Back to Journals » Infection and Drug Resistance » Volume 16
Microbiologic Cure with a Simplified Dosage of Intravenous Colistin in Adults: A Retrospective Cohort Study
Authors Al-Zubairy SA ![]()
Received 6 March 2023
Accepted for publication 10 June 2023
Published 29 June 2023 Volume 2023:16 Pages 4237—4249
DOI https://doi.org/10.2147/IDR.S411381
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Sulaiman A Al-Zubairy
Clinical Pharmacy Services, Johns Hopkins Aramco Healthcare, Dhahran, Saudi
Correspondence: Sulaiman A Al-Zubairy, Johns Hopkins Aramco Healthcare, 6th St, Dhahran, 34465, Saudi, Tel +966 138706287, Email [email protected]
Purpose: Colistin’s FDA weight-based dosing (WBD) and frequency are both expressed in a broad range. Therefore, a simplified fixed-dose regimen (SFDR) of intravenous colistin based on three body-weight segments has been established for adults. The SFDR falls within the WBD range of each body-weight segment and accounts for the pharmacokinetic features. This study compared microbiologic cure with colistin SFDR to WBD in critically ill adults.
Patients and Methods: A retrospective cohort study was conducted for colistin orders from January 2014 to February 2022. The study included ICU patients who received intravenous colistin for carbapenem-non-susceptible, colistin-intermediate Gram-negative bacilli infections. Patients received the SFDR after the protocol was implemented, as the WBD was previously used. The primary endpoint was microbiologic cure. Secondary endpoints were 30-day infection recurrence and acute kidney injury (AKI).
Results: Of the 228 screened patients, 84 fulfilled the inclusion and matching criteria (42 in each group). The microbiologic cure rate was 69% with the SFDR and 36% with the WBD [p=0.002]. Infection recurred in four of the 29 patients who had a microbiologic cure with the SFDR (14%), and in six of the 15 patients with WBD (40%); [p=0.049]. AKI occurred in seven of the 36 SFDR patients who were not on hemodialysis (19%) and 15 of the 33 WBD patients (46%); [p=0.021].
Conclusion: In this study, colistin SFDR was associated with a higher microbiologic cure in carbapenem-non-susceptible, colistin-intermediate Gram-negative bacilli infections and with a lower incidence of AKI in critically ill adults compared to WBD.
Keywords: Acinetobacter, multidrug resistance, ESBL, carbapenem, polymyxin, FDA dosing
Plain Language Summary
The FDA recommends a wide range for how much per weight and how often to give the intravenous antibiotic colistin. To make dosing easier, a simplified dosing plan was made with fixed doses based on three body weight groups. The simplified dosing is within the range set by the FDA for each body weight group and takes into account how the medicine works in the body. This study compared the FDA’s and simplified colistin dosing for adult ICU patients.
Colistin prescriptions were reviewed from January 2014 to February 2022. The study looked at adult ICU patients with Gram-negative bacterial infections that were resistant to antibiotics called carbapenems but could be treated with colistin. The goals of the study were to see how well the antibiotic regimens got rid of bacteria, stopped infections from coming back within 30 days, and caused less acute kidney injury.
Only 84 of the 228 patients checked out were eligible for the study (42 in each group). The FDA dose killed 36% of bacteria, but the simplified dosing method killed 69%. Infection returned 40% of the time with the FDA dose, but only 14% with the simpler dose. The FDA dose caused 59% more acute kidney injury than the simplified dose.
At the end of this study, the simplified dose of colistin was more likely than the FDA dose to treat Gram-negative bacterial infections in ICU patients that were resistant to carbapenem antibiotics. The simpler dose seemed to cause less kidney injury than the FDA dose.
Introduction
Carbapenem resistance (CR) has brought the world closer to the challenge of extreme drug resistance to Gram-negative bacilli (GNB). The prevalence of CR in Acinetobacter baumannii isolates was 21% in Africa, the Eastern Mediterranean, and Europe,1 and up to 91% in some Asia-Pacific countries.2 Antibiograms from 15 Saudi hospitals between 2016 and 2022, with a total of 160,276 GNB isolates, were reviewed. The proportion of A. baumannii isolates not susceptible to at least one antipseudomonal carbapenem was 63%, Pseudomonas aeruginosa 31%, Klebsiella pneumoniae 19%, and Escherichia coli 1.9%.3 Colistin, in combination with meropenem, is one of the limited antibiotic treatment options for CR-GNB infection. Colistin works by altering the permeability of the bacterial outer membrane, allowing higher concentrations of meropenem to enter the cell to produce a synergistic effect against resistant bacteria (Figure 1).4,5 Between 2013 and 2017, carbapenem use in the UK remained stable, while colistin use increased.6
 |
Figure 1 Colistin-meropenem combination mechanism of action. The cationic colistin binds to anionic lipopolysaccharide molecules by displacing calcium and magnesium from the outer membrane of Gram-negative bacilli, resulting in altered permeability of the bacteria’s membrane. Abbreviation: PBP, penicillin binding protein. Note: Adapted from Journal of Infection, 69/1, Martis N, Leroy S, Blanc V, Colistin in multi-drug resistant Pseudomonas aeruginosa blood-stream infections: a narrative review for the clinician, 1-12, Copyright 2014, with permission from Elsevier.5 |
