to possible trauma resulting from the craniotomy. And some long term observational studies noticed that the recurrence rate increases significantly 5 years after MVD.4 Ablation refers to palliative destructive procedures involving controlled damage to the trigeminal gasserian ganglion or the peripheral branch of the trigeminal nerve with the aim of relieving pain. They can be performed for TN arising from any cause, including non-vascular decompression.5 Several methods of ablation have been developed over the past few decades. Radiofrequency thermocoagulation (RF) for TN involves puncturing the semilunar ganglion or trigeminal nerve branch with a CT- or X-ray-guided a RF ablation needle. Sensory and motor stimulation are used to replicate the patient’s pain and locate and destroy the responsible nerve. Recurrence is possible after RF ablation; some patients need to continue medication treatment, while others may require reoperation, and postoperative facial numbness is a notable problem. Glycerol and balloon compression can also be used for trigeminal gasserian ganglion ablation, however, they have poorer selectivity compared with RF.2 Gamma Knife is another ablation strategy aimed to selectively destroy the afferent fibers of trigeminal nerve, although it takes nearly a month for the completely work. In this meta-analysis, we chose the two widely used procedures, MVD and RF, to compare the efficacy and economic effectiveness of them for the treatment of TN.
Materials and methods
This review was conducted according to the methodological standards described in the Cochrane Handbook for Systematic Reviews of Interventions6 and the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) statement.7 This work has been reported in line with AMSTAR (Assessing the methodological quality of systematic reviews) Guidelines. We have registered our research at https://www.researchregistry.com.
The study name is Microvascular Decompression and Radiofrequency for the Treatment of Trigeminal Neuralgia: A Meta-Analysis.
Literature search
Studies were searched in three electronic databases (PubMed, Embase and Cochrane Library) in January 2018. Keywords were determined through expert opinion, Medical Subject Headings and Excerpta Medica Trees, and reviews of the primary search results. The search strategies were developed by information specialists and are presented in Supplement 1.
Selection criteria
We defined the inclusion criteria as follows: (1) Population (P): all patients who were diagnosed with TN; (2) Intervention (I) and comparisons (C): MVD versus RF thermocoagulation or rhizotomy; (3) Outcomes (O): the need for additional procedures after surgery, facial numbness, postoperative use of medication, incidence of any adverse events and specific adverse events, and total costs of intervention. (4) Study design (S): controlled studies.
Data extraction and risk of bias assessment
The data extraction form was developed and adapted by a pilot data extraction. The following items were extracted: first author, year of publication, total number of participants, length of follow up, patient characteristics (treated/newly diagnosed, age, gender distribution, pain score at baseline, side affected by TN), comparisons, numeric data for pre-defined outcomes and information relevant to risk of bias. Two authors extracted the data independently. Disagreements were resolved by consensus between the two authors or by consulting a third author when necessary.
The risk of bias of the included studies was assessed using the Newcastle-Ottawa Quality Assessment Scale Cohort Studies.8 Three domains of risk of bias were assessed: selection bias, comparability of exposure and non-exposure groups and detection/attrition bias relevant to outcomes.
Statistical analysis
RevMan 5.3 was used for statistical analysis. For dichotomous data, we used relative risk (RR) and 95% confidence intervals (CI) as the measurements of the pooled effect; for continuous data, the mean difference (MD) and 95% CI were used. The statistical heterogeneity of the studies’ measured effects was evaluated using P-values derived from the chi square test and I2 statistic. We considered heterogeneity statistically significant when the P-value was <0.1 and I2 was ≥50%. We used a random effects model for all meta-analyses. When significant heterogeneity was present, a sensitivity analysis was carried out to explore the sources of heterogeneity. A subgroup analysis was conducted if the source was identified. “Leave-one-out” sensitivity analyses were conducted to detect the influence of a single study on the overall estimate.
