Back to Journals » Journal of Inflammation Research » Volume 18
Metabolomic Profiling by UPLC-QTOF/MS Reveals Potential Biomarkers and Metabolic Alterations in Pediatric Septic Shock
Authors Xiao C, Wang C ![]() , Wang S, Xu F, Chen Y
, Wang S, Xu F, Chen Y
Received 5 July 2025
Accepted for publication 19 October 2025
Published 11 November 2025 Volume 2025:18 Pages 15645—15655
DOI https://doi.org/10.2147/JIR.S551775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anh Ngo
Changxue Xiao,* Chenhao Wang,* Sa Wang, Feng Xu, Yingfu Chen
Department of Critical Care Medicine, Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatric Metabolism and Inflammatory Diseases, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingfu Chen, Department of Critical Care Medicine, Children’s Hospital of Chongqing Medical University, No. 136, 2nd Zhongshan Road, Yuzhong District, Chongqing, 400014, People’s Republic of China, Email [email protected]
Purpose: Septic shock is a major cause of mortality in pediatric intensive care units (PICU). This study aimed to investigate metabolic alterations in PICU patients with septic shock using ultra-high performance liquid chromatography-quadrupole time-of-flight mass spectrometry (UPLC-QTOF/MS) to identify potential biomarkers and unique metabolic pathways for early diagnosis and improved treatment strategies.
Patients and Methods: Serum and urine samples from septic shock survivors (SS), septic shock non-survivors (SNS), and non-infected systemic inflammatory response syndrome (SIRS) patients were analyzed using UPLC-QTOF/MS. All differential metabolites from serum samples were subjected to multiple regression analysis. Bioinformatics analysis was conducted on metabolite data obtained from urine and serum samples of the SS and SNS groups to further investigate differences in metabolic pathways.
Results: Combinational metabolites demonstrated superior diagnostic performance compared with individual metabolites, with an area under the receiver operating characteristic curve (AUC) of 0.925 for SS vs SIRS and 0.901 for SNS vs SIRS. Key metabolic pathways, including glycerophospholipid metabolism, arginine and proline metabolism, were implicated in the development of septic shock. Importantly, alterations in glutamine and glutamate metabolism were associated with survival, suggesting the significant potential for further investigation.
Conclusion: Metabolomic profiling using UPLC-QTOF/MS represents a promising approach for early diagnosis of pediatric septic shock. The identified biomarkers and metabolic pathways provide insights into the pathogenic mechanisms and may assist in the development of targeted therapeutic strategies. Further validation in larger, prospective cohorts is required before clinical application.
Keywords: metabolomics, biomarker, metabolic pathways, septic shock, pediatric
Introduction
Septic shock is a severe consequence of sepsis in which underlying circulatory and cellular abnormalities are profoundly disturbed enough to substantially increase ill-consequence.1 Despite advances in diagnostic and therapeutic strategies, pediatric septic shock remains a major medical burden with persistently high morbidity and mortality.2–6 Clinically, septic shock can change rapidly with a dynamic process in pediatric patients, and if diagnosed early, it may be managed promptly with goal-directed therapy to attain a significant improvement in survival rate compared to patients with a late diagnosis.7–9 However, the complexity and heterogeneity of septic shock in pediatric patients present an obstacle to its early identification with conventional methods.10–12 Although biomarkers such as lactic acid and procalcitonin are clinically used, their limited specificity and prognostic value highlight the need for novel approaches. Metabolomics offers a more comprehensive view of host metabolic responses and may overcome these limitations.
Recent metabolomics studies have demonstrated that alterations in amino acid, lipid, and energy metabolism are closely associated with sepsis outcomes,13,14 with dynamic metabolic shifts observed in septic shock before and after treatment.15 In pediatric sepsis, metabolomic analyses using techniques such as 1H-NMR, LC-MS, and UPLC-MS/MS have characterized specific metabolic features.16–19 However, significant differences exist among reports in terms of methodology, sample types, and analytical coverage. Compared with the high-resolution metabolomics research in adults, pediatric studies remain scarce and often rely on a single biofluid, limiting the comprehensiveness of pathway interpretation.
Ultra-high performance liquid chromatography-quadrupole time-of-flight mass spectrometry (UPLC-QTOF/MS) provides high sensitivity and separation capacity, enabling detection of a broader range of metabolites,20,21 yet it has been rarely applied in pediatric populations.
In this study, we employed UPLC-QTOF/MS metabolomics to perform integrated metabolomic profiling of both serum and urine from pediatric intensive care units (PICU) patients. By analyzing these complementary biofluid data, we were able to identify concordant metabolic pathways, thereby providing a more accurate and robust characterization of metabolic alterations in children with septic shock. The primary aim was to identify diagnostic biomarkers that distinguish pediatric septic shock from non-infectious systemic inflammatory response syndrome (SIRS), and the secondary aim was to identify prognostic biomarkers and to explore metabolic pathways that differentiate survivors from non-survivors.