Colistin was introduced to the market in the 1950s and, as such, has not been subjected to the requirements of modern drug approvals, particularly with regard to dosing.7 The US FDA intravenous (IV) dosage is weight-based in a range of 75,000 to 150,000 international units (IU)/kg/day in two to four divided doses.8 Guideline IV dosage recommends a loading dose (LD) of 9 million IU (MIU) followed by a maintenance dose (MD) ranging from 4.5 to 5.4 MIU q12h.9 The European Medicines Agency (EMA) recommends 9 MIU daily, divided into two to three doses, with a 9 MIU LD for critically ill patients.10 While guideline and EMA dosing might have addressed the issue of variability found in the FDA dosing range,8–10 the administration of an LD and the time interval between doses remain contentious. In clinical studies, dosing colistin q8h resulted in a two-log bacterial kill effect,11 maintained therapeutic colistin levels,12 and reduced the emergence of resistance,13 when compared to the same daily dose given q12h or q24h. The aim of giving an LD, on the other hand, was to accelerate the achievement of therapeutic colistin concentrations and thus fight the infection faster. In a pharmacokinetics study of 19 patients, an LD of 9 MIU followed by an MD of 4.5 MIU q12h beginning 24 hours after the LD achieved a therapeutic colistin concentration of >2 mg/L within 8 hours.14 Nevertheless, the rate of acute kidney injury (AKI) in the study was 20%, although precautions were taken by excluding patients on renal replacement therapy (RRT) and reducing the LD to 4–6 MIU in patients with a creatinine clearance (CrCl) of 29–48 mL/min.14 Another pharmacokinetic study of 18 patients with normal renal function found that it took >36 hours to achieve therapeutic concentrations with colistin 3 MIU q8h.15 The bactericidal activity of colistin is concentration-dependent,9,12,13,16 as is its nephrotoxicity.12,17 This highlights the significance of appropriate dosing to keep plasma levels within a therapeutic window. In a randomized clinical trial of 40 patients, the AKI incidence with the guideline dosage was 60% compared to 15% with 2 MIU q8h.17 Regardless of kidney function, blood samples from patients who received an LD showed supratherapeutic colistin levels, but not when the LD was divided across two or more doses.12 Given that the recommended time interval between the LD and the MD is at least 12 hours,9,14 splitting the dose could be equivalent to beginning with an adequate q8h MD. In terms of efficacy, a study of 163 patients found no clinical benefit from adding an LD.18 As a result, the question remains: Does achieving faster therapeutic drug concentrations with colistin LD justify the increased risk of AKI if it does not necessarily translate into clinical benefit?
Another challenge with colistin dosing is that it can be expressed as colistin base activity (CBA) or colistimethate sodium, either in IU or milligrams. One milligram of colistimethate sodium is equivalent to 12,500 IU or 0.4 milligrams of CBA. In May 2017, a simplified fixed-dose regimen (SFDR) of IV colistimethate sodium was implemented for adults, dividing the daily dose into three doses every 8 hours for patients with preserved kidney function. As shown in Table 1, doses are allocated into three patient weight segments: <60 kg, 60–90 kg, and >90 kg, which all fall within the FDA weight-based dosing (WBD) range for each weight segment. The SFDR considers the colistin vial size and the patient’s renal function. The purpose of this study was to evaluate the microbiologic cure in carbapenem-non-susceptible, colistin-intermediate GNB infections with colistin SFDR compared to the FDA WBD in critically ill adult patients.
 |
Table 1 The Simplified Fixed-Dose Regimen of IV Colistimethate Sodium in Adults |
Materials and Methods
Patients
A retrospective cohort study was conducted on all ICU patients who received IV colistin for carbapenem-non-susceptible, colistin-intermediate GNB infections at Johns Hopkins Aramco Healthcare (JHAH), Dhahran, Saudi Arabia, between January 2014 and February 2022. The study compared patients who received IV colistin SFDR to those who received WBD. Patients received the SFDR after the protocol was implemented, as the WBD was previously used. Patients were excluded from the study if they received colistin for less than seven days, or colistin LD; did not receive a concomitant antipseudomonal carbapenem nor had a repeat culture after colistin use; were pregnant or younger than 14 years old; or were deemed to have contamination rather than infection by an infectious-disease specialist. Patients who received GNB coverage in addition to the colistin-antipseudomonal carbapenem combination were also excluded. The institutional age for pediatric inpatient admissions is <14 years. Propensity score matching (PSM) was used to match patients in the two groups based on baseline pre-existing conditions, initial lab data, SOFA score, and concurrent use of inhaled colistin. Only matched patients found within the caliper radius of 0.10*sigma were included in the study to account for baseline differences. The primary endpoint was microbiologic cure, which was defined as the absence of treated bacteria in the first repeat culture of the original site of infection within seven to 14 days of starting antibiotic treatment.19,20 Infection recurrence and AKI were secondary endpoints. The infection recurrence rate was determined by the presence of the same bacteria at the original site of infection within 30 days after the culture was negative after antibiotic therapy. The Kidney Disease Improving Global Outcomes (KDIGO) 2012 criteria were used to diagnose AKI: an increase in serum creatinine (SrCr) of 0.3 mg/dL or more within 48 hours or to 