Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Methods and Effectiveness of Communication Between Hospital Allied Health and Primary Care Practitioners: A Systematic Narrative Review
Authors Sheehan J, Laver K, Bhopti A, Rahja M ![]() , Usherwood T, Clemson L, Lannin NA
, Usherwood T, Clemson L, Lannin NA ![]()
Received 9 December 2020
Accepted for publication 14 January 2021
Published 22 February 2021 Volume 2021:14 Pages 493—511
DOI https://doi.org/10.2147/JMDH.S295549
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jacinta Sheehan,1 Kate Laver,2 Anoo Bhopti,1 Miia Rahja,2 Tim Usherwood,3,4 Lindy Clemson,5 Natasha A Lannin1,6,7
1Department of Occupational Therapy, Social Work and Social Policy, School of Allied Health, La Trobe University, Melbourne, Australia; 2Department of Rehabilitation, Aged and Extended Care, Flinders University, Adelaide, Australia; 3Westmead Clinical School, Faculty of Medicine and Health, The University of Sydney, Sydney, Australia; 4The George Institute for Global Health, Sydney, Australia; 5School of Health Sciences, Faculty of Medicine & Health, The University of Sydney, Sydney, Australia; 6Department of Neurosciences, Central Clinical School, Monash University, Melbourne, Australia; 7Alfred Health (Allied Health), Melbourne, Australia
Correspondence: Natasha A Lannin
Department of Neurosciences, Central Clinical School, Monash University, Level 6, 99 Commercial Road, Melbourne, VIC, 3004, Australia
Tel +61 3 9903 0304
Email [email protected]
Background: There is a compelling rationale that effective communication between hospital allied health and primary care practitioners may improve the quality and continuity of patient care. It is not known which methods of communication to use, nor how effectively they facilitate the transition of care when a patient is discharged home from hospital. Our systematic review aims to investigate the methods and effectiveness of communication between hospital allied health and primary care practitioners.
Methods: Systematic review of quantitative and qualitative studies with narrative synthesis. Medline, CINAHL, EMBASE, PsycInfo and Proquest Nursing and Allied Health Sources were searched from January 2003 until January 2020 for studies that examined hospital-based allied health professionals communicating with community-based primary care practitioners. Risk of bias in the different study designs was appraised using recognized tools and a content analysis conducted of the methodologies used.
Results: From the located 12,281 papers (duplicates removed), 24 studies met the inclusion criteria with hospital allied health communicating in some form with primary care practitioners. While none of the included studies specifically investigated the methods or effectiveness of communication between hospital allied health and primary care practitioners, 12 of the 24 studies described processes that addressed components of their discharge communication. Four enablers to effective communication between hospital allied health and primary care practitioners were identified: multidisciplinary care plans, patient and caregiver involvement, health information technology and a designated person for follow up/care management.
Conclusion: There is currently no “gold standard” method or measure of communication between hospital allied health and primary care practitioners. There is an urgent need to develop and evaluate multidisciplinary communication with enhanced information technologies to improve collaboration across care settings and facilitate the continuity of integrated people-centered care.
Keywords: multidisciplinary, collaboration, discharge plan, continuity of care
Introduction
Discharge planning is a routine feature of healthcare, with a goal of improving the coordination of services following discharge from hospital.1 Discharge communication provides a vital link between hospitals and primary care and is an important determinant of positive patient outcomes following hospitalization,2 helping to facilitate seamless transitions of care between healthcare providers. Ineffective communication and information transfer, particularly during transitions of care,3 can have substantial implications for patient safety and continuity of care,4 patient and healthcare provider comprehension and satisfaction,2 as well as resource use.5
Despite the quality and economic imperatives to improve discharge planning1 and facilitate transitions of care,5 no single intervention has consistently demonstrated a reduction in re-hospitalization when implemented alone.6 The World Health Organization set global priorities in 2018 to promote integrated people-centered health services through collaboration and integration across sectors, settings, providers and users,7 yet coordination and timely transfer of information remain great challenges to optimized outcomes during transitions of care.8 According to the WHO, people-centered care adopts the perspectives of individuals, caregivers, families and communities relative to the comprehensive needs and social preferences of people, rather than individual diseases.7 A person-centered (or patient-centered) approach is less encompassing but still allows the person to be seen as a whole,9 with needs and goals derived from their own social determinants of health.7 Such an approach should allow patients to share their health information at the appropriate time with the right person.10
The patient is often the only constant when healthcare teams change during transitions of care,11 yet differences in patient attitude12 and patient ability can compromise the sharing of their health information.13 Mixed evaluations to date14 and persistent problems with data interoperability means that personal health records are not yet commonplace.15 Health information technology (IT) developments have the potential to improve communication16 and collaboration17 at the time of discharge. Yet despite the increased adoption of health IT, there is very little research that evaluates the effectiveness of these information and communication systems.10 Furthermore, evidence of system incompatibility and security issues11 suggest that health IT solutions do not yet support sufficiently detailed or timely communication to or from hospitals to enable primary care practitioners to coordinate patient care effectively.18 Many gaps in the system remain, and one-way discharge summaries from hospital medical practitioners to primary care practitioners continue to be the mainstay of discharge communication, even when multidisciplinary teams are internationally recognized as the preferred method of healthcare delivery.19
Multidisciplinary teams are an integral component of improved health outcomes and collaboration between people, professions, systems and settings.20 Within the multidisciplinary team, allied health professionals provide specialized patient support and contribute important information regarding patients’ function, social situation, recovery goals and discharge needs in addition to nursing and medical care.21 Variability in the way discharge information is transferred2 suggests processes are not standardized and anecdotally such information rarely encompasses the allied health view. The multidisciplinary team should provide the necessary diversity for collaborative discharge care planning, yet it is not known if hospital allied health perspectives are sufficiently represented nor how well they are communicated to primary care practitioners.1
Discharge communication remains a recognized problem area in spite of the international research22,23 and regulatory attention it receives.24 In the most recent review of 30 trials of discharge planning,1 none reported on the quality of communication. Effective communication is essential for multidisciplinary collaboration within and between healthcare settings is, thus a key indicator of quality of care, yet it has not been systematically reviewed and synthesized. There is a particular gap in the knowledge base regarding communication between hospital allied health and primary care practitioners. Therefore, this systematic review sought to answer the following research questions:
- What are the effective methods and/or models of communication between hospital allied health and primary care practitioners?
- What are the enablers and barriers to effective communication between hospital allied health and primary care practitioners?
For the purpose of the review, the “3C Collaboration Model”25 is used to define “communication” as the exchange of information to generate commitments that are then managed by “coordination” so that individual care activities interact through shared spaces to work “cooperatively” to ensure the success of the overall care process. These three components work together to comprise healthcare collaboration.17
Method
The protocol for this review was developed and prospectively registered with PROSPERO International Prospective Register of Systematic Reviews [PROSPERO CRD42019120410]. Using a systematic review process, the search was performed to identify both quantitative and qualitative studies published in English between January 2003 and January 2020. The “SPIDER” (Sample, Phenomenon of Interest, Design, Evaluation, Research Type) tool26 was used to define the inclusion and exclusion criteria to facilitate the identification and selection of studies in this review.
