Back to Journals » Cancer Management and Research » Volume 14
Metastatic or Locally Recurrent Anal Squamous Cell Carcinoma (SCAC): Current Clinical Trial Landscape and Novel Approaches
Authors Rogers JE, Leung M, Johnson B
Received 5 March 2022
Accepted for publication 10 June 2022
Published 21 June 2022 Volume 2022:14 Pages 2065—2077
DOI https://doi.org/10.2147/CMAR.S331429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Jane E Rogers,1 Michael Leung,1 Benny Johnson2
1U.T. M.D. Anderson Cancer Center, Pharmacy Clinical Programs, Houston, TX, USA; 2U.T. M.D. Anderson Cancer Center, Department of Gastrointestinal Medical Oncology, Houston, TX, USA
Correspondence: Jane E Rogers, U.T. M.D. Anderson Cancer Center, 1515 Holcombe Blvd, Houston, TX, 77030, USA, Tel +713-794-3082, Fax +713-794-1586, Email [email protected]
Abstract: Anal squamous cell carcinoma (SCAC) is a human papillomavirus (HPV) driven malignancy. Given inadequate HPV-vaccination rates, SCAC will continue to be a public health concern. SCAC is commonly diagnosed in the local or locoregional setting in which definitive chemoradiation provides the opportunity for cure and has high control rates. A minority of patients will develop recurrence or present with metastatic SCAC. Given the rarity of this disease, research has lagged compared to many other solid tumors. Historically, treatment has been based on extrapolating management approaches from more common squamous cell carcinoma malignancies and/or small case series or case reports. Fortunately, dedicated prospective clinical trial investigation in the advanced setting has emerged in recent years. Here, we review the current strategies for treatment along with remaining challenges and viable next steps for the management of metastatic SCAC.
Keywords: anus neoplasms, immunotherapy, squamous cell carcinoma
Introduction
Cancers occurring in the anus, anal canal, or anorectum represent approximately 2.7% of all digestive system cancers.1 Alarmingly, the incidence of these tumors has been steadily increasing over the last several decades. In 2021, the United States’ estimated new cases are reported at 9090 with 1430 estimated deaths. Anal squamous cell carcinoma (SCAC) is the dominant histology and will be the focus of this review. Other histologies such as anal adenocarcinoma, melanoma, neuroendocrine, and others will not be discussed due to vastly different treatment paradigms to SCAC.
SCAC is a malignancy associated with the human papillomavirus (HPV), with a reported association of ≥95% of cases.1 Other risk factors consist of a history of receptive anal intercourse or sexually transmitted disease, history of other HPV-associated malignancies (ie, cervical, vulvar, or vaginal cancer), chronic immune suppression (ie, solid organ transplant, human immunodeficiency virus (HIV) infection, certain autoimmune diseases), and smoking. Despite the availability of the HPV vaccine, vaccine adherence remains a critical issue with a need for significant improvement and the potential to most substantially reduce SCAC’s burden and occurrence. Recent statistics report only 22% of those aged 18–26 years are reported to have completed the HPV vaccine series, and only 58.6% of those 13–17 years old have completed the series.2,3 Chronic immune suppression is an additional risk factor.1 With immunomodulator introduction and increased use for autoimmune disease treatment, this may pose a potential increase in SCAC incidence. Although correlation with these remains to be determined, other chronic immunosuppression has been linked to increase in developing SCAC.1 A contributing challenge to SCAC is the current inadequate screening modalities and screening guidelines for anal malignancies.4 Lacking adequate screening limits the ability for prevention through early detection. Given these factors, we anticipate the burden of SCAC will remain a relevant healthcare concern in the future.
Often patients will present with rectal bleeding, rectal pain, and/or a sensation of a rectal mass.1 Given this symptomatic presentation, most SCAC cases present in a curable stage, with localized or locoregional disease. Treatment for localized and locoregional disease is with definitive chemoradiation (CRT) with 5-fluorouracil (5-FU) + mitomycin C or 5-FU + cisplatin as CRT sensitizer regimens. A salvage abdominoperineal resection (APR) is reserved for patients refractory to definitive CRT. The decision for an APR is made after at least six months post definitive CRT unless growth is detected sooner. This six-month timeframe allows CRT to reach its full effect. Current survival rates for those with localized or locoregional disease show these treatment modalities to be effective with five-year survival at 81.9% and 65.5%, respectively.5
Recurrent and metastatic disease is relatively rare and represents 10–20% of SCAC cases occurring most often as metachronous disease after primary definitive therapy.1 Data from the Surveillance Epidemiology and End Results (SEER) database collected between 2009 and 2018 showed that only 12.5% of patients with SCAC presented with distant metastases.6 Common metastatic sites are the liver and lungs along with other sites including extra pelvic lymphadenopathy, peritoneum, and bone metastases.1,7 As the incidence of SCAC rises, there is an increasing need for novel approaches. Given the rarity of metastatic disease, prospective trials have been limited. However, as we show in this review, when there is an unmet need for a rare tumor, cooperative group trials can be enrolled quickly as seen with NCI9673.8 Here, we discuss current treatment challenges along with potential solutions to advance the management of recurrent and metastatic SCAC.
Discussion
Current Front-Line Metastatic SCAC Treatment Strategies: Doublet vs Triplet Therapy
Data supporting advanced SCAC treatment have historically been derived from retrospective studies, case reports, or case series involving combinations of fluoropyrimidines, platinums, taxanes, and/or anti-epidermal growth factor receptor (anti-EGFR) therapies.9–15 Treatment decisions have historically been extrapolated from more common SCC malignancies such as head and neck tumors, non-small cell lung cancer (NSCLC), and cervical cancer. Cisplatin + 5-FU emerged as a standard therapy given activity in a small cohort (n = 19).10 Cisplatin + 5-FU showed an overall response rate (ORR) of 66%, median overall survival (OS) of 34.5 months, and relative safety (grade 3–4 neutropenia of 13%). Along with cisplatin + 5-FU, carboplatin + paclitaxel was also routinely considered a suitable regimen given activity in other SCC malignancies and allowed for a non-cisplatin-based therapy for those not suitable Retrospective data from our institution on these two regimens (n = 42 cisplatin + 5-FU; n = 24 carboplatin + paclitaxel) were reported by Eng et al16 The authors showed a median progression-free survival (PFS) of 7 months and median OS of 22 months.
Given the use and activity reported with these regimens but a lack of a prospective head-to-head comparison, The International Rare Cancers Initiative Anal Cancer Working Group devised the InterAACT trial. InterAACT, a Phase 2 trial, randomized patients to cisplatin 60 mg/m2 IV on day 1 + 5-FU 1000 mg/m2/day CI on days 1–4 every 21 days or carboplatin area under the curve (AUC) of 5 on day 1 and paclitaxel 80 mg/m2 on days 1, 8, and 15 every 28 days.17 Forty-two patients were enrolled in each arm over a four-year time period through multiple centers. The ORR was 57% (95% CI, 39.4% to 73.7%) with cisplatin + 5-FU vs 59% (95% CI, 42.1% to 74.4%) with carboplatin + paclitaxel. Complete responses (CRs) were seen in 17% and 12.8% of patients, respectively. The median PFS was 5.7 months (95% CI, 3.3 to 9.0 months) for cisplatin + 5-FU vs 8.1 months (95% CI, 6.6 to 8.8 months) for carboplatin + paclitaxel. A clinically significant difference in OS favored treatment with carboplatin + paclitaxel (median OS was 12.3 months for cisplatin + 5-FU (95% CI, 9.2 to 17.7 months) versus 20 months (95% CI, 12.7 to not reached) for carboplatin + paclitaxel). There were more serious grade 3–4 adverse events associated with treatment with cisplatin + 5-FU (62% versus 36%, p = 0.016) than with carboplatin + paclitaxel which is not surprising given how dosing was selected for each regimen. Considering the similarities in ORR and median PFS and clinical improvement in median OS along with a more favorable safety profile, the authors concluded that carboplatin + paclitaxel would comprise the new standard front-line regimen for untreated advanced SCAC for clinical trials.