1.5 times baseline or more within the previous seven days, or urine output of less than 0.5 mL/kg/h for 6 hours or more.21 The Cockcroft-Gault formula was used to calculate CrCl from SrCr, age, body weight, and gender.22 The CrCl value was capped at 125 mL/minute, and the weight used for calculation was the actual body weight (ABW) in underweight patients, the ideal body weight (IBW) in normal weight patients, and 0.4 adjusted body weight in overweight patients.23 All susceptibility tests adhere to the most recent Clinical and Laboratory Standards Institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. The minimum inhibitory concentration (MIC) breakpoints are updated in tandem with the CLSI. Non-susceptible isolates for imipenem and meropenem are either resistant or intermediate, with MICs >1 µg/mL for Enterobacterales and >2 µg/mL for A. baumannii and P. aeruginosa.24,25 The current MIC breakpoint for colistin is <2 µg/mL, which is considered intermediate, but allows colistin to be used.26 The SOFA score was used to assess organ function at the start of therapy. The score is based on different ratings, one each for respiratory, renal, cardiovascular, coagulation, hepatic, and neurological systems, as well as the use of vasopressors.27 The required sample size for the primary endpoint was 26 patients in each arm, based on Parchem et al 87% microbiologic cure rate,28 80% power, 0.05 alpha level, and a 1:1 enrollment ratio.29
Antibiotic Therapy
The SFDR is shown in Table 1. Colistin vial size is 1 MIU manufactured by Hikma Italia©, Italy, for Jazeera Pharma©, Saudi. WBD was 75,000 to 150,000 IU/kg/day in two to four divided doses if CrCl was >80 mL/min, 75,000 to 114,000 IU/kg/day in two divided doses if CrCl was 50 to 79, 75,000 IU/kg once daily or in two divided doses if CrCl was 30 to 49, and 45,000 IU/kg q36h if CrCl was 10 to 29.8 WBD used ABW unless the BMI was >30, in which case IBW was used.8 On the other hand, the concomitant antipseudomonal carbapenems were either imipenem or meropenem, dosed according to the institution’s renal dosing protocol. The imipenem dose was 500 mg q6h, 500 mg q8h, 250 mg q8h, or 250 mg q12h for CrCl >60, 30–59, 15–29, or <15 mL/min, respectively. The dose in patients on continuous RRT (CRRT) was 500 mg q8h, and in patients on peritoneal dialysis (PD) or hemodialysis, 250 q12h, with one dose scheduled post-hemodialysis on hemodialysis days. The meropenem dose was 1000 mg q8h, 1000 mg q12h, 500 mg q12h, or 500 mg q24h for CrCl >50, 26–50, 10–25, or <10 mL/min, respectively. The dose in patients on CRRT was 1000 mg q12h, and in patients on PD or hemodialysis, 500 mg q24h; post-hemodialysis was scheduled on hemodialysis days. All dosing regimens are approved by the JHAH Drug and Therapeutics Committee.
Statistical Analysis
The Chi-squared test was used to compare nominal data, presented as frequencies (percentages). The t-test was used to compare continuous, normally distributed means presented with a standard deviation (SD). The Mann–Whitney U-test was used for nonparametric frequencies, presented as medians (Q1, Q3). The Kolmogorov–Smirnov test determined distribution normality. A two-sided p value of 0.05 was used to define statistical significance. PSM was performed using Addinsoft’s XLSTAT statistical software. Regression analysis was used to assess the effect of baseline characteristics on microbiologic failure; not achieving microbiologic cure. IBM SPSS Statistics software version 26 was used for statistical test comparisons and regression analyses. Patients who were on RRT at baseline were excluded from the AKI analysis.
Results
Patients
Only 134 of the 228 patients screened met the inclusion criteria (92 received colistin’s WBD and 42 received the SFDR). As part of the PSM, 42 (46%) of the eligible WBD patients were matched with the same number of eligible SFDR patients. The study ultimately compared 42 matched eligible WBD patients to 42 SFDR recipients (Figure 2). The key baseline characteristics of patients in the study comparison are shown in Table 2. The MICs of all isolates in the study were >16 µg/mL for imipenem or meropenem and <2 µg/mL for colistin. Figure 3 depicts a multiple logistic regression model for microbiologic failure based on baseline characteristics.
 |
Table 2 Baseline Characteristics |
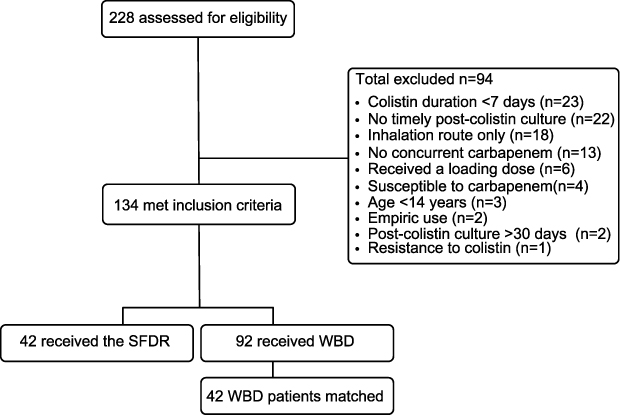 |
Figure 2 Patient allocation. Abbreviations: SFDR, simplified fixed-dose regimen; WBD, weight-based dosing. |
 |
Figure 3 Forest plot for multiple logistic regression of baseline patient characteristics with microbiologic failure. Abbreviations: BMI, body mass index; CI, confidence interval; DM, diabetes mellitus; Hgb, hemoglobin; IHD; ischemic heart disease; OR, odds ratio; SOFA, Sequential Organ Failure Assessment; SrCr, serum creatinine; WBC, white blood cells. |
Treatment
Table 3 summarizes the colistin antibiotic therapy that was prescribed to the studied patients. The WBD was lower than the SFDR-equivalent total daily dose for body weight and CrCl in 26 patients (62%), and higher in 16 (38%). All SFDR orders were carried out after protocol implementation, while 23 of 42 (55%) WBD orders were carried out prior to protocol implementation. After the protocol, 19 eligible patients received the WBD. The study site switched to EUCAST-CLSI-compliant broth microdilution (BMD) for colistin susceptibility testing on February 15, 2018.30 Previously, both the VITEK-2® automated susceptibility testing platform and the gradient MIC strip (Etest®) were used. Thus, 33 patients in the SFDR group used BMD susceptibility testing, while only 19 did so in the WBD group.
