")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 6
Methods to improve joint attention in young children with autism: a review
Authors Paparella T, Freeman S
Received 8 December 2014
Accepted for publication 18 March 2015
Published 19 May 2015 Volume 2015:6 Pages 65—78
DOI https://doi.org/10.2147/PHMT.S41921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Laurens Holmes, Jr
Tanya Paparella, Stephanny F N Freeman
Department of Child Psychiatry and Biobehavioral Sciences, University of California Los Angeles, Los Angeles, CA, USA
Abstract: We provide an overview of studies in the past 10 years (2004–2014) that have aimed to improve joint attention (JA) in young children at risk for, or with, autism spectrum disorder. Thirteen randomized controlled trial (RCT) interventions were found, which received particular focus. Three studies used intervention methods with a developmental orientation and focused on caregiver-mediated methods. Others used combined developmental and behavioral approaches and delivered intervention via trained interventionists, caregivers, and teachers. Interventions ranged widely in density, both with respect to the amount of intervention delivered weekly and the total duration of intervention. Fourteen single-subject research design (SSRD) studies and one quasi-experimental pre–post design study were also included. Notably absent in the RCTs were studies using only behavioral methods, while behavioral methods dominated in the SSRDs. The outcomes of the RCTs using combined behavioral and developmental methods generally demonstrate short-term social communication gains. While some studies demonstrated long-term maintenance and positive outcomes in related areas such as language, many did not. The mixed results for language outcomes indicate a need for further investigation. In addition, future studies should further examine participants' developmental readiness and intervention dose in relation to outcome, as well as aim to isolate active ingredients of interventions.
Keywords: intervention, joint attention, joint engagement, language, randomized controlled trial
Introduction
Joint attention (JA) is the ability to share experiences and interests about objects and events with others. Whereas neurotypical children develop a range of verbal and nonverbal social communicative skills within the first 2 years of life, children with autism spectrum disorders (ASDs) present with delayed and atypical social development.1 Children with ASD use less communicative gestures, such as pointing and showing, to establish a shared focus of attention. They are also less likely to spend time in joint engagement (JE) when a child and a social partner are involved with the same object or event. This is concerning as children who engage in more JA and JE may facilitate increased social learning opportunities for themselves. Further, JA skills and longer time in JE are linked to language acquisition, which in turn facilitates social skill development.2–7 Initiating skills are strongly related to spoken language development, responding to JA (eg, following another person’s gaze to join their focus) predicts preschool children’s language outcome 8 years later, and a summary variable of all JA gesture use (both initiating and responding) also predicts better social outcomes.4–10 Even when spoken language is not specifically targeted, interventions that improve JA appear to facilitate language development.11,12 The effects of treatments aiming to increase JA have been assessed in a growing number of randomized controlled trials (RCTs).
In this review, we focus on RCT interventions that have aimed to improve JA in young children with ASD and provide an overview of results of research in the past 10 years. Second, we also summarize the outcomes from single-subject research design (SSRD) studies and a group experimental design study.
Defining social communication
Many would argue that all communication is inherently social, because by definition it involves at least two people engaging with one another with the aim of achieving mutual understanding.13 Indeed, in the literature on neurotypical development, communication that is social or not social is seldom differentiated. This is not the case for young children with ASD, where it is important to distinguish between communication used for a social reason (JA) versus communication to regulate another person’s behavior (requesting) because the former is impaired to the extent that it is considered a core deficit, while the latter is less affected.1,14,15 Although communication to regulate another’s behavior is to some extent social, because it involves a social partner, the underlying reason for the communication is not inherently motivated by a desire to share with others. Thus, in this review, only studies that targeted JA as an outcome were included. RCT studies that measured communication more generally without a clear differentiation of motivation as outlined above (eg, Hanen’s “More than Words” program) were excluded.16 Researchers have approached the study of JA in two ways. Some studies have examined JA as a context or state, with adult and child jointly attending to the same object for a period of time.17,18 For example, a parent and a child looking at a book together, with both drawing each other’s attention to the pictures by pointing and labeling, may be viewed as an ongoing dyadic state of JE. Other studies have measured JA gestures for sharing purposes (eg, showing and pointing) to define both responding (RJA) and initiating (IJA) behaviors. Thus, child responses to caregiver JA bids (eg, following an adult point with eye gaze) and children’s JA initiations (eg, holding up something for another person to see, or pointing at something themselves) are accounted for.
Methods
Search strategy
Six electronic databases (PsycINFO, Melvyl, PubMed, ERIC, Google Scholar, ASHA Journals) covering education, medicine, communication, and psychology were searched in September 2014. The search was restricted to materials published in peer-reviewed journals between January 2004 and September 2014. Keyword search terms were autism, intervention, and JA or JE. This search identified 324 studies for possible inclusion. Removal of duplicates yielded 167 manuscripts. Next, a review of titles and abstracts was conducted with a Level 1 Screening (autism, age, and JA intervention), excluding 43 original and 2 review articles whose references were examined, thus resulting in 122 full manuscripts to be reviewed. The Level 1 Screening (autism, age, and JA intervention) was then applied to the full manuscript because, at times, the abstract did not provide enough information for judgment. This yielded 56 manuscripts. The inclusion and exclusion criteria defined below were then applied to the full text, resulting in 28 articles that met all inclusion criteria. In all, there were 13 RCTs, 1 group experimental, and 14 SSRD articles (Figure 1).
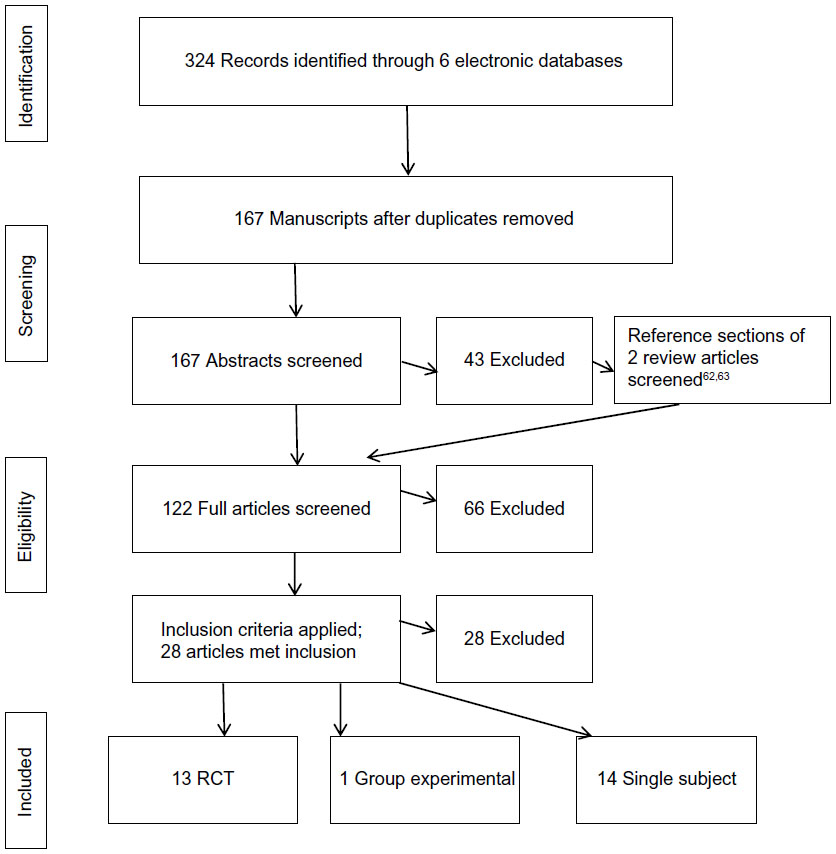 | Figure 1 Flow chart for eligibility for inclusion in study. |
Inclusion and exclusion criteria
A set of inclusion and exclusion criteria was applied to the manuscripts obtained from the search. Included studies had the following features:
- Used a quantitative, RCT design, group experimental design, or SSRD.