Sample
Only studies with mention of communication between hospital-based allied health professionals (including occupational therapists, physiotherapists, dietitians, speech and language pathologists, psychologists, social workers and case managers) and community-based primary care practitioners (including primary care nurse practitioners, primary care practitioners, geriatricians and general practitioners) working with adults were included. Papers that only examined forms of communication between pharmacists and medical practitioners were excluded to allow a review of issues beyond medication. Papers where healthcare professionals worked only in mental health or substance abuse settings were also excluded as their transitional care commonly involves the same healthcare teams (as opposed to the transfer of care from one team to another). Pediatric samples were similarly excluded.
Phenomenon of Interest
The review was not restricted by communication method, and thus any type of communication was included (including written documentation, such as discharge summaries/letters/reports, interim reports; verbal communications, such as handovers, telephone calls; electronic communications such as emails, telehealth, videoconferencing; and face-to-face communications such as case conferences and team meetings). It was essential that communication was between hospital allied health professionals and primary care practitioners.
Design
We excluded protocols, abstracts, meeting summaries, theses, letters, editorials, opinions and conference papers. Qualitative research without thematic analysis was also excluded.
Evaluation
Since the review aimed to identify, analyze and synthesize the literature relating to all forms of communication between hospital allied health and primary care practitioners, we considered any types of outcomes reported in the studies.
Research type
There were no restrictions of research type; qualitative, quantitative and mixed method were included, provided publications met the design inclusion criteria.
Identification and Selection of Studies
The search was conducted in the following databases: MEDLINE, PsycInfo, EMBASE, CINAHL and Proquest Nursing and Allied Health Source. To identify studies relating to the communication between hospital allied health and primary care practitioners, the key search terms included: “communication”, “interaction”, “collaboration” “allied health”, “primary care” and “general practice” [full search strategy available as Additional File 1]. We excluded studies published prior to 2003 to reflect the more recently evolved methods and models of communication within healthcare, including electronic discharge summaries. One author [JS] conducted the searches. Reference lists of included studies were also screened by one author [JS] to identify relevant studies, and authors were contacted for further information as required. The search results from all databases were merged and duplicate articles removed using EndNote software. The Covidence platform was used for screening and eligibility assessment of the retrieved citations. The citations from the search, after excluding duplicates using EndNote, were uploaded into Covidence by one author [JS]. Two authors independently assessed all retrieved citations meeting the inclusion criteria on the basis of title and abstract [involved authors JS, NAL, KL, AS]. Potentially eligible studies were then reviewed in full text independently by two authors [involved authors JS, MR, KL] and a third author was consulted in cases of disagreement [involved authors NAL, KL].
Data Extraction
A standardized data extraction form based on the SPIDER tool26 was developed to collate the sample, phenomenon of interest, design, evaluation and research type of the included studies. One author [JS] extracted all data, with an independent review from a second author [MR]. Extraction tool available on request.
Data Synthesis
A narrative synthesis strategy was then used to organize, summarize and present the data, based on Guidance on the Conduct of Narrative Synthesis in Systematic Reviews.27 This structured process thematically summarized studies based on Berlo’s Model of Communication,28 which categorized findings where possible into components of communication by “sender/source” and/or “receiver” and/or “message/channel”. As the included studies were diverse, this initial synthesis allowed a breakdown of the varied and complex characteristics of healthcare communication. Following this classification, one author [JS] used an inductive approach to thematic analysis,29 coding the studies line-by-line to elucidate common patterns of meaning and areas of potential interest.30 Data were