")
Back to Journals » OncoTargets and Therapy » Volume 13
Metastatic Hormone-sensitive Prostate Cancer: Current Perspective on the Evolving Therapeutic Landscape
Authors Hall ME , Huelster HL , Luckenbaugh AN, Laviana AA, Keegan KA, Klaassen Z, Moses KA, Wallis CJD
Received 13 February 2020
Accepted for publication 7 April 2020
Published 29 April 2020 Volume 2020:13 Pages 3571—3581
DOI https://doi.org/10.2147/OTT.S228355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Mary E Hall,1 Heather L Huelster,1 Amy N Luckenbaugh,1 Aaron A Laviana,1 Kirk A Keegan,1 Zachary Klaassen,2 Kelvin A Moses,1 Christopher JD Wallis1
1Department of Urology, Vanderbilt University Medical Center, Nashville, TN, USA; 2Division of Urology, Department of Surgery, Medical College of Georgia, Augusta, GA, USA
Correspondence: Mary E Hall
Department of Urology, Vanderbilt University Medical Center, 1301 Medical Center Dr, Suite 3823, Nashville, TN 37232, USA
Email [email protected]
Introduction: The treatment landscape for patients with metastatic hormone-sensitive prostate cancer (mHSPC) has changed dramatically in the past five years, despite little change in the preceding 20 years. Such rapid change can make it difficult for clinicians to remain abreast of the current literature and synthesize the relevant data to inform evidence-based treatment decisions.
Methodology: We performed a narrative, comprehensive review of treatment options for patients with mHSPC as of December 31, 2019. Specifically, we focused on phase II and III randomized controlled trials assessing the role of chemotherapy, novel androgen axis targeting agents, local-(prostate) directed therapy, and metastasis-directed therapy.
Results: The data support a survival benefit with the addition of four different agents to androgen deprivation among men with newly diagnosed prostate cancer—docetaxel, abiraterone acetate, enzalutamide, and apalutamide. While not directly compared, the efficacy of these agents appears similar. That said, there are differences in their toxicity profiles and notable differences in cost between agents. Although analyses encompassing men with low- and high-volume metastases failed to demonstrate a significant survival benefit for radiotherapy treatment to the prostate, new data demonstrates a benefit for men with low-volume metastatic disease. Ongoing trials will assess whether this applies to local surgical treatment. Similarly, metastasis-directed therapy appears beneficial among carefully selected patients.
Conclusion: Treatment options for patients with mHSPC are rapidly changing following years of stagnation. A number of systemic therapies offer benefit without significant clinical differences between them. The role for local treatment of the prostate as well as metastatic sites continues to evolve.
Keywords: prostate cancer, abiraterone, enzalutamide, apalutamide, docetaxel
Introduction
Prostate cancer is the second most common malignancy and the second leading cause of cancer mortality among men in the United States and Europe.1 Approximately 7% of men in the US initially present with metastatic disease, although this number is on the rise with changing trends in screening practices.2,3 This number is even higher in emerging market economies and as high as 64% in parts of Asia.4
For the past 70 years, androgen deprivation therapy (ADT) has been the mainstay of therapy for locally advanced and metastatic prostate cancer. While the majority of patients will realize a biochemical and clinical response to ADT, nearly all will eventually develop castrate resistance. Since 2004, there has been considerable progress in the development of treatment options and improved survival for men with castrate-resistant prostate cancer (CRPC).5 However, until very recently, there have been no appreciable advancements in the treatment of metastatic hormone-sensitive prostate cancer (mHSPC), also known as metastatic castrate-sensitive or hormone-naïve disease. Survival in this cohort has been essentially stagnant over the preceding 20 years.6 Thankfully, recent developments have changed this landscape dramatically. As such, we report the existing treatment options for men with mHSPC and discuss the current data driving their use.
Methods
We searched PubMed for studies published from inception until December 31st, 2019 using the search terms “metastatic castrate-sensitive prostate cancer” or “metastatic hormone-naïve prostate cancer” AND “treatment” or “therapy”, along with free-text, related, derivative, and exploded terms. We additionally searched for “metastatic castrate-sensitive prostate cancer” or “metastatic hormone-naïve prostate cancer” AND “docetaxel,” “abiraterone,” “enzalutamide,” OR “apalutamide” to ensure complete results for pharmacotherapies in this disease space. On the basis of the literature search, the first (MEH), second (HLH), and senior (CJDW) authors compiled a manuscript framework including relevant sub-topics and a proposed bibliography. This was iteratively revised by co-authors. Following agreement on manuscript structure, the first, second, and senior authors drafted this narrative review that was critically revised by co-authors. The final manuscript represents the consensus of the authors.
Agents with Survival Benefit
Docetaxel
Over the past decade, several trials have elucidated whether a survival benefit can be achieved with the addition of adjuvant therapies near the time of diagnosis of metastatic disease. Docetaxel, a taxane-based chemotherapy agent, was one of the first to emerge as a therapy with strong evidence for an overall survival (OS) benefit in patients with metastatic prostate cancer.7–10 Three key trials were the foundation in establishing this pattern of care, allowing for its now widespread use within the mHSPC space.
In February 2013, the results of the GETUG-AFU15 trial were published.8 This trial focused on 385 patients with metastatic prostate cancer, randomized to treatment with ADT alone vs ADT plus docetaxel. Patients were selected based on histologically confirmed prostate cancer and radiologically diagnosed metastatic disease. All included patients had a Karnofsky score of at least 70%, life expectancy greater than or equal to three months, and acceptable hepatic, hematologic, and renal function. Patients who had previously received chemotherapy for metastatic disease were excluded, and patients must have been initiated on ADT for metastatic disease for no more than two months prior to enrollment. Neoadjuvant ADT and/or chemotherapy was permitted if it had been stopped at least 12 months prior to enrollment.8
Patients were randomized to treatment with either ADT alone (which consisted of orchiectomy vs medical castration with luteinizing hormone-releasing hormone (LHRH) agonists with/without nonsteroidal androgen receptor inhibitors), or ADT plus docetaxel, which they received as 75 mg/m2 every 21 days for up to nine cycles. In 385 patients, median OS was not significantly different in the ADT group vs the ADT plus docetaxel group (48.6 months vs 62.1 months, HR: 0.88, 95%CI: 0.68–1.14, p=0.3), over a median follow-up of 83.9 months.