While the InterAACT study was recruiting, Kim et al performed The Epitopes HPV02 trial. Epitopes HPV02, a phase 2 trial, examined adding docetaxel to cisplatin + 5-FU.18 The rationale for adding docetaxel originated from the knowledge that loss of p53 function due to E6 oncoprotein expression from HPV-16 and HPV-18 co-infection may confer sensitivity to taxane-induced cytotoxicity. This rationale was supported by favorable findings in the initial retrospective study.11 Epitopes-HPV02 gave standard DCF (docetaxel 75 mg/m2 day 1 + cisplatin 75 mg/m2 day 1 + 5-FU 750 mg/m2/day on days 1–5, every 21 days) for 6 cycles or modified DCF (docetaxel 40 mg/m2 day 1 + cisplatin 40 mg/m2 day 1 + 5-FU 1200 mg/m2/day on days 1–2 every 14 days) for 8 cycles at the discretion of the treating physician based on clinical status and age.18 Sixty-six patients enrolled in the study over approximately three years. ORR was 89%, including 45% demonstrating a complete response. Only two patients experienced disease progression at the first evaluation. The median PFS was 11.0 months (95% CI, 9.3 to 16.4) in the overall population, 10.7 months (95% CI, 8.7 to not reached) in the standard DCF group, and 11.0 months (95% CI, 6.8 to 16.4) in the modified DCF group. The OS at 12 months for the total population was 83.1% (95% CI, 71.5 to 90.3) and the median OS was not reached (95% CI, 25.2 to not reached) on the initial report. Patients who received modified DCF maintained a higher dose intensity and had fewer dose reductions than the standard DCF group. They also experienced less than half fewer serious adverse events. Notably, a post-hoc exploratory analysis revealed that 21% underwent a localized curative intent approach via surgery or radiotherapy. Of these 14 patients, nine (64%) achieved 12-month PFS and the median PFS was not reached at the time of final analysis. Of the 52 patients who did not undergo a localized curative therapy after DCF treatment, 45% achieved 12-month PFS, with a median PFS of 10.1 months (95% CI, 7.56 to 15.34) showing that multidisciplinary care in this setting can be beneficial like that concluded in Eng et al’s retrospective evaluation at our institution.16 Eng et al reported those patients that underwent multidisciplinary care had more than double improvement in median PFS and OS (median PFS of 16 months; median OS of 53 months). We feel advanced SCAC patients warrant a tumor board discussion given these accounts of a localized multidisciplinary curative intent approach.
The authors of the Epitopes-HPV02 study argue that the addition of docetaxel to cisplatin + 5-FU is largely responsible for the higher complete response rate (45%) compared to historical retrospective studies.18 Additionally, there was a higher rate of patients alive and PFS at 12 months in those patients who did not undergo localized curative intent therapy, compared to cisplatin + 5-FU alone. An updated analysis with longer follow-up time pooled the results of the Epitopes-HPV01 and the Epitopes-HPV02 studies together.19 A pooled analysis (n = 115) showed a median PFS of 12 months (95% CI, 10.6 to 16.0) and median OS of 50.2 months (95% CI, 26.0 to 120.0). The ORR was 87.7%, comprised of 40.7% CRs. As noted in the earlier analyses, no differences in efficacy were noted between the standard and modified DCF cohorts. While standard DCF is associated with higher severity of toxicity, the modified DCF regimen could pose an attractive alternative to carboplatin + paclitaxel to patients who could tolerate a triplet regimen, those in need of a high response, and those possibly that could be transitioned to a curative multidisciplinary approach. Questions remain as to whether the use of sequential doublet therapies would fare better than triplet upfront therapy in efficacy and safety outcomes. Unfortunately, this question will remain unanswered in the current future as competing trial strategies are underway that are not comparing these regimens head-to-head (DCF vs carboplatin + paclitaxel).
Current Refractory Metastatic SCAC Treatment Strategies: Role of Immunotherapy and Targeted Therapy
HPV expresses a variety of different proteins. Most notably, the oncoproteins E6 and E7 independently induce carcinogenesis within the anal canal via inactivation of tumor suppressor p53 proteins and retinoblastoma proteins, respectively.20 Programmed death-ligand-1 (PD-L1) expressing tumor cells bind to the inhibitory programmed death-1 (PD-1) receptor to downregulate T-cell activation.8 PD-1/PD-L1 inhibition is thought to trigger the appropriate anti-tumor host immune response through T-cell cytotoxicity.
The NCI9673 trial, a phase 2 trial, utilized the PD-1 inhibitor, nivolumab, in previously treated (median two lines of therapy) metastatic or surgically unresectable SCAC patients.8 Over six months, 37 of 39 screened patients were enrolled to receive nivolumab 3 mg/kg IV every two weeks. Notably, this study enrolled two patients who were HIV-positive. ORR was 24% with two CRs and seven partial responses (PRs) per local investigator assessment. At the time of data cutoff, six (67%) of the nine responders remained on study with the longest ongoing duration of response of 10.4 months, demonstrating a durable response to immunotherapy can be achieved. Furthermore, in responders, the median reduction in target lesions from baseline was 70% (IQR 57% to 90%). Median PFS was 4.1 months (95% CI, 3.0 to 7.9) and the six-month PFS rate was 38% (95% CI, 24% to 60%). The median OS was 11.5 months (95% CI, 7.1 to not estimable) and the estimated 1-year OS was 48% (95% CI, 32% to 74%). From a safety perspective, nivolumab monotherapy was well tolerated as only two patients required corticosteroid intervention for grade 2 pneumonitis and hypothyroidism, respectively. All patients enrolled in the study tested positive for HPV, but patients showed a low prevalence of somatic mutations. The authors concluded that HPV, not somatic mutation burden, is the driving force behind immunotherapy response to nivolumab.
Pembrolizumab, an anti-PD-1 antibody, was also investigated for use in the refractory setting. Based on the results of the multicohort Phase 1b KEYNOTE-028 study, investigators developed the phase 2 trial giving pembrolizumab in previously treated metastatic or surgically unresectable SCAC.21 The study enrolled 112 eligible treatment refractory patients (>70% of whom received two or more prior therapies). Pembrolizumab 200 mg IV was administered every 3 weeks. ORR was 11.6% with five CRs and eight PRs. The median OS was 12.0 months (95% CI, 9.1 to 15.4), and median PFS was 2.0 months (95% CI, 2.0 to 2.1). Grade 3 or greater adverse events occurred in 21 (18.8%) patients and four patients discontinued therapy due to treatment-related adverse events. A pooled analysis was also presented included the patients in the phase Ib KEYNOTE-028 study to the cohort in the KEYNOTE-158 trial, with a longer median follow-up time of 11.7 months.22 The ORR was 10.9% in the pooled analysis (95% CI, 6.3% to 17.4%). Median PFS was 2.1 months (95% CI, 2.0 to 2.1) and the median OS was 11.7 months (95% CI, 8.8 to 14.5), which was consistent with the earlier reported results.
