Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Metacognitive Beliefs, Cognitive Functioning, Psychiatric Symptoms and Empathy in People with Schizophrenia
Authors Chuang SP ![]() , Wu JYW, Wang CS
, Wu JYW, Wang CS
Received 9 April 2021
Accepted for publication 17 June 2021
Published 7 July 2021 Volume 2021:17 Pages 2209—2217
DOI https://doi.org/10.2147/NDT.S313932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Shu Ping Chuang,1 Jo Yung Wei Wu,2 Chien Shu Wang3
1Department of Psychiatry, Zuoying Branch of Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan; 2Good-Day Psychology Clinic, Tainan, Taiwan; 3Department of Psychiatry, Kaohsiung Armed Forces General Hospital, Kaohsiung, Taiwan
Correspondence: Shu Ping Chuang
Department of Psychiatry, Zuoying Branch of Kaohsiung Armed Forces General Hospital, No. 553, Jiunshiau Road, Zuoying District, Kaohsiung, 81342, Taiwan
Tel +886-7-5817121 #3352
Fax +886-7-5818816
Email [email protected]
Background: People with schizophrenia often exhibit deficits in empathy, which plays a major role in social cognition and interpersonal relationship. However, little work has investigated potential factors that influence empathy in schizophrenia. The study aimed to investigate the relationship among metacognition, psychiatric symptoms, cognitive functioning and empathy in patients diagnosed with schizophrenia.
Methods: Forty-eight people with schizophrenia were enrolled in the study group. All subjects participated in the metacognitions questionnaire-30 (MCQ-30), brief psychiatric rating scale (BPRS), neurocognitive functioning, interpersonal reactivity index (IRI), and the pictorial empathy test (PET).
Results: Stepwise regression analysis revealed that cognitive self-consciousness (domain of metacognitions questionnaire-30) accounted for 37% of the variance in perspective taking scores (domain of interpersonal reactivity index). Resistance (subscale of brief psychiatric rating scale) and positive beliefs about worry (domain of metacognitions questionnaire-30) accounted for 34% of the variance in fantasy (domain of interpersonal reactivity index). Activation (subscale of brief psychiatric rating scale) was a significant predictor for empathic concern (domain of interpersonal reactivity index). Resistance, cognitive confidence (domain of metacognitions questionnaire-30), intellectual processes and inhibitory control (go-no-go task) accounted for 38% of the variance in personal distress. Negative symptoms (subscale of brief psychiatric rating scale) and cognitive self-consciousness were significant predictors for the pictorial empathy test.
Conclusion: The study was aimed to examine self-perception of metacognitive beliefs and empathy. More research is needed to explore the association between metacognitive beliefs, cognitive functioning and psychiatric symptoms on empathy in people with schizophrenia.
Keywords: empathy, metacognitive beliefs, psychiatric symptoms, cognitive functioning, schizophrenia
Introduction
Empathy is a complex construct of interpersonal relationships that allow us to understand and respond to the emotional experiences of others.1,2 Empathy is a multidimensional construct that includes cognitive and affective components.3–5 Cognitive empathy could be defined as the capacity to infer others’ mental states, such as understanding others’ thoughts and perspective taking. Affective empathy refers to the perception and response of the emotional states or experiences of other people.6,7 Empathy contributes to the development of interpersonal networks, forgiveness and altruism.7–9 Individuals with schizophrenia showed lower objective empathic resonance compared to the healthy group and the self-rated empathic concern did not correlate with objective empathic resonance. The two groups showed no significant differences in self-rated empathic concern.10 Several meta-analysis studies indicated that people with schizophrenia showed medium deficits in objective affective empathy, reduced self-rated empathy (including perspective-taking, fantasy, empathic concern, and greater reduced personal distress) compared to the healthy group.11,12 Broadly speaking, people with schizophrenia may have difficulty in understanding and experiencing emotional connections with others and the reduced empathic ability are thought to play an important role in social interaction.13,14 Although most studies have demonstrated deficits of empathy in schizophrenia, less is known about their potential factors. One important potential factor in terms of metacognition involves the thinking about thoughts, feelings and mental experiences to form integrated representations of self and others.15,16 Hasson-Ohayon et al17 showed that metacognition may overlap with social cognition (of which empathy was one domain). However, some results indicated the two constructs were independent and have different impact outcomes in schizophrenia.17,18 Two different measures are used to assess metacognitive capacity, including the objective metacognition assessment scale-abbreviated19 (MSA) and subjective metacognition questionnaire20 (MCQ-30).
The MAS-A assessed the capacity to conceptualize reflections about the self and others and used multiple perspectives to cope with information in the face of psychosocial challenges; the MCQ-30 assessed metacognitive beliefs, beliefs related to worry, cognitive confidence, self-consciousness and need for control. The results by Bonfils et al21 found through correlational analyses that empathy was not correlated with metacognitive self-reflectivity (subscale of MAS-A) in people with schizophrenia-spectrum disorders. Low metacognitive self-reflectivity was a moderator between reduced ability to tolerate distress and have less empathy. Another study showed that metacognition was positively associated with cognitive and affective empathy performance in people with schizophrenia or schizoaffective disorder.22 However, these studies use objective measures of empathy or metacognition, and not focusing attention on their self-perception of empathy and metacognition. No study has yet examined an in-depth understanding of the relationship between domains of empathy and domains of metacognitive beliefs. Little is known about how people with schizophrenia view their own empathic and metacognitive beliefs experiences.