- Were published in the English language.
- Were published in a peer-reviewed journal between January 2004 to September 2014.
- Included participants between the ages of 1 year and 7 years diagnosed with an ASD or were at risk for an ASD.
- Examined an intervention for which JA or JE was an outcome. This excluded communication that was solely to request, protest, or regulate another’s behavior. It also excluded communication that was not clearly defined (eg, an outcome variable that combined requesting and JA gestures, interaction in which the function/nature of the interaction was not clearly described as JE).
- Included measurement of JA as a direct target. Studies were excluded if JA was measured as a collateral outcome.
Results
A total of 13 RCT studies were found based on these terms. Most were conducted in the USA, with one each from Norway, Belgium, and the UK. The number of participants across studies ranged from 15 to 152. Three studies used intervention methods with a developmental orientation and focused on caregiver-mediated methods. Other studies used combined developmental and behavioral approaches and delivered intervention via trained interventionists, caregivers, and teachers. Interventions ranged widely in density, with respect to the amount of intervention delivered weekly and the total duration of intervention. In addition, 14 more SSRD studies – most using a multiple baseline approach and one using a group experimental design – were also identified.
Review and discussion of RCT studies
In the 13 RCT interventions (refer to Table 1 for definitions of the outcome variables and Table 2 for study characteristics and findings), three developmental methods were tested, a Parent-Mediated Communication-Focused Treatment in Children with Autism (PACT), Focused Playtime Intervention (FPI), and Joint Attention-Mediated Learning (JAML).19–21 Of these, two were caregiver mediated and designed to increase parent responsiveness.19,21 The studies testing a combined developmental behavioral approach included Interpersonal Synchrony (IS), Reciprocal Imitation Training (RIT), and the Joint Attention and Symbolic Play/Engagement and Regulation Treatment (JASPER).22–24 Indeed, JASPER dominated the RCTs in the past 10 years; eight studies examined variations of JASPER treatment across multiple settings and delivery models (specialist, caregiver, and teacher). Table 2.
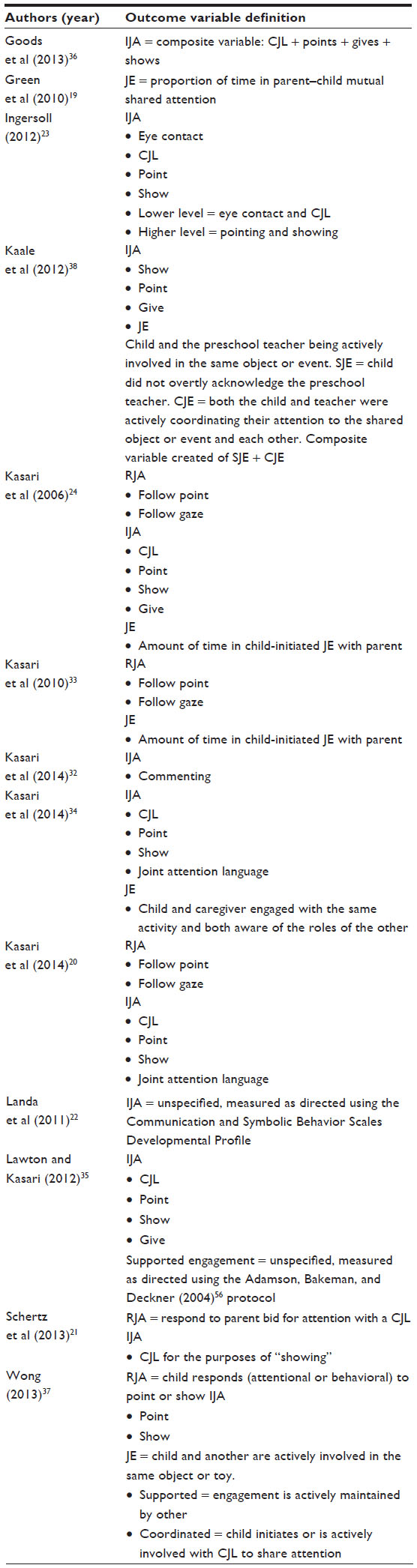 | Table 1 Definitions of IJA, RJA, and JE for the RCT outcome variables |
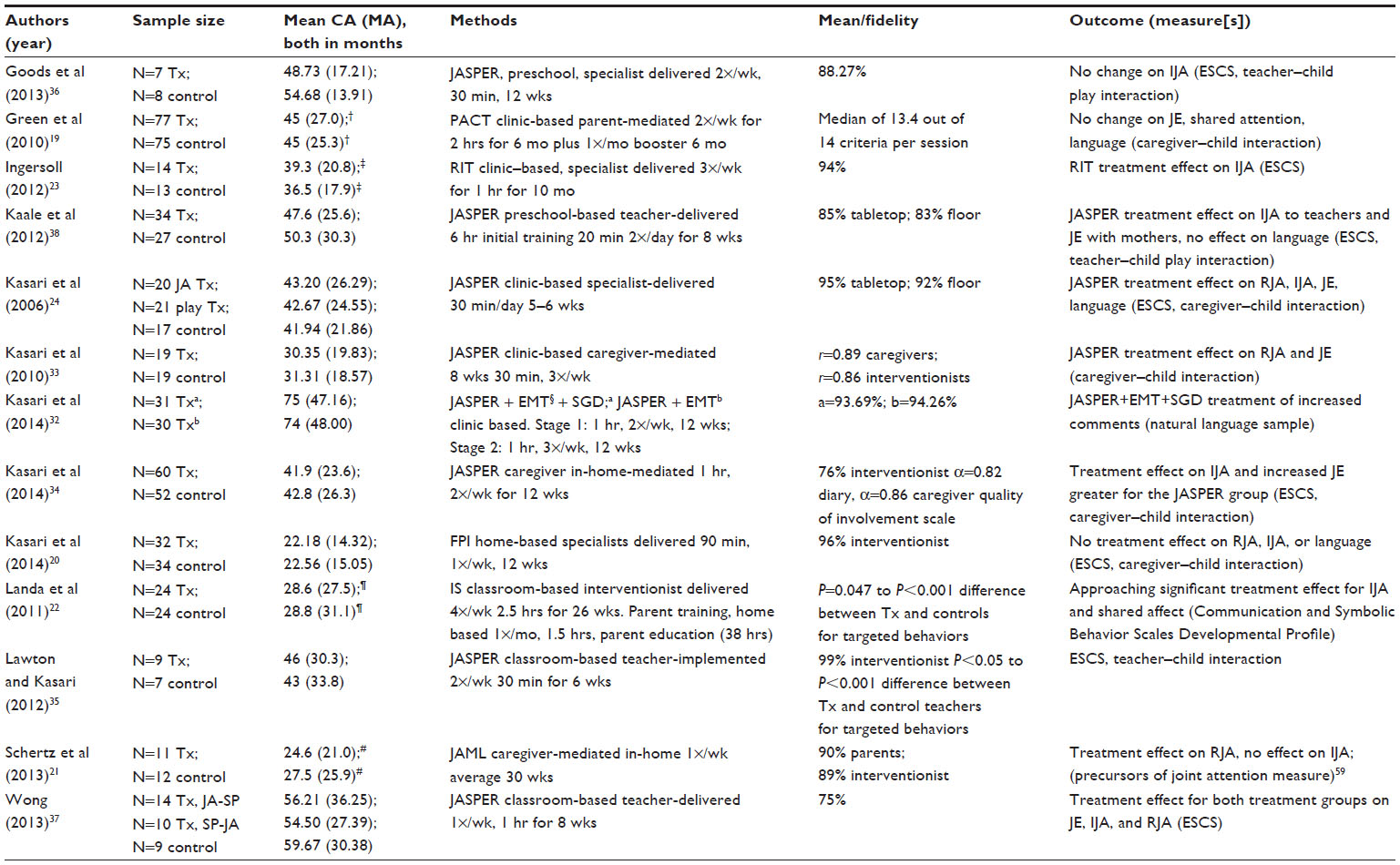 | Table 2 RCT study characteristics and findings on IJA, RJA, and JE |
Methods with a developmental orientation
As the need for effective early intervention continues to be a focus, policy and practice recommendations have called for more developmentally appropriate and systematically delivered interventions that can be easily carried out in the natural setting, can be integrated into everyday experiences, and are supportive of the parent–child relationship.25 Caregiver-mediated interventions are viewed as desirable because they are evidence based and parents can deliver the intervention throughout the day, thereby maximizing density. In 2002, Siller and Sigman26 showed in a prospective longitudinal study that early developmentally responsive parental behaviors predicted long-term language outcomes of children with ASD. Their study showed that parents who engaged with their child during play using responsive strategies had children who made larger subsequent gains in language abilities over the course of 10 years and 16 years than parents who were less responsive initially.
With language being a strongly desirable outcome and caregiver implementation a practical delivery model, three studies examined the effectiveness of responsive styles of parent interaction in a play context. These interventions supposed that a naturally responsive and sensitive style of caregiver interaction could be adapted to facilitate increased communication and social engagement in young children with ASD. In general, responsive interactions were those wherein a parent followed in and joined the child’s actions using contingent language and/or actions. The approach encouraged child choice and parents were to follow their child’s lead, join their focus, and build on the interaction in a nondemanding style.
Parent-mediated communication-focused treatment
Green et al19 tested a PACT strategy. The manualized treatment was organized according to normative prelinguistic and early language skill development. The aim of the intervention was to increase parent responsiveness and sensitivity to child communication and decrease mistimed parent responses. Strategies used to develop the child’s communication included action routines, familiar repetitive language, and pauses.
