Back to Journals » Infection and Drug Resistance » Volume 17
Microbiota-Based Live Biotherapeutic Products for Clostridioides Difficile Infection- The Devil is in the Details
Authors Monday L ![]() , Tillotson G
, Tillotson G ![]() , Chopra T
, Chopra T
Received 4 November 2023
Accepted for publication 12 February 2024
Published 15 February 2024 Volume 2024:17 Pages 623—639
DOI https://doi.org/10.2147/IDR.S419243
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Lea Monday,1 Glenn Tillotson,2 Teena Chopra1
1Division of Infectious Diseases, Wayne State University School of Medicine, Detroit, MI, USA; 2GlennTillotson PhD, FIDSA, GSTMicro, Henrico, VA, USA
Correspondence: Lea Monday, Harper University Hospital, Division of Infectious Diseases, 3990 John R Street, 5 Hudson, Suite 5911, Detroit, MI, 48201, USA, Tel +1 734-344-8392, Fax +1 313-9930302, Email [email protected]
Abstract: Clostridioides difficile infection (CDI) remains a significant contributor to healthcare costs and morbidity due to high rates of recurrence. Currently, available antibiotic treatment strategies further disrupt the fecal microbiome and do not address the alterations in commensal flora (dysbiosis) that set the stage for CDI. Advances in microbiome-based research have resulted in the development of new agents, classified as live biotherapeutic products (LBPs), for preventing recurrent CDI (rCDI) by restoring eubiosis. Prior to the LBPs, fecal microbiota transplantation (FMT) was available for this purpose; however, lack of large-scale availability and safety concerns have remained barriers to its widespread use. The LBPs are an exciting development, but questions remain. Some are derived directly from human stool while other developmental products contain a defined microbial consortium manufactured ex vivo, and they may be composed of either living bacteria or their spores, making it difficult to compare members of this heterogenous drug class to one another. None have been studied head-to head or against FMT in preventing rCDI. As a class, they have considerable variability in their biologic composition, biopharmaceutic science, route of administration, stages of development, and clinical trial data. This review will start by explaining the role of dysbiosis in CDI, then give the details of the biopharmaceutical components for the LBPs which are approved or in development including how they differ from FMT and from one another. We then discuss the clinical trials of the LBPs currently approved for rCDI and end with the future clinical directions of LBPs beyond C. difficile.
Keywords: Clostridioides difficile infection, microbiome, microbiome therapeutic, indirect treatment comparison
Introduction
The study of bacteria and their role in disease has been queried by humans for centuries. In the last two decades, advances in genomic sequencing technology have accelerated understanding of the gut microecosystem and led to a surge in microbiome-based research.1–3 The quest to harness the power of the human microbiome into a commercially available product has resulted in a proverbial gold rush in drug development. Biotechnology startups have worked to discover novel microbiome-based drug candidates, and those with exceptional promise have been acquired by large pharmaceutical companies with the capital to bring them to commercial development.4,5 In 2022 and 2023, the Food and Drug Administration (FDA) issued the first approvals of such agents for the prevention of recurrent Clostridioides difficile infection (rCDI) in the United States (US).6 These drugs, derived from the human gut microbiome, have been designated a new class of medication called live biotherapeutic products (LBPs) or microbiome-based therapeutics (MBTs). Prior to these drugs, the only option for rCDI was fecal microbiota transplant (FMT). The FDA defines an LBP as a biological product that: 1) contains live organisms, such as bacteria; 2) is applicable to the prevention, treatment, or cure of a disease or condition of human beings; 3) is not a vaccine; and 4) as a general matter, is not administered by injection.7 FDA approval of two LBPs represents a major milestone in the path from bench to bedside for drug development; however, significant questions remain about this drug class. The LBPs currently approved or under investigation are either derived directly from human stool or contain a defined microbial component isolated from human stool during development and then processed for manufacture ex vivo.8–16 None of the LBPs have been studied either head-to head or against FMT in preventing rCDI. There is variability among the LBPs in their composition, biopharmaceutical science, dosage form design, and stages of development.3,17 Lastly, the human clinical trials for these agents in preventing rCDI had heterogeneity in study design, patient population, and clinical endpoints which make their comparison difficult. In this review, we aim to clear up some of this confusion by discussing the LBPs and explaining how they differ not only from conventional FMT but from one another. First, we will explain the role of the gut microbiome in Clostridioides difficile infection (CDI) and the morbidity of its recurrence. Next, we provide a history of stool-based therapies and explain the differences between LBPs and FMT. Last, we discuss the biopharmaceutics and clinical trials of the LBPs currently on the market and being investigated for approval, as well as their future directions.
Methodology
The literature search for this review was completed on July 1st, 2023, utilizing the keyword, “difficile” in the title/abstract section of PubMed. To capture important future drugs for CDI in early clinical development, the clinical trial database was also queried utilizing, “difficile” in the “condition of disease” term search on August 1st, 2023. Detailed information about the National Clinical Trial (NCT) numbers cited in this manuscript can be searched on the clinicaltrials.gov database.18 Therapies falling under the broad category of LBT or MBT were included as defined by the FDA definition.7 Drugs and investigational agents for CDI or rCDI falling out of this category were excluded including the following: antibiotic containing therapies, novel small molecules under investigation as antibiotics for CDI, immunoglobulin-based therapies (monoclonal or polyclonal antibodies) including those aimed at neutralizing C. difficile toxins, inhibiting growth, or preventing germination to the adult vegetative form, charcoal-based colon-specific antibiotic inactivators, and therapeutic beta-lactamase inhibitors.
Role of the Gut Microbiome in Colonization Resistance and Clostridioides Difficile Infection
The microbiome of human mucous membranes constitutes a micro-ecosystem containing trillions of microorganisms including bacteria, fungi, viruses, and bacteriophages.19,20 Over 1000 known species of bacteria reside in the human intestine, but upwards of 90% are from two main phyla; the Firmicutes (which include the Clostridioides, Lactobacillus, Bacillus), and the Bacteroidetes which include Bacteroides species.19,20 Disruption in these bacterial communities (dysbiosis) has been correlated to a broad range of negative health effects including gastrointestinal conditions like rCDI and inflammatory bowel disease (IBD), as well as extraintestinal conditions such as obesity and depression.8,19–21 When healthy and balanced, this population of microorganisms provides resistance to colonization of the gut from exogenous pathogens through a variety of mechanisms known as colonization resistance. These microbiota compete for key nutrients, produce inhibitory bile acids and short-chain fatty acids, lower the enteric luminal pH, and produce bacteriocins.20,22 This colonization resistance is crucial to understanding the pathophysiology of CDI and rCDI.8,19,22,23
The mechanism by which dysbiosis causes a loss of colonization resistance and predisposes to initial CDI and rCDI is increasingly being understood. Antibiotic use leads directly to dysbiosis by reducing the microbial diversity, or relative abundance of this ecosystem and is the most strongly associated risk factor for precipitating an initial episode of CDI.24–27 Changes in sleep, diet, lifestyle, and immune senescence that occur during aging also modify the microbiome.28 Gastric acid suppressant medications change the gut microecosystem pH and cause an imbalance in bacterial species resulting in increased proportions of Enterococcus, Streptococcus, and Staphylococcus species in older adults.29 Bile acid metabolism is also crucial in the human gut because alterations in the concentrations of primary and secondary bile acids as a result of dysbiosis are directly related to the risk of developing CDI after ingestion of C. difficile spores.30–35 Primary bile acids are produced by hepatocytes and converted into secondary bile acids by commensal anaerobic bacteria in the human intestine.32–34 The concentrations of these bile acids substantially determine whether an ingested C. difficile spore will remain dormant or will germinate into its metabolically active vegetative form as a gram-positive anaerobic rod.22,32–35 Hosts with higher levels of microbiome-derived secondary bile acids are more resistant to developing CDI after spore ingestion in both animal and human studies, whereas those with higher concentrations of primary bile acids are more susceptible to CDI.31–34 If the C. difficile spore germinates under the influence of primary bile acids, and the strain expresses genes for exotoxin production (Toxin A, Toxin B, or binary toxin), then active CDI occurs with symptoms ranging from mild diarrhea to toxic megacolon and death.30 Thus, alterations in the commensal gut microbiome and its metabolites set the stage for pathogens like C. difficile to cause disease as well as recur.
Burden and Morbidity of Recurrent Clostridioides Difficile Infection
Standard treatment of CDI includes administering antibiotics to target C. difficile while supporting the patient with resuscitative measures and surgical assessment as needed.36 Bezlotoxumab (a monoclonal antibody directed against C. difficile exotoxin B) offers protection against future recurrence by providing passive temporary immunity to toxin.36,37 Unfortunately, recurrence is common because none of the standard treatment strategies correct the underlying pathophysiology of dysbiosis and loss of colonization resistance that led to CDI. Around 35% of patients who experience an initial CDI will go on to have rCDI, and approximately 65% with a first recurrence will experience additional recurrences.38–40 Morbidity, severity of illness, and complications such as sepsis and the need for surgical intervention increase with each recurrent episode.41 A 2021 analysis of claims data found that in patients with three or more recurrences of CDI, rates of subtotal colectomy or diverting loop ileostomy within a year were 10%.41 These cases require considerable expenditure from patients and the health system with prolonged lengths of stay (median 33 days), yet have high rates of in-hospital mortality of 36–80%42 Aside from the burden of critical illness and medical complications, the toll of ongoing diarrhea experienced by rCDI patients can be substantial. Ongoing diarrhea prevents patients from performing their usual activities and engaging in social events which leads to emotional distress and reduced quality of life.43,44 A recent systematic review and cost synthesis analysis estimated the per-patient per-year rCDI attributable cost is $67,837 to $82,268.45 Ultimately, CDI recurrence is common and increasingly morbid with each episode in a self-perpetuating cycle. The lack of a standardized easily obtained therapy aimed at breaking this cycle of recurrence by restoring eubiosis to the gut microbiome has long been a missing piece of CDI management.