Materials and Methods
Participants
Pediatric patients with septic shock or non-infected SIRS admitted to the PICU of the Children’s Hospital of Chongqing Medical University between July 2018 and February 2020 with an age range of 29 days to 18 years were selected. Diagnosis of septic shock and SIRS was made by trained specialists in the PICU based on the criteria of the International Consensus Conference on Pediatric Sepsis,22 and SIRS patients with non-infectious causes were designated as non-infectious SIRS for study control (SIRS control). The exclusion criteria were as follows: pediatric patients aged ≤ 29 days or > 18 years, or patients diagnosed with septic shock for more than 24 hours. The study protocol was reviewed and approved by the Institutional Review Board of the Children’s Hospital of Chongqing Medical University on November 22, 2017 (No.2017-3-1). Informed consent for this study was obtained from the guardians of all pediatric patients. The study procedures were performed in accordance with the institutional ethical standards for human experimentation and the 1975 Helsinki Declaration.
Sample Preparation
Serum samples were acquired from all patients with septic shock within 24 h after diagnosis, whereas SIRS control samples were collected within 24 h after PICU admission, to reflect the early host metabolic response during the critical phase of pediatric septic shock. Following the protocol, whole blood was drawn into a 5 mL vacutainer blood collection tube without EDTA, centrifuged for 10 min at 3500 rpm, and serum supernatants were extracted. All the aliquots (200 μL) of the serum samples were saved in a −80°C freezer for future use in UPLC-QTOF/MS analysis.
Before UPLC-QTOF/MS, all the samples were gradually thawed at 4°C, then 100 μL was taken out from each sample and mixed thoroughly with 400 μL of cold methanol/acetonitrile at a ratio of 1:1 (v/v). The mixtures were further centrifuged for 20 min at 14,000 × g and 4°C, and following centrifugation, the supernatant was completely dehydrated in a vacuum centrifuge. Next, the pellets left in the tubes were resuspended in 100 μL acetonitrile/water at 1:1 ratio (v/v), which were further centrifuged for 15 min at 14,000 × g at 4°C. Subsequently, the supernatants were analyzed by UPLC-QTOF/MS. Quality control (QC) for UPLC-QTOF/MS was processed by pooling 10 μL of each sample for verifying the stability and repeatability of analytical instrument. We also collected urine samples from 27 septic shock survivors (SS) and 10 septic shock non-survivors (SNS), the collection and preparation of urine samples have been clarified in our published article on sepsis-associated acute kidney injury.23
UPLC-QTOF/MS Analysis
The samples were loaded into a 1290 Infinity LC system (Agilent Technologies, Santa Clara, California, USA) coupled with an AB SCIEX Triple TOF 6600 system (AB SCIEX, Framingham, MA, USA) for analysis. During the HILIC separation phase, the samples were run through a 2.1×100 mm ACQUITY UPLC BEH 1.7 μm column (Waters, Ireland). In both ESI positive and negative modes, the mobile phase contained A of the mixture of 25 mM ammonium acetate and 25 mM ammonium hydroxide in water and B of acetonitrile with the gradient elution procedure as initiation of 85% B for 1 min, which was sequentially followed by linearly reducing to 65% for 11 minutes, then to 40% for 0.1 minutes, and maintaining at 40% for 4 minutes, afterward going back to 85% for 0.1 minutes with a re-equilibration period for 5 minutes.
The ESI source was made from follows: Ion Source Gas1 (Gas1) as 60, Ion Source Gas2 (Gas2) as 60, Curtain gas (CUR) as 30, source temperature as 600 °C, IonSpray Voltage Floating (ISVF) as ±5500 V. For MS acquisition, the instrument was operated over the m/z range of 60–1000 Da with the accumulation time for TOF MS as 0.20 s/spectra, while the instrument was calibrated to acquire over the m/z range of 25–1000 Da in auto MS/MS acquisition with the accumulation time for product ion scan as 0.05 s/spectra. The product ion scan was acquired with information-dependent acquisition (IDA) in high-sensitivity mode. The collision energy (CE) was fixed at 35 V at ± 15 eV and the declustering potential (DP) was set to ± 60 V.
Metabolomic Data Processing and Data Analysis
The original data from the spectrometry were in the wiff.scan format, which were initially converted into MzXML files through an open-online platform, ProteoWizard’s msConvert (https://proteowizard.sourceforge.io/download.html). Subsequently, the converted data were further processed using the XCMS for feature detection, retention time correction, and alignment. Metabolites from the samples were identified by mass analysis with a mass accuracy of less than 22 ppm. The acquired MS/MS raw data were verified by matching with our standards database, and the variables retained in the extracted ion features were those that were more than 50% of the nonzero measurement values in at least one group. Multivariate statistical analysis was performed using MetaboAnalyst, a web-based platform (www.metaboanalyst.ca).
After Pareto scaling, metabolites were examined using principal component analysis (PCA) and orthogonal partial least squares discriminant analysis (OPLS-DA). The validity of the model and sample distribution was evaluated using leave-one-out cross-validation and response permutation testing, respectively. Significantly different metabolites were identified through a combination of a statistically significant threshold of variable influence on projection (VIP) values acquired from the OPLS-DA model and a two-tailed Student’s t-test (p-value) on the raw data. In general, metabolites with VIP values greater than 1.0, and p values less than 0.05 were designated as the criteria for significance.