Retifanlimab, anti-PD-1 antibody, was also evaluated for use in patients with previously treated advanced SCAC.23 The POD1UM-202 study, a phase 2 trial, gave retifanlimab 500 mg IV every 4 weeks following disease progression on standard therapy. Ninety-four patients were enrolled with nine who were HIV-positive. ORR was 13.8% with one CR and 12 PRs. Another 35.1% had stable disease. Response to retifanlimab was observed independent of PD-L1 expression, liver metastases, or HIV status. Median PFS and median OS were 2.3 months (95% CI, 1.9 to 3.6) and median OS at 10.1 months (95% CI, 7.9 to not estimable), respectively. As seen with other PD-1 inhibitors, patients who demonstrated response to retifanlimab had durable responses and continued treatment for a median of 9.5 months. Findings from the safety assessment were as expected for a therapy that inhibits PD-1.
These phase 2 explorations showed activity of anti-PD-1 inhibitor monotherapy (12–24% ORR) but additionally highlighted a need for improvement as there is clear intrinsic resistance and acquired resistance with checkpoint monotherapy and predictive biomarkers for checkpoint resistance have not been identified.8,21–23 In October 2018, NCI9673 expanded to randomize newly enrolled patients to receive nivolumab ± ipilimumab, an anti-cytotoxic T-lymphocyte associated antigen 4 inhibitor.24 In this new expansion, patients would receive nivolumab 480 mg IV every 4 weeks with either placebo or ipilimumab 1 mg/kg every 8 weeks. The updated primary endpoint was PFS comparing nivolumab versus nivolumab with ipilimumab. Currently, enrollment is ongoing.
To try and enhance checkpoint inhibitor therapy in SCAC, vascular endothelial growth factor (VEGF) signaling pathway has been identified as a possible immunotherapy resistance mechanism and VEGF inhibitors have shown activity in other SCC malignancies.25–27 Morris et al reported on 20 patients with unresectable SCAC treated with atezolizumab, anti-PD-L1, + bevacizumab, anti-VEGF monoclonal antibody (mAb).25 Most patients (60%) had received at least one prior therapy. Patients were from the NCT03074513 basket trial of HPV-driven malignancies treated with this combination. ORR was 10% with 55% showing stable disease. Median PFS was 4.1 months with median OS of 11.6 months. One patient had a bowel perforation and grade 3 or 4 adverse events with hypertension, hyponatremia, and infection being most common were seen in 35% of patients. Given safety concerns and no added benefit to checkpoint monotherapy, this combination regimen will likely not be further investigated.
EGFR inhibition has been used in various capacities for the treatment of SCAC.14,15 Prior research showed that tissue SCAC characteristically universally overexpress EGFR.28 As other investigators have previously discussed, this is in line with other SCC malignancies. Genomic profiling of patients with metastatic SCAC has additionally revealed a low incidence of resistant mutations along the MAPK pathway, including low to no incidence of KRAS, NRAS, and BRAF.29 The largest retrospective analysis of the role of cetuximab or panitumumab, anti-EGFR mAbs, in metastatic SCAC patients was by our institution.14 Most patients received anti-EGFR mAbs in combination with chemotherapy, the reported median PFS for all patients was 4.3 months (95% CI, 2.63 to 5.86), with a median OS of 16.1 months (95% CI, 13.01 to 19.19). Furthermore, seven patients de-escalated to maintenance therapy with cetuximab monotherapy with a median PFS of 13.8 months (95% CI, 7.24 to 20.25) and median OS of 31.4 months (95% CI, 21.73 to 40.98). Despite prior studies of anti-EGFR mAbs with CRT in the localized setting showing untoward toxicities,30,31 the current analysis showed no grade 3 or 4 adverse events attributable to anti-EGFR therapy.14
Recently, investigators sought to combine anti-PD-1 with avelumab in combination with cetuximab, anti-EGFR mAb, in patients with previously treated metastatic SCAC.32 Given that prior studies described earlier demonstrate clinical activity and durable responses for those that do respond, it is rational to combine it with an anti-EGFR mAb in the setting of high EGFR expression and low KRAS, NRAS, and BRAF mutations within the metastatic SCAC population. The phase 2 CARACAS trial recruited advanced SCAC patients who had received at least one prior line of treatment for metastatic disease. Patients were randomized 1:1 to receive avelumab alone or avelumab with cetuximab. Despite randomization, endpoints were analyzed in parallel. Over approximately 10 months, 30 patients were enrolled in each arm. Notably, there were three patients enrolled in the study with an ECOG performance status of 2. As with other SCAC trials, HIV-positive patients were enrolled but made up a small percent of the population. ORR was 10% for avelumab alone and 17% in the combination arm. Disease control rate was 50% for avelumab alone and 57% for the combination. The median duration of disease control was approximately 4 months for both arms. The median PFS was 2.0 months (95% CI, 1.8 to 4.0) with anti-PD-1 monotherapy and 3.9 months (95% CI, 2.1 to 5.6) with the combination. Median OS was 13.9 months (95% CI 7.7 to 19.4) with avelumab alone and 7.8 months (95% CI 6.2 to 11.2) with combination. Adverse effects were similar to what has been described with each agent alone. As this study was designed with a “pick the winner” approach, the combination arm met the prespecified threshold for ORR to warrant further investigation in future trials. While the observed OS findings for each arm were not consistent with the ORR or median PFS findings, the authors suggested that the shorter OS in the combination regimen could be attributable to an unbalanced burden of disease or the number of lines of prior treatments. Unfortunately, these phase 2 results did not prove to be of much benefit. We believe a combination approach with chemotherapy is warranted along with more translational research to determine the role of anti-EGFR + anti-PD-1/PD-L1 therapy in SCAC.
BCA101, a bifunctional EGFR/TGFB fusion protein, was studied by Janku et al in patients with EGFR-driven advanced malignancies.33 Patients received BCA101 at escalating doses from 64 mg to 1000 mg intravenously weekly across 6 dose levels using a 3+3 design to determine dose limiting toxicities, maximum tolerated dose, and/or recommended dose. Twenty-one patients received single agent BCA101 at 64 (n = 3), 240 (n = 7), 500 (n = 2), 750 (n = 3), 800 (n = 3) or 1000 (n = 3) mg IV weekly. One patient had SCAC. Patients had a median of 4 prior lines of therapy. Grade 3 toxicity was reported in one patient. Best response was stable disease in 30% evaluable patients, with 1 patient on drug ≥4 months. Given the tolerability, BCA101 is now being studied in combination with pembrolizumab in patients with SCC head and neck cancer and SCAC.34 We look forward to these results. Additionally, cetuximab has been reported in combination with IL-15 agonist, NKTR-255, to try and enhance activation of NK cells.35 Early activity has been seen and this combination is now underway in phase 1/2 exploration in SCC head and neck patients, colorectal cancer with expansion to SCAC patients.36 We anticipate further EGFR exploration in SCAC and hope strategies elucidate clear roles for these agents in anal cancer.