Individual sessions were delivered to parent–child dyads by six trained speech and language therapists, mostly in specialist centers. After an initial orientation meeting, families attended biweekly 2-hour clinic sessions for 6 months (total 18), followed by monthly booster sessions for 6 months. Between sessions, families were asked to do 30 minutes of daily home practice, and video feedback was provided on intervention strategies. The study achieved positive results in terms of increasing synchronous parental responses but did not affect child outcomes of social communicative responding, initiating, shared attention, or language.
Focused playtime intervention
FPI was developed as a systematic intervention specifically designed to increase parental responsiveness considering the evidence of long-term language gains.26,27 The primary goal of the following recently published RCT20 was to determine whether a developmentally informed, low-intensity parent-education intervention to increase parent responsiveness (FPI) would improve children’s JA and language skills both postintervention and after 1 year.
Caregivers and their 66 toddlers at high risk for ASD were randomized into the FPI treatment or a control group. Intervention strategies were organized into topics delivered in a specific sequence. Topics included understanding the child’s communication skills, how to create play routines, parent’s communication and language during play, the importance of coordinated attention between parent and child, recognizing the child’s attentional cues, strategies to support coordinated attention, responsiveness to the child’s bids for JA, and communicative gestures.
In the first half of each intervention session, the parent–child dyad engaged in play with the interventionist present. The interventionist also demonstrated strategies related to the targeted topic and provided feedback on parent use of strategies and their child’s responses. In the second half, the parent received education without the child being present. During this session, the interventionist elaborated on the targeted topic using video feedback, conventional teaching, a workbook, and weekly homework.
Although parental responsiveness improved, there were no treatment effects on child outcomes of RJA, IJA, or language both posttreatment and after 1 year.
Joint Attention-Mediated Learning
JAML is an interaction-based approach that directly and exclusively addresses the social functions of preverbal communication by targeting engagement at progressively complex levels within parent–child relationships. Schertz et al21 tested the effects of their JAML intervention on the acquisition of JA for toddlers with ASD.
The JAML intervention was structured with three developmentally sequenced phases. In the “Focusing on Faces” phase, the child was scaffolded to look often to the parent’s face. In the “Turn Taking” phase, the child and parent engaged in reciprocal repetitive play that acknowledged the other’s shared interest by accommodating the parent’s turn. Finally, toys were used to promote triadic engagement in the “Joint Attention” phase (both responding and initiating).
The intervention delivery was guided by five principles of mediated learning. It emphasized “learning how to learn” about social communication through the parent–child relationship instead of training the parent in specific strategies. The principles applied to both toddler and parent learning. For toddlers, parents used the principles to help their children 1) focus their attention on the objectives in a phase (eg, Turn Taking), 2) improve self-regulation, 3) develop confidence related to the phase goals, 4) recognize interaction cues that are socially important, and 5) interact more frequently in a variety of settings and with different people.
As parents applied mediation principles to promote their toddlers’ learning, intervention coordinators applied the same principles with parents in weekly home-based intervention sessions. The approach was intended to develop parents’ internalization of JAML’s aims so that they could apply the principles within parent–child interactions and daily activities.
Trained interventionists conducted at least 16 home-based intervention sessions with parents; however, if a child had not made sufficient progress in a phase, then sessions were added. There was considerable variability in the time to intervention completion, with a range of 4–12 months (average of 7 months). In each session, parents interacted with their toddlers for 10 minutes. The interaction was recorded and used to facilitate feedback focusing on the targeted phase and the principles of mediated learning. In the second part of the session, new material was introduced: either the next mediated-learning principle in the sequence or a new intervention phase if appropriate. Multiple teaching tools were used, including handouts, daily activity logs, video feedback, and video examples of other ASD toddlers and parents. Parents were expected to spend 30 minutes daily dedicated to face-to-face interaction, as well as integrating the content naturally in daily activities.