Shortly after the results of the GETUG-AFU145 trial became available, the CHAARTED data emerged in August 2015.10 This trial consisted of 790 men with metastatic prostate cancer, randomized to ADT alone vs ADT plus docetaxel. Patient selection was similar, largely enrolling patients with a histological diagnosis of prostate cancer and radiologic findings of metastatic disease, an Eastern Cooperative Oncology Group (ECOG) performance status ranging from 0–2, and appropriate renal, hematologic, and hepatic function. Here, patients could have received prior ADT if the total duration was less than two years and it had not been given in the last 12 months, or if recent ADT administration for metastatic disease had been initiated within the previous three months prior to enrollment. Those randomized to the ADT arm received ADT either via medical or surgical castration plus a nonsteroidal antiandrogen, and those randomized to the ADT + docetaxel arm received 75 mg/m2 every 21 days for six cycles.10
The patients were followed for a median of 28.9 months. Median OS was 13.6 months longer (57.6 months vs 44.0 months) in the ADT plus docetaxel group (HR: 0.61, 95%CI: 0.47–0.80, p<0.0001). Subgroup analysis of high-volume disease (HVD), defined as presence of visceral metastases and/or greater than or equal to four bone lesions with at least one beyond the spine and pelvis, vs low-volume disease (LVD) was performed. The survival benefit of adding docetaxel to ADT was even more pronounced in HVD, with median survival increased by 17.0 months (HR: 0.60, 95%CI: 0.45–0.81, p<0.0001. Additional benefits to early docetaxel administration in non-castrate disease included longer time to development of castration-resistance, higher rate of decline of PSA to less than 0.2 ng/mL at 12 months, and lower incidence of prostate-cancer-related deaths.10
To account for the discrepancies between significant results in the two studies, the investigators of the GETUG-AF15 trial retrospectively evaluated the number and site of metastases to stratify groups with high vs low volume of disease. HVD used the same classification as the CHAARTED data, and all other patients were classified as having LVD. For men with HVD, an OS benefit was noted (4.7 months longer) in the GETUG-AF15 cohort as well, but this was not statistically significant. Importantly, the CHAARTED trial included a larger number of participants with a higher median PSA (median PSA 50 in the docetaxel plus ADT group vs 52 in the ADT alone group, as compared to 26.7 and 25.8 in these groups, respectively, in the GETUFG-AFU15 trial), as well as a higher proportion of patients classified to HVD (64% and 66% in ADT and ADT plus docetaxel arms, vs 47% and 48% in GETUG-AFU15, respectively). These factors, along with study population size (780 vs 385), may be responsible for this statistical discrepancy.7,8
In early 2016, data from the multi-arm, multi-stage STAMPEDE trial was published assessing the role of docetaxel in this disease space. There were 2962 men that underwent four-way randomization to ADT alone (arm A), ADT plus docetaxel (arm C), ADT plus zoledronic acid (arm B), or ADT plus both docetaxel and zoledronic acid (arm E). Patient selection in this trial notably included not only men with metastatic disease (61% of participants), but also those with node-positive and high-risk localized disease. In comparisons of ADT plus docetaxel group to ADT alone, STAMPEDE again suggested a survival benefit with ADT and docetaxel for the subset of patients with metastatic disease (sub HR: 0.80, 95%CI: 0.65–0.99, p=0.033). The addition of zoledronic acid was not noted to improve survival, consistent with the findings of other series.9
A meta-analysis was performed with the combined data from GETUG-AF15, CHAARTED, and STAMPEDE in order to further evaluate the OS and progression-free survival (PFS) benefits due to the addition of docetaxel. Men with metastatic disease across all three studies had a statistically significant survival benefit with the addition of docetaxel to ADT (HR: 0.72, 95%CI: 0.06–0.90, p=0.0002). However, a statistically significant difference in efficacy between HVD and LVD could not be shown. Similarly, a significant benefit in PFS was found in those patients who also received docetaxel (HR: 0.63, 95%CI: 0.57–0.70). The combined data yielded an overall 27% risk reduction for death of patients with metastatic disease (HR: 0.73), and a 33% risk reduction for death in HVD patients (HR: 0.67).11
Based on the strong evidence above, the addition of docetaxel to ADT has become increasingly utilized in the first-line management of patients with mHSPC. However, thoughtful patient selection for utilization remains paramount. Patients selected for all three trials had good performance status and acceptable hepatic, renal, and hematologic organ function, suggesting that docetaxel should be considered in relatively healthy patients who would be able to tolerate the systemic effects of docetaxel. The trials above did show some uncommon but serious adverse effects including fatigue, febrile neutropenia, and rarely, death, for which patients should be counseled prior to beginning therapy.8–10 Regardless, the compelling survival benefit noted in the combination docetaxel plus standard ADT regimen underscores its increasing use in the metastatic hormone-sensitive space.
