Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Metabolic Regulation in Acute Respiratory Distress Syndrome: Implications for Inflammation and Oxidative Stress
Received 15 August 2024
Accepted for publication 1 December 2024
Published 18 February 2025 Volume 2025:20 Pages 373—388
DOI https://doi.org/10.2147/COPD.S491687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Lixia Yue, Yihe Yan
Department of Critical Care Medicine, Shaoxing People’s Hospital, Shaoxing, Zhejiang, 312000, People’s Republic of China
Correspondence: Yihe Yan, Email [email protected]
Abstract: Acute respiratory distress syndrome (ARDS) is a severe and life-threatening pulmonary condition characterized by intense inflammation and disrupted oxygen exchange, which can lead to multiorgan failure. Recent findings have established ARDS as a systemic inflammatory disorder involving complex interactions between lung injury, systemic inflammation, and oxidative stress. This review examines the pivotal role of metabolic disturbances in the pathogenesis of ARDS, emphasizing their influence on inflammatory responses and oxidative stress. Common metabolic abnormalities in ARDS patients, including disruptions in carbohydrate, amino acid, and lipid metabolism, contribute significantly to the disease’s severity. These metabolic dysfunctions interplay with systemic inflammation and oxidative stress, further exacerbating lung injury and worsening patient outcomes. By analyzing the regulatory mechanisms of various metabolites implicated in ARDS, we underscore the potential of targeting metabolic pathways as a therapeutic approach. Such interventions could help attenuate inflammation and oxidative stress, presenting a promising strategy for ARDS treatment. Additionally, we review potential drugs that modulate metabolic pathways, providing valuable insights into the etiology of ARDS and potential therapeutic directions. This comprehensive analysis enhances our understanding of ARDS and highlights the importance of metabolic regulation in the development of effective treatment strategies. Key findings from this review demonstrate that metabolic disturbances, particularly those affecting carbohydrate, amino acid, and lipid metabolism, play critical roles in amplifying inflammation and oxidative stress, underscoring the potential of metabolic-targeted therapies to improve patient outcomes.
Keywords: acute respiratory distress syndrome, pathogenesis, lung injury, metabolism, medication
Introduction
Acute Respiratory Distress Syndrome (ARDS) is an intense lung disease that typically occurs in patients hospitalized with other illnesses or major injuries, resulting in reduced oxygen in the bloodstream, affecting the normal functioning of organs.1 Symptoms primarily include severe shortness of breath, usually within hours to days of infection or injury.2 ARDS patients are often associated with pulmonary hypertension risk,3 high mortality,4 and lack of effective treatment.5 Based on the definition of Berlin, the diagnosis of ARDS depends on a PaO2/FiO2 ratio below 300 and unproven cardiogenic pulmonary edema.6 The occurrence of ARDS in the United States is assessed to be 64.2 to 78.9 cases /100,000 person-years,7 and the mortality rate corresponds with the disease severity: 27%, 32%, and 45% for mild, moderate, and severe cases, appropriately.8 The occurrence of ARDS in intensive care units (ICUs) in mainland China is low, but the high mortality rate and withdrawal rate of life-saving treatment in patients with moderate-to-severe ARDS are concerning.9 The pathogenic mechanism underlying ARDS remains largely unclear and there are currently no specific drugs available for its effective treatment in clinical practice.1
There is an urgent need to comprehensively elucidate the pathogenic mechanisms underlying ARDS to identify potential targets for novel therapeutic interventions. Recent research has shed light on the intricate interactions among systemic inflammation, oxidative stress, and metabolic disturbances that drive disease progression. Emphasizing these emerging insights and contextualizing them within current literature is essential for advancing the understanding of ARDS and fostering the development of effective treatment strategies. Glucocorticoid (GC) therapy for ARDS, particularly during the COVID-19 pandemic, remains debated despite growing insights into its mechanisms and clinical use. Effective GC treatment hinges on key pharmacological principles, including the choice of agent (eg, hydrocortisone, methylprednisolone, dexamethasone), dosing, timing, and treatment duration. Recent studies emphasize early intervention, an initial bolus for optimal GR saturation, and continuous infusion to sustain therapeutic levels. Variability in patient response due to differing plasma concentrations necessitates dose adjustments tailored to clinical progress, followed by careful tapering to restore HPA axis function. The heterogeneity of ARDS and inconsistent GC regimens complicate outcomes, underscoring the need for standardized approaches informed by current pharmacological knowledge.10,11
In recent years, research on ARDS has gradually increased, and understanding of ARDS has deepened. As a systemic inflammatory disease, it involves the interaction between the lungs and other organ systems, resulting in not only lung damage but also a significant elevation of numerous inflammatory cytokines.10 Regulation of metabolism in inflammation and oxidative stress takes place a major function before and during the onset of ARDS.11 Metabolic disturbances are common in patients with ARDS. Alveolar epithelial cells and endothelial cells in ARDS patients are damaged, leading to cell metabolism disorders, such as mitochondrial dysfunction,12 amino acid metabolism,13 and lipid metabolism abnormalities,14 among others. These metabolic disturbances interact with inflammatory responses to further aggravate the condition of ARDS patients.15 For example, it was found that energy metabolism disturbance caused by mitochondrial dysfunction can lead to increased apoptosis and worsened inflammatory response in patients with ARDS.16 In terms of amino acid metabolism, a study found that phenylalanine metabolism was the major significantly altered pathway among non-survivors and survivors of ARDS patients, and increased phenylalanine levels may be related to more severe lung injury and high rate of mortality in ARDS.17 In addition, abnormal lipid metabolism, such as phosphatidic acid choline metabolism disorder18 and decreased desaturase activity,19 may lead to a decrease in alveolar surfactant, which in turn aggravates lung damage in ARDS patients.
Second, oxidative stress takes place a vital role in the pathophysiology of ARDS. Oxidative stress refers to the imbalance between oxidants and antioxidants in organisms, which leads to the accumulation of oxidants in organisms and induces cell damage.20 Oxidative stress in ARDS patients is mainly manifested as increased oxygen free radicals production and decreased antioxidant system capacity.21 Oxygen free radicals can directly lead to the peroxidation of cell membrane phosphatidic acid, destroy cell structure, and aggravate lung damage.22,23 At the same time, oxygen free radicals can also indirectly trigger the deterioration of the inflammatory response in ARDS patients by inducing the stimulation of inflammatory cells and promoting the inflammatory cytokines production.24 Studies have found that antioxidants like vitamin E25 and N-acetylcysteine26 have a certain therapeutic effect on ARDS patients, which may be associated with the reduction of oxidative stress. The decrease in antioxidant system capacity weakens the antioxidant defense of ARDS patients and makes them more susceptible to oxidative stress damage. For example, the activities of antioxidant enzymes like superoxide dismutase (SOD)27 and glutathione peroxidase (GPx)28 are reduced in patients with ARDS, which cannot effectively scavenge oxygen free radicals, resulting in exacerbated oxidative stress damage. It can be seen that the regulation of metabolism on oxidative stress takes place a major part in the pathophysiological process of ARDS.
Cell metabolism disorder is nearly associated with the inflammatory response and oxidative stress, which further aggravate the patient’s condition. Therefore, improving the inflammatory response and oxidative stress in patients with ARDS through metabolic regulation, such as improving mitochondrial function, regulating lipid metabolism, and enhancing the ability of the antioxidant system, may become an important direction for future ARDS treatment strategies. In conclusion, it is required to contemplate the alterations in metabolite levels and their regulatory effects on ARDS, which will help monitor and control the development of the disease, improve patients’ prognosis, and even save their lives. Therefore, this review aims to summarize the regulation of metabolism on inflammatory response and oxidative stress in the pathogenesis of ARDS, explain the regulatory effects of various metabolites and the mechanisms involved, and finally introduce the current potential therapeutic drugs for metabolic regulation in ARDS. This will help provide more evidence support for the etiology and pathophysiology of ARDS.
Metabolic Dysfunction and ARDS
In healthy individuals, metabolism takes place an important part in maintaining homeostasis by controlling energy production,29 nutrient breakdown,30 and waste removal.31 However, in ARDS patients, metabolic dysregulation occurs, affecting inflammatory responses and oxidative stress.32 This dysregulation involves disruptions in carbohydrate, amino acid, and lipid metabolism, among others,33 thereby leading to aggravate lung damage in ARDS patients. The findings from these studies are summarized in Table 1.