A few studies demonstrated that people with schizophrenia have several impaired cognitive functions (including immediate memory, language, delayed memory, verbal ability, processing speed, verbal learning and executive function) compared to healthy samples.23,24 Cognitive deficits have an effect on functional outcomes25 that may contribute to their deficits in empathic response. Different response in empathy may reflect the strength of mental flexibility.26,27 In other words, deficits in specific aspects of empathy may reflect a breakdown in neurocognitive processes. Subjective empathy was not correlated with verbal skills (information test, subscale of WAIS-R and verbal fluency), working memory (auditory consonant trigrams) and executive function (Stroop color-word test) in schizophrenia.28 Objective cognitive empathy mediated the relationship between working memory and social competence.14 The prefrontal activation during objective empathic performances was positively predicted by working memory in the healthy group.29 The inconsistent results may be due to the different cognitive functioning measures, subjective and objective empathy tests. The neurocognitive assessment used in this study included cognitive flexibility, inhibition control, receptive speech, memory and intellectual processes.
Some studies showed that greater fantasy (domain of empathy) increases hallucinations and delusions in schizophrenia30 and greater fantasy has been correlated with psychosis risk (ie, a history of subclinical delusional ideation) in relatives of schizophrenia.31 The results by Montag et al32 indicated that decreased perspective taking ratings of empathy was correlated with an increased duration of illness. It seemed that empathy may be affected by these psychiatric symptoms and duration of illness.
This exploratory study aimed at investigating various aspects of empathy in chronic and remitted schizophrenic patients by using a self-reported questionnaire of empathy and metacognitive beliefs. Furthermore, we explored the impact of psychiatric symptoms and neuropsychological function and empathy. We also included objective assessments of affective-empathy (the pictorial empathy test; PET) to investigate empathy and metacognition beliefs. It is important to note that self-reported empathy and actual empathic responding may not be correlated.33 Unlike many questionnaires which are retrospective in nature, the PET is short and easy to complete and the empathic feelings could be captured immediately. Furthermore, a photo-based measure has stronger ecological validity compared to questionnaires and may facilitate responding in clinical samples who have difficulty expressing their responses in questionnaires.34
Thus, the purpose of the present study attempted to understand the extent to which duration of illness, psychiatric symptoms, metacognitive beliefs and neuropsychological factors were independently related to empathy in people with schizophrenia.
Methods
Participants
The study protocol was reviewed and approved by Kaohsiung Armed Forces General Hospital institutional review board. Prior to receiving assessments, written informed consent was obtained from all participants. This study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki (1964). Patients were excluded if they met the diagnostic criteria of active substance dependence, acute depressive episode, acute psychotic episode, intellectual disabilities, organic brain disease, and irregular medication adherence and decreased functional abilities. We approached 65 patients by telephone to request their participation in the study; ten patients refused to participate due to work or lengthiness to attend the study. Seven patients were excluded due to intellectual disabilities, irregular medication adherence and decreased functional abilities.
Forty-eight schizophrenia outpatients were interviewed using the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria35 (American Psychiatric Association, 2013) from the department of psychiatry at the Zuoying Branch of Kaohsiung Armed Forces General Hospital in Taiwan from March 2 to October 30, 2020. All participants were stably adhered on medical treatment (stably adhered on medical regimen without changes in the dosage of medications and hospitalization within 30 days) and currently in the chronic phase of disorder (average of twenty years of illness duration) at time of study. The average onset was 26 years old and only three participants were currently employed.
Measurement
Interpersonal Reactivity Index (IRI)
The IRI is a 28-item self-reported scale used to assess two components of empathy, including cognitive and affective aspects of empathy (I). Perspective taking: the tendency to spontaneously adopt another psychological perspective. (II). Fantasy: the participants’ tendency to transpose themselves imaginarily of fictitious characters in books, movies. (III). Empathic concern: other-oriented feelings of emotion and concerns for unfortunate others. (IV). Personal distress: self-oriented feelings of personal discomfort or unease in tense interpersonal contexts. All items are answered using a 5-point Likert scale ranging from 1 (does not describe me well) to 4 (describes very well). Items with negative statements are reverse scored and higher scores indicated higher empathy.36
The Pictorial Empathy Test (PET)
It includes seven photographs of people with physical and/or emotional distress and is thought to assess affective empathy. Participants were asked “How emotionally touching do you find the photograph?” and rated a 5-point Likert scale from “not at all” to “very much” on each photograph. The PET is scored by calculating the average score.34 The PET displayed high internal consistency and good seven-month test-retest reliability and supported convergent and discriminant validity.
Metacognitions Questionnaire-30 (MCQ-30)
The MCQ-30 is a 30-item self-report measured on five dimensions of metacognitive beliefs in a range of mental health conditions.20 (I) Cognitive confidence (eg, “I have a poor memory”; “My memory can mislead me at times”). (II) Positive beliefs about worry (eg, “I need to worry in order to remain organized”; “Worrying helps me cope”). (III) Cognitive self-consciousness (“I think a lot about my thoughts”; “I monitor my thoughts”). (IV) Negative beliefs about uncontrollability and danger (“My worrying is dangerous for me”; “My worrying could make me go mad”). (V) Need to control thoughts (“If I did not control a worrying thought, and then it happened, it would be my fault”; “I should be in control of my thoughts all of the time”). Higher scores indicated greater dysfunctional metacognitive beliefs. The MCQ-30 has good reliability and validity.37
Brief Psychiatric Rating Scale (BPRS)
The BPRS is an 18-item scale to measure a number of symptoms, including five subscales: affect (anxiety, guilt, depression, somatic), positive symptoms (grandiosity, unusual thought, hallucinatory behavior content, conceptual disorganization), negative symptoms (motor retardation, blunted affect, emotional withdrawal), resistance (suspiciousness, hostility, uncooperativeness), and activation (tension, excitement, mannerisms and posturing). The items were scored by a clinician based on a 7-point scale ranging from 1 (not present) to 7 (extremely severe) and total scores ranged from 18 to 126, with the higher scores indicating greater severity of symptoms.38,39
Subtests of Test of Attentional Performance (TAP)
The TAP is designed for the assessment of attentional deficits in children and adults with cerebral lesions. Participants were orally instructed to perform the computerized tasks during pretest trials before entering test trials.40
(1). The flexibility task: the “set shifting” task. The simple condition: requires the participant to place each hand on a separate response button on which a letter and a number are displayed simultaneously on screen. The participant has to press the left or right button according to whether the target stimulus (eg, a letter or a number) appears to the left or the right side. The complex condition: requires the participant to follow alternating target stimulus (the order is letter-number and so on; if the participant makes the wrong response, the target stimulus will be marked and the participant would be asked to press it. On the next trial, an alternated order may be presented, such as, number-letter).
