Back to Journals » Cancer Management and Research » Volume 14
“Micro” Extrathyroidal Extension in Risk Stratification for Papillary Thyroid Carcinoma: Should It Be in the Intermediate-Risk or High-Risk Group? A Single-Center Retrospective Study
Authors He Q ![]() , Ji F, Fu X, Li Z, Qiu X
, Ji F, Fu X, Li Z, Qiu X ![]()
Received 23 September 2022
Accepted for publication 9 November 2022
Published 16 November 2022 Volume 2022:14 Pages 3181—3190
DOI https://doi.org/10.2147/CMAR.S390468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Qi He, Feihong Ji, Xinghao Fu, Zehao Li, Xinguang Qiu
Department of Thyroid Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China
Correspondence: Xinguang Qiu, Email [email protected]
Introduction: Currently, there is no consensus on the specific effect of Extrathyroidal Extension (ETE) on prognosis. The purpose of our study was to study the relationship between different states of ETE and its disease-free survival rate and to determine the basic standard of Micro ETE (tumor extends through capsule only) in risk stratification.
Material and Methods: We conducted a retrospective and single-center study that included the clinical data of all papillary thyroid carcinoma (PTC) patients with ETE in our hospital from 2013 to 2017 and followed them up after rigorous screening. According to ETE state, it is divided into four groups: Microscopic, Micro, Minimal, Macro. Kaplan–Meier method was used to calculate disease-free survival (DFS). Log-rank test was used to compare the differences between the groups and to polt the survival curves. P< 0.05 was considered statistically significant. Micro ETE was included in different risk stratification subgroups and their DFS was compared.
Results: A total of 436 patients were included: Microscopic group N=50 (11.47%), Micro group N=74 (16.97%), Minimal group N=135 (30.96%), and Macro group N=177 (40.60%). The frequency of ETE was in strap muscles N=191, trachea N=114, laryngeal recurrent nerve N=92, and capsule N=74, etc. The 5-year DFS rate in Micro group was 95.3%, higher than that in Macro group (P< 0.05). The 5-year DFS rate of Micro ETE was 90.0% in the intermediate-risk group and 84.9% in the high-risk group when Micro ETE was included in different risk stratification subgroups.
Conclusion: Micro ETE deserves more attention, has a batter prognosis than Macro ETE, and may have little effect on recurrence. It seems more appropriate to treat Micro ETE as the intermediate-risk group in risk stratification.
Keywords: extrathyroidal extension, risk stratification, papillary thyroid carcinoma, prognosis
Introduction
For nearly half a century, thyroid carcinoma has become the most common surgical solid tumor, with a sharp spike in global incidence.1 Differentiated Thyroid Carcinoma (DTC) has mild biological behavior, including Papillary Thyroid Carcinoma (PTC) and Follicular Thyroid Carcinoma (FTC).2 As the most common type of thyroid cancer pathology, PTC’s treatment mainly relies on surgery, and the overall cure rate is high, with a 10-year survival rate of more than 95%.3 However, there are also some risk factors that have an impact on prognosis, with Extrathyroidal Extension (ETE) of thyroid cancer being a hot topic of concern for clinicians.4 ETE was defined as breakthrough of the thyroid capsule and infiltration of other tissues.5
In the latest eighth edition of the American Joint Committee on Cancer (AJCC) TNM staging, T3 staging was first divided into T3a and T3b, and “minimal” thyroid invasions were removed from the T3 staging.6 The reason was probably based on the understanding that “minimal” ETE did not affect survival or recurrence.7 Meanwhile, what did not change was the clinicopathological features associated with ETE as prognostic recurrence risk grouping. As microscopic ETE was intermediate-risk and macroscopic ETE was high-risk group, however, the extent of ETE was not clearly stated.8 Less controversially, both microscopic ETE and macroscopic ETE are strongly associated with lymph node metastasis. Arora suggested that it should be stratified into groups of none, microscopic, and macroscopic ETE, even the significance of microscopic ETE is undetermined.9
Moreover, the stratification of recurrence risk in ETE varies from country to country. Differences in ethnic genetics, ethnic differences, living environments, and regional medical technology levels of patient groups analyzed in different studies make the treatment approach and prognosis impact of ETE still controversial.10 The TSH suppression treatment standards taken by different intermediate-risk and high-risk recurrence risk stratifications are also different, and long-term TSH treatment also has certain risks, and more aggressive therapies may result in overtreatment posing a risk to some patients. In this study, relevant clinical data were collected from single centers in China, and patients were strictly followed up. Disease-free survival (DFS) was used as an indicator to explore the impact of Micro ETE on prognosis.