Abiraterone
The next agent critically evaluated in the treatment of mHSPC was abiraterone acetate. Another analysis of the STAMPEDE trial utilized arms A (ADT alone) and G (ADT + abiraterone) to assess its role in men with metastatic disease, N1 disease, and high-risk localized disease (N0M0). 1917 patients were randomized to receive either abiraterone alone (1000 mg) daily with prednisolone (5 mg daily) in addition to ADT or ADT alone. Fifty-two percent of the group had metastatic disease. Over a three-year follow-up, OS was 83% in the abiraterone plus ADT group vs 76% in the ADT alone subset (HR: 0.63, 95%CI: 0.52–0.76, p<0.0001).12
The LATITUDE trial, published concurrently, also sought to prove a similar benefit.13 This was a placebo-controlled study of 1199 with metastatic prostate cancer, blinded to receiving 1000 mg daily of abiraterone acetate plus 5 mg prednisone daily plus ADT vs ADT plus placebo. Patients were required to have at least two of the following high-risk features: Gleason score greater than or equal to eight (ie grade group four and higher), at least three bone metastases, and/or visceral metastases, and in addition could not have received previous chemotherapy, radiation, or surgery for metastatic prostate cancer other than for palliative intent. At an interim analysis with a median follow up of 30.4 months, OS was 66% in the abiraterone group vs 49% in the placebo group, with a relative risk reduction of 38% in the abiraterone versus placebo groups (HR: 0.62, 95%CI: 0.51–0.76, p<0.0001). These two studies strongly demonstrate a similar survival benefit to adding abiraterone to ADT.13
Enzalutamide
In 2019, trials emerged evaluating androgen receptor inhibitors in mHSPC, starting with enzalutamide, which is now used widely in the management of castration-resistant disease. The ARCHES trial evaluated 1150 men with metastatic hormone-sensitive disease.14 Men were eligible if they had appropriate performance status and pathologically confirmed prostate adenocarcinoma with radiologic evidence of metastasis. Participants could have received prior local therapy, previous ADT, and up to six preceding cycles of docetaxel (17% of the cohort). Sixty-three percent of the study participants had HVD, defined as either visceral metastases or ≥4 bony metastases with at least one outside the spine/pelvis. Participants were randomized 1:1 to receive either 160 mg enzalutamide daily plus ADT or ADT plus placebo. The primary end point was radiographic PFS, defined as time from randomization to either first evidence of radiographic progression or death. Imaging was performed at time of screening for enrollment and then every 12 weeks during treatment. At an interim analysis at a median follow-up of 14.4 months, enzalutamide plus ADT was found to reduce the risk of radiographic progression vs ADT plus placebo by 61% (HR: 0.39, 95%CI: 0.30–0.50, p<0.001). This effect was similar in subgroup analyses of high- vs low-volume disease and in men with prior docetaxel. Secondary end points including time to PSA progression, time to initiation of an alternate therapy, and undetectable PSA rate were also favorable in the enzalutamide plus ADT group, with data for OS still pending with ongoing analysis of the trial.14
Another contemporary trial, ENZAMET, randomized 1125 men with metastatic prostate cancer to treatment with enzalutamide 160 mg daily vs a standard nonsteroidal antiandrogen (bicalutamide, flutamide, or nilutamide) in addition to continuous ADT.15 Participants had good performance status, pathologically proven prostate cancer and radiologic evidence of metastasis, and were eligible if they had received previous testosterone suppression as long this had been discontinued at least 12 months prior. Interim analysis after a median follow-up of 34 months showed a significant survival benefit in the enzalutamide group vs those receiving standard nonsteroidal antiandrogens (HR: 0.67, 95%CI: 0.52–0.86, =0.0002).15
Apalutamide
Apalutamide is another oral nonsteroidal antiandrogen which works by inhibiting the androgen receptor and emerged for use in this space in 2019 as the result of the TITAN trial.16 Here, 525 patients with metastatic prostate cancer were randomized to receive 240mg daily of apalutamide or placebo in addition to continuous ADT. Similar to the ENZAMET trial, patients could have received up to six prior cycles of docetaxel and been started on ADT (for no more than six months prior if for mHSPC, or no more than three years prior if for localized disease). At an interim analysis at 24 months, OS was 82.4% in the apalutamide group and 73.5% in the placebo group (HR for death: 0.67, 95%CI: 0.51–0.89, p=0.005) which resulted in a 33% lower risk of death for the apalutamide group. The benefit of apalutamide was consistent across subgroups stratified by volume of disease, planned docetaxel, and Gleason score.16
Comparative Data
All four agents (docetaxel, abiraterone, enzalutamide, and apalutamide) have been FDA-approved for treatment of mHSPC and are now listed as category 1 recommendations within the NCCN guidelines.17 Table 1 highlights the main findings of each of the studies supporting their use, as discussed above. Additional trials are underway, which include patients who have received prior docetaxel within the “standard of care” group, as ADT alone is becoming less commonly utilized in the primary treatment of newly diagnosed metastatic disease. Given these advances, there have been efforts to compare the benefits of the agents above, with most trials focusing on abiraterone vs docetaxel as the enzalutamide and apalutamide data are more recent.
 |
Table 1 Summary of Key Findings from Trials for Metastatic hormone-sensitive Prostate Cancer |
A meta-analysis by Wallis et al in 2018 compared outcomes across the GETUG-AFU15, CHAARTED, LATITUDE, and docetaxel and abiraterone arms of the STAMPEDE trial, focusing on comparison between abiraterone and docetaxel. An indirect comparison between abiraterone plus ADT vs docetaxel plus ADT did not show a significant difference in OS; however, Bayesian meta-analyses suggest that abiraterone may be the preferred agent.18 Sathianathen et al recently published a meta-analysis including the above studies as well as TITAN and ENZAMET, demonstrating that, as expected from the primary data, all four examined agents (docetaxel, abiraterone, enzalutamide, apalutamide), showed improved OS compared to ADT alone. This analysis found no statistically significant differences between agents with respect to OS. However, additional SUCRA analysis suggested that enzalutamide may be the preferred agent.19
With the advent of the trials showing benefit with enzalutamide and apalutamide, new studies and analyses will undoubtedly continue to emerge comparing these to docetaxel and abiraterone. A more recent meta-analysis by Marchioni et al, recently published online in The Journal of Urology ahead of print, examined 13 studies including those mentioned above to examine treatment effect of these agents within the hormone-sensitive metastatic space. Their findings suggest that abiraterone, enzalutamide, and apalutamide have superior OS when compared to docetaxel, as well as delayed disease progression. In addition, they examine adverse events across the pooled studies, and found higher rates of adverse events with abiraterone and docetaxel compared to ADT, and lower rates with abiraterone and enzalutamide compared to docetaxel, with rates similar to treatment with ADT alone.20 Although meta-analyses of this nature are limited given varying factors including patient selection across multiple studies, there will certainly be more data emerging on comparisons between agents as utilization in this disease space grows.