(2). The inhibition task (inhibitory control): the task examines the ability to perform an appropriate response under time pressure and to simultaneously inhibit an inappropriate response. Test form “1 of 2”: an up-right (+) and a diagonal cross (x) are presented in an altering sequence on the screen. The participant has to press the button as quickly as possible whenever the diagonal cross appears.
Subtests of Luria-Nebraska Neuropsychological Battery-Screening test Form-I (LNNB)
The LNNB Form-I is a standardized and multidimensional battery to access a range of neuropsychological impairments. It includes 269 items, 11 clinical scales, five summary scales, eight localization scales and twenty-eight factor scales. Higher scores indicated more cognitive deficits in that area.41
(1) C5 (Receptive Speech): The scale examined the capacity of participants to understand receptive speech, from simple phonemic analysis to complex sentences.
(2) C10 (Memory): The scale examined short-term and intermediate memory, including verbal and non-verbal memory.
(3) C11 (Intellectual Processes): The scale is differentiated from a standardized intelligence test and tends to evaluate a functional intellectual level, including complex reasoning and problem solving skills.
Statistical Analysis
Study data were evaluated using SPSS 22.0 software. Mean standard deviation and percentages were calculated. Pearson correlation analysis was performed for duration of illness, brief psychiatric symptoms, metacognitive beliefs, cognitive functioning, and empathy questionnaires. The significance level for all statistical analyses was set at p < 0.05 (2-tailed test). Step-wise linear regression analyses were performed to explore the relative contribution of each significant variable between metacognitive beliefs, cognitive functioning and brief psychiatric symptoms as independent variables, and empathy as a dependent variable.
Results
Sample Description
Sample demographics were as follows: The mean age of the participants was 46.4 years (SD=9.8). Only 6.3% of the participants were currently employed who were blue-collar workers (Table 1). Description of clinical variables is presented in Table 2. Duration of illness was not correlated with the domains of IRI and PET, respectively. Perspective taking was positively correlated with cognitive self-consciousness (r=0.624). Fantasy was significantly correlated positively with resistance (r=0.412), cognitive confidence (r=0.380), positive beliefs about worry (r=0.493) and need to control thoughts (r=0.356). Empathic concern was positively associated with affect (r=0.311) and activation (r=0.313). Personal distress was positively correlated with affect (r=0.30), resistance (r=0.441), cognitive confidence (r=0.437), negative beliefs about uncontrollability and danger (r=0.405) and go/no-go (r=0.356) and negatively correlated with intellectual