Results
Study selection and study characteristics
The initial search identified 426 references; after duplicates were removed, 374 references were screened by viewing their titles and abstracts. After the first-level screening, 34 full texts were inspected for eligibility. Finally, 25 studies were excluded, and the 9 remaining studies9–17 were included in this review. (Figure 1)
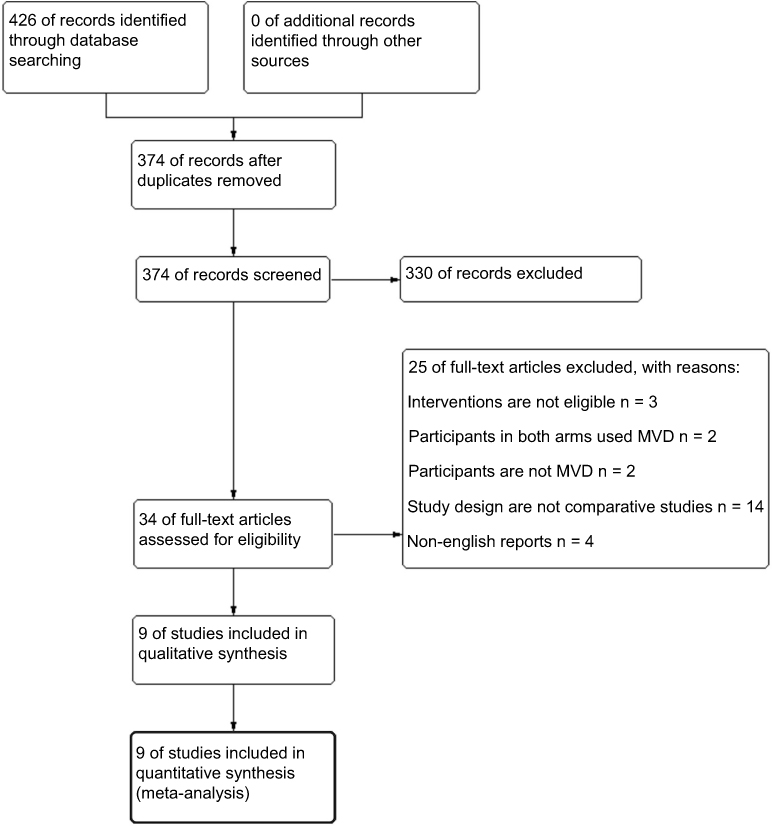 |
Figure 1 Study screening flow diagram. |
For the 9 included studies,9–17 the sample sizes ranged from 50 to 759, and a total of 2163 participants were included. All the participants were diagnosed with TN. The ages of the included participants ranged from 20 to 90 years, and the average age of the participants in each study varied from 50 to 76.2 years. There were 2 studies only noted the outcome events while not mentioned the follow up period. The follow-up of the other 7 studies ranged from 16 months to 14 years. All studies compared MVD (835 participants) with RF rhizotomy or thermocoagulation (1328 participants). Table 1 lists the study characteristics in detail.
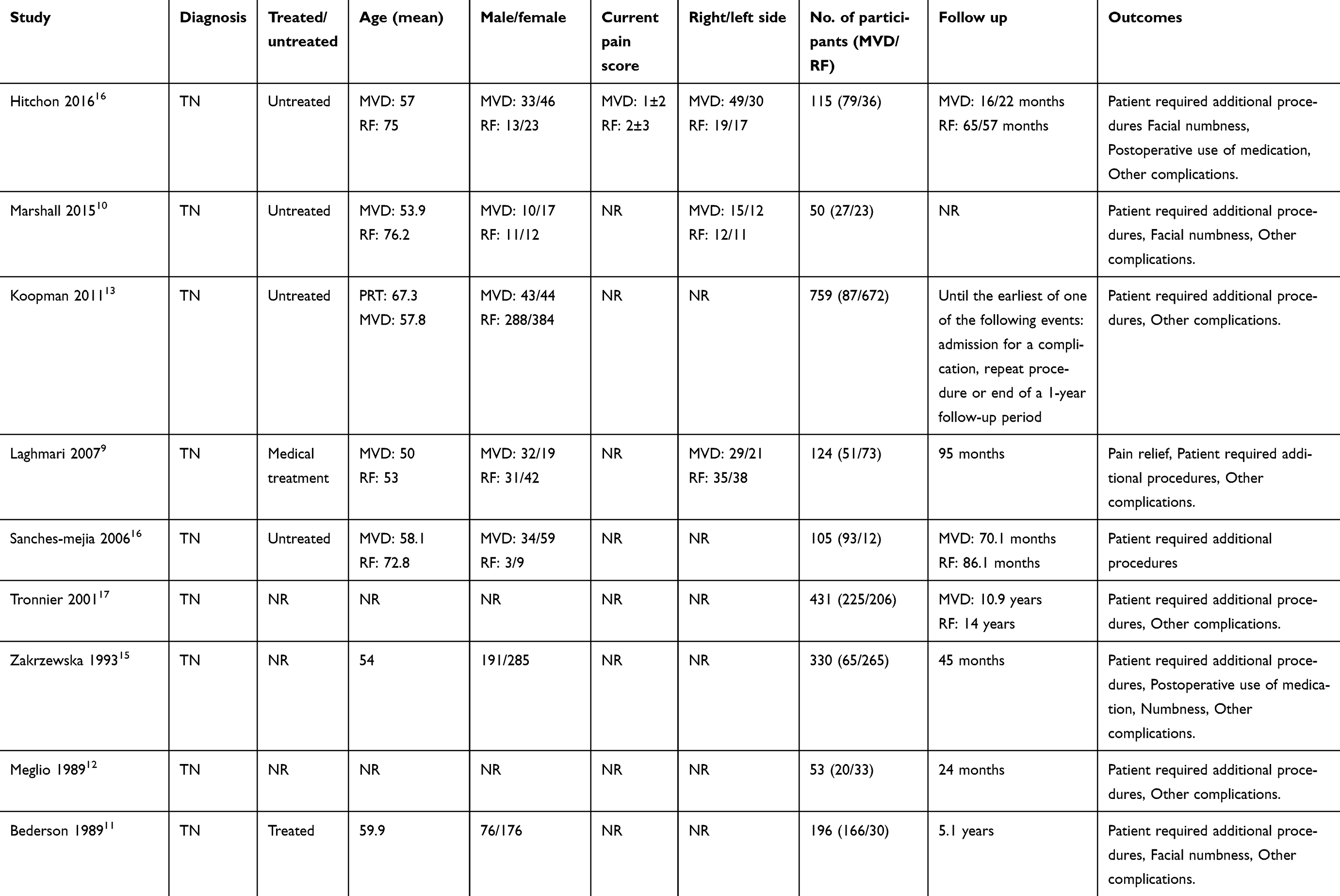 |
Table 1 Study characteristics |
Risk of bias assessment
The included studies were assigned ratings of 3 to 7 stars. Overall, the representativeness of the exposed and non-exposed cohorts and the ascertainment of exposure were good in all the included studies. However, the comparability between groups was not good as the studies were non-randomized. The baseline characteristics of the participants were not balanced between groups. The attrition rates of the included studies were not high. The details of the risk of bias assessment are presented in Supplement 2.
