Back to Journals » Nature and Science of Sleep » Volume 13
Mental Activity During Episodes of Sleepwalking, Night Terrors or Confusional Arousals: Differences Between Children and Adults
Authors Castelnovo A, Loddo G ![]() , Provini F
, Provini F ![]() , Miano S, Manconi M
, Miano S, Manconi M ![]()
Received 16 March 2021
Accepted for publication 21 May 2021
Published 21 June 2021 Volume 2021:13 Pages 829—840
DOI https://doi.org/10.2147/NSS.S309868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Elena Urrestarazu
Anna Castelnovo,1– 3 Giuseppe Loddo,4 Federica Provini,5,6 Silvia Miano,1 Mauro Manconi1,2,7
1Sleep Medicine Unit, Neurocenter of Southern Switzerland, Ospedale Civico, Lugano, Switzerland; 2Faculty of Biomedical Sciences, Università della Svizzera Italiana, Lugano, Switzerland; 3University Hospital of Psychiatry and Psychotherapy, University of Bern, Bern, Switzerland; 4Department of Primary Care, Azienda USL di Bologna, Bologna, Italia; 5IRCSS Istituto delle Scienze Neurologiche di Bologna, Bologna, Italia; 6Department of Biomedical and Neuromotor Sciences, University of Bologna, Bologna, Italia; 7Department of Neurology, University Hospital, Inselspital, Bern, Switzerland
Correspondence: Anna Castelnovo Ospedale Civico Via Tesserete 46, Lugano, 6900, Switzerland
Email [email protected]
Objective/Background: Night terrors, sleepwalking and confusional arousals are behavioral manifestations of incomplete awakenings from sleep. According to international diagnostic criteria, these behaviors occur in the absence of any mental experience, or in the presence of very limited cognition or dream imagery (eg, a single visual scene). The aim of this study was to systematically and retrospectively investigate the mental content associated with sleep terrors and/or sleepwalking in both children and adults.
Patients and Methods: Forty-five consecutive patients referred for a diagnosis of disorders of arousal (DOA) of all subtypes (sleepwalking/sleep terrors/confusional arousals) (25 adults: 30 ± 6 y, 15 females; 20 children: 10 ± 3 y, 6 females) underwent a detailed semi-structured interview about the mental content associated with their nocturnal episodes. The interview was comprehensive of specific questions about their subjective recall rate, several content details (characters, emotions, actions and setting/context), and hallucinatory or dissociative experiences during clinical episodes. Patients’ reports were classified for complexity (Orlinsky scale) and content (Hall and Van de Castle categories).
Results: More than two-third of the children (n = 14) could not recall any mental activity associated with their episodes, whereas more than two-third (n = 16) of the adults recalled at least one mental experience. Half of the adult patients (n = 8) estimated that a specific mental content was subjectively present around 50% or more of the times. Seven adults and one child described clear and vivid hallucinatory experiences of “dreamed” objects or characters projected onto their real home environment, in the absence of any reality testing. Five adults and two children described one or more dissociative experiences. The content of the collected reports was dominated by dynamic actions acted out from a self-perspective, often with apprehension and in response to misfortune and danger, in a home-setting environment.
Conclusion: These results suggest that current diagnostic criteria are tailored around the typical presentation of DOA in children, and do not always fit to adult patients with DOA. Furthermore, they support the concept that consciousness may reemerge in DOA patients during clinical episodes, in a peculiar dissociated, psychotic-like form.
Keywords: somnambulism, confusional arousal, parasomnia, dream, consciousness, mental content, amnesia
Introduction
Up to 34% of toddlers, 13.4% of school-age children1 and 4.8% of adults2 occasionally display complex behaviors during sleep, such as walking around, abruptly sitting up in bed screaming or looking around while partially asleep. After the episodes, patients typically fall asleep again quickly and display a partial or complete amnesia for their episodes the subsequent morning. These manifestations belong to the same family of disorders, namely Non-Rapid Eye Movement (NREM) sleep parasomnias, or more specifically disorders of arousals (DOA). DOA are broadly defined as recurrent episodes of incomplete awakening from NREM sleep and are classified in 3 clinical subtypes: sleepwalking, night terrors and confusional arousals. Despite behavioral differences, they share common features: they typically occur during NREM slow wave sleep, mainly during the first third of the major sleep episodes,3–5 their prevalence and incidence decrease progressively during adulthood, and they typically display a strong and often overlapping familiar recurrence and a similar genetic background.1,6–9
International classification systems3,4 recognize unanimously the absence of, or the presence of only limited dream imagery or cognition during DOA episodes. This might not seem surprising, considering that DOA arise from NREM slow wave sleep, which is traditionally considered a dreamless unconscious state. However, several studies have shown that dreaming and mental activity during sleep occur independently of the sleep state, and can occur in one third or more of the awakenings out of NREM sleep.10,11 These findings support the hypothesis that oneiric mental activity might in theory occur during DOA episodes.