Treatment choice between agents for mHSPC is a challenge, and there is currently no clear consensus on preferential initial selection or sequencing of these agents. Certainly, indirect comparisons (and qualitative assessment of the effects of each agent compared to placebo) suggest few differences in OS. Health economic considerations and ease of administration often play large roles in treatment selection, as does treatment toxicity based on side effects and adverse effects of the agents. The degree to which of these imparts the most influence in treatment selection can vary by country, health-care setting, and practitioner. For example, in the UK the National Health Service (NHS) has mandated use of docetaxel based on health economic analyses. In most of the rest of the world, use of oral androgen axis targeting agents is common as the first line, except perhaps among patients with high volume or visceral disease in which cytotoxic chemotherapy may be preferred.
Understanding common side effects and treatment toxicities with these agents is important when choosing a therapy. For example, individual treatment considerations and treatment-related adverse events and toxicities have played a large role in choosing between abiraterone (eg dysglycemia due to the need for concomitant steroids in diabetic patients) and enzalutamide (eg associated asthenia). The major limiting side effect with docetaxel is neutropenia resulting from bone marrow suppression.8–10 Abiraterone can additionally lead to mineralocorticoid excess and resultant hypertension and hypokalemia, as well as elevation in transaminases, necessitating close lab monitoring during therapy.12,13 The most common side effects with enzalutamide include arthralgias/asthenias, diarrhea, and fatigue. In addition it must be used with caution in patients with a history of seizure due to rare incidence of this during therapy.14,15 Apalutamide similarly has been associated with fatigue, diarrhea, rash, hypothyroidism, and rarely it was associated with ischemic cardiovascular events.16,21 Consequently, providers should be thoughtful and take a patient’s overall functional status, health, and comorbidities into close consideration when selecting an agent. Table 2 summarizes the pharmacokinetics of each agent, suggested monitoring, adverse effects, and level of evidence supporting the studies examining their use in this population.
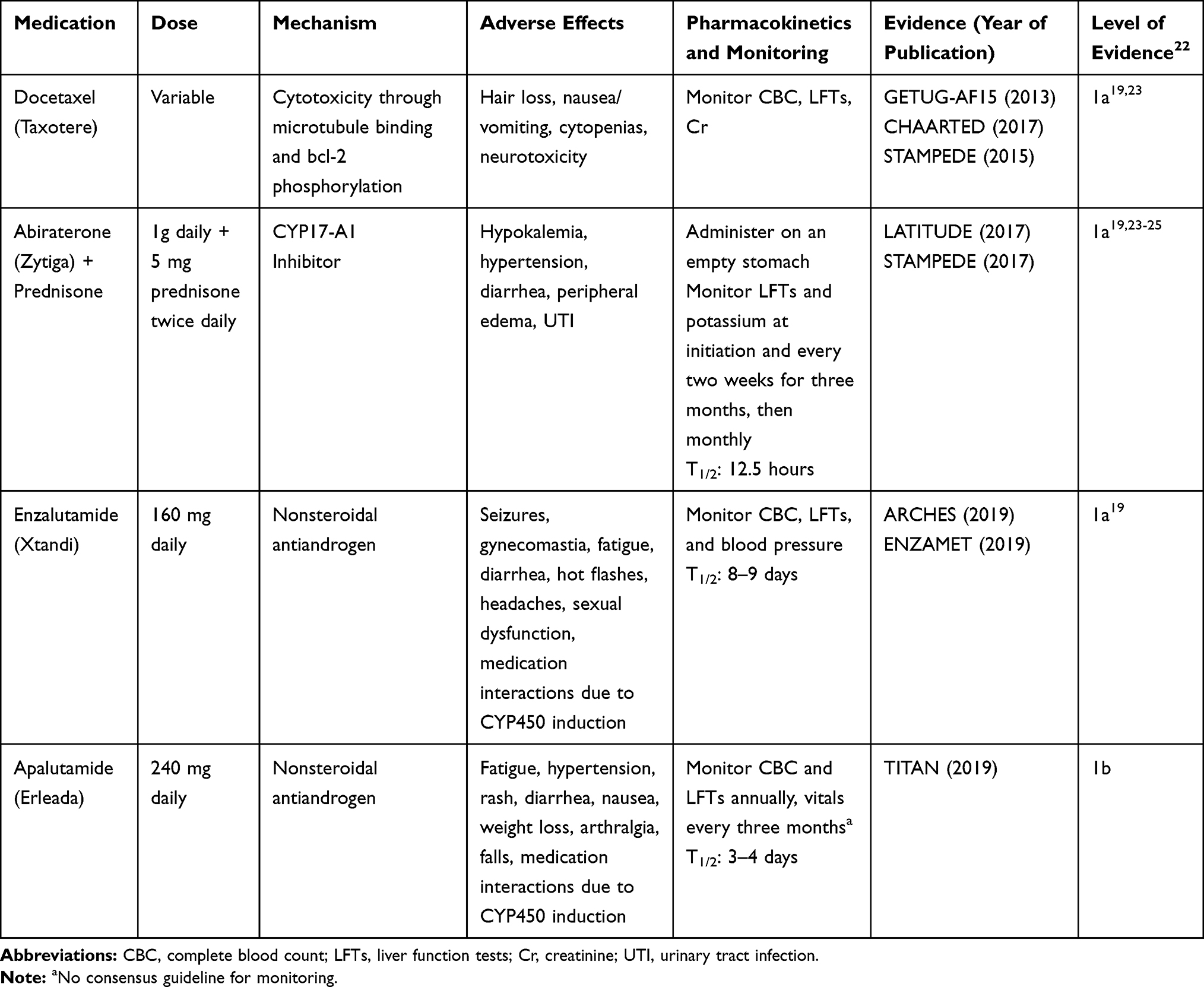 |
Table 2 Agents with Survival Benefit in Metastatic Hormone-sensitive Prostate Cancer |
The evidence for optimal sequencing of these agents remains relatively sparse and varies in its application, as these agents have been approved for multiple indications within advanced prostate cancer and much of the literature to date has been focused within the mCRPC space. Factors such as concern for acquired resistance, the potential for cross-resistance, and the timing of cytotoxic chemotherapy drive investigations into optimal timing. A randomized control trial in mCRPC patients sought to determine optimal sequencing of abiraterone and enzalutamide, as well as their second-line efficacy.26 Two hundred and two patients were randomly assigned to one of the two drugs, which they continued until the time of either PSA, clinical, or radiographic progression, or unacceptable treatment toxicity, and were then switched to the alternate agent until progression again occurred. Using a primary endpoint of second PSA progression (defined as the time from start of initial therapy to the time of PSA progression on second-line therapy after crossover), the investigators observed increased benefit (median 19.3 months vs 15.2 months) with the sequence of abiraterone followed by enzalutamide than with the opposite (HR: 0.66, 95%CI: 0.45–0.97, p=0.036). They also observed improved second-line activity with enzalutamide than with abiraterone (median time to second PSA progression 3.5 months vs 1.7 months, HR: 0.42, 95%CI: 0.28–0.65, p<0.0001).26 Others have proposed alternating androgen-targeting therapies and cytotoxic chemotherapies. The CARD study in the mCRPC population examined the use of cabazitaxel, a next-generation taxane, vs switch to another androgen-targeted inhibitor (abiraterone or enzalutamide) in patients who had previously been treated with docetaxel and either abiraterone or enzalutamide. They observed improved imaging-based PFS in the group receiving cabazitaxel (HR: 0.54, 95%CI: 0.40–0.73, p<0.001) than in the group receiving an androgen-signaling-targeted inhibitor (ie either abiraterone or enzalutamide), as well as improved OS (13.6 mo vs 11 mo, HR: 0.64, 95%CI: 0.46–0.89, p=0.008), suggesting that alternating treatment mechanisms of action may have improved overall benefit.27 However, these data are not strong enough to drive prescriptive treatment recommendations.
