Back to Journals » Nature and Science of Sleep » Volume 14
Men’s Sleep Quality and Assisted Reproductive Technology Outcomes in Couples Referred to a Fertility Clinic: A Chinese Cohort Study
Authors Du CQ ![]() , Zhang DX, Chen J, He QF
, Zhang DX, Chen J, He QF ![]() , Lin WQ
, Lin WQ
Received 15 December 2021
Accepted for publication 22 March 2022
Published 2 April 2022 Volume 2022:14 Pages 557—566
DOI https://doi.org/10.2147/NSS.S353131
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sarah L Appleton
Cong-Qi Du,1 Dong-Xue Zhang,1 Jing Chen,1,2 Qiu-Fen He,1,2 Wen-Qin Lin1
1Reproductive Medicine Center, the First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2Department of Embryo Laboratory, the First Affiliated Hospital, College of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
Correspondence: Wen-Qin Lin, Tel +86-0571-87235031, Email [email protected]
Background: Poor sleep quality has been linked to lower semen quality, but it is unclear whether this result in decreased fertility. To address this question, we retrospectively evaluated the relationship between men’s sleep quality and treatment outcomes in subfertile couples receiving assisted reproductive technology (ART).
Patient Enrollment and Methods: From September 2017 to November 2019, 282 subfertile couples referred to a Chinese fertility clinic and eligible for ART procedures were enrolled in our study. Sociodemographic characteristics, life habits, and sleep habits in the year prior to ART were recorded. Sleep quality was measured using the Pittsburgh Sleep Quality Index (PSQI). We first divided the patients into two groups based on sleep quality (good sleep: PSQI < 5 and poor sleep: PSQI ≥ 5). Then, the ART outcomes (fertilization rate, good quality embryo rate, implantation rate, positive pregnancy rate, clinical pregnancy rate, live birth rate, miscarriage rate, and birth weight) of each group were analyzed. Finally, multivariate linear and logistic regression analysis were used to examine the relationship between sleep quality (discrete variable or dichotomous variable) and ART outcomes.
Results: The participants in the poor sleep group showed a lower fertilization rate of 60.13% (543/903) when compared with 67.36% for the good sleep group (902/1339), P < 0.001. The global PSQI score had a significant influence on birth weight (β, − 63.81; 95% CI, − 119.91- − 8.52; P = 0.047), and live birth rate (OR, 0.88; 95% CI, 0.78- 0.99; P = 0.047) after adjusting for the interfering factors. Men’s sleep quality was unrelated to good quality embryos rate, implantation rate, positive pregnancy rate, clinical pregnancy rate, or miscarriage rate.
Conclusion: Men’s sleep quality was positively associated with fertilization rate, birth weight, and live birth rate among couples undergoing ART.
Keywords: sleep quality, PSQI, fertility, male reproduction, in vitro fertilization, intracytoplasmic sperm injection
Introduction
According to the World Health Organization (WHO), approximately 15% of the couples of childbearing age face fertility issues, and male factors contribute to 40%–50% of all infertility cases.1,2 The prevalence of infertility has increased significantly over the past decades, while the increasing prevalence of not optimal lifestyle factors such as obesity,3,4 tobacco5 or alcohol consumption. Because these lifestyle factors are modifiable, they represent an improved way of infertility management. In addition to the widely studied unhealthy lifestyle parameters associated with infertility, the short sleep duration and poor sleep quality6 were proved to be potential risk factors. Sleep is a naturally recurring state that is modulated by the circadian rhythm7 and homeostatic system.8 Inadequate sleep duration has been linked to adverse health outcomes, including all-cause mortality,9 cardiovascular diseases,10 hypertension,11 and diabetes.12
Therefore, the influence of sleep on reproduction and fertility has aroused widespread concern in recent years.13,14 Goldstein et al15 previously reported that women’s total sleep time was positively related to the oocytes retrieved during in vitro fertilization (IVF) treatment among 22 women presenting to an infertility clinic. Our previous studies in men confirmed those of other researchers, demonstrating that sleep quality16,17 and sleep duration17,18 are related to sperm concentration and sperm motility. However, other studies have not validated this relationship.19,20 Therefore, it is unclear whether the recently described sleep-related variations in semen quality translate into diminished fertility. Moreover, one study to date has evaluated whether sleep impacts couple fecundity rather than semen quality. Wise21 and colleagues found that fecundability ratios (FRs) were 0.62 (95% CI 0.42–0.87) in men who slept less than 6 hours per night compared to men who slept 8 hours per night. To further understand how sleep impacts male fertility, we evaluated the association of men’s sleep quality with infertility treatment outcomes of subfertile couples undergoing assisted reproductive technology (ART).