Metastatic SCAC Vaccine Strategy Results: Inconsistent Activity
Axalimogene filolisbac (ADXS11-001), a live, irreversibly attenuated and nonpathogenic strain of the intracellular bacterium Listeria monocytogenes bioengineered to secrete an antigen-adjuvant fusion protein between Listeriolysin O and the HPV-16 E7 oncoprotein, was studied by Eng et al in a phase 2 trial in patients with persistent/recurrent, loco-regional or metastatic SCAC.37 Patients received ADXS11-001, 1×109 colony-forming units IV every 3 weeks. Thirty-six patients were treated with 29 patients evaluable for response. One patient had a prolonged PR (3.4% ORR) with a 6-month PFS rate was 15.5%. Grade 3 adverse event (mostly cytokine-release symptoms) was noted in 10 patients. Unfortunately, ADXS11-001 monotherapy failed to make a clinically significant advancement in SCAC treatment, though perhaps a solution is to examine this therapy in combination with other agents to help improve the efficacy.
Glisson et al conducted a phase 2 trial of ISA 101, a synthetic long-peptide HPV-16 vaccine, in combination with nivolumab in patients with incurable HPV-16+ cancer.38 ISA101 100 mcgs/peptide was given Days 1, 22, 50 + nivolumab 3 mg/kg was given iv every 2 weeks beginning day 8 for up to one year. Twenty-four patients enrolled with 22 with oropharynx cancer and 1 patient each with anal and cervical cancer. ORR was 33% with 13% showing stable disease. Median duration of response was greater than 30 weeks. Of the eight patients who achieved a PR, five continued to have response. Median PFS was 2.7 months and median OS was not reached with median follow up time among censored pts 8.6 months. PFS rate at 6 months was 33% and OS rate at 6 months was 74%. Grades 3 and 4 toxicity was infrequent. This combination met its primary endpoint and warrants further evaluation in SCAC.
MEDI0457, a DNA vaccine containing plasmids for E6 and E7 oncogenes for HPV-16/18 and IL-12 adjuvant was tested in combination with durvalumab, anti-PD-L1 by Morris et al in a phase 2 trial of recurrent or metastatic HPV-associated cancers.39 Patients received 7 mg of MEDI0457 intramuscularly (weeks 1, 3, 7, 12, and every 8 weeks thereafter) and durvalumab 1500 mg intravenously every 4 weeks starting at week 4. Twenty-one patients (12 cervical, 7 anal, 2 penile) were treated with most having SCC (n = 17). ORR was 21% with disease control rate of 42% (95% CI, 20–67%). All responses were noted among SCCs with two SCAC patients. Median duration of response among responders was 16 months, median PFS was 3.7 months, and median OS was 13.5 months (95% CI, 10.1-NA) revealing some activity.
Metastatic SCAC: Future Steps
NCI9673 recognized that SCAC is not a cancer that is commonly associated with a high somatic mutation burden in tumor cells unlike other solid tumor malignancies.8 The current standard doublet chemotherapy with a taxane and platinum agent has formed the framework for chemotherapy in the advanced SCAC setting. With immunotherapy activity shown in the later line settings, combination of platinum- and taxane-based regimen with the addition of PD-1/PD-L-1 checkpoint inhibition is the next strategy underway.40–43
Exploratory analyses suggest that taxanes can also deplete immunosuppressive cells to sustain the potential restoration of effective tumor immunity. While taxane-based therapies may synergize with immune checkpoint inhibitors to drive anti-tumor immune responses, it is possible that “cold” tumors like SCCA may require a combined modality approach to overcome primary resistance to immunotherapy.41 Current combination evaluations are underway such as with the InterAACT2/POD1UM-303 is a Phase 3 front-line trial of carboplatin + paclitaxel ± retifanlimab with an expected completion date in 2024.40 After six months, patients in the retifanlimab arm receive retfanlimab for one year. Similarly, EA2176, a phase 3 trial, is evaluating the nivolumab to conventional carboplatin + paclitaxel chemotherapy.42 After six cycles of carboplatin + paclitaxel, patients in the nivolumab arm will be placed on nivolumab for two years. The study is currently enrolling, with an expected completion date in 2023. Additionally, the SCARCE trial, phase 2 trial, is evaluating the addition of atezolizumab to the modified DCF regimen for eight cycles.43 Patients in the atezolizumab arm would subsequently complete 1 year of atezolizumab monotherapy.
Tumors subject to radiation can induce single point mutations and double strand breaks in DNA to increase the prevalence of tumor-related antigens and the tumor mutation burden to augment anti-tumor immunity. Combined with anti-PD-1 therapy, this combined approach formed the basis of the SPARTANA study, a phase 2 trial.41 SPARTANA additionally will help to evaluate locoregional treatment for oligometastatic disease sites. As seen with Eng et al, retrospective evaluation median PFS and OS can be greatly improved when multidisciplinary care is feasible (median PFS of 16 months and median OS of 53 months). SPARTANA is being conducted in four sequential phases for enrolled patients. The phase 1 portion entails the administration of eight Gy radiotherapy to target lesions. During Phase 2, mDCF is administered for 8 cycles and concurrently given with spartalizumab, an anti-PD-1 antibody, given every 4 weeks for 4 doses. Phase 3 involves ablative treatment of the metastatic sites of disease and CRT for the primary site of disease. In the final phase, patients are continued on spartalizumab maintenance for the remainder of 1 year of therapy. This study is ongoing with an expected completion date of November 2025. SPARTANA will help to prospectively analyze how to incorporate local therapy into recurrent/metastatic SCAC therapy. Challenges remain on how should undergo multidisciplinary care, what multidisciplinary care is best for that patient, and what sequence of therapy is best. We hope future trial design in this area will help elucidate these issues. Checkpoint inhibitor therapy is also being studied in SCAC early-stage disease as seen with the CORINTH, RADIANCE, and EA2165.44–46 CORINTH is a phase 1b/2 trial evaluating pembrolizumab with radiation in stage III/IV patients.44 RADIANCE is a phase 2 trial investigating durvalumab with chemoradiation for those with stage II/III patients, and EA2165 is a phase 3 trial looking at nivolumab vs observation in those with stage III anal cancer who underwent chemoradiation.45,46 This may present a challenge when patients have recurrence disease as checkpoint resistance and re-challenge will need to be determined and established.
There is still a need for more discoveries particularly in the refractory setting. Given the lack of somatic mutation burden seen with SCAC, investigation into the few mutations that have been seen warrant further exploration. Phosphatidylinositol-3-kinase catalytic subunit alpha (PIK3CA) mutations have been reported in metastatic SCAC with a frequency of approximately 20–30%.29,47–49 Additionally, PIK3CA mutations in SCAC have been identified as a potential poor prognostic feature.48 Agents like alpelisib, a PI3K inhibitor, are being studied in other SCC cancers alone or in combination.50–52 Additionally, mTOR inhibitors such as everolimus might be an area of potential activity for those with a PIK3CA mutation.47,52 These mutations additionally have presented a potential resistance pathway in other tumors for anti-EGFR mAbs representing an area to investigate as EGFR inhibition continues to be explored.53 As molecular analyses continue to mature, targetable mutations hope to be identified in SCAC.
