Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Mental Health and Sleep Quality of Healthcare Providers After Partial Relief of COVID-19 in Saudi Arabia: A Cross-Sectional Study
Authors Al Harbi MK, Alsabani MH, Olayan LH, Alrifai D, Alobaid SA, Althanyyan AF, Alsahli NM, Alsubaie WS, Alotaibi WM, Alosaimi SD
Received 29 November 2022
Accepted for publication 18 January 2023
Published 24 January 2023 Volume 2023:16 Pages 209—217
DOI https://doi.org/10.2147/JMDH.S399546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohammed K Al Harbi,1– 3 Mohmad H Alsabani,2,4 Lafi H Olayan,2,4 Derar Alrifai,1,2 Shaden A Alobaid,4 Alhanouf F Althanyyan,4 Najla M Alsahli,4 Wejdan S Alsubaie,4 Wafa M Alotaibi,4 Sarah D Alosaimi4
1Department of Anesthesia, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 2King Abdullah International Medical Research Centre, Riyadh, Saudi Arabia; 3King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 4Anesthesia Technology Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia
Correspondence: Mohammed K Al Harbi, Department of Anesthesia, Ministry of National Guard Health Affairs, PO Box 22490, Riyadh, 11426, Saudi Arabia, Tel +966 011 8011111 Ext 19431, Email [email protected]
Purpose: We aimed to assess sleep quality and psychological distress among healthcare workers (HCWs) in the context of mitigated governmental restrictions during COVID-19 pandemic in Saudi Arabia.
Methods: This cross-sectional study included 370 HCWs from a single tertiary healthcare institution in Riyadh, Saudi Arabia. Sleep quality and psychological distress were measured using the Pittsburgh Sleep Quality Index (PSQI) and the Depression, Anxiety and Stress Scale – 21 (DASS-21).
Results: The median stress score for HCWs aged between 20 and 29 years was higher compared to HCWs aged between 30 and 39 years (p=0.002) and HCWs aged between 50 and 59 years (p< 0.001). The median anxiety score of the age group between 20 and 29 years was also significantly higher compared to the age groups between 40 and 49 and 50– 59 years (all p< 0.05). HCWs living with family showed higher anxiety and depression scores compared to those living with non-family members (p=0.006 and p=0.005, respectively). Handling COVID-19 patients on multiple occasions during routine patient care was significantly associated with higher anxiety and depression scores among HCWs. The results also showed higher PSQI scores among younger HCWs (20– 29 years) and trainees (all p< 0.05). In addition, PSQI correlate significantly with depression (r=0.268) and anxiety (r=0.278) scores of DASS-21 scale (all p< 0.001).
Conclusion: Poor psychological well-being and sleep quality were observed among certain groups of HCWs, even after the mitigation of COVID-19 restrictions. This study highlights the need for strategies to manage HCWs at risk of developing psychological distress during future catastrophes.
Keywords: the Depression Anxiety and Stress Scale-21, Pittsburgh Sleep Quality Index, psychological distress, sleep quality, post-lockdown period, COVID-19
Introduction
In recent years, coronavirus disease (COVID-19) has affected nearly all segments of the population and has developed into a worldwide pandemic since December 2019. The pandemic has had substantial disturbances to global health of the general population but was particularly detrimental to frontline healthcare workers (HCWs).1 The profound effects of the containment measures of the pandemic – namely quarantine and social distancing – have led to negative consequences on the psychological well-being and mental health of HCWs.2 The pandemic could not only generate fear, anxiety, and depression but may also contributed to prolonged effects such as panic and trauma-related disorders.3
Exposure to workplace hazards such as COVID-19 has been demonstrated to negatively impact the mental health of HCWs.4 Studies on the burden of COVID-19 on mental health of HCWs have accumulated over years. In China, the prevalence of psychological and sleep disturbances such as anxiety, depression, and insomnia were high (~35–50%) among the general population and HCWs during the pandemic.5–7 Symptomatic anxiety due to COVID-19 was reported in a multinational survey-based study, with approximately 30% of the HCWs reported that they experienced physical symptoms due to anxiety.8 High rates of psychological disturbances among HCWs and general population due to COVID-19 have been also reported in France,9 the United States,10 Turkey,11 India,12 Italy,13 the United Kingdom,14 Germany,15 and Australia.16 In Saudi Arabia, poor psychological well-being has been found among HCWs, with the prevalence of anxiety, depression and stress was approximately 17–27% during the pandemic.17 Factors that predispose HCWs to psychological distress have been extensively studied in the current literature. Several of previous worldwide studies suggested that younger age, pre-existing psychological difficulties, and chronic conditions are at risk of developing psychological distress during the pandemic. In addition, governmental restriction to economic and social activities, including social distancing, can impose a substantial risk for developing psychological distress.18,19 Moreover, economic crisis is another critical factor that predisposes individuals to psychological morbidities and even suicide attempts.20
Documenting the progression of psychological morbidities during and after the pandemic is of particular importance to ensure optimal responses in similar future situations. The impact of the lifting of lockdown measures on the mental health status was previously studied among the general population admitted to psychiatric emergency department in Switzerland.21 The authors reported an increase in serious psychiatric conditions such as suicidal behaviour and psychomotor agitation after the lockdown has been lifted. Still, little is known about the impact of partial relief of COVID-19 restrictions on psychological status and sleep quality of HCWs in Saudi Arabia. Therefore, we aimed in the current observational cross-sectional study to measure sleep quality and the levels of stress, anxiety, and depression experienced by a sample HCWs during the partial relief of strict economic and social restriction of the COVID-19 pandemic in Saudi Arabia.