Follow-up visits occurred 4 and 8 weeks after intervention ended. The JAML intervention children showed significantly more responses to parents’ JA bids, with a large effect size that was maintained at follow-up. IJA generated a modest effect size but did not reach statistical significance. Although language was not directly targeted in the intervention, receptive language was significantly improved in the JAML group.
Summary
Three different developmentally-based interventions were used to target increased social communication in young children with autism. Two of the interventions, PACT and FPI, did not elicit treatment effects on social communication or language. The third intervention, JAML, did improve both children’s ability to respond to JA bids initiated by adults and the child’s receptive language. (Table 2).
It is notable that there were minimal treatment effects in two studies and one improved the RJA but not IJA. One explanation is that JA as a core deficit in autism may require much more direct teaching to facilitate change.20 While it is important to target parental responsiveness, parent change alone may not be enough to significantly affect areas of core deficit in the children. A second possibility is that some outcome targets of these studies were not yet observable in such developmentally young children.1 Although the children’s ages varied from <30 months of age in the JAML and FPI studies to 45 months of age in the PACT study, all of the children were developmentally around 2 years of age.
Specialist-delivered intervention also did not favor targeted outcomes; rather, it appeared that density of intervention may have been a salient factor. The JAML study delivered intervention once per week over 30 weeks. However, individual intervention sessions were added as needed to facilitate child progress, which may have been a salient strategy to facilitate change in skills. The FPI intervention occurred once per week over 12 weeks, and PACT was delivered every other week over 6 months in association with monthly booster sessions for the following 6 months. All three studies reported high levels of intervention fidelity.
Methods with a combined developmental and behavioral approach
Historically, clinicians and researchers have been polarized, adopting either a behavioral or a developmental approach. It is only in recent years that the unique strengths of both methods have been combined to utilize their respective contributions.
In the following studies, developmental methods were combined with a behavioral approach, offering the addition of a direct and highly systematic approach for teaching skills. Behavioral strategies include priming of skills, use of a prompt hierarchy to shape skills, reinforcement to increase motivation, repeated practice and targeting of successive smaller goals toward a larger goal, and ensuring generalization of skills. Behavioral strategies directly shape skills, provide dense practice, and account for learning differences that characterize many children with ASD, particularly with respect to decreased naturalistic learning. On the other hand, the developmental methods offer opportunity for child initiation and ideation, generalization to more natural learning environments, and account for attentional difficulties in that the adult follows in on the child’s attention and creates opportunities for learning within the child’s existing attention focus.
Interpersonal synchrony
Landa et al22 evaluated the impact of supplementing a comprehensive intervention with a curriculum targeting social synchronous behaviors in toddlers with ASD. Fifty toddlers were randomized to one of two 6-month interventions: IS or Non-IS.
The Assessment, Evaluation, and Programming System for Infants and Children curriculum was used for both groups.28 The treatment group received a supplementary curriculum with increased and systematically focused learning opportunities targeting JA, including RJA, IJA, and sharing positive affect. The instructional strategies included adult-directed behavioral instruction such as discrete trial training (DTT), behavioral strategies in the natural environment, and developmental routine-based interactions wherein interventionists followed the child’s lead and expanded on child language and behavior. The interventions provided identical intensity (10 hours per week in classroom), student-to-teacher ratio (5:3), home-based parent training (1.5 hours per month), and parent education (38 hours).
In this study, between-group differences for treatment effects of initiating JA and shared positive affect did not reach statistical significance but were trending in the direction of significance.
Reciprocal imitation training
Ingersoll23 (2012) used specialist-implemented RIT for 3 hours per week over 10 weeks and improved IJA in 14 children with autism. RIT teaches imitation within the context of social imitation using both behavioral and naturalistic strategies. Specific strategies used included modeling, contingent imitation of nonverbal and verbal behavior, and contingent language to describe the children’s actions. Treatment effects were maintained at a 3-month follow-up.
Joint attention and symbolic play/engagement and regulation treatment
JASPER is a manualized developmental/behavioral intervention. It was not explicitly named JASPER in the beginning stages; however, the foundation for the methods was established in the first 2006 RCT and evolved since then in a series of studies across multiple settings with different delivery models.24
Interventionist/specialist delivered
In an initial study, Kasari et al24 increased both RJA and IJA skills in young children with autism after specialist-delivered treatment. Although language and affect were not specifically targeted in the active treatment, follow-up assessments showed effects on positive affect within JA 6 months and 12 months after intervention and on targeted JA skills and expressive language at 1 year and 5 years after the end of treatment.11,12,29 This is notable as JA interventions rarely report on changes in the quality of children’s JA upon follow-up.
In this intervention, JA gestures were taught directly using developmental norms to determine initial individualized treatment objectives. Treatment combined discrete trial training (DTT) at a table with enhanced milieu teaching (EMT) on the floor. The principles of EMT included following the child’s lead, imitating the child, using contingent language, sitting close to the child and making eye contact, making environmental adjustments to engage the child, and developing play routines.30,31
The results suggested that using a combination of a behavioral and a developmental approach was effective in improving JA in young children with autism. Indeed, the combined approach lent itself to frequent practice and direct shaping of skills through the behavioral method on the one hand and ideation and generalization facilitated through the developmental milieu method on the other.
In a second interventionist-delivered intervention, Kasari et al32 tested the effect of a speech-generating device (SGD) to improve spontaneous communicative utterances in minimally verbal children with autism. The SGD was used to model a minimum of 50% of all spoken communication. The study used a sequential multiple assignment randomized trial (SMART) design to allow for individualization of dosage and timing of the intervention based on child response. The findings suggested that an intervention beginning with JASPER + EMT + SGD and intensification of that intervention in a second stage for children who were slow responders was successful in increasing commenting, which was a verbal expression of JA. This was in a short period of time in a relatively low-intensity treatment of 2–3 hours per week supplementing school-based education.
Caregiver mediated
Given the positive outcomes of specialist-delivered JASPER in the original studies, it became a question as to whether parents could improve their child’s JA using similar strategies.11 To make the JASPER content more accessible to parents, the core principles of the intervention were developed into modules. The modules were individualized to each dyad so that the beginning point was determined from the initial caregiver–child interaction session. Treatment included interventionist coaching of the caregiver while engaging in play routines. Coaching included direct instruction, modeling, guided practice, feedback, and review of handouts that summarized the main objectives of each module.
Caregivers implemented the intervention with a high degree of fidelity and helped their toddlers move from primarily object-focused engagement states to increased levels of JE and improved RJA. These improvements were maintained over a 1-year follow-up.33 Unlike in the specialist-delivered JASPER; however, IJA did not improve despite direct intervention. In the early JASPER studies, initiations did improve but the intervention was therapist mediated and delivered more densely as an everyday intervention.24 Also worth considering is that the children were younger in the caregiver study than in the original RCT; perhaps again, developmental readiness affected their ability to learn responding skills but not initiations.
