Back to Journals » Clinical Ophthalmology » Volume 18
Micropulse Transscleral Cyclophotocoagulation in Non-Incisional Eyes with Ocular Hypertension and Primary Open-Angle Glaucoma
Authors Murtaza F ![]() , Kaba Q
, Kaba Q ![]() , Somani S
, Somani S ![]() , Tam ES
, Tam ES ![]() , Yuen D
, Yuen D
Received 2 November 2023
Accepted for publication 8 April 2024
Published 11 May 2024 Volume 2024:18 Pages 1295—1312
DOI https://doi.org/10.2147/OPTH.S447875
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fahmeeda Murtaza,1 Qayim Kaba,2 Sohel Somani,3– 5 Eric S Tam,3– 5 Darana Yuen3,4
1Temerty Faculty of Medicine, University of Toronto, Toronto, ON, Canada; 2Cardiff University, Cardiff, Wales, UK; 3Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, ON, Canada; 4Uptown Eye Specialists, Brampton, ON, Canada; 5Division of Ophthalmology, William Osler Health System, Brampton, ON, Canada
Correspondence: Darana Yuen, Uptown Eye Specialists, 401-7900 Hurontario Street, Brampton, ON, L6Y 0P6, Canada, Tel +1 416-292-0330, Fax +1 416-292-0331, Email [email protected]
Purpose: To investigate the safety and effectiveness of micropulse transscleral cyclophotocoagulation (MPTSCPC) in non-incisional eyes with ocular hypertension (OHT) and early, moderate, and severe primary open-angle glaucoma (POAG).
Methods: Retrospective cohort study of eyes that underwent MPTSCPC from 2016 to 2019 at an outpatient clinic in Canada. Eyes were excluded if any incisional procedures, except cataract surgery, were performed prior to MPTSCPC treatment. Laser power ranged from 900 to 2500mW.
Results: A total of 153 eyes from 93 patients were included (OHT n=22; early POAG n=46; moderate POAG n=35; severe POAG n=50). The baseline IOP was 18.37 ± 4.76mmHg in the total cohort. All cohorts experienced a significant mean IOP reduction by final follow-up (total p< 0.001; OHT p=0.003; early POAG p< 0.001; moderate POAG p=0.022; severe POAG p=0.015). Overall, 52.9% of eyes achieved an IOP reduction of ≥ 20% from baseline to final follow-up (OHT 59.1%; early POAG 58.7%; moderate POAG 45.7%; severe POAG 50.0%). There was worsening in best-corrected visual acuity in the total cohort (mean difference=0.11 ± 0.36 logMAR, p=0.11), mostly attributable to cataract progression (34.1% of phakic eyes) and ocular surface disease (7.2%). The number of topical medications and drug classes remained unchanged in the total cohort (p=0.425 and p=0.791, respectively). Twenty-two eyes (14.4%) required retreatment, which provided an additional IOP reduction of 1.26mmHg (p=0.344). By final follow-up, 8 eyes (5.2%) required escalation to incisional procedures.
Conclusion: MPTSCPC is a safe and effective adjunct IOP-lowering treatment in non-incisional eyes with OHT and POAG.
Keywords: micropulse, cyclophotocoagulation, primary open-angle glaucoma, ocular hypertension
Introduction
Primary open-angle glaucoma (POAG) is a progressive optic neuropathy and is the leading cause of irreversible blindness worldwide, with intraocular pressure (IOP) being the only modifiable risk factor.1,2 Large-scale clinical trials have shown that adequate IOP control can reduce the risk of progression from ocular hypertension (OHT) to glaucoma.3–5 In the Early Manifest Glaucoma Trial, every 1 mmHg reduction in IOP was associated with a 10% reduction in glaucoma progression.5 A lower IOP is also associated with stable visual fields.4 IOP management can involve IOP lowering drops, laser treatments, minimally invasive glaucoma surgery, filtration surgery, and glaucoma drainage devices. There is a growing interest in using minimally invasive, non-incisional techniques such as lasers to control IOP.
Transscleral cyclophotocoagulation (TSCPC) is a non-incisional laser procedure that uses infrared light at a wavelength of 810 nm to target melanin in the pigmented ciliary body epithelium at the level of the pars plicata.6,7 This causes a reduction in aqueous humour production, and subsequently, IOP.6,7 TSCPC can be performed using two different modalities: continuous wave (CWTSCPC) and Micropulse (MPTSCPC).
Traditional CWTSCPC, due to its nonselective nature, causes collateral damage to the ciliary body stroma and ciliary muscle, which has been confirmed histologically.8,9 There is also risk of developing serious postoperative complications such as persistent hypotony, persistent ocular inflammation, serous choroidal detachment, cystoid macular edema, phthisis bulbi, and sympathetic ophthalmia. As such, CWTSCPC is mostly reserved for refractory glaucoma and eyes with poor visual potential.
In contrast, MPTSCPC more selectively targets the ciliary body epithelium.6 Laser energy is delivered in repetitive short pulses. The “on” and “off” cycling mode allows energy to reach the coagulative threshold with minimal collateral damage to non-pigmented ciliary body epithelium, the ciliary body stroma, and adjacent tissue.6 As the rates of complications are reportedly lower in comparison to CWTSCPC, MPTSCPC may have a role in treating a broader patient population and potentially be utilized earlier in the glaucoma treatment paradigm.10,11
The majority of published literature on MPTSCPC consists of small case series of eyes with severe or refractory glaucoma, that have poor vision and prior glaucoma surgery at baseline.12–17 A few studies have found MPTSCPC to be safe and effective in treating OHT and primary open-angle glaucoma (POAG), but there remains a paucity of literature on well-seeing eyes with no history of incisional procedures.12–17 This study investigates the safety and effectiveness of MPTSCPC in non-incisional eyes with OHT and early, moderate, and severe POAG.
Methods
This retrospective cohort study was approved by the William Osler Health Systems Research Ethics Board (WOHS REB) and all research adhered to the tenets of the Declaration of Helsinki. Due to the retrospective nature of this study, patient consent to review medical records was not required by the WOHS REB. Patient confidentiality, including the use of de-identified patient data, was maintained at all times.
Patient Selection
All consecutive patients over 18, with a diagnosis of ocular hypertension (OHT) or primary open-angle glaucoma (POAG), who received MPTSCPC treatment between May 2016 and July 2019 at a single outpatient clinic in Ontario, Canada, were included. The following eyes were excluded: eyes with a follow-up of <6 months following MPTSCPC treatment; prior ocular surgeries except cataract extraction and intraocular lens insertion; and any glaucoma laser treatments 6 months prior to initial MPTSCPC treatment.
Baseline Parameters
Baseline parameters included age, sex, ethnicity, POAG severity, previous glaucoma laser treatments, intraocular pressure (IOP) measured by Goldmann applanation tonometry, best-corrected distance visual acuity (BCVA), number and drug classes of topical glaucoma medications. The Canadian Ophthalmological Society clinical practice guidelines were used for staging of OHT and POAG.18 Snellen BCVA was converted to logarithm of the minimum angle of resolution logarithm (logMAR) BCVA. BCVAs of “light perception”, “hand motion”, and “counting fingers” were assigned logMAR values of 2.7, 2.3 and 2.0, respectively.19
Study Outcomes
Postoperative data were recorded at 1, 3, 6, and 12 months following initial MPTSCPC treatment. The primary outcome measures were change in IOP from baseline and treatment success defined as IOP reduction ≥20% from baseline, achieved with or without topical or oral IOP lowering medications.