processes (r=−0.31). Pictorial empathy test was negatively correlated with negative symptoms (r=−0.304). Pictorial empathy test was positively correlated with empathic concern (r=0.355), not with other domains of interpersonal reactivity index (data not shown). Gender was not correlated with the domains of IRI and PET, respectively (data not shown) (Table 3).
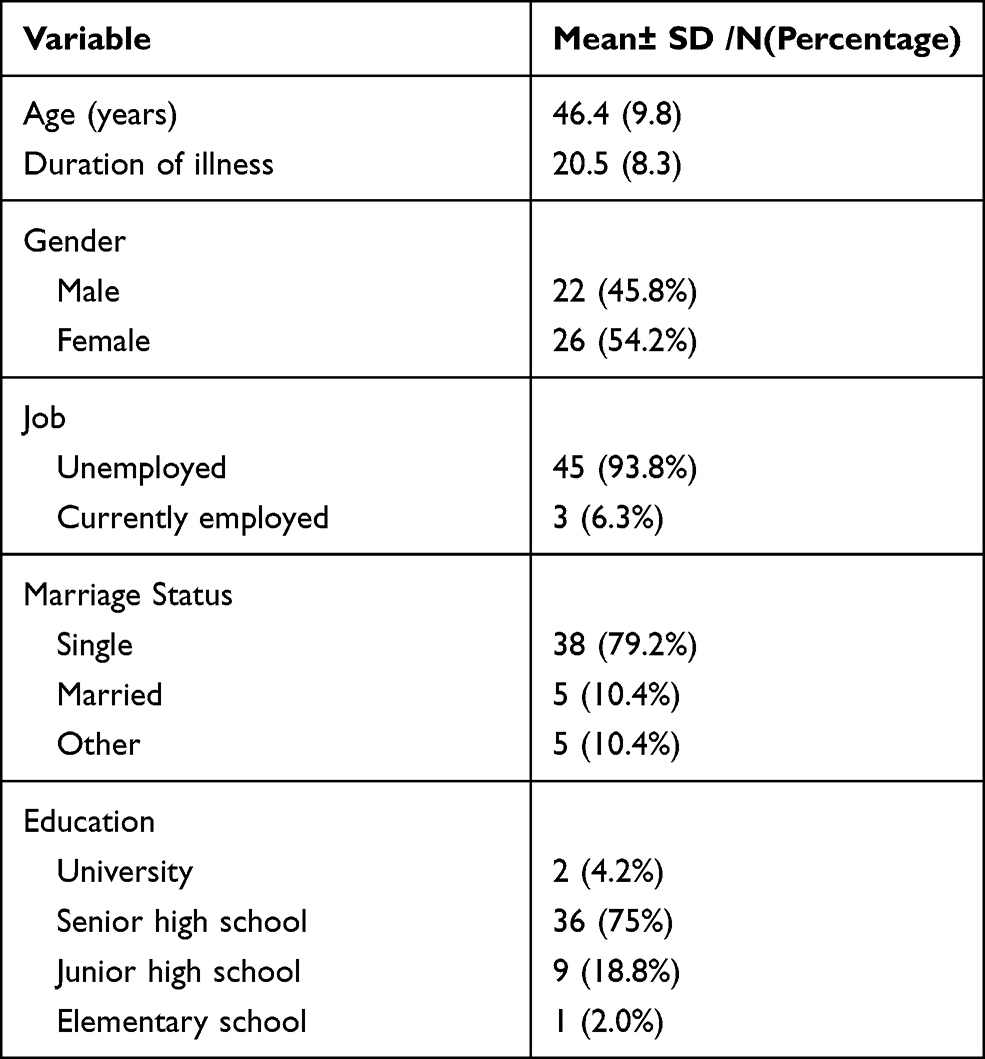 |
Table 1 Characteristics of Study Participants (N=48) |
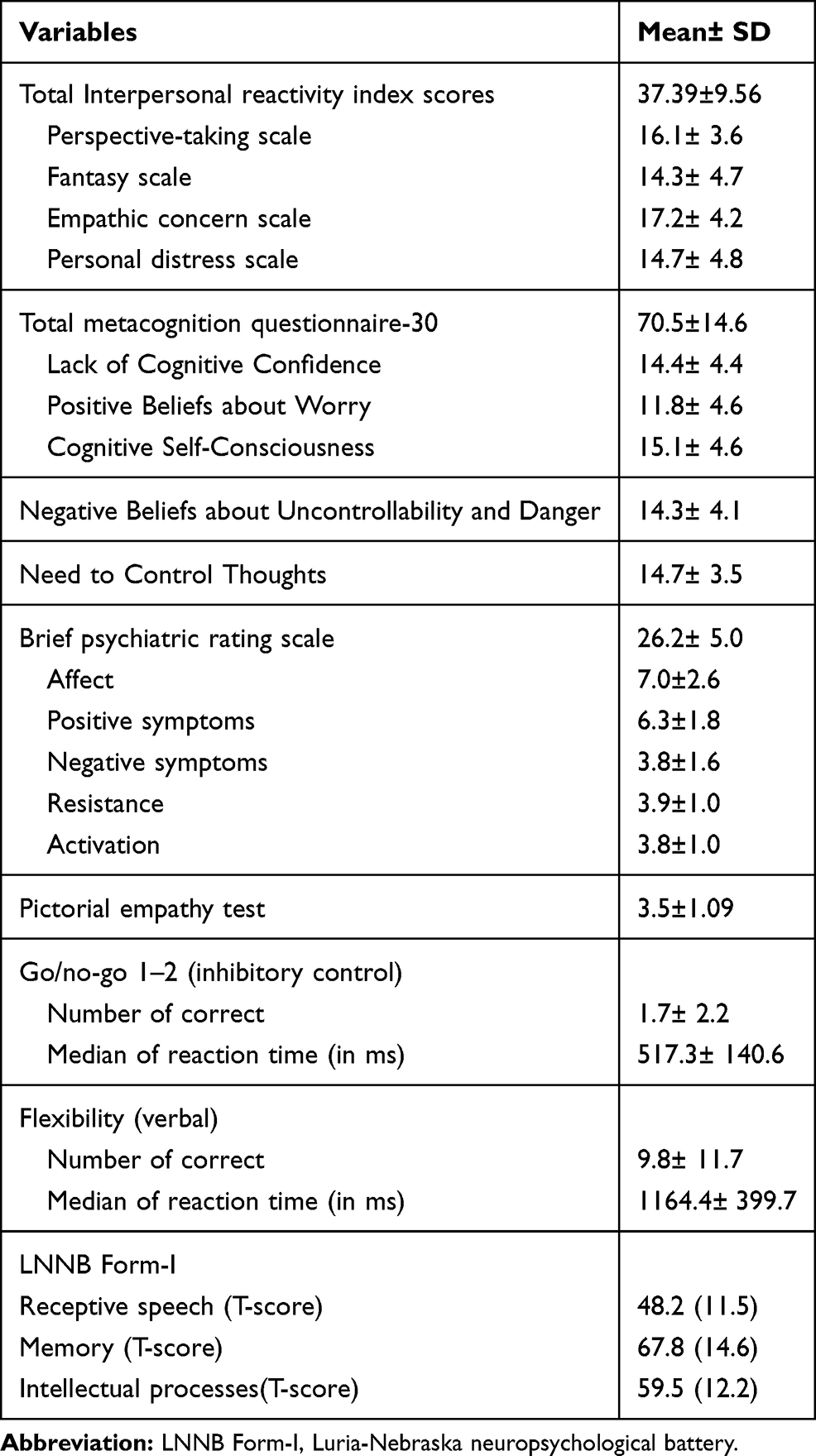 |
Table 2 Description of Clinical Characteristics of Participants (N=48) |
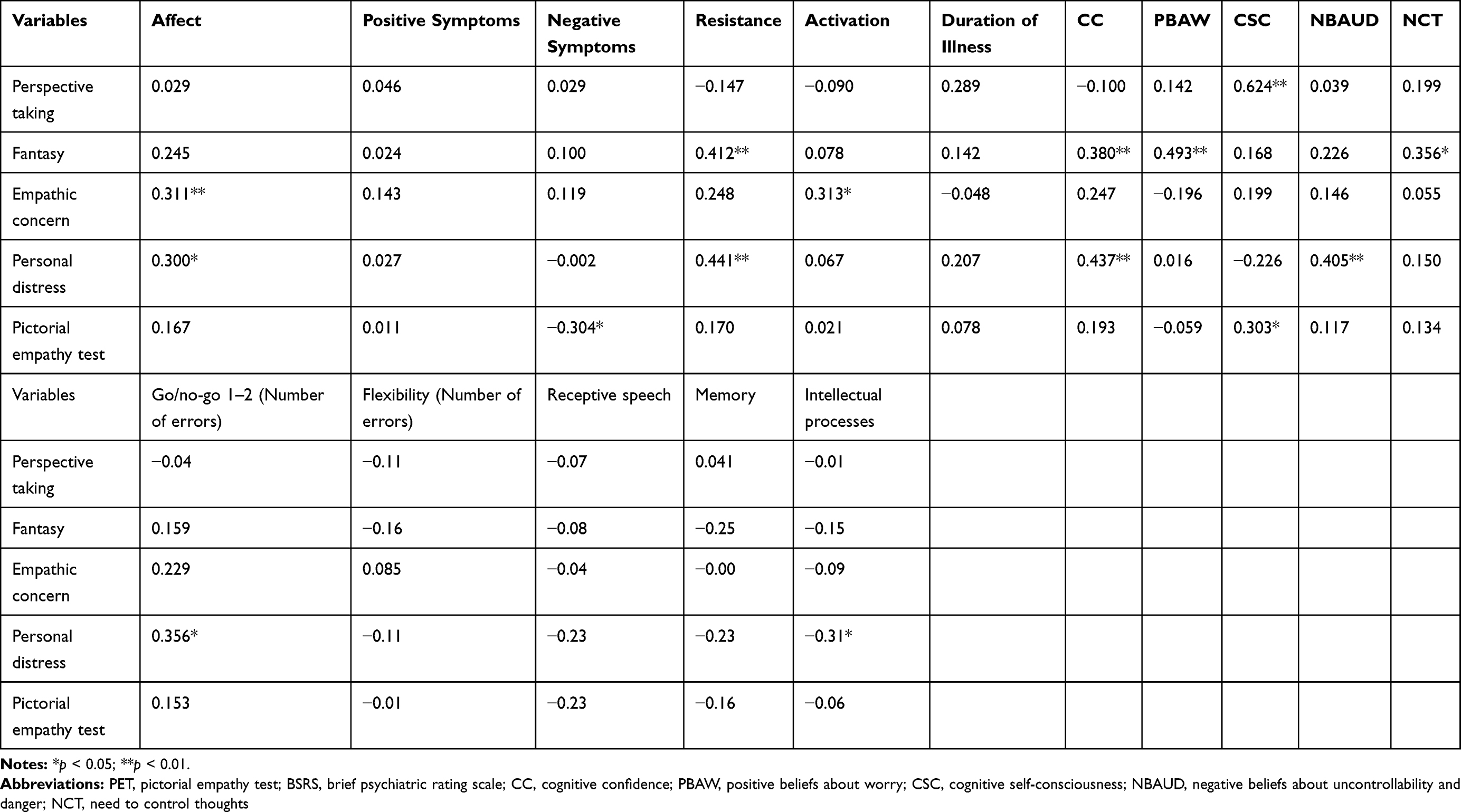 |
Table 3 Correlations of Clinical Characteristics of Participants (n=48) |
Regression Analysis
As summarized in Table 4, cognitive self-consciousness emerged to contribute significantly as predictors of subjects’ perspective taking (adjusted R2=0.37, p<0.001). Resistance and positive beliefs about worry emerged as significant contributors to fantasy (adjusted R2=0.34, p<0.001). Activation was a predictor for empathic concern (adjusted R2=0.07, p=0.031). Resistance, cognitive confidence, Intellectual processes and go/no-go emerged as significant contributors to personal distress (adjusted R2=0.38, p=0.049), respectively. Negative symptoms and cognitive self-consciousness were significant predictors for pictorial empathy test (adjusted R2=0.14, p=0.033). Table 4 presents the details of beta weights of each contributing variable.