Materials and Methods
Study Population
This retrospective study was conducted on 342 infertile couples undergoing their first ART cycle with in vitro fertilization/ intracytoplasmic sperm injection (IVF/ICSI) in a reproductive medicine center from September 2017 to November 2019. Among couples attending the infertility clinic, the female partners were 20–42 years old. Of these 342 couples, 60 were excluded: 45 male partners used sperm retrieval techniques (testicular sperm extraction or percutaneous epididymal sperm aspiration), 4 male partners did not join the study, and 11 treatment cycles were canceled due to ovarian hyporesponse or natural pregnancy.
During the study period, the controlled ovarian stimulation protocols for women undergoing ART treatments included: long agonist protocol, antagonist protocol, ultra-long protocol. Only the first fresh embryo transfer cycle was analyzed in this study, and all the couples agreed to participate in this study with a signed informed consent form. This study was approved by the Research Ethics Committee of the First Affiliated Hospital, College of Medicine, Zhejiang University (No. 2017–708). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Questionnaire
Patient demographics, including age, education, occupation and duration of infertility, and lifestyle habits such as smoking, alcohol, coffee consumption, and exercise, were collected. Any history of chronic illness, urinary or reproductive disease, neurological or psychiatric condition, and a recent fever (≥38°C within the past 3 months) were also disclosed, and the Pittsburgh Sleep Quality Index (PSQI) was used to measure the sleep quality.22 The self-survey included 19 items reflecting the sleep quality of respondents in the past month. These items reflect sleep quality through seven components, namely: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. Each component was scored between 0–3, and the overall PSQI scores ranged from 0 to 21.
Ovarian Stimulation and Outcome Survey
Women underwent one of three ovarian stimulation treatment protocols for ART: long agonist protocol, antagonist protocol, or ultra-long protocol. Briefly, gonadotropins were initiated on day 3 of induced menses or after 14 days of down-regulation, and the GnRH agonist or antagonist was continued or started according to the usual ovarian stimulation protocols.23 The HCG trigger injection was administered when a transvaginal ultrasound revealed at least three dominant follicles (≥16 mm), and oocyte retrieval was completed after 36 hours. Oocytes underwent either conventional IVF or ICSI as clinically specified. The percentage of normally fertilized oocytes (2PN) in the inseminated oocytes was calculated as fertilization rate. The good-quality embryo rate was defined as the percentage of optimal embryos among the total number of cleavage embryos. Consequently, clinical outcomes were measured following the transfer of one or two embryos. The positive pregnancy rate referred to the percentage of positive pregnancies in the total fresh embryo transfer cycles, defined by an elevation in plasma β-HCG levels above 10 IU/L, measured 12 days after embryo transfer. The clinical pregnancy rate was defined as the percentage of clinical pregnancies in total fresh embryo transfer (ET) cycles, characterized by the presence of an intrauterine pregnancy confirmed by ultrasound at 6 weeks of gestation. The miscarriage rate referred to the percentage of early miscarriages in the clinical pregnancies, indicating pregnancy termination before 12 gestational weeks. The live birth rate referred to the percentage of live births to fresh embryo transfer cycles, defined as the birth of a neonate on or after 24 weeks of gestation.