Historical Context of Fecal Microbiota Transplantation and Live Biotherapeutic Products
In the 4th century AD, Chinese alchemist Ge Hong described a treatment for food poisoning made by mixing herbs with the feces of a healthy person who consumed a diet of grain and fruit.46 Hong’s description of this, “Yellow Soup”, in his ancient text, “Baopuzi” (抱朴子), may have been the first recorded use of FMT.46–48 In 1958, Eismann et al published the first scientific manuscript describing FMT in a case series of 4 patients with pseudomembranous enterocolitis cured using fecal enemas.49 It would not be until the late 1970s that C. difficile was recognized as the pathogen responsible for antibiotic-associated diarrhea and pseudomembranous colitis.50,51 Incidence rates and severity of CDI increased throughout the US in the 1990s and early 2000s when the hypervirulent NAP1 strain of C. difficile emerged as a major public health issue.38,52 By 2013, CDI was deemed an urgent threat by the Centers for Disease Control and Prevention.53 During this time, FMT re-emerged as a non-conventional solution for CDI and rCDI.
FMT is a heterogenous process that involves harvesting stool from a healthy donor and transplanting it into the gastrointestinal tract of a recipient patient. FMT can be given by rectal enema, nasogastric tube, esophagogastroduodenoscopy (EGD), colonoscopy, or filled capsules.54–58 Medical centers began establishing FMT programs to meet patient demand; however, no standardized donor stool procurement process initially existed. Patients were asked to identify their own donors (often a healthy partner, friend, or family member).59,60 As use of FMT increased, the FDA took note of the lack of regulation and safety concerns associated with this practice and determined that FMT met the legal definition of a “drug” (since it was being used to prevent, treat, or cure a human disease or condition).61 In addition, since FMT had not been FDA approved for any clinical indication, it constituted an investigational drug that required providers to hold an investigational new drug (IND) permit.61 This led to significant administration burdens, not only for physicians treating rCDI with FMT, but also for clinical pharmacists tasked with creating policies to store or procure FMT.61 As a result, a joint society recommendation was released in 2013 from the Infectious Diseases Society of America (IDSA) and the American College of Gastroenterology (ACG) to guide the screening of donors and petition the FDA to relax its enforcement of IND applications and their burden on physicians treating acutely ill patients.62 Later that year, the IND application requirement was relaxed, and an IND was encouraged but not required for use of FMT to treat rCDI.63 Even with the relaxation of absolute requirements for an IDN, this process remained heterogenous. First, donors and their stool are tested for a variety of infectious diseases and the donated stool is quarantined, then certain screening tests are repeated prior to administration to the recipient. The logistics of this process have proven to be difficult, costly, and time consuming; resulting in donors not being identified or stool being discarded after donation.60,61,64 Furthermore, there was much heterogeneity in the manufacturing process for donated stool itself. FMT programs varied in where the donated samples were blended for administration (in a laboratory verses a clinical space), the time from donation to administration, the diluent choice (normal saline versus water), stool mass and volume administered, and infection control procedures.64 As a result of these difficulties, stool banks (such as OpenBiome) emerged as a means to address the limitations of procuring stool with a heterogenous patient-selected donor model. OpenBiome offered a centralized facility to screen donors, process stool, and store FMT preparations for use by clinicians and researchers.65,66 In order to meet FDA requirements, OpenBiome distributes investigational FMT preparations manufactured by the University of Minnesota under an IND application to physicians who are registered as, “Clinical Partners.”67 As part of the application, OpenBiome provides assurance of appropriate product storage and shipment, and clinicians must agree to assume the potential risk of any infectious agents not detected by the screening assays employed by OpenBiome and to notify the company within 24 hours of any adverse events.67 Despite having this stool bank to obtain product, most academic physicians do not have the regulatory experience to partake in this process, and FMT has remained a second-line treatment for rCDI.63 In addition, ongoing safety concerns of donor stool and a paucity of reliable access out of academic centers have further hampered FMT use.68,69 The clinical space, oversight, and resources to run an FMT practice have limited it to large academic centers with research experience.64,68 FMT has not traditionally been available for primary care doctors or sub-specialists caring for patients in rural areas without access to a larger medical center.
The clinical efficacy of FMT reported in the medical literature varies greatly. Over the preceding decades, a multiple of observational studies, systematic reviews, and clinical trials have been published giving FMT through various administration forms, to different patient populations, and for different indications (rCDI versus fulminant CDI). In terms of efficacy for rCDI, a meta-analysis of observational studies found efficacy rates of around 85%.70 The efficacy rates of FMT in clinical trials have shown more variation. For example, FMT efficacy rates for rCDI were much higher than placebo in a 2016 randomized clinical trial (90% vs 62.5%, respectively).71 Conversely, a clinical trial the following year showed efficacy rates of FMT given via enema for rCDI to be 44% versus 54% in a vancomycin taper group.72 A subsequent systematic review and meta-analysis of FMT found overall lower cure rates of around 67% in randomized trials (95% CI, 54.2%–81.3%, p < 0.001).73 Cure rates were even lower in a subgroup analysis of patients who received FMT via enema (66%) compared to colonoscopy (87%).73 The evidence for treating fulminant CDI with FMT is sparse and limited to mostly case-reports or small case-series. In a 2021 systematic review and meta-analysis of FMT for fulminant CDI, only one of the ten included studies was a randomized trial.74
As mentioned previously, widespread use of FMT has also been limited by safety concerns. Safety events including gram-negative bacteremia and aspiration of feculent material have been reported.75–78 In 2019, the FDA issued a safety alert after two immunocompromised patients developed invasive disease with extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli linked to FMT.79,80 FMT centers began screening for ESBL organisms in subsequent donations as a result of this tragedy. A reactive strategy of responding by adding additional testing for infectious pathogens as they arise is less ideal than a proactive strategy; however, it is impossible to anticipate most emerging infections. SARS-CoV-2 and mpox (formerly monkey pox) have continued to disrupt FMT programs and limit the availability of FMT to the masses.81 The logistic difficulties limiting the availability of FMT have led some patients to pursue dangerous do-it-yourself stool preparations with no physician oversight.82
Research and development of commercially available LBPs have emerged as a way to overcome these limitations by expanding access for patients outside of academic centers. It is exciting to imagine a future where a patient might simply undergo a single procedure such as a rectal administration or have specific bowel preparation before swallowing pills on an empty stomach and restore eubiosis; however, the biopharmaceutics needed to deliver these organisms outside of FMT remains quite complex. Most of the beneficial microbiota are obligate anaerobes or have various degrees of aerotolerance which make engineering their survival outside of the stool or laboratory complicated.83 Lyophilization (also known as freeze-drying) is used in biotechnology to preserve microorganisms and offered one possible solution for prolonging shelf stability of bacteria. Unfortunately, the membrane integrity and survival after lyophilization is suboptimal for many bacteria particularly for some gram negatives.84 As a result, scientists have had to develop new technology or other solutions (such as using spores) to overcome these limitations and bring new products to market.
LBPs and FMT: Similarities, Differences, and the Intricacies of Biopharmaceutical Drug Development
There are two commercially available off-The-shelf FMT stool bank products available in the US; MTP-101LR (for rCDI) and MTP-101LF (for fulminant CDI) from Open Biome.67 Both are delivered as a cryobag of 35 mL FMT for delivery via colonoscopy, sigmoidoscopy, enema, nasogastric tube or EGD, and neither are FDA approved.67 The MTP-101LF suspension contains ≥ 5×1011 bacteria while the MTP-101LF suspension for fulminant CDI contains ≥ 2.5×1012 bacteria (5-fold higher number of bacteria).85 Both contain human fecal matter sourced from qualified healthy traceable donors after screening for a panel of 29 transmissible pathogens including bacteria, viruses, and protozoa.85 Some FMT centers in the US have used freezing techniques to lyophilize FMT for administration in capsules; however, none are commercially available drug products.86–89
Commercially available LBPs have the potential to increase patient access to therapies capable of restoring the microbiome, but there are still some open questions about this drug class. The goal of an LBP is to inoculate the recipient’s intestinal microflora and restore eubiosis. Two broad differences to consider when comparing the LBPs to traditional FMT are the procurement process and the concept of selective manufacturing. Current LBPs are donor-derived (meaning they rely on thoroughly screening donor stool as the original source for their microbiologic components), while other developmental products are designed consortia (meaning they are cultivated in a laboratory).15,90–92 It should be noted that this distinction can be somewhat blurred and difficult to discern due to the proprietary nature of manufacturing. For example, some products described as designed consortiums were originally derived from the stool of a healthy donor but then subsequent manufacturing is done through in vitro proliferation of purified intestinal bacterial cultures.92,93 The donor-derived LBPs are similar to FMT in that they too require rigorous testing of donor stool to minimize the risk of transmitted pathogens. There are currently two donor-derived LBPs approved for rCDI; REBYOTA RBL™ (formerly RBX2660), VOWST, VOS ™(formerly SER-109), and two others which progressed into clinical trials but have since been halted from further development (RBX7455, and CP-101).11–15,94 The biologic components of these agents, which vary greatly when compared to FMT and to each other, will now be discussed.