Bioinformatics Analysis and Biomarker Identification
First, binary logistic regression along with a receiver operating characteristic curve (ROC) was performed to illustrate the diagnostic and prognosis-indicating potential of metabolites. We also examined the metabolic phenotypes and significantly involved metabolic pathways in the different study groups using online tools of MetaboAnalyst (https://www.metaboanalyst.ca/) and the Kyoto Encyclopedia of Genes and Genomes (KEGG) database (http://www.genome.jp/kegg/). All data from every part of this study were statistically processed using SPSS 20.0. A schematic flowchart summarizing the workflow of sample collection, processing, UPLC-QTOF/MS analysis, and data processing is provided in eFigure 1.
Results
Clinical Characteristics of Patients
Serum samples were collected from 80 PICU patients, including 35 septic shock survivors (SS; male/female: 20/15), 32 septic shock non-survivors (SNS; male/female: 20/12), and 13 non-infected SIRS controls (SIRS; male/female: 9/4). The demographic and clinical data of the patients did not reveal any significant differences between the three groups (shown in Table 1); however, it was noted that there were significantly increased serum lactic acid concentrations in septic patients, especially in SNS (p < 0.001). The urine samples were collected from 37 PICU patients, including 27 septic shock survivors (SS; male/female: 16/11) and 10 septic shock non-survivors (SNS; male/female: 5/5). Their demographic and clinical data are shown in eTable 1.
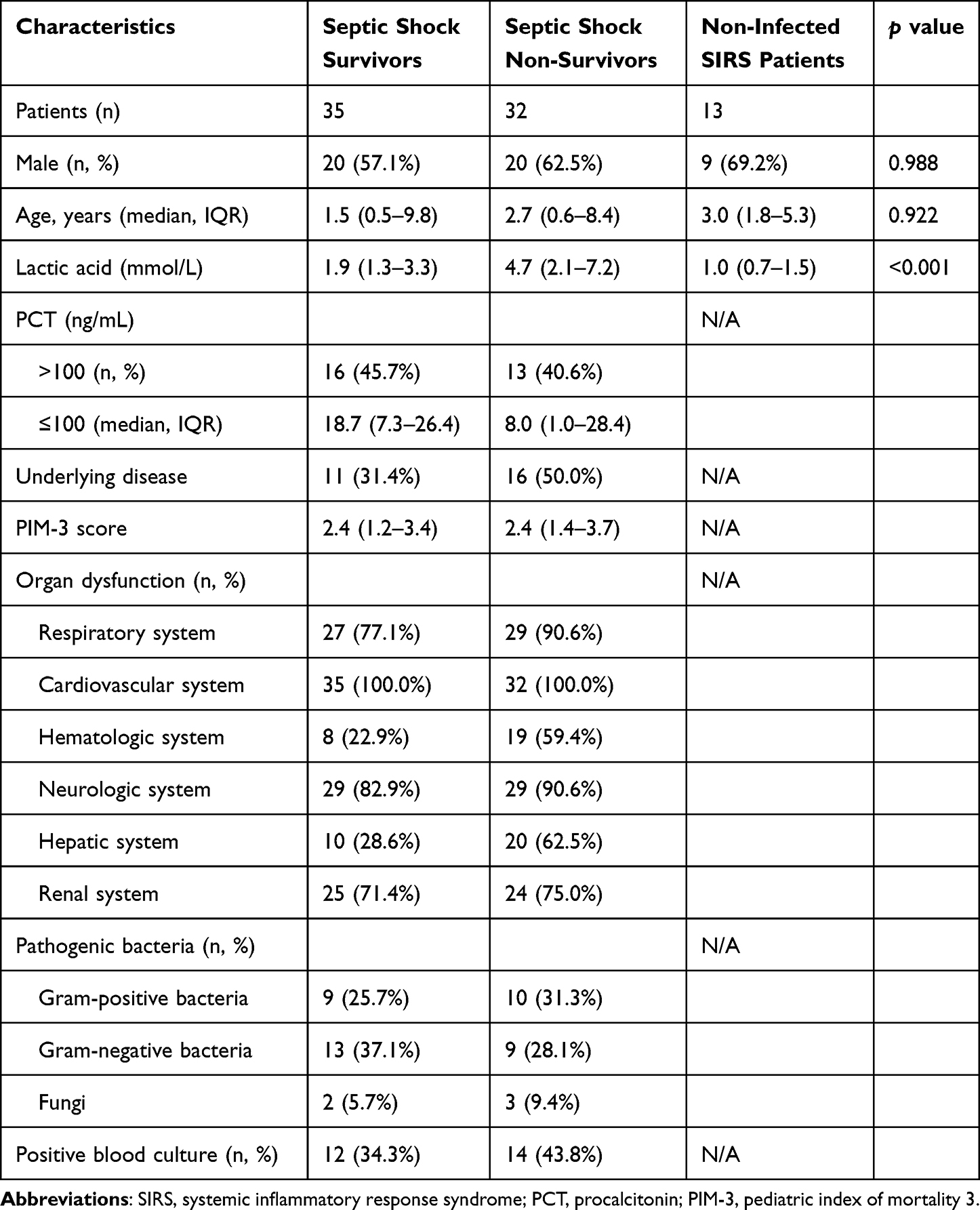 |
Table 1 Clinical Characteristics of Pediatric Patients with Blood Samples |
Metabolomic Analysis
The untargeted metabolomics analysis was performed on 80 serum samples to identify 5703 positive and 5728 negative-mode features, which were processed for multidimensional statistical analysis (PCA, OPLS-DA). The samples obtained either in positive or negative mode were sent to QC, which found them to be tightly clustered on PCA score plots (eFigure 2), thereby suggesting that the experimental system was stable with satisfactory reproducibility. OPLS-DA scores were plotted out with obvious separations between the positive and negative modes to identify differences in the metabolic profiles among the three comparative groups (eFigure 3). The different metabolites between the study groups were then revisited using the criteria of VIP > 1 and p value less than 0.05, and further analyzed using multivariate and univariate analyses. Finally, 78 and 33 distinct metabolites, mainly involved in amino acid, lipid, and carbohydrate metabolism, satisfied the criteria for positive and negative modes, respectively. The details of these metabolites are shown in eTables 2 and 3, in which 60 metabolites showed significant variations between SS and SIRS, 58 between SNS and SIRS, and 48 between SNS and SS.