The financial toxicity of these novel androgen-axis inhibitors must also be considered as monthly costs regularly exceed $10,000 USD. Although funding is jurisdiction-specific, patient-borne costs are significant even for those with health insurance. Pricing can be difficult to fully assess given differences in insurance reimbursement and payment methods, but a search of the general prices of these drugs quickly highlights their steep costs. When compared on drugs.com as of February 2020, the quoted prices are as follows: For abiraterone, $94.80 per 250 mg pill ($379 daily, $11,376 monthly), for enzalutamide, $103.77 per 40 mg pill ($415 daily, $12,452 monthly), and for apalutamide, $106.61 per 60 mg pill ($426 daily, $12,793 monthly).28 For patients without the personal means to afford many of these oral therapies, compassionate use programs have often provided coverage. Given similar efficacy and much lower cost, health economic analyses favor the use of docetaxel in this disease space with an incremental cost-effectiveness ratio (ICER) that is almost one-tenth that of abiraterone, which makes this a viable, more cost-effective option for many patients.29 Abiraterone is now available as a generic formulation; as additional generic options emerge, cost will hopefully lessen. Finally, a 2018 study examined lower doses (1/4 standard dose) of abiraterone taken with food, finding that this dosing strategy resulted in similar PSA response and time to progression as full dose abiraterone taken fasting, which suggests the possibility of decreasing recommended dosing and thus, cost.30 At the present, however, cost continues to remain noteworthy during patient and physician selection.
Agents Without Survival Benefits
Although the evidence for the agents discussed so far is promising, additional agents have also been studied which have not shown benefit in prolonging OS. Bisphosphonates such as zoledronic acid have been examined based on the theory that reducing skeletal-related events may be of overall benefit in the course of metastatic prostate cancer. Sodium clodronate, a first-generation bisphosphonate, was examined in 2003 during the MRC PR05 trial. In this trial 311 men with metastatic prostate cancer who were on ADT were randomized to receive either oral sodium clodronate or placebo. At a median follow-up of 59 months, no statistical difference was detected in either bone PFS (the primary outcome measure) or OS with the addition of the drug.31 The STAMPEDE trial, as mentioned above, also added zoledronic acid as an additional experimental agent, comparing ADT alone to ADT plus zoledronic acid, as well as ADT plus docetaxel plus zoledronic acid to ADT plus docetaxel. In comparing the addition of zoledronic acid alone to ADT, there was no evidence of an OS advantage (HR: 0.94, 95%CI: 0.79–1.11). In adding zoledronic acid to ADT plus docetaxel, both groups had an OS advantage compared to ADT alone but there was no evidence of an advantage of adding zoledronic acid to docetaxel (HR: 1.06, 95%CI: 0.86–1.30, p=0.592).9
Since 2003, multiple additional trials have been performed evaluating the use of bisphosphonates in the metastatic hormone-sensitive space. The CALGB 90202 trial in 2014 did not demonstrate an increased time to first skeletal related event, PFS, or OS with the addition of zoledronic acid to ADT.32 Similarly, the ZAPCA trial in 2017 overall did not demonstrate increased time to treatment failure (as defined either by PSA or clinical progression, skeletal-related event, or death or discontinuation of treatment for any reason) or improvement in OS with the addition of zoledronic acid to ADT. That said, they did postulate there may be increased time to reaching castration-resistance with addition of zoledronic acid in a select predefined subgroup of patients with PSA <200 (time to treatment failure 9.8 months with ADT alone vs 23.7 months with addition of zoledronic acid, HR: 0.58, 95%CI: 0.35–0.93, log-rank p=0.023).33
STAMPEDE also examined the use of celecoxib, a nonsteroidal anti-inflammatory drug, in patients with metastatic disease in the early phases of their trial. Five hundred and eighty-four patients from the subgroups randomized to ADT alone (control) vs ADT plus celecoxib were analyzed. There was no evidence of failure-free survival benefit with celecoxib at an interim analysis, and therefore, the independent data-monitoring committee stopped accrual of this cohort and celecoxib in patients on the drug.34
Systemic Therapy Future Directions
New agents are constantly being developed and evaluated in the mHSPC space. The ARASENS trial, which began in June 2016, is targeting enrollment of 1300 patients with metastatic prostate cancer and seeks to compare ADT plus docetaxel plus darolutamide (a next-generation antiandrogen) to ADT plus docetaxel alone. As mentioned above, given the advent of more recent changes in therapy for metastatic castrate-sensitive disease, it notably uses ADT plus docetaxel as the standard of care treatment and examines the addition of darolutamide to this regimen. Given the favorable results with darolutamide in the castrate-resistant space, this may also have a role within the early mHSPC realm.35,36
The Role of Surgery, Radiotherapy, and Ablation in Oligometastatic Prostate Cancer
The concept of oligometastatic prostate cancer is an evolving paradigm, principally as a result of the rapid advancement of diagnostic and molecular-imaging modalities. As imaging techniques have become more sensitive, the detection of previously occult prostate cancer raises the question of whether patients with low-volume metastatic disease should be treated with targeted therapy, observation, or systemic therapy, as described above. In men with mHSPC there are two related, but independent, questions: first, is there benefit with treatment of the primary tumor in patients with low volume metastatic disease and second, is there benefit with treatment of metastatic disease sites?