 |
Table 1 Summary of Key Findings on Metabolism and Health |
Carbohydrate Metabolism in ARDS
Carbohydrate metabolism is essential in maintaining energy homeostasis within the body. This process involves the breakdown of carbohydrates, such as glucose, into smaller molecules to generate ATP, which serves as a primary energy source for various cellular functions. Essential for the maintenance of blood glucose, there are other pathways including gluconeogenesis, the synthesis and breakdown of glycogen that takes place the blood glucose homeostasis regulation. In addition, in carbohydrate metabolism, the metabolites intersect with signaling pathways, and regulate the activities of cells through post-translational modification of key proteins in the pathways. Moreover, carbohydrate metabolism takes place an important part in the control of immune responses, cellular growth and repair processes, along with inflammatory responses and oxidative stress.34
In ARDS patients, abnormalities in carbohydrate metabolism can have detrimental effects on their condition. It has been established that elevated blood glucose levels can negatively impact the survival and prognosis of patients with ARDS (Figure 1). Hyperglycemia is frequently observed in critically ill patients and is closely correlated with high rate of mortality and morbidity, and it has been shown to worsen inflammation and oxidative stress in ARDS animal models.35 A study evaluating the effect of blood glucose on cognitive effects in ARDS patients one year after hospital discharge demonstrated a significant association between blood glucose concentrations and cognitive sequelae, as evidenced by a longer duration of mechanical ventilation.36 Mechanistic studies have shown that increased glucose levels can stimulate reactive oxygen species (ROS) production through protein kinase C (PKC)-dependent stimulation of NAD(P)H oxidase. NAD(P)H oxidase-dependent ROS generation may damage DNA in tissues, that causes various complications37(Figure 1). Additionally, glucose-6-phosphate dehydrogenase (G6PD) takes place a crucial part in both ROS generation and removal by supplying NADPH (Figure 1). G6PD activation has been associated with enhanced oxidative inflammation during acute lung injury (ALI). ALI is defined by high inflammatory response, which, if left untreated, can progress to ARDS. However, disturbances in blood sugar levels can exacerbate inflammation and contribute to ARDS development. A case report documented the onset of diabetic ketoacidosis (DKA) inducing a cytokine storm, which led to the development of ARDS. Inhibiting G6PD may be a potential strategy to limit oxidative damage and improve airway function during ALI, as glucose metabolism is involved in ROS regulation and inflammation activation, thereby inducing ARDS.38 It seems like that tight glycemic control has been related to high outcomes in some clinical trials.39 Hence, other studies have reported conflicting results,40 highlighting the complexity of glucose metabolism in ARDS.
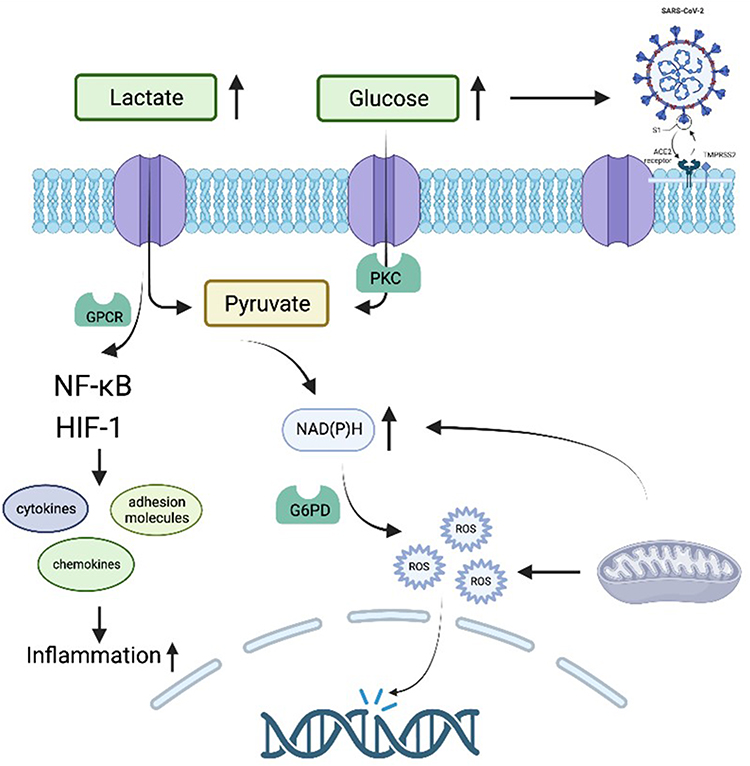 |
Figure 1 A schematic representation showing the alterations in carbohydrate metabolites’ metabolic pathways amid ARDS. During ARDS, the metabolic pathways encompassing carbohydrates, such as glucose and lactate, undergo transformative changes. This diagram tentatively demonstrates that perturbations in glucose and lactate concentrations instigate a cascade of intermediate receptor regulation, notably GPCR and PKC, affecting downstream signaling molecules. Concurrently, the disruption in energy metabolism precipitates ROS generation and free radicals, which consequently inflict DNA damage and instigate inflammation. For further information, refer to the main text. Abbreviations: PKC, Protein kinase C; GPCR, G-protein-coupled receptors; NF-κB, Nuclear factor kappa B; HIF-1, Hypoxia-Inducible Factor; G6PD, Glucose-6-phosphate dehydrogenase; ROS, Reactive oxygen species. |
Lactate is also implicated in the pathophysiology of ARDS patients (Figure 1). A study involving samples from 194 critically ill patients with various diagnoses and 306 dogs found that patients with respiratory failure due to ARDS can exhibit increased pulmonary lactate production, which is proportional to disease severity.41 In recent years, research on the differential genes expression and associated pathways in ARDS patient phenotypes has revealed that elevated plasma lactate levels are associated with oxidative phosphorylation and increased gene expression, potentially caused by mitochondrial dysfunction and alterations in energy metabolism42 (Figure 1). Lactate’s effects on inflammatory processes can vary depending on the metabolic state, cell type, and pathological process analyzed, as well as its interactions with various targets, such as G-protein-coupled receptors, post-translational modifications and transcription factors like NF-κB and HIF-1.43 These interactions enable lactate to regulate cytokines, chemokines, adhesion molecules, and signaling pathways (Figure 1) for the expression of several enzymes taking part in immune response and metabolism, elucidating its differential effects on inflammatory processes beyond its role as a well-known metabolic waste product.
Moreover, impaired carbohydrate metabolism can affect immune responses, contributing to a pro-inflammatory state and exacerbating lung injury. A study modeling ARDS caused by the COVID-19 novel coronavirus, it was found that elevated glucose provides optimum conditions for the virus to avoid and weakening the lungs first-level immune defense system. Because of the presence of glucose, it assists the progression of virus-induced ARDS in patients, further promotes cell death, and induces an inflammatory response in the lungs, which can overwhelm the already weakened innate immune system, triggering systemic infection, inflammation, etc.44 (Figure 1). Additionally, glycolysis, the process of breaking down glucose to produce energy is elevated in the immune cells of ARDS patients,45 such as metabolic changes in leukocytes, which takes place a vital part in the immune response, have been linked to immune paralysis in sepsis, a condition that shares similarities with ARDS. Consequently, addressing these metabolic disturbances through interventions, such as proper nutritional support, may improve outcomes in ARDS patients.
Lipid Metabolism in ARDS
Lipid metabolism refers to the biological processes accountable for the synthesis, storage, and breakdown of lipids, which are the main components of cell membranes and serve as energy sources for the body.46 Lipid mediators, such as prostaglandins and leukotrienes,47 play crucial roles in modulating inflammation by regulating the recruitment and stimulation of immune cells.48 Additionally, certain lipids, like plasmalogens, can act as antioxidants, neutralizing ROS and preventing oxidative damage to cellular structures.49
In patients with ARDS, dysregulation of lipid metabolism contributes to the inflammatory response and regulation of ROS, promoting inflammation and lung injury (Figure 2). Moreover, disrupted lipid metabolism can affect the production and clearance of ROS, leading to oxidative stress that damages cellular components and exacerbates ARDS severity. A study demonstrated that alterations in phosphatidylcholine (PC) metabolism in ARDS patients correlated with increased inflammation and oxidative stress,50 resulting in more severe lung injury and lower levels of surfactant PC species, which contribute to alveolar collapse and heightened inflammation51 (Figure 2). Some studies have employed mass spectrometry (MS) to analyze differences in lipid metabolites between ARDS patients and healthy individuals. In comparison to healthy controls, ARDS patients exhibited significantly different plasma PC compositions, with an overall increase in methyl-D9-PC enrichment but considerably lower enrichment of methyl-D3-PC and methyl-D6-PC, indicating significant changes in the PC synthesis pathway in ARDS patients.52 Research has confirmed that PCs produced via different pathways yield distinct effects (Figure 2). Importantly, PCs can synthesize precursors of inflammation-inducing substances53 that are released and subsequently produce modulatory oxidative metabolites implicated in the pathogenesis of ARDS.54,55 In compared with, DHA (sn-2 22:6), synthesized by PC, can reduce inflammation.56 Additionally, ARDS patients are characterized by reduced plasma PUFA concentrations;57 however, these mechanisms remain unelucidated. The lipid metabolism pathway is also related to ROS regulation. Phospholipids (PL) are converted into lipid biomarkers under the action of phospholipases and ROS, which are activated or released under specific physiological and pathophysiological conditions, potentially implicating them in ARDS regulation. Notably, during tissue repair in later inflammation stages, the inflammatory cells produce excess ROS accumulation, it can cause irreversible DNA damage in new cells, such as deletions, point mutations and rearrangements58 (Figure 2). Additionally, excess intracellular and extracellular oxygen free radicals can initiate various destructive reactions. Oxygen free radicals can binds with lipids on the plasma membrane surface, resulting in peroxidation of lipid and the new free radicals formation, that are highly unreliable and readily decompose into carbonyls, malondialdehyde and volatile hydrocarbons like ethane and pentane59,60 (Figure 2). The lipid peroxidation process disrupts the cell membrane structure, results in alterations in the phospholipid bilayer’s physical properties, and oxygen free radicals inflict significant damage on lung cells through these processes. These detrimental effects compromise cellular integrity and function, ultimately contributing to the aggravation of pulmonary injury in diseases like ARDS.