Identification of Biomarkers from Serum Samples
To identify diagnostic biomarkers and prognostic predictors of pediatric septic shock, we conducted a stepwise binary logistic regression and ROC analysis. For diagnostic biomarkers, 34 significantly changed metabolites overlapped in comparisons between SS and SIRS as well as between SNS and SIRS. Binary logistic regression revealed that acamprosate (Wald χ2 = 4.807, p = 0.028) and benzoic acid (Wald χ2 = 5.622, p = 0.018) were significantly associated with distinguishing SS from SIRS, whereas norharmane (Wald χ2 = 7.473, p = 0.006) and diethyltoluamide (Wald χ2 = 4.281, p = 0.039) were predictive of distinguishing between SNS and SIRS. As prognostic biomarkers, sn-Glycerol 3-phosphoethanolamine (Wald χ2 = 5.905, p = 0.015), oxindole (Wald χ2 = 4.338, p = 0.037), and N6-methyladenosine (Wald χ2 = 4.704, p = 0.030) demonstrated significant predictive capacity for differentiating SS from SNS. ROC analysis further evaluated the diagnostic and prognostic performance of these metabolites, individually and in combination (Table 2 and Figure 1). Since lactic acid levels have been clinically validated as a risk factor for septic shock severity and poor prognosis,24 we compared the area under the curve (AUC) of the combined metabolites with that of lactic acid, showing that combined metabolites were superior (Figure 1) and could be considered an independent parameter for predicting the prognosis of pediatric septic shock.
 |
Table 2 Individual and Combined Metabolites and Their Predictabilities in the Pediatric Septic Patients |
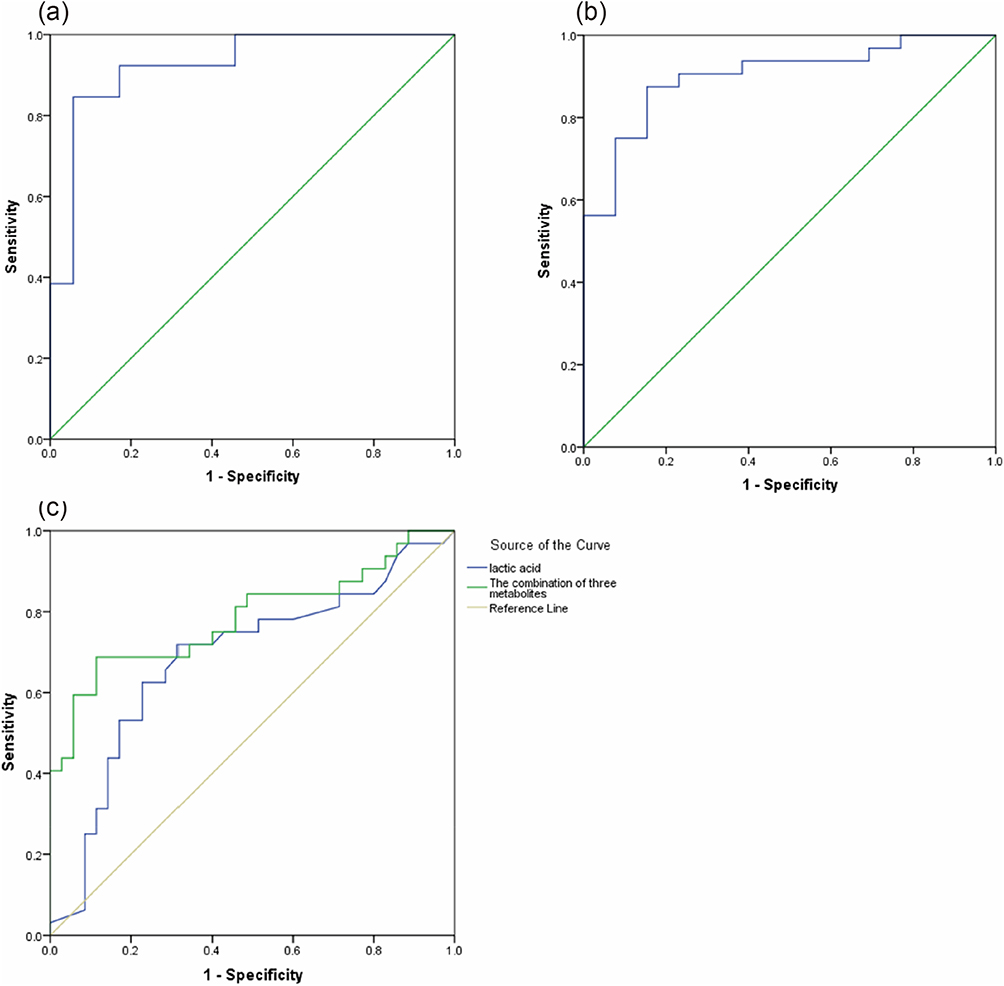 |
Figure 1 ROC analysis of predictive performance of combined metabolites among SIRS, SS and SNS patients. (a) Combined metabolites for SS-SIRS. (b) Combined metabolites for SNS-SIRS. (c) Combined metabolites for SNS-SS and compared with lactic acid of patients. |
Metabolic Pathway Analysis
Bioinformatics analysis of clusters and KEGG were applied to differentiate the metabolites identified in the different study groups. Cluster analysis was used to map differences in metabolites in similar metabolic processes (eFigures 4 and 5). In comparison, the expression of metabolites related to phospholipids, sphingolipids, fatty acids, and carbohydrate metabolism was decreased in pediatric septic shock patients (both SS and SNS), whereas the expression of amino acid metabolites, such as arginine, proline, and