Statistical Analysis
Data were presented as frequencies and percentages for categorical variables and mean standard deviation (SD) for continuous variables. The participants were divided into two groups according to a previously validated24–26 cut-off point (PSQI= 5), namely the good sleep group and the poor sleep group. A total PSQI score of 5 or more points indicates poor sleep quality.24–26 The PSQI features a diagnostic sensitivity of 98% and a specificity of 55%.24
We assessed the relationship between sleep quality and potential confounders using the Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables. To study the association of sleep quality (continuous variable or dichotomous variable, independent variables) with fertilization rate, good quality embryos rate, and birth weight (dependent variables), multivariate linear regressions were conducted. In contrast, binary logistic regressions were performed to study the relationship between sleep quality (continuous variable or dichotomous variable, independent variables) and positive pregnancy, clinical pregnancy, live birth, and miscarriage (dependent variables). Both continuous variable methods (general PSQI scores) and dichotomous variable methods (PQSI< 5 vs PQSI≥ 5) were both employed to analyze sleep quality. Two models were created: an unadjusted model with only the sleep quality (independent variables); and a second model with the main effects adjusted for potential confounders (independent variables) associated with ART outcomes (dependent variables), such as paternal age, BMI, smoking, alcohol drinking, and maternal age, BMI, duration of infertility, type of ovarian stimulation protocol, the number of retrieved oocytes, oocyte insemination technique (IVF/ICSI), global PSQI score, duration of sleep (categorical variable), endometrial thickness, number of embryos transferred, embryo transfer day.
Throughout the study, to reduce the probability of obtaining false positive results, the P-value was adjusted using Benjamini-Hochberg False Discovery Rate (FDR).27 Differences were considered to be statistically significant if P<0.05. Statistical analyses were performed using the Statistical Package for the Social Sciences version 23.0 (SPSS, Inc., IBM) software.
Results
Oocyte retrieval was performed on all 282 participating females. A total of 274 cycles were successfully fertilized, while no oocyte was retrieved, or fertilization was failed in 8 cycles. In addition, embryo transfer was completed in 267 cycles but failed in 7 cycles (3 with no cleavage and 4 with poor embryo quality). Finally, 183 positive pregnancies were recorded, leading to 164 clinical pregnancies and 141 cycles with live birth (Figure 1).
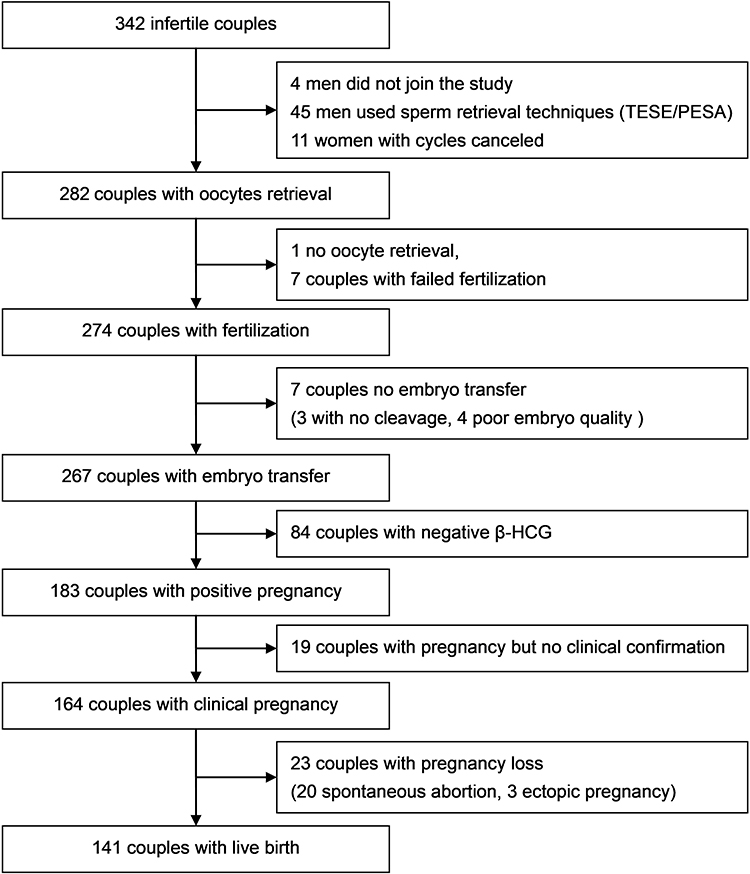 |
Figure 1 A cohort study population flowchart. Abbreviations: TESE, testicular sperm extraction; PESA, percutaneous epididymal sperm aspiration; HCG, human chorionic gonadotropin. |
The demographic characteristics are displayed in Table 1. The study population included 282 participants, with a mean age of 32.49 ±4.98 years and a BMI of 24.11 ±3.45 kg/m2. The median PSQI score was 4 (interquartile range, 3–6), and the mean PSQI score was 4.02 ±2.42, with an average sleep duration of 7.44 ±0.94 hours. A total of 110 participants (39%) were classified into the poor sleep group (general PSQI scores ≥5). Compared with the good sleep group, they experienced a shorter sleep duration (7.06 ±1.04 hrs), while their female partners had higher general PSQI scores (4.06 ±2.39). In Table S1, we re-grouped according to PSQI>5 as cut-off, a total of 62 participants (21.99%) were classified into the poor sleep group (PSQI>5). Compared with the good sleep group (PSQI≤5), they experienced a shorter sleep duration (6.69 ±1.00 hrs), while their female partners had higher general PSQI scores (4.44 ±2.31). Out of 282 female partners (mean age = 30.05 ±3.76 years; BMI = 22.28 ±3.46 kg/m2), 267 completed assisted reproductive technology- embryo transfer (ART-ET) cycles and retrieved 7.95 ±3.85 oocytes. Consequently, embryo transfer failed in 15 (5.32%) cases, and 18.79% (53/282) couples reported a primary diagnosis of male factor infertility.
