")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mentoring for Black and Minoritized Allied Health Professionals in Health and Social Care: A Scoping Review
Authors Atwal A , Sriram V , McKay EA
Received 1 April 2023
Accepted for publication 30 June 2023
Published 9 August 2023 Volume 2023:16 Pages 2251—2259
DOI https://doi.org/10.2147/JMDH.S413085
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anita Atwal,1 Vimal Sriram,2,3 Elizabeth A McKay4
1London South Banking University, School of Allied and Community Health, London, UK; 2University Hospitals Bristol and Weston NHS Foundation Trust, Bristol, UK; 3Collaborative Learning and Capacity Building Theme, NIHR Applied Research Collaboration in Northwest London, London, UK; 4Edinburgh Napier University, School of Health and Social Care, Edinburgh, UK
Correspondence: Anita Atwal, Tel +44 20 7974403011, Email [email protected]
Introduction: Diversity, equality and belonging are important aspects within Allied Health Professional (AHP) groups. Mentoring is considered as a solution to improve career progression. To date, there is no consensus on what good mentoring looks like and whether current models are fit for purpose for Black and Minoritised Ethnicity AHPs.
Methods: Scoping review to understand mentoring among Black and Minoritised Ethnicity (BME) AHPs through searches in four electronic databases using pre-defined criteria.
Results: From 1440 studies screened, 2 studies were included in this review that researched mentoring for BME AHPs in a health and/or social care setting. Themes that emerged from the literature were related to access and amount of mentoring for BME AHPs, psychosocial mentoring may influence cross-race mentorship outcomes and organisational issues related to workforce pressures and management support. There is uncertainty around the importance of same race relationships in mentoring but there is some evidence that within cross-race mentoring this could influence outcomes.
Conclusion: It is unknown if mentoring enables career success in BME AHPs. There is emerging evidence on the importance of psychosocial mentoring within cross-race relationships. Careful reflection and further research is needed on how current mentoring models work and ensure fair access to mentorship and support for BME AHPs.
Keywords: mentoring, ethnic minority, career progression, allied health, psychosocial
Background
Allied Health Professionals (AHPs) are an important part of the health and care service system. Within the United Kingdom (UK) the Health and Care Professionals Council (HCPC) regulates Allied Health Professionals from 14 different professional groups.1 There were 252,269 AHPs in the HCPC register in March 2023.2 Where ethnicity of the registrants is known, AHPs from black, asian and minoritised ethnicities make up 7.2% of total number of registrants. In the United Kingdom, there is a recognition for the need for the AHPs workforce to be more proactive to tackle racial inequality.3 The Allied Health Professions Strategy recognises the need for positive action to examine current recruitment and career progression strategies.4 There is a growing awareness of the disparity of AHPs career progression outcomes between white and BME therapists.5 Black and Minoritized Ethnic therapists are underrepresented within higher leadership roles with white applicants significantly more likely than BME applicants to be appointed from shortlisting.6 A more diverse AHP workforce leads to better quality of care for patients, wider talent pool and improves productivity and innovation.7 A rapid review that explored how AHPs can support disadvantaged groups and reduce inequalities found that access to the AHPs health services, unequal workforce distribution and lack of inclusive clinical guidelines were key issues.8 For the purposes of this review, we have taken into consideration the Law Society statement on race and ethnicity,
Race is a categorisation that is based mainly on physical attributes or traits, assigning people to a specific race simply by having similar appearances or skin colour. It’s now widely accepted that race is a social construct. However, having been racialised and shared common experiences of racism, racial identity is important to many and can be a basis for collective organising and support for racially minoritised individuals.9
Career advancement is important within health and social care to retain and recruit the AHP workforce. It is thought to have a positive impact on how a person engages with an organisation and their commitment to their own role.10 Mentorship is one tool used to achieve personal goals and/or career-related outcomes.11 Whilst no consistent definition of mentoring is used across studies,12 mentorship is reported to have two distinct functions. (1) Career related that includes sponsorship, promoting exposure and visibility, coaching, protecting 2. Psychosocial/personal development such as role modelling, friendship, and counselling.13 Mentorship is different from supervision in that the mentee is not required to formally report to the mentor and competences are not assessed and/or measured.14 The positive outcomes attributed to mentoring are dependent on the quality of the mentoring process and the mentees experience. Mentees that report experiences of lower-quality mentoring report higher intentions to leave their jobs compared to those who have a more positive experience of mentoring.15 Mentoring success is related to the quality of the relationship between the mentor and mentee that are dynamic in nature.13 Thus, matching of the mentor and the mentee, is an important part of the mentoring process.