Methods
Setting and Population
In order to ensure a longer follow-up period, the clinicopathological data of patients with PTC who were admitted to our hospital at least five years ago (2013–2017) were collected. The collected clinicopathological features include age, sex, maximum tumor diameter, unilateral or bilateral lesions, single or multiple lesions, with or without ETE, lymph node metastasis and I131 conditions, etc.
The inclusion criteria were as follows: Adults, older than 18 years old; patients who underwent thyroid surgery for the first time, and the routine results of postoperative pathology confirmed to be PTC; the clinical feature data and follow-up data of the case were complete.
The exclusion criteria included: The first surgical treatment in the outer hospital; other pathological types such as FTC, medullary thyroid carcinoma (MTC) and other anaplastic thyroid cancer (ATC); case data are incomplete and there are no follow-up records.
Patients were stratified by degree of ETE into 1 of 4 groups: “Microscopic” (Microscopic invasion of tumor into the perithyroidal soft tissues), “Micro” (tumor extends through capsule only), “Minimal” (tumor extends into any of the strap muscles, including the omohyoid, sternohyoid, sternothyroid, or thyrohyoid), and “Macro” (tumor extends to soft tissues or other anatomy beyond the strap muscles). Multiple tumors can be identified as ETE if any of the lesions are accompanied by invasion.
Treatment Modalities
All patients were treated with a combination of surgery–I131–TSH suppression therapy. All patients were operated on by the same experienced thyroid surgery team. Total thyroidectomy was performed on all patients with ETE. For patients with CN0 (lymph node negative), preventive central lymph node dissection (cervical VI lymph node) is routinely performed. Patients with partial CN1 (enlarged lymph nodes) may undergo modified (enlarged) radical thyroidectomy ranging from cervical zone II to cervical zone VI lymph node resection.11 The presence of ETE was assessed by either intra- or post-operative pathology findings. Surgical safety is a main concern. R0 should be excised as far as possible, and the complications should be strictly controlled.12 Further radiation iodine-131 consolidation therapy were given after surgery, depending on the patient’s condition13,14 and TSH suppression was given to all patients according to the ATA guideline for risk stratification .15
Follow-Up Mode
Thyroid hormone and antibody tests should be performed at least every three months, thyroid neck ultrasound should be reviewed every six months, and chest CT should be reviewed at least once. According to the latest ATA Guidelines, disease-free status is defined as follows: Thyroglobulin (Tg) was not detected in negative anti-thyroglobulin antibody (TgAb) (<10ng/mL), no residual lesions or enlarged lymph nodes were found on cervical ultrasound, and negative systemic iodine-131 scans.16 Recurrence was defined as metachronous lesions with a postoperative interval of more than three months, ie local recurrence (residual thyroid tissue recurrence or regional lymph node metastasis) and distant metastasis (lung or bone, etc.). For suspected recurrence, oral levothyroxine tablets may be discontinued for two weeks until TSH levels are elevated and a systemic diagnostic iodine-131 scan, or FNAB, is performed for confirmation. The initial time to surgery is defined as the initial event, and the time to recurrence is defined as the end event. For patients without recurrence, strict follow-up criteria were applied, with the end time defined as the time since the patient was last seen at our hospital for a negative ultrasound. Follow-up time and disease status (asymptomatic or recurrent) were obtained and DFS recorded.
Statistical Methods
SPSS26.0 statistical software was used for data analysis. Continuous variables are reported as median and range, and categorical variables as frequency and proportion. The DFS was calculated by the Kaplan–Meier method, the differences between different groups were compared using by the Log-rank test and the recurrence survival curves wee plotted. P<0.05 is considered statistically significant.
Ethics Approval and Guidelines Statement
The study was approved by the Medical Ethics Committee of Zhengzhou University (Approval No.2021-KY-0202-002). All of the procedures performed with human participants conformed to the research committee’s ethical standards and to the 1964 Declaration of HELSINKI and its subsequent amendments and comparable ethical standards.