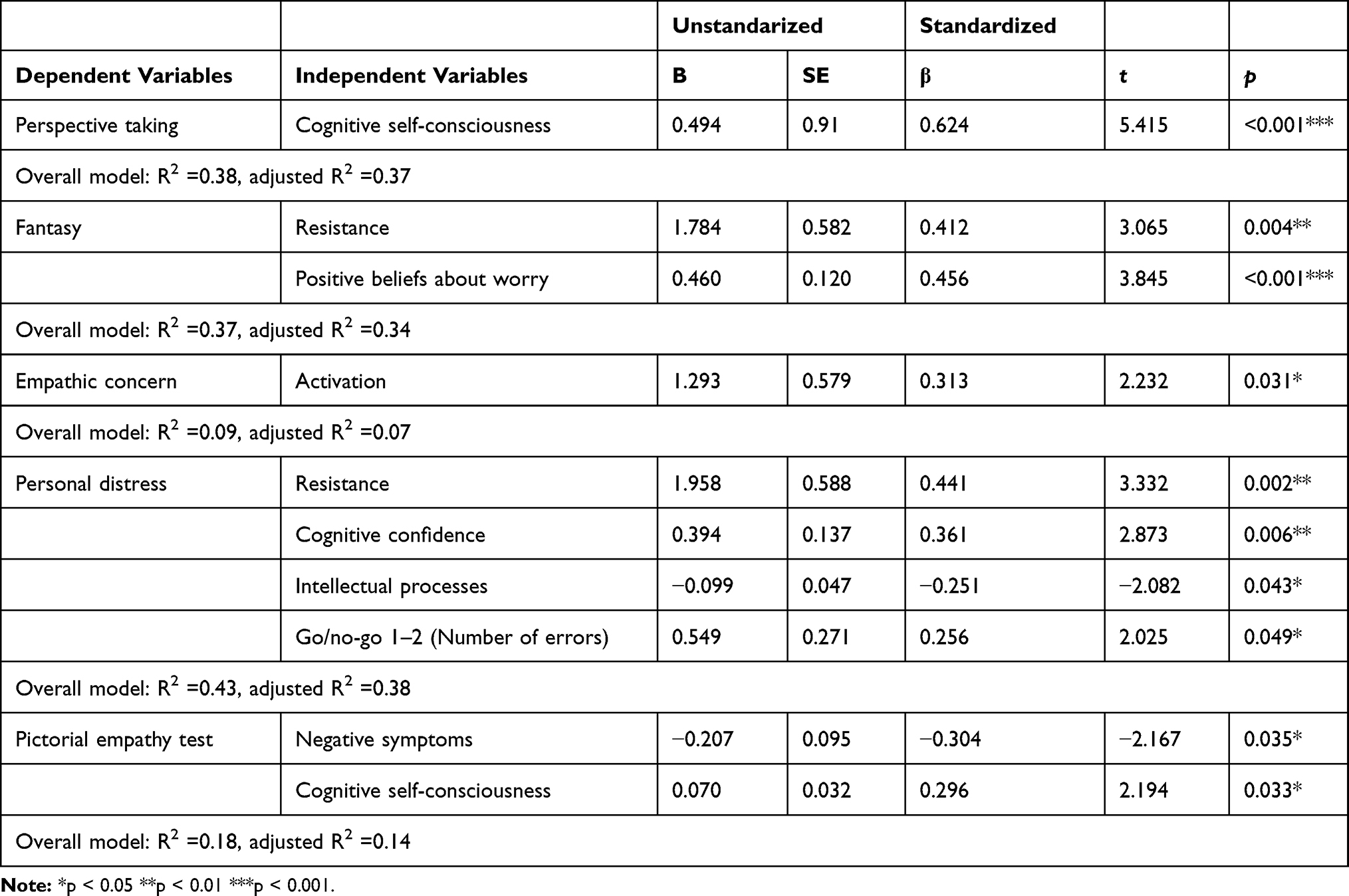 |
Table 4 Multiple Regressions Predicting Empathy from Metacognitive Beliefs, Cognitive Functioning and Psychiatric Symptoms (N = 48) |
Discussion
This study examined the relationships between subjective metacognitive beliefs, cognitive functioning, psychiatric symptoms and subjective and objective empathy among people with schizophrenia. In the regression analysis, perspective-taking was explained by cognitive self-consciousness which indicated that when people with schizophrenia have difficulty in reflecting their own mental state, they may have a reduced ability to take into the perspectives of others. The results of Stoica and Depue42 suggested that the awareness of one’s own mind body integration was related to perspective-taking. The authors found that fantasy was predicted by resistance and positive beliefs about worry, and empathic concern was predicted by activation (including excitement and tension). Results might suggest that people with schizophrenia are involved in more fantasy activities, and may have more worrying attitudes to cope with life and more resistance symptoms (including suspiciousness and hostility). It also showed that schizophrenia patients who felt more empathic concerns may be affected by heightened emotional states. Fantasy measures the tendency for a person to become or to transpose themselves into feelings or actions of fictitious characters in books and movies. In short, fantasy indexes that the facet of personality can amplify affective experiences. The results of Vuoskoski et al43 discovered that university students who enjoyed sad music scored high on self-reported empathic concern and fantasy. However, perspective-taking and personal distresses were not associated with a preference for sad music. Results indicated that emotional contagion may need high empathic concern (compassion) and imaginative absorption (fantasy).
Personal distress was explained by resistance, cognitive confidence, intellectual processes and inhibitory control. It suggested that when people with schizophrenia felt more personal distress when they experience the discomfort of others’ distress, they may have poor confidence of their memory, become more suspicious, have hostile symptoms and gain more errors of inhibitory control. In other words, when patients observed others’ facing adversity, they felt more personal distress leading to limited cognitive fluency. The findings of Israelashvili et al44 showed that healthy participants who scored high on self-report empathic concern also increased their accuracy of recognizing nonverbal facial emotions, whereas those who scored high on personal distress generally had poor performances. It may suggest that the two facets of empathic concern and personal distress have opposite influences in affective empathy. We also found that personal distress was correlated with intellectual processes, indicating that people with schizophrenia who have higher cognitive functioning are more likely to perceive their discomfort.
Picture empathy test was predicted by negative symptoms and positively associated with cognitive self-consciousness. Findings suggested that when schizophrenia patients have more negative symptoms and have difficulty understanding their mental state, their ability to perceive emotional reactions and distress of others tend to decrease. Other results also found that negative symptoms were negatively associated with observer-rated empathy (which assesses the quality and quantity of social relationships).21 The self-report empathy, domain of empathic concern was positively correlated with the picture empathy test (r=0.355, data not shown), implying that the pictorial test induced affective empathy reactions among people with schizophrenia.