To ensure that all AHPs can advance in their careers and achieve personal goals, it is essential that there is fair and equitable access to programmes. Demographic similarity has been found to play a greater role for mentors than that for mentees.16 Thomas17 suggests that same race relationships provided more psychosocial support than cross-race relationships. Richard et al18 suggest that mentoring quality is the most crucial factor to mediate the effect of racial dissimilarity and liking your mentee played a limited role in the mentorship process.16 Access to sponsorship opportunities was viewed as more important than demographics19 since the outcome of mentorship for the mentee can be influenced by the status and sponsorship of the mentor.20 Power equity was also viewed as important.21
There is evidence to suggest that age may be an important factor in impacting on access to a mentorship programme. In higher education environments older employees experienced less career mentoring, had shorter relationships and were closer in age to their mentor and reported more mutual learning than younger persons experiencing mentorship. Younger persons reported experiencing more mentorship from younger persons as their age increased.22
What we do know is that the experiences of BME AHPs are different from white colleagues in that many experience and continue to experience racism.5,23 Hence, the need to create an environment where people from different backgrounds can work in an environment that is safe, compassionate and inclusive.3 What is unknown is how surface characteristics such as race has on the outcome of the mentoring process.24,25 As part of creating an inclusive environment, we need to understand the effect of mentorship on career outcomes for BME AHPs. To address this, we conducted a scoping review to scope the literature on mentoring and career progression for BME AHPs working in health and social care settings.
Method
The scoping review used the methodological framework by Arksey and O’Malley.26 This suggests five stages of conducting a scoping review (1) identifying the research question (2) Identifying relevant studies (3) Study selection (4) Charting the data and (5) Collating, summarizing, and reporting the results. We decided on a scoping review as the review question was exploratory, needed to have a wider scope and be more inclusive of wider literature due to the concern about the type and amount of literature available within the 14 AHPs groups, and more importantly it enabled us to analyse knowledge gaps.27 The aim of a scoping reviews is not to critically appraise and synthesise evidence for the review question but to provide an overview of the evidence.27,28 In this scoping review, we used the Joanna Briggs Institute (JBI) general guidance for a scoping review28 and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-ScR) extension for scoping reviews.29
The aim of this review was to explore the existing literature on mentoring and career progression for BME AHPs working in health and social care settings. We did a preliminary search of MEDLINE, the Cochrane Database of Systematic Reviews and JBI Evidence Synthesis at the start of this scoping review in March 2022 and there were no existing or planned systematic reviews or scoping reviews on this topic.
Ethical permission was not needed for this scoping review but was obtained for later phases of the research project.
Inclusion/Exclusion Criteria
Mentorship
There is no definition of mentoring from a BME perspective, and there is no standardised definition for mentorship in the literature.30 Concept analysis of mentoring in nursing31 defines the attributes as role model, nurturing, friendship, experienced person, regular meeting, and endurance.
For this scoping review we defined mentorship as
A one-to-one learning relationship designed to support you with the quality of your thinking, decision-making and growth, facilitated by purposeful interaction with a mentor.32
We excluded studies that focussed only on management and leadership styles and not on mentoring for career progression for AHPs.
Types of Participants
Research articles on mentorship that involved one or more of the 14 AHP professions (Drama therapists, music therapists, podiatrists, dieticians, occupational therapists, operating department practitioners, orthoptists, osteopaths, paramedics, physiotherapists, prosthetics and orthotists, radiographers and speech and language therapists) who identified as BME and occurred within health or social care organisations were included. We excluded participants who had access to mentoring if they occurred exclusively with students in practice, research, post graduate students and if it was not within health and social care workplace settings. Studies that included health and care professionals were included as long as they had at least one of the AHP professionals and data could be separated out for AHPs.
Types of Studies
To answer the review question, both quantitative and qualitative study designs were included. The full-text article or report of the study needed to be available (ie abstracts alone were excluded) and had to have been peer-reviewed. Letters to the editor, abstract and conference proceedings, and book reviews were not included. Study protocols and theses/dissertations were also excluded. To make this review as inclusive as possible, we included studies published in any language.