Exciting immunotherapy-driven concepts via therapeutic vaccines are underway for advanced HPV-driven malignancies of which recurrent/metastatic SCAC is included. Vaccine combination strategies are underway in HPV associated cancers such as in the phase 1/2 PRGN-2009, an adenovirus HPV vaccine, alone or in combination with bifunctional anti-PD-L1/TGF-β (M7824).54 TGF-β is overexpressed in HPV positive malignancies and is thought to help these tumors evade immune surveillance.55 Data from phase 1 and phase 2 exploration have shown a 30.5% ORR in M7824 in checkpoint naïve HPV associated tumor patients.56 To add onto combination strategies with M7824, a phase 1/2 trial is underway evaluating PDS0101, a short-peptide-based HPV vaccine, in combination with M7824 and NHS-IL12, interleukin-12.57 A phase 2 looking at MEDI0457 as mentioned earlier is examining its role as a combination of plasmid encoding human interleukin 12 to enhance the pro-inflammatory response to HPV antigens encoded in VGX-3100 in combination with durvalumab in advanced HPV malignancies.58 UCPVax, a peptide vaccine, is being evaluated with atezolizumab in phase 2 trial in immunotherapy naïve HPV malignancies.59 Another phase 1 trial is evaluating MG1-E6E7, an adenovirus, with Ad-E6E7 and atezolizumab.60 SQZ-PBMC-HPV, a CART therapy, is being evaluated via phase 1 as monotherapy and in combination with atezolizumab or other immune checkpoint inhibitors in HLA-A*02+ patients with recurrent, locally advanced or metastatic HPV16+ solid tumors.61 We await results of these novel strategies.
Continuing to understand the underlying biology as well as novel markers of response and resistance in SCAC is needed. Circulating tumor DNA (ctDNA) offers this potential as repeat biopsies in localized anal cancer are often not available and invasive. Additionally, HPV ctDNA appears to be a potential predictor for resistance to therapy and prognostic implications.62–65 Considering HPV DNA is found in greater than 90% of patients with SCAC, the use of a novel droplet-digital PCR (ddPCR) that can detect and quantify tumor-derived HPV DNA sequences in patient blood (HPV ctDNA) with high sensitivity and specificity represents an attractive tool available to the majority of patients for monitoring and treatment response.64 Cabel et al evaluated the prognostic impact of residual HPV ctDNA in patients treated with chemoradiation. Furthermore, early detection of molecular relapse is clinically relevant as the current standard of care for local failure or persistent disease after chemoradiation is an abdominoperineal resection. Of note, the authors reported two notable findings. First HPV ctDNA can be detected before chemoradiation for nearly 90% of patients and subsequently cleared upon completion of chemoradiation. Secondly, all patients in the cohort with persistent HPV ctDNA post chemoradiation experienced disease recurrence highlighting the prognostic impact of HPV ctDNA clearance in locally advanced SCAC.64 Lefèvre et al showed similar results particularly describing the relationship of ctDNA dynamics in relation to therapeutic outcomes. Their data revealed patients can be divided into three groups stratifying their specific risk of treatment failure (fast responders, slow responders, and persistent molecular responders).65 We believe ctDNA will continue to be explored in this malignancy with key impact on personalization of patient care.
Conclusions