Limitations
Some limitations should be acknowledged in interpreting the current study results. Further limitations of these results include the cross-sectional design, precluding the ability to infer cause directional statements. Additionally, our samples included outpatients that were relatively stable and chronic with less severe symptoms; therefore, the results may not be representative of all individuals with schizophrenia. The measures of empathy and metacognition were self-reported scales rather than objective or performance-based ability or experience, implying participants’ perception may vary from the real-world capacities.11,45 Stepwise regression analysis was applied in the present study which may exclude meaningful variables that may show low significance. Due to the sample size, no correction for multiple correlations was performed. A number of variables that showed significant correlations were not significant predictors in the regression analysis. Further work is needed to acquire objective and multiple measures of empathy and metacognition, and to make comparisons with a healthy group in order to examine the relationships between metacognition to cognitive and affective, empathy.
Conclusions
In the present study, self-reported metacognitive beliefs, psychiatric symptoms and cognitive functioning were associated with the domains of empathy. These findings serve implications for interventions designed to enhance metacognitive capacities in psychosocial treatments.
Acknowledgment
This study was supported by grant from Zuoying Armed Forces General Hospital, Kaohsiung, Taiwan (KAFGH-ZY-D-109037).
Author Contributions
All authors made significant contributions to the conception, study design, acquisition of data, analysis and interpretation of data; took part in drafting or revising the article; agreed to submit to this journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declared that this study has no competing interests.
References
1. De Vignemont F, Singer T. The empathic brain: how, when and why? Trends Cogn Sci. 2006;10(10):435–441. doi:10.1016/j.tics.2006.08.008
2. Gallese V. The roots of empathy: the shared manifold hypothesis and the neural basis of intersubjectivity. Psychopathology. 2003;36(4):335–346. doi:10.1159/000072786
3. Decety J, Jackson PL. A social neuroscience perspective on empathy. Curr Dir Psychol Sci. 2006;15:54e8.
4. Shamay-Tsoory SG. The neural bases for empathy. Neuroscientist. 2011;17(1):18e24. doi:10.1177/1073858410379268
5. Decety J, Jackson P, Brunet E. The cognitive neuropsychology of empathy. In: Farrow T, Woodruff P, editors. Empathy in Mental Illness and Health. New York: Cambridge University Press; 2007.
6. Decety J, Jackson PL. The functional architecture of human empathy. Behav Cogn Neurosci Rev. 2004;3(2):71–100. doi:10.1177/1534582304267187
7. Hoffman ML. Empathy and Moral Development: Implications for Caring and Justice. New York: Cambridge University Press; 2000.
8. Salovey P, Mayer JD. Emotional intelligence. Imagin Cogn Pers. 1989;9(3):185–211. doi:10.2190/DUGG-P24E-52WK-6CDG
9. McCullough ME, Rachal KC, Sandage SJ, Worthington EL, Brown JSW, Hight TL. Interpersonal forgiving in close relationships: II. Theoretical elaboration and measurement. J Pers Soc Psychol. 1998;75(6):1586–1603. doi:10.1037/0022-3514.75.6.1586
10. Haker H, Rossler W. Empathy in schizophrenia: impaired resonance. Eur Arch Psychiatry Clin Neurosci. 2009;259(6):352–361. doi:10.1007/s00406-009-0007-3
11. Bonfils KA, Lysaker PH, Minor KS, Salyers MP. Affective empathy in schizophrenia: a meta-analysis. Schizophr Res. 2016;175(1–3):109–117. doi:10.1016/j.schres.2016.03.037
12. Bonfils KA, Lysaker PH, Minor KS, Salyers MP. Empathy in schizophrenia: a meta-analysis of the interpersonal reactivity index. Psychiatry Res. 2017;249:293–303. doi:10.1016/j.psychres.2016.12.033
13. Michaels TM, Horan WP, Ginger EJ, Martinovich Z, Pinkham AE, Smith MJ. Cognitive empathy contributes to poor social functioning in schizophrenia: evidence from a new self-report measure of cognitive and affective empathy. Psychiatry Res. 2014;220(3):803–810. doi:10.1016/j.psychres.2014.08.054
14. Smith MJ, Horan WP, Cobia DJ, et al. Performance-based empathy mediates the influence of working memory on social competence in schizophrenia. Schizophr Bull. 2014;40(4):824–834. doi:10.1093/schbul/sbt084
15. Lysaker PH, Vohs JL, Ballard R, et al. Metacognition, self-reflection and recovery in schizophrenia. Future Neurol. 2013;8(1):103–115. doi:10.2217/fnl.12.78
16. Semerari A, Carcione A, Dimaggio G, et al. How to evaluate metacognitive functioning in psychotherapy? The metacognition assessment scale and its applications. Clin Psychol Psychother. 2003;10(4):238–261. doi:10.1002/cpp.362
17. Hasson-Ohayon I, Avidan-Msika M, Mashiach-Eizenberg M, et al. Metacognitive and social cognition approaches to understanding the impact of schizophrenia on social quality of life. Schizophr Res. 2015;161(2):386–391. doi:10.1016/j.schres.2014.11.008
18. Lysaker PH, Gumley A, Luedtke B, et al. Social cognition and metacognition in schizophrenia: evidence of their independence and linkage with outcomes. Acta Psychiatr Scand. 2013;127(3):239–247. doi:10.1111/acps.12012
19. Lysaker PH, Carcione A, DiMaggio G, et al. Metacognition amidst narratives of self and illness in schizophrenia: associations with insight, neurocognition, symptom and function. Acta Psychiatr Scand. 2005;112(1):64–71. doi:10.1111/j.1600-0447.2005.00514.x
20. Wells A, Cartwright-Hatton S. A short form of the metacognitions questionnaire: properties of the MCQ-30. Behav Res Ther. 2004;43(4):385–396. doi:10.1016/S0005-7967(03)00147-5
21. Bonfils KA, Minor KS, Leonhardt BL, Lysaker PH. Metacognitive self-reflectivity moderates the relationship between distress tolerance and empathy in schizophrenia. Psychiatry Res. 2018;265:1–6. doi:10.1016/j.psychres.2018.04.042
22. Bonfils KA, Lysaker PH, Minor KS, Salyers MP. Metacognition, personal distress, and performance-based empathy in schizophrenia. Schizophr Bull. 2019;45(1):19–26. doi:10.1093/schbul/sby137
23. Han M, Huang XF, Chen DC, et al. Gender differences in cognitive functioning of patients with chronic schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2012;39(2):358–363. doi:10.1016/j.pnpbp.2012.07.010
24. Torniainen M, Suvisaari J, Partonen T, et al. Cognitive impairments in schizophrenia and schizoaffective disorder: relationship with clinical characteristics. J Nerv Ment Dis. 2012;200(4):316–322. doi:10.1097/NMD.0b013e31824cb359
25. Fervaha G, Foussias G, Agid O, Remington G. Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr Scand. 2014;130(4):290–299. doi:10.1111/acps.12289
26. Grattan LM, Eslinger PJ. Higher cognition and social behavior: changes in cognitive flexibility and empathy after cerebral lesions. Neuropsychology. 1989;3(3):175–185.