Search Strategy
To capture the concept of BME mentoring, we searched social media and Google Scholar to explore general index terms related to ethnicity and mentorship. This allowed us to explore general index terms and become familiar with terminology. We consulted an experienced information specialist and developed a comprehensive search strategy for electronic citation databases. For this scoping review, we searched in CINAHL (1980-January 2023), MEDLINE, EBSCO (1960 – January 2023), PscycINFO, EBSCOHost (1980-January 2023) and Web of Science Core Collection (1980-January 2023) databases.
We spent time thinking carefully about how to find studies related to ethnicity and ensured that we used varied terms. In addition, the reference list of all included sources of evidence was screened for additional studies. During the initial search strategy phase, it became evident that terminology on race and ethnicity has changed over time, and this is reflected in terms used in the included articles in this review, which may be regarded as culturally insensitive.
Our search strategy utilised index terms, where appropriate and free-text terms to capture the following concepts: (1) mentorship, mentee, business, organisations and expanded on terms related to the 14 Professions that make up the Allied Health Professions. We also translated these professions into international workforce terminology. We utilised terminology related to ethnicity as suggested by the Law Society in the UK9, UK Government writing about ethnicity,33 Bhopal34 (2004) and the United States Census.35 The search strategy and terms used are included in Appendix 1.
Screening and Data Extraction
Following the search, all identified citations were collated and uploaded into Covidence (https://www.covidence.org/) and duplicates removed. Titles and abstracts were screened by three reviewers of the research team (AA, ST, and EAM) against the inclusion/exclusion criteria for the review, any disagreements were resolved by mutual discussion with the fourth reviewer (VS). Potentially relevant sources of research from reference lists of screened articles were retrieved in full and assessed against the inclusion and exclusion criteria by two reviewers (AA and VS) and disagreements resolved by discussion with the third reviewer (EAM).
Results