coded by collating in columns, colors and concepts to identify potential themes, which were then reviewed across the full data set to map and further refine the specifics of each prevalent theme. Generated themes were then tabulated in word documents relative to the research questions to determine the effective methods and/or models of communication, as well as the barriers and enablers to effective communication, between hospital allied health and primary care practitioners. To further contribute to thematic analysis, full texts of included studies were uploaded to NVivo 12.2 software program,31 enabling identification of word frequency and word mapping for further data-driven exploration of conceptual relationships.
Quality Appraisal
Given the heterogeneity of the included study designs, studies were appraised for reporting quality using the most appropriate tool for their design. Specifically, we used the Joanna Briggs Institute Critical Appraisal Checklist for Qualitative Studies,32 the McMaster Critical Review Form for Quantitative Studies33 and the Mixed Methods Appraisal Tool34 to assess the risk of bias in qualitative, quantitative and mixed-method designs, respectively. Acceptable quality was pre-defined as meeting ≥50% of applicable criteria.
Results
A total of 24 studies were included in this systematic review. Of these studies, 13 were qualitative, seven were quantitative and four used mixed-method designs. Studies were conducted in the United States (n=9, 38%), Australia (n=5, 21%), Sweden (n=3, 13%), The Netherlands (n=2, 8%), the United Kingdom (n=2, 8%), Canada (n=1, 4%), New Zealand (n=1, 4%) and Norway (n=1, 4%). Health professionals in these studies included nurses, nurse practitioners, doctors, medical students, occupational therapists, dieticians, physiotherapists, speech and language pathologists, social workers and case managers. Table 1 outlines the included study characteristics; Figure 1 presents the study PRISMA flow diagram.35
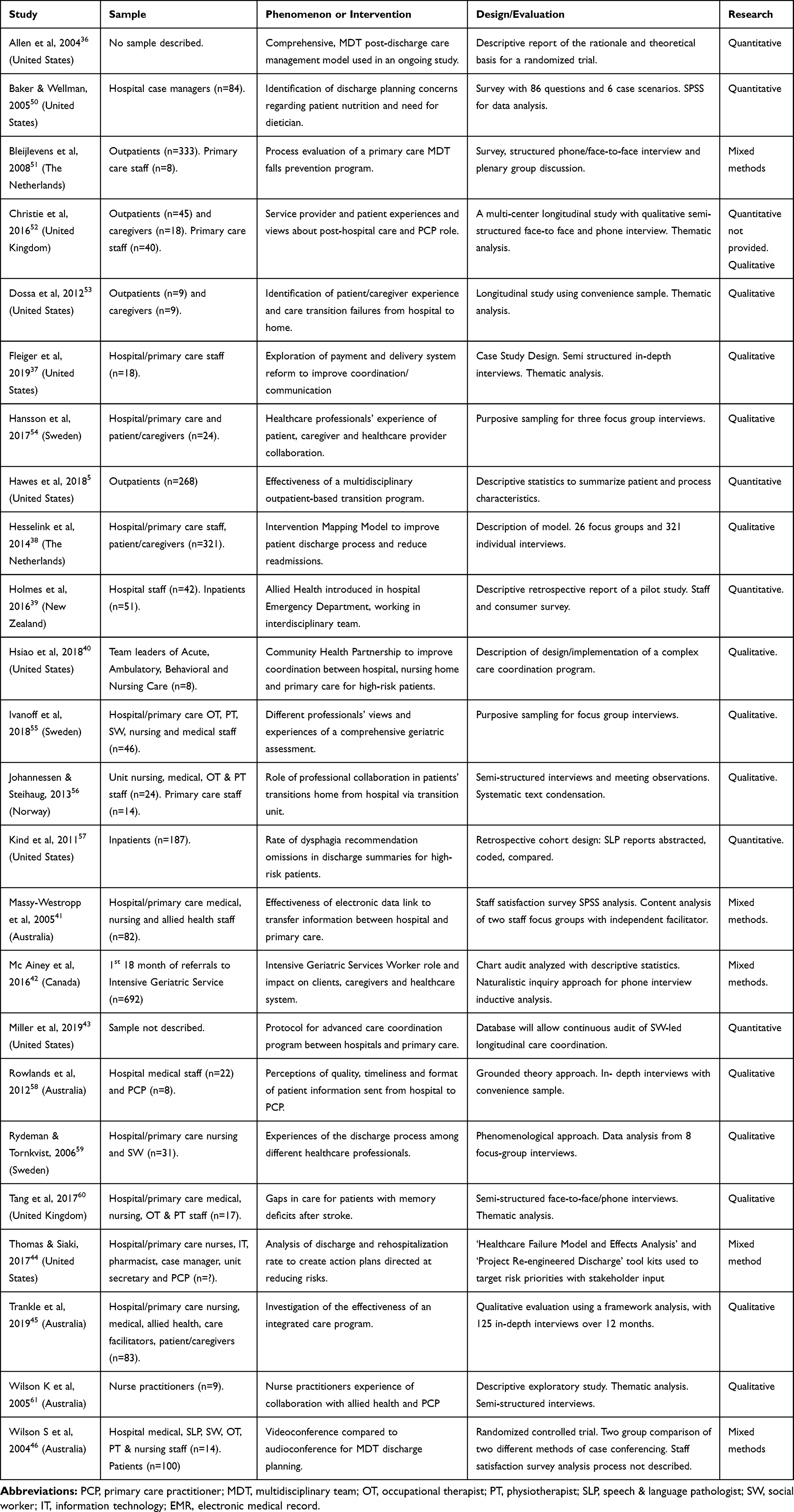 |
Table 1 Summary of Included Studies Using SPIDER Tool Categories |
 |
Figure 1 PRISMA flow diagram. Notes:PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons. |
Overall study quality was rated as acceptable across all appraisal checklists, with all relevant studies met at least minimal standards of adequacy in accordance with their respective quality appraisal tools. The summary of the results of quality appraisals for qualitative, quantitative and mixed-method studies are presented in Table 2–4, respectively. Findings were summarized to address the two research questions separately and narratively synthesized to develop the themes.
 |
Table 2 Summary of Quality of Qualitative Studies Using JBI Critical Appraisal Checklist for Qualitative Research |
 |
Table 3 Summary of Quality of Quantitative Studies Using McMaster Critical Review Form – Quantitative Studies |
 |
Table 4 Summary of Quality of Mixed Methods Studies Using Mixed Method Appraisal Tool (MMAT) Version 2018 |
The characteristics of the different communication methods for each study are categorized according to Berlo’s Model of Communication28 in Table 5, highlighting the roles and processes of different healthcare professions, healthcare teams and healthcare settings. Clear categorization was not possible where study samples included both hospital-based and community-based healthcare professionals but generally, hospitals were the senders or source of discharge communication to primary care practitioners, the intended receivers of patient information, using various messages and/or channels.
 | 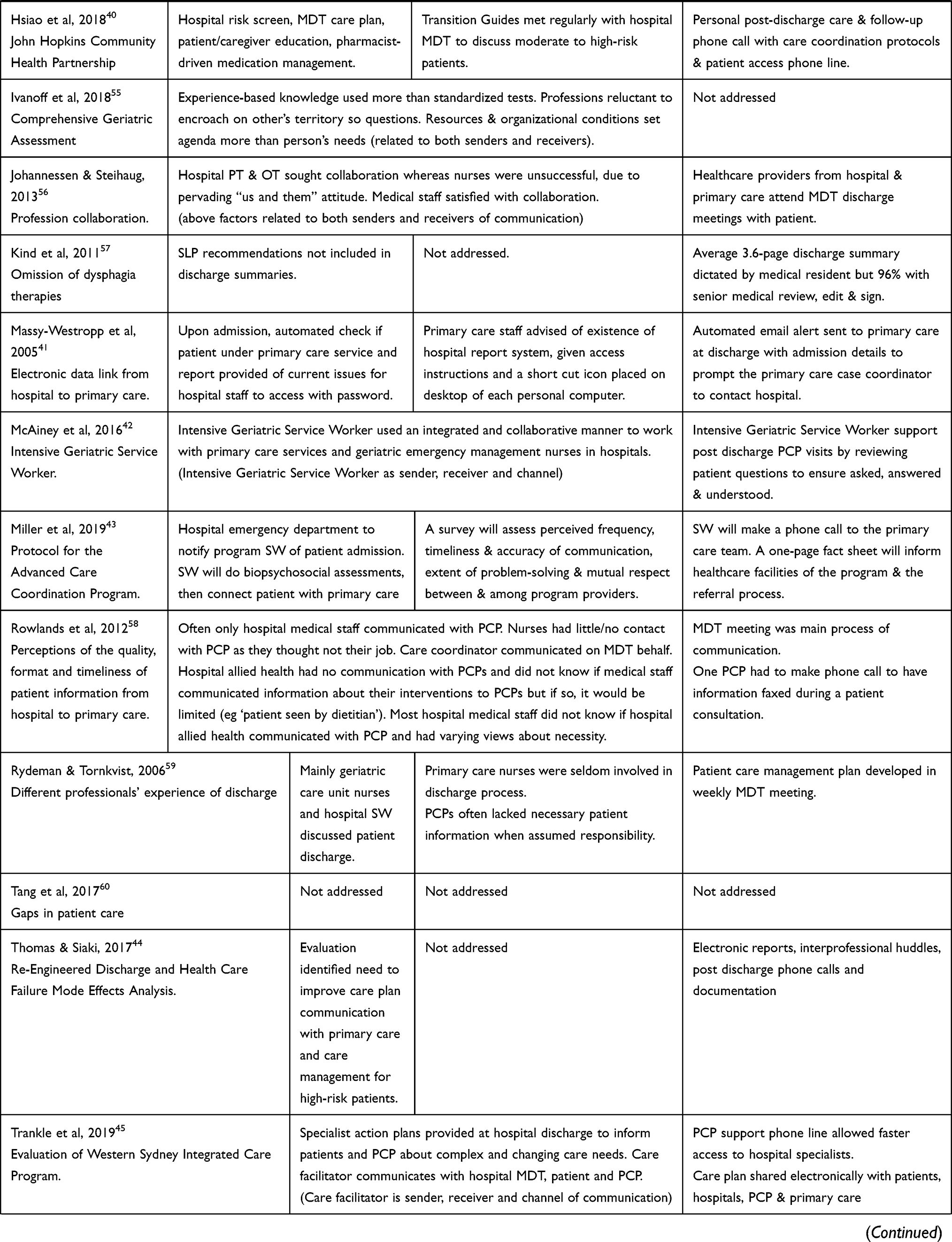 |  |
Table 5 Categorization of Studies Based on Berlo’s Model of Communication |
Effective Methods and/or Models of Communication Between Hospital Allied Health and Primary Care Practitioners
None of the included studies specifically investigated the methods of communication or evaluated the effectiveness of communication between hospital allied health and primary care practitioners. However, 12 of the 24 studies did describe programs or processes that indirectly addressed components of discharge communication between hospital allied health and primary care practitioners.5,36–46 Narrative synthesis of each study included exploration of these 12 interventions within the context of their relationship to some guiding theoretical models of care, namely, the chronic care model,47 the collaborative care model48 and the integrated care model.49 The relevance of the theoretical underpinnings of each model of care will be briefly discussed in relation to evolving healthcare practice, based on our analyses of these 12 interventions from the included studies.