Materials and Methods
Study Design and Participants
This was a cross-sectional study conducted at a tertiary hospital in Riyadh, Saudi Arabia. The recruitment was conducted after partial relief of COVID-19 restrictions in the country. All HCWs including physicians, medical residents, interns, nurses, and allied healthcare practitioners who worked during the COVID-19 pandemic were included in the study. Other HCWs who were working in administrative positions were excluded from the study.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki. The study was conducted in King Abdulaziz Medical City after obtaining the Institutional Review Board (IRB) approval (SP21R/215/05). All participants were informed about study and provided informed consent. No personally identifiable information was collected to maintain participants confidentiality.
Sample and Data Collection
The sample size was calculated using Raosoft online sample size calculator. The minimum required sample size was 366, with a margin of error 5%, 95% confidence level and 50% response distribution. HCWs were recruited by a non-probability convenience sampling technique, where participants were invited to participate through a web-link sent to their phones via Airdrop or WhatsApp. Consent to participate was provided electronically to those who agreed to participate.
Instruments
The survey was constructed using Google Forms. The study’s survey had three sections: sociodemographic variables, and two validated questionnaires from previous studies to measure mental health and sleep quality. The first section included sociodemographic variables of participants including gender, age, job title, housing status, marital status, and frequency of contact with COVID-19 patients. In the second section, mental health of HCWs was measured using the Depression Anxiety Stress Scale-21 (DASS-21) to determine the extent of psychological impact of COVID-19.22 The DASS-21 is a well-established instrument and has been applied in research related to COVID-19.23,24 The DASS-21 scale is a valid and reliable tool with reliabilities for the sub-scale’s depression (Cronbach’s alpha =.91), stress (Cronbach’s alpha = 0.89), and anxiety (Cronbach’s alpha = 0.85).25 It consists of 21 Likert-scale items to assess three major sub-scales including depression, stress, and anxiety. Each sub-scale consisted of 7 Likert-scale items ranging from 0 (Did not apply to me at all) to 3 (Applied to me very much or most of the time). The total score of each sub-scale is measured by adding together the score of each item and multiplying it by 2.
In the last section, sleep quality of HCWs was measured using the Pittsburgh Sleep Quality Index (PSQI) to evaluate the extent of sleep disturbance among HCWs.26 The PSQI is a valid and reliable self-reported questionnaire to evaluate sleep quality over a one-month time interval. The diagnostic sensitivity and specificity of the instrument is 89.6% and 86.5%, respectively.27 It has been applied previously in COVID-related research and among HCWs.28 It consists of 19 self-rated questions and 5 questions rated by the bedpartner or roommate.
Statistical Analysis
Descriptive statistics were calculated to compare DASS-21 components and PSQI scores according to sociodemographic variables. Categorical data were presented as frequency and percentages, while continuous variables were presented as median and interquartile range (IQR). Mann–Whitney U and Kruskal–Wallis H-test tests were used to assess the association of sociodemographic variables with anxiety, depression, and stress scores from DASS-21 and PSQI score. Post hoc test (Bonferroni test) was used to test differences among more than three groups. The Spearman correlation analysis was used to assess correlation between stress, anxiety, depression and PSQI scores. A p value (two-tailed) of <0.05 was considered significant. Statistical analysis was performed on IBM SPSS v28.