Secondary outcome measures included change in BCVA, number and drug classes of topical glaucoma medications, and ocular complications at 1, 3, 6, and 12 months following initial MPTSCPC treatment. Poor vision was defined as Snellen BCVA worse than 20/50. A clinically significant change in vision was defined as a change of ≥2 Snellen lines in BCVA from baseline. Recorded adverse effects included persistently elevated IOP defined as IOP ≥25% from baseline for ≥2 consecutive visits or 3 months; persistent hypotony defined as IOP of ≤5mmHg for ≥2 consecutive visits or 3 months; persistent inflammation defined as inflammation lasting for ≥3 months; vision loss defined as a decrease in ≥2 Snellen lines BCVA from baseline, not attributable to a shift in refractive error as determined by pinhole VA or subjective autorefraction; corneal edema; cystoid macular edema; serous choroidal detachment; transient mydriasis; cataract formation or progression; phthisis bulbi; sympathetic ophthalmia; vitreous hemorrhage; and hyphema.6,10
Medical therapy was reduced via a stepwise approach starting with oral glaucoma medication, at the surgeon’s discretion and with consideration of target IOP. Retreatment was considered if IOP reduction was over the target. Retreatment was not considered if a lack of effectiveness became apparent or if significant complications occurred. Retreatment with MPTSCPC took place at least 1 month following initial MPTSCPC treatment.
Micropulse Transscleral Cyclophotocoagulation Procedure
MPTSCPC laser treatments were performed by two surgeons (D.Y. or E.S.T.) using a fixed treatment protocol and standardized technique, as described extensively in our previous paper.20
All patients received 1g of acetaminophen, if no contraindications existed, before arrival at the surgical center. On arrival, 2% lidocaine gel, topical tetracaine, and topical brimonidine were instilled in the preoperative-holding area. At least 30 minutes before the laser procedure, a 0.5-mL subconjunctival injection of 2% lidocaine with epinephrine was administered in each hemisphere. The injection was aimed at being posterior from the limbus with an effort to avoid blood vessels to minimize the occurrence of subconjunctival hemorrhage. All patients received concurrent intravenous neurolept anesthesia using a combination of midazolam and fentanyl, with a dosage titrated to the patient’s need. The Cyclo G6 Laser System (Iridex, Mountain View, CA) in its MicroPulse treatment mode with the MicroPulse P3 handpiece was used for all treatments. Laser settings were maintained at 80 seconds per hemisphere for a total of 160s in each eye and a duty cycle of 31.3% (0.5-ms duration, 1.1-ms interval). The laser power ranged from 900 to 2500mW and was titrated at the discretion of the surgeon based on glaucoma severity, baseline VA, baseline IOP, target IOP, and previous response to MPTSCPC. In general, patients with higher baseline IOP were treated with higher laser power. Laser power was decreased if audible “pops” were heard or if the patient could not tolerate the current power. The laser fibre-optic probe was oriented with the curved side toward the limbus and the flat side toward the eyelid. The handpiece was positioned 1–2 mm posterior to the limbus and was held perpendicular to the globe. The mobilization of the probe was via a continuous sliding arc motion. Dwell time was 10 seconds per pass in each hemisphere, with a total of 8 passes per hemisphere (80 seconds total treatment time per hemisphere), resulting in a sweep velocity of 2.8 mm/seconds. The 3- and 9-o’clock positions were avoided to prevent damage to the ciliary nerves which increases the risk of mydriasis.6 Areas of scleral thinning were also avoided. Moderate to firm steady pressure was applied on the probe for well-controlled contact with the globe. A coupling liquid interface consisting of lidocaine 2% gel and viscous artificial tears was used. All patients were prescribed difluprednate 0.05% four times daily for one week after treatment.
Statistical Analysis
Data analyses were carried out using SPSS Statistics version 27 (IBM, Armonk, NY). Descriptive statistics were reported as mean ± standard deviations and 95% confidence intervals (CI) for continuous variables. The distribution of continuous variables was examined using histograms and Kolmogorov–Smirnov tests. Categorical variables were reported as proportions and percentages. Changes in primary and secondary outcomes were compared using paired t-tests or Wilcoxon signed-rank tests. Hierarchical random intercept multivariate regression models were used to investigate change in study outcomes with treatment. These models adjusted for the following variables: age, inter-eye variability, sex, ethnicity, surgeon, prior SLT procedures, prior cataract surgery, laser power, retreatment, baseline IOP, baseline BCVA, and baseline number of topical glaucoma medications. The analyses accounted for interrelationships between both eyes of the same patient. The one-way ANOVA, Kruskall Wallis or Chi-square (χ2) tests were used to determine differences between study cohorts. A p-value of <0.05 was used to confer statistical significance.
Results
Patient Demographics
One hundred and fifty-three eyes (n=153) from 93 patients (N) were included: 22 eyes (N=15) with OHT, 46 eyes (N=31) with early POAG, 35 eyes (N=28) with moderate POAG and 50 eyes (N=35) with severe POAG (Table 1). The majority of patients were Caucasian (55.6%), followed by Asian (30.7%), Hispanic (11.1%) and African (2.6%). The mean age was 67.73 ± 12.41 years [range 40–96] and 49.7% of patients were female. Nearly 90% of patients received an SLT procedure prior to the MPTSCPC treatment, with an average of 2.96 ± 1.85 SLT procedures [range 0–8]. All patients were followed for a minimum of 6 months after the initial MPTSCPC treatment. The mean follow-up time for all patients was 318 ± 96 days or 10 ± 3 months (Table 2). During the study follow-up, none of the eyes underwent any ocular lasers, procedures, or surgeries, with the exception of PRP (n=1) and anti-VEGF injections (n=6).