Meta-analysis results
Number of patients requiring additional procedures after surgery
Eight studies9–16 with 1640 participants reported this outcome. The results indicated that MVD reduced the risk of requiring a secondary procedure after surgery compared with RF (RR 0.33, 95% CI 0.19 to 0.56, I2=67%, Figure 2). We explored the sources of heterogeneity but failed to identify an explanation. However, we tested the influence of each study with a sensitivity analysis. The results showed that the pooled effect was robust and did not differ considerably after each study was removed.
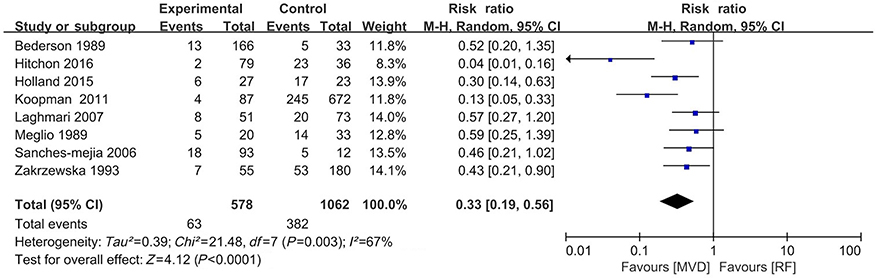 |
Figure 2 Forest plot of the number of patients requiring additional procedures after surgery. Abbreviations: MVD, microvascular decompression; RF, radiofrequency thermocoagulation and rhizotomy; RR, risk ratio; CI, confidence interval. |
Facial numbness
Four studies10,11,14,15 with 599 participants contributed data for this analysis. The participants in the MVD group had a lower risk of facial numbness than those in the RF group (RR 0.27, 95% CI 0.19 to 0.39, I2=0%, Figure 3). We did not identify significant statistical heterogeneity. When each study was removed individually from the meta-analysis, the results still favor the MVD group with a lower risk of facial numbness.