With regard to the first question, a SEER analysis of 8185 men diagnosed with metastatic prostate cancer from Culp et al found that definitive treatment of the prostate with radical prostatectomy or local radiation conferred a significant OS and DSS benefit (67.4% OS and 75.8% DSS for RP, vs 52.6% OS and 61.3% DSS for RT, vs 22.5% OS and 48.7% DSS for no local treatment; p<0.001).37 Men undergoing local treatment of the prostate also experienced fewer local symptoms and complications of disease progression.
Subsequently, several trials have sought to assess the impact of radiotherapy to the prostate in the setting of metastatic disease. The HORRAD trial randomized 432 patients with metastatic prostate cancer and bone metastases to receive external beam radiation therapy (EBRT) of the prostate with ADT vs ADT alone. Sixty-three percent of patients had five or more osseous metastases, and median follow-up was 47 months.38 They found OS was not statistically different between groups with a median survival of 45 months in the group receiving EBRT (95%CI: 40.4–49.6) vs 43 months in the control group (95%CI: 32.6–53.4). Similarly, there was no significant difference in PSA recurrence-free survival (HR: 0.86, 95%CI: 0.69–1.08, p=0.20), with a mean time to progression in the EBRT group of 15 months (95%CI: 11.8–18.2) vs 12 months in the control group (95%CI: 10.6–13.4).38
Another arm of the STAMPEDE trial (arm H) also sought to examine the effect of radiotherapy to the prostate in metastatic disease.39 In this arm, 2061 patients with metastatic disease were randomized to receive EBRT plus standard systemic therapy (ADT ± docetaxel), vs standard systemic therapy alone (ADT ± docetaxel). 89% of the study population had osseous metastases, and overall metastatic burden was defined as low-volume in 40%, high-volume in 54%, and unknown in the remainder. Over a median follow-up of 37 months, there was no benefit in OS demonstrated in those receiving EBRT (HR: 0.92, 95%CI: 0.80–1.06, p=0.266). In a prespecified subgroup analysis of patients with low metastatic burden, however, there was a significant improvement in OS (HR: 0.68, 95%CI: 0.52–0.90, p=0.0007).39
SWOG 1802 (NCT03678025) is an ongoing study that sets out to compare OS, PFS, and rate of symptomatic local progression utilizing standard systemic therapy with or without local therapy (radical prostatectomy or radiation) in men with mHSPC.40 Randomized prospective trials such as this will better clarify the subset of patients who may benefit from local treatment in the face of metastatic disease.
A number of studies assess the second question of whether there is benefit to treatment of metastatic disease sites, both in prostate cancer and oncologic disease in general. Ost et al recently published the first randomized evidence supporting the role of image-guided metastasis-directed therapy (MDT) in the setting of oligometastatic HSPC. Sixty-two men with biochemical recurrence after primary prostate cancer treatment and three or fewer extracranial metastatic lesions on choline-PET underwent observation vs surgery or stereotactic body radiotherapy (SBRT or SABR) of metastatic lesions and were followed until developing symptomatic or metastatic progression on imaging. At a median follow-up of three years, the primary outcome of median ADT-free survival was 13 months for the surveillance group and 21 months for the MDT group (HR: 0.60, 80%CI: 0.40–0.90, log-rank p=0.11). Quality of life remained similar between groups and toxicity was low. Therefore, while this was a relatively small phase II study, benefit was demonstrated in delaying disease progression and initiation of hormonal therapy with the select treatment of metastases in men with hormone-sensitive disease.41 This supports data from several nonrandomized studies, including Suardi et al, who found a 59% biochemical response and 38% eight-year recurrence-free survival for salvage lymph node dissection after BCR in HSPC patients with lymph node metastases.42
In 2019, the SABR-COMET trial was published, which assessed the use of SABR to oligometastatic disease sites.43 Patients with various types of metastatic malignancy (primarily breast, colorectal, lung, and prostate) and up to five sites of metastatic disease were randomized to receive either standard palliative-care treatments vs standard of care treatments plus SABR to all sites of metastatic disease. Standard of care treatments, follow-up imaging, and decision to treat new metastatic sites if disease progression occurred (in the SABR group) was up to the discretion of the treating physician. Ninety-nine patients were enrolled with a 2:1 ratio of randomization to the SABR vs the control group. At a median follow-up of 25.5 months, the median OS in the control group was 28 months (95%CI: 19–33) vs 41 months (26 not reached) in the SABR group (HR: 0.57, 95%CI: 0.30–1.10, stratified log-rank p=0.090). Twenty-six of the 66 patients (39%) in the SABR group were still alive at study end. Adverse events grade 2 or higher were noted in three (9%) patients in the control group and 19 (29%) in the SABR group (p=0.026), with the most common being pain, (12%), fatigue (6%), and dyspnea (3%). There were three (4.5%) treatment-related deaths in the SABR group, and none in the control group. Overall, the authors concluded that in patients with metastatic disease, SABR was associated with a 13-month improvement in OS, although these groups did experience more toxicity and adverse events with treatment.43
The budding field of theranostics, which utilizes prostate-specific membrane antigen (PSMA) bound radionuclide-labeled molecular targets, is also being explored in metastatic prostate cancer treatment. Its utility is both as a diagnostic and therapeutic modality. Initial safety and efficacy studies using7,17 Lutetium-labeled PMSA have shown durable PSA response improvement and symptomatic relief in men with metastatic CRPC.44 This therapy is being investigated within other applications in advanced prostate cancer, along with additional α-emitting PMSA agents and other experimental formulations.45
Conclusions
The landscape of treatment for metastatic HSPC has changed substantially over the last decade and continues to evolve with the advent of new systemic agents, use of surgery and radiotherapy in oligometastatic disease, and evolving role of theranostics. While treatment with ADT alone was long considered the standard of care for men with newly diagnosed metastatic prostate cancer, this is no longer the case. Multiple trials in the mHSPC space are enrolling worldwide, which will continue to elucidate the role and sequence of administration for each of these agents and more. As treatment options continue to become available and the data supporting their use evolves, clinicians should be aware of the foundational data, look to foreseeable comparative studies, as well as practice informed and shared decision-making in treating men with metastatic prostate cancer.