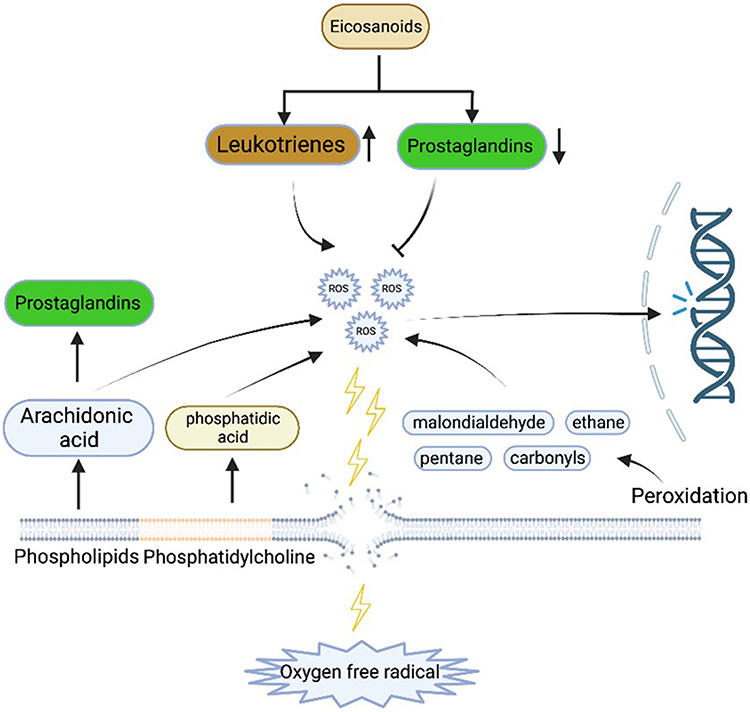 |
Figure 2 A schematic representation elucidating the transformations in the metabolic pathways of lipid metabolites amid ARDS. The metabolic pathways of lipidic substances, including eicosanoids, phospholipids, and phospholipidic cells, are notably transformed during ARDS. This diagram broadly illustrates that lipid constituents of the cellular membrane are compromised by various provocateurs, including oxygen-free radicals, leading to a perturbation and decomposition of lipid metabolism. This results in the generation of pro-inflammatory and ROS-inducing lipid secondary metabolites, in turn exacerbating DNA damage and cellular membrane detriment. Refer the main text for additional information. |
One of the lipids that play an essential role in ARDS is eicosanoids, derived from arachidonic acid. These lipid mediators significantly regulate inflammation (Figure 2). An imbalance in eicosanoid production, such as increased pro-inflammatory leukotrienes and decreased anti-inflammatory prostaglandins levels, has been implicated in ARDS pathogenesis. Excessive pro-inflammatory eicosanoids production contributes to sustained inflammation and increased ROS generation in ARDS patients (Figure 2). According to a lipidomic analysis, bronchoalveolar lavage fluid (BALs) of patients with COVID-19-induced ARDS is categorized by high levels of fatty acids and inflammatory lipid mediators, with thromboxanes and prostaglandins predominating. There is also an increased level of Leukotrienes, especially LTE4, LTB4 and eoxin E4. Additionally, monohydroxylated 15-lipoxygenase metabolites of linoleic acid, arachidic acid, eicosapentaenoic acid, and docosahexaenoic acid were increased. Notably, however, lysis-promoting mediators, specifically lipotoxin A4 and D-series lysins also increased, emphasizing the lipid mediator storm occurring in severe COVID-19 involving pro-inflammatory and anti-inflammatory lipids balance. Eicosanoids exert complex regulation on many physiological systems in inflammatory and immune responses and act as messengers in the central nervous system. Eicosanoic acid controls pro-inflammatory and anti-inflammatory effectors closely related to inflammation, forming one of the human body’s most complex regulatory networks. Many studies have suggested that arachidonic acid metabolites takes place a major role in acute lung injury/ARDS development. Normally, arachidonic acid is bound to cell membrane phospholipids. After injury, under various mediators’ action and phospholipase, arachidonic acid is released from membrane phospholipids. The lung is an essential organ in the cascade of arachidonic acid due to its enzymatic capacity to synthesize all arachidonic acid derivatives while being largely responsible for the selective breakdown of circulating eicosanes. This might explain why Eicosanoids levels increased after lung injury in ARDS patients.61
Moreover, lipid metabolism is involved in immune regulation in ARDS patients. For instance, dysregulated sphingolipid metabolism, including elevated ceramide levels, can promote immune cell apoptosis, thus weakening the immune response. Furthermore, alterations in surfactants’ lipid composition, such as PC described earlier, can compromise innate immune defense mechanisms in the lung, resulting in increased susceptibility to infections. Overall, lipid metabolism dysregulation in ARDS patients takes place a significant part in modulating immune function and influencing disease outcomes.
Amino Acid Metabolism in ARDS
Amino acid metabolism encompasses the series of biochemical reactions responsible for the synthesis, degradation and utilization of amino acids, which are the fundamental components of proteins.62 These metabolic processes are essential for protein production, energy generation, and the creation of various biologically significant molecules such as hormones and neurotransmitters.63 By participating in the maintenance of cellular balance and the regulation of multiple physiological processes, amino acid metabolism serves a crucial role in immune function,64 inflammation,65 and oxidative stress management.66
In the context of ARDS, abnormalities in the metabolism of amino acid can influence the development of the disease and aggravate the inflammatory response and ROS generation (Figure 3). Altered concentrations of specific amino acids, like glutamine and arginine, have been associated with immune dysfunction and increased inflammation in ARDS patients.67,68 Glutamine is necessary for growth of immune cell and activation and helps maintain the intestinal mucosa integrity, which acts as a barrier against pathogens.69 A study assessing the glutamine treatment effects on leukocyte numbers in bronchoalveolar lavage fluid (BALF), inflammatory status in lung tissue and lung morphology and function in an endotoxin-induced pulmonary ARDS mouse model suggested that glutamine treatment reduced functional and morphological damage, inflammation and ROS release. This has also been supported by animal experiments, such as in C57BL/6 mice, where glutamine was pre-supplemented in the diet before ARDS induction. Researchers observed activation of anti-inflammatory pathways in alveolar macrophages despite increased early inflammatory cytokines and neutrophil recruitment.70–72Arginine also plays a role in lung injury, specifically involving endothelial nitric oxide synthase (eNOS) activity.73 Arginine deficiency causes eNOS to produce superoxide, which subsequently generates cytotoxic peroxynitrite. This leads to alterations in protein structure and function, such as PKC74 (Figure 3). Arginine’s involvement in the regulation of lung injury has been corroborated by other studies that demonstrated its effect on ARDS.75 A clinical trial supplementing L-arginine twice daily in patients with COVID-19-induced ARDS determined that it reduced the length of hospital stays and respiratory support compared to the placebo group, without increasing serious adverse events, indicating a beneficial effect.76 Many other amino acids have similar effects. For instance, a metabolic analysis revealed that at the onset of ARDS, non-survivors had remarkably higher rates of tryptophan degradation and concentrations of metabolites downstream of the kynurenine pathway than survivors. A regression analysis identified that kynurenine pathway stimulation is related to mortality in ARDS patients.77
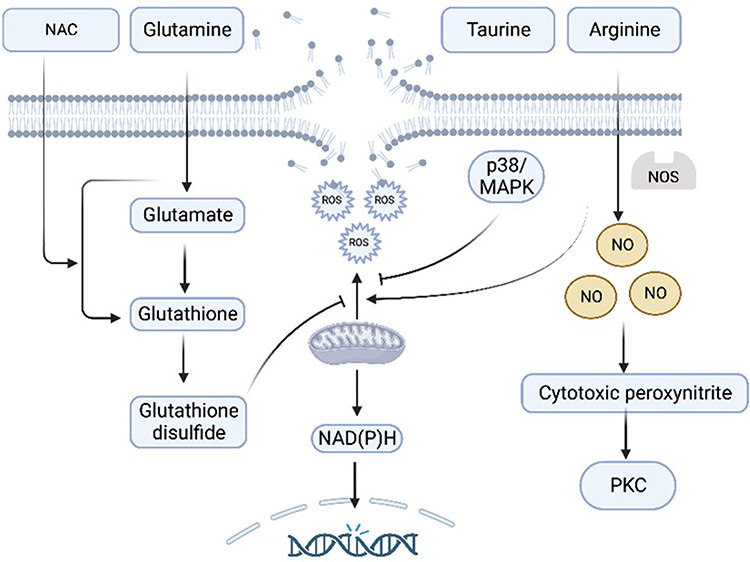 |
Figure 3 A schematic representation showing the changes in metabolic pathways of amino acid metabolites amid ARDS. During ARDS, there exist aberrations in the levels of certain amino acids like glutamine and arginine. The metabolism of these amino acids is regulated by other amino acids or signaling molecules, acting to either stimulate or curtail the mitochondrial oxygen free radicals production. However, these free radicals possess the potential to damage DNA and cellular membranes. For further information, refer to the main body of the text. |
Amino acid metabolism is disrupted in ARDS patients, and the availability of these amino acids may be reduced, compromising immune function and increasing vulnerability to infections. In addition to the amino acids described above, some substances can improve the immune function of ARDS patients by regulating inflammation and ROS. For example, taurine is a sulfur-containing non-essential amino acid with antioxidant, cell membrane-stabilizing, and anti-inflammatory effects (Figure 3). An animal study demonstrated that taurine improves lung injury by suppressing the inflammatory response and oxidative stress through the p38/MAPK signaling pathway78 (Figure 3). In patients with COVID-19-induced ARDS, taurine can reduce oxidative stress levels and inflammatory damage, effectively improving immune function.79 N-acetylcysteine (NAC) is a cysteine derivative with antioxidant and anti-inflammatory properties. NAC can increase the body’s glutathione (GSH) levels, thereby enhancing antioxidant capacity (Figure 3). It has also been effective in treating ARDS patients in ICUs.26
Collectively, abnormal amino acid metabolism can lead to excessive ROS production, causing oxidative stress and cellular damage, which ultimately exacerbates lung injury and worsens ARDS severity. Investigating and targeting amino acid metabolism in ARDS patients may offer innovative therapeutic approaches for modulating inflammation, oxidative stress, and disease progression.