Results
A total of 370 HCWs completed the survey. The sociodemographic characteristics of the surveyed HCWs are shown in Table 1. Most of the participants were female gender (70.8%) and 29.2% were male. The majority of participants were between the age of 20 to 29 (61.9%) and only (1.1%) of respondents were older than 60 years. More than half of the sample were single (63.5%) and 36.5% were married. Regarding the housing status, 17.3% participants lived alone, 10.3% lived with others, and 72.4% lived with family. Among the enrolled subjects, 30.3% were applied health practitioner, 26.8% nurses, 24.3% trainees and 18.6% physicians. Only 22.2% of the enrolled subjects reported that they did not had contact with COVID-19 patients, whereas the majority (37%) had contacted COVID patients once a week and 25.4%, 22.2% participants had no contact with infected cases, 37% had contact once a week, 25.4% responded 2–3 times a week, and 15.4% answered more than three times a week.
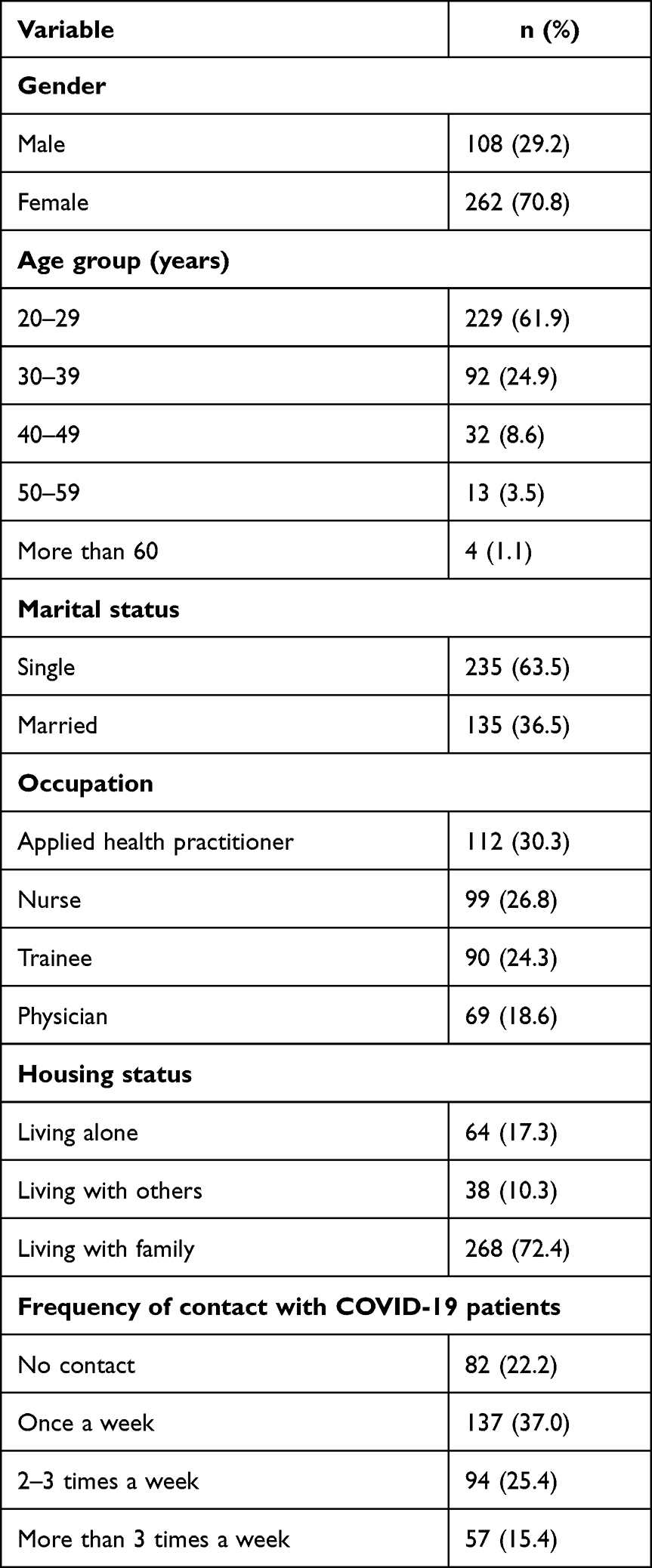 |
Table 1 Sociodemographic Characteristics |
Table 2 categorises DASS-21 parameters by sociodemographic variables. The five categories of age groups had significantly different scores on anxiety (p=0.006) and stress (p<0.001). Pairwise post hoc comparison showed that the stress scores for the age group between 20 and 29 years to be the highest [median (IQR): 3.00 (5.00)] compared to age group of 50–59 years [1.00 (2.00); p<0.001], age group of 30–39 years [1.00 (3.00); p=0.002] and age group of 40–49 years [1.00 (3.00); p=0.024]. Pairwise post hoc comparison also showed that the anxiety scores of the age group between 20 and 29 years [5.00 (7.00)] is significantly higher compared to the age groups between 40 and 49 years [1.50 (6.50); p=0.005] and 50–59 years [0.00 (4.00); p=0.007].