In a second caregiver-mediated intervention, JASPER was used to coach low-resourced parents of children with ASD.34 All children improved in time spent in JE and IJA, with significantly greater improvement by the JASPER group. JE was maintained over a 3-month follow-up in the JASPER group, and IJA was maintained in both groups over time. Comparably, this study had a longer duration than the previous caregiver-mediated study, the children were older, and more time was spent with the interventionist; however, the intervention was less dense (two versus three times per week).
Teacher implemented
Because most young children with autism attend preschool, a further natural progression of using JASPER was to determine whether teachers in preschools could be successful in improving JA. Four classroom-based studies all demonstrated clear JASPER treatment effects. Lawton and Kasari35 published the first RCT of a teacher-implemented intervention for preschoolers with autism. This intervention was delivered at a lower dose than previous JASPER interventions and teachers implemented the treatment. Targeted strategies were presented to teachers in modules and again individual coaching was used. Modules included recognizing and responding to child IJA, methods for facilitating and maintaining JE, and allowing the child to initiate communication. The coaching protocol included elements such as correctly judging the level of support the dyad required, providing brief feedback about what strategies were working, and helping the teacher develop routines with the child.
Results showed that public preschool teachers successfully learned how to improve the frequency of IJA and JE. It is noteworthy not only that JASPER intervention improved such difficult-to-teach skills but also that child and teacher treatment effects were found during regularly occurring public preschool activities. A limitation is the lack of follow-up data to assess the long-term impact of the treatment’s effects. In contrast, a relatively brief and low-density intervention using JASPER for minimally verbal children (fewer than 10 spontaneous functional words) with ASD in a nonpublic preschool setting was not effective in improving generalized JA gestures.36
A third study involved 14 different classroom teachers using the JASPER principles but incorporating significantly greater variability in intervention delivery than used previously.37 The intervention adopted an individualized approach, wherein teachers could choose to implement activities for the whole class, in small groups, and/or in one-to-one individualized settings. They could also choose to implement the intervention strategies using a range of intervention methods and approaches. For example, in behaviorally-based classrooms using DTT, teachers received training on how to task analyze those skills, then target and integrate JA into their existing curricula. In other classrooms, such as those with children showing more advanced developmental abilities, teachers targeted JA during group instruction. In this case, the intervention focused more on curriculum content and less on adhering to a specific treatment approach. Results showed that teachers significantly improved their children’s JE, RJA, and IJA within a classroom setting.
Most recently, the efficacy of JASPER was replicated in a Norwegian study, wherein JASPER was delivered in addition to the mainstream preschool program by preschool teachers to children with ASD. Treatment effects showed improved IJA with teachers, which generalized to significantly longer duration of JE with their mothers, and at 1-year follow-up, similar to specialist-delivered treatment, preschool-based treatment appeared to produce small, but possibly clinically important, long-term changes in children’s initiation of JA with teachers.38,39 The treatment did not affect language or global ratings of social functioning and communication.
Summary
Overall, these studies22–24,32–38 suggest that a combination of behavioral and developmental methods is generally effective in improving JA. It seems to matter less which specific approach is used, although JASPER and RIT appear to be more effective. Rather, it may be that direct targeting of skills through behavioral methods such as modeling, shaping, and prompting, along with contingent responding to child attention and ideation, is what facilitates change.