Informed Consent Statements
All data was queried by the hospital system, was only open only to medical practices, not to private individuals, and all patients have signed informed consent forms. When it comes to privately identifiable information, it is only represented by numbers, so this study will not cause harm to the interests of the individuals concerned.
Results
A total of 35,227 patient medical records were detected from 2013 to 2017. After screening and statistics, a total of 436 cases meeting the criteria were included in this study (Figure 1).
Figure 2 shows the distribution of different states of aggression in 436 PTC patients with ETE, which is dominated by Macro ETE (40.6%). The frequency of invasion was strap muscles, trachea, recurrent laryngeal nerve and extends through capsule only, etc. (Figure 3) Of 46 cases of invasion of two kinds of tissues and organs at the same time, more than three and three kinds of tissues and organs 38 cases, 16 cases of lymph node invasion organ.
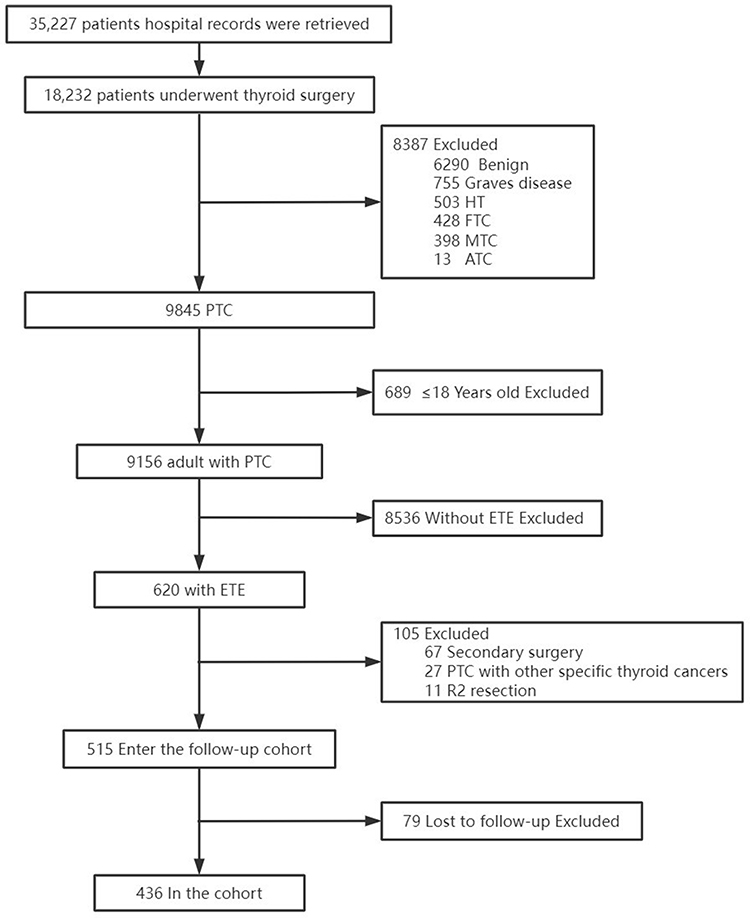 |
Figure 1 Flow diagram for study participants. Abbreviations: ETE, Extrathyroidal Extension; HT, Hashimoto’s thyroiditis; PTC, Papillary thyroid microcarcinoma; FTC, Follicular thyroid carcinoma; MTC, Medullary thyroid carcinoma; ATC, anaplastic thyroid carcinoma. |
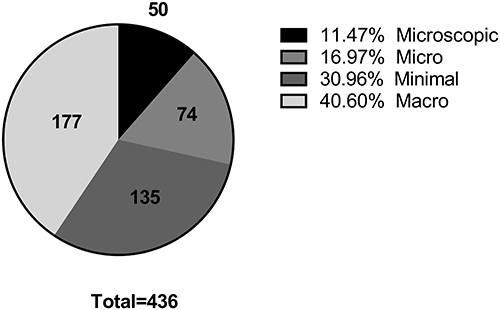 |
Figure 2 Extrathyroidal extension state. |
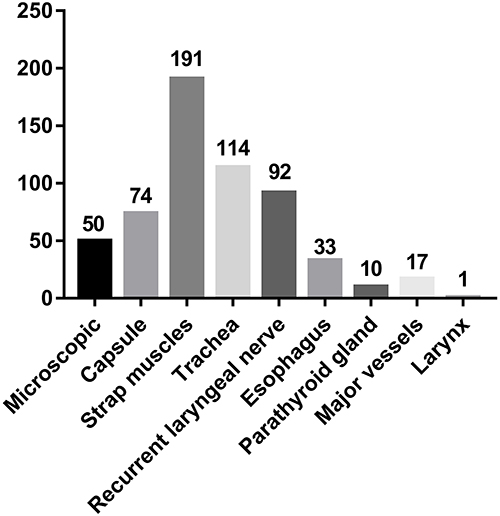 |
Figure 3 Frequency histogram of each site of extrathyroidal extension. |
Table 1 shows the sample’s baseline characteristics. All the patients with ETE were mainly female (76.6%), aged 49 (19–80) years, 54.6% of them were associated with lymph node metastasis, and almost 86.7% of them were associated with BRAF600E gene mutation. Group, as the degree of invasion becomes more severe, the maximum diameter of the tumor becomes larger, and more bilateral and multifocal tumors are accounted for, suggesting that the primary tumor is becoming more aggressive. All patients received a total thyroidectomy in principle, but 11 of them underwent only a lobectomy due to postoperative routine pathological findings with microscopic ETE, so these patients also did not receive iodine-131 treatment. The reason why one patient in the Micro ETE chose lobectomy was that the patient was a young woman and strongly requested unilateral lobectomy before surgery. Eight patients abandoned iodine-131 treatment because their bodies could not tolerate it.
The last follow-up was in April 2022, with follow-up periods ranging from 6 to 105 months and median follow-up of 46 months, during which 79 cases were lost to follow-up.Among the remaining patients with complete follow-up data, a total of 38 patients with recurrence(8.7%), including 34 patients had lymph node recurrence, one patient had lymph node metastasis in the muscle of the left shoulder chest wall, one patient had mediastinal metastasis and two patients had lung metastasis. There were no death and the overall survival rate was 100%. A total of 130 patients with temporary hypocalcemia were improved after calcium supplement therapy, and 24 patients with hoarseness recovered within half a year.
 |
Table 1 The Sample’s Baseline Characteristics |