Other Metabolism Pathways
ARDS is intricately connected to metabolism. In addition to the traditional pathways of carbohydrate, lipid, and amino acid metabolism, other metabolic pathways such as purine metabolism,15 heme metabolism,80 etc. also provide the regulation of inflammation and oxidative stress, subsequently influencing ARDS.
Purine metabolism takes place a significant part in maintaining cellular energy balance and nucleic acid synthesis, while being closely linked to inflammation regulation and oxidative stress.81 Studies have revealed that abnormal purine metabolism may exacerbate the inflammatory response in ARDS patients (Figure 4). Purine metabolism has long been associated with ARDS.82 One research focused to examining the function of serum uric acid levels in predicting ARDS patients’ outcomes. The study included 33 ARDS patients and determined that serum uric acid levels could predict the mortality rate of these patients. This observation may be attributed to uric acid, a final product of purine degradation, which increases in a sensitive but nonspecific manner during lung tissue injury and inflammation.83 Another study reached a consistent conclusion. Researchers included 237 ARDS patients and compared the survival rates of patients with varying uric acid levels through survival analysis. They discovered that ARDS patients with low serum uric acid levels had a reduced risk of in-hospital death.84 Indeed, these findings are corroborated by a study demonstrating that during hypoxia, the end product of purine degradation, serum uric acid, is markedly increased,85 a characteristic feature in patients with ARDS. Impaired lung function diminishes oxygen intake, leading to tissue hypoxia, which becomes more pronounced during chronic obstructive pulmonary disease (COPD) exacerbations, potentially causing elevated levels of circulating uric acid resulting from damage to the lungs and surrounding tissues. Elevated uric acid levels are related to high levels of inflammatory markers namely C-reactive protein (CRP) and interleukin-6,86 which are also elevated in patients with ARDS. In the purine pathway, in addition to uric acid, studies have also identified inosine, an endogenous purine, as capable of downregulating the TNF-α, IL-1β, IL-6, and Macrophage inflammatory protein-2 (MIP-2) expression induced by LPS, and reducing MIP-1α (Figure 4). Moreover, in ARDS of inbred BALB/c mice challenged with intratracheal LPS, it can increase the production of IL-4.87,88 IL-4 is a potent inducer of M2-specific protein expression, accelerating ALI resolution and lung repair by reprogramming endogenous inflammatory macrophages.89 Consequently, intervention strategies targeting purine metabolism may hold potential for the treatment of ARDS patients.
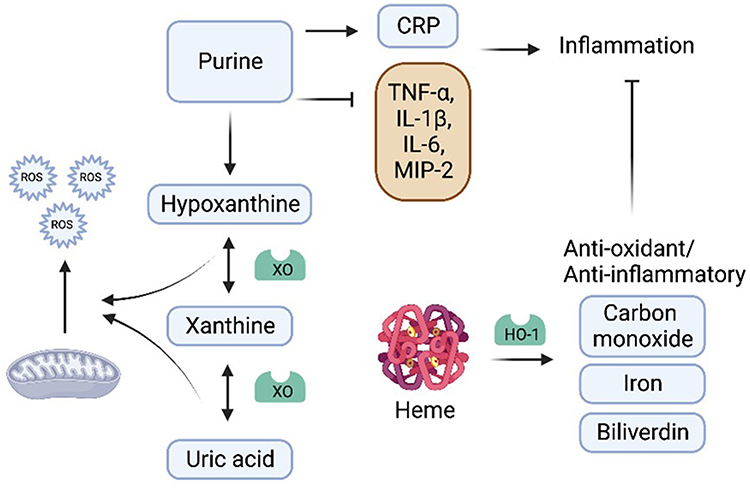 |
Figure 4 A schematic representation illustrating the perturbations in metabolic pathways of miscellaneous metabolites during ARDS. During ARDS, the metabolism of purine and heme is disrupted, which further instigates the generation of secondary metabolites promoting inflammation and ROS production. Generally, the byproducts resulting from the metabolic pathway of heme exhibit protective effects on pulmonary cells. For additional information, refer to the main text. |
The heme molecule is an essential cofactor for the activities of transport of oxygen and storage proteins, as well as cellular metabolic enzymes, namely those involved in xenobiotic metabolism, mitochondrial respiration and antioxidant responses.90 Disorders of heme metabolism may also exacerbate the condition of ARDS patients91 (Figure 4). In one study, the relationship between ARDS and heme was investigated by quantifying the concentration of inducible heme oxygenase (HO)-1 in the lungs of patients with ARDS and assessing its function as a source of ferrous iron and an iron-regulated signaling agent. The results revealed that, compared to patients who underwent lung resection in the control group, the hemoglobin concentration in the lung tissue and BALF fluid of ARDS patients increased significantly, and heme oxygenase protein levels were increased in the lungs of ARDS patients. This finding suggests that hemoglobin and heme oxygenase proteins provide alterations in iron signaling, mobilization and regulation that are prognostic in ARDS.92 The HO system degrades heme to carbon monoxide (CO), iron, and biliverdin-iXα, which is converted to bilirubin-iXα by biliverdin reductase (Figure 4). This degradation is cytoprotective,80 activating anti-inflammatory, anti-oxidative, and anti-apoptotic defense mechanisms, while stimulating mitochondrial quality control programs and biogenesis. Pharmacological stimulation of the HO-1/CO system by inhalation of low doses of CO produces protective effects against inflammation, oxidative stress, sepsis, lung inflammation, ischemia/reperfusion injury, ALI and other pathological conditions. To date, pilot clinical trials of inhaled CO (iCO) therapy, including those for ARDS,93 have initially demonstrated good tolerance, and many clinical trials are still ongoing.94
Heightened inflammation and oxidative stress levels are observed in patients with ARDS and these responses are metabolically regulated. In addition to the aforementioned metabolism, numerous metabolic pathway substances are involved in the regulation of ARDS.13,95,96 Disruption of metabolic pathways exacerbates inflammatory responses and oxidative stress. Intervention strategies targeting these metabolic pathways hold promise for providing new treatments for ARDS patients. However, current research on the role of these metabolic pathways in ARDS is limited, and further basic and clinical research is required to gain a better understanding of their involvement in the pathogenesis of ARDS and to develop more effective treatments for patients.
Therapeutic Implications for ARDS
Understanding the regulation of different metabolic pathways in ARDS is of great significance for drug development and application. As mentioned above, the occurrence and development of ARDS involve various metabolic pathways, namely lipid metabolism, glucose metabolism, amino acid metabolism, purine metabolism, and heme metabolism. In-depth investigation of the mechanisms of action of these metabolic pathways in ARDS can uncover new therapeutic targets and provide individualized treatment options for ARDS patients. Imbalances in metabolic pathways in ARDS patients may exacerbate inflammatory responses and oxidative stress, thereby affecting disease severity and prognosis. Consequently, drug interventions targeting these metabolic pathways are crucial for improving the rate of survival and ARDS patient life’s quality. In experimental and clinical studies, some drugs targeting metabolic pathways have demonstrated promising therapeutic effects, such as anti-inflammatory, anti-oxidative, and tissue repair promotion. A wide understanding of the regulatory mechanisms of different metabolic pathways in ARDS will aid the development and application of drugs, offering more effective treatments for ARDS patients. The information on medication with potential effects on different metabolic pathways is summarized in Table 2.