amphetamine, was increased, indicating that the metabolism of septic shock patients was obviously disordered. KEGG pathway analysis of the serum samples from the studied patients identified 28 metabolic pathways that were significantly perturbed in SIRS and septic shock patients; among these, arginine, proline, and glycerophospholipid metabolism that coexist in the SS and SNS patients were tentatively suggested to be associated with the pathogenesis of septic shock. Moreover, glutamine and glutamate metabolism pathways, assessed by both urine and serum analyses, could differentiate septic shock survivors from non-survivors (Figure 2).
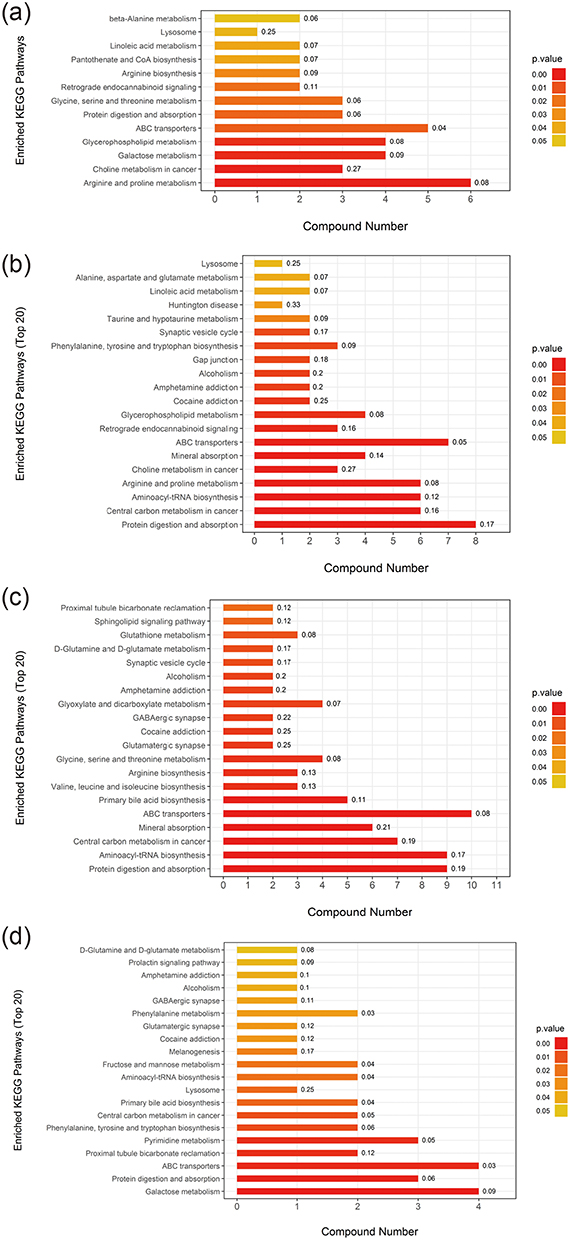 |
Figure 2 Metabolic pathway analysis of identified metabolites in serum or urine samples from septic patients. (a) SS vs SIRS in serum samples. (b) SNS vs SIRS in serum samples. (c) SNS vs SS in serum samples. (d) SNS vs SS in urine samples. |
Discussion
Both early diagnosis and metabolic alterations have been the focus of clinical and basic scientific research in sepsis.7,25 In our study, we applied a UPLC-QTOF/MS-based approach to differentiate the metabolomics of pediatric septic shock from non-infected SIRS in the PICU, differentiate septic shock survivors from non-survivors, and identify novel potential biomarkers and signature metabolic pathways for the early diagnosis and management of septic shock in pediatric patients.
First, our results from blood and urine samples revealed significant alterations in amino acid metabolism among pediatric septic shock patients, particularly in the histidine, glutamate, glutamine, and proline metabolism pathways (Figure 3). Notably, metabolic changes in glutamate and glutamine were present in both the blood and urine samples. Amino acids play an important role in host defense against pathogens and in modulating excessive inflammatory responses,26 including the regulation of immune cell activation and antibody production.27 A recent study demonstrated that plasma glutamine levels correlated with clinical outcomes in intensive care unit patients.28 Furthermore, glutamine has been shown to mitigate excessive inflammation and reduce organ damage by promoting macrophage M2 polarization in a mouse model of burn-induced sepsis.29 While glutamine is recognized for its involvement in nutrient metabolism and immune regulation during sepsis, the precise underlying mechanisms remain unclear.