In November 2022, the first FDA approved LBP was REBYOTA (fecal microbiota, live – jslm), formerly RBX2660 from Rebiotix, a Ferring pharmaceuticals company. REBYOTA is manufactured from human fecal matter sourced from qualified healthy traceable donors after screening for a panel of 29 transmissible pathogens including bacteria, viruses, and protozoa.95 The fecal microbiota suspension is filtered and processed in a pre-defined ratio with a solution of polyethylene glycol (PEG) 3350 and saline into a 150 mL enema. Each enema is verified to contain between 1×108 and 5×1010 colony forming units (CFU) per mL of fecal microbes including >1x105 CFU/mL of Bacteroides.95 The product requires storage at −80°C and is then thawed and then administered rectally via retention enema. No bowel preparation before the enema is required and it is administered as a one-time dose by any HCP. The second FDA approved LBP is VOWST (fecal microbiota spores, live-brpk) formerly SER-109. In 2021, Seres and Nestlé Health Science entered into an agreement to commercialize VOWST in the US and Canada, with FDA approval following in April 2023.96 VOWST is sourced from qualified donors after screening for pathogens; however, it is composed of spores rather than an isolated consortium of specific bacteria. The donated stool suspension is treated with ethanol to kill living vegetative organisms and the slurry is filtered to remove solids and isolate spores from the Firmicutes phyla such as Bacilli and Clostridia.13,97 The purified spores are resistant to gastric acid and are formulated into capsules each containing between 1×106 and 3×107 Firmicutes spore CFU in glycerol and saline.97 VOWST requires an initial dose of 10 ounces of magnesium citrate as a bowel washout for the previously consumed antibiotics, which is then followed by three consecutive days of four capsules orally once daily on an empty stomach.97
A third LBP which progressed to clinical trials, RBX7455, is from the same manufacturer of REBYOTA.12 RBX7455 is derived from the approved RBX2660 suspension and treated with a proprietary formulation of lyoprotectant and cryoprotectant excipients to stabilize the lyophilized bacteria at room temperature and against gastric acid into capsule form.12 Phase 1 trials of RBX7455 (NCT02981316) were published in 2021 with plans for further study; however, subsequent trials have not occurred.12 A fourth donor-derived LBP, CP101, was developed by Finch Therapeutics.94 Finch had partnered with Takeda Pharmaceutical Company in 2019 to develop several microbiome-based products including products they patented as Full-Spectrum Microbiota ® and Rationally Selected Microbiota®.98 CP101 was developed as a lyophilized capsule of, “full-spectrum microbiota containing diverse microorganisms”, and received FDA designations as both a breakthrough therapy and fast track status.94,98,99 The exact bacterial components and CFU per dose contained in CP101 were never specified; however, Finch does hold patents for C. difficile treatment containing a mixture of Actinobacteria, Proteobacteria, Firmicutes, and Bacteroidetes.100 CP101 was studied for rCDI and completed its Phase 2 trial (PRISM3) in 2021.99 In January 2023, Finch announced the decision to discontinue the Phase 3 trial of CP101 and halt all further development.101
All of the donor-derived LBPs may potentially contain donor-derived food allergens and carry a risk of transmitting known infectious agents, though this risk is considerably mitigated and no cases of food allergen events have been published to date.8,11,12,14,95,97 Similar to FMT, the donated stool used in LBPs is susceptible to emerging pathogens that may initially go undetected due to incorrect assay selection or a delay in recognition and development of a screening test.102 The manufacturing process for LBPs requires additional procedures beyond deep-freezing such as lyophilization or inactivation with ethanol. Whether the risk of infectious transmission of an emerging pathogen will be lower or mitigated by these additional manufacturing steps is unknown. The package inserts of both REBYOTA and VOWST state that the exact mechanisms of action have not been established, though both are approved for use in rCDI based on safety and efficacy data which will be discussed.95,97
In contrast to both donor-derived LBPs, designed LBPs have standardized compositions processed by batch culture for individual strains of microbes that are rationally defined and combined in a specific formulation.90,92 The term “rationally” designed or defined is often used by the companies to self-describe these agents based on the inclusion of only certain bacterial species selected for manufacture in a laboratory environment based on their proposed biologic functions. As of late 2023, all the designed LBPs (VE303, NTCD-M3, ADS024, MET-2, and SER-262) remain under clinical investigation. The first of these, VE303, was developed by Vedanta Biosciences based on the ability of commensal Clostridium species to increase secondary bile acids and short chain fatty acids associated with colonization resistance against C. difficile.103,104 VE303 is a defined consortium of eight commensal strains of clonally derived and distinct Clostridium species (5 strains from Clostridia cluster XIVa, 2 from cluster IV, and 1 from cluster XVII) manufactured into an enteric capsule. Each capsule contains 1×108 CFU of lyophilized bacteria from each species for a total 8×108 CFU of bacteria in 400mg combined with sucrose, histidine, yeast extract, cysteine, and other excipients.103,104 Clinical Phase 2 trials of VE303 are complete (NCT03788483). A phase 3 trial of VE303 was planned to initiate in 2023 but is yet to be listed on clinicaltrials.gov.
Another designed LBP under investigation is non-toxigenic C. difficile strain M3 (NTCD-M3), formerly known as VP20621. It was previously observed that strains of C. difficile lacking the genes for toxin production could prevent CDI upon exposure to a toxigenic strain in animal models and healthy human volunteers.105,106 Takeda (Shire) pharmaceuticals completed Phase 2 trials in 2015 on an oral capsule formulation of NTCD-M3 (NCT01259726).106 Initially, there was a concern about utilizing non-toxigenic strains such as NTCD-M3 due to in vitro data demonstrating that a toxigenic C. difficile strain was able to pass its toxin genes to a nontoxic strain CD37 via horizontal gene transfer.107 In 2022, the passive gene transfer experiment was replicated on NTCD-M3 using the same toxin donor strain and no toxin gene transfer occurred.108 Additionally, this phenomenon has not been documented in humans and was not reported in the phase 2 trials of NTCD-M3. A phase 1 colonization study using NTCD-M3 in healthy Dutch volunteers was planned to commence in 2023; however, no other trials of NTCD are currently registered (NCT05693077).
A third designed LBT, called MET-2, was developed by Microbial Ecosystem Therapeutics (a merger between Takeda Pharmaceuticals and NuBiyota LLC).109,110 Prior to MET-2, MET-1 (formerly known as RePOOPulate) was developed as a stool substitute designed to be an alternative to FMT.111 MET-1 contained a defined microbial consortium of 33 bacterial strains in 100 mL (3.5 x 109 CFU/mL) made from purified intestinal bacterial cultures originally derived from the stool of a single healthy human donor.111 MET-2 contains a proprietary consortium of 40 species from strains which are then purified and combined as a lyophilized product into capsules for oral delivery.93 Phase 1 trials of MET-2 for treating CDI were completed and published in 2021 (NCT02865616).93 This oral lyophilized product falls somewhere between a donor-derived LBP and designed LBP in that the bacterial species were initially isolated from the stool of a healthy screened donor, but subsequently manufactured independently of the donor thus eliminating potential risks introduced by changes in donor health.93,110 Phase 2 trials of MET-2 are planned.
A fourth designed LBP under active study is ADS024 (formerly ART24). ADS024 is a strain of Bacillus velezensis owned by Artugen Therapeutics which merged with Bacainn Therapeutics in 2022 to form Adiso Therapeutics.112 Adiso classifies ADS024 as a single strain LPB, or SS-LBP, since it is composed of a single strain of B. velezensis.113 B. velezensis has been shown to combat C. difficile through two main mechanisms; by directly killing it via inhibition of translation and membrane permeabilization and by reducing toxicity through proteases capable of degrading C. difficile toxin.9 Phase 1 trials administering capsules containing lyophilized ADS024 were completed in October 2022 (NCT04891965). A February 2023 review of emerging CDI therapies notes that Artugen currently holds two patents on ADS024, one listing a composition of lyophilized ART24 spores and another composed of spores or a vegetative form of the bacteria along with edible legumes.114–116 In addition, clinicaltrials.gov lists a study for B. velezensis designated DSM3384 (DifProtecTM) sponsored by Novozymes A/S, a subsidiary of the Novo Nordisk Foundation (NCT05606159).117 DifProtec TM is patented as a probiotic capsule rather than an LBP, but analogous to ADS024 it contains Bacillus velezensis. A table summarizing the LBPs approved or in clinical trials including their formulation and administration parameters is summarized in Table 1.