Remarkably, JASPER appeared to be effective when delivered not only by clinicians but also by caregivers in homes and by teachers in preschools, emphasizing the validity of the intervention content. The generalization to natural environments without adverse effects on outcomes is extremely promising. Furthermore, JASPER was effective in the context of both general education and self-contained special education classrooms when delivered by teachers with different methodologies and the teachers benefited, as indicated by significant positive outcomes in their students.37 The exception in this group of studies was the lack of improvement in social communication in minimally verbal children using JASPER.36 Perhaps for minimally verbal preschoolers, we must revisit again the developmental readiness for JA skills at approximately 1 year or less expressive language age at entry.1 Further, the short duration and group intervention delivery (in contrast to longer, individual, direct instructional methods generally used for this population) may have affected the lack of improvement in this critical core deficit. This may be the case as shown in the individualized blended EMT + JASPER intervention.32 IS was another combined method that did not achieve clear change in JA skills despite a 6-month fairly dense intervention. In this study, it may be that treatments received by both groups were not clearly differentiated. Another possible variable affecting outcome may have been which specific IJA skills were targeted; however, this remains unclear as they were not specified.22 Evidence of high fidelity among the teachers across studies was extremely encouraging. It is notable that few studies have follow-up data probably due to the difficulty in conducting research in school settings and thus, maintenance of skills and longer-term outcomes remain an area for further investigation. Moreover, given the positive effects of RIT, it is hoped that further research with caregiver and teacher delivery models will be investigated.
Single-subject and quasi-experimental studies
Although RCTs to improve JA are the focus of this review, we include group design and SSRDs to provide a broader overview of the treatment research in this area.40–54 These studies are presented in summary format in Tables 3 and 4.
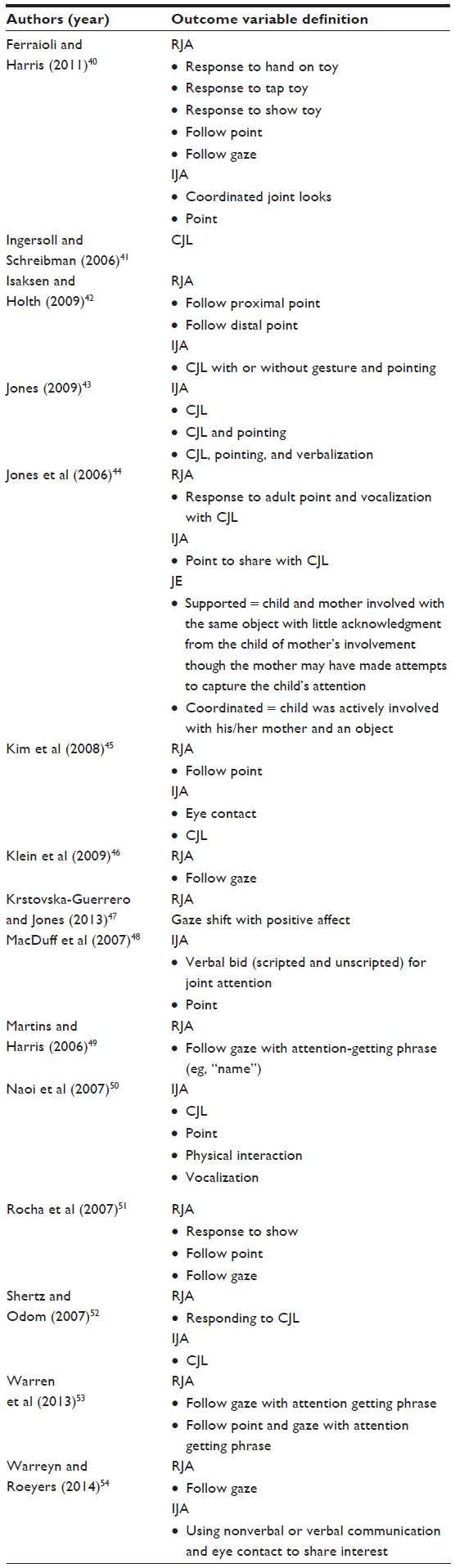 | Table 3 Definitions of IJA, RJA, and JE for the single-subject outcome variables |
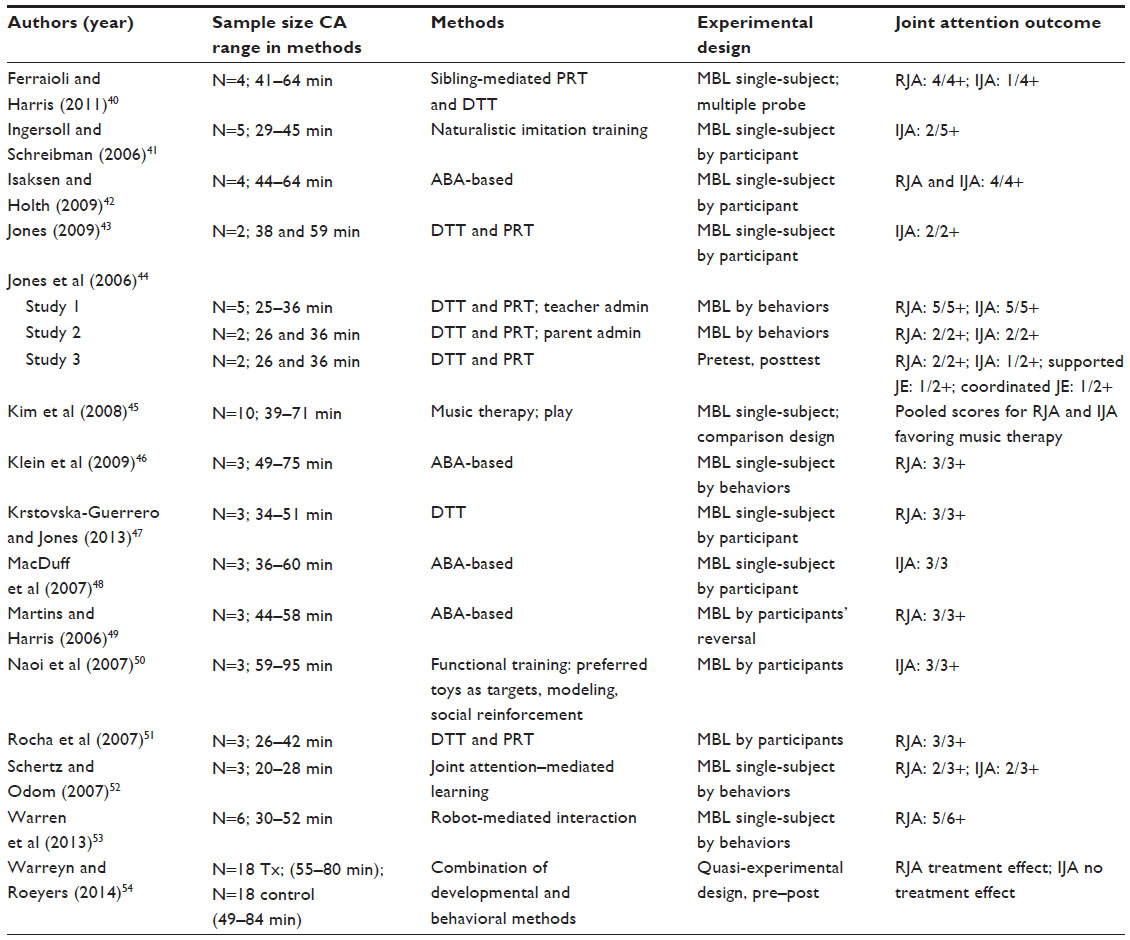 | Table 4 Single-subject study characteristics and findings |
The treatment research base becomes more than double when these smaller studies are included, a testament to the increased efforts in the past decade to experiment with different methods to improve JA. In sum, in quasi-experimental and SSRD studies, there has been success in teaching both RJA and IJA. Whereas none of the RCT studies used behavioral methods to increase JA, nearly all of the SSRD studies did. The majority of these interventions were clinician delivered, one was parent delivered, one was sibling mediated, and one was robot mediated. With a primarily behavioral approach, it is not surprising that with the exception of two studies, all focused on increasing specific skills rather than JA as a state. Most targeted either RJA or a combination of RJA and IJA. Only three studies targeted IJA only. In this group of studies with a stronger behavioral emphasis, use of shaping and skill approximation using less naturalistic methods was more evident. For example, one study taught child responding to an adult bid for JA (showing) by first teaching the child to respond to an adult hand on a toy, then respond to a tap on a toy, and then progressed to having the child respond to an adult showing a toy.40 While the methods were successful, the quality of child response does come into question. Of course, this pertains to all studies; however, regardless of the methods used, and to date, defining and measuring the quality of children’s JA after treatment has received little attention.
Except for Warreyn and Roeyers (2014)54 who used their own unique pre–post assessment to measure JA, the SSRDs charted behavioral observations of JA outcomes to demonstrate change. Whereas the RCT studies used standardized, accepted, and well-defined outcome measures of JA, the SSRD studies exhibited significant variability in what they measured and how they defined their outcomes (Table 3). For example, RJA gaze following was defined in one study as following a point and gaze with an attention-getting phrase.53 In another, it was defined as following a gaze shift with positive affect.47 Comparisons of treatment efficacy across studies is thus very difficult due to the differences in outcome definitions and differences in skill complexity. The methods used in some of the SSRDs to teach IJA also raise questions of validity with regard to the use of primary reinforcement as a consequence for JA initiations. This may be a means to an end in that the maintaining consequence is shaped over time from a nonsocial to a social consequence; however, without clearly establishing social attention as the function of IJA, it is difficult to say for certain that JA skills are being exhibited.
These comments are not intended to criticize behavioral methods used alone to teach JA as many studies demonstrate success but rather to highlight the need to pay close attention to details within each study to understand what was taught and the nature of the outcome achieved.