Disclosure
Dr Kelvin A Moses reports personal fees from Astellas, Pfizer, and Dendreon, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
2. Butler SS, Muralidhar V, Zhao SG, et al. Prostate cancer incidence across stage, NCCN risk groups, and age before and after USPSTF Grade D recommendations against prostate-specific antigen screening in 2012. Cancer. 2019;126(4):717–724. doi:10.1002/cncr.32604
3. Kelly SP, Anderson WF, Rosenberg PS, Cook MB. Past, current, and future incidence rates and burden of metastatic prostate cancer in the United States. Eur Urol Focus. 2018;4(1):121–127. doi:10.1016/j.euf.2017.10.014
4. Uemura H, Ye D, Kanesvaran R, et al. United in fight against prOstate cancer registry (UFO): first results from a large, multi-centre, prospective, longitudinal cohort study of advanced prostate cancer in Asia. BJU Int. 2019.
5. Teo MY, Rathkopf DE, Kantoff P. Treatment of advanced prostate cancer. Annu Rev Med. 2019;70:479–499. doi:10.1146/annurev-med-051517-011947
6. Wu JN, Fish KM, Evans CP, Devere White RW, Dall’Era MA. No improvement noted in overall or cause-specific survival for men presenting with metastatic prostate cancer over a 20-year period. Cancer. 2014;120(6):818–823. doi:10.1002/cncr.28485
7. Gravis G, Boher JM, Joly F, et al. Androgen deprivation therapy (ADT) plus docetaxel versus ADT alone in metastatic non castrate prostate cancer: impact of metastatic burden and long-term survival analysis of the Randomized Phase 3 GETUG-AFU15 Trial. Eur Urol. 2016;70(2):256–262. doi:10.1016/j.eururo.2015.11.005
8. Gravis G, Fizazi K, Joly F, et al. Androgen-deprivation therapy alone or with docetaxel in non-castrate metastatic prostate cancer (GETUG-AFU 15): a randomised, open-label, phase 3 trial. Lancet Oncol. 2013;14(2):149–158. doi:10.1016/S1470-2045(12)70560-0
9. James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016;387(10024):1163–1177. doi:10.1016/S0140-6736(15)01037-5
10. Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015;373(8):737–746. doi:10.1056/NEJMoa1503747
11. Tucci M, Bertaglia V, Vignani F, et al. Addition of docetaxel to androgen deprivation therapy for patients with hormone-sensitive metastatic prostate cancer: a systematic review and meta-analysis. Eur Urol. 2016;69(4):563–573. doi:10.1016/j.eururo.2015.09.013
12. James ND, de Bono JS, Spears MR, et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med. 2017;377(4):338–351. doi:10.1056/NEJMoa1702900
13. Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017;377(4):352–360. doi:10.1056/NEJMoa1704174
14. Armstrong AJ, Szmulewitz RZ, Petrylak DP, et al. ARCHES: a randomized, phase iii study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J Clin Oncol. 2019;37(32):2974–2986. doi:10.1200/JCO.19.00799
15. Davis ID, Martin AJ, Stockler MR, et al. enzalutamide with standard first-line therapy in metastatic prostate cancer. N Engl J Med. 2019;381(2):121–131. doi:10.1056/NEJMoa1903835
16. Chi KN, Agarwal N, Bjartell A, et al. Apalutamide for metastatic, castration-sensitive prostate cancer. N Engl J Med. 2019;381(1):13–24. doi:10.1056/NEJMoa1903307
17. National comprehensive cancer network. Prostate cancer (Version 4.2019). Available from: https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.
18. Wallis CJD, Klaassen Z, Bhindi B, et al. comparison of abiraterone acetate and docetaxel with androgen deprivation therapy in high-risk and metastatic hormone-naive prostate cancer: a systematic review and network meta-analysis. Eur Urol. 2018;73(6):834–844. doi:10.1016/j.eururo.2017.10.002
19. Sathianathen NJ, Koschel S, Thangasamy IA, et al. Indirect comparisons of efficacy between combination approaches in metastatic hormone-sensitive prostate cancer: a systematic review and network meta-analysis. Eur Urol. 2019.
20. Marchioni M, Di Nicola M, Primiceri G, et al. new anti-androgen compounds compared to docetaxel in metastatic hormone sensitive prostate cancer: results from a network meta-analysis. J Urol. 2019;101097JU0000000000000636.