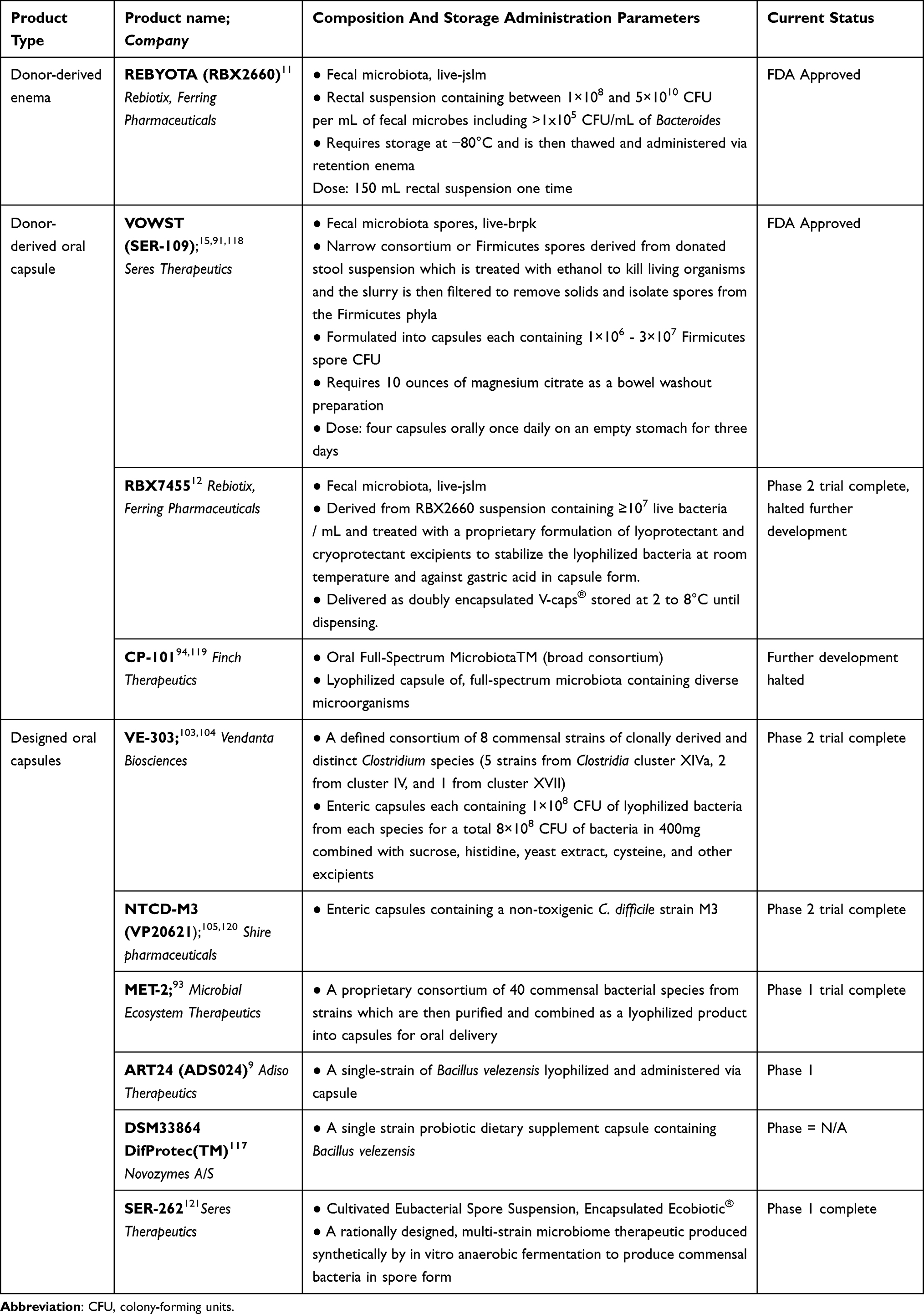 |
Table 1 Live Biotherapeutic Products Approved or in Clinical Trials for Preventing Recurrent Clostridioides Difficile Infection |
The definition of an LBP may seem straight forward, but the distinctions between the LBP products can be confusing for providers unfamiliar with this drug class. Some LBPs are composed of broad microbiota consortia (either spores or bacteria), while others contain a single phylum or even a single species.12,93,94,99,110,122 Some LBPs are delivered via enema, while others are administered as oral capsules after lyophilization which may or may not require a bowel preparation before-hand. It makes logical sense to consider a product with a set number of bacterial species distinct from one with hundreds or thousands, however, there is no consensus on the where this distinction lies and LBPs currently exist on a spectrum. In a scientific sense, some LBPs may not be drastically different from an FMT, but in a practical sense these products are quite different. Lyophilization of an FMT for oral administration required patients to take large numbers of capsules (average 27–40) in one dose whereas the oral LBPs require far fewer capsules.14,86 Furthermore, the FDA approved LBPs can be ordered like any other medication and produced in facilities capable of mass production using good manufacturing practice standards. They not only expand availability for patients but also transfer the oversight and liability in procuring a microbiome product from the physician to the drug manufacturer and FDA.8,17 In a similar vein, the distinction between a narrow spectrum LBT verses a probiotic can also seem arbitrary. Single strain commensal bacterial such as Lactobacillus species have long been used by patients with gastrointestinal issues, yet these probiotic products have always been classified as dietary supplements rather than drugs since they have not undergone the FDA approval regulatory process. Similarly, DifProtec (which contains B. velezensis) is listed in the clinical trials website as a probiotic dietary supplement (NCT05606159). In contrast, ADS024 is classified as a single strain LBP, yet it contains only B. velezensis (NCT04891965). As the biopharmaceutics and clinical use of this heterogenous drug class expands, our definitions and categories of LBPs may continue to be refined over time.
Clinical Trials of the FDA Approved LBPs (REBYOTA and VOWST)
REBYOTA and VOWST were both recently FDA approved for prevention of rCDI based on clinical trial data demonstrating safety and efficacy.11,14 Neither agent has been compared head to head or to bezlotoxumab or FMT in their ability to prevent rCDI. There was considerable heterogeneity between the trials leading to the FDA approval of these agents which must be discussed. REBYOTA (formerly RBX 2660) was studied in the PUNCH CD trials. This started with a phase 1 open-label, noncomparative study in 2016 showing that it was safe and effective in preventing rCDI in patients who had had two or more recurrences (at least 3 life time episodes), or two episodes requiring hospitalization.123 After two enemas of REBYOTA, 87% (27/31) had no further recurrences at 8 weeks.123 This study was followed by a multi-center open-label phase 2 (PUNCH CD2) trial including a similar patient population (≥2 previous rCDI episodes or ≥2 severe CDI requiring hospitalization).124 One cohort of patients were given up to 2 doses of REBYOTA (143 participants received 2 doses and 6 participants received one dose) and compared to a cohort of historical matched controls. REBYOTA patients had 79% treatment success compared to 31% success in the historic group at 8 weeks (P<0.0001).124 Durability of this protective response at 6, 12, and 2 years was demonstrated in a subsequent publication.125 A phase 2B, placebo-controlled, dose-ranging study followed, showing favorable recurrence rates after a single dose of REBYOTA; in the per-protocol population, 19% (3/24) of participants had recurrence after one dose of drug and one dose of placebo, compared to 52% (13/31) of those who received two doses placebo (p = 0.017).126 These results culminated in PUNCH CD3, the randomized, double-blind phase 3 trial comparing REBYOTA to placebo that gained FDA approval.11 Inclusion criteria were less strict than the prior PUNCH CD trials in that patients had ≥1 previous recurrences (at least 2 lifetime episodes), or to recruitment challenges, the FDA proposed with an analysis of the primary endpoint (absence of CDI diarrhea at 8 weeks) using a Bayesian hierarchical model that borrowed information from the phase IIb trial, PUNCH CD2. Within 30 days of enrollment, participants had to have tested positive for CDI by polymerase chain reaction (PCR), enzyme immunoassay (EIA), or another assay. Notably, 73% of total patients had positive PCR testing at inclusion, and only 17% had positive glutamate dehydrogenase (GDH) (20% in the REBYOTA arm and 11.5% in the placebo arm). Statistical modeling showed that 71% of participants treated with REBYOTA and 58% of participants treated with placebo remained free of CDI recurrence through 8 weeks, meeting the threshold for superiority to placebo determined by Bayesian analysis.11 This 13.1 percentage difference in blinded treatment success corresponds to a 99.1% posterior probability that REBYOTA is superior to Placebo (95% Credible Interval: 2.3, 24.0).11 In the per protocol analysis, 72% (120/167) of REBYOTA patients had treatment success compared to 62% (48/78) of placebo patients.11 The observed treatment difference at 8 weeks was maintained at 6 months across all analysis populations (ITT and per protocol). After confirmation of treatment failure, 65 participants (41 who had received REBYOTA and 24 who had received placebo) were subsequently given REBYOTA in an open-label treatment arm. Treatment success at 8 weeks occurred in 54% (22/41) in the group that had already received blinded REBYOTA and 63% (15/24) who had received blinded placebo.11 Most adverse effects were mild to moderate gastrointestinal side effects such as abdominal pain, diarrhea, or bloating and were similar between drug and placebo. No new or unexpected events were reported and no pathogen transfer from donor to recipient, product-related significant adverse events, or procedure-related events occurred.11 In a subsequent safety analysis from five prospective clinical trials (PUNCH CD, PUNCH CD2, PUNCH Open-Label) and two Phase III trials (PUNCH CD3, PUNCH CD3-OLS) including 978 patients, no cases of bacteremia, fungemia, or treatment-related infections occurred.127 In a secondary analysis of PUNCH CD3 patients comparing quality of life scores at weeks 1, 4, and 8, REBYOTA treated patients showed significantly greater improvements in mental health domains than those receiving placebo.128
Notable limitations of the PUNCH CD3 trial include the high success rate in the placebo arm and the diagnostic inclusion criteria. One hypothesis for the high rates of placebo response is the influence of positive PCR as the most common diagnostic modality for inclusion. The PCR assay is for detecting toxin genes. This method can be overly sensitive since it cannot determine whether the genes are being transcribed and cannot distinguish between living and dead organism containing the gene; none-The-less, patients presenting with diarrhea may have PCR testing as part of their diagnosis.129 Seventy-three percent of participants included in PUNCH CD3 had positive PCR as their CDI confirmation method.11 While this approach is less rigorous to avoid false-positive results, it is practical for real-world practice. About one-third of patients enrolled in PUNCH CD3 had had only one rCDI occurrence at inclusion and thus may have been at lower baseline risk for recurrence compared to cohorts with two or more recurrences prior to inclusion.11 If included patients did not truly have rCDI due to the diagnostic testing, then this could perhaps explain the high rates of clinical success in the placebo group. Another limitation is the paucity of patients who were treated with fidaxomicin, which is known to have lower rates of recurrence compared to vancomycin and metronidazole.36 The study randomization was stratified by antibiotics used for the qualifying CDI event (vancomycin alone, vancomycin in combination with another antibiotic, fidaxomicin alone, or other); however, the trial was conducted prior to more recently updated IDSA guidelines preferentially recommending fidaxomicin as first-line treatment over oral vancomycin both for the first episode of CDI and for rCDI. About 6% (17/267) of participants received fidaxomicin for their qualifying rCDI event.11 Whether the clinical success of REBYOTA would be as robust in a cohort treated with fidaxomicin is unknown. Lastly, some patients who experience rCDI such as those with immunocompromise or IBD were excluded from participating; however, subsequent data has shown promising results for such patients.130 Outcomes on 94 patients who were excluded from PUNCH CD3 due to immunocompromise or bowel disease conditions were later given RBX2660 under FDA discretion. Results presented at the ACG 2021 National Meeting showed efficacy of 83% and no significant safety events.130