Conclusion
While many years of research evidence clearly established JA in ASD as a core deficit, it has only been within the past 10 years that empirical evidence has guided intervention. The outcomes of the studies reviewed generally demonstrate short-term improvements for targeted goals and, in some cases, also long-term benefits and other related improvements (language, affect). It is noteworthy that all 13 RTCs used direct observation and measurement of JA, with the vast majority using either the Early Social Communication Scales or video coding of caregiver–child or teacher–child interactions to capture JA as an engagement state, or a combination of both approaches.17,55,56 Regardless, all used standardized direct observation outcome measures, which reduced idiosyncrasy among outcome variables across studies and allowed for greater transparency in examining outcomes.57,58 One question relates to outcome difficulty. Could positive outcomes be related to earlier-developing or less-challenging skills? This does not appear to be the case as the majority of studies examined a similar range of skills from less to more challenging, defined by the same measurement protocols. In addition, closer inspection shows, eg, that JAML measured coordinated joint looks as an IJA outcome, a very early developing skill, yet did not find a treatment effect on IJA.21 In contrast, most JASPER studies measured a range of skills, including those considered to be at lower and higher levels.55
When examining the contents of the interventions, when placed within similar philosophies (eg, developmental vs combined), the concepts are somewhat similar. On the basis of this review, it seems that the likelihood and impact of effects are related more to the philosophy of approach (combined), dense but practical implementation, and the developmental considerations of the skills and abilities of the children involved. The findings do seem to indicate that direct, targeted instruction is needed to change skills in a meaningful manner and at least in the short term can be achieved by relatively brief interventions. This seems to bear out across several studies and also, interestingly, when one looks at interventions with different philosophies but similar content, such as caregiver-mediated FPI and JASPER.20,34 Furthermore, it appears that instruction on RJA will not necessarily increase IJA and vice versa. Thus, although RJA and IJA are both considered JA, they should be treated as separate instructional objectives. Further, choosing what to teach remains an interesting question. Children with autism do not follow typical developmental trajectories with regard to JA. As a start, research should further investigate the relationship between child characteristics and specific strategies, but many questions remain regarding the effective methods to significantly improve social communication in ASD.
One question relates to the interaction between method and strength of outcome. Given the large number of services in which children with ASD participate, how can a child gain these critical skills in an efficient and practical manner? This would require a number of targeted studies examining dosage. A second question relates to the potential to modify approaches that are currently being used as whole interventions and curricula (eg, pivotal response training, applied behavior analysis, and Denver model).31,59,60 Many of these approaches have instructional targets related to JA, but no RCTs have specifically measured social communication outcomes; moreover, developmental readiness remains a question. Third, a couple of studies reviewed in this article began to address the need for individualized and ongoing assessment and modification of intervention goals and duration to maximize progress, but this is an area that requires considerably more attention.21,32 Indeed, the field is trending away from one-size-fits all treatment for children with ASD.61 How to make modifications to the interventions given child characteristics and rate of progress from a manualized intervention remains a challenging but important area for further investigation. In addition, a clear purpose of early JA interventions is to improve related language skills for children with ASD as that relationship has been made very clear. Several RCTs did not demonstrate effect on language and many did not investigate language outcomes; this should remain at the forefront of JA literature not only to improve the quality of life for individuals with ASD but also to contribute to our understanding of how language develops. Related, further research should investigate continued maintenance of skills and also the long-term relationship between JA, language, and more distal outcomes such as social competence. Last, we recognize that this review is limited in that it only focused on studies that directly targeted JA as an outcome; however, a number of interesting RCTs have targeted treatment in other areas of development and found collateral improvements in JA.
Acknowledgments
The authors thank Joanne Kim for her assistance in edits to this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Paparella T, Stickles K, Freeman S, Kasari C. The emergence of joint attention and requesting skills in young children with autism. J Communication Disord. 2011;44:569–583. | |
Billstedt E, Gillberg IC, Gillberg C. Autism in adults: symptom patterns and early childhood predictors. Use of the DISCO in a community sample followed from childhood. J Child Psych Psych. 2011;48:1102–1110. | |
Rutter M. Diagnosis and definitions of childhood autism. J Aut Childhood Schiz. 1978;8:139–161. | |
Dawson G, Toth K, Abbott R, Osterling J, Munson J, Estes A. Early social attention impairments in autism: social orienting, joint attention, and attention to distress. Dev Psych. 2004;40:271–283. | |
Mundy P, Sigman M, Kasari C. A longitudinal study of joint attention and language development in autistic children. J Autism Dev Disord. 1990;20:115–128. | |
Paul R, Chawarska K, Cicchetti D, Volkmar F. Language outcomes in toddlers with ASD: a 2 year follow up. Aut Res. 2008;1:97–107. | |
Paul R, Campbell D, Gilbert K, Tsiouri I. Comparing spoken language treatments for minimally verbal preschoolers with autism spectrum disorders. J Autism Dev Disord. 2013;43:418–431. | |
Sigman M, Ruskin E. Continuity and change in the social competence of children with autism, Down syndrome, and developmental delays. Monographs Soc for Res Child Dev. 1999;64:1–114. | |
Charman T, Taylor E, Drew A, Cockerill H, Brown J, Baird G. Outcome at 7 years of children diagnosed with autism at age 2: predictive validity of assessments conducted at 2 and 3 years of age and pattern of symptom change over time. J Child Psych Psych. 2005;46:500–513. | |
Watt N, Wetherby A, Shumway S. Prelinguistic predictors of language outcome at 3 years of age. J Speech Lang Hearing Res. 2006;49:1224–1237. | |
Kasari C, Paparella T, Freeman S, Jahromi LB. Language outcome in autism: randomized comparison of joint attention and play interventions. J Consulting Clin Psych. 2008;76:125–137. | |
Kasari C, Gulsrud A, Freeman S, Paparella T, Helleman G. Longitudinal follow-up of children with autism on joint attention and play. J Am Acad Child Adol Psych. 2012;51:487–495. | |
Tomasello M. Origins of Human Communication. Cambridge: MIT Press; 2008:57–108. | |
Shumway S, Wetherby A. Communicative acts of children with autism spectrum disorders in the second year of life. J Speech Lang Hearing Res. 2009;52:1139–1156. | |
Volkmar F, Lord C, Bailey A, Schultz R, Klin A. Autism and pervasive developmental disorders. J Child Psych Psych. 2004;45:135–170. | |
Carter AS, Messinger DS, Stone WL, Celimli S, Nahmias AS, Yoder P. A randomized controlled trial of ‘Hanen’s ‘More Than Words’ in toddlers with early autism symptoms. J Child Psych Psych. 2011;52:741–752. | |
Bakeman R, Adamson LB. Coordinating attention to people and objects in mother-infant and peer-infant interaction. Child Dev. 1984;55:1278–1289. | |