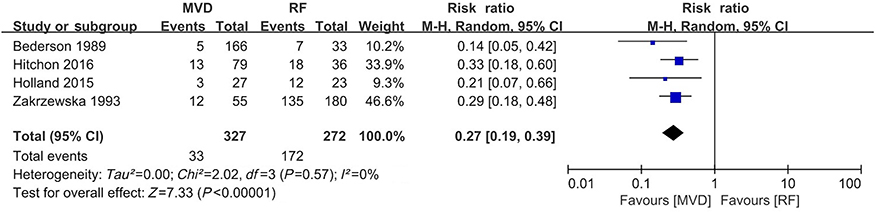 |
Figure 3 Forest plot of facial numbness. Abbreviations: MVD, microvascular decompression; RF, radiofrequency thermocoagulation and rhizotomy; RR, risk ratio; CI, confidence interval. |
Postoperative use of medication
Only two studies14,15 with 350 participants reported this outcome. There was no significant difference between the two groups (RR 0.34, 95%CI 0.06 to 1.86, I2=82%, Figure 4). The statistical heterogeneity was significant, but the source of the heterogeneity was unclear. The sensitivity analysis also showed an unstable pooled effect; when either study was removed, the result became statistically significant in favor of MVD, with fewer events of postoperative medication use.
 |
Figure 4 Forest plot of postoperative use of medication. Abbreviations: MVD, microvascular decompression; RF, radiofrequency thermocoagulation and rhizotomy; RR, risk ratio; CI, confidence interval. |
Incidence of any adverse events and specific adverse events
Four studies9,10,13,14 with 1048 participants reported the incidence of any adverse events. A higher risk of adverse events was observed in the MVD group than in the RF group (RR 2.25, 95%CI 1.13 to 4.48, I2=0%, Figure 5). We did not identify significant statistical heterogeneity. The sensitivity analysis did not show a robust result. When either Holland et al.10 or Koopman et al.13 was removed, the meta-analysis showed no difference between the groups.
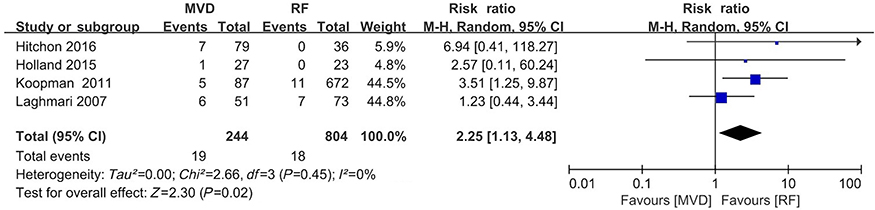 |
Figure 5 Forest plot of the incidence of any adverse events and specific adverse events. Abbreviations: MVD, microvascular decompression; RF, radiofrequency thermocoagulation and rhizotomy; RR, risk ratio; CI, confidence interval. |
Other specific adverse events included spinal fluid leakage from the incision, meningitis, headache and nausea, pulmonary embolism, keratitis, ipsilateral numbness, hearing loss, facial nerve palsy, facial pain, hypacusis, hypesthesia, herpes labialis and so on. MVD showed an increased risk of hypacusis but a decreased risk of hypesthesia compared to RF.