Initial investigations on this topic, based on a rather limited number of children and/or young adults with sleepwalking, reported complete amnesia for any mental content or behavior they displayed soon after spontaneous awakening from sleepwalking episodes and/or the following morning.12–14 However, subsequent studies that actively probed patients about their generic mental activity during episodes (without using specifically the word “dream”), contradicted earlier findings. A systematic study on young adults with a diagnosis of sleep terrors showed a 58% average recall rate of mental imagery upon awakening after episodes, although recall was often fragmentary and consisting of a single scene or thought.15 Later, occasional reports confirmed the presence of some kind of activity including perceptual, cognitive, and affective elements in at least the more complex and agitated DOA episodes.16–19 Few and more recent case-reports further reinforced this concept, illustrating extreme examples of complex, dreamlike and enacted mental activity during DOA episodes.20–24 Retrospective studies on adult DOA patients (with sleepwalking and/or sleep terrors) showed that 71–77% of patients were able to recall a mentation associated with at least one of their lifetime episodes, usually consisting of one single visual scene.25,26 The content analysis of these (retrospectively collected) reports26,27 revealed that they were frequently unpleasant and often contained misfortune and apprehension. When compared to REM sleep behavior disorder (RBD) they displayed less aggressive contents, with patients being more often the victims rather than the aggressors.27
Taken together, the literature challenges the classic view of DOAs as amnesic, non-dreaming states. However, the great majority of available published data refer exclusively to adult samples. Although it is generally acknowledged among sleep experts that children are more frequently completely amnesic of their episodes than adults, surprisingly almost no systematic study on this topic has been conducted to date in children. Moreover, no study specifically addressed the issue on how dream-like perceptual experiences are phenomenologically integrated with real perceptions. Indeed, DOA patients open their eyes during episodes and are able to deambulate through space usually without falling or stumbling on objects, but at the same time they at times display behaviors like pointing or grasping inexistent objects, which have been suggested to reflect the enactment of an ongoing mental content.20,21,26
In this study, we investigated the lifetime prevalence and the qualitative features of mental activity associated with DOA episodes in both children and adults, with a specific attention towards hallucinatory and dissociative experiences.
Methods
This is an observational, single-center cross-sectional study carried out at the Neurocenter of Southern Switzerland on a population of patients affected by DOA. The protocol of the study was approved by the local Independent Ethics Committee (IEC) “Comitato Etico Cantonale”, according to the regulatory requirements of Switzerland, as part of a larger instrumental study (2017–01788 CE 3282). All research activities were conducted in accordance with the Helsinki Declaration. Eligible patients (and/or their caregivers according to their age) signed a written informed consent prior to participate in the study.
Patients
Participants were recruited consecutively among patients referred to the Sleep Medicine Center because of abnormal nocturnal behaviors. Patient’s inclusion criteria were: 1) a typical history of DOA (all subtypes: night terror, sleepwalking, confusional arousal) according to ICSD-3 criteria;4 2) a minimum of one parasomnia episode per month as defined from the clinical interview; 3) age between 6 and 17 years old for the children group, and from 18 to 45 years for the adult group. Exclusion criteria were: 1) parasomnia due to a medical disorder or due to a medication or substance; 2) parasomnia overlap disorder; 3) sleep-related sex disorder, and sleep-related eating disorder (as exclusive symptoms); 4) intellectual disability; 5) epilepsy and other major neurologic co-morbidities. All patients were also monitored with video-polysomnography (v-PSG), which excluded differential diagnosis like epilepsy or REM sleep behavior disorder.
Clinical Interview
Patients were thoroughly interviewed by a sleep specialist concerning their medical, psychiatric and sleep history. They also received a complete neurological examination, and filled in a set of validated sleep rating scales (Epworth Sleepiness Scale, Sleep condition Indicator, Insomnia Severity Index for the adult group and Sleep Disturbance Scale for Children). Patients who satisfied inclusion/exclusion criteria and (when available) their parents or bedpartners/relatives subsequently underwent a semi-structured interview focused on the mental content during life-time DOA episodes. The meaning of “DOA episodes” was explained to children and some examples were provided to them if necessary, making clear the difference between mental activity during episodes and normal dreams.
Patients were asked to rate how frequently they could remember their mental content during an episode on a Likert scale: 0 = never, 1 = unclear (the recollection of just the very last part of the episodes during the transition to wakefulness, or the feeling of having dreamt something but no or very vague associated content), 3 = once or few times, <10% of the times), 4 = seldom (10–40%), 5 = sometimes (40–60%, around 50%), 6 = often (60–90%), 7 = always or almost always (>90%).
Patients were also asked whether they woke up immediately after the remembered episodes and to estimate the overall rate of awakenings after DOA episodes (considering the estimated frequency of episodes reported by witnesses), according to the same 5-point Likert scale described above.
Patients were also systematically asked to describe their episodes from a subjective standpoint and whether they could remember or not what was going through their mind at the very moment of a DOA episode, whenever in their life. If they answered positively to this latter question, spontaneous mentation reports were prompted. Afterwards, patients were interviewed more pointedly to elicit other relevant details for each recollection, including characters, emotions, content and setting. Specific questions were made about hallucinations (defined as the perception of the normal external environment with overlapping elements from their dreams associated with a failure of reality testing3), dissociative/partial awareness experiences (derealization/depersonalization/“as if” feeling of being both in the real world and in a dream), and indirect evidence of acting out the mental content they recollected (eg, waking up in a specific location or position).
Available family members/bedpartners (20 out of 20 for children and 22 out of 25) were asked whether the patient ever told them what was going through his/her mind during DOA episodes and to describe in details each episode they could remember (behaviors, perceived emotions, vocalizations, indirect evidence of hallucinations, eg, pointing behaviors, grasping behaviors or other gestures, searching behaviors, verbalizations suggesting the presence of invisible objects or entities). When possible, the presence of witnessed episodes was matched with the recall by the patient in order to identify possible “isomorphic behaviors”, meaning mental contents acted out during the episodes.
Scoring Analysis
Mental contents were classified according to their complexity using the Orlinski’s score (see Supplementary Table 1).