 |
Table 3 Colistin Antibiotic Therapy Prescribed to the Studied Patients |
Study Endpoints
Table 4 displays the results of the study’s primary and secondary endpoints. The microbiologic cure rate with the SFDR was 69% and 36% with the WBD [p=0.002]. Infection recurred in four of the 29 patients who had a microbiologic cure with the SFDR (14%), and in six of the 15 patients who received WBD (40%) [p=0.049]. The SFDR group’s median (Q1, Q3) time to post-antibiotic culture was 11 (7, 14) days, while the WBD group’s was 12.5 (8, 14) days [p=0.271]. AKI occurred in seven of the 36 SFDR patients who were not on hemodialysis (19%) and 15 of the 33 WBD patients (46%); [p=0.021]. In the SFDR arm, infection recurrence occurred six to 12 days after post-antibiotic culture and eight to 21 days in the WBD arm. The 30-day all-cause mortality rate with the SFDR was 17% (7 patients) and 12% (5 patients) with the WBD [p=0.533]. Microbiologic cure rates for lower respiratory infection (LRTI) were 59% in SFDR patients (13/22) and 21% in WBD patients (6/28); [p=0.007]. The overall microbiologic cure rate for the study participants was 52%, with a 14% 30-day mortality rate. The logistic regression OR (95% CI) for microbiologic failure with the administered single colistin dose and daily dose was 0.46 (0.24, 0.88) and 0.76 (0.62, 0.93), respectively. For total dose per course and dosing frequency, the OR (95% CI) with microbiologic failure was 1 (0.98, 1.01) and 0.89 (0.47, 1.69), respectively. The logistic regression OR (95% CI) for AKI with the administered single colistin dose and daily dose was 0.52 (0.25, 1.06) and 0.82 (0.65, 1.03), respectively. For total dose per course and dosing frequency, the OR (95% CI) with AKI was 1 (0.99, 1.02) and 0.86 (0.38, 1.94), respectively. The logistic regression OR (95% CI) for microbiologic failure and AKI with the use of the SFDR as opposed to WBD was 0.25 (0.10, 0.62) and 0.36 (0.13, 0.97), respectively.
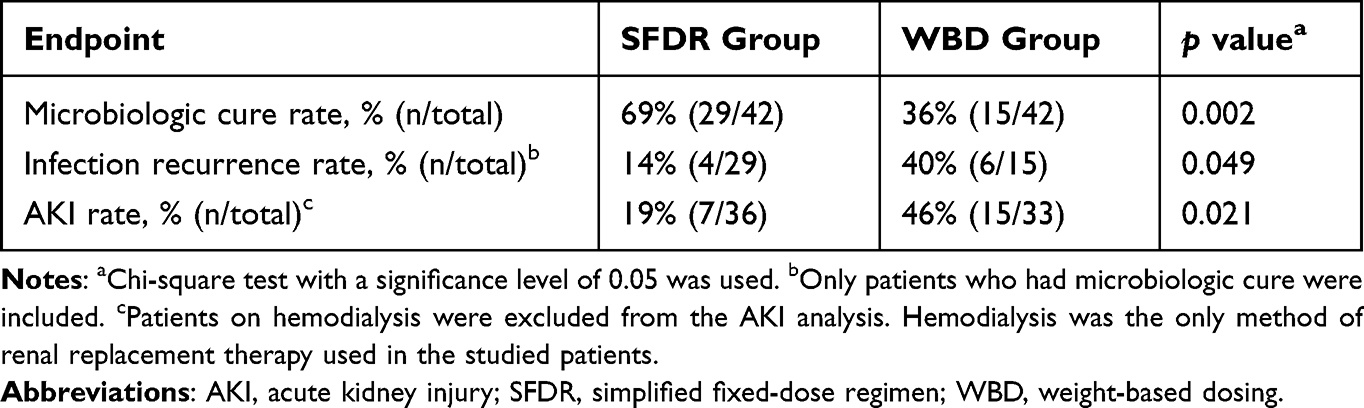 |
Table 4 Endpoints Outcomes of the Study |
Discussion
Research findings suggest that colistin SFDR is associated with better outcomes in ICU patients with carbapenem-non-susceptible, colistin-intermediate GNB infections. Despite having a higher equivalent mean total daily dose, patients receiving the SFDR had a significantly lower AKI rate. These findings may be related to the greater variability of individual colistin doses in WBD. The WBD has a wide range, and either the lower or upper end of the dosage range might have been used. The interquartile range for single doses of colistin in WBD was three times that of SFDR. WBD patients received single doses of 5, 4.5, and 3.5 MIU, while SFDR patients received single doses of 3 MIU or less. Nevertheless, most WBD patients received their doses every 12 hours, whereas SFDR patients often received them every 8 hours. Colistin doses at the lower end of the WBD range are likely insufficient, particularly in LRTI.31,32 In this study, inadequate colistin doses were linked to treatment failure, as previously found in other studies,7,32 and, surprisingly, higher AKI rates. Severe infection is a leading cause of AKI in ICU patients, with septic AKI patients faring worse than non-septic AKI patients.33 In this regard, inappropriate antibiotic doses were associated with ICU sepsis and mortality.34 It is worth noting that in studies, AKI has been linked to colistin LD rather than adequate divided MD.12,17 After all, the treatment regimen (WBD vs SFDR) was the strongest predictor of microbiologic failure and nephrotoxicity in this study.