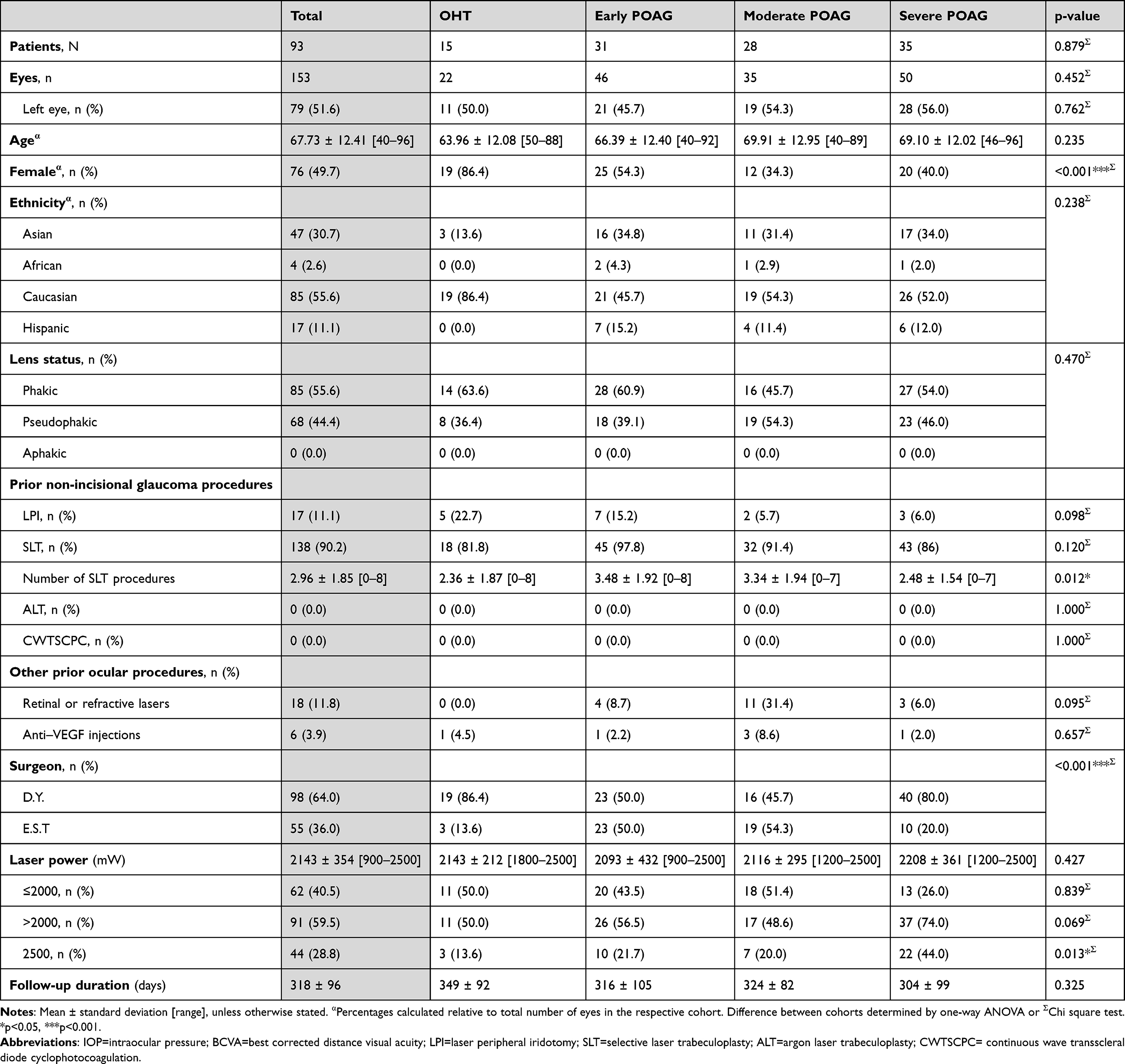 |
Table 1 Patient Demographics, Clinical Features and MPTSCPC Treatment Parameters |
 |
Table 2 Intraocular Pressure at Baseline and Final Follow-Up |
Intraocular Pressure
The baseline mean IOP was 18.37 ± 4.76mmHg in the total cohort (Table 2). There was a significant change in mean IOP from baseline to final follow-up in all cohorts (total cohort p<0.001; OHT p=0.003; early POAG p<0.001; moderate POAG p=0.022; severe POAG p=0.015; Table 3). Mean IOPs from baseline through follow-up months 1, 3, 6 and 12 for all study cohorts are displayed in Figure 1.
 |
Table 3 Visual Acuity at Baseline and Final Follow-Up |
 |
Figure 1 Mean intraocular pressure (IOP, mmHg) from baseline to 1, 3, 6 and 12-month follow-ups for all study cohorts. *Indicates a significant change in IOP from baseline (p<0.05) in univariate analysis. |
There was a greater proportion of eyes with a baseline IOP >21mmHg in the OHT and early POAG groups than in the moderate and severe PAOG cohorts (p=0.014). The proportion of eyes with IOP >21mmHg decreased from baseline to final follow-up in all cohorts, except for the severe POAG cohort, which remained unchanged (Table 2).
Overall, 52.9% (n=81) of eyes achieved IOP success by final follow-up (Table 2). This was similar across all cohorts (p=0.604; Table 2). Multivariate analysis revealed a significant change in mean IOP from baseline to final follow-up in the total, early and moderate cohorts (p<0.001, p<0.001 and p=0.009 respectively; Supplementary Table 1). Significant predictors in the multivariate analysis were Caucasian ethnicity (p=0.044) and baseline IOP (p<0.001). Between study cohorts, there were no significant differences between baseline IOP, final IOP and change in IOP (p>0.05; Table 2 and Supplementary Table 2).
There was a significant relationship between baseline IOP and IOP reduction with treatment (Pearson’s correlation coefficient r=−0.46, p<0.001). Eyes with baseline IOP >21mmHg (n=36) experienced significantly greater IOP reduction (mean reduction of 24.81%) as compared to eyes with IOP ≤21mmHg (n=117; mean reduction of 11.71%, MD=−3.94mmHg, 95% CI=[−2.48, −5.40], p<0.001).
Visual Acuity
The baseline logMAR BCVA was 0.33 ± 0.44 (Snellen 20/43 ± 20/55) in the total cohort. All cohorts, with the exception of the OHT cohort, experienced a significant worsening in BCVA by final follow-up (Table 3). Multivariate analysis revealed a statistically significant change in BCVA from baseline to final follow-up in the total cohort (p<0.001), but not moderate or severe cohorts (p=0.174 and p=0.314, respectively; Table 3). Significant predictors were baseline BCVA (p<0.001) and laser power (p=0.036).
There was a significant relationship between baseline BCVA and change in BCVA with treatment (r=0.193, p<0.001). Eyes with baseline BCVA worse than 20/50 experienced significantly greater worsening in vision after treatment than eyes with a BCVA better than 20/50 (MD=0.413, 95% CI=[0.30, 0.53], p<0.001).
Nearly 20% of eyes (n=30) had baseline poor vision, defined as BCVA less than 20/40, due to a visually significant cataract (n=6) or concurrent retinal (n=11) or corneal pathologies (n=3). The proportion of eyes with poor vision increased by final follow-up in all POAG cohorts and remained unchanged in the OHT cohort (Table 3). Eyes (n=13) that developed poor vision following treatment were secondary to cataract progression (n=6), ocular surface disease (n=4), and persisting iritis (n=3).
LogMAR BCVA from baseline through follow-up months 1, 3, 6 and 12 for all study cohorts are displayed in Figure 2. Supplementary Table 2 highlights differences in baseline BCVA, final BCVA and change in BCVA from baseline to final follow-up between cohorts.
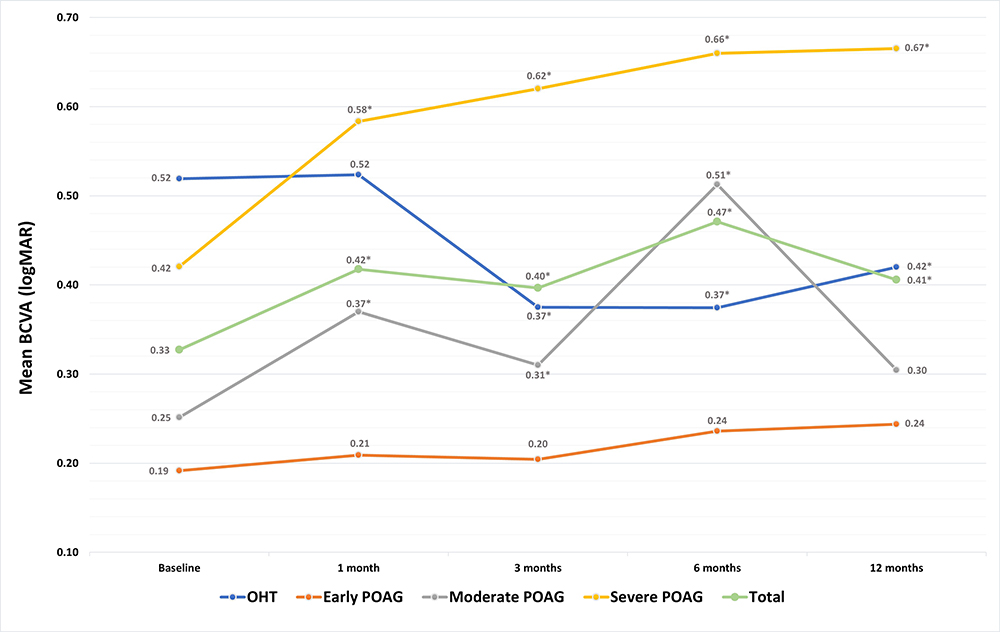 |
Figure 2 Mean best corrected distance visual acuity (BCVA, logMAR) from baseline to 1, 3, 6 and 12-month follow-ups for all study cohorts. *Indicates a significant change in logMAR BCVA from baseline (p<0.05) in univariate analysis. |
Topical Medications
At baseline, eyes in the total cohort used an average of 1.45 ± 1.01 topical glaucoma medications (Table 4). Commonly used medications were prostaglandin analogs (61.4%), fixed combination brimonidine and timolol (22.9%) and carbonic anhydrase inhibitors (14.4%).