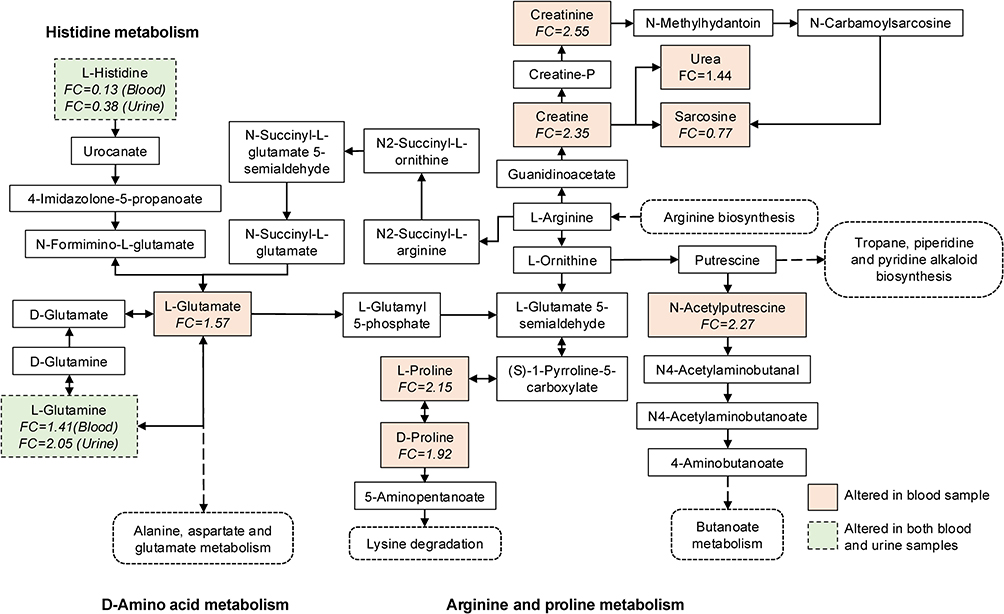 |
Figure 3 Metabolic pathway alterations in pediatric septic shock patients. This schematic diagram highlights significant changes in glutamate and glutamine metabolism, arginine and proline metabolism, and related pathways observed in sepsis. Metabolites altered in blood samples are indicated by orange solid boxes, while those altered in both blood and urine samples are indicated by green dashed boxes. |
Our study showed that pediatric septic shock patients had elevated levels of serum creatine, creatinine, and phenylalanine, which are tentatively associated with muscle tissue damage, amino acid oxidation perturbation, and energy deprivation during septic shock.30–32 We also noted decreased levels of oleic acid and palmitic acid in the studied patients, both of which are involved in the pathways of fatty acid β-oxidation, reflecting insufficient energy supply in children with septic shock.33 These observations are consistent with prior metabolomics-based studies in systemic inflammatory conditions, which similarly reported dysregulation in amino acid and lipid metabolism.34
Furthermore, this study revealed novel alterations in phospholipid pathways. Glycerophospholipid metabolism was undermined in septic shock patients, with decreased levels of phosphorylcholine, sn-Glycerol-3-phosphoethanolamine, PC (16:0/16:0) and 1-stearoyl-2-oleoylphosphatidylcholine (SOPC), suggesting that glycerophospholipid metabolism may be associated with the pathogenesis of pediatric septic shock. Previous studies have putatively suggested the role of oxidized phospholipids in pro-inflammatory effects in animal models;35–37 however, experimental evidence has associated decreased levels of choline glycerophosphate with sepsis mortality.38 Taken together, alterations in glycerophospholipid metabolism, along with the dysregulation of glutamine metabolism, may represent not only biomarkers but also potential therapeutic targets, given their central role in immune regulation and energy metabolism. Nevertheless, further mechanistic and clinical studies are required for validation.
We also examined these data to identify potential diagnostic and prognostic biomarkers. The combined metabolites of acamprosate and benzoic acid (AUC=0.925), and norharmane and diethyltoluamide (AUC=0.901) were significantly lower in septic shock patients than in non-infected SIRS patients. Moreover, the combinational metabolites of sn-Glycerol 3-phosphoethanolamine, oxindole, and N6-methyladenosine (AUC=0.786), all involved in glycerophospholipid metabolism, were the most remarkable metabolites in survivors and non-survivors, suggesting that these three metabolites could be superior to lactic acid levels in predicting the prognosis of septic shock. A previous study suggested that changes in metabolism of individuals were mainly associated with disease conditions rather than age or sex.17 However, in pediatric populations, potential confounding by age, sex, or other factors cannot be entirely excluded. Due to the relatively small sample size, further sensitivity analyses were not feasible in the present study.
Our study had several limitations. First, the collection of bodily fluid samples from children is more difficult than from adults; therefore, our study had a relatively small sample size from a single center and lacked external validation. This may limit the statistical power, clinical applicability, and generalizability of our findings. Second, metabolic profiles may be influenced by nutritional status, medications, underlying comorbidities or instrument batch effects, stratified analysis based on a large sample size is preferable. Third, all samples were obtained within 24 hours of diagnosis to capture the acute metabolic response; however, longitudinal sampling could provide additional insights into dynamic metabolic changes over the disease course. Further prospective validation with larger sample sizes, targeted quantitative analyses are required to assess the feasibility and practicality of these novel biomarkers.