VOWST (formerly SER-109) was studied in the ECOSPOR trials starting with ECOSPOR I, a phase 1 trial conducted at four US medical centers.131 Participants in ECOSPOR I had ≥3 laboratory-confirmed CDI episodes in the previous 12 months. SER-109 manufactured for the trial was taken from seven adult donors after screening and processing which included a deep freeze to −80°C followed by homogenization, filtration, ethanol washing and several steps of centrifugation to isolate Firmicutes spores.131 Twenty-six of 30 (87%) participants met the primary efficacy end point of no recurrence at 8 weeks. Three patients with self-limiting diarrhea and positive CDI testing had clinical resolution without antibiotics bringing overall clinical success to 97% (29/30 participants). The gut microbiota of participants were also studied to verify whether the Firmicutes spores had engrafted and confirmed a diversified microbiome and no outgrowth of non–spore-forming bacteria after VOWST treatment.131 A significant setback occurred during ECOSPOR II, the subsequent phase 2 double-blind trial comparing VOWST to placebo in patients with 3 or more CDI episodes within 9 months. Rates of rCDI at 8 weeks were lower in the VOWST arm versus placebo (44% vs 53%), however, this did not meet statistical significance (NCT02437487).13 This was attributed to the use of PCR testing for diagnosis in most participants, as well as engraftment kinetics which suggested that VOWST was suboptimally dosed (1 x 108 spores).13 In the following phase 2b/3 trial (ECOSPOR III), the trial design and dose of VOWST were adjusted based on these previously observed issues. The daily dose of spores contained in the four VOWST capsules was increased three-fold (3 x 107 spores contained in a total of four capsules), and the doses were given for three consecutive days instead of once.14,16 VOWST capsules were taken on an empty stomach after a bowel preparation of 10 ounces of magnesium citrate was administered the night before treatment initiation to limit inactivation of the spores. Participants had three or more episodes of CDI within 12 months, and the inclusive qualifying acute episode had to be diagnosed with a positive C. difficile toxin test by EIA or cell cytotoxicity neutralization assay.14 CDI recurrence was significantly lower with VOWST compared to placebo at 8 weeks (12% versus 40%, respectively; P<0.001).14 Results were consistent in analyses with stratification according to age and antibiotic received (vancomycin versus fidaxomicin). Vancomycin was given prior to VOWST in 133/182 (73%) patients, and fidaxomicin was given to 49/182 (27%). Risk of recurrence was reduced in the VOWST cohort regardless of previous antibiotic regimen (relative risk, 0.41 [95% CI, 0.22 to 0.79] with vancomycin and 0.09 [95% CI, 0.01 to 0.63] with fidaxomicin).14 Durability and safety at 24 weeks were subsequently shown in an open-label single-arm trial. (ECOSPOR IV)132,133 The most common significant adverse events were mild to moderate gastrointestinal complaints and were observed at rates similar to that of placebo.14,132,133
A notable strength of ECOSPOR III was the strict inclusion criteria for toxin testing which ensured appropriate candidate selection and accuracy of the definition of recurrence; however, real-world diagnosis of rCDI is seldom this stringent. While encouraging, it is unknown if these robust results would be demonstrated in routine clinical practice. ECOSPOR IV attempted to address this by separating patients into two cohorts: one including ECOSPOR III rollover patients and another less strict cohort of de novo patients with at least 1 CDI recurrence diagnosed by any detection method.132 This included 69/263 (26%) patients who had their rCDI episode diagnosed using PCR alone.132 Rates of rCDI at 8 weeks were low, even in patients with a first recurrence (6.5%) or enrollment based on positive PCR results (4.3%).132 Rates of fidaxomicin use were higher in ECOSPOR III than PUNCH CD3 (30% versus 6%, respectively), but neither trial was powered to detect superiority in only those patients.11,14 Similar to the REYBOTA trials, patients who were immunocompromised or had IBD were excluded from the VOWST trials. Investigational use in an expanded access program is ongoing (NCT02437500).134
Given the heterogeneity in data used to approve these agents based on their performance against placebo, it is impossible to compare their clinical efficacy directly. Both appear to have only mild to moderate gastrointestinal side effects and no major safety events, though post-marketing surveillance is ongoing.127,132 Some patients may be interested in an oral regimen that can be taken discreetly at their home, while others may prefer a one-time treatment in a clinical setting. A recent survey of LBP-naïve subjects with prior CDI showed that 87% were likely to consider a rectally administered treatment and that patients who had received a rectal LBP found it easy, quick, and appealing due to lack of bowel preparation.135 Future financial analysis studies may show the high cost of these products ($17,500 USD for VOWST and $9100 USD for REBYOTA) is worth avoiding a high expenditure hospitalization for rCDI where the direct attributable medical cost can range from $67,837 to $82,268.45,136 Budget impact analysis of potential cost savings for new LBPs is already being published.137 Similar analyses advocating for bezlotoxumab have been performed and yet pharmacy budgets have not been increased to account for inpatient use and payors continue to impede prescribing it without prior authorization.138,139 Whether an increased number of therapeutic options for rCDI will influence the costs of existing agents on the market remains to be seen. Ultimately, the choice of LBP selected for rCDI prevention will depend on patient preference, prescriber opinion, and cost. A summary of REBYOTA and VOWST clinical trial parameters is shown in Table 2.
 |
Table 2 Clinical Trial Data for REBYOTA and VOWST |
Future Directions and Conclusion
The LBPs are important new tools in our armamentarium against CDI, but some questions remain. FMT has traditionally only been prescribed by subspecialists in gastroenterology and infectious diseases, but LBPs can be prescribed by any provider. The impact of practitioners with little experience using microbiome-based treatments prescribing these drugs is unknown.17 As we approach four years from the start of the SARS-CoV2 pandemic, we are left to wonder if an unknown pathogen may be encountered in the future which would require additional screening in the LBP manufacturing process. Bioscience companies and pharmaceutical companies have merged to gain the capital needed to bring LBPs to the market, but the exact components are sometimes proprietary emerging biotechnology. It is difficult to provide full information to patients for informed consent when some of these products are ambiguous about the exact species contained therein.
The LBPs continue to push the boundaries of their potential by branching into conditions beyond CDI. As of late 2023, there are clinical trials sponsored by several companies with a foothold in the LBP market. Ferring pharmaceuticals is studying RBX7455 before surgery in operable breast cancer (NCT04139993), Vedanta Biosciences is investigating VE303 for hepatic encephalopathy (NCT04899115), and VE 202 for ulcerative colitis (NCT05370885), and Seres therapeutics is studying SER-155 for preventing graft-versus host disease in hematopoietic stem cell transplantation (NCT04995653) and antimicrobial-resistant bacterial infections.140–143 Early pre-trial exploration of the bidirectional relationship between the gut microbiome and other conditions including depression, obesity, and other malignancies are also already underway.21,144
LBPs such as REBYOTA & VOWST, appear poised to strike the perfect balance between traditional healing and emerging science; restoring eubiosis as nature intended while simultaneously giving patients the guarantee of safety that comes inherently with an FDA-approved medication. These products are an exciting addition to our limited options for rCDI. Whether their widespread availability will result in unfettered use is unknown. Post-marketing surveillance will be crucial for monitoring their appropriate use and detecting rare safety events or latent events not seen in clinical trials. Even the greatest breakthroughs in medicine must be tempered with cautious optimism, healthy skepticism, and ongoing data collection. As the idiom goes, the devil is in the details.
Disclosure
Dr Glenn Tillotson is a consultant for Ferring Pharmaceuticals, Spero Therapeutics, and Taro Pharmaceuticals, outside the submitted work. The author reports no other conflicts of interest in this work.
References
1. Martin TC, Visconti A, Spector TD, et al. Conducting metagenomic studies in microbiology and clinical research. Appl Microbiol Biotechnol. 2018;102(20):8629–8646. doi:10.1007/s00253-018-9209-9
2. Integrative, HMP. The integrative human microbiome project. Nature. 2019;569(7758):641–648. doi:10.1038/s41586-019-1238-8
3. Oliveira RA, Pamer EG. Assembling symbiotic bacterial species into live therapeutic consortia that reconstitute microbiome functions. Cell Host Microbe. 2023;31(4):472–484. doi:10.1016/j.chom.2023.03.002
4. Eid AJ, Razonable RR. New developments in the management of cytomegalovirus infection after solid organ transplantation. Drugs. 2010;70(8):965–981. doi:10.2165/10898540-000000000-00000
5. Seres therapeutics announces strategic collaboration with nestlé health science for microbiome-based clostridium difficile and inflammatory bowel disease therapies in markets outside of north America. 2016.
6. FDA approves first fecal microbiota product. 2022.
7. Claro T, Widaa A, O’Seaghdha Met al. Staphylococcus aureus protein A binds to osteoblasts and triggers signals that weaken bone in osteomyelitis. PLoS One. 2011;6(4):e18748.
8. Wang R. Clostridioides difficile infection: microbe-microbe interactions and live biotherapeutics. Front Microbiol. 2023; 14:1182612.
9. O’Donnell MM, Hegarty JW, Healy B, et al. Identification of ADS024, a newly characterized strain of bacillus velezensis with direct Clostridiodes difficile killing and toxin degradation bio-activities. Sci Rep. 2022;12(1):9283. doi:10.1038/s41598-022-13248-4
10. Xie Y, Chupina Estrada A, Nelson B, et al. ADS024, a Bacillus velezensis strain, protects human colonic epithelial cells against C. difficile toxin-mediated apoptosis. Front Microbiol. 2022;13:1072534. doi:10.3389/fmicb.2022.1072534
11. Khanna S, Assi M, Lee C, et al. Efficacy and safety of RBX2660 in PUNCH CD3, a phase III, randomized, double-blind, placebo-controlled trial with a bayesian primary analysis for the prevention of recurrent clostridioides difficile infection. Drugs. 2022;82(15):1527–1538. doi:10.1007/s40265-022-01797-x
12. Khanna S, Pardi DS, Jones C, et al. RBX7455, a non-frozen, orally administered investigational live biotherapeutic, is safe, effective, and shifts patients’ microbiomes in a phase 1 study for recurrent clostridioides difficile infections. Clin Infect Dis. 2021;73(7):e1613–e1620. doi:10.1093/cid/ciaa1430
13. McGovern BH, Ford CB, Henn MR, et al. SER-109, an investigational microbiome drug to reduce recurrence after clostridioides difficile infection: lessons learned from a phase 2 trial. Clin Infect Dis. 2021;72(12):2132–2140. doi:10.1093/cid/ciaa387
14. Feuerstadt P, Louie TJ, Lashner B, et al. SER-109, an oral microbiome therapy for recurrent clostridioides difficile Infection. N Engl J Med. 2022;386(3):220–229. doi:10.1056/NEJMoa2106516
15. McChalicher C, Abdulaziz A, Zhou SS, et al. Manufacturing Process of SER-109, a purified investigational microbiome therapeutic, reduces risk of coronavirus transmission from donor stool. Open Forum Infect Dis. 2022;9(9):448. doi:10.1093/ofid/ofac448
16. Khanna S, et al. SER-109: an oral investigational microbiome therapeutic for patients with recurrent clostridioides difficile infection (rCDI). Antibiotics. 2022;11(9):1.