Total cost of intervention
Two studies10,14 with 218 participants reported this outcome. Holland just calculated the total cost of the initial index treatment including physician charges and hospital charges. However, in Hitchon’s study, the cost of additional procedures was also summated into total charges with the follow-up of 32±46 months. The total cost of MVD was much higher than that of RF (MD $37,190, 95% CI $19,900 to $54,470, I2=91%, Figure 6).
 |
Figure 6 Forest plot of the total cost of intervention. Abbreviations: MVD, microvascular decompression; RF, radiofrequency thermocoagulation and rhizotomy; RR, risk ratio; CI, confidence interval. |
Discussion
Summary of main findings
In this study, we performed a meta-analysis to compare the clinical outcomes of MVD and RF used as the first surgery for TN. Overall, MVD was associated with a greater rate of freedom from pain and lower incidences of facial numbness, but greater postoperative complications and total costs compared to RF.
Epidemiology and pathophysiology of TN
TN is characterized by paroxysms of unilateral, severe electric shock-like pain along the trigeminal nerve divisions. It can be triggered by common activities, such as eating, talking, brushing teeth, and so on.18 It is estimated that approximately 1 per 5,500 people worldwide suffer from TN; the morbidity is higher among females than males, and it increases with age.19,20 At present, the cause of TN is still controversial. The most common view is that vascular compression is involved in the pathogenesis of TN.21,22
Efficacy analysis
In the studies that we included, most investigators reported the need for additional procedures as an outcome. We found that MVD reduced the risk of needing a secondary procedure after surgery compared with RF (RR 0.33, 95% CI 0.19 to 0.56, I2=67%), indicating that MVD is superior to RF in terms of pain recurrence.23 These results are not dissimilar to those in the literature showing that MVD provides an approximately 80% chance of being pain-free, with a recurrence rate of approximately 10% over 10–20 years,24,25 whereas RF patients report pain-free results of 80% at 1 year after treatment, 75% at 3 years, and 73% at 5 years.26
Although the postoperative medication usage analysis did not show any significant difference between the two procedures, it is unlikely that MVD and RF are equally efficient. Because only two studies (n=350) were included in these analyses, we cannot draw firm conclusions. Given that the most common origin of TN pain is nerve compression, it stands to reason that the pain will be more effectively treated directly, with open MVD, than with minimally invasive RF.9,27 However, surgical interventions are selected via discussions between the patient and the surgeon on a case-by-case basis. Patients who undergo MVD are often younger, healthier, and have fewer comorbidities.28,29 These patient characteristics may also affect the outcomes of these two procedures. Consider that, this evidence drawn out based on limited studies was uncertain and further investigation of efficacy analysis was needed.
Facial numbness
This study found that RF had a greater association with facial numbness than MVD did, which is consistent with Tatli’s findings.30 Compared with MVD, RF carries a specific risk of facial numbness as an extension of its therapeutic mechanism; additionally, there seems to be a correlation between pain relief and the intensity of facial numbness. The sensory branches of the trigeminal nerve are composed of different types of sensory nerve fibers, including unmyelinated c fibers, which transmit nociceptive signals, and myelinated Aα and Aβ fibers, which conduct tactile sensations.31,32 In clinical practice, it is difficult to realize the highly selective ablation of pain conduction c fibers without damaging Aα and Aβ fibers, which are the main cause of postoperative facial numbness. However, although the permanent facial numbness (mainly hypesthesia, although paresthesias have also been described) is common, it seems to be tolerable to most patients.33,34 Moreover, clinicians have found choosing an appropriate thermocoagulation temperature, can balance the intensity of RF-related facial numbness and pain relief.35 Therefore, we considered that the cause of facial numbness is not the most important factor in the choice of preferred treatment.
Other complications
As an invasive procedure, MVD has been widely reported to have greater surgical risks than RF, including cerebrospinal fluid leak, wound infection, cranial venous sinus thrombosis, hearing loss, pneumonia, facial paresis, and stroke.30,36–38 In our study, a higher risk of adverse events was also observed in the MVD group, but with the exceptions of hypacusis and hypesthesia, we could not find significant differences of any other complications between MVD and RF. Possible complications may not have been reported either because they did not occur or because the investigators did not classify them as side effects. Moreover, we could not analyze the temporal evolution of side effects because many studies did not report the time course (transient or permanent) of the complications. Given the safety and fair success rate of RF, many surgeons prefer this procedure for their elderly patients.34,39–41 While the results are overwhelmingly promising, the protocol of same-day discharge and follow-up by external clinicians after RF may lead to an underreporting of its complications.