After years of limited prospective research, it is an exciting time for recurrent/metastatic SCAC as many concepts are being evaluated. We have summarized current findings and future steps in Table 1.8,21,23,25,32,34,36–43,57,59–61 We anticipate in the coming years, answers to current questions surrounding the role of checkpoint inhibitor therapy in the front-line setting as well as the role of dual checkpoint inhibitor therapy in the second-line setting will be elucidated. Additionally, we expect certain HPV-driven immunotherapy strategies to evolve and potentially play a role in precision management. Areas that need further investigation include the roles and sequencing of multidisciplinary care and appropriately identifying patients who will benefit from this strategy. Novel approaches incorporating HPV ctDNA may better inform patient selection.62,63 We anticipate increased utilization of HPV ctDNA in subsequent clinical trial design thereby generating additional data supporting the pivotal role of this blood-based marker in patient care and surveillance monitoring. Additionally, the area of EGFR inhibition with novel combination strategies are areas with potential promise in the refractory setting.
 | 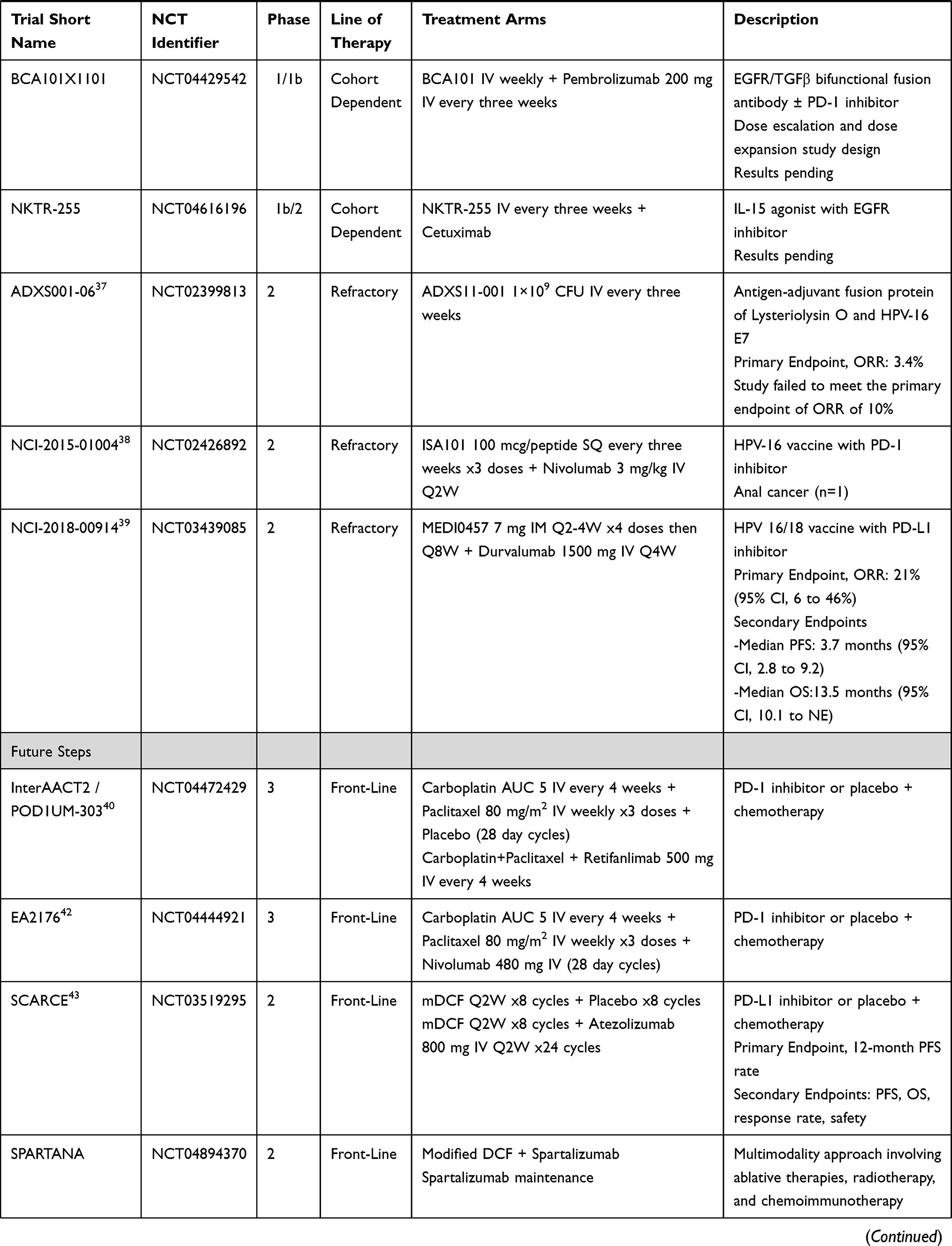 | 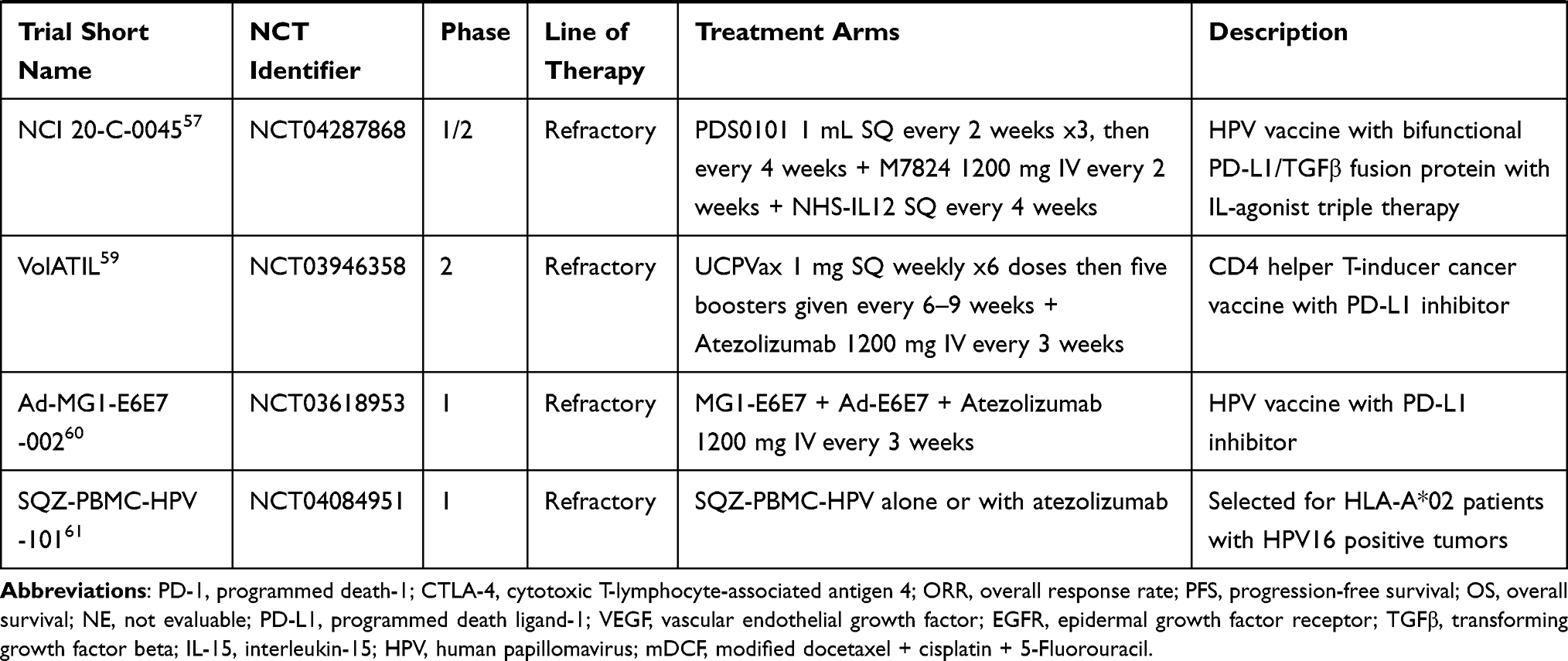 |
Table 1 Emerging Studies and Novel Approaches to the Treatment of Metastatic Anal Cancer8,21,23,25,32,34,36–40 |
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Comprehensive Cancer Network. Anal carcinoma. Version 2; 2021. Available from: www.nccn.org.
2. Boersma P, Black LI. Human papillomavirus vaccination among adults aged 18−26, 2013−2018. NCHS Data Brief, no 354. Hyattsville, MD: National Center for Health Statistics; 2020.
3. Pingali C, Yankey D, Elam-Evans LD, et al. National, regional, state, and selected local area vaccination coverage among adolescents aged 13–17 years — United States. MMWR Morb Mortal Wkly Rep. 2020;70:1183–1190. doi:10.15585/mmwr.mm7035a1external
4. Leeds IL, Fang SH. Anal cancer and intraepithelial neoplasia screening: a review. World J Gastrointest Surg. 2016;8(1):41–51. doi:10.4240/wjgs.v8.i1.41
5. National Cancer Institute. Surveillance, epidemiology, and end results program. cancer stat facts: anal cancer. Available from: https://seer.cancer.gov/statfacts/html/anus.html.
6. National Cancer Institute. Surveillance, epidemiology, and end results program. anus, anal canal & anorectum stage distribution of SEER incidence cases, 2009–2018. Available from: https://seer.cancer.gov/explorer/application.html?site=111&data_type=1&graph_type=4&compareBy=sex&chk_sex_3=3&chk_sex_2=2&race=1&age_range=1&advopt_precision=1&advopt_display=2.
7. Rogers JE, Eng C. Pharmacotherapy of anal cancer. Drugs. 2017;77:1519–1530. doi:10.1007/s40265-017-0792-3
8. Morris VK, Salem ME, Mimeiri H, et al. Nivolumab for previously treated unresectable metastatic anal cancer (NCI9673): a multicentre, single-arm, phase 2 study. Lancet Oncol. 2017;18(4):446–453. doi:10.1016/S1470-2045(17)30104-3
9. Ajani JA, Carrasco CH, Jackson DE, et al. Combination of cisplatin plus fluoropyrimidine chemotherapy effective against liver metastases from carcinoma of the anal canal. Am J Med. 1989;87(2):221–224. doi:10.1016/s0002-9343(89)80702-8
10. Faivre C, Rougier P, Ducreux M, et al. [5-fluorouracile and cisplatinum combination chemotherapy for metastatic squamous-cell anal cancer]. Bull Cancer. 1999;86(10):861–865. Danish.
11. Kim S, Jary M, Mansi L, et al. DCF (docetaxel, cisplatin and 5-fluorouracil) chemotherapy is a promising treatment for recurrent advanced squamous cell anal carcinoma. Ann Oncol. 2013;24(12):3045–3050. doi:10.1093/annonc/mdt396
12. Abbas A, Nehme E, Fakih M. Single-agent paclitaxel in advanced anal cancer after failure of cisplatin and 5-fluorouracil chemotherapy. Anticancer Res. 2011;31(12):4637–4640.