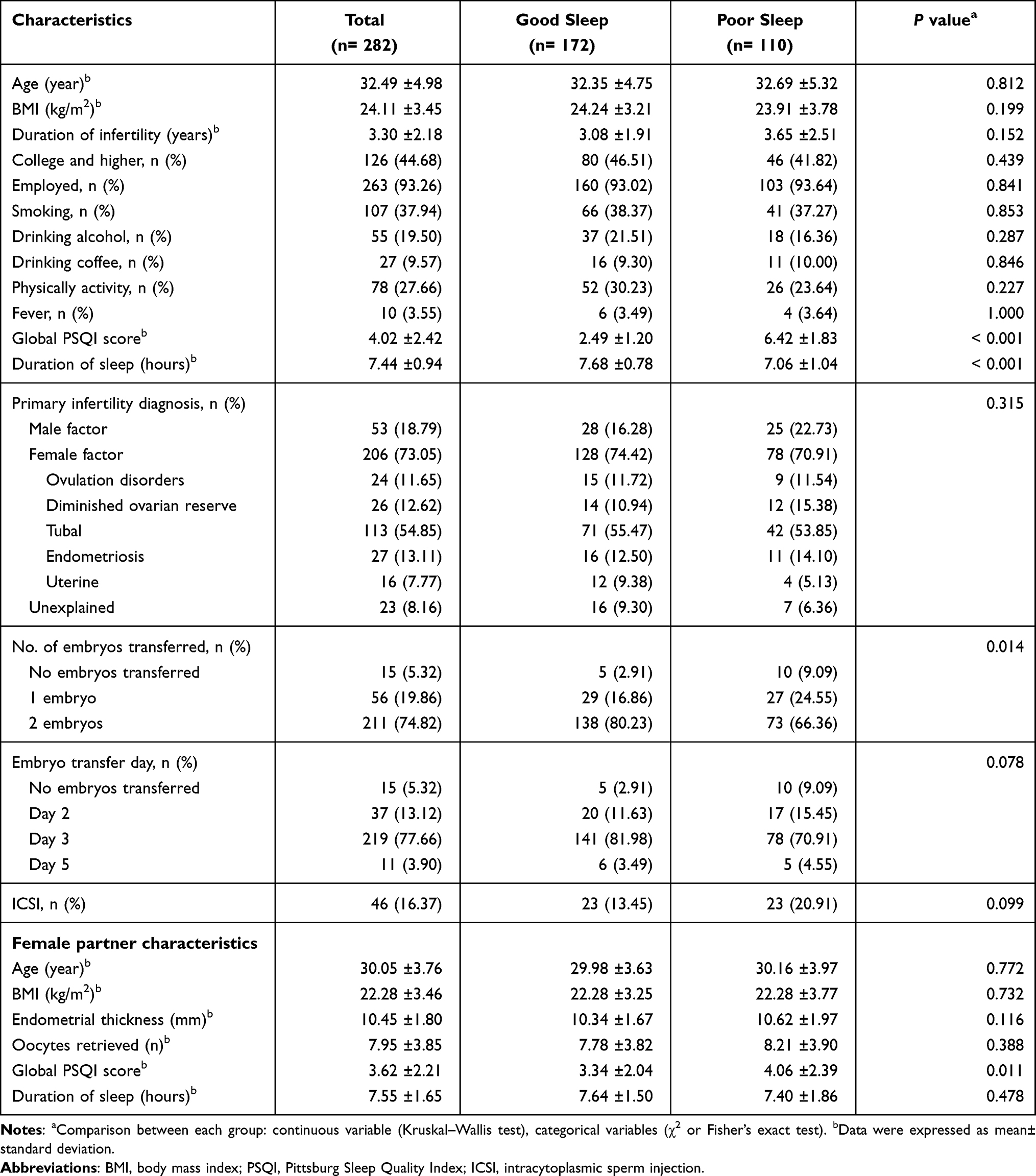 |
Table 1 Demographic and Reproductive Characteristics of Study Populations |
Table 2 shows the laboratory and clinical outcomes of ART for both groups. The comparison showed that the fertilization rate (60.13%) of the poor sleep group (PQSI≥ 5) participants was significantly lower than those in the good sleep group (PQSI< 5) (67.36%) (P = 0.001). In Table S2, we re-grouped according to PSQI>5 as cut-off, the poor sleep group (PSQI> 5) had a significantly lower fertilization rate (55.01%) when compared with the good sleep group (PSQI≤ 5) (67.22%)(P < 0.001). However, there was no statistically significant difference between the two groups in good quality embryos rate, implantation