21. Smith MR, Saad F, Chowdhury S, et al. apalutamide treatment and metastasis-free survival in prostate cancer. N Engl J Med. 2018;378(15):1408–1418. doi:10.1056/NEJMoa1715546
22. CEBM(Centre for Evidence-Based Medicine). Oxford centre for evidence-based medicine-levels of evidence (March 2009); 2009. Available from: http://www.cebm.net/index.aspx?o=1025.
23. Di Nunno V, Santoni M, Mollica V, et al. Systemic treatment for metastatic hormone sensitive prostate cancer: a comprehensive meta-analysis evaluating efficacy and safety in specific sub-groups of patients. Clin Drug Investig. 2020;40(3):211–226. doi:10.1007/s40261-020-00888-5
24. Rydzewska LHM, Burdett S, Vale CL, et al. Adding abiraterone to androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer: A systematic review and meta-analysis. Eur J Cancer. 2017;84:88–101. doi:10.1016/j.ejca.2017.07.003
25. Tan PS, Aguiar P
26. Khalaf DJ, Annala M, Taavitsainen S, et al. Optimal sequencing of enzalutamide and abiraterone acetate plus prednisone in metastatic castration-resistant prostate cancer: a multicentre, randomised, open-label, Phase 2, crossover trial. Lancet Oncol. 2019;20(12):1730–1739. doi:10.1016/S1470-2045(19)30688-6
27. de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus abiraterone or enzalutamide in metastatic prostate cancer. N Engl J Med. 2019;381(26):2506–2518. doi:10.1056/NEJMoa1911206
28. Drugs.com. Drug Price Information; 2020. Available from: https://www.drugs.com/price-guide/.
29. Sathianathen NJ, Alarid-Escudero F, Kuntz KM, et al. A cost-effectiveness analysis of systemic therapy for metastatic hormone-sensitive prostate cancer. Eur Urol Oncol. 2019;2(6):649–655. doi:10.1016/j.euo.2019.01.004
30. Szmulewitz RZ, Peer CJ, Ibraheem A, et al. Prospective international randomized phase ii study of low-dose abiraterone with food versus standard dose abiraterone in castration-resistant prostate cancer. J Clin Oncol. 2018;36(14):1389–1395. doi:10.1200/JCO.2017.76.4381
31. Dearnaley DP, Sydes MR, Mason MD, et al. A double-blind, placebo-controlled, randomized trial of oral sodium clodronate for metastatic prostate cancer (MRC PR05 Trial). J Natl Cancer Inst. 2003;95(17):1300–1311. doi:10.1093/jnci/djg038
32. Smith MR, Halabi S, Ryan CJ, et al. Randomized controlled trial of early zoledronic acid in men with castration-sensitive prostate cancer and bone metastases: results of CALGB 90202 (alliance). J Clin Oncol. 2014;32(11):1143–1150. doi:10.1200/JCO.2013.51.6500
33. Kamba T, Kamoto T, Maruo S, et al. A phase III multicenter, randomized, controlled study of combined androgen blockade with versus without zoledronic acid in prostate cancer patients with metastatic bone disease: results of the ZAPCA trial. Int J Clin Oncol. 2017;22(1):166–173. doi:10.1007/s10147-016-1037-2
34. James ND, Sydes MR, Mason MD, et al. Celecoxib plus hormone therapy versus hormone therapy alone for hormone-sensitive prostate cancer: first results from the STAMPEDE multiarm, multistage, randomised controlled trial. Lancet Oncol. 2012;13(5):549–558. doi:10.1016/S1470-2045(12)70088-8
35. Bastos DA, Antonarakis ES. Darolutamide for castration-resistant prostate cancer. Onco Targets Ther. 2019;12:8769–8777. doi:10.2147/OTT.S197244
36. ODM-201 in addition to standard adt and docetaxel in metastatic castration sensitive prostate cancer. Available from: https://ClinicalTrials.gov/show/NCT02799602.
37. Culp SH, Schellhammer PF, Williams MB. Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur Urol. 2014;65(6):1058–1066. doi:10.1016/j.eururo.2013.11.012
38. Boeve LMS, Hulshof M, Vis AN, et al. Effect on survival of androgen deprivation therapy alone compared to androgen deprivation therapy combined with concurrent radiation therapy to the prostate in patients with primary bone metastatic prostate cancer in a prospective randomised clinical trial: data from the HORRAD trial. Eur Urol. 2019;75(3):410–418. doi:10.1016/j.eururo.2018.09.008
39. Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): a randomised controlled phase 3 trial. Lancet. 2018;392(10162):2353–2366. doi:10.1016/S0140-6736(18)32486-3
40. Standard systemic therapy with or without definitive treatment in treating participants with metastatic prostate cancer. Available from: https://ClinicalTrials.gov/show/NCT03678025.
41. Ost P, Reynders D, Decaestecker K, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase ii trial. J Clin Oncol. 2018;36(5):446–453. doi:10.1200/JCO.2017.75.4853
42. Suardi N, Gandaglia G, Gallina A, et al. Long-term outcomes of salvage lymph node dissection for clinically recurrent prostate cancer: results of a single-institution series with a minimum follow-up of 5 years. Eur Urol. 2015;67(2):299–309. doi:10.1016/j.eururo.2014.02.011
43. Palma DA, Olson R, Harrow S, et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial. Lancet. 2019;393(10185):2051–2058. doi:10.1016/S0140-6736(18)32487-5
44. Baum RP, Kulkarni HR, Schuchardt C, et al. 177Lu-labeled prostate-specific membrane antigen radioligand therapy of metastatic castration-resistant prostate cancer: safety and efficacy. J Nucl Med. 2016;57(7):1006–1013. doi:10.2967/jnumed.115.168443
45. Virgolini I, Decristoforo C, Haug A, Fanti S, Uprimny C. Current status of theranostics in prostate cancer. Eur J Nucl Med Mol Imaging. 2018;45(3):471–495. doi:10.1007/s00259-017-3882-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.