Tomasello M, Farrar MJ. Joint attention and early language. Child Dev. 1986;47:1454–1463. | |
Green J, Charman T, McConachie H, PACT Consortium, et al. Parent-mediated communication-focused treatment in children with autism (PACT): a randomized controlled trial. Lancet. 2010;375:2152–2160. | |
Kasari C, Siller M, Huynh LN, et al. Randomized controlled trial of parental responsiveness intervention for toddlers at high risk for autism. Infant Beh Dev. 2014;37:711–721. | |
Schertz HH, Odom SL, Baggett KM, Sideris JH. Effects of joint attention mediated learning for toddlers with autism spectrum disorders: an initial randomized controlled study. Early Child Res Quarterly. 2013;28:249–258. | |
Landa RJ, Holman KC, O’Neill AH, Stuart EA. Intervention targeting development of socially synchronous engagement in toddlers with autism spectrum disorder: a randomized controlled trial. J Child Psych Psych. 2011;52:13–21. | |
Ingersoll B. Brief report: effect of a focused imitation intervention on social functioning in children with autism. J Autism Dev Disord. 2012;42:1768–1773. | |
Kasari C, Freeman S, Paparella T. Joint attention and symbolic play in young children with autism: a randomized controlled intervention study. J Child Psych Psych. 2006;47:611–620. | |
Bruder MB. Early childhood intervention: a promise to children and families for their future. Except Child. 2010;76:339–355. | |
Siller M, Sigman M. The behaviors of parents of children with autism predict the subsequent development of their child’s communication. J Autism Dev Disord. 2002;32:77–89. | |
Siller M, Hutman T, Sigman M. A parent mediated intervention to increase responsive parental behaviors and child communication in children with ASD: a randomized clinical trial. J Autism Dev Disord. 2013;43:540–555. | |
Bricker D. Assessment, Evaluation and Programming System for Infants and Children. Birth to Three Years. 2nd ed. Baltimore: Brookes Publishing Co; 2002. | |
Lawton K, Kasari C. Brief report: longitudinal improvements in the quality of joint attention in preschool children with autism. J Autism Dev Disord. 2012;42:307–312. | |
Warren SF, Kaiser AP. Generalization of treatment effects by young language-delayed children; a longitudinal analysis. J Speech Hearing Disord. 1986;51:239–251. | |
Koegel RL, Koegel LK. Teaching Children With Autism: Strategies For Initiating Positive Interactions And Improving Learning Opportunities. Baltimore: Brookes Publishing Co; 1995. | |
Kasari C, Kaiser A, Goods K, et al. Communication interventions for minimally verbal children with autism: a sequential multiple assignment randomized trial. J Am Acad Child Adoles Psych. 2014;53:635–646. | |
Kasari C, Gulsrud AC, Wong C, Kwon S, Locke J. Randomized controlled caregiver mediated joint engagement intervention for toddlers with autism. J Autism Dev Disord. 2010;40:1045–1056. | |
Kasari C, Lawton K, Shih W, et al. Caregiver-mediated intervention for low-resourced preschoolers with autism: an RCT. Pediatrics. 2014;134:72–79. | |
Lawton K, Kasari C. Teacher implemented joint attention intervention: pilot randomized controlled study for preschoolers with autism. J Consult Clin Psych. 2012;80:68–693. | |
Goods KS, Ishijima E, Chang Y, Kasari C. Preschool based JASPER intervention in minimally verbal children with autism: pilot RCT. J Autism Dev Disord. 2013;43:1050–1056. | |
Wong C. A play and joint attention intervention for teachers of young children with autism: a randomized controlled pilot study. Autism. 2013;17:340–357. | |
Kaale A, Smith L, Sponheim E. A randomized controlled trial of preschool-based joint attention intervention for children with autism. J Child Psych Psych. 2012;53:97–105. | |
Kaale A, Fagerland MW, Martinsen EW, Smith L. Preschool-based social communication treatment for children with autism: 12-month follow-up of a randomized trial. J Am Acad Child Adol Psych. 2014;53:134–188. | |
Ferraioli SJ, Harris SL. Teaching joint attention to children with autism through a sibling mediated behavioral intervention. Beh Interv. 2011;26:261–281. | |
Ingersoll B, Schreibman L. Teaching reciprocal imitation skills to young children with autism using a naturalistic behavioral approach: effects on language, pretend play and joint attention. J Autism Dev Disord. 2006;36:487–505. | |
Isaksen J, Holth P. An operant approach to teaching joint attention skills to children with autism. Beh Interv. 2009;24:215–236. | |
Jones EA. Establishing response and stimulus classes for initiating joint attention in children with autism. Res Autism Spectrum Disord. 2009;3:375–389. | |
Jones EA, Carr EG, Feeley KM. Multiple effects of joint attention intervention for children with autism. Beh Modification. 2006;30:782–834. | |
Kim J, Wigram T, Gold C. The effects of improvisational music therapy on joint attention behaviors in autistic children: a randomized controlled study. J Autism Dev Disord. 2008;38:1758–1766. | |
Klein JL, MacDonald RPF, Vaillancourt G, Ahearn WH, Dube WV. Teaching discrimination of adult gaze direction to children with autism. Res Autism Spectrum Disord. 2009;3:42–49. | |
Krstovska-Guerrero I, Jones EA. Joint attention in autism: teaching smiling coordinated with gaze to respond to joint attention bids. Res Autism Spectrum Disord. 2013;7:93–108. | |
MacDuff JL, Ledo R, McClannahan LE, Krantz PJ. Using scripts and script-fading procedures to promote bids for joint attention by young children with autism. Res Autism Spectrum Disord. 2007;1:281–290. | |
Martins M, Harris SL. Teaching children with autism to respond to joint attention initiations. Child Fam Beh Therapy. 2006;28:51–68. | |
Naoi N, Tsuchiya R, Yamamoto J, Nakamura K. Functional training for initiating joint attention in children with autism. Res Dev Disablities. 2007;29:595–609. | |
Rocha ML, Schreibman L, Stahmer AC. Effectiveness of training parents to teach joint attention in children with autism. J Early Interv. 2007;29:154–172. | |
Schertz HH, Odom SL. Promoting joint attention in toddlers with autism: a parent mediated developmental model. J Autism Dev Disord. 2007;37:1562–1575. | |
Warren ZE, Zheng Z, Swanson AR, et al. Can robotic interaction improve joint attention skills? J Autism Dev Disord. 2013. Available from: http://dx.doi.org/10.1007/s10803-013-1918-4. Accessed February 2, 2015. | |
Warreyn P, Roeyers H. See what I see, do as I do: promoting joint attention and imitation in preschoolers with autism spectrum disorder. Autism. 2014;18:658–671. | |
Mundy P, Sigman MD, Ungerer J. Defining the social deficits of autism: the contribution of non-verbal communication measures. J Child Psych Psych. 1986;27:657–699. | |
Adamson LB, Bakeman R, Deckner DF. The development of symbol-infused joint engagement. Child Dev. 2004;75:1171–1187. | |
Wetherby AM, Prizant BM. CSBS DP Manual: Communication and Symbolic Behavior Scales Developmental Profile. Baltimore: Paul H Brookes; 2002. | |
Yoder P, Symons FJ. Observational Measurement of Behavior. New York: Springer; 2010. | |
Leaf R, McEachin J. A Work in Progress: Behavioral Management Strategies and a Curriculum for Intensive Behavioral Treatment of Autism. New York: DRL Publishing; 1999. | |
Smith M, Rogers S, Dawson G. The early start Denver model: a comprehensive early intervention approach for toddlers with autism. In: Handleman JS, Harris SL, editors. Preschool Education Programs for Children with Autism. 3rd ed. Austin, TX: Pro-Ed Corporation, Inc.; 2008:65–101. | |
Sherr MR, Schreibman L. Individual behavioral profiles and predictors of treatment effectiveness for children with autism. J Consult Clin Psych. 2005;73:525–538. | |
Meindl JN, Cannella-Malone HI. Initiating and responding to joint attention bids in children with autism: a review of the literature. Res Dev Disablities. 2011;32:1441–1454. | |
White PJ, O’Reilly MO, Streusand W, et al. Best practices for teaching joint attention: a systematic review of the intervention literature. Res Aut Spectrum Disorders. 2011;5:1283–1295. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.