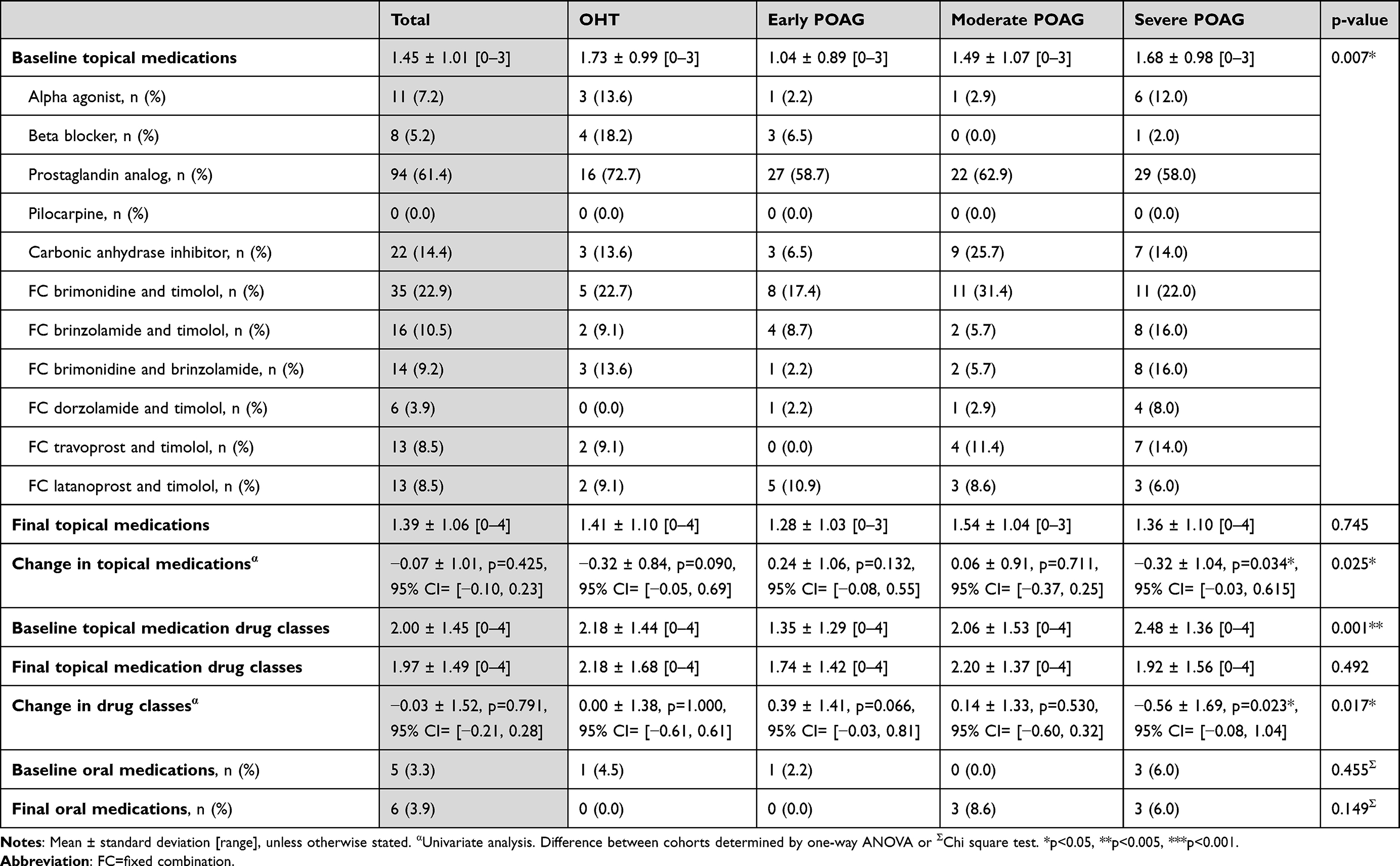 |
Table 4 Medications at Baseline and Final Follow-Up |
There was a reduction in the number of topical medications and topical drug classes in the total cohort from baseline to final follow-up (p=0.425 and p=0.791, respectively; Table 4). The severe POAG cohort experienced a significant reduction in both the number of topical medications and topical drug classes (p=0.034 and p=0.023, respectively), but lost this significance in multivariate analysis (p=0.316 and p=0.227, respectively; Supplementary Table 1). Significant predictors in the multivariate analysis were surgeon (p=0.004), baseline number of topical medications (p<0.001) and baseline number of topical drug classes (p<0.001). Eyes treated by D.Y. experienced a significantly greater reduction in the number and classes of topical glaucoma medications by final follow-up as compared to eyes treated by E.S.T.
Eyes that were administered a laser power >2000mW (n=91) experienced a greater reduction in number of topical medications and drug classes than eyes administered a laser power of ≤2000mW (n=62; MD=−0.229, 95% CI=[−0.46, 0.007], p=0.057 and MD=−0.352, 95% CI=[−0.69, 0.02], p=0.039, respectively). Supplementary Table 2 highlights differences in the number of topical medications and topical drug classes between cohorts at baseline, final follow-up and change from baseline to final follow-up.
Prior Cataract Surgery
Our study does not include eyes with prior incisional glaucoma procedures, with the exception of cataract surgery. Changes in IOP and BCVA from baseline to final follow-up were not significantly different between pseudophakic (n=68) and phakic (n=85) eyes (pseudophakic=−2.71 ± 5.75mmHg; phakic=−3.01 ± 5.75mmHg; MD=−0.306mmHg, 95% CI=[−1.61, 1.00], p=0.644 and p=0.114, respectively). However, pseudophakic eyes experienced a reduction in the number of topical medications from baseline to final follow-up, whereas phakic eyes experienced an increase (pseudophakic=−0.37 ± 1.03, phakic=0.18 ± 0.93, MD=0.544, 95% CI=[0.32, 0.77], p<0.001). This was similar for the change in topical drug classes from baseline to final follow-up (pseudophakic=−0.49 ± 1.62; phakic=0.33 ± 1.34; MD=0.815, 95% CI=[0.48, 1.15], p<0.001). Changes in medications were not related to baseline IOP differences between the two groups (p>0.05).
Laser Power
The average MPTSCPC laser power was 2143 ± 354mW [range 900–2500] in the total cohort (Table 1). Nearly 60% of eyes (n=91) were treated with a laser power >2000mW, with 29% of eyes (n=44) treated with a laser power of 2500mW. No significant associations were found between laser power and change in BCVA with treatment (r=0.036, p=0.528) or IOP reduction with treatment (r=−0.008, p=0.885).