Each mental content was analyzed according to the nominal categories of the Hall and Van De Castle method28 by two independent scorers (AC and GL): characters (people, mythical figures, and animals), social interactions (aggressiveness, friendliness, sexuality), activities (physical activities with the character remaining more or less in the same place, self-propelled movements, location changes using tools other than muscular activity, expressive communication, verbal activity, auditory, visual activity, thinking), emotions (happiness, anger, apprehension, sadness, and confusion), striving (success and failure), fortune (misfortune and good fortune), settings (indoor, outdoor, familiar, unfamiliar, distorted, geographical), objects (architecture, household, food, implements, travel, streets, regions, body parts, clothing, communication, money, miscellaneous), and descripting elements (modifiers, temporal scale, negative scale). The presence or absence of any given category was determined in accordance with the “at least” procedure. Because most of the sleep mentation reports contained fewer than 50 words, and the normative values have been established for 50–350-word contents, only the categories were used. All repetitions and hesitations as well as the content that referred to what the dreamers thought of their dreams rather than the actual dream were eliminated prior to this analysis.
Statistics
Data are presented as numbers, percentages (%), mean ± standard deviation (M ± SD).
The between-group (children vs adults) difference in recall (taken as a binary yes/no variable) was measured using a chi-square test for independence (with Yates Continuity correction). The relationship between the mental content recall rate and the awakening recall rate (measured on an 8-point Likert scale as described above) was investigated using Spearman rho product-moment correlation coefficient.
Results
Forty-five consecutive patients with DOA (25 adults: 30 ± 6 y, 15 females; 20 children: 10 ± 3 y, 6 females) were recruited and considered for current analyses. Demographics and clinical features of the adult and the children groups are described in Supplementary Table 2.
Children
Only four children out of 20 (20%) stated they rarely remembered the mental content associated with their DOA episodes (9 mental imageries in total, see Supplementary Table 3). In 2 cases (10%) the report was unclear, eg:
“I think I remember going upstairs to the granny but I am not sure, maybe I remember it because I think I woke up upstairs and my parents the day after told me about what happened”
“I somehow recall the feeling of being alone or very small or scared to be tiny or getting smaller to the point of disappearing during my episodes, but I do not recall anything else)”.
Fourteen children (70%) reported to be amnestic about their episodes. A graphical representation of these data is available in Figure 1.
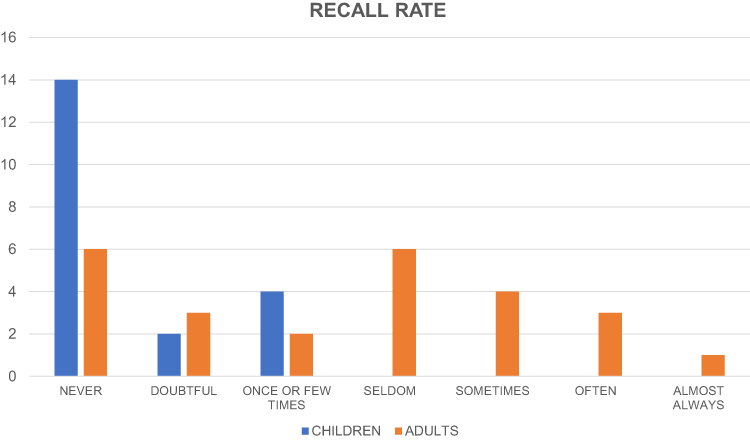 |
Figure 1 Subjective recall rate for the children group and the adult group. X-axis: number of patients. Y-axis: recall rate according to a 7-point Likert scale (see Methods). |
Five children (25%) reported they woke up at least once or very few times, 2 (10%) were not sure about the answer, 13 (65%) reported they never woke up after an episode and they knew about the episodes only because somebody else told them. A graphical representation of these data is available in Figure 2. There was a strong, positive correlation between the content recall rate and the subjective awakening rate after episodes, r = 0.91, n = 20, p < 0.001.
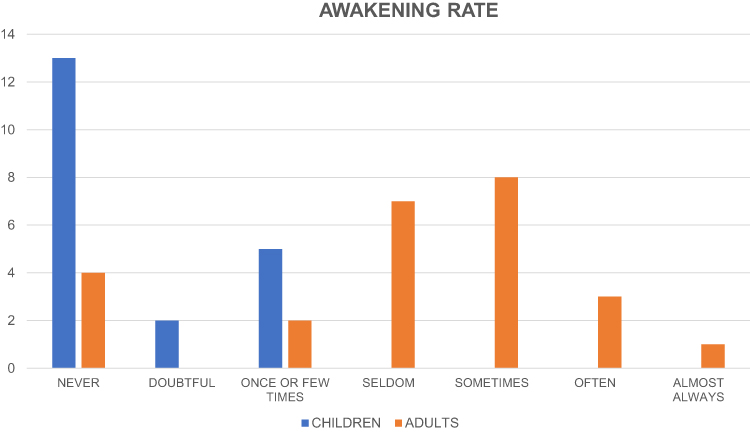 |
Figure 2 Post-episode awakening for the children group and the adult group. X-axis: number of patients. Y-axis: frequency of post-episode awakening according to a 7-point Likert scale (see Methods). |
One of the children (5%) was able to report a full hallucinatory experience (“I truly saw the ball going out of the window of my room, but it was like it went out of the football field and I didn’t realize it was not possible”). In two cases (10%) the recollection was less clear:
“I saw the referee in the dream and the day after dad told me I was talking to him as he was the referee, but I can’t remember precisely the context in which I saw the referee, neither if he was similar to dad”
“I heard the doorbell but I do not remember if I was already out of the bed when I heard it or what I was doing”.