17. Hota SS, Poutanen SM. Microbiome-Based Therapeutics for Clostridioides Difficile Infection: Helpful Solutions or Unclear Cocktails? Lancet Infect Dis; 2023.
18. Murillo O, Roset A, Sobrino B, et al. Streptococcal vertebral osteomyelitis: multiple faces of the same disease. Clin Microbiol Infect. 2014;20(1):O33–8. doi:10.1111/1469-0691.12302
19. Gou HZ, Zhang Y-L, Ren L-F, et al. How do intestinal probiotics restore the intestinal barrier? Front Microbiol. 2022;13:929346. doi:10.3389/fmicb.2022.929346
20. Haran JP, McCormick BA. Aging, frailty, and the microbiome-How dysbiosis influences human aging and disease. Gastroenterology. 2021;160(2):507–523. doi:10.1053/j.gastro.2020.09.060
21. Mohan A, Godugu S, Joshi SS, et al. Gut-brain axis: altered microbiome and depression - review. Ann Med Surg Lond. 2023;85(5):1784–1789. doi:10.1097/MS9.0000000000000573
22. Seekatz AM, Safdar N, Khanna S. The role of the gut microbiome in colonization resistance and recurrent Clostridioides difficile infection. Therap Adv Gastroenterol. 2022;15:17562848221134396. doi:10.1177/17562848221134396
23. Dawkins JJ, Allegretti JR, Gibson TE, et al. Gut metabolites predict Clostridioides difficile recurrence. Microbiome. 2022;10(1):87. doi:10.1186/s40168-022-01284-1
24. Feuerstadt P, Nelson WW, Teigland C, et al. Clinical burden of recurrent clostridioides difficile infection in the medicare population: a real-world claims analysis. Anti Stewar Healthcare Epid. 2022;2(1):e60. doi:10.1017/ash.2022.2
25. Davies K. Risk factors for primary clostridium difficile infection; results from the observational study of risk factors for clostridium difficile infection in hospitalized patients with infective diarrhea; 2020. 8.
26. Tabak YP, Srinivasan A, Yu KC, et al. Hospital-level high-risk antibiotic use in relation to hospital-associated Clostridioides difficile infections: retrospective analysis of 2016–2017 data from US hospitals. Infect Control Hosp Epidemiol. 2019;40(11):1229–1235. doi:10.1017/ice.2019.236
27. Brown KA, Langford B, Schwartz KL, et al. Antibiotic prescribing choices and their comparative c. difficile infection risks: a longitudinal case-cohort study. Clinl Infect Dis. 2020;72(5):836–844. doi:10.1093/cid/ciaa124
28. Nagpal R, Mainali R, Ahmadi S, et al. Gut microbiome and aging: physiological and mechanistic insights. Nutr Healthy Aging. 2018;4(4):267–285. doi:10.3233/NHA-170030
29. Imhann F, Bonder MJ, Vich Vila A, et al. Proton pump inhibitors affect the gut microbiome. Gut. 2016;65(5):740–748. doi:10.1136/gutjnl-2015-310376
30. Abt MC, McKenney PT, Pamer EG. Clostridium difficile colitis: pathogenesis and host defence. Nat Rev Microbiol. 2016;14(10):609–620. doi:10.1038/nrmicro.2016.108
31. Aguirre AM, Sorg JA. Gut associated metabolites and their roles in Clostridioides difficile pathogenesis. Gut Microbes. 2022;14(1):2094672. doi:10.1080/19490976.2022.2094672
32. Giel JL, Sorg JA, Sonenshein AL, et al. Metabolism of bile salts in mice influences spore germination in Clostridium difficile. PLoS One. 2010;5(1):e8740. doi:10.1371/journal.pone.0008740
33. Mullish BH, Allegretti JR. The contribution of bile acid metabolism to the pathogenesis of Clostridioides difficile infection. Therap Adv Gastroenterol. 2021;14:17562848211017725. doi:10.1177/17562848211017725
34. Sorg JA, Sonenshein AL. Bile salts and glycine as cogerminants for Clostridium difficile spores. J Bacteriol. 2008;190(7):2505–2512. doi:10.1128/JB.01765-07
35. Theriot CM, Koenigsknecht MJ, Carlson PE, et al. Antibiotic-induced shifts in the mouse gut microbiome and metabolome increase susceptibility to Clostridium difficile infection. Nat Commun. 2014;5(1):3114. doi:10.1038/ncomms4114
36. Johnson S, Lavergne V, Skinner AM, et al. Clinical practice guideline by the infectious diseases society of America (IDSA) and society for healthcare epidemiology of America (SHEA): 2021 focused update guidelines on management of clostridioides difficile infection in adults. Clinl Infect Dis. 2021;73(5):e1029–e1044. doi:10.1093/cid/ciab549
37. Wilcox MH, Gerding DN, Poxton IR, et al. Bezlotoxumab for prevention of recurrent clostridium difficile infection. New England J Med. 2017;376(4):305–317. doi:10.1056/NEJMoa1602615
38. Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile Infection in the United States. New England J med. 2015;372(9):825–834. doi:10.1056/NEJMoa1408913
39. Leong C, Zelenitsky S. Treatment strategies for recurrent clostridium difficile infection. Can J Hosp Pharm. 2013;66(6):361–368. doi:10.4212/cjhp.v66i6.1301
40. Cornely OA, Miller MA, Louie TJ, et al. Treatment of first recurrence of Clostridium difficile infection: fidaxomicin versus vancomycin. Clin Infect Dis. 2012;2(Suppl 2):S154–61. doi:10.1093/cid/cis462
41. Feuerstadt P, Boules M, Stong L, et al. Clinical complications in patients with primary and recurrent Clostridioides difficile infection: a real-world data analysis. SAGE Open Med. 2021;9:2050312120986733. doi:10.1177/2050312120986733
42. Hall JF, Berger D. Outcome of colectomy for Clostridium difficile colitis: a plea for early surgical management. Am J Surg. 2008;196(3):384–388. doi:10.1016/j.amjsurg.2007.11.017
43. Lurienne L, Bandinelli P-A, Galvain T, et al. Perception of quality of life in people experiencing or having experienced a Clostridioides difficile infection: a US population survey. J Patient Rep Outcomes. 2020;4(1):14. doi:10.1186/s41687-020-0179-1
44. Guillemin I, Marrel A, Lambert J, et al. Patients’ experience and perception of hospital-treated Clostridium difficile infections: a qualitative study. Patient. 2014;7(1):97–105. doi:10.1007/s40271-013-0043-y
45. Reveles KR, Yang M, Garcia-Horton V, et al. Economic impact of recurrent clostridioides difficile infection in the USA: a systematic literature review and cost synthesis. Adv Ther. 2023;40(7):3104–3134. doi:10.1007/s12325-023-02498-x
46. Wells M. Self as historical artifact: ge Hong and early Chinese autobiographical writing. Early Med China. 2003;2003(1):71–103. doi:10.1179/152991003788138465
47. Stripling J, Rodriguez M. Current evidence in delivery and therapeutic uses of fecal microbiota transplantation in human diseases-clostridium difficile disease and beyond. Am J Med Sci. 2018;356(5):424–432. doi:10.1016/j.amjms.2018.08.010
48. de Groot PF, Frissen MN, de Clercq NC, et al. Fecal microbiota transplantation in metabolic syndrome: history, present and future. Gut Microbes. 2017;8(3):253–267. doi:10.1080/19490976.2017.1293224
49. Eiseman B, Silen W, Bascom GS, et al. Fecal enema as an adjunct in the treatment of pseudomembranous enterocolitis. Surgery. 1958;44(5):854–859.
50. Bartlett JG, Moon N, Chang TW, et al. Role of Clostridium difficile in antibiotic-associated pseudomembranous colitis. Gastroenterology. 1978;75(5):778–782. doi:10.1016/0016-5085(78)90457-2
51. George WL, Goldstein EC, Sutter V, et al. Aetiology of antimicrobial-agent-associated colitis. Lancet. 1978;1(8068):802–803. doi:10.1016/S0140-6736(78)93001-5
52. Giancola SE, Williams RJ, Gentry CA. Prevalence of the clostridium difficile bi/nap1/027 strain across the United States veterans health administration. Clin Microbiol Infect. 2018;24(8):877–881. doi:10.1016/j.cmi.2017.11.011
53. Prevention CJTR. Antibiotic resistance threats in the United States, 2013; 2013;50–52.
54. van Nood E, Vrieze A, Nieuwdorp M, et al. Duodenal infusion of donor feces for recurrent clostridium difficile. New England J med. 2013;368(5):407–415. doi:10.1056/NEJMoa1205037
55. Postigo R, Kim JH. Colonoscopic versus nasogastric fecal transplantation for the treatment of Clostridium difficile infection: a review and pooled analysis. Infection. 2012;40(6):643–648. doi:10.1007/s15010-012-0307-9
56. Schwan A. Relapsing clostridium difficile enterocolitis cured by rectal infusion of homologous faeces. Lancet. 1983;2(8354):845. doi:10.1016/S0140-6736(83)90753-5
57. Allegretti JR, Fischer M, Sagi SV, et al. Fecal microbiota transplantation capsules with targeted colonic versus gastric delivery in recurrent clostridium difficile infection: a comparative cohort analysis of high and Lose dose. Dig Dis Sci. 2019;64(6):1672–1678. doi:10.1007/s10620-018-5396-6
58. Aas J, Gessert CE, Bakken JS. Recurrent Clostridium difficile colitis: case series involving 18 patients treated with donor stool administered via a nasogastric tube. Clin Infect Dis. 2003;36(5):580–585. doi:10.1086/367657
59. Woodworth MH, Carpentieri C, Sitchenko KL, et al. Challenges in fecal donor selection and screening for fecal microbiota transplantation: a review. Gut Microbes. 2017;8(3):225–237. doi:10.1080/19490976.2017.1286006
60. Khoruts A. Fecal microbiota transplantation-early steps on a long journey ahead. Gut Microbes. 2017;8(3):199–204. doi:10.1080/19490976.2017.1316447
61. Koopman N, van Leeuwen P, Brul S, et al. History of fecal transplantation; camel feces contains limited amounts of Bacillus subtilis spores and likely has no traditional role in the treatment of dysentery. PLoS One. 2022;17(8):e0272607. doi:10.1371/journal.pone.0272607
62. Relman D, Rustgi A, Vender R. Joint Society letter to FDA—Current consensus guidance on donor screening and stool testing for FMT; 2013.