27. Shamay-Tsoory SG, Tomer R, Berger BD, Aharon-Peretz J. Characterization of empathy deficits following prefrontal brain damage: the role of the right ventromedial prefrontal cortex. J Cogn Neurosci. 2003;15(3):324–337. doi:10.1162/089892903321593063
28. Bora E, Gökçen S, Baybars V. Empathic abilities in people with schizophrenia. Psychatry Res. 2008;160(1):23–29. doi:10.1016/j.psychres.2007.05.017
29. Taiwo Z, Bezdek M, Mirabito G, Light SN. Empathy for joy recruits a broader prefrontal network than empathy for sadness and is predicted by executive funtioning. Neuropsychology. 2021;35(1):90–102. doi:10.1037/neu0000666
30. Sparks A, McDonald S, Lino B, O’Donnell M, Green MJ. Social cognition, empathy and functional outcome in schizophrenia. Schizophr Res. 2010;122(1–3):172–178. doi:10.1016/j.schres.2010.06.011
31. Montag C, Neuhaus K, Lehmann A, et al. Subtle deficits of cognitive theory of mind in unaffected first degree relatives of schizophrenia patients. Eur Arch Psychiatry Clin Neurosci. 2012;262(3):217–226. doi:10.1007/s00406-011-0250-2
32. Montag C, Heinz A, Kunz D, Gallinat J. Self-reported empathic abilities in schizophrenia. Schizophr Res. 2007;92(1–3):85–89. doi:10.1016/j.schres.2007.01.024
33. Locher SC, Barenblatt L, Fourie MM, Stein DJ, Gobodo-Madikizela P. Empathy and childhood maltreatment: a mixed-methods investigation. Ann Clin Psychiatry. 2014;26(2):97–110.
34. Lindeman M, Koirikivi I, Lipsanen J. Pictorial Empathy Test (PET). An easy-to-use method for assessing affective empathic reactions. Eur J Psychol Assess. 2018;34(6):421–431. doi:10.1027/1015-5759/a000353
35. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. Am Psychiatr. 2013.
36. Davis MH. Measuring individual differences in empathy: evidence for a multidimensional approach. J Pers Soc Psychol. 1983;44(1):113–126. doi:10.1037/0022-3514.44.1.113
37. Spada MM, Mohiyeddini C, Wells A. Measuring metacognitions associated with emotional distress: factor structure and predictive validity of the metacognitions questionnaire 30. Pers Individ Differ. 2008;45(3):238–242. doi:10.1016/j.paid.2008.04.005
38. Overall JE, Gorham DR. The brief psychiatric rating scale. Psychol Rep. 1962;10(3):799–812. doi:10.2466/pr0.1962.10.3.799
39. Hafkenscheid A. Psychometric evaluation of a standardized and expanded brief psychiatric rating scale. Acta Psychiatr Scand. 1991;84(3):294–300. doi:10.1111/j.1600-0447.1991.tb03147.x
40. Zimmermann P, Fimm B. A test battery for attentional performance. In: Leclercq M, Zimmermann P, editors. Applied Neuropsychological of Attention: Theory, Diagnosis and Rehabilitation. New York: Psychology Press; 2002:110–151.
41. Golden CJ, Purisch AD, Hammeke TA. Luria-Nebraska Neuropsychological Battery: Forms I & II (Manual). Los Angeles: Psychological Services; 1985.
42. Stoica T, Depue B. Shared characteristics of intrinsic connectivity networks underlying interceptive awareness and empathy. Front Hum Neurosci. 2020;14:571070. doi:10.3389/fnhum.2020.571070
43. Vuoskoski JK, Thompson WF, Mcllwain D, Eerola T. Who enjoys listening to sad music and why? Music Percept. 2012;29(3):311–317. doi:10.1525/mp.2012.29.3.311
44. Israelashvili J, Sauter D, Fischer A. Two facets of affective empathy: concern and distress have opposite relationships to emotion recognition. Cogn Emot. 2020;34(6):1112–1122. doi:10.1080/02699931.2020.1724893
45. Lysaker PH, Hasson-Ohayon I, Kravetz S, Kent JS, Roe D. Self perception of empathy in schizophrenia: emotion recognition, insight, and symptoms predict degree of self and interviewer agreement. Psychiatry Res. 2013;206(2–3):146–150. doi:10.1016/j.psychres.2012.10.021
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.