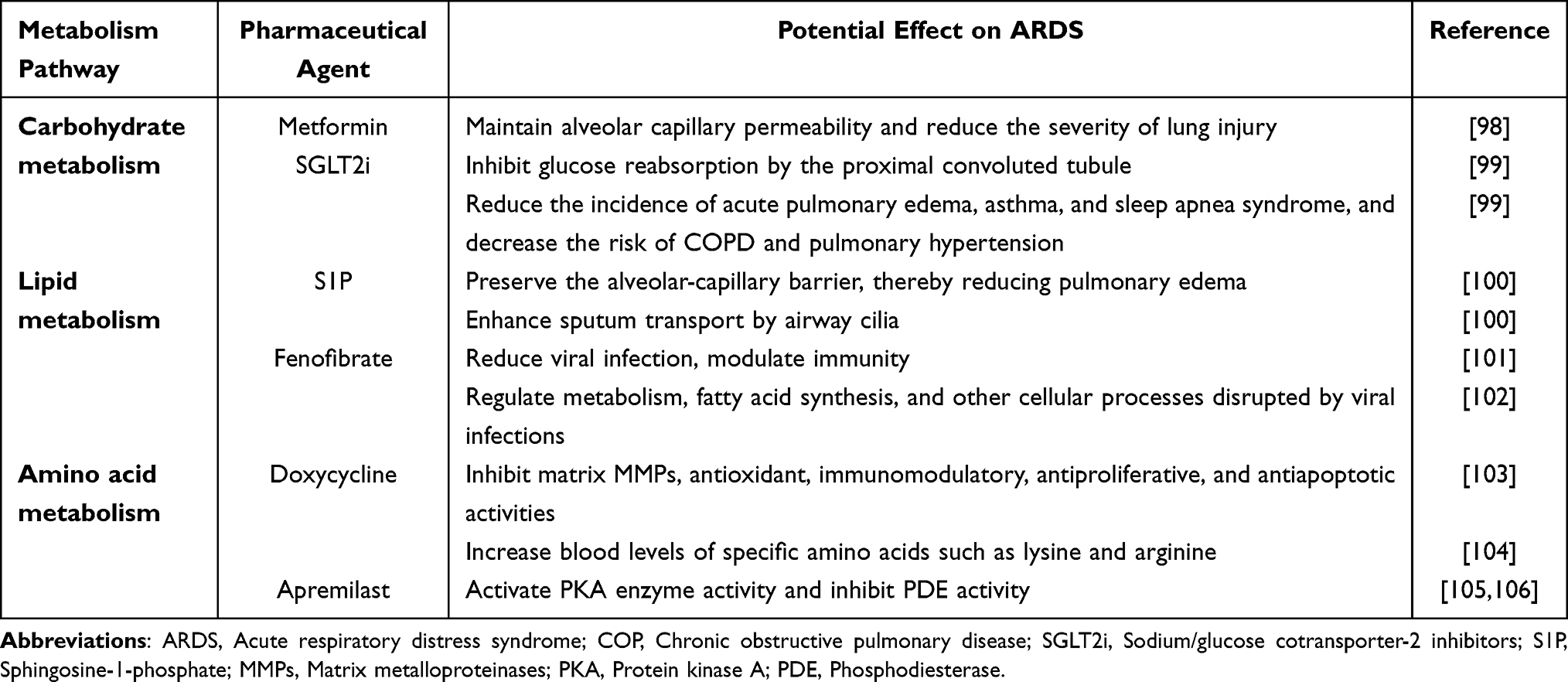 |
Table 2 Medication with Potential Effects on ARDS Based on Different Metabolic Pathways |
Several drugs are currently being tested to modulate metabolism to improve prognosis and survival in patients with ARDS. For example, metformin is well-known for its diverse effects, including recently reported anti-inflammatory activity. One study enrolled patient with type 2 diabetes mellitus (T2D) diagnosed with ARDS and treated them with metformin. It found no difference in ARDS severity index and reduced mortality compared to non-users.106 The protective effect of metformin on lung injury has been studied and confirmed in animal models, possibly by maintaining alveolar capillary permeability and thus reducing lung injury severity.97 Another drug, sodium-glucose cotransporter 2 inhibitors (SGLT2i), primarily acts on the carbohydrate metabolism pathway. A recent study on the relationship between the SGLT2i use and the adverse respiratory events risk in real-world settings found that patients with T2D had a lesser risk of adverse respiratory events with SGLT2s using propensity score matching, indicating that it does not cause damage to the respiratory tract.107 This finding is compatible with the conclusion of another study: a meta-analysis of SGLT2i’s large randomized controlled trials (RCTs) for drug risk assessment found that SGLT2 inhibitors remarkably decrease the incidence of acute asthma, pulmonary edema and sleep apnea syndrome and decrease the risk of COPD and pulmonary hypertension. The possible mechanism is that SGLT2i inhibits glucose reabsorption by the proximal convoluted tubule, leading to a decrease in serum glucose levels, which reduces the glucose available for metabolism, thereby reducing endogenously produced carbon dioxide and relieving carbon dioxide retention, ultimately providing potentially beneficial effects.98 These drugs have the potential to treat ARDS, so in-depth research on carbohydrate metabolism pathways is of great significance for clinical drug use.
Recent studies have also shown potential benefits of drugs that regulate lipid metabolism in ARDS patients, such as surfactants previously used to treat infant respiratory distress syndrome (IRDS), and sphingosine-1-phosphate (S1P), which has been found to have a protective effect in improving symptoms in ALI patients, although it did not improve survival. In a neonatal piglet-based ARDS model, it was found that experimental supplementation with phosphatidylglycerol reduced interleukin-6 (IL-6) and alveolar apoptosis while preserving the alveolar-capillary barrier, thereby reducing pulmonary edema. Mechanistically, lipopolysaccharide (LPS)-induced lung injury was less severe and had less neutrophil infiltration and endothelial exudation in sphingosine kinase (SPK)1-/- mice compared to wild type (WT) mice, with decreased numbers of inflammatory cells in theBAL. Clinical trials using surfactants to treat chronic bronchitis have demonstrated improvements in lung function through enhanced sputum transport by airway cilia.99 However, the efficacy of surfactants in treating ARDS remains less clear.108 Recently, another drug targeting lipid metabolism pathways has garnered interest. Fenofibrate, a peroxisome proliferator-activated receptor alpha (PPAR-α) agonist, is a widely available, low-cost generic drug approved by the FDA and various other regulatory agencies worldwide for the treatment of dyslipidemia. In cellular experiments, fenofibrate was found to reduce viral infection, modulate immunity, and inhibit the replication of the COVID-19 virus.100 Consequently, researchers have become interested in whether fenofibrate could improve ARDS caused by COVID-19. A double-blind clinical trial compared the clinical benefits of fenofibrate in patients with COVID-19-induced ARDS to a control group of ARDS patients receiving a placebo. Although no remarkable variations were observed in the outcomes, no additional adverse events were induced. Prior studies have reported that active metabolites of fenofibrate can regulate metabolism, fatty acid synthesis, and other cellular processes disrupted by viral infections. These findings suggest that the metabolic regulation of fenofibrate can be safely employed in patients diagnosed with ARDS and dyslipidemia, potentially reducing disease burden.101
There are also related studies on drugs for treating ARDS by regulating amino acid metabolism. Doxycycline, a tetracycline antibiotic, interferes with bacterial protein synthesis by interacting with the 30S subunit of the bacterial ribosome, inhibiting bacterial growth, and is thought to possess anti-inflammatory effects. Additionally, it has been shown to reduce serum levels of branched-chain amino acids (BCAAs), essential amino acids involved in protein synthesis and energy metabolism. This effect may be attributable to doxycycline’s ability to decrease the activity of enzymes responsible for BCAA catabolism. Moreover, some research suggests that doxycycline might increase blood levels of specific amino acids, such as lysine and arginine. The development of second-generation tetracyclines, including doxycycline and minocycline, has revealed non-antibiotic properties, such as inhibition of matrix metalloproteinases (MMPs), antioxidant, immunomodulatory, antiproliferative, and antiapoptotic activities.102,103 These properties have prompted their evaluation in various noninfectious diseases, including neurological disorders, cancer and complex inflammatory conditions like ARDS and tissue damage. Animal studies have demonstrated doxycycline’s role in various lung diseases, such as LPS-induced lung inflammation,109 lung injury,110 COPD111 and ARDS.112 The effects may be mediated through the inhibition of inflammatory factors, NO production, and other mechanisms.113 Some clinical studies have also shown potential therapeutic effects on ARDS.114 Another drug, apremilast, is a cAMP-specific phosphodiesterase (PDE4) inhibitor with anti-inflammatory properties commonly used to treat psoriasis. Recent studies have indicated potential roles in modulating oxidative stress in neutrophils and treating ARDS. One study evaluated the effectiveness of apremilast for treating ARDS using an animal model and found that, in addition to reducing ROS generation and activating neutrophil adhesion, it could also activate protein kinase A (PKA) enzyme activity and inhibit PDE activity. Notably, the cAMP/PKA pathway plays a significant part in controlling amino acid metabolism in immune cells, potentially involving the downregulation of gene and protein expression of BCAAs.104,105 These drugs have demonstrated potential therapeutic effects on ARDS and warrant further investigation.
Conclusion
ARDS, a severe respiratory disease, poses a significant threat to patients’ lives and well-being, making its study imperative. In ARDS development, ROS and inflammatory responses serve as key contributors, with metabolic processes influencing ARDS progression by modulating these aspects. Firstly, imbalanced carbohydrate metabolism may result in elevated blood glucose levels, subsequently exacerbating inflammatory responses and ROS production in ARDS patients. Secondly, a disturbance in lipid metabolism might augment the inflammatory response while concurrently increasing the production of free radicals, ultimately causing further lung cell damage. Lastly, amino acid metabolism plays essential roles in ARDS, such as modulating immune cell function and ROS generation. Pharmaceutical interventions influence ARDS development by targeting these metabolic pathways. In conclusion, a thorough investigation of the metabolic mechanisms in ARDS is expected to offer novel insights and approaches for its treatment, ultimately providing a crucial foundation for enhancing patient prognosis.
Targeting metabolic pathways offers significant promise for ARDS treatment, as these pathways play a central role in modulating inflammation and oxidative stress, which are key contributors to disease progression. Drug interventions aimed at regulating metabolic processes, such as glucose, lipid, and amino acid metabolism, can potentially reduce lung injury, improve patient prognosis, and enhance survival rates. Continued research in this area is essential to develop effective therapeutic strategies that leverage these metabolic mechanisms. ARDS, a severe respiratory disease, poses a significant threat to patients’ lives and well-being, underscoring the importance of advancing its study. This review highlights the novel understanding that metabolic processes are not just secondary consequences but active modulators of ARDS progression, primarily through their impact on ROS and inflammatory responses. By exploring the intricate links between metabolism, inflammation, and oxidative stress, this study offers a fresh perspective that could pave the way for targeted metabolic interventions as a new strategy for ARDS treatment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Matthay MA, Zemans RL, Zimmerman GA, et al. Acute respiratory distress syndrome. Nat Rev Dis Primers. 2019;5(1):18.