In 12 cases (60%) an indirect evidence of hallucinatory experiences was inferred by the parents: in 4 cases by finger pointing behaviors, in 1 case from grasping behaviors, in 3 (more doubtful) cases by searching behaviors and in 4 cases from verbalizations, suggesting the presence of invisible objects or entities associated or not with pointing behaviors (eg “Look, look, mum”, “I want those colors mum, please let me draw”, “Leave me, leave me!”, “Help me, help me, what is that head floating in the air?”, or “stop it, stop it”, “get this reindeer out” or “a light over there, look!”). Two children out of 20 were able to describe dissociative/partial awareness features:“I dreamt I was in a room that looked like mine … but I was on the first floor, instead of the second floor where I usually sleep … I was actually at the second floor, but I realized it later”
“I was in my room but it was like I was in a football game”.
Four reports of mental contents associated with DOA episodes out of 9 were classified as “static” (score: 4) and 5 (4 with score 5 and 1 with score 6) as “dynamic” dreams according to the Orlinsky’s Modified Scale. All reported imageries had direct or indirect evidence of being acted out. In all of them the patient was the first-person character. Only in 3 cases the first-person character interacted with another (human) character. All recollections contained a purposeful action (either a physical action, a movement with or without a change in location or a verbal interaction) usually within the house environment. In most cases, the protagonist was trying to do something with active effort, but it was difficult to apply the Van De Castle Category Failure or Success because only the protracted attempt was remembered and reported. In 2 cases, there was a clear environmental barrier (misfortune of the Van De Castle scale). An emotion was associated in 4 out of 9 reports (3 were coded as apprehension and one as happiness).
Adults
Adults were more likely to recall their mental activity during DOA episodes than children (χ2 (1, n = 45) = 7.75, p = 0.05, phi = 0.46). Six adult patients stated they never remembered what was going through their mind during clinical episodes, while in other 3 cases the recollection was doubtful (in 2 cases there was the feeling of having dreamt something without any specific associated content, and in 1 case the recall of the few moments before waking up “I was brushing my teeth and it still made sense, like in a sort of dissociative state”). Sixteen (76%) were able to report at least one specific mental experience associated with their episodes at the clinical interview (for a total of 48 reports, see Supplementary Table 3).
Two patients answered “one or few times”, 6 patients “seldom” (less than half of the times), 4 patients “sometimes” (nearly half of the times), 3 answered “often” (more than half of the times) and 1 answered almost always (see Figure 1). This latter case has been recently described in a case report, given the exceptionality of the frequency and complexity of the dream-like imageries he reported.29
Only 4 subjects (16%) reported they never woke up after their clinical episodes, while the great majority reported they woke up between 10 and 60% of the times (see Figure 2). Qualitatively, all patients stated that they usually remembered those episodes that were followed by an awakening and the recollected episodes were followed almost invariably by an awakening. There was a strong, positive correlation between the content recall rate and the subjective awakening rate after episodes, r(23) = 0.82, p < 0.001. Similar results were obtained also pooling adult and children together and correcting for age (see Supplementary Figure 1).
Seven subjects (almost 30%) were able to describe clear hallucinatory experiences, meaning that they both perceived the real environment plus one or more overlapping images or distorted features and at the same time they were not aware that their perception was unreal, strange or bizarre. Specific examples are:
“Yes, I am sure I saw some rabbits jumping around my house, I could see clearly both my house and the rabbits”, “Yes, I was really seeing an unknown man at the end of my house’s hallway.”
In other two cases, the description was unclear or the patient was unsure about his/her memory. Indirect evidence of hallucinatory experiences was collected by bedpartners in 14 cases (pointing behaviors in 3 cases, other behaviors like grasping or trying to escape from something in other 3 cases, and combinations of gestures and exclamations in the remaining 8 cases). In the other cases, the description was unclear or the bedpartner was unsure about the interpretation of the patients’ gestures or mumblings. Dissociative experiences clearly emerged from 9 reports (from 5 different patients) out of 48, while in 2 cases the description was unclear, eg:“I was brushing my teeth and I realized the absurdity of the situation slowly, I think I kept brushing my teeth for a little while”.
In 8 cases, dissociation emerged from the discrepancy between being aware of seeing a specific scenario and being at the same time aware of being at home and seeing one’s own home setting or seeing distorted images, eg:“I was patting a dog, but at the same time I was somehow aware it was the blanket covering my boyfriend”.
In 1 case, the experience was described as a depersonalization state (the patient had the impression of observing himself while walking along the hallway of his house).Twenty-five reports were classified as “static” and 23 as “dynamic” dreams according to the Orlinsky’s Modified Scale.
Twelve reports (25%) were associated with direct evidence of being acted out (from witnesses), 2 (0.05%) with indirect proofs found by patients the following morning (objects moved from their usual position), the remaining 34 cases with indirect evidence from the actions the patients were carrying out at the time they woke up. In 17 of these latter cases the description was unequivocable, eg: “I woke up when I was closing the closet” with the associated mental recollection
“I was seeing an unknown man in my house, at the end of the stairs, he wanted to have a shower in my house, after a brief discussion with him, I went to my closet and took the towel”,
while in the other 17 cases the description was more unspecific, eg: “I woke up while walking around” with the associated recollection:
“I was looking for someone in the house”.