The search was conducted between June 2022–February 2023. One thousand four hundred and forty articles from the search were imported into Covidence and a check for duplicate records was conducted electronically through Covidence. From the records retrieved from the database search 355 were removed as duplicates. AA and ST independently screened the titles and abstracts of the remaining records. An additional 55 records were removed at this stage based on inclusion and exclusion criteria. The remaining 1030 records were independently assessed for inclusion based on full texts, with an additional 1028 articles excluded. Two papers met the inclusion criteria (Table 1) and were included in this review.
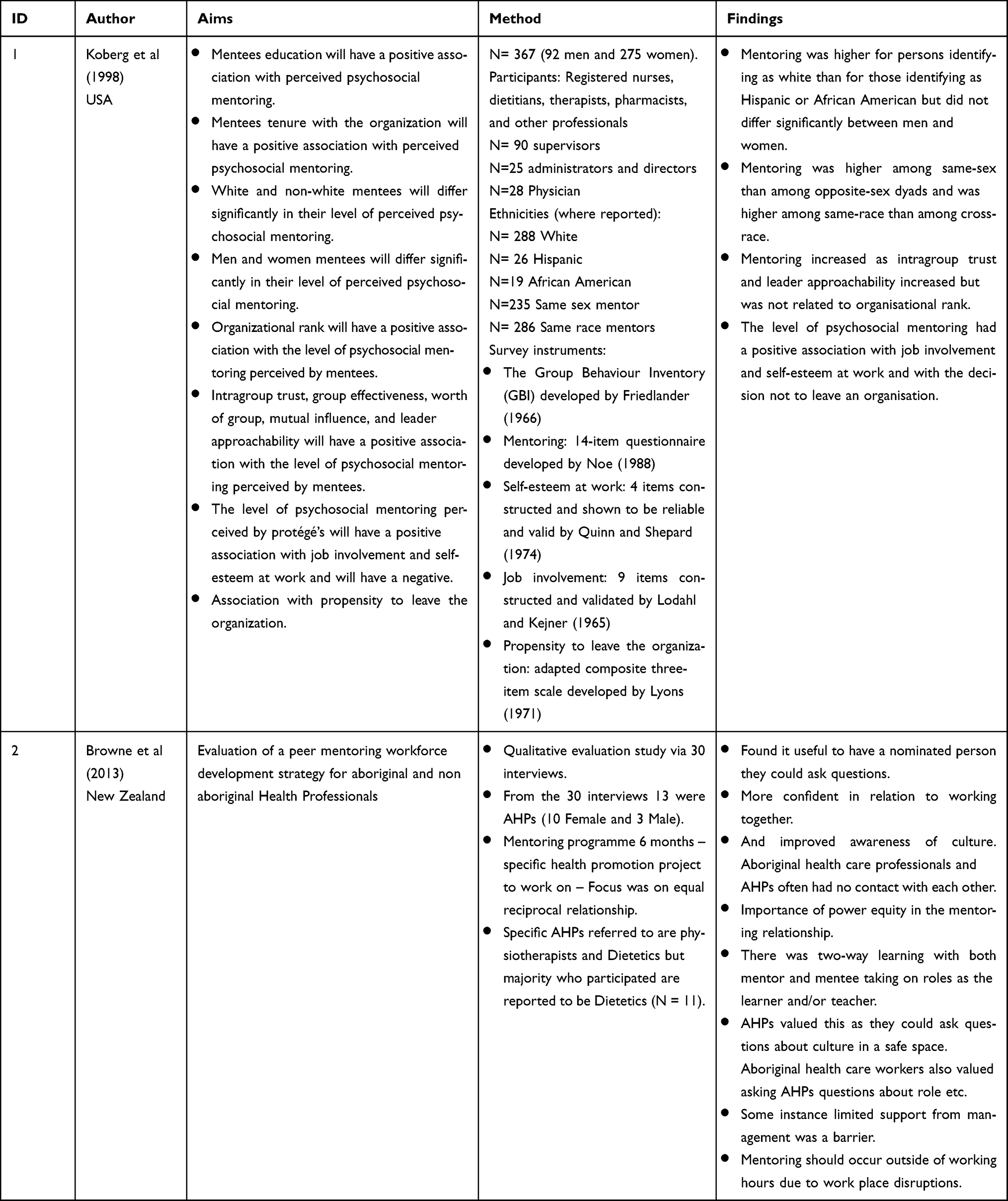 |
Table 1 Characteristics of Included Studies |
Reasons for exclusion of the full-text papers were documented and are listed separately along with a PRISMA flow diagram (Figure 1).
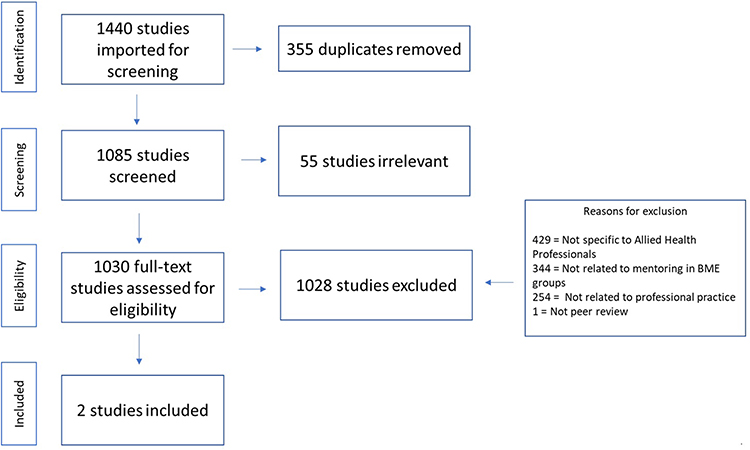 |
Figure 1 Prisma Flowchart of included studies. Note: Adapted from Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850.29 |
For the included studies, we undertook a conceptual content analysis as we wanted to understand the occurrence of terms, we were interested in. These were race, career, mentoring, health care and organisations. As we were coding, we added additional codes for gender and social status where this was reported. The research team discussed how concepts that are related but different should be coded. We then took the concepts of interest to conduct a relationship analysis which meant that we coded for signs of a relationship between career progression, mentorship, and race.
Two studies included BME Allied Health Professionals and other personnel within a hospital setting (Koberg et al 1998, Browne et al 2013) in the USA and New Zealand, respectively. It should be noted that specific data is not given by Koeberg et al36 to carefully refer to which AHPs were from a minority background and that white participants outnumbered Hispanic (N = 26) and/or African American (N = 19). In contrast, 288 were white. Browne et al21 compared Aboriginal and non-Aboriginal Health Professionals. Both Koberg et al and Browne et al make specific reference to professionals from dietetics. Koberg et al describe the traditional one to one mentoring model whilst Browne et al describe peer mentoring.
Access and Amount of Mentoring
Mentoring was higher for professionals who identified as white than for Hispanic or African American but did not differ significantly between men and women. Mentoring was higher among same gender than among opposite gender dyads and was higher among same-race than among cross-race. Browne et al additionally state that, cross-race mentoring could also be a mechanism to increase confidence in relation to working together and improved awareness of culture and Race issues for AHPs and psychosocial mentorship may be important in cross-race mentoring.