Two of the included studies provided cost-effectiveness analyses. The results showed that these two procedures may differ in total cost by a large degree. Holland described a savings of $27,000 to $42,000 per patient for patients who underwent RF compared with MVD.10 Hitchon performed an in-depth, decision-based cost-effectiveness analysis, which concluded that although the total charges for subsequent procedures in the RF group increased over time but remained lower than the cost of MVD.14
Strengths and limitations of the review
The current study has several strengths. We followed the Cochrane standards to conduct this review. Bias was well controlled during the process of conducting the review. Our search strategy was developed by an information specialist, which allowed us to identify as many relevant studies as possible. The study selection, data extraction and risk of bias assessment were performed by two independent reviewers.
However, the poor comparability between groups may limit the reliability of the meta-analysis. Because this analysis is based on previously reported data, it may have imported bias from the studies that were included. The number of patients was not balanced between the MVD and RF groups. In addition, the patients in our study were not matched according to age, gender, affected trigeminal branch, or the specific vessel involved. Most articles used their own scales to measure treatment success and pain relief, thus leaving the results open to interpretation and causing stratification problems during the analytic process. Furthermore, with the development of intraoperative electrophysiological monitoring in recent years, the associated complications can be theoretically reduced in these two therapies.42,43 Consequently, the present analysis shows the need for improved study protocols to increase the current level of evidence.
Conclusion
MVD yields better pain relief efficacy than RF. The risks and side effects of the 2 treatment modalities should be carefully weighed. Although the surgical complications associated with MVD are not negligible and total costs of MVD are much more than RF, facial numbness after RF may also compromise the patient’s quality of life. For patients without specific surgical contraindications, MVD is a better option as the surgical treatment for TN; otherwise, RF could be used as an alternative therapy.
Disclaimer
The poor comparability between groups and limited studies may diminish the reliability of the meta-analysis. Further investigations should be done in order to increase the current level of evidence.
Acknowledgments
This work was supported by China Postdoctoral Science Foundation (2019M650769), Beijing Postdoctoral Research Foundation (2018-ZZ-108,2018) and Beijing Municipal Administration of Hospitals Clinical Medicine Development of Special Funding Support (ZYLX201810).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zakrzewska JM, McMillan R. Trigeminal neuralgia: the diagnosis and management of this excruciating and poorly understood facial pain. Postgrad Med J. 2011;87(1028):410–416. doi:10.1136/pgmj.2009.080473
2. Zakrzewska JM, Akram H. Neurosurgical Interventions for the Treatment of Classical Trigeminal Neuralgia. Hoboken, NJ: John Wiley & Sons, Ltd; 2008.
3. Adams CB. Microvascular compression: an alternative view and hypothesis. J Neurosurg. 1989;70(1):1–12. doi:10.3171/jns.1989.70.1.0001
4. Barker FG, Jannetta PJ, Bissonette DJ, Larkins MV, Jho HD. The long-term outcome of microvascular decompression for trigeminal neuralgia. New England J Med. 1996;334(17):1077–1084. doi:10.1056/NEJM199604253341701
5. Bakker N, Wagemakers M, Beese U, Metzemaekers J. Treatment of trigeminal neuralgia. Ned Tijdschr Geneeskd. 2014;158:A7468.
6. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [Updated March 2011]. London, UK: The Cochrane Collaboration; 2011.
7. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2651
8. Wells GA, Shea B, O’connell D, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses.Ottawa, ON: Ottawa Hospital Research Institute; 2009. Accessed March, 2016.