Forty reports contained the self as the main character while making a motor action, in the remaining 6 case there was just the description of an image or a thought, eg:
“I saw some insects in my bed” or “there were snakes in the room”, “I had the feeling something was missing”
and were labeled as unclear.According to the categories of the Hall and Van de Castle method (see Figure 3), 19 (40%) of the reports contained the presence of at least one person, 12 (25%) animals (insects in 50% of the cases), and 1 a mythological creature (a “monster”). The people seen during sleepwalking/sleep terrors were more often (58%) unknown by the dreamer (uncertain identity: 21%, strangers: 26%, occupational label: 21%), and in 42% of the cases were family members or other relatives of the dreamer. Nighty-six percent of the reports contained an action (and 46% two or more actions), the great majority a motor activity (n = 36), followed by visual activities (n = 16), thinking (n = 9), verbal (n = 4), or auditory (n = 1) activities. The majority of the reports could not be scored according to the category success (n = 3) and failure (n = 2), as it was only described an ongoing activity. Social interactions were sporadically present (23%), and were friendly in more than half of the cases (n = 6) and aggressive in the remaining cases (n = 5). Aggressive behaviors by the dreamer were almost invariably defense behaviors in reaction to misfortune, which was present in 30 out of 48 recollections (63%). Misfortune included any mishap, injury, harm, danger, threat which happened to the characters as a result of circumstances over which they did not have control. The recall of thieves or strangers at homes, which was very frequent, was included in this category. There were no sexual elements in the dreamlike mentation reports. A specific emotion was recalled in 65% of the cases, and it was almost invariably apprehension (30 out of 31), which included fear, anxiety, and uneasiness. Eighty-five percent of the reports contained the description of a setting, in the great majority of cases indoor (75%) and familiar (69%, usually at home). Eighty-five percent of the reports contained the description of an object, usually an architectural (56%) or household (38%) elements. Overall, an in-home setting could be recognized in 37 descriptions out of 48 (77%), of which 8 cases contained a mixture of the real in-home features and details from an internally generated (usually out-home) environment. Descriptive elements were almost absent.
 |
Figure 3 Content categories scored using the Hall and Van de Castle system in dreams over a lifetime in the adult group. The values for each category are expressed as % (y-axis). Main categories are in capitals, sub-items in cursive (x-axis). |
Discussion
This study offered for the first time a systematic retrospective evaluation of the mental activity associated with lifetime DOA episodes in a fairly large sample of children by means of a systematic semi-structured interview collected with both children and their parents. The same investigation was extended to a group of adult patients with DOA for a qualitative comparison with the children group and for a confirmation of the previous limited literature.25–27
The Recollection of Mental Content Associated with DOA Episode is to Be Low in Children but High in Adults
Although it was difficult for the patients to provide a precise estimation of their recall rate (as in26), they all easily provided an answer to our ranked scale.
While the majority of children reported complete amnesia for their episodes, about one third was able to recollect episodically some short sketches of mental activity like images, sounds, thoughts and actions. One child was also able to report one long dreamlike scenario.
The reports collected from the adult group confirmed instead a subjective high prevalence of dreamlike mentation contents during their DOA episodes, in line with the previous literature.15,26,27 In our sample, more than three quarters (76%) of the adult subjects were able to recollect at least one mentation related to their nocturnal episodes. This percentage is comparable with two previous similar retrospective works (71%26 and 77%,25 respectively). Regarding the content, the Van de Castle’s scale revealed results in line with the only two previous existing studies26,27 and confirmed high levels of apprehension, misfortune, self-defense behaviors, occurring in at-home settings.
Notably, about one third of adult patients stated that they frequently recalled some form of mental activity (>40%). This percentage express the ratio between the number of episodes associated with a mental recollection divided the total number of episodes. Therefore, it might be biased both in the direction of an overestimation, as many DOA episodes could pass unnoticed by both patients and bedpartners, and in the direction of an underestimation due to memory loss with time and the retrospective nature of the study. While a real estimation of prevalence of DOA episodes associated with mental activity could not be inferred by the current study, our results suggest that this association is not rare or uncommon in adults.
This is in line with the finding by a recent study that showed that the sensitivity for the diagnosis of DOA in adults increased when the ICSD-3/DSM-53,4 items about mental content recollection and event amnesia were not taken into consideration.30 The only study that systematically investigated the ongoing mental content upon awakenings in DOA (12 adult subjects with a diagnosis of night terrors, with over 250 in-laboratory recording nights) found an average recall rate of 58% from 275 spontaneous episodes.15 Similar studies on other DOA subtypes are not currently available. One study on a mixed sample of 32 patients with sleepwalking and sleep terrors, in which patients were also interviewed on spontaneous awakening in the morning (except for potentially dangerous motor events requiring the intervention of the technicians, which were interviewed after nighttime awakenings), showed that 38% of the patients remembered at least one “dream” associated with their episodes.27 Interestingly, this percentage was higher in the DOA group compared with a group of patients with RBD, and DOA “dreams” were longer and more complex than RBD dreams.
Why the Recollection of Mental Content Associated with DOA Episode is Lower in Children Than in Adults?
The subjective lower recall rate in children might potentially be explained by different hypotheses.
Trivially, children might have less episodes to recall because they had overall less lifetime episodes. However, the observation that the great majority of children appeared to be completely unaware of their episodes makes this hypothesis less likely.
Adults might recall more frequently what was going through their mind during their DOA episodes because they more often wake up at the end of an episode. This is supported by the positive association we found between subjective mental content recall rate and post-episode awakenings in both groups. This association was also spontaneously noted by many adults and reported during their interviews.
Another possibility, which might be complementary, is that the different recall rate between children and adults relies on differences in brain activity during DOA episodes. Indeed, it is known that DOA episodes arise from the local “switch” to a wake-like EEG pattern in specific “isles” of the brain,31,32 under the background activity of NREM sleep (over fronto-parietal high-order associative areas and the hippocampus). These “isles” have been identified in brain areas controlling motor activity (eg, primary motor cortex) and emotions (eg, cingulate cortex, amygdala). In other words, there seem to be a state dissociation between different brain areas, or perhaps, even within the same brain region.33 The specific pattern of brain activity may vary in different individuals, and also among the same subjects across different episodes, possibly explaining the variability in the subjective recall rate. The progressive decline of slow wave activity with age34 may allow for more brain regions to display a wake-like pattern, and therefore an increasing frequency and complexity of mental activity.