Guidelines for risk stratification of ETE vary from country to country, and the effect of ETE on prognosis was not differentiated in detail (Table 2). Therefore, we first calculated and plotted disease-free survival curves of four groups and compared them. Results show that the Macro and Microscopic group, Macro and Micro group contrast was statistically significant (P<0.05) (Figure 4A). Micro group of 5-year disease-free survival rate was 95.3%. To further discuss the effect of Micro ETE on prognosis, we innovatively included Micro ETE into different subgroups, that is, only intermediate-risk group or only high-risk group, and analyzed disease-free survival curves of different subgroups with ETE. The results showed that if the Micro ETE was included in the intermediate-risk group, the 5-year disease-free survival rate was 90.0%, as shown in Figure 4B, and the 5-year disease-free survival rate was 84.9% in the high-risk group, as shown in Figure 4C. It seems that inclusion in the intermediate-risk group is closer than 95.3%.
 |
Figure 4 Kaplan–Meier survival plots stratified by extent of ETE for patients with PTC. (A) Disease-free survival of four groups; (B) Disease-free survival of Micro ETE was included in the intermediate-risk group; (C) Disease-free survival of Micro ETE was included in the high-risk group. |
Discussion
The incidence of PTC is increasing year by year, and up to 30% of PTC patients are found to be accompanied by ETE, which makes the population accompanied by ETE more and more large. It has been suggested that this increase may be partly due to environmental factors and lifestyle changes. In addition, studies have reported that Asians are more prone to ETE than whites and blacks.1,23,24 However, in this study, the ETE ratio is only 4.7% (436/9156). Mete believed that there are two thin layers of fibrous tissue covering the surface of normal thyroid gland tissue, namely “true capsule” and “false capsule”.25 There are neurovascular and parathyroid structures between the two capsular layers. This special anatomical structure leads to the lack of accuracy and objectivity in ETE judgment. Kowalski believed that ETE could be divided into the “eye ETE” and “microscopic ETE”, that is, judging from the naked eye during imaging or clinical operation and direct postoperative microscopic pathological evidence.26 The “eye ETE” can be evaluated and judged by experienced clinicians, but due to the “adhesion” of tumor and tissue and the limitation of operation in special position, there is a great interference on whether the tumor really “invaded”, especially micro ETE. On the other hand, the microscopic ETE was relatively accurate, and could be accurately judged if words such as “invasion” and “infiltration” appeared in the pathological report. However, the level of medical treatment varies greatly in different countries and regions, especially in the department of pathology, and it is still unknown whether the microscopic ETE can be accurately diagnosed. Thyroid invasion of the capsule is a common feature in thyroid surgery, which is most common in PTC. In the case of capsule invasion, the cancer foci protruded outwardly and broke through the outer capsule during the operation, and sometimes the gray and white cancer foci were seen, which were tough and difficult to push.27 With the improvement of the accuracy and popularity of high-resolution ultrasound instruments, more and more nodules facing the capsule have been found, and these nodules are often not recommended for conservative observation, which makes the occurrence of micro ETE less and less during surgery. Therefore, whether micro ETE really affects prognosis deserves further consideration.