Chronic Care Model
A descriptive paper by Allen et al in 2004 described the theoretical basis for a randomized trial of a comprehensive post-discharge care management program.36 The report included details of a clinical information system allowing hospital care plans to be communicated directly to primary care. Within the paper, the authors ascribed what they termed a chronic care model to their program36 however, has since become recognized as a proactive, person-centered, evidence-based approach with features more consistent with a collaborative care model.48
Collaborative Care Model
Chronic care management has evolved to incorporate a collaborative care model, which includes the active engagement of hospital and primary care providers in the shared care of patients beyond usual discharge summaries.48 All 12 of the interventions identified in the literature5,36–46 included features consistent with a collaborative model of care in their initiatives to improve hospital discharge planning and continuity of care, even though they did not all reference a theoretical basis.
A collaborative care model may have formed the theoretical framework for the “Accountable Care in Transitions Program”5 described by Hawes et al in 2018, however was not specifically named. A well-coordinated, multidisciplinary team approach was used within the outpatient transition setting to support patients in the community after hospital discharge, facilitated by direct communication between social workers acting as care managers in both the hospital and primary care settings.5 Social workers too were described as ‘boundary spanners’ to facilitate communication between a medical cancer center and primary care in an intervention described by Flieger et al in 2019.37 In this study, the payment and delivery system innovation adapted an identified chronic care management model to become a more collaborative model of care. The reform prompted the routine sharing of information between hospital social workers and primary care chronic care coordinators, allowing improved care coordination and communication across healthcare settings.37
Improved communication between hospital and primary healthcare providers was also attributed to hospital allied health, in a 2016 retrospective report by Holmes et al describing the trial of a new allied health service in an emergency department.39 The pilot project indicated that the inclusion of a combined social work and physiotherapy service increased patient links to primary care after hospital discharge. Stakeholder and staff feedback via a questionnaire suggested communication had improved between the hospital and primary care,39 however, objective data were not provided so the findings need to be interpreted with caution.
Early attempts to use information technology (IT) to improve the hospital-primary care interface were described by two earlier studies. An electronic data linking system evaluated by Massy-Westropp et al in 200541 allowed hospital access to a primary care data base and alerted primary care providers to patient discharge from hospital. A study by Wilson et al in 200446 indicated that using videoconferencing between the hospital multidisciplinary team and primary care providers provided a better patient management plan than telephone conferencing.46 Unfortunately, both studies relied on the opinions of a small sample of staff rather than finding statistically significant measures of effect, so the findings are difficult to generalize.
Health IT developments have enabled more sophisticated programs to measure and improve care coordination such as those described by Thomas and Siaki (2017)44 and Hsiao et al (2018).40 Both interventions are comprehensive, multidisciplinary approaches to facilitate communication of hospital discharge plans with primary care through the integration of electronic health records, promotion of patient engagement and ongoing monitoring of patients to ensure timely follow up with primary care. Both studies concluded that more efficient IT systems are required to support improved communication across the healthcare continuum.40,44 Hsiao et al suggested that access to hospital medical records (inclusive of allied health documentation) enhanced primary care outcomes and recognized the need for input from community-based organizations to address social and economic issues.40 This more integrated model of care, which they identified as a “care coordination approach”, was reported to strengthen relationships between the hospital and community healthcare providers.40
Integrated Care Model
Hesselink et al38 used an intervention mapping framework, commencing first with a systematic review of effective discharge interventions, to develop a comprehensive guide to improve communication between hospital and primary care. Integrated care was identified as one of the theory-based methods used to identify that discharge templates, a liaison person, reconciliation of medication and regular site visits were strategies to support high-quality discharge information, well-coordinated care, and direct and timely communication with primary care.38 As mental healthcare and social services were not mentioned in the study, it would seem that these strategies were more closely aligned with a collaborative model than an integrated model of care.
As one component of an identified “integrated program of services”, McAiney et al (2016)42 described the role of an intensive geriatric service worker, developed to address the challenges faced by seniors transitioning from hospital to community care that place them at risk of poor outcomes including preventable hospital readmission. A theoretical model was not specifically mentioned; however, the intensive geriatric service worker role was developed with the collaboration of a geriatric health services network and a community-based mental health service to help seniors navigate a complex and disjointed healthcare system.42
In another example of the extension of a collaborative model of care, Trankle et al (2019)45 noted that integrated care aims to improve communication, not just between hospitals and primary care but also between physical care and mental healthcare, as well as between healthcare and social care. The authors evaluated a program, the Western Sydney Integrated Care Program, which enabled shared patient care plans to be developed and accessed by hospital and community healthcare providers and patients. Within this broader evaluation, it was concluded that the program improved patient/caregiver experience of healthcare and built capacity in primary care, acknowledging electronic communication across healthcare sectors remained difficult.45
The “Advanced Care Coordination Program” proposed by Miller et al (2019)43 also seemed to be based on an integrated model of care, to address the gaps in care during patient care transitions, although a theoretical framework was not discussed. Their social worker-led program focused on social determinants of health in a comprehensive and longitudinal care coordination intervention. The core components of care coordination were initial notification of patient hospital admission, a comprehensive needs assessment, clinical intervention as indicated and a phone call to the primary care providers.43 The comprehensive needs assessment addressed access to health care, economic status, housing status, psychological status, and social support. The program included the development of a shared data base, as well as the provision of continuing education and outreach to bridge healthcare and social care communication after hospital discharge.43
To summarize, while no specific methods or measures of communication between hospital allied health professionals and primary care practitioners were evaluated, elements of a collaborative care model48 seemed to underpin the majority of studies describing interventions aiming to improve discharge planning and communication between hospitals and primary care settings. The more recent studies suggest that the collaborative model of care can evolve to become an integrated model of care, providing a theoretical framework for interventions to facilitate collaboration between healthcare and community services, including mental healthcare and social care services. There were some common concepts and components identified in the included studies which have helped and hindered general communication within and between hospital and primary care, which will be further discussed in relation to the enablers and barriers highlighted within each study.
Enablers and Barriers to Effective Communication Methods Between Hospital Allied Health and Primary Care Practitioners
Coding of the literature allowed the identification of the four most common themes in relation to components and processes of communication between hospital and primary care, allowing an insight into the factors affecting discharge communication between hospital allied health and primary care practitioners. The four emerging themes of “multidisciplinary care plans”, “patient and/or caregiver involvement”, “information technology” and “follow up”, are outlined in Table 6 as the enablers to communication; however, they have their own barriers as described below and included in Table 7.