Complications
By final follow-up, the most common complication was cataract progression, observed in 34.1% of phakic eyes (Table 5). Other complications included persistently elevated IOP (7.8%), symptomatic mydriasis (5.9%), hyphema (3.9%), and persistent iritis (2.0%). None of the eyes in the total cohort experienced any serious complications including corneal edema, cystoid macular edema, serous choroidal detachment, phthisis bulbi, sympathetic ophthalmia, vitreous hemorrhage, or persistent hypotony.
 |
Table 5 Complications, Repeat MPTSCPC Treatments and Further Glaucoma Procedures During Study Follow-Up |
Retreatment and Surgical Escalation
Twenty-two (14.4%) eyes received an additional MPTSCPC treatment during the follow-up period, with one eye receiving two additional treatments (Table 5). The average time to retreatment was 125 ± 116 days. Retreatment offered an additional IOP reduction of 1.260 mmHg (p=0.344). Ten eyes (6.5%) required escalation to SLT. Eight eyes (5.2%) required escalation to an incisional glaucoma procedure which included Xen gel microstent (Allergan, Dublin, Ireland; n=6), iStent trabecular micro-bypass stent (Glaukos, San Clemente, CA; n=1), and CyPass supraciliary microstent (Novartis, Basel, Switzerland; n=1).
Discussion
Treatment Success and IOP Reduction
Our study investigated the safety and effectiveness of MPTSCPC treatment in non-incisional eyes with OHT and early, moderate, and severe POAG. Nearly 53% of the 153 eyes in our total cohort achieved an IOP reduction of 20% or more by final follow-up. The success rates were not significantly different across cohorts and are in keeping with the literature. The average success rate of MPTSCPC treatment in the literature, typically defined as a final IOP between 6 and 21 mmHg or 20–30% reduction from baseline, ranges between 26% and 96%, with a mean IOP percent reduction from baseline ranging between 27% and 51%.12–18,21,22 However, the literature is heterogeneous with respect to treatment parameters, patient demographics, follow-up durations and glaucoma types and severities, making it difficult to compare these endpoints between studies. Our rates of success and IOP reduction are most in keeping with Tong et al who achieved a mean IOP reduction of 21.1% from a baseline IOP of 24.8 mmHg, and 45.5% treatment success in 55 eyes with POAG at 12 months.23
Our IOP reduction was modest, and likely due to a lower baseline IOP of 18.37 ± 4.76 mmHg. Only 23.5% of eyes in our total cohort had a baseline IOP >21 mmHg, which decreased to 11.8% at final follow-up. Eyes with a baseline IOP >21 mmHg experienced a greater IOP reduction than eyes with an IOP ≤21 mmHg (p<0.001). Our multivariate model further found that baseline IOP was a significant predictor in IOP reduction with treatment (p<0.001).
The majority of the studies on MPTSCPC have reported baseline mean IOPs above 21 mmHg, typically ranging from 21.9 to 40.1 mmHg, with the exception of a few.12,20,24–27 Some studies have found that a greater baseline IOP was associated with a greater reduction in IOP.21,28 In our previous report, IOP stratification demonstrated a significantly greater mean IOP reduction at 12 months when baseline IOP was >21 mmHg as compared to ≤21 mmHg (30.5% vs 20.1%).20 On the other hand, Preda et al found that eyes with a baseline IOP <26 mmHg achieved the highest treatment success rate as compared to eyes with baseline IOP ≥26–30 mmHg, 31–49 mmHg and ≥50 mmHg.29 As in MPTSCPC, a greater IOP-lowering effect is seen in eyes with a higher baseline IOP treated with selective laser trabeculoplasty (SLT).30 Future studies on MPTSCPC treatment in normal tension glaucomatous eyes would be useful in confirming this assumption.
We did not find a dose–response relationship between MPTSCPC laser power and reduction in IOP in our total cohort (p=0.885). This may be a result of the small range of laser powers used and low baseline IOPs of included eyes. In our study, laser power ranged from 900 to 2500mW. The total energy (TE = duty cycle x dwell time x laser power) delivered was between 45.1J and 125.2J (mean 107.3J). Our findings contradict some of the literature, which suggests that higher laser power is associated with greater IOP reduction.10,23,25,31 In their 18-month prospective study, Marchand et al reported mean IOP reduction of 40.1% in eyes treated at 200.4J and 30.8% in eyes treated at 150.2J.31 Sarrafpour et al found mean IOP reduction of 57% at 2500mW and 30% at 2000mW.28 Tong et al also found greater IOP reduction with higher laser power in eyes with POAG.23 Balendiran et al observed a significantly greater IOP reduction at 3 and 6-months follow-up in non-incisional eyes with POAG treated with a TE of 93.9J as compared to 78.25J.25
The effectiveness of MPTSCPC treatment is a function of three major treatment parameters including laser power, duration, and dwell time.10,32 Again, the literature is largely heterogeneous with regard to these treatment parameters. In our study, the dwell time and duration were the same for all eyes between both surgeons, but the laser power varied based on iris pigmentation, severity of glaucoma, baseline IOP, target IOP, and patient’s pain tolerance. A few studies extended the treatment duration for eyes with higher baseline IOPs.15,29,33,34 Williams et al used a “stop-and-go” application technique which is purported to have a lower thermal effect than the traditional back-and-forth sweeping technique.14,22 To date, there has been no standardization of MPTSCPC treatment parameters. Sanchez et al suggest that a balance of efficacy and safety is best achieved between 112 and 150J.10 We recommend that future studies investigate the ideal parameters that balance effectiveness and safety.
Our multivariate regression model found that patient ethnicity, specifically Caucasian ethnicity, was a significant predictor of IOP reduction. We believe this association is a result of a higher laser power used in lightly pigmented eyes. Although we did not formally document iris colour or pigmentation levels in our patients, there was a tendency to select higher laser settings in less pigmented eyes as there is typically less uptake.
In our study, 14.4% of eyes were retreated (laser power 1800–2700mW, TE 45.1J–125.2J), which provided an additional 1.260mmHg of IOP reduction (p=0.344). Due to the variety of different glaucoma types, severities, and TE administered, the retreatment rates reported in the literature are highly variable, ranging between 0% and 46%.11,14,35 The literature suggests that a lower TE is associated with higher rates of retreatment. Aquino et al and Tan et al used the same amount of TE (62.6J) and reported retreatment rates of 48% and 35%, respectively.11,36 Tong et al also used a similar TE but reported a much lower retreatment rate of 13% in their study of POAG eyes.23 The rates of retreatment were significantly lower in studies by Al Habash et al (5.6%, TE 165.2J) and Yelenskiy et al (8.6%, TE 111.6–148.8J), both of which used some of the highest energy settings reported in the literature.21,22 Our retreatment rate was most similar to Tong et al, although they used a higher TE on average.23 Notably, only one eye with OHT required retreatment, suggesting that a single MPTSCPC treatment may be sufficient to achieve IOP reduction in eyes with OHT.
Our study includes only eyes with OHT and POAG. Yelenskiy et al observed greater IOP reduction in eyes with POAG, while Souissi et al did not observe a significant difference between eyes with POAG and secondary glaucoma.22,34,37 Tekeli and Köse found no difference in treatment success and medications between POAG and pseudoexfoliation glaucoma, both of which, however, required fewer retreatments than other secondary glaucoma.16 Wong et al found that eyes with POAG had a higher likelihood of success than neovascular glaucoma and other diagnoses.13 They hypothesized that in eyes with refractory, advanced glaucoma, prolonged inflammation or chronic fibrovascular changes might lead to the formation of a hydrophobic layer on the pars plana that may inhibit the effects of MPTSCPC.