Mentoring Outcome
Mentoring increased as intragroup trust and leader approachability increased but was not related to organizational rank. Cross-race mentoring increased confidence in relation to working together and improved awareness of culture. There was an acknowledgement of the importance of power equity within mentoring relationships. The level of psychosocial mentoring had a positive association with job involvement and self-esteem at work and with the decision not to leave an organization. Our review found that the level of psychosocial mentoring had a positive association with job involvement and self-esteem at work and with retention. The amount of mentoring increased as trust and leader approachability increased.
Organisational Issues and Mentorship
In some instance limited support from management was a barrier and the suggestion that mentoring should occur outside of working hours due to workplace disruptions.
Discussion
This scoping review highlights the lack of sufficient literature with a focus on mentoring for Black and other minoritised ethnic AHPs. We will discuss our findings from the two included studies within the broader literature involving other professional groups as there could be likely cross-over. Mentoring research involving BME persons has occurred in US organisations such as telecommunications,37 insurance companies,16 public utility companies,17 and a combination of different organisations.18 One study occurred in a laboratory,38 whilst some studies focusing on master’s in business administration graduates employed in various companies.17,18,39,40
The studies included in this review described different types of mentorships, and it is important that AHPs are aware of the different types and their potential use within professional practice. Koberg et al describe the traditional one to one model which involves a mentor (usually more experienced and senior). This is different from reverse mentoring when the mentor is more junior than the mentee and/or has less experience and/or status and often provides a new perspective.41 In contrast, Browne et al describe peer mentoring but unlike one to one mentoring all the participants were health care professionals and both parties mutually benefited from the mentoring experience.
Social exchange theory suggests that a successful mentorship relationship occurs when the mentoring relationships have positive outcomes and/or gains for both the mentor and mentee.42 Social capital is an important outcome of mentoring in relation to whether mentoring is worth the investment for example, does mentoring create value in response to the investment?43 Mentorship as a mechanism to facilitate career advancement have been found to have positive outcomes on career advancements.11 (Eby et al 2008). To date, we do not know whether mentoring does facilitate career success in AHPs from BME backgrounds. The findings from this scoping review emphasise the need for AHPs to determine the value of mentoring on career progression.
Social networks and connections are important components of social capital. Our scoping review adds new understanding to the importance of social networks within the mentoring process in cross-race relationships.44 It has been suggested that if a person has the same demographic characteristics and is perceived to be similar then this can result in stronger identification and make persons more at ease.24 Ensher et al45 suggests that attitudinal similarity was more important than demographic/characteristic similarity. Our review highlighted the need for trust in mentoring relationships. There is need for mentoring programmes to determine and/or put in place trust activities that can promote trust between mentor and mentee. Mentors trust in a mentee is influenced by their initial perceptions of the mentee’s ability, integrity and munificence.46 We need further research to explore how trust is established in AHP mentorship, and mentoring programs must include activities that assist in establishing and fostering trust between mentor and the mentee. Psychosocial support is viewed as important to enable the mentee to achieve career goals and may consist of strategies such as role modelling, coaching and friendship.47 This is an important finding since most AHPs are reporting issues related to burn out and retention of staff.48 Our findings from this scoping review and the wider literature suggest that if mentoring is to be seen as delivering social capital and return on investment, then AHPs and organisations need to review how mentors and mentees are matched. Our scoping review found that mentees reported more mentoring by mentors of the same gender.36 Richard et al18 suggest that mentoring quality is the most crucial factor to mediate the effect of race differences and in the wider literature Randel et al19 examine career advancement through sponsorship of African Americans within cross-race relationships. Women have reported greater barriers, such as lack of culture, fit and being excluded from informal networks and greater importance of having a good track record and developing relationships to facilitate advancement than did men.49
It has been suggested that demographics are not as important as ensuring that the mentor is able to ensure that the mentee has access to potential opportunities. Mentorship has better outcomes when both the mentor and mentee agreed their strategy to manage their cross-race relationship.37,38 Mentees reported higher levels of mentoring from same race rather than from cross-race mentors.36 Likewise, within peer mentorship relationships21 it is perceived that peer mentorship was effective since non Aboriginal and Aboriginal health professionals and AHPs were more confident working together as they often had no direct contact. This was achieved by developing rapport and understanding.