The study’s primary endpoint was microbiologic cure due to its objectivity. Clinical cure lacks a consensual definition and is highly subjective, particularly in critically ill patients, where symptoms may be related to concomitant events or diseases.35 However, a microbiologic cure requires a post-antibiotic culture of the initial site of infection. Insufficient timely post-antibiotic cultures led to the exclusion of 10% of the study’s evaluated patients. The study required at least seven days of antibiotic therapy because the average published duration for colistin therapy in CR-GNB infection was seven to 14 days,19,20 which was the time frame for post-antibiotic culture in this study. The post-antibiotic culture collection time frame was shortened to improve patient matching. All included patients had only one post-antibiotic culture within the time frame, except for one patient in the WBD group who had two cultures collected at seven and 14 days, and both showed no clearance of GNB. On the other hand, mortality as an endpoint requires a large sample size and is only partially related to the infectious process as opposed to concurrent conditions. One limitation of the study was insufficient power to detect a difference in mortality. Another limitation was that the sample size required to detect infection recurrence in WBD arms was not met because infection recurrence is only measured in patients who have had a microbiologic cure. As a result, the study’s conclusion makes no mention of infection recurrence.
Because the study was conducted retrospectively, PSM and logistic regression were utilized to account for group differences. The odds of microbiologic failure with baseline characteristics were similar, except for pulmonary disease. Nonetheless, underlying pulmonary disease was more prevalent in the SFRD patients, who ultimately had better outcomes. Despite the fact that SFDR patients had more lung disease than WBD patients, the LRTI was lower and the UTI was higher. Colistin is most commonly used for LRTI,36,37 but due to its pharmacokinetics, it is more effective for UTI,38 particularly at low doses.31,32 With multiple IV doses, colistin concentrations in plasma and the LRT epithelial lining fluid were similar in a study involving ICU patients.39 Previous studies claiming that colistin was ineffective in LRTI were most likely due to insufficient dosing,31,32 as its efficacy in this study was nearly 60% when administered via the SFDR. In this study, nearly a third of the LRTI patients in each group were also given inhaled colistin, but a meta-analysis found that this did not reduce mortality unless a low IV dose was co-administered.31 The Infectious Diseases Society of America (IDSA) 2023 guidelines do not recommend the use of nebulized antibiotics in CR-GNB infections.38 A significantly greater proportion of cancer patients in the SFDR arm is likely related to the fact that pharmacists caring for oncology patients pursued optimization of colistin orders according to the institution’s SFDR more than pharmacists serving other patient populations. Neoplastic disease and neutropenia are associated with an increased risk of serious infections that can be challenging to cure.32 Interestingly, despite having more cancer patients with lower blood counts in the SFDR arm, the microbiologic cure rate was higher. The SFDR was applied to all colistin orders, regardless of the level of care. Nevertheless, only ICU patients were included in the study in order to compare groups with similar demographics and because it is the most studied population. The study site has three adult ICUs: surgical, medical, and cardiovascular, as well as an infection control program.
The combination of colistin and carbapenem is aimed at increasing treatment success rates (Figure 1). However, high-quality evidence supports colistin monotherapy.40,41 As a result, some patients received only colistin and were thus excluded from the study to avoid confounding effects. The IDSA 2023 guidelines recommend antibiotic combinations for CR A. baumannii but not for Enterobacterales or P. aeruginosa.38 This study had a lower microbiologic cure rate (52% vs 87%) but a lower 30-day mortality (14% vs 48%) than other colistin-meropenem studies for CR-GNB in ICU patients.1,28 All SFDR orders were carried out after the implementation of the protocol, and most WBD orders were prior to implementation. Meropenem replaced imipenem in the drug formulary after the implementation of the SFDR. Hence, meropenem was used more with the SFDR and imipenem with the WBD. After March 2020, two patients from each group were enrolled and tested for CoVID-19 infection, with one in the SFDR group testing positive.
The majority of those who were excluded from the study had used colistin for less than seven days. This is because these patients were most likely switched to ceftazidime-avibactam or had their treatment discontinued due to a positive culture interpreted as contamination by an infectious-disease physician. Ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam, and cefiderocol are safer alternatives to colistin for CR Enterobacterales (CRE), with lower incidences of AKI. However, other β-lactam antibiotics might select resistance to the novel extended-spectrum β-lactams,42 which may explain the recent rise in resistance.43 Thus, colistin, as a different molecule, is still a viable option for treating CR-GNB infections, especially those caused by A. baumannii or in situations where carbapenemase testing is not readily available. Polymyxins, of which polymyxin B and colistin (polymyxin E) are clinically used examples, are a distinct class of antibiotics. During the last 15 years, there have been reports of colistin resistance (ColR) outbreaks with K. pneumoniae in various parts of the world.44–48 ColR has been linked to 26% of ICU mortality;45 however, it is avoidable with an adequate dose.12,13 In a randomized clinical trial, carbapenem-colistin combination therapy did not reduce ColR emergence compared to monotherapy in CR-GNB.49 While research for newer antibiotics continues, repurposing existing drugs or experimenting with different colistin combinations are options in areas where newer, more expensive antibiotics are unavailable. In clinical isolates, the combination of colistin and vancomycin, aztreonam, ceftazidime, or imipenem showed strong synergy against ColR A. baumannii.50 Despite encouraging in vitro results, the clinical utility of synergistic colistin combinations is still being debated.