Tran showed that regardless of the age of patients, the risk of recurrence in patients with ETE increased by two times compared with patients without ETE.28 Relevant studies have shown that micro ETE and minimal ETE are not important influencing factors for staging, but there are significant differences in local recurrence and survival rate, which may be the reason why micro ETE was removed from T3 staging in the eighth edition of AJCC guidelines.29 Other studies held different opinions, arguing that micro ETE did not affect survival and recurrence rates. Therefore, comprehensive consideration could be taken according to individual differences and tumor characteristics to ensure the integrity of tumor resection and individualized treatment.30
From Table 2, we can see that every guideline only defines microscopic invasion and macroscopic invasion, micro ETE was ignored. ETA risk stratification even removes microscopic invasion, and only a Chinese guideline for risk stratification of thyroid cancer appears to classify microscopic ETE as intermediate-risk. The results of this study showed that the 5-year disease-free survival rate of micro ETE was 95.3%, which was close to 90.0% in the intermediate-risk group and much higher than 84.9% in the high-risk group. Higher risk stratification is faced with more stringent TSH inhibition treatment. Subclinical hyperthyroidism is the consequence of patients taking super-physiological dose of thyroid hormone after thyroid surgery. In particular, when TSH of some high-risk patients needs to be maintained at <0.1mu/L for a long time, the heart load of patients, especially elderly patients, may be aggravated, leading to arrhythmia, atrial fibrillation and other cardiovascular diseases, resulting in an increased risk of death.31 The 2015ATA guidelines strongly recommend 131I therapy for patients with ETE in high risk of recurrence. Radiation 131I treatment may cause acute complications and long-term side effects, and the incidence and severity of adverse reactions are related to the accumulation of therapeutic doses.32
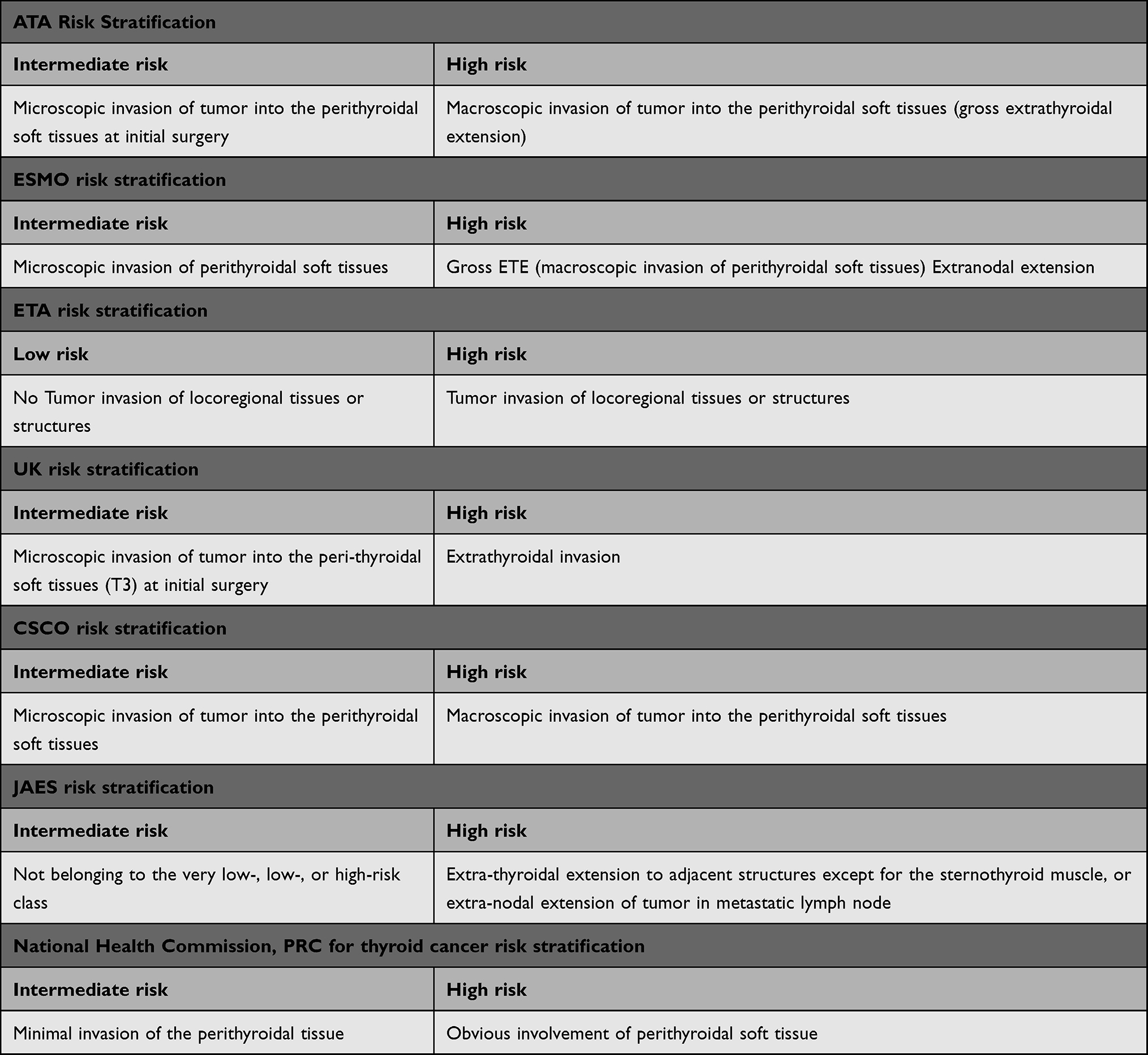 |
Table 2 Guidelines for Risk Stratification of ETE in Different Country |