Can We Call the Mental Recollection Associated with DOA Episodes “Dreams”?
It has been previously hypothesized that the mental activity associated with DOA episodes in adults may reflect the dreaming activity during NREM sleep.26 Under this framework, dreams may: 1) precede and possibly “trigger” partial awakenings in subjects predisposed to DOA episodes and/or 2) may arise from the ongoing internal mental activity during behavioral episodes, sustained by “activated” brain areas.
The discovery of high dream recall-rates from awakenings out of NREM sleep have overturned the traditional view of rigidly demarcated global sleep stages and suggested that localized areas of the brain behave as in “covert REM sleep”.35 In support of this interpretation, reports of dream experience in both NREM and REM sleep were associated with local decreases in low-frequency activity and increases in high-frequency activity in posterior cortical regions.36 This concept of local REM-like sleep within the global state of NREM sleep is extraordinary similar to the afore mentioned concept of local wake-like activity in the context of NREM sleep during DOA episodes. Thus, the brain dissociation observed during DOA episodes might represent the pathological drawback of a physiological condition, occurring many times per night. Indeed, the physiological dissociation occurring during dreams might act as a trigger of a larger scale and more extreme dissociation in predisposed subjects. In support of this hypothesis, mental activity typically displayed during DOA episodes seems to share similar features with NREM dreams: they are often limited to one visual scene or brief sketches of action, in line with the description of NREM sleep dreams, which are on average shorter and less elaborate than REM-sleep dreams.37 Moreover, the higher recall rate of mental activity in adults than in children with DOA also seems to parallel the gradual development of dream imagery and cognitive abilities in children.38,39 These observations support the idea that there is a similarity or even a continuity between dreams and mental contents during episodes.
Even more notably, one third of the adult patients with DOA and one child (the one who reported the most complex, dreamlike and longest mentation) were able to clearly describe full hallucinatory experiences, in which characters and objects from their mind were projected in their real home-setting environment, in the absence of any reality testing. In some cases, the “dreamed” scenario somehow coexisted with the real perception of the external environment, without apparent contradiction for the patients until the subsequent full awakening. We classified these experiences as dissociative states. These experiences might represent the tail of an ongoing dream or an ex-novo mental production triggered by the interaction with the environment. In any case, they seem to represent a different brain state compared to dreams, as suggested by the following observations: 1) brain activity must be different given the fact that the patient is acting a behavior, interacting with the environment, and clearly “seeing” somehow external objects; otherwise, he/she would not be able to deambulate through space without stumbling or falling; 2) the hallucinatory experiences described by our patients suggest that also phenomenologically, the mental contents associated with DOA episodes phenomenologically resemble more psychotic-like experiences than dreaming experiences, incorporating and/or distorting features of the real external environment with internally generated elements. Although highly speculative, the finding of a clear-cut increase in beta activity in the thalamus recorded by stereo-EEG in a patient with DOA40 goes in the same direction, given the role of the thalamus in sensory gating, and its postulated role in the generation of hallucinations.41,42
Last but not least, these observations suggest that DOA patients can be conscious during at least some of their episodes, although consciousness is clearly altered in its form compared to the one usually displayed during wakefulness (due to clear differences in brain physiology43). This concept is also sustained by both a well-established literature on consciousness during dreams and its neurobiological substrates.36,39
Limitations and Future Perspectives
Of note, the study could not offer an objective estimate of the prevalence of the mental experiences associated with DOA episodes given its intrinsic retrospective and subjective nature. There are two caveats to consider here.
First, its subjective design. It is conceptually impossible for a subject to estimate the real number of his/her episodes given that some of them might pass unnoticed by both the patient and/or his/her bedpartners/parents. Second, the retrospective nature of the study. Time might have altered and weakened the memory of the mentation associated with DOA episodes, progressively diminishing the recall rate (especially when emotional content was less intense). The consequent and unavoidable memory bias might also have affected some Van de Castle categories. For example, the emotional category might be biased towards negative emotions. Moreover, the bias associated with possible confabulation (for example, on the basis of wounds observed the subsequent morning, awakenings in places different from bed, recounts of witnesses), should induce cautiousness in interpretation of the data.44
These issues could only be addressed by experimental studies comprehensive of serial night recordings and/or the use of episodes’ promoting paradigms like sleep deprivation/acoustic stimuli, which allows to capture several DOA episodes and a direct interview of the patients soon after each episode. However, our study offered a complementary and more clinically oriented piece of information. We presented what real patients might report to physicians during their clinical interviews, adding details that might further advance the diagnosis of DOA, which is currently only relies on clinical criteria. Our results encourage clinician to not discard a possible diagnosis of DOA when patients report rich mental activity during their nocturnal episodes.
Another potential caveat includes the fact that we did not have a control condition, like for example the dreams’ recall rate and content. There is a known inter-subject variability in the ability to retrieve mental experiences during sleep when wake, and we cannot say at present whether this variability goes in parallel with the episodes recall rate. Neither we can say whether the mental content during episodes differ statistically and in which details from normal, physiological dreams. There is limited evidence suggesting that the recall rate of dreams from both REM and NREM sleep in sleepwalking is reduced,12 and this represents for sure an interesting area to cover in future studies.