 |
Table 2 Association of Sociodemographic Variables with Anxiety, Depression, and Stress Scores from DASS-21 |
Furthermore, there were significant differences on anxiety (p=0.02) and depression (p=0.013) scores between the three categories of housing status (Table 2). Pairwise post hoc test showed that those living with family displayed higher anxiety scores compared to those living with others [5.00 (6.00) vs 2.00 (7.00); p=0.006]. Similarly, those living with family displayed higher depression scores compared to those living with others [4.00 (8.00) vs 1.00 (6.50); p=0.005]. In addition, median depression score was significantly higher among those living alone compared to median score of those living with others [4.50 (9.00) vs 1.00 (6.50); p=0.007].
Our analyses also showed significantly different anxiety and depression scores with frequency of contact with COVID-19 patients (all p<0.001; Table 2). Further analyses from pairwise post hoc test showed that those who had contact with COVID patients once a week had lower median anxiety score [3.00 (6.00)] compared to those who were exposed to COVID patient for 2–3 times a week [6.00 (7.00); p<0.001] and to those who were exposed to COVID-19 for more than 3 times per week [5.00 (9.00); p=0.010]. Similarly, we observed lower median depression score among those who had single contact with COVID patients compared to those who had multiple contacts. Nevertheless, we did not observe any significant differences on all DASS-21 parameters with gender, marital status, and profession.
Table 3 demonstrates the relationship between sociodemographic variables and PSQI score. Our analysis showed significant differences between age groups and profession on PSQI score. Upon further analyses using pairwise post hoc test, we observed that trainees had slightly higher median PSQI score [10.00 (3.50)] compared to all other professions including allied health