In those PTC with ETE, the microscopic-micro-minimal ETE process may be a gradual process, all of which are manifestations of different stages of tumor high aggressiveness. Microscopic is difficult to detect in surgery, and Micro and Minimal do not have a unified diagnostic standard. Today, precision therapy is gradually advocated, and the effect of subdivision ETE on risk stratification is particularly important. It is not controversial that macro ETE has a worse prognosis than microscopic and micro ETE (P<0.05). The ATA included trachea and recurrent laryngeal nerve invasion in macro ETE. However, the ETE caused by the special location of the tumor in some patients may not be caused by the aggressiveness of the tumor itself, and it remains to be seen whether these patients have received excessive treatment. ETE is a manifestation of high aggressiveness of tumor, which is equivalent to “external appearance”, while high-risk subtypes are its “core”. It seems that the emphasis on highly invasive subtypes as the criteria for diagnosis and inclusion of relapse risk stratification may be more intuitive than the clinical characteristics of ETE, which have a greater impact on prognosis. It is expected that future guideline studies will be updated.
We should develop an appropriate comprehensive treatment plan according to the individual situation, find a balance between tumor eradication and surgical risk, avoid over-conservative or over-treatment, guarantee the postoperative quality of life of patients, and improve long-term survival rate. Long-term regular follow-up of ETE patients, strict monitoring of TSH inhibition treatment, neck ultrasound and serum Tg monitoring for early detection of possible recurrence and timely intervention. To establish a dynamic risk assessment model for PTC patients with ETE and actively explore the impact of different ETE levels and clinical characteristics on prognosis, so that patients will benefit most from refined patient management in the future.
The conclusion of this study is that micro ETE may have little impact on recurrence, and it should pay more attention to, risk stratification as intermediate-risk group seems to be more appropriate. Clinical studies of the scope of surgery associated with micro ETE will continue in order to maximize the benefit to patients.