Suggested areas to explore in BME AHP mentoring for career progression:
Bainbridge50 concluded that there was insufficient evidence to prescribe a best practice model for mentorship. Deng et al51 developed general evidence-based guidance for matching mentor and mentees, which we believe can be apgplied through the following steps for BME AHPs. (1) Ask mentor and mentee input about the match, and review match based on feedback, (2) Understand the development needs mentees have then find the mentor with the relevant knowledge, skills, and experience, (3) Ask both mentor and mentee about preferences for being matched on surface-level characteristics and (4) Assess mentor and mentees’ deep-level characteristics using psychometric measures.
Based on current evidence from the wider literature, we encourage consideration of the following for cross-race mentorship for AHPs. (1) Need to ensure that mentee has fair access to mentorship opportunities. (2) Need to ensure that if cross-race relationships are formed and agreed then both mentor and mentee need to agree on strategy to manage any issues that may arise. (3) Need to reflect on both race and gender when matching mentor and mentee. (4) Need to reflect carefully on the role of psychosocial factors within cross-race relationships and (5) Trust activities are important to strengthen the mentor/mentee relationship.
Limitations of This Review
A limitation of this review is the fact that there is very little peer-reviewed literature on mentoring and career progression for BME AHPs. The two studies included in this review are from the US and New Zealand and transfer of the findings within other healthcare contexts needs to be accounted for. There are likely to be concerns about some of the terminology used, even if outdated, which may cause harm in ongoing research in this area. There is also an absence of research that has specifically evaluated mentorship with BME AHPs looking at different subgroup of ethnicities. This review only included two studies, it does highlight that this is an important topic area that needs further research. This review has shown the need for more research in this area to ensure fairness and equity to reflect the diversity of the population and the AHP workforce.
Conclusion
There are considerable gaps in our knowledge and understanding of mentoring for career advancement for BME AHPs. To date, this absence of research and any associated action may be hindering career advancement. It is uncertain whether current mentoring opportunities meet the needs of BME AHPs. There is a need to understand the needs of specific minority groups and to ascertain how mentoring programmes should operate. There is a need to explore further cross-race relationships and how they are managed within the mentoring process.
Strengths and Limitation of Study
This is the first review exploring mentoring in the context of BME Allied Health Professionals. Due to the paucity of research in this area, meaningful conclusions cannot be made from existing literature, but we have identified areas for future research enquiry.
Funding
This study was funded by the Elizabeth Casson Trust.
Disclosure
Dr Vimal Sriram is a paid employee of NIHR Applied Research Collaboration. The author declares that this article presents independent research supported by the National Institute for Health Research (NIHR) under the Applied Health Research (ARC) programme for Northwest London. The views expressed in this publication are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health. The authors report no other conflicts of interest in this work.
References
1. NHS England and NHS Improvement. The 14 allied health professions; 2023. Available from: https://www.england.nhs.uk/ahp/role/.
2. Health and Care Professions Council. Registrant snapshot; 2023. Available from: https://www.hcpc-uk.org/resources/data/2023/registrant-snapshot-march-2023/.
3. NHS England and NHS Improvement. NHS people plan; 2021. Available from: https://www.england.nhs.uk/ournhspeople/.
4. NHS England and NHS Improvement. The Allied Health Professions (AHPs) strategy for England – aHPs deliver; 2022. Available from: https://www.england.nhs.uk/wp-content/uploads/2022/06/allied-health-professions-strategy-for-england-ahps-deliver.pdf.
5. Atwal A, Sriram V, McKay EA, Bame OT. Making a difference: belonging, diversity and inclusion in occupational therapy. Br J Occup Ther. 2019;1(1):1–2. doi:10.1177/03080226211031797
6. NHS England and NHS Improvement. NHS workforce race equality standard; 2022. Available from: https://www.england.nhs.uk/about/equality/equality-hub/workforce-equality-data-standards/equality-standard/.
7. Hemmings N, Buckingham H, Oung C, Palmer B. Attracting, Supporting and Retaining a Diverse NHS Workforce. London: Nuffield Trust; 2021.
8. Gkiouleka A, Aquino MRJ, Ojo-Aromokudu O, et al. Allied health professionals: a promising ally in the work against health inequalities- A rapid review. Public Heal Pract. 2022;3:100269. doi:10.1016/J.PUHIP.2022.100269
9. The Law Society. A guide to race and ethnicity terminology and language; 2022. Available from: https://www.lawsociety.org.uk/topics/ethnic-minority-lawyers/a-guide-to-race-and-ethnicity-terminology-and-language.