During the study, the colistin susceptibility method was modified from VITEK-2® plus Etest® to BMD, which is considered to be more accurate, in accordance with EUCAST-CLSI revisions.30 As a result, colistin susceptibility testing was different between the two groups. Despite this, the rate of essential agreement of colistin test results between BMD and VITEK-2 alone was 93.4%,30 and the only colistin-resistant isolate in the study was detected by using the older method. Only one (0.5%) of the 222 ICU patients with CR-GNB in this study had ColR; A. baumannii. ColR was found to be 15% in CRE isolates and 7% in A. baumannii in other studies.51,52 During the course of the study, CLSI reclassified a colistin MIC of <2 µg/mL from susceptible to intermediate,26 while the MIC breakpoints for imipenem and meropenem remained unchanged.24,25 The CLSI permits the use of colistin with an MIC of <2 µg/mL but recommends using it in combination with other active antimicrobial agents whenever possible and at the maximum renally adjusted doses.24 It is noteworthy that the MIC for colistin in this study was <2 µg/mL in all samples and did not differ significantly between groups. While colistin MICs were found to be low at the study site, meropenem MICs among CR-GNB isolates were at least twice the resistance breakpoint value.24,25 Plasma concentrations determine efficacy in the same way that colistin MIC does.12 Because the MIC must be at most 2 µg/mL, the steady-state serum concentration must be at least 2 mg/L, especially in LRTIs.9,12 Colistin has a narrow therapeutic window, with plasma levels ranging from 2 to 2.42 mg/L.12 Rapid bacterial killing occurs at concentrations above the colistin MIC breakpoint value,9,13 but levels above 2.42 mg/mL are associated with nephrotoxicity.12 Given this, therapeutic drug monitoring of colistin in individual patients to achieve the target free-drug area under the concentration-time curve to MIC ratio can improve its efficacy.9,11 Approximately half of the CR-GNB isolated in the study were P. aeruginosa, one-third were A. baumannii, and 18% were Enterobacterales.
Following the release of colistin dosing guidelines,9 an LD was added to the SFDR in some patients who were subsequently excluded from the study. It is worth noting that the SFDR went into effect in 2017, prior to the publication of the guideline’s fixed dosing in 2019.9 The SFDR does not include an LD due to the risk of AKI,14,16 and the fact that an adequate q8h colistin dose maintained serum levels within the therapeutic range while an LD did not.12 While the guideline and EMA recommend a flat fixed dose for colistin in adults,9,10 the SFDR stratified the fixed doses based on patient body weight in an attempt to maximize antibiotic efficacy while limiting the risk of resistance,13,53 and AKI development.12 The SFDR values are comparable to those found in a linear pharmacokinetic study, which revealed that a daily dose of 7 MIU divided q8h is optimal for a 60 kg patient with normal renal function.12
Conclusion
This study has shown that IV colistin SFDR was associated with a higher microbiologic cure in carbapenem-non-susceptible, colistin-intermediate GNB infections and a lower incidence of AKI compared to the FDA WBD in critically ill adults. Microbiologic failure was observed at low colistin doses without a corresponding decrease in the incidence of AKI. Larger studies with prospective designs are warranted to confirm these findings.
Data Sharing Statement
The author confirms that the data supporting the findings of this study are available within the article.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of JHAH (IRB-18-51). The author acknowledges the use of JHAH facilities for the research data utilized in this article. The views expressed in this article are solely those of the author and do not necessarily reflect those of JHAH.
Informed Consent
Patient consent was waived because the study relied on retrospective analysis of existing patient records.
Privacy of Participants
The patient data accessed was maintained confidentially and in accordance with applicable data protection and privacy regulations.
Disclosure
The authors declare no conflicts of interest.
References
1. Katip W, Uitrakul S, Oberdorfer P. A Comparison of colistin versus colistin plus meropenem for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients: a propensity score-matched analysis. Antibiotics. 2020;9(10):647. doi:10.3390/antibiotics9100647
2. Suwantarat N, Carroll KC. Epidemiology and molecular characterization of multidrug-resistant Gram-negative bacteria in Southeast Asia. Antimicrob Resist Infect Control. 2016;5:15. doi:10.1186/s13756-016-0115-6
3. Johns Hopkins Aramco Healthcare. Saudi: Antibiogram reports, 2023. Available from: https://insite.jhah.com/orgs/SamsoMembers/Lists/Infection%20Control%202011/AllItems.aspx . Accessed
4. Shi H, Lee JS, Park SY, et al. Colistin plus carbapenem versus colistin monotherapy in the treatment of carbapenem-resistant Acinetobacter baumannii pneumonia. Infect Drug Resist. 2019;12:3925–3934. doi:10.2147/IDR.S234211
5. Martis N, Leroy S, Blanc V. Colistin in multi-drug resistant Pseudomonas aeruginosa blood-stream infections: a narrative review for the clinician. J Infect. 2014;69(1):1–12. doi:10.1016/j.jinf.2014.03.001
6. National Institute for Healthcare Excellence. UK: NICE impact antimicrobial resistance; 2018. Available from: https://www.nice.org.uk/Media/Default/About/what-we-do/Into-practice/measuring-uptake/NICEimpact-antimicrobial-resistance.pdf.
7. Haseeb A, Farida HS, Al Ghamdi S, et al. Dose optimization of colistin: a systematic review. Antibiotics. 2021;10(12):1454. doi:10.3390/antibiotics10121454
8. FDA. Coly-Mycin (Colistimethate) [Package Insert]. Chestnut Ridge, NY: Par Pharmaceutical (per FDA); 2017.
9. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
10. European Medicines Agency. Polymyxin-containing medicines; 2018. Available from: https://www.ema.europa.eu/en/medicines/human/referrals/polymyxin-containing-medicines.