rate, positive pregnancy rate, clinical pregnancy rate, live birth rate, miscarriage rate, and birth weight.
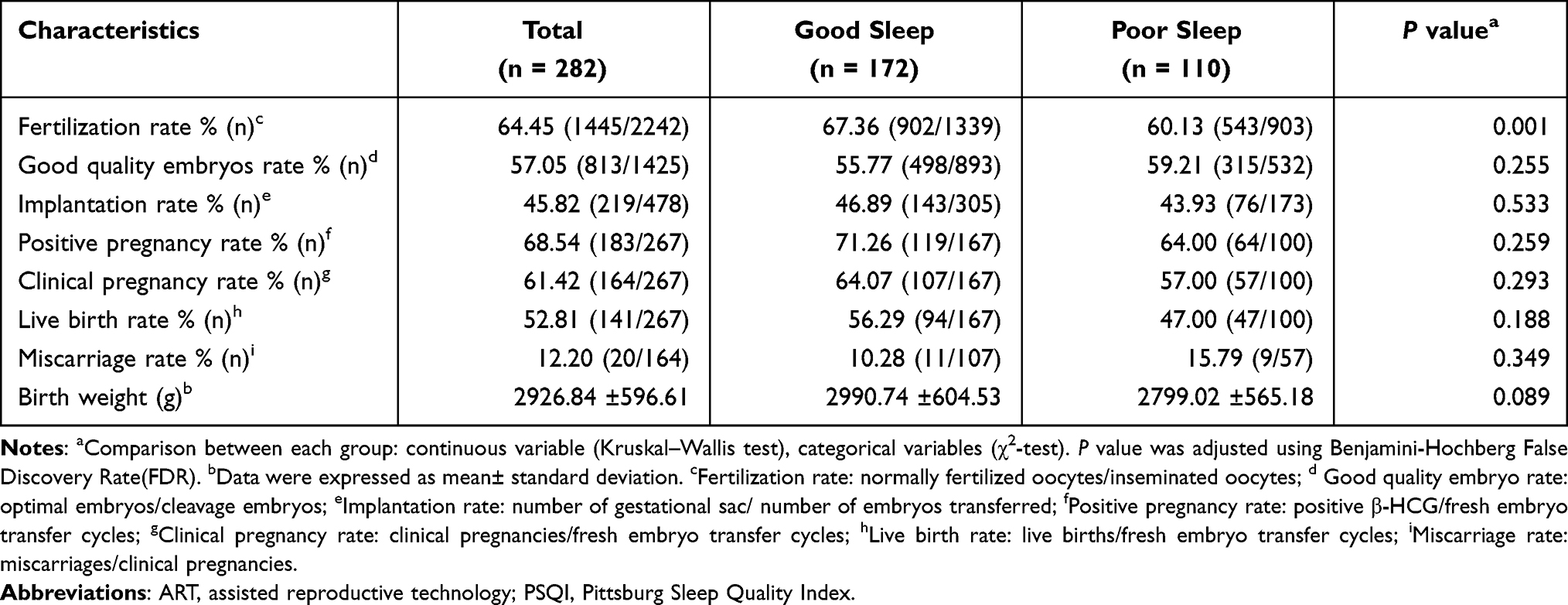 |
Table 2 Laboratory and Clinical Outcomes of ART in Each Group According to the Paternal Global PSQI Scores |
Regression analysis is shown in Table 3. In crude analyses, linear regression analysis illustrated that the global PSQI score had a negative influence on fertilization rate (β, −1.43; 95% CI, −2.67- −0.19; P = 0.045), and birth weight (β, −55.08; 95% CI, −104.70- −5.46; P = 0.045) (Figure 2A and C). After adjustment for confounders, the global PSQI score had a negative influence on birth weight (β, −63.81; 95% CI, −119.91- −8.52; P = 0.047). Moreover, binary