Another limitation is the rather limited sample size. While the total number of subjects is in line with the previous literature26,27 and it is sufficient to give an indication of the estimated subjective recall rate of mental imageries associated with DOA episodes, the wide age-range, the heterogeneity of DOA subtypes and their frequent overlap limited the possibility of several interesting intra-group comparisons and stratification analyses.
Conclusion
While current diagnostic criteria of DOA suit the great majority of DOA diagnoses in children, clinicians should be aware that some degree of mental dream-like activity might be reported by adult DOA patients, and even though more rarely, also by children with DOA. The lower subjective recall rate in children than in adults might reflect differences in brain physiology, such as the intensity and globality of slow wave activity and in the likelihood of waking up soon after DOA episodes.
The reported mental activity during clinical DOA episodes suggests that consciousness reemerges, at least episodically, during at least some of the DOA episodes. Both the subjective description of mental contents by patients and the description of their behaviors by witnesses suggest a complex interaction between internally and externally generated percepts. The phenomenology described seems to be more evocative of a hallucinatory, psychotic-like mental state rather than a dreamlike state, which may occur while a “dreaming” subject partially wake up and start to interact with the external environment.
Acknowledgments
We are grateful to all the patients and their parents/bedpartners who carefully and patiently answered to our detailed interview.
Funding
This study was supported by an ABREOC grant (Advisory Board of Scientific Research of the Ente Ospedaliero Cantonale).
Disclosure
Professor Federica Provini report personal fees from Italfarmaco, Zambon Italia, Eisai Japan, Pfizer, outside the submitted work. The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
References
1. Petit D, Pennestri MH, Paquet J, et al. Childhood sleepwalking and sleep terrors: a longitudinal study of prevalence and familial aggregation. JAMA Pediatr. 2015;169(7):653–658. doi:10.1001/jamapediatrics.2015.127
2. Ohayon MM, Priest RG. Night terrors, sleepwalking, and confusional arousals in the general population: their frequency and relationship to other sleep and mental disorders. J Clin Psychiatry. 1999;60(4):268–276. doi:10.4088/JCP.V60N0411
3. APA. Diagnostic and Statistical Manual of Mental Disorders.
4. AASM. The International Classification of Sleep Disorders (ICSD-3).
5. Proserpio P, Loddo G, Zubler F, et al. Polysomnographic features differentiating disorder of arousals from sleep-related hypermotor epilepsy. Sleep. 2019. doi:10.1093/sleep/zsz166
6. Hublin C, Kaprio J, Partinen M, Heikkilä K, Koskenvuo M. Prevalence and genetics of sleepwalking: a population-based twin study. Neurology. 1997;48(1):177–181. doi:10.1212/WNL.48.1.177
7. Lecendreux M, Bassetti C, Dauvilliers Y, Mayer G, Neidhart E, Tafti M. HLA and genetic susceptibility to sleepwalking. Mol Psychiatry. 2003;8(1):114–117. doi:10.1038/sj.mp.4001203
8. Licis AK, Desruisseau DM, Yamada KA, Duntley SP, Gurnett CA. Novel genetic findings in an extended family pedigree with sleepwalking. Neurology. 2011;76(1):49–52. doi:10.1212/WNL.0b013e318203e964
9. Heidbreder A, Stefani A, Brandauer E, et al. Gray matter abnormalities of the dorsal posterior cingulate in sleep walking. Sleep Med. 2017;36:152–155. doi:10.1016/j.sleep.2017.05.007
10. Siclari F, LaRocque JJ, Postle BR, Tononi G. Assessing sleep consciousness within subjects using a serial awakening paradigm. Front Psychol. 2013;4. 10.3389/fpsyg.2013.00542.
11. Foulkes WD. Dream reports from different stages of sleep. J Abnorm Soc Psychol. 1962;65(1):14–25. doi:10.1037/h0040431
12. Jacobson A, Kales A. Somnambulism: all-night EEG and related studies. Res Publ Assoc Res Nerv Ment Dis. 1967;45:424–455.
13. Jacobson A, Kales A, Lehmann D. Somnambulism: all-night electroencephalographic studies. Science (80-). 1965;148(3672):975–977. doi:10.1126/science.148.3672.975
14. Kales A, Jacobson A, Paulson MJ, Kales JD, Walter RD. Somnambulism: psychophysiological correlates: i. All-night EEG studies. Arch Gen Psychiatry. 1966;14(6):586–594. doi:10.1001/archpsyc.1966.01730120026004
15. Fisher C, Kahn AE, Davis D. A psychophysiological study of nightmares and night terrors. Psychoanal Contemp Sci. 1974;3:317–398. doi:10.1109/APMC.2009.5384284
16. Arnulf I, Zhang B, Uguccioni G, et al. A scale for assessing the severity of arousal disorders. Sleep. 2014;37(1):127–136. doi:10.5665/sleep.3322
17. Guilleminault C, Moscovitch A, Leger D. Forensic sleep medicine: nocturnal wandering and violence. Sleep. 1995;18(9):740–748. doi:10.1093/sleep/18.9.740
18. Pilon M, Montplaisir J, Zadra A. Precipitating factors of somnambulism symbol: impact of sleep deprivation and forced arousals. Neurology. 2008;70(24):2284–2290. doi:10.1212/01.wnl.0000304082.49839.86