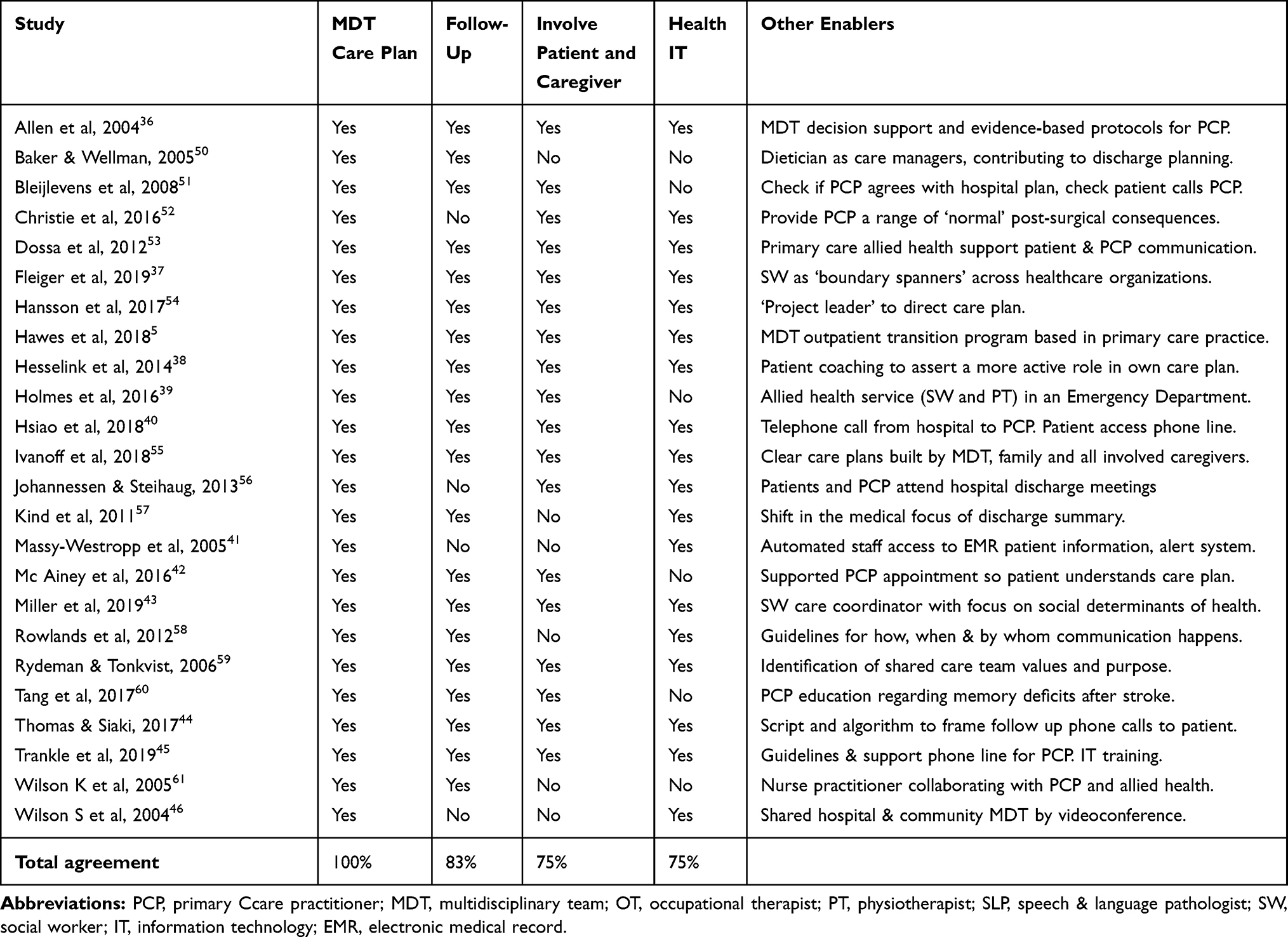 |
Table 6 Enablers to Communication Between Hospital Allied Health and Primary Care |
 |
Table 7 Barriers to Communication Between Inpatient Allied Health and Primary Care |
Multidisciplinary Care Plans
Multidisciplinary care plans were important components of the 12 interventions aiming to improve communication processes between hospitals and primary care.5,36–46 The remaining 12 studies50–61 assumed or suggested that multidisciplinary care plans were a means of facilitating healthcare communication, as outlined in Table 6. There were, however, multiple barriers to the practice and process of multidisciplinary care plans mentioned in the 24 included studies, including ineffective relationships between health professions,50–56,61 junior doctors responsible for the discharge summary54 and allied health reports and recommendations omitted from the care plan.50,57 Multidisciplinary care plans that are collaborative and person-centered may be a common goal, however, there is little evidence in the literature to determine their quality, consistency or whether they support or are supported by effective communication between hospital allied health and primary care practitioners. A word frequency search across all of the included studies using NVivo software31 revealed that the term “communication” was not one of the ten most frequent words, only appearing in the 50 most frequent words [see Figure 2], despite the accepted understanding that communication is one of the cornerstones of collaborative healthcare.62
 |
Figure 2 Word cloud of 50 most frequent words. |
Patient and Caregiver Involvement
According to the World Health Organization, person-centered care takes into account the patient’s values, beliefs and preferences while encouraging them to actively participate in their own individualized care plan.7 Involving the patient and caregiver in discharge planning and encouraging self-management was incorporated in 18 (75%) of the 24 included studies5,36–40,42–45,51–56,59,60 as seen in Table 6. Several of the studies reported negative patient experiences of the discharge process where they did not feel sufficiently involved or informed.38,42,52,53
Despite theoretical models, healthcare policies and hospital guidelines, it seems barriers remain to the involvement of patients in their own care planning, preventing healthcare practice from being truly person-centered and compromising initiatives to become more people-centered. Two studies focused specifically on the unmet communication needs of patients and their caregivers, leading to issues with continuity of care.52,53 Other studies found some patients do not dare to speak up,38 are unable to comprehend information or may be too medically unstable to contribute to discharge planning.54 Furthermore, healthcare professionals may not feel equipped to broach certain topics with patients and caregivers.60 Insufficient time and knowledge to allow effective communication with patients50,54 could be further barriers to involving patients and caregivers in the planning of the transition from hospital to home.
Health Information Technology
There was a general consensus in the literature with 18 (75%) of the 24 included studies suggesting that advances in health IT may offer a promising solution to the inconsistency of healthcare communication,5,36–38,40,41,43–46,52–59 as seen in Table 6, but multiple barriers to its implementation were identified. Logistical barriers to health IT include the lack of staff access and training,41,46 lack of appropriate technology36,40 and system incompatibility.37,38,43,45
Follow-Up
In the absence of consistent, compatible health IT systems to share care plans and standardize communication across healthcare settings, the importance of a designated person to support the transition of care was highlighted by 20 (83%) of the 24 included studies5,36–40,42–45,50,51,53–55,57–61 as seen in Table 6. “Care manager” and “case manager” were the most common titles attributed to the healthcare professional identified to follow up patients after hospital discharge;5,36,44,50,55 however, they were also referred to as ‘chronic care coordinator,37 “transition guide”,40 “care facilitator”,45 “health coach”,54 and “intensive geriatric service worker”.42 One study recommended that an occupational therapist and a geriatrician should provide post-discharge follow-up and communicate with primary care practitioner.51 Other studies recommended various healthcare professionals could provide such follow-up and communication with primary care: a liaison nurse or pharmacist,38 nurse practitioner,61 advanced practice nurse53 or social worker.39 Of the four studies that did not refer to a designated person to provide follow up, all four studies suggested an alternative process to encourage patient follow-up by primary care; two of them recommended primary care providers be involved in hospital discharge planning meetings,46,56 another relied on an automated hospital discharge alert system41 and one recommended patient provision of follow-up service information, including whom to call if follow up does not occur.52 Unlike the interventions recommending a designated person to provide follow up, these four studies41,46,52,56 did not seem to include a process to ensure follow up had occurred after hospital discharge.