Conclusion
In this proof-of-concept study, we identified distinctive metabolic alterations associated with several metabolic pathways in pediatric septic shock and highlighted combinational metabolites as potential early diagnostic and prognostic indicators. Our findings suggest that, in this cohort, combinational metabolites may outperform lactate for early diagnosis and risk stratification. However, these results are preliminary, and prospective, multicenter validation is required before clinical application in the PICU.
Abbreviations
UPLC-QTOF/MS, Ultra-high performance liquid chromatography-quadrupole time-of-flight mass spectrometry; SIRS, systemic inflammatory response syndrome; PICU, pediatric intensive care unit; SS, septic shock survivors; SNS, septic shock non-survivors; IDA, information dependent acquisition; PCA, principal component analysis; OPLS-DA, orthogonal partial least squares discriminant analysis; VIP, variable influence on projection; ROC, receiver operating characteristic; KEGG, Kyoto Encyclopedia of Genes and Genomes; AUC, area under the curve.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was reviewed and approved by the Institutional Review Board of the Children’s Hospital of Chongqing Medical University on November 22, 2017 (No.2017-3-1). Informed consent for this study was obtained from the guardians of all pediatric patients. The study procedures were performed in accordance with the institutional ethical standards for human experimentation and the 1975 Helsinki Declaration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Natural Science Foundation of Chongqing (Grant No. CSTB2023NSCQ-MSX0196) and Chongqing Science and Technology Bureau (Grant No. cstc2017shmsA130075).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
2. Watson RS, Carrol ED, Carter MJ, et al. The burden and contemporary epidemiology of sepsis in children. Lancet Child Adolesc Health. 2024;8(9):670–681. doi:10.1016/S2352-4642(24)00140-8
3. Sanchez-Pinto LN, Bennett TD, DeWitt PE, et al. Development and validation of the phoenix criteria for pediatric sepsis and septic shock. JAMA. 2024;331(8):675–686. doi:10.1001/jama.2024.0196
4. Wang Y, Sun B, Yue H, et al. An epidemiologic survey of pediatric sepsis in regional hospitals in China. Pediatr Crit Care Med. 2014;15(9):814–820. doi:10.1097/PCC.0000000000000247
5. Liu R, Yu Z, Xiao C, et al. Epidemiology and clinical characteristics of pediatric sepsis in PICUs in Southwest China: a prospective multicenter study. Pediatr Crit Care Med. 2024;25(5):425–433. doi:10.1097/PCC.0000000000003450
6. Bassat Q, Blau DM, Ogbuanu IU, et al. Causes of death among infants and children in the Child Health and Mortality Prevention Surveillance (CHAMPS) network. JAMA Network Open. 2023;6(7):e2322494. doi:10.1001/jamanetworkopen.2023.22494
7. Weiss SL, Peters MJ, Alhazzani W, et al. Surviving sepsis campaign international guidelines for the management of septic shock and sepsis-associated organ dysfunction in children. Pediatr Crit Care Med. 2020;21(2):e52–e106. doi:10.1097/PCC.0000000000002198
8. Davis AL, Carcillo JA, Aneja RK, et al. American college of critical care medicine clinical practice parameters for hemodynamic support of pediatric and neonatal septic shock. Crit Care Med. 2017;45(6):1061–1093. doi:10.1097/CCM.0000000000002425
9. Schlapbach LJ, Watson RS, Sorce LR, et al. International consensus criteria for pediatric sepsis and septic shock. JAMA. 2024;331(8):665–674. doi:10.1001/jama.2024.0179
10. Weiss SL, Fitzgerald JC. Pediatric sepsis diagnosis, management, and sub-phenotypes. Pediatrics. 2024;153(1). doi:10.1542/peds.2023-062967
11. Atreya MR, Huang M, Moore AR, et al. Identification and transcriptomic assessment of latent profile pediatric septic shock phenotypes. Crit Care. 2024;28(1):246. doi:10.1186/s13054-024-05020-z
12. Vincent JL. Current sepsis therapeutics. EBiomedicine. 2022;86:104318. doi:10.1016/j.ebiom.2022.104318
13. Siddiqui MA, Pandey S, Azim A, et al. Metabolomics: an emerging potential approach to decipher critical illnesses. Biophys Chem. 2020;267:106462. doi:10.1016/j.bpc.2020.106462
14. Pandey S. Sepsis, management & advances in metabolomics. Nanotheranostics. 2024;8(3):270–284. doi:10.7150/ntno.94071
15. Pandey S, Azim A, Sinha N. Longitudinal NMR based serum metabolomics to track the potential serum biomarkers of septic shock. Nanotheranostics. 2023;7(2):142–151. doi:10.7150/ntno.79394
16. Wildman E, Mickiewicz B, Vogel HJ, et al. Metabolomics in pediatric lower respiratory tract infections and sepsis: a literature review. Pediatr Res. 2023;93(3):492–502. doi:10.1038/s41390-022-02162-0