63. Kelly CR, Kunde SS, Khoruts A. Guidance on preparing an investigational new drug application for fecal microbiota transplantation studies. Clin Gastroenterol Hepatol. 2014;12(2):283–288. doi:10.1016/j.cgh.2013.09.060
64. Hota SS. Regional variability in fecal microbiota transplantation practices: a survey of the southern Ontario fecal microbiota transplantation movement. Can Med Assoc J. 2018;6(2):E184–E190.
65. Panchal P, Budree S, Scheeler A, et al. Scaling safe access to fecal microbiota transplantation: past, present, and future. Curr Gastroenterol Rep. 2018;20(4):14. doi:10.1007/s11894-018-0619-8
66. Chen J, et al. Stool banking for fecal microbiota transplantation: methods and operations at a large stool bank. Front Cell Infect Microbiol. 2021;11:622949.
67. OpenBiome Product Order Form. Available from: https://openbiome.org/wp-content/uploads/Order-Form_August-2023.pdf.
68. Hota SS, Poutanen SM. Microbiome-based therapeutics for Clostridioides difficile infection: helpful solutions or unclear cocktails? Lancet Infect Dis. 2023;23(9):999–1000. doi:10.1016/S1473-3099(23)00484-X
69. Sandhu A, Chopra T. Fecal microbiota transplantation for recurrent Clostridioides difficile, safety, and pitfalls. Therap Adv Gastroenterol. 2021;14:17562848211053105. doi:10.1177/17562848211053105
70. Kassam Z, Lee CH, Yuan Y, et al. Fecal microbiota transplantation for Clostridium difficile infection: systematic review and meta-analysis. Am J Gastroenterol. 2013;108(4):500–508. doi:10.1038/ajg.2013.59
71. Kelly CR, Khoruts A, Staley C, et al. Effect of fecal microbiota transplantation on recurrence in multiply recurrent clostridium difficile infection: a randomized trial. Annals of Internal Medicine. 2016;165(9):609–616. doi:10.7326/M16-0271
72. Hota SS, Sales V, Tomlinson G, et al. Oral vancomycin followed by fecal transplantation versus tapering oral vancomycin treatment for recurrent clostridium difficile infection: an open-label, randomized controlled trial. Clin Infect Dis. 2017;64(3):265–271. doi:10.1093/cid/ciw731
73. Tariq R, Pardi DS, Bartlett MG, et al. Low Cure rates in controlled trials of fecal microbiota transplantation for recurrent clostridium difficile infection: a systematic review and meta-analysis. Clin Infect Dis. 2019;68(8):1351–1358. doi:10.1093/cid/ciy721
74. Song YN. Fecal microbiota transplantation for severe or fulminant clostridioides difficile infection. Systematic Review and Meta-Analysis J Can Assoc. 2022;5(1):e1–e11.
75. Quera R, Espinoza R, Estay C, et al. Bacteremia as an adverse event of fecal microbiota transplantation in a patient with Crohn’s disease and recurrent Clostridium difficile infection. J Crohns Colitis. 2014;8(3):252–253. doi:10.1016/j.crohns.2013.10.002
76. Trubiano JA, Gardiner B, Kwong JC, et al. Faecal microbiota transplantation for severe Clostridium difficile infection in the intensive care unit. Eur J Gastroenterol Hepatol. 2013;25(2):255–257. doi:10.1097/MEG.0b013e32835b2da9
77. Solari PR, Fairchild PG, Noa LJ, et al. Tempered enthusiasm for fecal transplant. Clin Infect Dis. 2014;59(2):319. doi:10.1093/cid/ciu278
78. Baxter M, Ahmad T, Colville A, et al. Fatal aspiration pneumonia as a complication of fecal microbiota transplant. Clin Infect Dis. 2015;61(1):136–137. doi:10.1093/cid/civ247
79. Roberts MJ, Parambi A, Barrett L, et al. Multifocal abscesses due to multiresistant Escherichia coli after transrectal ultrasound-guided prostate biopsy. Med J Aust. 2013;198(5):282–284. doi:10.5694/mja12.11719
80. DeFilipp Z, Bloom PP, Torres Soto M, et al. Drug-resistant E. coli bacteremia transmitted by fecal microbiota transplant. N Engl J Med. 2019;381(21):2043–2050. doi:10.1056/NEJMoa1910437
81. Safety alert regarding use of fecal microbiota for transplantation and additional safety protections pertaining to monkeypox Virus. 2022.
82. Ekekezie C, Perler BK, Wexler A, et al. Understanding the scope of do-it-yourself fecal microbiota transplant. Am J Gastroenterol. 2020;115(4):603–607. doi:10.14309/ajg.0000000000000499
83. Browne HP, Neville BA, Forster SC, et al. Transmission of the gut microbiota: spreading of health. Nat Rev Microbiol. 2017;15(9):531–543. doi:10.1038/nrmicro.2017.50
84. Halaweish HF, Boatman S, Staley C. Encapsulated fecal microbiota transplantation: development, efficacy, and clinical application. Front Cell Infect Microbiol. 2022;12:826114. doi:10.3389/fcimb.2022.826114
85. Khoruts A, Kabaga A. Investigator’s brochure, fecal microbiota; mtp-101-lf. Program UMTEditor;.2022;22.
86. Jiang ZD, Jenq RR, Ajami NJ, et al. Safety and preliminary efficacy of orally administered lyophilized fecal microbiota product compared with frozen product given by enema for recurrent Clostridium difficile infection: a randomized clinical trial. PLoS One. 2018;13(11):e0205064. doi:10.1371/journal.pone.0205064
87. Kao D, Roach B, Silva M, et al. Effect of oral capsule– vs colonoscopy-delivered fecal microbiota transplantation on recurrent clostridium difficile infection. JAMA. 2017;318(20):1985–1993. doi:10.1001/jama.2017.17077
88. Ramai D, Zakhia K, Fields PJ, et al. Fecal Microbiota Transplantation (FMT) with colonoscopy is superior to enema and nasogastric tube while comparable to capsule for the treatment of recurrent clostridioides difficile infection: a systematic review and meta-analysis. Dig Dis Sci. 2021;66(2):369–380. doi:10.1007/s10620-020-06185-7
89. Youngster I, Russell GH, Pindar C, et al. Oral, capsulized, frozen fecal microbiota transplantation for relapsing clostridium difficile Infection. JAMA. 2014;312(17):1772–1778. doi:10.1001/jama.2014.13875
90. McChalicher CW, Auniņš JG. Drugging the microbiome and bacterial live biotherapeutic consortium production. Curr Opin Biotechnol. 2022;78:102801. doi:10.1016/j.copbio.2022.102801
91. McChalicher CWJ, Lombardo M-J, Khanna S, et al. Manufacturing processes of a purified microbiome therapeutic reduce risk of transmission of potential bacterial pathogens in donor stool. J Infect Dis. 2023;228(10):1452–1455. doi:10.1093/infdis/jiad298
92. Qiu K, Anselmo AC. Batch culture formulation of live biotherapeutic products. Adv Ther. 2021;4(2). doi:10.1002/adtp.202000226
93. Kao D, Wong K, Franz R, et al. The effect of a microbial ecosystem therapeutic (MET-2) on recurrent Clostridioides difficile infection: a phase 1, open-label, single-group trial. Lancet Gastroenterol Hepatol. 2021;6(4):282–291. doi:10.1016/S2468-1253(21)00007-8
94. Khanna S. S131 CP101, an investigational orally administered microbiome therapeutic, increases intestinal microbiome diversity and prevents recurrent c. difficile infection: results from a randomized, placebo-controlled trial. Am J Gastroenterol. 2021;116:S57.
95. Argemi X, Prévost G, Riegel P, et al. VISLISI trial, a prospective clinical study allowing identification of a new metalloprotease and putative virulence factor from Staphylococcus lugdunensis. Clin Microbiol Infect. 2017;23(5):
96. Seres Therapeutics and Nestlé Health Science Announce FDA Approval of VOWST™ (fecal microbiota spores, live-brpk) for Prevention of Recurrence of C. difficile infection in adults following antibacterial treatment for recurrent CDI; Available from: https://ir.serestherapeutics.com/news-releases/news-release-details/seres-therapeutics-and-nestle-health-science-announce-fda.
97. Assimacopoulos A, Johnston B, Clabots C, et al. Post-prostate biopsy infection with Escherichia coli ST131 leading to epididymo-orchitis and meningitis caused by Gram-negative bacilli. J Clin Microbiol. 2012;50(12):4157–4159. doi:10.1128/JCM.02026-12
98. Fantoni M, Rossi TE, Rossi B, et al. Epidemiological and clinical features of pyogenic spondylodiscitis.. Eur Rev Med Pharmacol Sci. 2012;16:2–7.
99. Jr A,Late breaking abstract: an investigational oral microbiome drug, cp101, for the prevention of recurrent clostridioides difficile infection: a randomized, placebo-controlled, multi-center trial (prism3). Uni Eur Gastro J, 2021. 8(10): p. 1270–1271
100. Hamilton MJ, Sadowski KA, Staley MJ; Compositions and methods for C. difficile Treatment. Regent of the University of Minnesota; Available fromhttps://image-ppubs.uspto.gov/dirsearch-public/print/downloadPdf/10849936.