9. Laghmari M, El Ouahabi A, Arkha Y, Derraz S, El Khamlichi A. Are the destructive neurosurgical techniques as effective as microvascular decompression in the management of trigeminal neuralgia? Surg Neurol. 2007;68(5):505–512. doi:10.1016/j.surneu.2006.11.066
10. Holland M, Noeller J, Buatti J, He W, Shivapour ET, Hitchon PW. The cost-effectiveness of surgery for trigeminal neuralgia in surgically naive patients: a retrospective study. Clin Neurol Neurosurg. 2015;137:34–37. doi:10.1016/j.clineuro.2015.06.011
11. Bederson JB, Wilson CB. Evaluation of microvascular decompression and partial sensory rhizotomy in 252 cases of trigeminal neuralgia. J Neurosurg. 1989;71(3):359–367. doi:10.3171/jns.1989.71.3.0359
12. Meglio M, Cioni B, Moles A, Visocchi M. Microvascular decompression versus percutaneous procedures for typical trigeminal neuralgia: personal experience. Stereotact Funct Neurosurg. 1990;54–55:76–79. doi:10.1159/000100194
13. Koopman JS, de Vries LM, Dieleman JP, Huygen FJ, Stricker BH, Sturkenboom MC. A nationwide study of three invasive treatments for trigeminal neuralgia. Pain. 2011;152(3):507–513. doi:10.1016/j.pain.2011.02.053
14. Hitchon PW, Holland M, Noeller J, et al. Options in treating trigeminal neuralgia: experience with 195 patients. Clin Neurol Neurosurg. 2016;149:166–170. doi:10.1016/j.clineuro.2016.08.016
15. Zakrzewska JM, Thomas DG. Patient’s assessment of outcome after three surgical procedures for the management of trigeminal neuralgia. Acta Neurochir. 1993;122(3–4):225–230. doi:10.1007/BF01405533
16. Sanchez-Mejia RO, Limbo M, Cheng JS, Quintana JC, Ward MM, Barbaro NM. Ronald tasker award: retreatment of medically refractory trigeminal neuralgia. Clin Neurosurg. 2006;53:313–315.
17. Tronnier VM, Rasche D, Hamer J, Kienle AL, Kunze S. Treatment of idiopathic trigeminal neuralgia: comparison of long-term outcome after radiofrequency rhizotomy and microvascular decompression. Neurosurgery. 2001;48(6):
18. Devor M, Amir R, Rappaport ZH. Pathophysiology of trigeminal neuralgia: the ignition hypothesis. Clin J Pain. 2002;18(1):4–13. doi:10.1097/00002508-200201000-00002
19. Rothman KJ, Monson RR. Epidemiology of trigeminal neuralgia. J Chronic Dis. 1973;26(1):3–12. doi:10.1016/0021-9681(73)90075-1
20. Katusic S, Williams DB, Beard CM, Bergstralh EJ, Kurland LT. Epidemiology and clinical features of idiopathic trigeminal neuralgia and glossopharyngeal neuralgia: similarities and differences, Rochester, Minnesota, 1945–1984. Neuroepidemiology. 1991;10(5–6):276–281. doi:10.1159/000110284
21. Obermann M, Holle D, Katsarava Z. Trigeminal neuralgia and persistent idiopathic facial pain. Expert Rev Neurother. 2011;11(11):1619–1629. doi:10.1586/ern.11.156
22. Maarbjerg S, Di Stefano G, Bendtsen L, Cruccu G. Trigeminal neuralgia–diagnosis and treatment. Cephalalgia. 2017;37(7):648–657. doi:10.1177/0333102416687280
23. Liang X, Dong X, Zhao S, Ying X, Du Y, Yu W. A retrospective study of neurocombing for the treatment of trigeminal neuralgia without neurovascular compression. Ir J Med Sci. 2017;186(4):1033–1039. doi:10.1007/s11845-017-1581-4
24. Zhang H, Lei D, You C, Mao BY, Wu B, Fang Y. The long-term outcome predictors of pure microvascular decompression for primary trigeminal neuralgia. World Neurosurg. 2013;79(5–6):756–762. doi:10.1016/j.wneu.2012.01.040
25. Sarsam Z, Garcia-Fiñana M, Nurmikko TJ, Varma TR, Eldridge P. The long-term outcome of microvascular decompression for trigeminal neuralgia. Br J Neurosurg. 2010;24(1):18–25. doi:10.3109/02688690903370289
26. Obermann M. Treatment options in trigeminal neuralgia. Ther Adv Neurol Disord. 2010;3(2):107–115. doi:10.1177/1756285609359317