professions [9.00 (5.00); p=0.003], nurses [9.00 (5.50); p=0.020] and physicians [9.00 (4.00); p=0.015]. We also observed that older age group (between 50 and 59 years) had slightly lower PSQI score [9.00 (5.50)] compared to younger age groups [from 20 to 29 years: 10.00 (4.00); p<0.001] and [from 30 to 39 years: 10.00 (6.00); p=0.002].
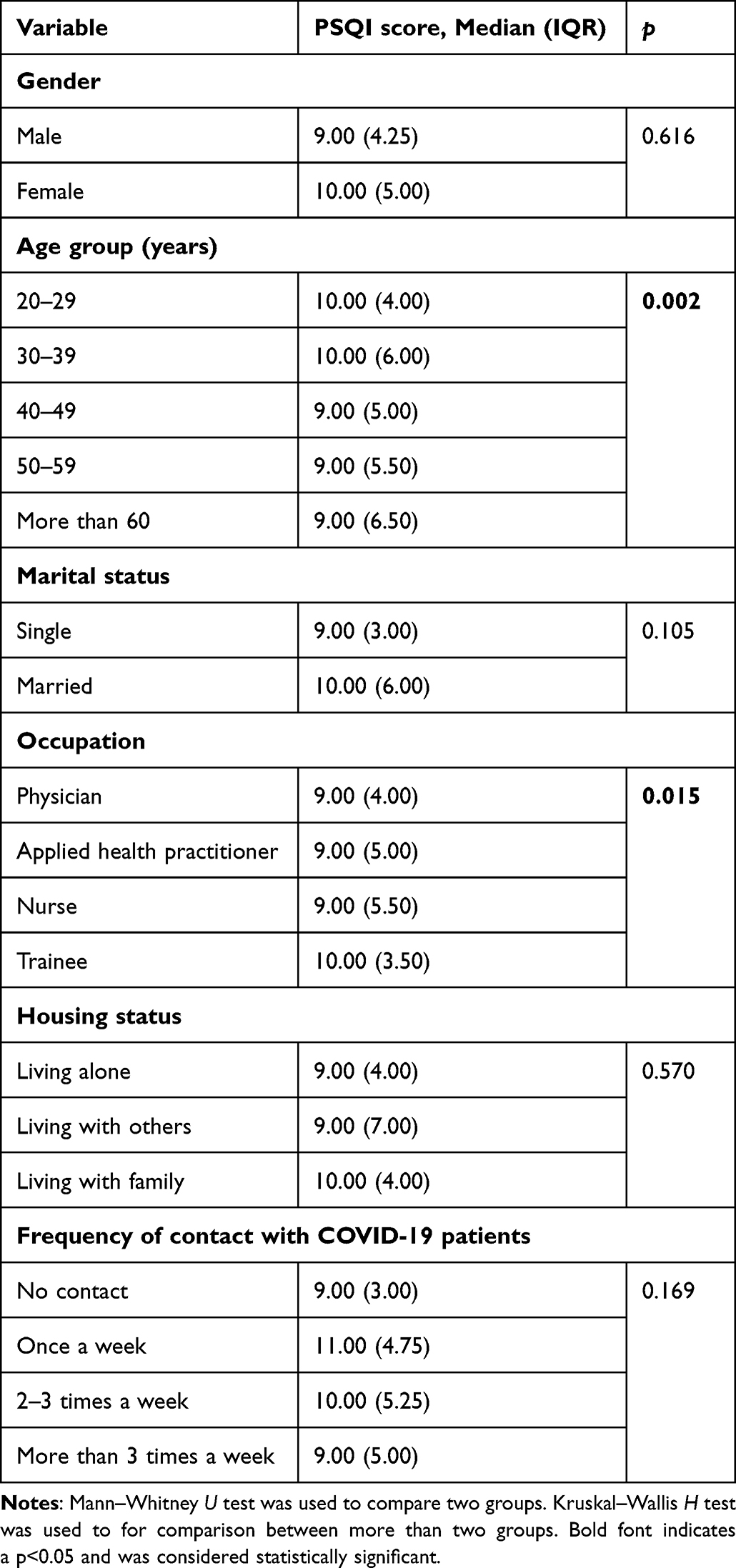 |
Table 3 Association Between Sociodemographic Variables and PSQI Scores |
Table 4 describes Spearman’s rank correlation analysis between anxiety, depression, stress, and sleep disturbance scores. The DASS-21 stress scale was positively associated with the DASS-21 depression scale (r = 0.137; p < 0.01) and the DASS-21 anxiety scale (r = 0.154; p < 0.01). In addition, the depression DASS-21 scale was positively and strongly associated with the DASS-21 anxiety scale (r = 0.814; p < 0.001), and the PSQI score (r = 0.268; p < 0.001). The PSQI score was positively associated with the DASS-21 anxiety scale (r = 0.278; p < 0.001). There was no significant correlation between the DASS-21 stress score and PSQI score.
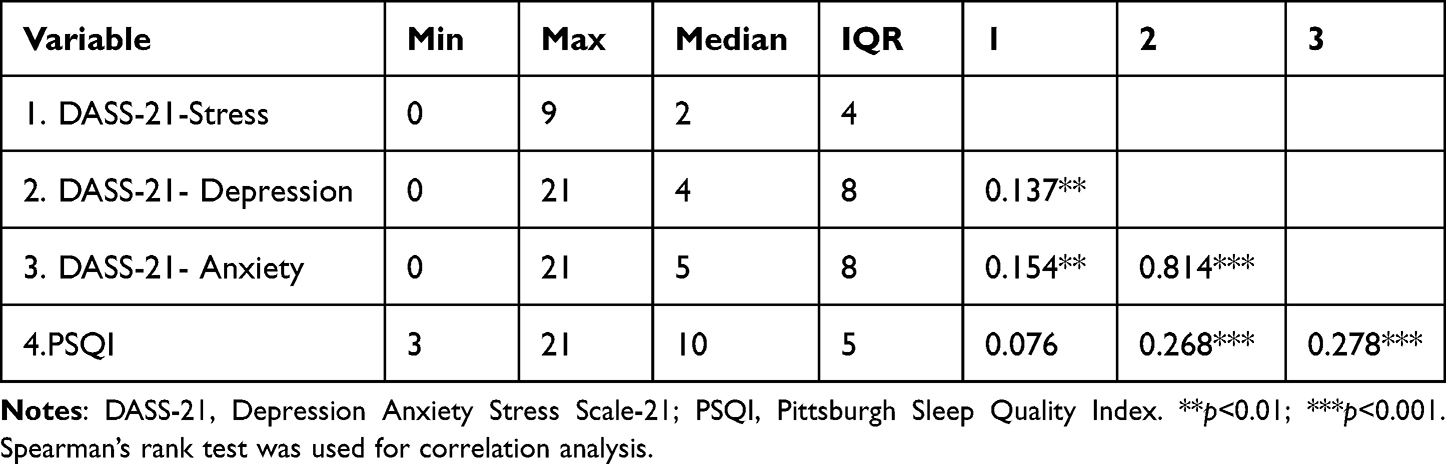 |
Table 4 Correlation Analysis of DASS-21 Parameters Scores and PSQI |
Discussion
To the best of our knowledge, this is the first study to explore mental health and sleep quality among HCWs in the context of the COVID-19 pandemic and the partial relief of governmental restrictions in Saudi Arabia. The key findings of our study are that younger HCWs and those living with family tend to have higher levels of anxiety and stress scores. Furthermore, providing care for COVID-19 patient of more than once per week was associated with higher anxiety and depression scores. We also observed poor sleep quality among younger HCWs and trainees. Lastly, our correlation analysis showed positive and significant correlation between all DASS-21 parameters and PSQI with anxiety and depression scores.