The main barrier to a designated person to follow up and ensure continuity of care appears to be ineffective relationships between healthcare organizations, due to and resulting in a lack of collaboration between healthcare providers50 and between healthcare settings.38,53–55,57–59 Siloed healthcare is clearly a contributing factor,38,51,54,55 resulting in one-way communication,51 with hospital discharge summaries often not received in time to be relevant to primary care practitioners53,59 and/or without establishing a shared understanding by determining if the information is according to need and/or understood.54
In summary, enablers to effective communication between hospital allied health and primary care practitioners are multidisciplinary care plans, made in collaboration with patient and caregivers, electronically communicated to primary care, with a designated person to follow up to ensure that there is continuity of care in the community after hospital discharge. The barriers to such communication include that discharge communication can remain medically focused and may not include allied health recommendations or the preferences of patients and/or their caregivers. Even when multidisciplinary care plans aimed to be collaborative and person-centered or ideally based on a people-centered integrated model of care,7 health IT systems do not consistently support effective communication between hospitals and primary care.
Discussion
Despite the wide-held assertion that hospital discharge processes and care transitions are improved through timely and accurate communication,1,63 this narrative systematic review is the first to synthesize data on communication specifically between hospital allied health professionals and primary care practitioners. Given the paucity of research in the field, the review took a broad and inclusive approach to study across qualitative and quantitative research. In doing so, we have identified the lack of well-designed, intervention-based research related to communication between these key healthcare provider groups, which potentially suggests that hospital allied health professionals do not communicate at all with primary care practitioners.
Previous systematic reviews investigating healthcare collaboration have highlighted the importance of effective multidisciplinary communication.17,64 While important to collaboration, there has been little recognition of the role of hospital allied health from the perspective of primary care practitioners. The terms “multidisciplinary” and “interdisciplinary” are used interchangeably to denote a healthcare team working together; however, it has been suggested that the terms are conceptually different, with only the latter allowing the coordination of a common and coherent approach to the care required for collaboration.65 The teams mentioned in the included studies were comprised of various healthcare professionals, acknowledged at times to be poorly described, with some relying on a social worker as the only mentioned hospital allied health representative. The World Health Organization recommends an interdisciplinary approach to healthcare;7 however, differences in culture, resources and expectations of healthcare professionals, systems and populations may result in different interpretations of definitions, theoretical models and guidelines. Similarly, patient-, person-, and people-centered care are not interchangeable nor universal terms. The goal of patient-centered communication is to provide care concordant with patient’s values, needs and preferences, allowing patients to actively participate in decisions about their health and care.66 The core values of patient-centered communication are shared with the World Health Organization’s definition of person-centered care, which they recommend extending to people-centered care by adopting the perspectives of individuals, caregivers, families and communities relative to people’s comprehensive needs and social preferences.7 The heterogeneity of the included studies within this review, although deliberate to capture the scope of the issue, may be reflective of these ambiguities in terminology, suggesting a need to establish what constitutes effective multidisciplinary and/or interdisciplinary, patient/person/people-centered care and/or communication before they can be further evaluated.
Despite the limitations in the breadth of the literature, a number of key observations may be drawn from our data synthesis. Firstly, multi-component interventions using an integrated model of care could improve the success of communicating the multidisciplinary, person-centered care plan from the hospital setting to the primary care setting. Secondly, a designated person to provide follow-up such as a case/care manager working across healthcare settings may be required to support care plans.67 Thirdly, standardization of health IT processes to include hospital allied health input regarding patient function, social situation and recovery goals could facilitate more multidisciplinary collaboration with greater consideration of individual needs and preferences, especially during transitions of care. These findings are particularly relevant since the COVID-19 pandemic has placed increased pressure on health and social systems, affecting hospital to home transitions on many levels and highlighting the particular vulnerability of older adults with complex health and social care needs.68 Public health measures such as social distancing, as well as shorter hospital stays to minimize infection, may have negative consequences for the management of chronic conditions including mental health issues however they have also accelerated some developments in virtual care.67 Health IT developments such as telemonitoring, telehealth and web-based portals could facilitate communication between healthcare providers,69 patients and caregivers.15 Findings from this review can be integrated into clinical practice: multidisciplinary care plans with input from hospital allied health made in conjunction with patients (and their caregivers) need to be routinely included in electronic discharge summaries. Also, including the details of a designated follow-up person/process would facilitate discharge communication and similarly could be done electronically or virtually. While health IT has the potential to improve the quality and continuity of care,70 research findings on the impact of electronic communication on clinical practice and outcomes have been mixed71 hence further development is needed to be able to leverage this potential.
Heterogeneity of the included studies prevented a meta-analytic synthesis of studies, and this remains a limitation of the review. In addition, the reliance of this review on qualitative and mixed-method studies may reduce the representativeness of our findings. The majority of included studies originated from the United States and Australia, so the generalizability of their findings beyond these healthcare systems may be limited. We have also excluded relevant manuscripts in languages other than English, and by restricting our systematic evaluation to peer-reviewed literature we may have omitted additional publications of interest. Excluding studies from mental health and substance abuse settings prevented the narrative synthesis of the integrated care model used in these settings despite their relevance to WHO recommendations.7 Truly person-centered and people-centered care cannot exclude mental health or the social determinants of health; however, many healthcare systems do not yet integrate physical and mental healthcare with social care, hence the exclusion criteria for the purposes of this literature review. We also acknowledge that we excluded studies involving children. Pediatric healthcare also incorporates an integrated care model; however, it draws from other theoretical frameworks, most notably family-centered care; hence, the associated research would not necessarily be applicable to an adult population.
Conclusion
In conclusion, despite the paucity of research investigating communication between hospital allied health professionals and primary care practitioners, our findings do offer a way forward. Further research is needed to understand how healthcare providers can collaborate across healthcare settings and in partnership with patients to improve continuity and strive for integrated people-centered care. Importantly, research must involve allied health to ensure full consideration of the social determinants of health, especially in response to the COVID-19 pandemic.
Health IT systems must be improved to facilitate the consistent development, sharing and follow-up of multidisciplinary person-centered care plans. Such improvements may eventually integrate all health and care systems, allowing communication and coordination between hospitals and primary care, as well as mental and physical healthcare with social care, ensuring collaboration across the care continuum. Integrated people-centered care will only move from theory into practice with effective communication between hospital allied health and primary care practitioners.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article [and its supplementary information file].
Acknowledgments
We thank Alana Saggese (Flinders University, Adelaide, Australia) for assistance with the acquisition of the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by an Australian Government Research Training Program Scholarship (JS). JS was supported by La Trobe University (PhD scholarship); KL was supported by an Australian Research Council Discovery Early Career Research Award (DECRA) Fellowship; NAL was supported by a Future Leader Fellowship (102055) from the National Heart Foundation of Australia.
Disclosure
The authors declare that they have no competing interests.