101. News release: finch therapeutics announces decision to discontinue phase 3 trial of cp101 and focus on realizing the value of its intellectual property estate and other assets. 2023.
102. Blaser MJ. Fecal microbiota transplantation for dysbiosis - predictable risks. N Engl J Med. 2019;381(21):2064–2066. doi:10.1056/NEJMe1913807
103. Dsouza M, Menon R, Crossette E, et al. Colonization of the live biotherapeutic product VE303 and modulation of the microbiota and metabolites in healthy volunteers. Cell Host Microbe. 2022;30(4):583–598.e8. doi:10.1016/j.chom.2022.03.016
104. Louie T, Golan Y, Khanna S, et al. VE303, a defined bacterial consortium, for prevention of recurrent clostridioides difficile infection. JAMA. 2023;329(16):1356–1366. doi:10.1001/jama.2023.4314
105. Villano SA, Seiberling M, Tatarowicz W, et al. Evaluation of an oral suspension of VP20621, spores of nontoxigenic Clostridium difficile strain M3, in healthy subjects. Antimicrob Agents Chem. 2012;56(10):5224–5229. doi:10.1128/AAC.00913-12
106. Gerding DN, Meyer T, Lee C, et al. Administration of spores of nontoxigenic clostridium difficile strain m3 for prevention of recurrent c difficile infection. JAMA. 2015;313(17):1719–1727. doi:10.1001/jama.2015.3725
107. Brouwer MS. Horizontal gene transfer converts non-toxigenic Clostridium difficile strains into toxin producers. Nat Commun, 2013. 4: p. 2601.
108. Sambol SP, Johnson S, Cheknis A, et al. Absence of toxin gene transfer from Clostridioides difficile strain 630Δerm to nontoxigenic C. difficile strain NTCD-M3r in filter mating experiments. PLoS One. 2022;17(6):e0270119. doi:10.1371/journal.pone.0270119
109. Takeda enters into strategic collaboration with nubiyota for microbiome therapeutics. 2017.
110. NuBiyota MET Pipeline 2021 Available from: https://nubiyota.com/pipeline/.
111. Petrof EO, Gloor GB, Vanner SJ, et al. Stool substitute transplant therapy for the eradication of clostridium difficile infection: ‘RePOOPulating’ the gut. Microbiome. 2013;1(1):3. doi:10.1186/2049-2618-1-3
112. Morningside ventures launches adiso therapeutics to advance novel therapies for inflammatory diseases. 2022.
113. Therapeutics A Portfolio of single strain live biotherapeutic products (SS-LBP) 2023.Available from: https://adisotx.com/science-and-pipeline/#pipeline.
114. Alshrari AS, Hudu SA, Elmigdadi F, et al. The urgent threat of clostridioides difficile infection: a glimpse of the drugs of the future, with related patents and prospects. Biomedicines. 2023;11(2):426. doi:10.3390/biomedicines11020426
115. Farquhar RC, Hill L, Ross C, et al. Edible Products Comprising BacterialStrains and Methods of Use. P. Patent, Editor; 2021.
116. Farquhar RM, Hill CK, Ross C, Rea P, O’Donnell M. Methods and Compositions for the Treatment of C. Difficile. U.S. Patent, Editor; 2022.
117. Fromm M. DIFPROTEC - Trademark Details. Denmark; 2021.
118. Khanna S, Sims M, Louie TJ, et al. SER-109: an oral investigational microbiome therapeutic for patients with recurrent clostridioides difficile infection (rCDI). Antibiotics. 2022;11(9):doi:10.3390/antibiotics11091234
119. Jr A, Louie KC, Fisher T, et al. Late breaking abstract: an investigational oral microbiome drug, CP101, for the prevention of recurrent clostridioides difficile infection: a randomized, placebo-controlled, multi-center trial (PRISM3). Uni Eur Gastro J. 2021;8(10):1270–1271.
120. Pharma D NTCD-M3 Phase 3 Design – Agreed with FDA and EMA, Partnership with Sebela Pharmaceuticals. 2023 Available from: https://www.destinypharma.com/pipeline/ntcd-m3/.
121. Ford C, Litcofsky K, McGovern B, et al. Engraftment of Investigational microbiome drug, SER-262, in subjects receiving vancomycin is associated with reduced rates of recurrence after primary clostridium difficile infection (CDI). Open Forum Infect Diseases. 2019;6(Supplement_2):S547–S548. doi:10.1093/ofid/ofz360.1367
122. BiomeBank Submits for Market Authorisation of World First Microbial Therapy. 2021 Available from: https://www.biomebank.com/news/media-release/market-authorisation-of-world-first-microbial-therapy/.
123. Orenstein R, Dubberke E, Hardi R, et al. Safety and durability of RBX2660 (microbiota suspension) for recurrent clostridium difficile infection: results of the punch cd study. Clin Infect Dis. 2016;62(5):596–602. doi:10.1093/cid/civ938
124. Orenstein R, Dubberke ER, Khanna S, et al. Durable reduction of Clostridioides difficile infection recurrence and microbiome restoration after treatment with RBX2660: results from an open-label phase 2 clinical trial. BMC Infect Dis. 2022;22(1):245. doi:10.1186/s12879-022-07256-y
125. Orenstein R. The role of microbiome-based therapeutics in clostridioides difficile infection: durable, long-term results of RBX2660. Infect Dis Ther. 2023;12(1):1–7. doi:10.1007/s40121-022-00714-9
126. Dubberke ER, Orenstein R, Khanna S, et al. final results from a phase 2b randomized, placebo-controlled clinical Trial of RBX2660: a microbiota-based drug for the prevention of recurrent clostridioides difficile infection. Infect Dis Ther. 2023;12(2):703–709. doi:10.1007/s40121-022-00744-3
127. Lee C, Louie T, Bancke L, et al. Safety of fecal microbiota, live-jslm (REBYOTA™) in individuals with recurrent Clostridioides difficile infection: data from five prospective clinical trials. Therap Adv Gastroenterol. 2023;16:17562848231174277. doi:10.1177/17562848231174277
128. Garey KW, Dubberke ER, Guo A, et al. Effect of fecal microbiota, live-jslm (REBYOTA [RBL]) on health-related quality of life in patients with recurrent clostridioides difficile infection: results from the punch cd3 clinical trial. Open Forum Infect Dis. 2023;10(8):383. doi:10.1093/ofid/ofad383
129. Koo HL, Van JN, Zhao M, et al.Real-time polymerase chain reaction detection of asymptomatic clostridium difficile colonization and rising c. difficile –associated disease rates. Infect Control Hosp Epidemiol. 2014;35(6):667–673.doi:10.1086/676433
130. Feuerstadt P, Bancke HA. Abstract P2217: RBX2660, an investigational live microbiota-based biotherapeutic, improves outcomes of Clostridioides difficile infection in a real-world population: a retrospective study of use under enforcement discretion. In:American College of Gastroenterology (ACG 2021) Annual Meeting. 2021. Las Vegas, NV;2024.
131. Khanna S, Pardi DS, Kelly CR, et al. A novel microbiome therapeutic increases gut microbial diversity and prevents recurrent clostridium difficile infection. J Infect Dis. 2016;214(2):173–181. doi:10.1093/infdis/jiv766
132. Sims MD, Khanna S, Feuerstadt P, et al. Safety and tolerability of SER-109 as an investigational microbiome therapeutic in adults with recurrent clostridioides difficile infection. JAMA Network Open. 2023;6(2):e2255758–e2255758. doi:10.1001/jamanetworkopen.2022.55758
133. Cohen SH, Louie TJ, Sims M, et al. Extended follow-up of microbiome therapeutic SER-109 through 24 weeks for recurrent clostridioides difficile infection in a randomized clinical trial. JAMA. 2022;328(20):2062–2064. doi:10.1001/jama.2022.16476
134. Therapeutics S Expanded Access Program. Available from: https://www.serestherapeutics.com/patients-and-physicians/Expanded_Access.pdf.
135. Feuerstadt P. Patient perception of route of rectal administration of live biotherapeutic product for recurrent clostridioides difficile infection. Patient Prefer Adherence, 2023. 17:2153–2159.
136. Jain N, Umar TP, Fahner A-F, et al. Advancing therapeutics for recurrent clostridioides difficile infections: an overview of vowst’s FDA approval and implications. Gut Microbes. 2023;15(1):2232137. doi:10.1080/19490976.2023.2232137
137. Lodise T, Guo A, Yang M, et al. Budget impact analysis of REBYOTA™ (fecal microbiota, live-jslm [fmbl]) for preventing recurrent clostridioides difficile infection in the US. Adv Ther. 2023;40(6):2801–2819. doi:10.1007/s12325-023-02506-0
138. Bainum TB, Reveles KR, Hall RG, et al. Controversies in the prevention and treatment of clostridioides difficile infection in adults: a narrative review. Microorganisms. 2023;11(2):387. doi:10.3390/microorganisms11020387
139. Mohamed MFH. Efficacy, safety, and cost-effectiveness of bezlotoxumab in preventing recurrent clostridioides difficile infection. J Clin Gastro. 2023;2023:1.
140. Vazquez Roque M. RBX7455 Before Surgery for the Treatment of Operable Breast Cancer. Mayo Clinic; 2023.
141. Bloom P. VE303 for Treatment of Hepatic Encephalopathy (HE); 2021.
142. Garfield M. VE202 in Patients with Mild-to-Moderate Ulcerative Colitis. Clinicaltrials.gov; 2023.
143. Tejura B. A Multiple Dose Study to Evaluate Safety, Tolerability, PK, and Efficacy of SER-155 in Adults Undergoing HSCT. clinicaltrials.gov;2021.
144. Horvath A, Zukauskaite K, Hazia O, et al. Human gut microbiome: therapeutic opportunities for metabolic syndrome-Hype or hope? Endocrinol Diabetes Metab. 2023;7(1):e436. doi:10.1002/edm2.436
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.