To the best of our knowledge, our current and prior studies are the only ones in the literature to investigate the use of MPTSCPC in OHT.20 Overall, eyes with OHT achieved the highest mean IOP reduction as compared to the POAG cohorts (p=0.426). The retreatment rate was also lower in the OHT cohort as compared to the POAG cohorts (p=0.447). The rates of adverse events in the OHT cohort were similar or lower to the POAG cohorts. There was a near-significant reduction in the number of topical glaucoma medications in the OHT cohort (p=0.090); however, the number of drug classes remained unchanged (p=1.000). The OHT cohort did not experience any changes in BCVA (p=0.277), while all POAG cohorts experienced worsening in vision mostly due to cataract progression or ocular surface disease. Our findings suggest that MPTSCPC is safe and effective in treating OHT. Future studies with a larger sample of eyes with OHT could further investigate this assumption.
Our study is also the first in the literature to focus primarily on eyes without prior incisional glaucoma procedures. There is limited literature comparing the effectiveness of MPTSCPC treatment in eyes with and without prior incisional procedures. Garcia et al and Yelenskiy et al found that eyes with prior incisional procedures experienced a greater IOP reduction success, while de Crom et al found that although preoperative and postoperative IOPs were significantly lower in eyes with prior incisional procedures, there were no significant differences in the change in IOP with treatment between eyes with and without prior incisional procedures.22,33,34 Eyes with prior incisional procedures may respond more favourably to MPTSCPC treatment due to a pre-existing external aqueous outflow pathway.33 Regardless, our study findings suggest that MPTSCPC treatment is effective and safe in eyes without prior incisional procedures. MPTSCPC may play an important role in the management of IOP in patients for whom incisional procedures are contraindicated due to ocular or medical co-morbidities, in patients who refuse incisional procedures, and as a temporizing measure before definitive surgery.15
Medications
There was a significant reduction in the number of topical medications (p=0.034), and drug classes (p=0.023) in the severe POAG cohort; however, both these associations lost their significance in multivariate analysis adjusting for the baseline number of topical medications and drug classes (p=0.316 and p=0.227, respectively). The surgeon was found to be a significant predictor in the multivariate analysis, where eyes treated by D.Y. experienced a greater reduction in topical medications than eyes treated by E.S.T. This change was not associated with glaucoma severity or treatment response, rather surgeon practice preference. The other study cohorts did not experience a change in the number of topical medications and drug classes in both univariate and multivariate analyses. Only one person was started on oral acetazolamide during our study follow-up. Tong et al also did not experience a reduction in the number of topical medications and classes in eyes with POAG.23 The combined findings of our group and that of Tong et al suggest that MPTSCPC may be more effective as an adjunct to medication than a replacement.
Vision Loss
Vision loss (worsening in vision by ≥2 Snellen lines) in the OHT group was attributable to persistent iritis in a patient with a history of iritis. In the mild and moderate POAG group, the most common cause of vision loss was ocular surface disease (OSD), followed by cataract progression. In the severe cohort, the most common cause of vision loss was cataract progression, followed by persistent iritis and OSD. Our rate of cataract progression was 34% in phakic eyes in the total cohort (or 19% of total eyes); however, only 4.6% of total eyes experienced vision loss secondary to cataract progression. Further, we did not find a significant difference in change in BCVA by final follow-up between pseudophakic and phakic eyes (p=0.114).
Our rate of vision loss (8.5%) is within the range reported in the literature (0–26.2%).12,17,35 In their study of eyes with good central vision (BCVA ≥20/60), Varikuti et al observed cataract progression in 40%, while 21% experienced vision loss of ≥2 Snellen lines.38 Similarly, in our total cohort, cataract progression developed in 40% of eyes and was the most common cause of vision loss. Varikuti et al identified prior glaucoma surgery as a significant factor for vision loss.38 The rate of vision loss in CWTSCPC-treated eyes is reported to be up to 30.6% in eyes with good central vision (BCVA ≥20/60).39 The rate of vision loss for tube shunts and trabeculectomy is reported to be up to 42% and 46%, respectively.40 To date, an acceptable rate of vision loss for MPTSCPC or other glaucoma procedures has not been established. It is unclear whether cataract progression resulted from inflammation following treatment or whether these cataracts would have progressed irrespective of treatment. Although cataract progression is common after incisional glaucoma procedures, there appears to be a considerable rate of cataract progression after MPTSCPC.40–42 We recommend counselling phakic patients with good visual potential of the increased risk for cataract progression.
Safety and Adverse Events
Only a few eyes (n=12, 7.8%) experienced persistently elevated IOP (≥25% from baseline) following treatment. This may be in part from a steroid response to the topical steroids administered after treatment.42 Of these, ten received an SLT, and eight (IOPs >28mmHg) were ultimately escalated to incisional procedures. Retreatment with MPTSCPC was only done if there was a response to the initial MPTSCPC treatment.
Importantly, we did not observe any serious adverse events typically associated with CWTSCPC, such as phthisis bulbi, sympathetic ophthalmia, serous choroidal detachments, persistent hypotony, vitreous hemorrhage, and corneal or macular edema. The literature suggests that serious complications may develop with higher MPTSCPC laser energy settings. In eyes with refractory glaucoma treated at a laser energy of 200J, Williams et al reported several complications including hypotony (8.8%), corneal edema (2%), prolonged anterior chamber reaction (26%), and phthisis bulbi (2%).14 Emmanuel et al, using similarly high energy settings, reported postoperative inflammation at 3-month follow-up in 46% of eyes and vision loss in 26.2%. Our study used nearly half the energy on average (107J) and did not observe any serious complications. Sanchez et al have proposed that laser settings delivering a total energy between 112 and 150J are safe.10 Energy levels exceeding 200J cause greater IOP reduction, but also more severe complications, while energy levels less than 100J are safe, but only cause mild, transient IOP reduction.10 Although standardization of key steps in MPTSCPC treatment should be established, titration of laser energy should be customized to each patient.
Although some studies in the literature have reported corneal complications following MPTSCPC including neurotrophic keratitis in patients with predisposing factors, we are the only group to highlight OSD as a potential complication.43 One of the most common causes of vision loss in our previous report was OSD.20 In our present study, OSD was responsible for vision loss in the POAG cohorts. Radhakrishnan et al reported persistent superficial punctate keratitis (SPK) following MPTSCPC.44 They hypothesized that MPTSCPC may cause mechanical damage to the perilimbal corneal plexus and that persistent SPK observed were the earliest stage of neurotrophic keratitis characterized by punctate keratopathy without an epithelial defect.44 In our study, none of the eyes developed neurotrophic keratitis. Unfortunately, the presence and extent of OSD were not reported at baseline in our study, making it difficult to ascertain a causal relationship between MPTSCPC treatment and OSD. In an international review, the prevalence of OSD in glaucoma patients was found to range between 40% and 59%.45 The cumulative effect of preservatives and excipients in topical glaucoma medications can alter underlying cellular structures causing tear film abnormalities and loss in homeostasis of the ocular surface.45 We recommend counselling patients about the possibility of developing OSD or experiencing worsening symptoms following MPTSCPC treatment.
Symptomatic mydriasis, observed in 5.9% of eyes, was bothersome to some patients, but not contributory to vision loss. Studies on both CWTSCPC and MPTSCPC have reported symptomatic mydriasis, often persisting indefinitely.46–48 Radhakrishnan et al reported mydriasis in nearly two-thirds of eyes following MPTSCPC treatment by final follow-up, which was associated with a decrease in VA in nearly half.44 They found Asian race, primary open-angle glaucoma, and phakic status to be associated with mydriasis.44 Although the 3 and 6 o’clock positions at the limbus were to be avoided during MPTSCPC treatment, we speculate that mydriasis resulted from damage to the terminal branches of the short posterior ciliary nerves from the continuous sweeping motion of the laser probe during treatment.6 We believe it is prudent to counsel patients about this potential complication.