17. Mickiewicz B, Vogel HJ, Wong HR, et al. Metabolomics as a novel approach for early diagnosis of pediatric septic shock and its mortality. Am J Respir Crit Care Med. 2013;187(9):967–976. doi:10.1164/rccm.201209-1726OC
18. Wang L, Cha X, Zhang Z, et al. Discrimination of serum metabolomics profiles in infants with sepsis, based on liquid chromatography-mass spectrometer. BMC Infect Dis. 2023;23(1):46. doi:10.1186/s12879-023-07983-w
19. Li GB, Hu HR, Pan WF, et al. Plasma metabolic profiling of pediatric sepsis in a chinese cohort. Front Cell Dev Biol. 2021;9:643979. doi:10.3389/fcell.2021.643979
20. Zhu S, Han X, Yang R, et al. Metabolomics study of ribavirin in the treatment of orthotopic lung cancer based on UPLC-Q-TOF/MS. Chem Biol Interact. 2023;370:110305. doi:10.1016/j.cbi.2022.110305
21. Zhuang J, Tang X, Du Z, et al. Prediction of biomarkers of therapeutic effects of patients with lung adenocarcinoma treated with gefitinib based on progression-free-survival by metabolomic fingerprinting. Talanta. 2016;160:636–644. doi:10.1016/j.talanta.2016.08.007
22. Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. 2005;6(1):2–8. doi:10.1097/01.PCC.0000149131.72248.E6
23. Wang S, Xiao C, Liu C, et al. Identification of biomarkers of sepsis-associated acute kidney injury in pediatric patients based on UPLC-QTOF/MS. Inflammation. 2020;43(2):629–640. doi:10.1007/s10753-019-01144-5
24. Scott HF, Brou L, Deakyne SJ, et al. Association between early lactate levels and 30-day mortality in clinically suspected sepsis in children. JAMA Pediatr. 2017;171(3):249–255. doi:10.1001/jamapediatrics.2016.3681
25. Coopersmith CM, De Backer D, Deutschman CS, et al. Surviving sepsis campaign: research priorities for sepsis and septic shock. Crit Care Med. 2018;46(8):1334–1356. doi:10.1097/CCM.0000000000003225
26. Tome D. Amino acid metabolism and signalling pathways: potential targets in the control of infection and immunity. Nutr Diabetes. 2021;11(1):20. doi:10.1038/s41387-021-00164-1
27. Li P, Yin YL, Li D, et al. Amino acids and immune function. Br J Nutr. 2007;98(2):237–252. doi:10.1017/S000711450769936X
28. Blaauw R, Nel DG, Schleicher GK. Plasma glutamine levels in relation to intensive care unit patient outcome. Nutrients. 2020;12(2):402. doi:10.3390/nu12020402
29. Zhu Y, Chen X, Lu Y, et al. Glutamine mitigates murine burn sepsis by supporting macrophage M2 polarization through repressing the SIRT5-mediated desuccinylation of pyruvate dehydrogenase. Burns Trauma. 2022;10:c41. doi:10.1093/burnst/tkac041
30. Kovarik M, Muthny T, Sispera L, et al. Effects of beta-hydroxy-beta-methylbutyrate treatment in different types of skeletal muscle of intact and septic rats. J Physiol Biochem. 2010;66(4):311–319. doi:10.1007/s13105-010-0037-3
31. Patel SS, Molnar MZ, Tayek JA, et al. Serum creatinine as a marker of muscle mass in chronic kidney disease: results of a cross-sectional study and review of literature. J Cachexia Sarcopenia Muscle. 2013;4(1):19–29. doi:10.1007/s13539-012-0079-1
32. Mickiewicz B, Duggan GE, Winston BW, et al. Metabolic profiling of serum samples by 1H nuclear magnetic resonance spectroscopy as a potential diagnostic approach for septic shock. Crit Care Med. 2014;42(5):1140–1149. doi:10.1097/CCM.0000000000000142
33. McNamara RK. Role of omega-3 fatty acids in the etiology, treatment, and prevention of depression: current status and future directions. J Nutr Intermed Metab. 2016;5:96–106. doi:10.1016/j.jnim.2016.04.004
34. Pandey S, Adnan Siddiqui M, Azim A, et al. Serum metabolic profiles of septic shock patients based upon co-morbidities and other underlying conditions. Mol Omics. 2021;17(2):260–276. doi:10.1039/D0MO00177E
35. Esterbauer H, Schaur RJ, Zollner H. Chemistry and biochemistry of 4-hydroxynonenal, malonaldehyde and related aldehydes. Free Radic Biol Med. 1991;11(1):81–128. doi:10.1016/0891-5849(91)90192-6
36. Imai Y, Kuba K, Neely GG, et al. Identification of oxidative stress and Toll-like receptor 4 signaling as a key pathway of acute lung injury. Cell. 2008;133(2):235–249. doi:10.1016/j.cell.2008.02.043
37. Wyatt TA, Kharbanda KK, McCaskill ML, et al. Malondialdehyde-acetaldehyde-adducted protein inhalation causes lung injury. Alcohol. 2012;46(1):51–59. doi:10.1016/j.alcohol.2011.09.001
38. Johansson PI, Nakahira K, Rogers AJ, et al. Plasma mitochondrial DNA and metabolomic alterations in severe critical illness. Crit Care. 2018;22(1):360. doi:10.1186/s13054-018-2275-7
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.