19. Szucs A, Kamondi A, Zoller R, Barcs G, Szabó P, Purebl G. Violent somnambulism: a parasomnia of young men with stereotyped dream-like experiences. Med Hypotheses. 2014;83(1):47–52. doi:10.1016/j.mehy.2014.04.012
20. Mwenge B, Brion A, Uguccioni G, Arnulf I. Sleepwalking: long-term home video monitoring. Sleep Med. 2013;14(11):1226–1228. doi:10.1016/j.sleep.2013.04.027
21. Rocha AL, Arnulf I. NREM parasomnia as a dream enacting behavior. Sleep Med. 2020;75:103–105. doi:10.1016/j.sleep.2020.02.024
22. Pillmann F. Complex dream-enacting behavior in sleepwalking. Psychosom Med. 2009;71(2):231–234. doi:10.1097/PSY.0b013e318190772e
23. Oudiette D, Constantinescu I, Leclair-Visonneau L, Vidailhet M, Schwartz S, Arnulf I. Evidence for the re-enactment of a recently learned behavior during sleepwalking. PLoS One. 2011;6(3):1–8. doi:10.1371/journal.pone.0018056
24. Bhat S, Chokroverty S, Kabak B, Yang QR, Rosen D. Dream-enacting behavior in non-rapid eye movement sleep. Sleep Med. 2012;13(4):445–446. doi:10.1016/j.sleep.2011.10.029
25. Baldini T, Loddo G, Sessagesimi E, et al. Clinical features and pathophysiology of disorders of arousal in adults: a window into the sleeping brain. Front Neurol. 2019;10:1–9. doi:10.3389/fneur.2019.00526
26. Oudiette D, Leu S, Pottier M, Buzare MA, Brion A, Arnulf I. Dreamlike mentations during sleepwalking and sleep terrors in adults. Sleep. 2009;32(12):1621–1627. doi:10.1093/sleep/32.12.1621
27. Uguccioni G, Golmard JL, de Fontréaux AN, Leu-Semenescu S, Brion A, Arnulf I. Fight or flight? Dream content during sleepwalking/sleep terrors vs rapid eye movement sleep behavior disorder. Sleep Med. 2013;14(5):391–398. doi:10.1016/j.sleep.2013.01.014
28. Domhoff GW. Emotions, personality, and psychotherapy. Finding meaning in dreams: A quantitative approach. Springer; 1996th edition. 1996. doi:10.1007/978-1-4899-0298-6
29. Castelnovo A, Loddo G, Provini F, Manconi M. Frequent, complex and vivid dream-like/hallucinatory experiences during NREM sleep parasomnia episodes. Sleep Med. 2021;82:61–64. doi:10.1016/j.sleep.2021.03.032
30. Loddo G, La Fauci G, Vignatelli L, et al. The Arousal Disorders Questionnaire: a new and effective screening tool for confusional arousals, sleepwalking and sleep terrors in epilepsy and sleep disorders units. Sleep Med. 2021;80:279–285. doi:10.1016/j.sleep.2021.01.037
31. Terzaghi M, Sartori I, Tassi L, et al. Dissociated local arousal states underlying essential clinical features of non-rapid eye movement arousal parasomnia: an intracerebral stereo-electroencephalographic study. J Sleep Res. 2012;21(5):502–506. doi:10.1111/j.1365-2869.2012.01003.x
32. Terzaghi M, Sartori I, Tassi L, et al. Evidence of dissociated arousal states during NREM parasomnia from an intracerebral neurophysiological study. Sleep. 2009;32(3):409–412. doi:10.1093/sleep/32.3.409
33. Flamand M, Boudet S, Lopes R, et al. Confusional arousals during non-rapid eye movement sleep: evidence from intracerebral recordings. Sleep. 2018;41(10):1–11. doi:10.1093/sleep/zsy139
34. Kurth S, Jenni OG, Riedner BA, Tononi G, Carskadon MA, Huber R. Characteristics of sleep slow waves in children and adolescents. Sleep. 2010;33(4):475–480. doi:10.1093/sleep/33.4.475
35. Nielsen TA. A review of mentation in REM and NREM sleep: “Covert” REM sleep as a possible reconciliation of two opposing models. Behav Brain Sci. 2000;23(6):851–866. doi:10.1017/S0140525X0000399X
36. Siclari F, Baird B, Perogamvros L, et al. The neural correlates of dreaming. Nat Neurosci. 2017;20(6):872–878. doi:10.1038/nn.4545
37. Kales A, Hoedemaker FS, Jacobson A, Kales JD, Paulson MJ, Wilson TE. Mentation during sleep: REM and NREM recall reports. Percept Mot Skills. 1967;24(2):555–560. doi:10.2466/pms.1967.24.2.555
38. Foulkes D. Children’s Dreaming and the Development of Consciousness. Cambridge, MA: Harvard University Press; 1999. doi:10.2307/j.ctvk12rff
39. Nir Y, Tononi G. Dreaming and the brain: from phenomenology to neurophysiology. Trends Cogn Sci. 2010;14(2):88–100. doi:10.1016/j.tics.2009.12.001
40. Sarasso S, Pigorini A, Proserpio P, Gibbs SA, Massimini M, Nobili L. Fluid boundaries between wake and sleep: experimental evidence from Stereo-EEG recordings. Arch Ital Biol. 2014;152(2–3):169–177. doi:10.12871/0002982920142311
41. Pinault D. Dysfunctional thalamus-related networks in schizophrenia. Schizophr Bull. 2011;37(2):238–243. doi:10.1093/schbul/sbq165
42. Ferrarelli F, Tononi G. The thalamic reticular nucleus and schizophrenia. Schizophr Bull. 2011;37(2):306–315. doi:10.1093/schbul/sbq142
43. Tononi G, Koch C. The neural correlates of consciousness: an update. Ann N Y Acad Sci. 2008;1124(1):239–261. doi:10.1196/annals.1440.004
44. Pressman MR. Sleepwalking, amnesia, comorbid conditions and triggers: effects of recall and other methodological biases. Sleep. 2013;36(11):1757–1758. doi:10.5665/sleep.3144
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.