Limitations
The retrospective nature, small cohort sizes and relatively short follow-up period of our study limit the generalizability of our findings. Most of our patients were Caucasian, with possibly less pigmented eyes, which may limit the applicability of our findings to more pigmented eyes.
Conclusion
MPTSCPC appears to be a safe and effective treatment for non-incisional eyes with OHT and all severities of POAG. We found a modest, yet stable IOP lowering effect, and a similar medication burden by final follow-up. This supports the role of MPTSCPC as a potential adjunct to medical therapy in non-incisional eyes. There was some worsening in BCVA, which was mostly attributable to cataract progression and ocular surface disease.
Acknowledgments
The authors would like to thank Nadia Muhe, statistical support specialist at the University of Toronto, for her guidance on the statistical analyses. This study was presented at the American Society for Cataract and Refractive Surgery (ASCRS) Annual Meeting (Virtual) on April 22–26, 2022; the Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting (Virtual) on May 1–4, 2022; and the Canadian Ophthalmological Society (COS) Annual Research Meeting on June 9–12, 2022.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jonas JB, Aung T, Bourne RR, Bron AM, Ritch R, Panda-Jonas S. Glaucoma. Lancet. 2017;390(10108):2183–2193. doi:10.1016/S0140-6736(17)31469-1
2. Miglior S, Zeyen T, Pfeiffer N, et al. Results of the European glaucoma prevention study. Ophthalmology. 2005;112(3):366–375. doi:10.1016/j.ophtha.2004.11.030
3. Kass MA, Heuer DK, Higginbotham EJ, et al. The ocular hypertension treatment study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):701–830. doi:10.1001/archopht.120.6.701
4. Leske MC, Heijl A, Hyman L, Bengtsson B. Early manifest glaucoma trial: design and baseline data. Ophthalmology. 1999;106(11):2144–2153. doi:10.1016/s0161-6420(99)90497-9
5. The AGIS Investigators. The advanced glaucoma intervention study (AGIS): 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators Am J Ophthalmol. 2000;130(4):429–440. doi:10.1016/S0002-9394(00)00538-9
6. Sanchez FG, Peirano-Bonomi JC, Brossard Barbosa N, Khoueir Z, Grippo TM. Update on micropulse transscleral cyclophotocoagulation. J Glaucoma. 2020;29(7):598–603. doi:10.1097/IJG.0000000000001539
7. Pastor SA, Singh K, Lee DA, et al. Cyclophotocoagulation: a report by the American Academy of ophthalmology. Ophthalmology. 2001;108(11):2130–2138. doi:10.1016/s0161-6420(01)00889-2
8. Moussa K, Feinstein M, Pekmezci M, et al. Histologic changes following continuous wave and micropulse transscleral cyclophotocoagulation: a randomized comparative study. Transl Vis Sci Technol. 2020;9(5):22. doi:10.1167/tvst.9.5.22
9. Maslin JS, Chen PP, Sinard J, Nguyen AT, Noecker R. Histopathologic changes in cadaver eyes after MicroPulse and continuous wave transscleral cyclophotocoagulation. Can J Ophthalmol. 2020;55(4):330–335. doi:10.1016/j.jcjo.2020.03.010
10. Sanchez FG, Peirano-Bonomi JC, Grippo TM. Micropulse Transscleral Cyclophotocoagulation: a Hypothesis for the Ideal Parameters. Med Hypothesis Discov Innov Ophthalmol. 2018;7(3):94–100.
11. Aquino MC, Barton K, Tan AM, et al. Micropulse versus continuous wave transscleral diode cyclophotocoagulation in refractory glaucoma: a randomized exploratory study. Clin Exp Ophthalmol. 2015;43(1):40–46. doi:10.1111/ceo.12360
12. Souissi S, Le Mer Y, Metge F, et al. An update on continuous-wave cyclophotocoagulation (CW-CPC) and micropulse transscleral laser treatment (MP-TLT) for adult and paediatric refractory glaucoma. Acta Ophthalmol. 2021;99(5):e621–e653. doi:10.1111/aos.14661
13. Wong KYT, Aquino CM, Macasaet AM, Suwandono ME, Chew PTK, Koh VTC. MP3 Plus: a modified micropulse transscleral cyclophototherapy technique for the treatment of refractory glaucoma. J Glaucoma. 2020;29(4):264–270. doi:10.1097/IJG.0000000000001443
14. Williams AL, Moster MR, Rahmatnejad K, et al. Clinical efficacy and safety profile of micropulse transscleral cyclophotocoagulation in refractory glaucoma. J Glaucoma. 2018;27(5):445–449. doi:10.1097/IJG.0000000000000934
15. Vig N, Ameen S, Bloom P, et al. Micropulse transscleral cyclophotocoagulation: initial results using a reduced energy protocol in refractory glaucoma. Graefes Arch Clin Exp Ophthalmol. 2020;258(5):1073–1079. doi:10.1007/s00417-020-04611-0
16. Tekeli O, Köse HC. Outcomes of micropulse transscleral cyclophotocoagulation in primary open-angle glaucoma, pseudoexfoliation glaucoma, and secondary glaucoma. Eur J Ophthalmol. 2021;31(3):1113–1121. doi:10.1177/1120672120914231
17. Emanuel ME, Grover DS, Fellman RL, et al. Micropulse cyclophotocoagulation: initial results in refractory glaucoma. J Glaucoma. 2017;26(8):726–729. doi:10.1097/IJG.0000000000000715
18. Canadian Ophthalmological Society Glaucoma Clinical Practice Guideline Expert Committee; Canadian Ophthalmological Society. Canadian Ophthalmological Society evidence-based clinical practice guidelines for the management of glaucoma in the adult eye. Can J Ophthalmol. 2009;44:S7–S93. doi:10.3129/cjo44s1
19. Lange C, Feltgen N, Junker B, Schulze-Bonsel K, Bach M. Resolving the clinical acuity categories ”hand motion” and ”counting fingers” using the Freiburg Visual Acuity Test (FrACT). Graefes Arch Clin Exp Ophthalmol. 2009;247(1):137–142. doi:10.1007/s00417-008-0926-0
20. Kaba Q, Somani S, Tam E, Yuen D. The effectiveness and safety of micropulse cyclophotocoagulation in the treatment of ocular hypertension and glaucoma. Ophthalmol Glaucoma. 2020;3(3):181–189. doi:10.1016/j.ogla.2020.02.005
21. Al Habash A, AlAhmadi AS. Outcome of microPulse® transscleral photocoagulation in different types of glaucoma. Clin Ophthalmol. 2019;13:2353–2360. doi:10.2147/OPTH.S226554
22. Yelenskiy A, Gillette TB, Arosemena A, et al. Patient outcomes following micropulse transscleral cyclophotocoagulation: intermediate-term results. J Glaucoma. 2018;27(10):920–925. doi:10.1097/IJG.0000000000001023
23. Tong W, Shen TYT, Wong HC, Aquino MC, Chew P, Lim D. One-year outcomes of micropulse cyclophototherapy for primary open-angle glaucoma. J Glaucoma. 2021;30(10):911–920. doi:10.1097/IJG.0000000000001925