Our study has many limitations. This was a retrospective and single-center study, for example, with insufficient number of cases and insufficient follow-up. This is because we try to include cases by very strict selection criteria, and the evidence from patient descriptions from telephone follow-up alone is hardly convincing. Therefore, we consider our data to be highly valid.
Funding
This work was supported by a grant from Thermal Ablation of Thyroid Nodules International Joint Laboratory [Henan Province; YUKEWAI (2016), number 11]. We appreciate the help of the First Affiliated Hospital of Zhengzhou University in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li M, Dal Maso L, Vaccarella S. Global trends in thyroid cancer incidence and the impact of overdiagnosis. Lancet Diabetes Endocrinol. 2020;8(6):468–470. doi:10.1016/S2213-8587(20)30115-7
2. Pacini F, Castagna MG. Approach to and treatment of differentiated thyroid carcinoma. Med Clin North Am. 2012;96(2):369–383. doi:10.1016/j.mcna.2012.01.002
3. Haugen BR, Alexander EK, Bible KC, et al. 2015 American thyroid association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
4. Jin BJ, Kim MK, Ji YB, Song CM, Park JH, Tae K. Characteristics and significance of minimal and maximal extrathyroidal extension in papillary thyroid carcinoma. Oral Oncol. 2015;51(8):759–763. doi:10.1016/j.oraloncology.2015.05.010
5. Diker-Cohen T, Hirsch D, Shimon I, et al. Impact of minimal extra-thyroid extension in differentiated thyroid cancer: systematic review and meta-analysis [published online ahead of print, 2018 Mar 1]. J Clin Endocrinol Metab. 2018. doi:10.1210/jc.2018-00081
6. Shaha AR, Migliacci JC, Nixon IJ, et al. Stage migration with the new American Joint Committee on Cancer (AJCC) staging system (8th edition) for differentiated thyroid cancer. Surgery. 2019;165(1):6–11. doi:10.1016/j.surg.2018.04.078
7. Bortz MD, Kuchta K, Winchester DJ, Prinz RA, Moo-Young TA. Extrathyroidal extension predicts negative clinical outcomes in papillary thyroid cancer. Surgery. 2021;169(1):2–6. doi:10.1016/j.surg.2020.04.003
8. Mercante G, Frasoldati A, Pedroni C, et al. Prognostic factors affecting neck lymph node recurrence and distant metastasis in papillary microcarcinoma of the thyroid: results of a study in 445 patients. Thyroid. 2009;19(7):707–716. doi:10.1089/thy.2008.0270
9. Arora N, Turbendian HK, Scognamiglio T, et al. Extrathyroidal extension is not all equal: implications of macroscopic versus microscopic extent in papillary thyroid carcinoma. Surgery. 2008;144(6):942–948. doi:10.1016/j.surg.2008.07.023
10. Shin JH, Ha TK, Park HK, et al. Implication of minimal extrathyroidal extension as a prognostic factor in papillary thyroid carcinoma. Int J Surg. 2013;11(9):944–947. doi:10.1016/j.ijsu.2013.06.015
11. Cracchiolo JR, Wong RJ. Management of the lateral neck in well differentiated thyroid cancer. Eur J Surg Oncol. 2018;44(3):332–337. doi:10.1016/j.ejso.2017.06.004
12. Wang LY, Nixon IJ, Patel SG, et al. Operative management of locally advanced, differentiated thyroid cancer. Surgery. 2016;160(3):738–746. doi:10.1016/j.surg.2016.04.027
13. Fleeman N, Houten R, Chaplin M, et al. A systematic review of lenvatinib and sorafenib for treating progressive, locally advanced or metastatic, differentiated thyroid cancer after treatment with radioactive iodine. BMC Cancer. 2019;19(1):1209. doi:10.1186/s12885-019-6369-7
14. Schlumberger M, Tahara M, Wirth LJ, et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med. 2015;372(7):621–630. doi:10.1056/NEJMoa1406470