11. Tsala M, Vourli S, Georgiou P-C, et al. Exploring colistin pharmacodynamics against Klebsiella pneumoniae: a need to revise current susceptibility breakpoints. J Antimicrob Chemother. 2018;73(4):953–961. doi:10.1093/jac/dkx522
12. Gontijo AVL, Cavalieri AVG. Optimal control for colistin dosage selection. J Pharmacokinet Pharmacodyn. 2021;48(6):803–813. doi:10.1007/s10928-021-09769-6
13. Bergen PJ, Li J, Nation RL, Turnidge JD, Coulthard K, Milne RW. Comparison of once-, twice- and thrice-daily dosing of colistin on antibacterial effect and emergence of resistance: studies with Pseudomonas aeruginosa in an in vitro pharmacodynamic model. J Antimicrob Chemother. 2008;61(3):636–642. doi:10.1093/jac/dkm511
14. Karaiskos I, Friberg L, Pontikis K, et al. Colistin population pharmacokinetics after application of a loading dose of 9 MU colistin methanesulfonate in critically ill patients. Antimicrob Agents Chemother. 2015;59(12):7240–7248. doi:10.1128/AAC.00554-15
15. Plachouras D, Karvanen M, Friberg S, et al. Population pharmacokinetic analysis of colistin methanesulfonate and colistin after intravenous administration in critically ill patients with infections caused by Gram-negative bacteria. Antimicrob Agents Chemother. 2009;53(8):3430–3436. doi:10.1128/AAC.01361-08
16. Bergen PJ, Li J, Nation RL. Dosing of colistin-back to basic PK/PD. Curr Opin Pharmacol. 2011;11(50):464–469. doi:10.1016/j.coph.2011.07.004
17. Ordooei Javan A, Shokouhi S, Sahraei Z, Salamzadeh J, Azad Armaki S. Nephrotoxicity of high and conventional dosing regimens of colistin: a randomized clinical trial. Iran J Pharm Res. 2017;16(2):781–790.
18. Alshaya AI, Bin Saleh K, Aldhaeefi M, et al. Colistin loading dose in septic patients with Gram negative infections. Infect Drug Resist. 2022;15:2159–2166. doi:10.2147/IDR.S361244
19. Durante-Mangoni E, Signoriello G, Andini R, et al. Colistin and rifampicin compared with colistin alone for the treatment of serious infections due to extensively drug-resistant Acinetobacter baumannii: a multicenter, randomized clinical trial. Clin Infect Dis. 2013;57(3):349–358. doi:10.1093/cid/cit253
20. Katip W, Uitrakul S, Oberdorfer P. The effectiveness and nephrotoxicity of loading dose colistin combined with or without meropenem for the treatment of carbapenem-resistant A. baumannii. Int J Infect Dis. 2020;97:391–395. doi:10.1016/j.ijid.2020.05.100
21. Kellum JA, Lameire N, Aspelin P. Kidney Disease: improving Global Outcomes (KDIGO). Acute Kidney Injury Work Group. KDIGO clinical practice guidelines for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
22. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
23. Winter MA, Guhr KN, Berg GM. Impact of Various Body Weights and Serum Creatinine Concentrations on the Bias and Accuracy of the Cockcroft-Gault Equation. Pharmacotherapy. 2012;32:604–612. doi:10.1002/j.1875-9114.2012.01098.x
24. Humphries RM, Abbott AN, Hindler JA. Understanding and Addressing CLSI Breakpoint Revisions: a Primer for Clinical Laboratories. J Clin Microbiol. 2019;57(6):e00203–19. doi:10.1128/JCM.00203-19
25. Clinical and Laboratory Standards Institute (CLSI). Meropenem Breakpoints for Acinetobacter Spp.
26. Clinical and Laboratory Standards Institute (CLSI). Polymyxin Breakpoints for Enterobacterales, Pseudomonas Aeruginosa, and Acinetobacter Spp.
27. Lambden S, Laterre PF, Levy MM, et al. The SOFA score-development, utility and challenges of accurate assessment in clinical trials. Crit Care. 2019;23(1):374. doi:10.1186/s13054-019-2663-7
28. Parchem NL, Bauer KA, Cook CH, et al. Colistin combination therapy improves microbiologic cure in critically ill patients with multi-drug resistant Gram-negative pneumonia. Eur J Clin Microbiol Infect Dis. 2016;35(9):1433–1439. doi:10.1007/s10096-016-2681-1
29. Rosner B. Estimation of sample size and power for comparing two binominal proportions. In: Fundamentals of Biostatistics.
30. Chew KL, La MV, Lin RTP, et al. Colistin and Polymyxin B Susceptibility Testing for Carbapenem-Resistant and mcr-Positive Enterobacteriaceae: comparison of Sensititre, MicroScan, Vitek 2, and Etest with Broth Microdilution. J Clin Microbiol. 2017;55(9):2609–2616. doi:10.1128/JCM.00268-17
31. Vardakas KZ, Mavroudis AD, Georgiou M, et al. Intravenous plus inhaled versus intravenous colistin monotherapy for lower respiratory tract infections: a systematic review and meta-analysis. J Infect. 2018;76(4):321–327. doi:10.1016/j.jinf.2018.02.002
32. Markou N, Apostolakos H, Koumoudiou C, et al. Intravenous colistin in the treatment of sepsis from multiresistant Gram-negative bacilli in critically ill patients. Crit Care. 2003;7(5):R78–83. doi:10.1186/cc2358
33. Vandijck DM, Reynvoet E, Blot SI, Vandecasteele E, Hoste EA. Severe infection, sepsis and acute kidney injury. Acta Clin Belg. 2007;62 Suppl 2:332–336. doi:10.1179/acb.2007.075
34. Dewi RS, Radji M, Andalusia R. Evaluation of Antibiotic Use among Sepsis Patients in an Intensive Care Unit: a cross-sectional study at a referral hospital in Indonesia. Sultan Qaboos Univ Med J. 2018;18(3):e367–73. doi:10.18295/squmj.2018.18.03.017
35. Timsit JF, de Kraker M, Sommer H, et al. Appropriate endpoints for evaluation of new antibiotic therapies for severe infections: a perspective from COMBACTE’s STAT-Net. Intensive Care Med. 2017;43(7):1002–1012. doi:10.1007/s00134-017-4802-4
36. Giacobbe DR, Saffioti C, Losito AR, et al. Use of colistin in adult patients: a cross-sectional study. J Glob Antimicrob Resist. 2020;20:43–49. doi:10.1016/j.jgar.2019.06.009
37. Ehrmann S, Luyt CE. Optimizing aerosol delivery of antibiotics in ventilated patients. Curr Opin Infect Dis. 2020;33(2):197–204. doi:10.1097/QCO.0000000000000633
38. Tamma PD, Aitken SL, Bonomo RA, et al. Infectious Diseases Society of America Antimicrobial-Resistant Treatment Guidance: gram-Negative Bacterial Infections. Infectious Diseases Society of America 2023; Version 3.0. Available from: https://www.idsociety.org/practice-guideline/amr-guidance/.