There was a clear age-related relationship in anxiety and stress parameters of DASS-21 scale. These findings are important and highlight the need for more attention toward specific age groups, particularly younger personnel. This is, perhaps, noteworthy in the context of mitigated governmental restrictions because younger adults are at minimal risk of developing serious illness due to COVID-19 compared to older people. However, a previous analysis of COVID-19-related fears revealed that young subjects reported an increase in fear of dying and fear of getting sick when compared to adult and elderly subjects.29 Another probable justification for these findings includes fear from returning to lockdown and/or strict governmental restrictions, although lockdown on freedom of movement was eased during the study period. In addition, older people may have a context of resilience and adaptive mental health, with previous evidence suggesting that emotional well-being improves with age.30,31 Nevertheless, the association between age and mental health persisted during the acute full lockdown phase of the pandemic,17,32,33 and during the easing of strict governmental restrictions as demonstrated by our findings.
Besides age, our results indicate that HCWs providing care to COVID-19 patients more than once weekly had poorer mental health. In addition, the relationship status in our study showed that HCWs residing with family or alone reported higher depression scores than HCWs residing with non-family members. Possible explanations to these results include fear from infection and subsequent transmission of infection to family members.34 In support of our findings, Czepiel et al reported that psychological distress, depressive and post-traumatic stress symptoms were associated with fears from infection among HCW.35 Furthermore, a previous case-report of COVID-19-related concerns in HCWs has documented depressive and anxious symptoms in an HCW after spreading the infection to a family member.36
Previous national and international studies have shown that poor sleep quality is common among HCW during the COVID-19 outbreak, which was also linked to the development of psychological distress. Our results showed that younger age and trainees had slightly increased sleep disturbance compared to older age and other healthcare professionals, respectively. Moreover, we demonstrated that sleep quality index positively correlates with depression and stress parameters. These findings, nevertheless, are unexpected during the mitigation phase, but they concur with previous findings published during the acute phase of the pandemic where full governmental restrictions were imposed.37–40 However, it is possible that stress and depression are among the major contributing factors to sleep disturbance among respondents in the current study. This is evident by correlation between PSQI with depression and anxiety parameters.
This study has some limitations. This was an observational cross-sectional study; therefore, the analyses cannot be used to draw a final causal relationship about the effects of partial relief of COVID-19 restrictions on mental health and sleep quality. In addition, findings from the current study should be interpreted with caution since the study was conducted in a single institution in Saudi Arabia; therefore, these findings may not be generalisable to other settings or countries. Furthermore, respondents were not asked about their current psychological well-being and sleep quality status, which may play a substantial role in the mental health of HCWs.
Conclusion
The observations described in this study suggested that the psychological burden of the pandemic persists after the easing of governmental restrictions. HCWs at risk of psychological distress were likely to be younger, living with family, or in frequent contact with COVID-19 patients. It is therefore substantial for healthcare institutions to intervene and support mental health of vulnerable HCWs.
Acknowledgments
The authors thank all respondents involved in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sim MR. The COVID-19 pandemic: major risks to healthcare and other workers on the front line. BMJ Publishing Group. 2020;77:281–282.