logistic regression analysis demonstrated that the global PSQI score was negatively associated with the live birth (OR, 0.88; 95% CI, 0.78- 0.99; P = 0.047) (Figure 2D). In addition, we observed an inverse association between poor sleep group (PQSI≥ 5) and the fertilization rate, both before and after the adjustments. In Table S3, we also found the same conclusion, although we grouped according to PSQI>5 as cut-off. In contrast, regression analysis found no relationship between sleep quality and good quality embryos rate, positive pregnancy, clinical pregnancy, and miscarriage.
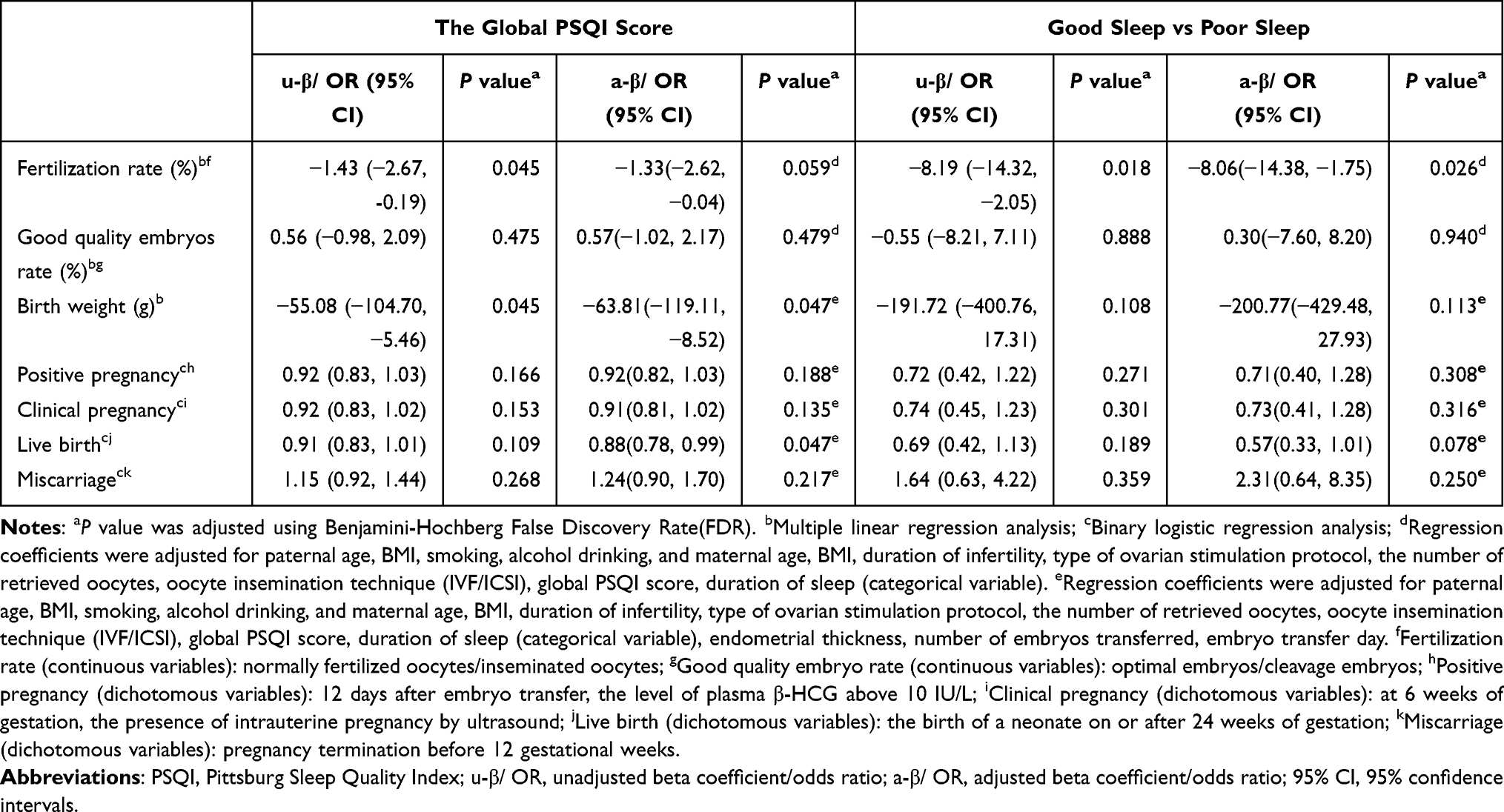 |
Table 3 Linear and Logistic Regression Analysis of the Association Between the Paternal Sleep Quality and Laboratory and Clinical Outcomes |