27. Kabatas S, Karasu A, Civelek E, Sabanci AP, Hepgul KT, Teng YD. Microvascular decompression as a surgical management for trigeminal neuralgia: long-term follow-up and review of the literature. Neurosurg Rev. 2009;32(1):87–93. doi:10.1007/s10143-008-0171-3
28. Jodicke A, Winking M, Deinsberger W, Boker DK. Microvascular decompression as treatment of trigeminal neuralgia in the elderly patient. Minim Invasive Neurosurg. 1999;42(2):92–96. doi:10.1055/s-2008-1053379
29. Copeland B. Microvascular decompression for trigeminal neuralgia in the elderly: a review of the safety and efficacy. Neurosurgery. 2006;58(4):E799. doi:10.1097/00006123-200604000-00033
30. Tatli M, Satici O, Kanpolat Y, Sindou M. Various surgical modalities for trigeminal neuralgia: literature study of respective long-term outcomes. Acta Neurochir. 2008;150(3):243–255. doi:10.1007/s00701-007-1463-z
31. Lin W, Zhu WP, Chen YL, et al. Large-diameter compression arteries as a possible facilitating factor for trigeminal neuralgia: analysis of axial and radial diffusivity. Acta Neurochir. 2016;158(3):521–526. doi:10.1007/s00701-015-2673-4
32. Li X, Yue J, Yang L, et al. Application of antidromic conduction monitoring in ganglion radiofrequency thermocoagulation for locating trigeminal branches in trigeminal neuralgia. Pain Pract. 2016;16(3):305–310. doi:10.1111/papr.12286
33. Tang YZ, Wu BS, Yang LQ, et al. The long-term effective rate of different branches of idiopathic trigeminal neuralgia after single radiofrequency thermocoagulation: a cohort study. Medicine. 2015;94(45):e1994. doi:10.1097/MD.0000000000001994
34. Tang YZ, Jin D, Bian JJ, Li XY, Lai GH, Ni JX. Long-term outcome of computed tomography-guided percutaneous radiofrequency thermocoagulation for classic trigeminal neuralgia patients older than 70 years. J Craniofac Surg. 2014;25(4):1292–1295. doi:10.1097/SCS.0000000000000591
35. Tang YZ, Yang LQ, Yue JN, Wang XP, He LL, Ni JX. The optimal radiofrequency temperature in radiofrequency thermocoagulation for idiopathic trigeminal neuralgia: a cohort study. Medicine. 2016;95(28):e4103. doi:10.1097/MD.0000000000004864
36. Amagasaki K, Watanabe S, Naemura K, Shono N, Nakaguchi H. Safety of microvascular decompression for elderly patients with trigeminal neuralgia. Clin Neurol Neurosurg. 2016;141:77–81. doi:10.1016/j.clineuro.2015.12.019
37. Xia L, Zhong J, Zhu J, et al. Effectiveness and safety of microvascular decompression surgery for treatment of trigeminal neuralgia: a systematic review. J Craniofac Surg. 2014;25(4):1413–1417. doi:10.1097/SCS.0000000000000984
38. Sekula RF
39. Huang Y, Ni J, Wu B, He M, Yang L, Wang Q. Percutaneous radiofrequency thermocoagulation for the treatment of different types of trigeminal neuralgia: evaluation of quality of life and outcomes. J Huazhong Univ Sci Technolog Med Sci. 2010;30(3):403–407. doi:10.1007/s11596-010-0365-0
40. Liu C, Zhou ZG, Yuan CY. Treatment of primary trigeminal neuralgia with radiofrequency thermocoagulation: report of 648 consecutive cases. Shanghai Kou Qiang Yi Xue. 2012;21(4):466–469.
41. Jin HS, Shin JY, Kim YC, et al. Predictive factors associated with success and failure for radiofrequency thermocoagulation in patients with trigeminal neuralgia. Pain Physician. 2015;18(6):537–545.
42. Zhong J, Zhu J, Sun H, et al. Microvascular decompression surgery: surgical principles and technical nuances based on 4000 cases. Neurol Res. 2014;36(10):882–893. doi:10.1179/1743132814Y.0000000344
43. Zhao YX, Miao SH, Tang YZ, et al. Trigeminal somatosensory-evoked potential: a neurophysiological tool to monitor the extent of lesion of ganglion radiofrequency thermocoagulation in idiopathic trigeminal neuralgia: a case-control study. Medicine. 2017;96(3):e5872. doi:10.1097/MD.0000000000005872
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.