10. Jia-jun Z, Hua-ming S. The impact of career growth on knowledge-based employee engagement: the mediating role of affective commitment and the moderating role of perceived organizational support. Front Psychol. 2022;13:945. doi:10.3389/FPSYG.2022.805208/BIBTEX
11. Eby LT, Durley JR, Evans SC, Ragins BR. Mentors’ perceptions of negative mentoring experiences: scale development and nomological validation. J Appl Psychol. 2008;93(2):358–373. doi:10.1037/0021-9010.93.2.358
12. Doyle NW, Gafni Lachter L, Jacobs K. Scoping review of mentoring research in the occupational therapy literature, 2002–2018. Aust Occup Ther J. 2019;66(5):541–551. doi:10.1111/1440-1630.12579
13. Baird L, Kram K. Career dynamics: managing the superior/subordinate relationship. Organ Dyn. 1983;11(4):46–64. doi:10.1016/0090-2616(83)90038-4
14. Schoen SA, Gee BM, Ochsenbein M. Preparing advanced clinicians and practitioners: a model for mentorship in occupational therapy practice. Occup Ther Int. 2021;2021:1–6. doi:10.1155/2021/3394478
15. Ragins BR, Cotton JL. Mentor functions and outcomes: a comparison of men and women in formal and informal mentoring relationships. J Appl Psychol. 1999;84(4):529–550. doi:10.1037/0021-9010.84.4.529
16. Lankau MJ, Riordan CM, Thomas CH. The effects of similarity and liking in formal relationships between mentors and protégés. J Vocat Behav. 2005;67(2):252–265. doi:10.1016/J.JVB.2004.08.012
17. Thomas DA. The impact of race on managers’ experiences of developmental relationships (mentoring and sponsorship): an intra-organizational study. J Organ Behav. 1990;11(6):479–492. doi:10.1002/JOB.4030110608
18. Richard OC, McKay PF, Garg S, Pustovit S. The impact of supervisor–subordinate racial-ethnic and gender dissimilarity on mentoring quality and turnover intentions: do positive affectivity and communal culture matter? Int J Hum Resour Manag. 2017;30(22):3138–3165. doi:10.1080/09585192.2017.1344288
19. Randel AE, Galvin BM, Gibson CB, Batts SI. Increasing career advancement opportunities through sponsorship: an identity-based model with illustrative application to cross-race mentorship of African Americans. Gr Organ Manag. 2021;46(1):105–142. doi:10.1177/1059601120978003/ASSET/IMAGES/LARGE/10.1177_1059601120978003-FIG1.JPEG
20. Schemm RL, Bross T. Mentorship experiences in a group of occupational therapy leaders. Am J Occup Ther. 1995;49(1):32–37. doi:10.5014/AJOT.49.1.32
21. Browne J, Thorpe S, Tunny N, Adams K, Palermo C. A qualitative evaluation of a mentoring program for Aboriginal health workers and allied health professionals. Aust N Z J Public Health. 2013;37(5):457–462. doi:10.1111/1753-6405.12118
22. Finkelstein LM, Allen TD, Rhoton LA. An examination of the role of age in mentoring relationships. Gr Organ Manag. 2003;28(2):249–281. doi:10.1177/1059601103028002004
23. Beagan BL, Sibbald KR, Bizzeth SR, Pride TM. Systemic racism in Canadian occupational therapy: a qualitative study with therapists. Can J Occup Ther. 2022;89(1):51–61. doi:10.1177/00084174211066676
24. Ragins BR. Diversified mentoring relationships in organizations: a power perspective. Acad Manag Rev. 1997;22(2):482. doi:10.2307/259331
25. Wanberg CR, Welsh ET, Hezlett SA. Mentoring research: a review and dynamic process model. Res Pers Hum Resour Manag. 2003;22:39–124. doi:10.1016/S0742-7301(03)22002-8/FULL/XML
26. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
27. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):1–7. doi:10.1186/S12874-018-0611-X/TABLES/1
28. Peters MDJ, Godfrey C, McInerney P, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth. 2022;20(4):953–968. doi:10.11124/JBIES-21-00242
29. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
30. Geraci SA, Thigpen SC. A review of mentoring in academic medicine. Am J Med Sci. 2017;353(2):151–157. doi:10.1016/j.amjms.2016.12.002
31. Olaolorunpo O. Mentoring in nursing: a concept analysis correspondence. Int J Caring Sci. 2019;12(1):142.
32. National Institute for Health Research. What is mentoring?; 2022. Available from: https://www.nihr.ac.uk/documents/before-embarking-on-a-mentoring-relationship/27682.