13. Boland PM, Wang K, Kohen A. Systemic therapy for advanced anorectal squamous cell carcinomas: a single institutional experience. J Clin Oncol. 2016;34(4):728. doi:10.1200/jco.2016.34.4_suppl.728
14. Rogers JE, Ohinata A, Silva NN, et al. epidermal growth factor receptor inhibition in metastatic anal cancer. Anticancer Drugs. 2016;27(8):804–808. doi:10.1097/CAD.0000000000000383
15. Kim DW, Byer J, Kothari N, et al. EGFR inhibitors in patients with advanced squamous cell anal carcinomas: a single-institution experience. Oncology. 2017;92(4):190–196. doi:10.1159/000452766
16. Eng C, Chang GJ, You YN, et al. The role of systemic chemotherapy and multidisciplinary management in improving the overall survival of patients with metastatic squamous cell carcinoma of the anal canal. Oncotarget. 2014;5(22):11133–11142. doi:10.18632/oncotarget.2563
17. Rao S, Sclafani F, Eng C, et al. International rare cancers initiative multicenter randomized Phase II trial of cisplatin and fluorouracil versus carboplatin and paclitaxel in advanced anal cancer: interAAct. J Clin Oncol. 2020;38(22):2510–2518. doi:10.1200/JCO.19.03266
18. Kim S, Francois E, Andre T, et al. Docetaxel, cisplatin, and fluorouracil chemotherapy for metastatic or unresectable locally recurrent anal squamous cell carcinoma (Epitopes-HPV02): a multicentre, single-arm, phase 2 study. Lancet Oncol. 2018;19(8):1094–1106. doi:10.1016/S1470-2045(18)30321-8
19. Kim S, Meurisse A, Spehner L, et al. Pooled analysis of 115 patients from updated data of Epitopes-HPV01 and Epitopes-HPV02 studies in first-line advanced anal squamous cell carcinoma. Ther Adv Med Oncol. 2020;12:1758835920975356. doi:10.1177/1758835920975356
20. Thomas MK, Pitot HC, Liem A, et al. Dominant role of HPV16 E7 in anal carcinogenesis. Virology. 2011;421(2):114–118. doi:10.1016/j.virol.2011.09.018
21. Marabelle A, Cassier PA, Fakih M, et al. Pembrolizumab for advanced anal squamous cell carcinoma (ASCC): results from the multicohort, phase II KEYNOTE-158 study. J Clin Oncol. 2020;38(4 _suppl):1. doi:10.1200/JCO.19.02105
22. Marabelle A, Cassier PA, Fakih M, et al. Pembrolizumab for previously treated advanced anal squamous cell carcinoma: pooled results from the KEYNOTE-028 and KEYNOTE-158 studies. J Clin Oncol. 2020;38(15):4020. doi:10.1200/JCO.2020.38.15_suppl.4020
23. Rao S, Capdevilla J, Gilbert D, et al. POD1UM-202: phase II study of retifanlimab in patients (pts) with squamous carcinoma of the anal canal (SCAC) who progressed following platinum-based chemotherapy. Ann Oncol. 2020. doi:10.1016/j.annonc.2020.08.2272
24. National Cancer Institute. Nivolumab with or without ipilimumab in treating patients with refractory metastatic anal canal cancer. Clinicaltrials.gov [Internet]. NLM Identifier: NCT02314169. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT02314169.
25. Morris V, Liu S, Johnson B, et al. 403MO Atezolizumab in combination with bevacizumab for patients with unresectable/metastatic anal cancer. Ann Oncol. 2020;31(4):S412. doi:10.1016/j.annonc.2020.08.514
26. National Comprehensive Cancer Network. Cervical cancer. Version 1; 2022. Available from: www.nccn.org.
27. National Comprehensive Cancer Network. Non-small cell lung cancer. Version 1; 2022. Available from: www.nccn.org.
28. Le LH, Chetty R, Moore MJ, et al. Epidermal growth factor receptor expression in anal canal carcinoma. Am J Clin Pathol. 2005;124(1):20–23. doi:10.1309/X4UADHVN317V2XMW
29. Morris V, Rao X, Pickering C, et al. Comprehensive genomic profiling of metastatic squamous cell carcinoma of the anal canal. Mol Cancer Res. 2017;15(11):1542–1550. doi:10.1158/1541-7786.MCR-17-0060
30. Garg MK, Zhao F, Sparano JA, et al. Cetuximab plus chemoradiotherapy in immunocompetent patients with anal carcinoma: a Phase II eastern cooperative oncology group-American college of radiology imaging network cancer research group trial (E3205). J Clin Oncol. 2017;35(7):718–726. doi:10.1200/JCO.2016.69.1667
31. Feliu J, Garcia-Carbonero R, Capdevila J, et al. VITAL phase 2 study: upfront 5-fluorouracil, mitomycin-C, panitumumab and radiotherapy treatment in nonmetastatic squamous cell carcinomas of the anal canal (GEMCAD 09-02). Cancer Med. 2020;9(3):1008–1016. doi:10.1002/cam4.2722
32. Lonardi S, Prete AA, Morano F, et al. Randomized phase II trial of avelumab alone or in combination with cetuximab for patients with previously treated, locally advanced, or metastatic squamous cell anal carcinoma: the Caracas study. J Immunother Cancer. 2021:9e002996. doi:10.1136/jitc-2021-002996
33. Janku F, Hanna GJ, Carvajal RD, et al. First-in-human Phase I study of the bifunctional EGFR/TGFβ fusion protein BCA101 in patients with EGFR-driven advanced solid cancers. J Clin Oncol. 2021;39(15):3074. doi:10.1200/JCO.2021.39.15_suppl.3074
34. Bicara Therapeutics. Study of safety and tolerability of BCA101 monotherapy and in combination therapy in patients with EGFR-driven advanced solid tumors. ClinicalTrials.gov [Internet]. NLM Identifier: NCT04429542. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04429542.
35. Altan M, Patnaik A, Barve MA, et al. NKTR-255 + cetuximab in patients with solid tumors: interim safety and efficacy results from the Phase 1b dose-escalation study. Doi: 10.1136/jitc-2021-SITC2021.957.
36. Nektar Therapeutics. Study of NKTR 255 in combination with cetuximab in solid tumors. ClinicalTrials.gov [Internet]. NLM Identifier: NCT04616196. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04616196.
37. Eng C, Fakih M, Amin M, et al. A phase II study of axalimogene filolisbac for patients with previously treated, unresectable, persistent/recurrent loco-regional or metastatic anal cancer. Oncotarget. 2020;11(15):1334–1343. doi:10.18632/oncotarget.27536
38. Glisson B, Massarelli E, William WN, et al. 1136O - Nivolumab and ISA 101 HPV vaccine in incurable HPV-16+ cancer. Ann Oncol. 2017;28(5):403–404. doi:10.1093/annonc/mdx376.002
39. Morris VK, Jazaeri AA, Westin SN, et al. Phase II trial of MEDI0457 and durvalumab for patients with recurrent/metastatic HPV-associated cancers. J Clin Oncol. 2021;39(15):2595. doi:10.1200/JCO.2021.39.15_suppl.2595
40. Incyte Corporation. Carboplatin-paclitaxel with retifanlimab or placebo in participants with locally advanced or metastatic squamous cell anal carcinoma (POD1UM-303/InterAACT 2). ClinicalTrials.gov [Internet]. NLM Identifier: NCT04472429. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://www.clinicaltrials.gov/ct2/show/NCT04472429.