References
1. Gonçalves-Bradley DC, Lannin NA, Clemson LM, Cameron ID, Shepperd S. Discharge planning from hospital. Cochrane Database Syst Rev. 2017;Issue 1:CD000313.
2. Newnham H, Barker A, Ritchie E, Hitchcock K, Gibbs H, Holton S. Discharge communication practices and healthcare provider and patient preferences, satisfaction and comprehension: a systematic review. Int J Qual Health Care. 2017;29(6):752–768. doi:10.1093/intqhc/mzx121
3. Shahid S, Thomas S. Situation, background, assessment, recommendation (SBAR) communication tool for handoff in health care: a narrative review. Saf Health. 2018;4:7. doi:10.1186/s40886-018-0073-1
4. Kripalani S, LeFevre F, Phillips CO, Williams MV, Basaviah P, Baker DW. Deficits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care. JAMA. 2007;297:831–834.
5. Hawes EM, Smith JN, Pinelli NR, et al. Accountable care in transitions (ACTion): a team-based approach to reducing hospital utilization in a patient-centered medical home. J Pharm Pract. 2018;31(2):175–182.
6. Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 30-day hospitalization: a systematic review. Ann Intern Med. 2011;155(8):520–528.
7. World Health Organization. Continuity and Coordination of Care: A Practice Brief to Support Implementation of the WHO Framework on Integrated People-Centred Health Services. Geneva; 2018.
8. Miller KK, Lin S, Neville M. From Hospital to Home to Participation: a Position Paper on Transition Planning Poststroke. Arch Phys Med Rehabil. 2019;100:1162–1175.
9. Davoody N, Koch S, Krakau I, Hagglund M. Post-discharge stroke patients’ information needs as input to proposing patient-centred eHealth services. BMC Med Inform Decis Mak. 2016;16:66. doi:10.1186/s12911-016-0307-2
10. Wu RC, Lo V, Rossos P, et al. Improving hospital care and collaborative communications for the 21st century: key recommendations for general internal medicine. Interact J Med Res. 2012;1:2. doi:10.2196/ijmr.2022
11. Australian Commission on Safety and Quality in Healthcare. Safety Issues at Transitions of Care: Consultation Report on Perceived Pain Points Relating to Clinical Information Systems. Sydney: ACSQH; 2017.
12. Whiddett R, Hunter I, Engelbrecht J, Handy J. Patients’ attitudes towards sharing their health information. Int J Medical Inform. 2006;75:530–541. doi:10.1016/j.ijmedinf.2005.08.009
13. Ledford CJW, Cafferty LA, Russell TC. The influence of health literacy and patient activation on patient information seeking and sharing. J Health Commun. 2015;20:77–82. doi:10.1080/10810730.2015.1066466
14. Gysels M, Richardson A, Higginson IJ. Does the patient-held record improve continuity and related outcomes in cancer care: a systematic review. Health Expect. 2010;75–91. doi:10.1111/j.1369-7625.2006.00415.x
15. Dameff C, Clay B, Longhurst C. Personal health records – more promising in the smart phone era? JAMA. 2019;321(4):339–340. doi:10.1001/jama.2018.20434
16. Lindberg B, Nilsson C, Zotterman D, Sooderberg S, Skar L. Using information and communications technology in home care for communications between patients, family members, and healthcare professionals. Int J Telmed Appl. 2013;46182.
17. Eikey V, Reddy M, Kuziemsky C. Examining the role of collaboration in studies of health information technologies in biomedical informatics: a systematic review of 25 years of research. J Biomed Inform. 2015;57:263–277. doi:10.1016/j.jbi.2015.08.006
18. Doty MM, Tikkanen R, Shah A, Schneider EC. Primary care physicians’ role in coordinating medical and health-related social needs in eleven countries. Health Aff. 2020;39:115–123. doi:10.1377/hlthaff.2019.01088
19. Janssen A, Robinson T, Brunner M, Harnett P, Museth KE, Shaw T. Multi-disciplinary teams and ICT: a qualitative study exploring the use of technology and its impact on multi-disciplinary team meetings. BMC Health Serv Res. 2018;18:444.
20. Baum FE, Legge DG, Freeman T, Lawless A, Labonte R, Jolley GM. The potential for multidisciplinary primary health care services to take action on the social determinants of health: actions and constraints. BMC Public Health. 2013;13:460.
21. Allied Health Professions Australia. Home page on the internet. Available from: https://ahpa.com.au/resources.
22. Vermier P, Vandijck D, Degroote S, et al. Communication in healthcare: a narrative review of the literature and practical recommendations. Int J Clin Practice. 2015;69(11):1257–1267. doi:10.1111/ijcp.12686
23. Stewart MA. Stuck in the middle: the impact of collaborative interprofessional communication on patient expectations. Shoulder Elbow. 2018;10(1):66–72. doi:10.1177/1758573217735325.
24. Transfer of care from acute inpatient services. Guidelines for managing the transfer of acute inpatients from Victoria’s public health service. Department of Health. 2014. Home page on the internet. Available from: https://www2.health.vic.gov.au/about/publications/policiesandguidelines/Transfer-of-care-from-acute-inpatient-services-Guidelines-for-managing-the-transfer-of-care-of-acute-inpatients-from-Victorias-public-health-services.
25. Fuks H, Raposo A, The GM. 3C collaboration model. Encycl Survey Link. 2008;637–644.
26. Cooke A, Smith D, Booth A. Beyond PICO: the SPIDER tool for qualitative evidence synthesis. Qual Health Res. 2012;22(10):1435–1443.
27. Popay J, Roberts H, Sowden A, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. A Product from the ESRC Methods Programme. 2006.
28. Janse B. Berlo’s SMCR Model of Communication. Tools Hero. 2018. Home page on the internet. Available from: https://www.toolshero.com/communication-skills/berlos-smcr-model-of-communication/.
29. Creswell JW, Creswell JD. Research Design.
30. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
31. QSR International Pty Ltd. NVivo Qualitative Data Analysis Software. Doncaster, Vic, Australia: QSR International Pty Ltd; 2020.
32. The Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews. [Home page on the internet]. Checklist for Qualitative Research. 2017. Available from: https://jbi.global/critical-appraisal-tools.
33. Law M, Stewart D, Pollock N, Letts L, Bosch J, Westmorland M Mc Master Critical Review Form – quantitative Studies. Adapted word version 2007. McMaster University. Home page on the internet. Available from: https://srs-mcmaster.ca/research/evidence-based-practice-research-group/.
34. Mixed Methods Appraisal Tool (MMAT) Version 2018. Mc Gill University. Home page on the internet. Available from: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf.
35. Moher D, Liberati A, Tetzlaff J, Altman D. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement. PLoS Med. 2009;6(6):e1000097. doi:10.1371/journal.pmed1000097
36. Allen K, Hazelett S, Jarjoura D, Wright K, Clough L. Weinhardt J: improving stroke outcomes: implementation of a post discharge care management model. J Clin Out Meas. 2004;11(11):707–714.
37. Flieger SP, Thomas CP, Prottas J. Improving interorganizational coordination between primary care and oncology: adapting a chronic care management model for patients with cancer. Med Care Res Rev. 2019;1–20. doi:10.1177/1077558719870699
38. Hesselink G, Zegers M, Vernooij-Dassen M, et al. Improving patient discharge and reducing hospital readmissions by using Intervention Mapping. BMC Health Serv Res. 2014;14:389.