15. Haugen BR, Sawka AM, Alexander EK, et al. American thyroid association guidelines on the management of thyroid nodules and differentiated thyroid cancer task force review and recommendation on the proposed renaming of encapsulated follicular variant papillary thyroid carcinoma without invasion to noninvasive follicular thyroid neoplasm with papillary-like nuclear features. Thyroid. 2017;27(4):481–483. doi:10.1089/thy.2016.0628
16. Van Nostrand D. Radioiodine refractory differentiated thyroid cancer: time to update the classifications. Thyroid. 2018;28(9):1083–1093. doi:10.1089/thy.2018.0048
17. Filetti S, Durante C, Hartl D, et al. Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(12):1856–1883. doi:10.1093/annonc/mdz400
18. Pacini F, Schlumberger M, Dralle H, et al. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium [published correction appears in Eur J Endocrinol. 2006 Aug;155(2):385]. Eur J Endocrinol. 2006;154(6):787–803. doi:10.1530/eje.1.02158
19. Mitchell AL, Gandhi A, Scott-Coombes D, Perros P. Management of thyroid cancer: United Kingdom national multidisciplinary guidelines. J Laryngol Otol. 2016;130(S2):S150–S160. doi:10.1017/S0022215116000578
20. Thyroid Cancer Working Group C. Chinese Society of Clinical Oncology (CSCO) diagnosis and treatment guidelines for persistent/recurrent and metastatic differentiated thyroid cancer 2018 (English version). Chin J Cancer Res. 2019;31(1):99–116. doi:10.21147/j.issn.1000-9604.2019.01.06
21. Ito Y, Onoda N, Okamoto T. The revised clinical practice guidelines on the management of thyroid tumors by the Japan associations of endocrine surgeons: core questions and recommendations for treatments of thyroid cancer. Endocr J. 2020;67(7):669–717. doi:10.1507/endocrj.EJ20-0025
22. National Health Commission of the People’s Republic of China. Diagnosis and treatment guidelines for thyroid cancer (2018 edition). Chin Arch Gener Surg. 2019;13(01):1–15.
23. Youngwirth LM, Adam MA, Scheri RP, Roman SA, Sosa JA. Extrathyroidal extension is associated with compromised survival in patients with thyroid cancer. Thyroid. 2017;27(5):626–631. doi:10.1089/thy.2016.0132
24. Oliveira KJ, Chiamolera MI, Giannocco G, Pazos-Moura CC, Ortiga-Carvalho TM. Thyroid function disruptors: from nature to chemicals [published online ahead of print, 2018 Jul 13]. J Mol Endocrinol. 2018;JME-18–0081. doi:10.1530/JME-18-0081
25. Mete O, Rotstein L, Asa SL. Controversies in thyroid pathology: thyroid capsule invasion and extrathyroidal extension. Ann Surg Oncol. 2010;17(2):386–391. doi:10.1245/s10434-009-0832-7
26. Kowalski LP, Filho JG. Results of the treatment of locally invasive thyroid carcinoma. Head Neck. 2002;24(4):340–344. doi:10.1002/hed.10058
27. Lee DY, Hwang SM, An JH, et al. Predicting extrathyroidal extension in patients with papillary thyroid microcarcinoma according to a BRAF mutation. Clin Exp Otorhinolaryngol. 2017;10(2):174–180. doi:10.21053/ceo.2015.01655
28. Tran B, Roshan D, Abraham E, et al. An analysis of the American joint committee on cancer 8th edition t staging system for papillary thyroid carcinoma. J Clin Endocrinol Metab. 2018;103(6):2199–2206. doi:10.1210/jc.2017-02551
29. Kim HI, Hyeon J, Park SY, et al. Impact of extranodal extension on risk stratification in papillary thyroid carcinoma. Thyroid. 2019;29(7):963–970. doi:10.1089/thy.2018.0541
30. Abraham E, Tran B, Roshan D, et al. Microscopic positive margins in papillary thyroid cancer do not impact disease recurrence. ANZ J Surg. 2018;88(11):1193–1197. doi:10.1111/ans.14490
31. Biondi B, Cooper DS. Thyroid hormone suppression therapy. Endocrinol Metab Clin North Am. 2019;48(1):227–237. doi:10.1016/j.ecl.2018.10.008
32. Clement SC, Peeters RP, Ronckers CM, et al. Intermediate and long-term adverse effects of radioiodine therapy for differentiated thyroid carcinoma--a systematic review. Cancer Treat Rev. 2015;41(10):925–934. doi:10.1016/j.ctrv.2015.09.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.