2. Clinic M ARDS. 2022; Available from: https://www.mayoclinic.org/diseases-conditions/ards.
3. Ñamendys-Silva SA, Santos-Martínez LE, Pulido T, et al. Pulmonary hypertension due to acute respiratory distress syndrome. Braz J Med Biol Res. 2014;47(10):904–910. doi:10.1590/1414-431X20143316
4. Revercomb L, Hanmandlu A, Wareing N, et al. Mechanisms of pulmonary hypertension in Acute Respiratory Distress Syndrome (ARDS). Front Mol Biosci. 2021;7:624093. doi:10.3389/fmolb.2020.624093
5. Horie S, McNicholas B, Rezoagli E, et al. Emerging pharmacological therapies for ARDS: COVID-19 and beyond. Intensive Care Med. 2020;46(12):2265–2283. doi:10.1007/s00134-020-06141-z
6. Palanidurai S, Phua J, Chan YH, et al. P/FP ratio: incorporation of PEEP into the PaO2/FiO2 ratio for prognostication and classification of acute respiratory distress syndrome. Ann Intens Care. 2021;11(1):124. doi:10.1186/s13613-021-00908-3
7. Rhee J, Dominici F, Zanobetti A, et al. Risk of acute respiratory distress syndrome among older adults living near construction and manufacturing sites. Epidemiology. 2020;31(4):468–477. doi:10.1097/EDE.0000000000001195
8. Fanelli V, Vlachou A, Ghannadian S, et al. Acute respiratory distress syndrome: new definition, current and future therapeutic options. J Thorac Dis. 2013;5(3):326–334. doi:10.3978/j.issn.2072-1439.2013.04.05
9. Huang X, Zhang R, Fan G, et al. Incidence and outcomes of acute respiratory distress syndrome in intensive care units of mainland China: a multicentre prospective longitudinal study. Crit Care. 2020;24(1):515. doi:10.1186/s13054-020-03112-0
10. Meduri GU, Annane D, Confalonieri M, et al. Pharmacological principles guiding prolonged glucocorticoid treatment in ARDS. Intensive Care Med. 2020;46(12):2284–2296. PMID: 33150472; PMCID: PMC7641258. doi:10.1007/s00134-020-06289-8.
11. Zhao Y, Yao Z, Xu S, Yao L, Yu Z. Glucocorticoid therapy for acute respiratory distress syndrome: current concepts. J Intensive Med. 2024;4(4):417–432. PMID: 39310055; PMCID: PMC11411438. doi:10.1016/j.jointm.2024.02.002.
12. Zhan B, Shen J. Mitochondria and their potential role in acute lung injury (Review). Exp Ther Med. 2022;24(1):479. doi:10.3892/etm.2022.11406
13. Metwaly S, Cote A, Donnelly SJ, et al. Evolution of ARDS biomarkers: will metabolomics be the answer? Am J Physiol Lung Cell Mol Physiol. 2018;315(4):L526–l534. doi:10.1152/ajplung.00074.2018
14. Alipanah-Lechner N, Neyton L, Mick E, et al. Plasma metabolic profiling implicates dysregulated lipid metabolism and glycolytic shift in hyperinflammatory ARDS. Am J Physiol Lung Cell Mol Physiol. 2023;324(3):L297–l306. doi:10.1152/ajplung.00278.2022
15. Metwaly S, Côté A, Donnelly SJ, et al. ARDS metabolic fingerprints: characterization, benchmarking, and potential mechanistic interpretation. Am J Physiol Lung Cell Mol Physiol. 2021;321(1):L79–L90. doi:10.1152/ajplung.00077.2021
16. Faust HE, Reilly JP, Anderson BJ, et al. Plasma mitochondrial DNA levels are associated with ARDS in trauma and sepsis patients. Chest. 2020;157(1):67–76. doi:10.1016/j.chest.2019.09.028
17. Xu J, Pan T, Qi X, et al. Increased mortality of acute respiratory distress syndrome was associated with high levels of plasma phenylalanine. Respir Res. 2020;21(1):99. doi:10.1186/s12931-020-01364-6
18. Nijmeh J, Levy BD. Lipid-derived mediators are pivotal to leukocyte and lung cell responses in sepsis and ARDS. Cell Biochem Biophys. 2021;79(3):449–459. doi:10.1007/s12013-021-01012-w
19. Pérez-Torres I, Guarner-Lans V, Soria-Castro E, et al. Alteration in the lipid profile and the desaturases activity in patients with severe pneumonia by SARS-CoV-2. Front Physiol. 2021;12:667024. doi:10.3389/fphys.2021.667024
20. Pizzino G, Irrera N, Cucinotta M, et al. Oxidative stress: harms and benefits for human health. Oxid Med Cell Longev. 2017;2017(1):8416763. doi:10.1155/2017/8416763
21. Zhang H, Slutsky AS, Vincent JL. Oxygen free radicals in ARDS, septic shock and organ dysfunction. Intensive Care Med. 2000;26(4):474–476. doi:10.1007/s001340051185
22. Ayala A, Muñoz MF, Argüelles S. Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev. 2014;2014:360438. doi:10.1155/2014/360438
23. Rogers LK, Cismowski MJ. Oxidative Stress in the Lung - The Essential Paradox. Curr Opin Toxicol. 2018;7:37–43. doi:10.1016/j.cotox.2017.09.001
24. Bezerra FS, Lanzetti M, Nesi RT, et al. Oxidative stress and inflammation in acute and chronic lung injuries. Antioxidants. 2023;12(3):548. doi:10.3390/antiox12030548
25. Erol N, Saglam L, Saglam YS, et al. The protection potential of antioxidant vitamins against acute respiratory distress syndrome: a rat trial. Inflammation. 2019;42(5):1585–1594. doi:10.1007/s10753-019-01020-2
26. Ghorbi M, Rashidi M, Olapour A, et al. Effect of N-Acetylcysteine on the treatment of acute respiratory distress syndrome in mechanically ventilated patients admitted to the intensive care unit. Med J Islam Repub Iran. 2021;35:87. doi:10.47176/mjiri.35.87
27. Tanaka KI, Tamura F, Sugizaki T, et al. Evaluation of lecithinized superoxide dismutase for the prevention of acute respiratory distress syndrome in animal models. Am J Respir Cell Mol Biol. 2017;56(2):179–190. doi:10.1165/rcmb.2016-0158OC
28. Metnitz PG, Bartens C, Fischer M, et al. Antioxidant status in patients with acute respiratory distress syndrome. Intensive Care Med. 1999;25(2):180–185. doi:10.1007/s001340050813
29. Galgani J, Ravussin E. Energy metabolism, fuel selection and body weight regulation. Int J Obes Lond. 2008;32(Suppl 7):S109–19. doi:10.1038/ijo.2008.246
30. Carneiro L, Pellerin L. Nutritional impact on metabolic homeostasis and brain health. Front Neurosci. 2021;15:767405. doi:10.3389/fnins.2021.767405
31. Onopiuk A, Tokarzewicz A, Gorodkiewicz E. Chapter two - cystatin C: a kidney function biomarker. In: Makowski GS, editor. Advances in Clinical Chemistry. Elsevier; 2015:57–69.
32. Forcados GE, Muhammad A, Oladipo OO, et al. Metabolic implications of oxidative stress and inflammatory process in SARS-CoV-2 pathogenesis: therapeutic potential of natural antioxidants. Front Cell Infect Microbiol. 2021;11:654813. doi:10.3389/fcimb.2021.654813
33. Zhu J, Thompson CB. Metabolic regulation of cell growth and proliferation. Nat Rev Mol Cell Biol. 2019;20(7):436–450. doi:10.1038/s41580-019-0123-5
34. Chandel NS. Carbohydrate Metabolism. Cold Spring Harb Perspect Biol. 2021;13(1):a040568. doi:10.1101/cshperspect.a040568
35. Laffey JG, Honan D, Hopkins N, et al. Hypercapnic acidosis attenuates endotoxin-induced acute lung injury. Am J Respir Crit Care Med. 2004;169(1):46–56. doi:10.1164/rccm.200205-394OC
36. Hopkins RO, Suchyta MR, Snow GL, et al. Blood glucose dysregulation and cognitive outcome in ARDS survivors. Brain Inj. 2010;24(12):1478–1484. doi:10.3109/02699052.2010.506861
37. Etoh T, Inoguchi T, Kakimoto M, et al. Increased expression of NAD(P)H oxidase subunits, NOX4 and p22phox, in the kidney of streptozotocin-induced diabetic rats and its reversibity by interventive insulin treatment. Diabetologia. 2003;46(10):1428–1437. doi:10.1007/s00125-003-1205-6
38. Nadeem A, Al-Harbi NO, Ahmad SF, et al. Glucose-6-phosphate dehydrogenase inhibition attenuates acute lung injury through reduction in NADPH oxidase-derived reactive oxygen species. Clin Exp Immunol. 2018;191(3):279–287. doi:10.1111/cei.13097
39. Hartmann B, Verket M, Balfanz P, et al. Glycaemic variability is associated with all-cause mortality in COVID-19 patients with ARDS, a retrospective subcohort study. Sci Rep. 2022;12(1):9862. doi:10.1038/s41598-022-13816-8