39. Boisson M, Jacobs M, Grégoire N, et al. Comparison of intrapulmonary and systemic pharmacokinetics of colistin methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically ill patients. Antimicrob Agents Chemother. 2014;58(12):7331–7339. doi:10.1128/AAC.03510-14
40. Paul M, Daikos GL, Durante-Mangoni E, et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: an open-label, randomised controlled trial. Lancet Infect Dis. 2018;18(4):391–400. doi:10.1016/S1473-3099(18)30099-9
41. Kaye KS, Marchaim D, Thamlikitkul V, et al. Colistin Monotherapy versus Combination Therapy for Carbapenem-Resistant Organisms. NEJM Evid. 2022;2(1):EVIDoa2200131. doi:10.1056/EVIDoa2200131
42. Zhang P, Hu H, Shi Q, et al. The Effect of β-Lactam Antibiotics on the Evolution of Ceftazidime/Avibactam and Cefiderocol Resistance in KPC-Producing Klebsiella pneumoniae [published online ahead of print, 2023 Feb 16]. Antimicrob Agents Chemother. 2023:e0127922. doi:10.1128/aac.01279-22
43. Marner M, Kolberg L, Horst J, et al. Antimicrobial Activity of Ceftazidime-Avibactam, Ceftolozane-Tazobactam, Cefiderocol, and Novel Darobactin Analogs against Multidrug-Resistant Pseudomonas aeruginosa Isolates from Pediatric and Adolescent Cystic Fibrosis Patients. Microbiol Spectr. 2023;11(1):e0443722. doi:10.1128/spectrum.04437-22
44. Giani T, Arena F, Vaggelli G, et al. Large Nosocomial Outbreak of Colistin-Resistant, Carbapenemase-Producing Klebsiella pneumoniae Traced to Clonal Expansion of an mgrB Deletion Mutant. J Clin Microbiol. 2015;53(10):3341–3344. doi:10.1128/JCM.01017-15
45. Capone A, Giannella M, Fortini D, et al. High rate of colistin resistance among patients with carbapenem-resistant Klebsiella pneumoniae infection accounts for an excess of mortality. Clin Microbiol Infect. 2013;19(1):E23–30. doi:10.1111/1469-0691.12070
46. Marchaim D, Chopra T, Pogue JM, et al. Outbreak of colistin-resistant, carbapenem-resistant Klebsiella pneumoniae in metropolitan Detroit, Michigan. Antimicrob Agents Chemother. 2011;55(2):593–599. doi:10.1128/AAC.01020-10
47. Antoniadou A, Kontopidou F, Poulakou G, et al. Colistin-resistant isolates of Klebsiella pneumoniae emerging in intensive care unit patients: first report of a multiclonal cluster. J Antimicrob Chemother. 2007;59(4):786–790. doi:10.1093/jac/dkl562
48. Sharma S, Banerjee T, Kumar A, et al. Extensive outbreak of colistin resistant, carbapenemase (blaOXA-48, blaNDM) producing Klebsiella pneumoniae in a large tertiary care hospital, India. Antimicrob Resist Infect Control. 2022;11(1). doi:10.1186/s13756-021-01048-w
49. Dickstein Y, Lellouche J, Schwartz D, et al. Colistin Resistance Development Following Colistin-Meropenem Combination Therapy Versus Colistin Monotherapy in Patients With Infections Caused by Carbapenem-Resistant Organisms. Clin Infect Dis. 2020;71(10):2599–2607. doi:10.1093/cid/ciz1146
50. Almutairi MM. Synergistic activities of colistin combined with other antimicrobial agents against colistin-resistant Acinetobacter baumannii clinical isolates. PLoS One. 2022;17(7):e0270908. doi:10.1371/journal.pone.0270908
51. Bir R, Gautam H, Arif N, et al. Analysis of colistin resistance in carbapenem-resistant Enterobacterales and XDR Klebsiella pneumoniae. Ther Adv Infect Dis. 2022;9:20499361221080650. doi:10.1177/20499361221080650
52. Zilberberg MD, Kollef MH, Shorr AF. Secular trends in Acinetobacter baumannii resistance in respiratory and blood stream specimens in the United States, 2003 to 2012: a survey study. J Hosp Med. 2016;11(1):21–26. doi:10.1002/jhm.2477
53. Michalopoulos AS, Falagas ME. Colistin: recent data on pharmacodynamics properties and clinical efficacy in critically ill patients. Ann Intensive Care. 2011;1(1):30. doi:10.1186/2110-5820-1-30
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.