2. Fiorillo A, Gorwood P. The consequences of the COVID-19 pandemic on mental health and implications for clinical practice. Eur Psychiatry. 2020;63:1. doi:10.1192/j.eurpsy.2019.3
3. Généreux M, Schluter PJ, Hung KK, et al. One virus, four continents, eight countries: an interdisciplinary and international study on the psychosocial impacts of the COVID-19 pandemic among adults. Int J Environ Res Public Health. 2020;17(22):8390. doi:10.3390/ijerph17228390
4. Shreffler J, Petrey J, Huecker M. The impact of COVID-19 on healthcare worker wellness: a scoping review. West J Emerg Med. 2020;21(5):1059. doi:10.5811/westjem.2020.7.48684
5. Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: implications and policy recommendations. General Psychiatry. 2020;33:2. doi:10.1136/gpsych-2020-100213
6. Cai Q, Feng H, Huang J, et al. The mental health of frontline and non-frontline medical workers during the coronavirus disease 2019 (COVID-19) outbreak in China: a case-control study. J Affect Disord. 2020;275:210–215. doi:10.1016/j.jad.2020.06.031
7. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
8. Chew NW, Lee GK, Tan BY, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020;88:559–565. doi:10.1016/j.bbi.2020.04.049
9. Fournier A, Laurent A, Lheureux F, et al. Impact of the COVID-19 pandemic on the mental health of professionals in 77 hospitals in France. PLoS One. 2022;17(2):e0263666. doi:10.1371/journal.pone.0263666
10. Pearman A, Hughes ML, Smith EL, Neupert SD. Mental health challenges of United States healthcare professionals during COVID-19. Front Psychol. 2020;11:2065. doi:10.3389/fpsyg.2020.02065
11. Uz B, Savaşan E, Soğancı D. Anxiety, depression and burnout levels of Turkish healthcare workers at the end of the first period of COVID-19 pandemic in Turkey. Clin Psychopharmacol Neurosci. 2022;20(1):97. doi:10.9758/cpn.2022.20.1.97
12. Menon GR, Yadav J, Aggarwal S, et al. Psychological distress and burnout among healthcare worker during COVID-19 pandemic in India—A cross-sectional study. PLoS One. 2022;17(3):e0264956. doi:10.1371/journal.pone.0264956
13. Di Tella M, Romeo A, Benfante A, Castelli L. Mental health of healthcare workers during the COVID‐19 pandemic in Italy. J Eval Clin Pract. 2020;26(6):1583–1587. doi:10.1111/jep.13444
14. Lamb D, Gnanapragasam S, Greenberg N, et al. Psychosocial impact of the COVID-19 pandemic on 4378 UK healthcare workers and ancillary staff: initial baseline data from a cohort study collected during the first wave of the pandemic. Occup Environ Med. 2021;78(11):801–808. doi:10.1136/oemed-2020-107276
15. Bäuerle A, Steinbach J, Schweda A, et al. Mental health burden of the COVID-19 outbreak in Germany: predictors of mental health impairment. J Prim Care Community Health. 2020;11:2150132720953682. doi:10.1177/2150132720953682
16. Smallwood N, Karimi L, Bismark M, et al. High levels of psychosocial distress among Australian frontline healthcare workers during the COVID-19 pandemic: a cross-sectional survey. General Psychiatry. 2021;34:5. doi:10.1136/gpsych-2021-100577
17. Sultan S, Bashar A, Nomani I, et al. Impact of COVID-19 pandemic on psychological health of a sample of the health care workers in the western region of Kingdom of Saudi Arabia. Middle East Curr Psyc. 2022;29(1):1–11. doi:10.1186/s43045-022-00174-4
18. Aknin LB, Andretti B, Goldszmidt R, et al. Policy stringency and mental health during the COVID-19 pandemic: a longitudinal analysis of data from 15 countries. Lancet Public Health. 2022;7(5):e417–e426. doi:10.1016/S2468-2667(22)00060-3
19. Fiorenzato E, Zabberoni S, Costa A, Cona G. Cognitive and mental health changes and their vulnerability factors related to COVID-19 lockdown in Italy. PLoS One. 2021;16(1):e0246204. doi:10.1371/journal.pone.0246204
20. Costanza A, Amerio A, Aguglia A, et al. From “the interpersonal theory of suicide” to “the interpersonal trust”: an unexpected and effective resource to mitigate economic crisis-related suicide risk in times of covid-19? Acta Bio Medica. 2021;92(Suppl):
21. Ambrosetti J, Macheret L, Folliet A, et al. Psychiatric emergency admissions during and after COVID-19 lockdown: short-term impact and long-term implications on mental health. BMC Psychiatry. 2021;21(1):1–8. doi:10.1186/s12888-021-03469-8
22. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the beck depression and anxiety inventories. Behav Res Ther. 1995;33(3):335–343. doi:10.1016/0005-7967(94)00075-U
23. Lenzo V, Quattropani MC, Sardella A, Martino G, Bonanno GA. Depression, anxiety, and stress among healthcare workers during the COVID-19 outbreak and relationships with expressive flexibility and context sensitivity. Front Psychol. 2021;12:623033. doi:10.3389/fpsyg.2021.623033
24. Gündoğmuş İ, Ünsal C, Bolu A, et al. The comparison of anxiety, depression and stress symptoms levels of healthcare workers between the first and second COVID-19 peaks. Psychiatry Res. 2021;301:113976. doi:10.1016/j.psychres.2021.113976
25. Beard C, Björgvinsson T. Beyond generalized anxiety disorder: psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. J Anxiety Disord. 2014;28(6):547–552. doi:10.1016/j.janxdis.2014.06.002
26. Buysse DJ, Reynolds III CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
27. Buysse DJ, Hall ML, Strollo PJ, et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med. 2008;4(6):563–571. doi:10.5664/jcsm.27351
28. Jahrami H, BaHammam AS, AlGahtani H, et al. The examination of sleep quality for frontline healthcare workers during the outbreak of COVID-19. Sleep Breath. 2021;25(1):503–511. doi:10.1007/s11325-020-02135-9
29. Costanza A, Macheret L, Folliet A, et al. COVID-19 related fears of patients admitted to a psychiatric emergency department during and post-lockdown in Switzerland: preliminary findings to look ahead for tailored preventive mental health strategies. Medicina. 2021;57(12):1360. doi:10.3390/medicina57121360
30. Carstensen LL, Pasupathi M, Mayr U, Nesselroade JR. Emotional experience in everyday life across the adult life span. J Pers Soc Psychol. 2000;79(4):644. doi:10.1037/0022-3514.79.4.644
31. Yu CC, Tou NX, Low JA. A comparative study on mental health and adaptability between older and younger adults during the COVID-19 circuit breaker in Singapore. BMC Public Health. 2022;22(1):1–11. doi:10.1186/s12889-022-12857-y
32. AlAteeq DA, Aljhani S, Althiyabi I, Majzoub S. Mental health among healthcare providers during coronavirus disease (COVID-19) outbreak in Saudi Arabia. J Infect Public Health. 2020;13(10):1432–1437. doi:10.1016/j.jiph.2020.08.013
33. Alghamdi BS, Alatawi Y, Alshehri FS, Tayeb HO, AboTaleb H, Binsalman A. Psychological distress during COVID-19 curfews and social distancing in Saudi Arabia: a cross-sectional study. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.792533
34. Quadros S, Garg S, Ranjan R, Vijayasarathi G, Mamun MA. Fear of COVID 19 infection across different cohorts: a scoping review. Front Psychiatry. 2021;12:1289.
35. Czepiel D, Hoek HW, van der Markt A, et al. The association between exposure to COVID-19 and mental health outcomes among healthcare workers. Front Public Health. 2022;2022:1566.
36. Berardelli I, Vaia A, Pompili M. Thoughts of death, depression and guilt in a healthcare worker who infected her husband with SARS-CoV-2: a case report. NS Neurol Disord Drug Targets. 2021;20(4):385–388.
37. Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: a web-based cross-sectional survey. Psychiatry Res. 2020;288:112954. doi:10.1016/j.psychres.2020.112954
38. Gupta R, Grover S, Basu A, et al. Changes in sleep pattern and sleep quality during COVID-19 lockdown. Indian J Psychiatry. 2020;62(4):370–378. doi:10.4103/psychiatry.IndianJPsychiatry_523_20
39. Pinto J, van Zeller M, Amorim P, et al. Sleep quality in times of Covid-19 pandemic. Sleep Med. 2020;74:81–85. doi:10.1016/j.sleep.2020.07.012
40. Targa AD, Benítez ID, Moncusí-Moix A, et al. Decrease in sleep quality during COVID-19 outbreak. Sleep Breath. 2021;25(2):1055–1061. doi:10.1007/s11325-020-02202-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Perceptions, Level of Government Trust, and Psychological Distress During COVID-19 Pandemic in Taiwan
Chang PY, Shih FY, Lee MB, Lin CF, Lyu SY
Psychology Research and Behavior Management 2022, 15:3313-3327
Published Date: 15 November 2022