24. Waibel S, Herber R, Pillunat LE, Pillunat KR. One-year follow-up of pars plicata versus pars plana application of transscleral micropulse cyclophotocoagulation. J Glaucoma. 2021;30(4):340–346. doi:10.1097/IJG.0000000000001775
25. Balendiran V, Landreneau J, An J. MicroPulse transscleral laser therapy dosimetry utilizing the revised P3 delivery device: a randomized controlled trial. Ophthalmol Glaucoma. 2022;S2589–4196(22):189. doi:10.1016/j.ogla.2022.09.004
26. Daas A, Sherman T, Danieliute L, et al. Phacoemulsification combined with micropulse cyclodiode laser in glaucoma patients: efficacy and safety. Eye. 2022;36(11):2188–2191. doi:10.1038/s41433-021-01826-1
27. Fili S, Vastardis I, Perdikakis G, Kohlhaas M. Transscleral cyclophotocoagulation with MicroPulse® laser versus cyclophotocoagulation with continuous diode laser in patients with open-angle glaucoma. Int Ophthalmol. 2022;42(2):525–539. doi:10.1007/s10792-021-02023-5
28. Sarrafpour S, Saleh D, Ayoub S, Radcliffe NM. Micropulse transscleral cyclophotocoagulation: a look at long-term effectiveness and outcomes. Ophthalmol Glaucoma. 2019;2(3):167–171. doi:10.1016/j.ogla.2019.02.002
29. Preda MA, Karancsi OL, Munteanu M, Stanca HT. Clinical outcomes of micropulse transscleral cyclophotocoagulation in refractory glaucoma-18 months follow-up. Lasers Med Sci. 2020;35(7):1487–1491. doi:10.1007/s10103-019-02934-x
30. De Keyser M, De Belder M, De Belder S, De Groot V. Where does selective laser trabeculoplasty stand now? A review. Eye Vis (Lond). 2016;3:10. doi:10.1186/s40662-016-0041-y
31. Marchand M, Singh H, Agoumi Y. Micropulse trans-scleral laser therapy outcomes for uncontrolled glaucoma: a prospective 18-month study. Can J Ophthalmol. 2021;56(6):371–378. doi:10.1016/j.jcjo.2021.01.015
32. Grippo TM, Sanchez FG, Stauffer J, Marcellino G. MicroPulse® transscleral laser therapy - fluence may explain variability in clinical outcomes: a literature review and analysis. Clin Ophthalmol. 2021;15:2411–2419. doi:10.2147/OPTH.S313875
33. de Crom RMPC, Slangen CGMM, Kujovic-Aleksov S, Webers CAB, Berendschot TTJM, Beckers HJM. Micropulse transscleral cyclophotocoagulation in patients with glaucoma: 1- and 2-year treatment outcomes. J Glaucoma. 2020;29(9):794–798. doi:10.1097/IJG.0000000000001552
34. Garcia GA, Nguyen CV, Yelenskiy A, et al. Micropulse transscleral diode laser cyclophotocoagulation in refractory glaucoma: short-term efficacy, safety, and impact of surgical history on outcomes. Ophthalmol Glaucoma. 2019;2(6):402–412. doi:10.1016/j.ogla.2019.08.009
35. Tan AM, Chockalingam M, Aquino MC, Lim ZI, See JL, Chew PT. Micropulse transscleral diode laser cyclophotocoagulation in the treatment of refractory glaucoma. Clin Exp Ophthalmol. 2010;38(3):266–272. doi:10.1111/j.1442-9071.2010.02238.x
36. Xu H, Lee D, Cho J, Voss J, McDaniel L, An JA. Netarsudil as a predictor of response for micropulse transscleral laser therapy: a pilot study. Ophthalmol Glaucoma. 2022;5(6):658–662. doi:10.1016/j.ogla.2022.06.005
37. Souissi S, Baudouin C, Labbé A, Hamard P. Micropulse transscleral cyclophotocoagulation using a standard protocol in patients with refractory glaucoma naive of cyclodestruction. Eur J Ophthalmol. 2021;31(1):112–119. doi:10.1177/1120672119877586
38. Varikuti VNV, Shah P, Rai O, et al. Outcomes of micropulse transscleral cyclophotocoagulation in eyes with good central vision. J Glaucoma. 2019;28(10):901–905. doi:10.1097/IJG.0000000000001339
39. Rotchford AP, Jayasawal R, Madhusudhan S, Ho S, King AJ, Vernon SA. Transscleral diode laser cycloablation in patients with good vision. Br J Ophthalmol. 2010;94(9):1180–1183. doi:10.1136/bjo.2008.145565
40. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. Treatment outcomes in the tube versus trabeculectomy study after one year of follow-up. Am J Ophthalmol. 2007;143(1):9–22. doi:10.1016/j.ajo.2006.07.020
41. Patel HY, Danesh-Meyer HV. Incidence and management of cataract after glaucoma surgery. Curr Opin Ophthalmol. 2013;24(1):15–20. doi:10.1097/ICU.0b013e32835ab55f
42. Phulke S, Kaushik S, Kaur S, Pandav SS. Steroid-induced glaucoma: an avoidable irreversible blindness. J Curr Glaucoma Pract. 2017;11(2):67–72. doi:10.5005/jp-journals-l0028-1226
43. Perez CI, Han Y, Rose-Nussbaumer J, Ou Y, Hsia YC. Neurotrophic keratitis after micropulse transscleral diode laser cyclophotocoagulation. Am J Ophthalmol Case Rep. 2019;15:100469. doi:10.1016/j.ajoc.2019.100469
44. Radhakrishnan S, Wan J, Tran B, et al. Micropulse cyclophotocoagulation: a multicenter study of efficacy, safety, and factors associated with increased risk of complications. J Glaucoma. 2020;29(12):1126–1131. doi:10.1097/IJG.0000000000001644
45. Nijm LM, De Benito-Llopis L, Rossi GC, Vajaranant TS, Coroneo MT. Understanding the dual dilemma of dry eye and glaucoma: an international review. Asia Pac J Ophthalmol. 2020;9(6):481–490. doi:10.1097/APO.0000000000000327
46. Vieira GM, Vieira FJ, Ritch R. Urrets-zavalia syndrome after diode laser transscleral cyclophotocoagulation. J Glaucoma. 2017;26(7):678–682. doi:10.1097/IJG.0000000000000666
47. Egbert PR, Fiadoyor S, Budenz DL, Dadzie P, Byrd S. Diode laser transscleral cyclophotocoagulation as a primary surgical treatment for primary open-angle glaucoma. Arch Ophthalmol. 2001;119(3):345–350. doi:10.1001/archopht.119.3.345
48. Nguyen AT, Maslin J, Noecker RJ. Early results of micropulse transscleral cyclophotocoagulation for the treatment of glaucoma. Eur J Ophthalmol. 2020;30(4):700–705. doi:10.1177/1120672119839303
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment of Open-Angle Glaucoma and Ocular Hypertension with the Fixed-Dose Combination of Preservative-Free Tafluprost/Timolol: Clinical Outcomes from Ophthalmology Clinics in Italy
Oddone F, Scorcia V, Iester M, Sisto D, De Cilla S, Bettin P, Cagini C, Figus M, Marchini G, Rossetti L, Rossi G, Salgarello T, Scuderi GL, Staurenghi G
Clinical Ophthalmology 2022, 16:1707-1719
Published Date: 1 June 2022
A Comprehensive Review of the Clinical Evidence Comparing Benzalkonium Chloride–Preserved and Benzalkonium Chloride–Free Latanoprost in the Treatment of Primary Open-Angle Glaucoma and Ocular Hypertension
Kumar H, Parikh R, Chagani A, Bhojani KG, Jain P, Dharmadhikari S, Bhargave C, Mane A, Mehta S
Clinical Ophthalmology 2026, 20:595069
Published Date: 28 May 2026