33. UK Government. Ethnicity facts and figures; 2022. Available from: https://www.ethnicity-facts-figures.service.gov.uk/.
34. Bhopal R. Glossary of terms relating to ethnicity and race: for reflection and debate. J Epidemiol Community Heal. 2004;58(6):441–445. doi:10.1136/JECH.2003.013466
35. US Census Bureau. 2020 census results; 2020. Available from: https://www.census.gov/programs-surveys/decennial-census/decade/2020/2020-census-results.html.
36. Koberg CS, Boss RW, Goodman E. Factors and outcomes associated with mentoring among health-care professionals. J Vocat Behav. 1998;53(1):58–72. doi:10.1006/JVBE.1997.1607
37. Thomas DA. Racial dynamics in cross-race developmental relationships. Adm Sci Q. 1993;38(2):169. doi:10.2307/2393410
38. Leitner JB, Ayduk Ö, Boykin CM, Mendoza-Denton R. Reducing negative affect and increasing rapport improve interracial mentorship outcomes. PLoS One. 2018;13(4):e0194123. doi:10.1371/JOURNAL.PONE.0194123
39. Dreher GF, Cox TH. Race, gender, and opportunity: a study of compensation attainment and the establishment of mentoring relationships. J Appl Psychol. 1996;81(3):297–308. doi:10.1037/0021-9010.81.3.297
40. Blake-Beard SD. The costs of living as an outsider within: an analysis of the mentoring relationships and career success of Black and White women in the corporate sector. J Career Dev. 1999;26(1):21–36. doi:10.1177/089484539902600103/ASSET/089484539902600103.FP.PNG_V03
41. Zauchner-Studnicka S. A model for reverse-mentoring in education. World Acad Sci Eng Technol Int J Soc Behav Educ Econ Bus Ind Eng. 2017; 2017:1.
42. Chaudhuri S, Ghosh R. Reverse mentoring: a social exchange tool for keeping the boomers engaged and millennials committed. Hum Resour Dev Rev. 2011;11(1):55–76. doi:10.1177/1534484311417562
43. Adler PS, Kwon S-W. Social capital: prospects for a new concept. Acad Manag Rev. 2002;27(1):17. doi:10.2307/4134367
44. Hezlett SA, Gibson SK. Linking mentoring and social capital: implications for career and organization development. Adv Dev Hum Resour. 2016;9(3):384–411. doi:10.1177/1523422307304102
45. Ensher EA, Grant-Vallone EJ, Marelich WD. Effects of perceived attitudinal and demographic similarity on protégés’ support and satisfaction gained from their mentoring relationships. J Appl Soc Psychol. 2002;32(7):1407–1430. doi:10.1111/J.1559-1816.2002.TB01444.X
46. Mayer RC, Davis JH, Schoorman FD. An integrative model of organizational trust. Acad Manag Rev. 1995;20(3):709. doi:10.2307/258792
47. Pethrick H, Nowell L, Oddone Paolucci E, et al. Psychosocial and career outcomes of peer mentorship in medical resident education: a systematic review protocol. Syst Rev. 2017;6(1):1–8. doi:10.1186/S13643-017-0571-Y/TABLES/2
48. House of Commons Health and Social Care Committee. Workforce burnout and resilience in the nhs and social care second report of session 2021–22. London; 2021. Available from: www.parliament.uk/hsccom.
49. Lyness KS, Thompson DE. Climbing the corporate ladder: do female and male executives follow the same route? J Appl Psychol. 2000;85(1):86–101. doi:10.1037/0021-9010.85.1.86
50. Bainbridge R, Tsey K, McCalman J, Towle S. The quantity, quality and characteristics of Aboriginal and Torres Strait Islander Australian mentoring literature: a systematic review. BMC Public Health. 2014;14(1):1–25. doi:10.1186/1471-2458-14-1263/FIGURES/4
51. Deng C, Gulseren DB, Turner N. How to match mentors and protégés for successful mentorship programs: a review of the evidence and recommendations for practitioners. Leadersh Organ Dev J. 2022;43(3):386–403. doi:10.1108/LODJ-01-2021-0032/FULL/XML
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.