41. Centre Hospitalier Universitaire de Besancon. Combination of spartalizumab, mDCF and radiotherapy in patients with metastatic squamous cell anal carcinoma (SPARTANA). ClinicalTrials.gov [Internet]. NLM Identifier: NCT04894370. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04894370.
42. National Cancer Institute. EA2176: Phase 3 clinical trial of carboplatin and pacliitaxel ± nivolumab in metastatic anal cancer patients. ClinicalTrials.gov [Internet]. NLM Identifier: NCT04444921. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/study/NCT04444921.
43. Kim S, Buecher B, Andre T, et al. Atezolizumab plus modified docetaxel-cisplatin-5-fluorouracil (mDCF) regimen versus mDCF in patients with metastatic or unresectable locally advanced recurrent anal squamous cell carcinoma: a randomized, non-comparative phase II SCARCE GERCOR trial. BMC Cancer. 2020;352(2). doi:10.1186/s12885-020-06841-1
44. Cardiff University. Phase 1b/II trial of pembrolizumab plus IMRT in Stage III/IV carcinoma of anus (CORINTH). ClinicalTrials.gov [Internet]. NLM Identifier: NCT04046133. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04046133.
45. Goethe University. Radiochemotherapy ± durvalumab for locally-advanced anal carcinoma. a multicenter, randomized, Phase II trial of the German anal cancer study group (RADIANCE). ClinicalTrials.gov [Internet]. NLM Identifier: NCT04230759. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04230759.
46. National Cancer Institute. Nivolumab after combined modality therapy in treating patients with high risk Stage II-IIIB anal cancer. ClinicalTrials.gov [Internet]. NLM Identifier: NCT03233711. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT03233711.
47. Alqahtani A, Ayesh HSK, Halawani H. PIK3CA gene mutations in solid malignancies: association with clinicopathological parameters and prognosis. Cancrs. 2019;12(1):93. doi:10.3390/cancers12010093
48. Cacheux W, Rouleau E, Briaux A, et al. Mutational analysis of anal cancers demonstrates frequent PIK3CA mutations associated with poor outcome after salvage abdominoperineal resection. Br J Cancer. 2016;114(12):1387–1394. doi:10.1038/bjc.2016.144
49. Mondaca S, Chatila WK, Bastes D, et al. FOLFCIS treatment and genomic correlates of response in advanced anal squamous cell cancer. Clin Colorectal Cancer. 2019;18(1):e39–e52. doi:10.1016/j.clcc.2018.09.005
50. Kura Oncology Inc.. Combination trial of tipifarnib and alpelisib in adult recurrent/ metastatic head and neck squamous cell carcinoma (R/M HNSCC). ClinicalTrials.gov [Internet]. NLM Identifier: NCT04997902. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04997902.
51. Dunn LA, Riaz N, Fury MG, et al. A Phase 1b study of cetuximab and BYL719 (Alpelisib) concurrent with intensity modulated radiation therapy in Stage III-IVB head and neck squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2020;106(3):564–570. doi:10.1016/j.ijrobp.2019.09.050
52. Jung K, Kang H, Mehra R. Targeting phosphoinositide 3-kinase (PI3K) in head and neck squamous cell carcinoma (HNSCC). Cancers Head Neck. 2018;3(3):2–13. doi:10.1186/s41199-018-0030z
53. Parseghian CM, Napolitano S, Loree JM, et al. Mechanisms of innate and acquired resistance to anti-EGFR therapy: a review of current knowledge with a focus on rechallenge therapies. Clin Cancer Res. 2019;25(23):6899–6908. doi:10.1158/1078-0432.CCR-19-0823
54. National Cancer Institute. HPV vaccine PRGN-2009 alone or in combination with anti-PDL1/TGF-beta trap (M7824) in subjects with HPV associated cancers. ClinicalTrials.gov. NLM Identifier: NCT04432597. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04432597.
55. Cimino SK, Ciombor KK, Chakravarthy AB, et al. Safety considerations with new treatment regimens for anal cancer. Expert Opin Drug Saf. 2021;20(8):889–902. doi:10.1080/14740338.2021.1915281
56. Strauss J, Gatti-Mays M, Cho BC, et al. Bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in patients with human papillomavirus associated malignancies. J Immunother Cancer. 2020;8:e001395. doi:10.1136/jitc-2020-001395
57. National Cancer Institute. Combination immunotherapy in subjects with advanced HPV associated malignancies. ClinicalTrials.gov [Internet]. NLM Identifier: NCT04287868. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04287868.
58. National Cancer Institute. DNA plasmid-encoding interleukin-12/HPV DNA plasmids therapeutic vaccine INO-3112 and durvalumab in treating patients with recurrent or metastatic human papillomavirus associated cancers. ClinicalTrials.gov [Internet]. NLM Identifier: NCT03439085. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT03439085.
59. ClinicalTrials.gov. Centre hospitalier universitaire de besancon combination of UCPVax vaccine and atezolizumab for the treatment of human papillomavirus positive cancers (VolATIL) (VolATIL). NLM Identifier: NCT03946358. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT03946358.
60. Turnstone Biologics, Corp. This is a trial of MG1-E6E7 with Ad-E6E7 and atezolizumab in patients with HPV associated cancers (Kingfisher). ClinicalTrials.gov [Internet]. NLM Identifier: NCT03618953. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT03618953.
61. SQZ Biotechnologies. Study of SQZ-PBMC-HPV in patients with HPV16+ recurrent, locally advanced or metastatic solid tumors. ClinicalTrials.gov [Internet]. NLM Identifier: NCT04084951. Bethesda (MD): National Library of Medicine (US); 2000. Available from: https://clinicaltrials.gov/ct2/show/NCT04084951.
62. Bernanrd-Tessier A, Jeannot E, Guenat D, et al. Clinical validity of HPV circulating tumor DNA in advanced anal carcinoma: an ancillary study to the epitopes-HPV02 trial. Clin Cancer Res. 2019;25(7):2109–2115. doi:10.1158/1078-0432.CCR-18-2984
63. Morris VK, Thomas MK, Pitot HC, Liem A, Lambert PF. Circulating tumor DNA in advanced anal cancer: a blood biomarker goes viral. Clin Cancer Res. 2019;25(7):2030–2032. doi:10.1158/1078-0432.CCR-18-3982
64. Cabel L, Jeannot E, Bieche I, et al. Prognostic impact of residual HPV ctDNA detection after chemoradiotherapy for anal squamous cell carcinoma. Clin Cancer Res. 2018;24(22):5767–5771. doi:10.1158/1078-0432.CCR-18-0922
65. Lefèvre AC, Pallisgaard N, Kronborg C, et al. The clinical value of measuring circulating HPV DNA during chemo-radiotherapy in squamous cell carcinoma of the anus. Cancers. 2021;13(10):2451. doi:10.3390/cancers13102451
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.