39. Holmes C, Hollebon D, Scranney A, Exton H. Embedding an allied health service in the Nelson Hospital emergency department: a retrospective report of a six-month pilot project. NZ J Physiother. 2016;44(1):17–25.
40. Hsiao YL, Bass EB, Wu AW, et al. Implementation of a comprehensive program to improve coordination of care in an urban academic health care system. J Health Organ Manag. 2018;32(5):638–657.
41. Massy-Westropp M, Giles LC, Law D, Phillips PA, Crotty M. Connecting hospital and community care: the acceptability of a regional data linkage scheme. Aust Health Rev. 2005;29(1):12–16.
42. McAiney CA, Hillier LM, Paul J, et al. Improving the seniors’ transition from hospital to the community: a case for intensive geriatric service workers. Int Psychogeriatr. 2016;29(1):149–163. doi:10.1017/51041610216001058
43. Miller LB, Sjoberg H, Mayberry A, Mc Creight MS, Ayele RA, Battaglia C. The advanced care coordination program: a protocol for improving transitions of care for dual-use veterans from community emergency departments back to the Veterans Health Administration (VA) primary care. BMC Health Serv Res. 2019;19:734. doi:10.1186/s12913-019-4582-3
44. Thomas DV, Siaki LA. A partnership for patients initiative: redesigning a medical-surgical unit’s discharge process to reduce readmissions. Nurs Econ. 2017;35:2.
45. Trankle S, Usherwood T, Abbott P, et al. Integrating health care in Australia: a qualitative evaluation. BMC Health Serv Res. 2019;19:954. doi:10.1186/s12913-019-4780-z
46. Wilson SF, Marks R, Collins N, Warner B, Frick L. Benefits of multidisciplinary care conferencing using audio-visual compared with telephone communication: a randomized controlled trial. J Telemed Telecare. 2004;10:351-354.
47. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Effect Clin Pract. 1998;1(1):2–4.
48. Von Korff M, Grumen J, Schaefer J, Curry SJ, Wagner EH. Collaborative management of chronic illness. Ann Int Med. 1997;127(12):1097–1102.
49. Valentijn PP, Schepman SM, Opheij W, Bruijnzeels MA. Understanding integrated care: a comprehensive conceptual framework based on the integrative functions of primary care. Int J Integr Care. 2013;13:e010.
50. Baker E, Wellman N. Nutrition concerns in discharge planning for older adults: a need for multidisciplinary collaboration. J Am Diet Assoc. 2005;105:603–607.
51. Bleijlevens MHC, Hendriks MRC, van Haastregt JCM, et al. Process factors explaining the ineffectiveness of a multidisciplinary fall prevention program: a process evaluation. BMC Public Health. 2008;8:332. doi:10.1186/1471-2458-8-332
52. Christie N, Beckett K, Earthy S, et al. Seeking support after hospitalisation for injury: a nested qualitative study of the role of primary care. Br J Gen Pract. 2016;1:154.
53. Dossa A, Bokhour B, Hoenig H. Care transitions from the hospital to home for patients with mobility impairments: patient and family caregiver experiences. Rehabil Nurs. 2012;37(6):277–285. doi:10.1002/rnj.047
54. Hansson A, Svensson A, Hedman Ahlstrom B, et al. Flawed communications: health professionals’ experience of collaboration in the care of frail elderly persons. Scand J of Public Health. 2017;46:680–689.
55. Ivanoff SD, Duner A, Eklund K, Wilhelmson K, Lidén E, Holmgren E. Comprehensive geriatric assessment of frail older people: ideals and reality. J Interprof Care. 2018;32(6):728–734.
56. Johannessen A, Steihaug S. The significance of professional roles in collaboration on patients’ transitions from hospital to home via an intermediate unit. Scand J of Caring Sci. 2013;28:364–372.
57. Kind A, Anderson P, Hind J, Robbins J, Smith M. Omission of dysphagia therapies in hospital discharge communications. Dysphagia. 2011;26(1):49–61.
58. Rowlands S, Callen J, Westbrook J. Are general practitioners getting the information they need from hospitals to manage their lung cancer patients: a qualitative exploration. Health Inf Manag. 2012;41:2.
59. Rydeman I, Tornkvist L. The patient’s vulnerability, dependence and exposed situation in the discharge process: experiences of district nurses, geriatric nurses and social workers. J Clin Nurs. 2005;15:1299–1307.
60. Tang EYH, Price C, Stephan BCM, Robinson L, Exley C. Gaps in care for patients with memory deficits after stroke: views of healthcare providers. BMC Health Serv Res. 2017;17:634. doi:10.1186/s12913-017-2569-5
61. Wilson K, Coulson L, Hilege S, Swann W. Nurse practitioners' experiences of working collaboratively with general practitioners and allied health professionals in New South Wales, Australia. Aust J Adv Nurs. 2005;23(2):22-27.
62. Irgens E, Henriksen N, Moe S. Communicating information and professional knowledge in acquired brain injury rehabilitation trajectories: a qualitative study of physiotherapy practice. Disabil Rehabil. 2018. doi:10.1080/09638288.2018.1544295
63. Connolly M, Deaton C, Dodd M, Grimshaw J, Hulme T, Everitt S. Discharge preparation: do healthcare professionals differ in their opinions? J Interprof Care. 2010;24:633–643. doi:10.3109/13561820903418614
64. Saint-Pierre C, Herskovic V, Sepulveda M. Multidisciplinary collaboration in primary care: a systematic review. Family Pract. 2018;35(2):132–141.
65. Guisti EM, Castelnuovo G, Molinari E. Differences in multidisciplinary and interdisciplinary treatment programs for fibromyalgia: a mapping review. Pain Res Manag. 2017. doi:10.1155/2017/7261468
66. Epstein RM, Franks P, Fiscella K, et al. Measuring patient centered communication in patient-physician consultations: theoretical and practical issues. Soc Sci Med. 2005;61:1516–1528. doi:10.1016/j.socscimed.2005.02.001
67. Low L, Yap M, Brodaty H. A systematic review of different models of home and community care services for older person. BMC Health Serv Res. 2011;11:93. doi:10.1186/1472-6963-11-93
68. Gauvin F, Markel-Reid M, Mc Ainey C, Gannan R McMaster Health Forum. Home page from the internet. Top ten insights into improving hospital-to-home transitions: part 2 – insights from the COVID-19 response. 2020. Available from: https://www.mcmasterforum.org/learn-how/public-events/event-item/top-ten-insights-into-improving-hospital-to-home-transitions-part-2-insights-from-the-covid-19-response.
69. Bygstad B, Hanseth O. From IT Silos to Integrated Solutions. A Study in e-Health Complexity. Proceedings of the 23rd European Conference on Information Systems (ECIS). Munster, Germany; 2015:26–29.
70. Stanhope V, Matthews EB. Delivering person-centred care with an electronic health record. BMC Med Inform Decis Mak. 2019;19:168. doi:10.1186/s12911-019-0897
71. Wu C, Tran K, Lo V, et al. Effects of clinical communication interventions in hospitals: a systematic review of information and communication. Int J of Med Inform. 2012;81(11):723.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.