40. Finfer S. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–1297.
41. De Backer D, Creteur J, Zhang H, et al. Lactate production by the lungs in acute lung injury. Am J Respir Crit Care Med. 1997;156(4 Pt 1):1099–1104. doi:10.1164/ajrccm.156.4.9701048
42. Robinson MJ, Krasnodembskaya AD. Therapeutic targeting of metabolic alterations in acute respiratory distress syndrome. Eur Respir Rev. 2020;29(156):200114. doi:10.1183/16000617.0114-2020
43. Manosalva C, Quiroga J, Hidalgo AI, et al. Role of lactate in inflammatory processes: friend or foe. Front Immunol. 2021;12:808799. doi:10.3389/fimmu.2021.808799
44. Logette E, Lorin C, Favreau C, et al. A machine-generated view of the role of blood glucose levels in the severity of COVID-19. Front Public Health. 2021;9:695139. doi:10.3389/fpubh.2021.695139
45. Santos AF, Póvoa P, Paixão P, et al. Changes in glycolytic pathway in SARS-COV 2 infection and their importance in understanding the severity of COVID-19. Front Chem. 2021;9:685196. doi:10.3389/fchem.2021.685196
46. Calvier L, Herz J, Hansmann G. Interplay of low-density lipoprotein receptors, LRPs, and lipoproteins in pulmonary hypertension. JACC Basic Transl Sci. 2022;7(2):164–180. doi:10.1016/j.jacbts.2021.09.011
47. Lee BR, Paing MH, Sharma-Walia N. Cyclopentenone prostaglandins: biologically active lipid mediators targeting inflammation. Front Physiol. 2021;12. doi:10.3389/fphys.2021.640374
48. Ricciotti E, FitzGerald GA. Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol. 2011;31(5):986–1000. doi:10.1161/ATVBAHA.110.207449
49. Lessig J, Fuchs B. Plasmalogens in biological systems: their role in oxidative processes in biological membranes, their contribution to pathological processes and aging and plasmalogen analysis. Curr Med Chem. 2009;16(16):2021–2041. doi:10.2174/092986709788682164
50. Dushianthan A, Goss V, Cusack R, et al. Altered molecular specificity of surfactant phosphatidycholine synthesis in patients with acute respiratory distress syndrome. Respir Res. 2014;15(1):128. doi:10.1186/s12931-014-0128-8
51. Ellis SR, Hall E, Panchal M, et al. Mass spectrometry imaging of phosphatidylcholine metabolism in lungs administered with therapeutic surfactants and isotopic tracers. J Lipid Res. 2021;62:100023. doi:10.1016/j.jlr.2021.100023
52. Dushianthan A, Cusack R, Grocott MPW, et al. Abnormal liver phosphatidylcholine synthesis revealed in patients with acute respiratory distress syndrome. J Lipid Res. 2018;59(6):1034–1045. doi:10.1194/jlr.P085050
53. Bonnans C, Levy BD. Lipid mediators as agonists for the resolution of acute lung inflammation and injury. Am J Respir Cell Mol Biol. 2007;36(2):201–205. doi:10.1165/rcmb.2006-0269TR
54. Caironi P, Ichinose F, Liu R, et al. 5-Lipoxygenase deficiency prevents respiratory failure during ventilator-induced lung injury. Am J Respir Crit Care Med. 2005;172(3):334–343. doi:10.1164/rccm.200501-034OC
55. Gust R, Kozlowski J, Stephenson A, et al. Role of cyclooxygenase-2 in oleic acid-induced acute lung injury. Am J Respir Crit Care Med. 1999;160(4):1165–1170. doi:10.1164/ajrccm.160.4.9811073
56. Levy BD, Zhang Q-Y, Bonnans C, et al. The endogenous pro-resolving mediators lipoxin A4 and resolvin E1 preserve organ function in allograft rejection. Prostaglandins Leukot Essent Fatty Acids. 2011;84(1–2):43–50. doi:10.1016/j.plefa.2010.09.002
57. Kumar KV, Rao SM, Gayani R, et al. Oxidant stress and essential fatty acids in patients with risk and established ARDS. Clin Chim Acta. 2000;298(1–2):111–120. doi:10.1016/S0009-8981(00)00264-3
58. Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. doi:10.1038/nature01322
59. Chance B, Sies H, Boveris A. Hydroperoxide metabolism in mammalian organs. Physiol Rev. 1979;59(3):527–605. doi:10.1152/physrev.1979.59.3.527
60. Panov AV, Dikalov SI. Cardiolipin, perhydroxyl radicals, and lipid peroxidation in mitochondrial dysfunctions and aging. Oxid Med Cell Longev. 2020;2020:1323028. doi:10.1155/2020/1323028
61. Garcia-de-Lorenzo y Mateos A, Montejo González JC, Quintana Diaz M. Eicosanoid synthesis and respiratory distress syndrome in intensive medicine. In: Rajendram R, Preedy VR, Patel VB, editors. Diet and Nutrition in Critical Care. New York, NY: Springer; 2015:63–74.
62. Wei Z, Liu X, Cheng C, et al. Metabolism of amino acids in cancer. Front Cell Dev Biol. 2020;8:603837. doi:10.3389/fcell.2020.603837
63. Nair KS, Short KR. Hormonal and signaling role of branched-chain amino acids. J Nutr. 2005;135(6):1547S–1552S. doi:10.1093/jn/135.6.1547S
64. Tomé D. Amino acid metabolism and signalling pathways: potential targets in the control of infection and immunity. Nut Diabetes. 2021;11(1):20. doi:10.1038/s41387-021-00164-1
65. Ye Z, Wang S, Zhang C, et al. Coordinated modulation of energy metabolism and inflammation by branched-chain amino acids and fatty acids. Front Endocrinol. 2020;11. doi:10.3389/fendo.2020.00617
66. Bala CG, Rusu A, Ciobanu D, Bucsa C, Roman G. Amino acid signature of oxidative stress in patients with Type 2 diabetes: targeted exploratory metabolomic research. Antioxidants. 2021;10(4):610.
67. Dushianthan A, Cusack R, Burgess VA, et al. Immunonutrition for adults with ARDS: results from a Cochrane systematic review and meta-analysis. Respiratory Care. 2020;65(1):99–110. doi:10.4187/respcare.06965
68. Reizine F, Lesouhaitier M, Gregoire M, et al. SARS-CoV-2-Induced ARDS associates with MDSC expansion, lymphocyte dysfunction, and arginine shortage. J Clin Immunol. 2021;41(3):515–525. doi:10.1007/s10875-020-00920-5
69. Cruzat V, Macedo Rogero M, Noel Keane K, Curi R, Newsholme P. Glutamine: metabolism and immune function. Supplementation Clin Transl Nutrients. 2018;10(11):1564.
70. Hou YC, Pai M-H, Chiu W-C, et al. Effects of dietary glutamine supplementation on lung injury induced by lipopolysaccharide administration. Am J Physiol Lung Cell Mol Physiol. 2009;296(3):L288–95. doi:10.1152/ajplung.90479.2008
71. Fernandez-Bustamante A, Agazio A, Wilson P, et al. Brief glutamine pretreatment increases alveolar macrophage CD163/Heme Oxygenase-1/p38-MAPK dephosphorylation pathway and decreases capillary damage but not neutrophil recruitment in IL-1/LPS-insufflated rats. PLoS One. 2015;10(7):e0130764. doi:10.1371/journal.pone.0130764
72. de Oliveira GP, Kitoko JZ, de Souza Lima-Gomes P, et al. Glutamine therapy reduces inflammation and extracellular trap release in experimental acute respiratory distress syndrome of pulmonary origin. Nutrients. 2019;11(4):831. doi:10.3390/nu11040831
73. Elms S, Chen F, Wang Y, et al. Insights into the arginine paradox: evidence against the importance of subcellular location of arginase and eNOS. Am J Physiol Heart Circ Physiol. 2013;305(5):H651–66. doi:10.1152/ajpheart.00755.2012
74. Honzawa N, Fujimoto K, Kobayashi M, et al. Protein kinase C (Pkc)-δ mediates arginine-induced glucagon secretion in pancreatic α-Cells. Int J Mol Sci. 2022;23(7):4003. doi:10.3390/ijms23074003
75. Kellner M, Noonepalle S, Lu Q, et al. ROS signaling in the pathogenesis of Acute Lung Injury (ALI) and Acute Respiratory Distress Syndrome (ARDS). Adv Exp Med Biol. 2017;967:105–137. doi:10.1007/978-3-319-63245-2_8
76. Fiorentino G, Coppola A, Izzo R, et al. Corrigendum to “Effects of adding L-arginine orally to standard therapy in patients with COVID-19: a randomized, double-blind, placebo-controlled, parallel-group trial. Results of the first interim analysis”. EClinicalMedicine. 2022;51:101636. doi:10.1016/j.eclinm.2022.101636
77. Chiu LC, Tang HY, Fan CM, et al. Kynurenine pathway of tryptophan metabolism is associated with hospital mortality in patients with acute respiratory distress syndrome: a prospective cohort study. Antioxidants. 2022;11(10):1884.
78. Chen J, Xue X, Cai J, et al. Protective effect of taurine on sepsis‑induced lung injury via inhibiting the p38/MAPK signaling pathway. Mol Med Rep. 2021;24(3). doi:10.3892/mmr.2021.12292
79. van Eijk LE, Offringa AK, Bernal ME, Bourgonje AR, van Goor H, Hillebrands JL. The disease-modifying role of taurine and its therapeutic potential in coronavirus disease 2019 (COVID-19). Adv Exp Med Biol. 2022;1370:3–21.
80. Ryter SW. Significance of heme and heme degradation in the pathogenesis of acute lung and inflammatory disorders. Int J Mol Sci. 2021;22(11):5509. doi:10.3390/ijms22115509
81. Pedley AM, Benkovic SJ. A new view into the regulation of purine metabolism: the purinosome. Trends Biochem Sci. 2017;42(2):141–154. doi:10.1016/j.tibs.2016.09.009
82. Evans CR, Karnovsky A, Kovach MA, et al. Untargeted LC-MS metabolomics of bronchoalveolar lavage fluid differentiates acute respiratory distress syndrome from health. J Proteome Res. 2014;13(2):640–649. doi:10.1021/pr4007624
83. Elshafey M, Mossalam AMA, Makharita MY, et al. Prognostic role of serum uric acid in acute respiratory distress syndrome patients: a preliminary study. Egypt J Chest Dis Tuberculosis. 2015;64(1):197–202. doi:10.1016/j.ejcdt.2014.11.007
84. Lee HW, Choi SM, Lee J, et al. Serum uric acid level as a prognostic marker in patients with acute respiratory distress syndrome. J Intensive Care Med. 2019;34(5):404–410. doi:10.1177/0885066617698911
85. Bartziokas K, Papaioannou AI, Loukides S, et al. Serum uric acid as a predictor of mortality and future exacerbations of COPD. Eur Respir J. 2014;43(1):43–53. doi:10.1183/09031936.00209212
86. Ruggiero C, Cherubini A, Miller E, et al. Usefulness of uric acid to predict changes in C-reactive protein and interleukin-6 in 3-year period in Italians aged 21 to 98 years. Am J Cardiol. 2007;100(1):115–121. doi:10.1016/j.amjcard.2007.02.065
87. Liaudet L, Mabley JG, Pacher P, et al. Inosine exerts a broad range of antiinflammatory effects in a murine model of acute lung injury. Ann Surg. 2002;235(4):568–578. doi:10.1097/00000658-200204000-00016
88. Puneet P, Moochhala S, Bhatia M. Chemokines in acute respiratory distress syndrome. Am J Physiol Lung Cell Mol Physiol. 2005;288(1):L3–15. doi:10.1152/ajplung.00405.2003
89. D’Alessio FR, Craig JM, Singer BD, et al. Enhanced resolution of experimental ARDS through IL-4-mediated lung macrophage reprogramming. Am J Physiol Lung Cell Mol Physiol. 2016;310(8):L733–46. doi:10.1152/ajplung.00419.2015
90. Coates CJ, Decker H. Immunological properties of oxygen-transport proteins: hemoglobin, hemocyanin and hemerythrin. Cell Mol Life Sci. 2017;74(2):293–317. doi:10.1007/s00018-016-2326-7
91. Nagasawa R, Hara Y, Murohashi K, et al. Serum heme oxygenase-1 measurement is useful for evaluating disease activity and outcomes in patients with acute respiratory distress syndrome and acute exacerbation of interstitial lung disease. BMC Pulm Med. 2020;20(1):310. doi:10.1186/s12890-020-01341-1
92. Mumby S, Upton RL, Chen Y, et al. Lung heme oxygenase-1 is elevated in acute respiratory distress syndrome. Crit Care Med. 2004;32(5):1130–1135. doi:10.1097/01.CCM.0000124869.86399.F2
93. Fredenburgh LE, Perrella MA, Barragan-Bradford D, et al. A Phase I trial of low-dose inhaled carbon monoxide in sepsis-induced ARDS. JCI Insight. 2018;3(23). doi:10.1172/jci.insight.124039
94. Artigas A, Camprubí-Rimblas M, Tantinyà N, et al. Inhalation therapies in acute respiratory distress syndrome. Ann Transl Med. 2017;5(14):293. doi:10.21037/atm.2017.07.21
95. Yan Y, Chen J, Liang Q, et al. Metabolomics profile in acute respiratory distress syndrome by nuclear magnetic resonance spectroscopy in patients with community-acquired pneumonia. Respir Res. 2022;23(1):172. doi:10.1186/s12931-022-02075-w
96. Umbrello M, Marini JJ, Formenti P. Metabolic support in acute respiratory distress syndrome: a narrative review. J Clin Med. 2023;12(9):3216. doi:10.3390/jcm12093216
97. Tsaknis G, Siempos II, Kopterides P, et al. Metformin attenuates ventilator-induced lung injury. Crit Care. 2012;16(4):R134. doi:10.1186/cc11439
98. Qiu M, Ding -L-L, Zhan Z-L, et al. Use of SGLT2 inhibitors and occurrence of noninfectious respiratory disorders: a meta-analysis of large randomized trials of SGLT2 inhibitors. Endocrine. 2021;73(1):31–36. doi:10.1007/s12020-021-02644-x
99. Anzueto A, Jubran A, Ohar JA, et al. Effects of aerosolized surfactant in patients with stable chronic bronchitis: a prospective randomized controlled trial. JAMA. 1997;278(17):1426–1431. doi:10.1001/jama.1997.03550170056032
100. Yasmin F, Zeeshan MH, Ullah I. The role of fenofibrate in the treatment of COVID-19. Ann Med Surg Lond. 2022;74:102974. doi:10.1016/j.amsu.2021.102974
101. Chirinos JA, Lopez-Jaramillo P, Giamarellos-Bourboulis EJ, et al. A randomized clinical trial of lipid metabolism modulation with fenofibrate for acute coronavirus disease 2019. Nat Metab. 2022;4(12):1847–1857. doi:10.1038/s42255-022-00698-3
102. Garrido-Mesa N, Zarzuelo A, Gálvez J. What is behind the non-antibiotic properties of minocycline? Pharmacol Res. 2013;67(1):18–30. doi:10.1016/j.phrs.2012.10.006
103. Fuoco D. Classification framework and chemical biology of tetracycline-structure-based drugs. Antibiotics. 2012;1(1):1–13. doi:10.3390/antibiotics1010001
104. Wilderman A, Guo Y, Taylor S, et al. cAMP/PKA-mediated regulation of amino acid metabolism in murine T-lymphoma cells (1095.16). FASEB J. 2014;28(S1):
105. Pérez-Pérez D, Santos-Argumedo L, Rodríguez-Alba JC, et al. Role of protein kinase a activation in the immune system with an emphasis on lipopolysaccharide-responsive and beige-like anchor protein in B cells. Int J Mol Sci. 2023;24(4):3098. doi:10.3390/ijms24043098
106. Jo YS, Choi SM, Lee J, et al. Effect of preadmission metformin use on clinical outcome of acute respiratory distress syndrome among critically III patients with diabetes. Tuberc Respir Dis. 2017;80(3):296–303. doi:10.4046/trd.2017.80.3.296
107. Jeong HE, Park S, Noh Y, et al. Association of adverse respiratory events with sodium-glucose cotransporter 2 inhibitors versus dipeptidyl peptidase 4 inhibitors among patients with type 2 diabetes in South Korea: a nationwide cohort study. BMC Med. 2023;21(1):47. doi:10.1186/s12916-023-02765-2
108. Agudelo CW, Samaha G, Garcia-Arcos I. Alveolar lipids in pulmonary disease. A review. Lipids Health Dis. 2020;19(1):122.
109. Hoyt JC, Ballering J, Numanami H, et al. Doxycycline modulates nitric oxide production in murine lung epithelial cells. J Immunol. 2006;176(1):567–572. doi:10.4049/jimmunol.176.1.567
110. Roy SK, Kendrick D, Sadowitz BD, et al. Jack of all trades: pleiotropy and the application of chemically modified tetracycline-3 in sepsis and the acute respiratory distress syndrome (ARDS). Pharmacol Res. 2011;64(6):580–589. doi:10.1016/j.phrs.2011.06.012
111. Herath SC, Normansell R, Maisey S, et al. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2018;10(10):Cd009764. doi:10.1002/14651858.CD009764.pub3
112. Maisi P, Kiili M, Raulo SM, et al. MMP inhibition by chemically modified tetracycline-3 (CMT-3) in equine pulmonary epithelial lining fluid. Ann N Y Acad Sci. 1999;878(1):675–677. doi:10.1111/j.1749-6632.1999.tb07759.x
113. Garrido-Mesa J, Adams K, Galvez J, et al. Repurposing tetracyclines for acute respiratory distress syndrome (ARDS) and severe COVID-19: a critical discussion of recent publications. Expert Opin Investig Drugs. 2022;31(5):475–482. doi:10.1080/13543784.2022.2054325
114. Sharma SK, Bhatt P, Asdaq SMB, et al. Combined therapy with ivermectin and doxycycline can effectively alleviate the cytokine storm of COVID-19 infection amid vaccination drive: a narrative review. J Infect Public Health. 2022;15(5):566–572. doi:10.1016/j.jiph.2022.03.014
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathophysiology of Cerebral Microbleeds in Patients with Severe Respiratory Failure and Acute Respiratory Distress Syndrome: A Scoping Review
Ziaka M, Zagalioti SC, Zgouridou A, Fyntanidou B, Exadaktylos A
International Journal of General Medicine 2026, 19:575001
Published Date: 10 February 2026