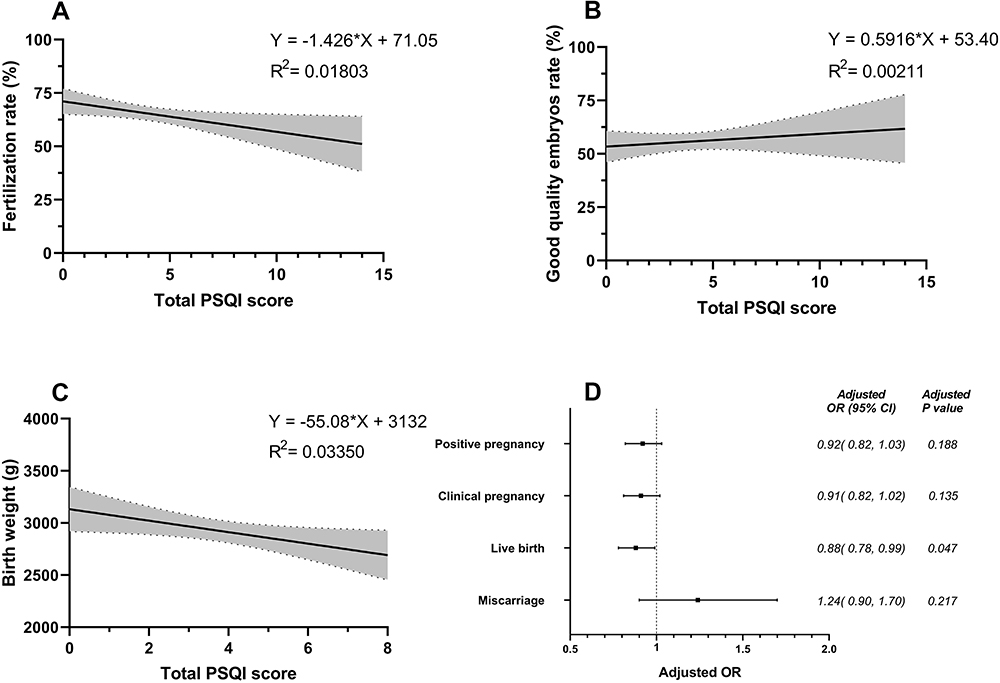 |
Figure 2 The paternal total PSQI score and ART outcomes. (A-C) respectively illustrate the linear regression analysis result between the global PSQI score and fertilization rate (N= 281), good quality embryos rate (N= 272); and birth weight (N= 141). The black line indicates the linear regression result, and the shaded area represents the 95% confidence interval. (D) shows the logistic regression analysis results between the global PSQI score and positive pregnancy (N= 183), clinical pregnancy (N= 164), live birth (N= 141), and miscarriage (N= 20). Abbreviations: PSQI, Pittsburg Sleep Quality Index; ART, assisted reproductive technology; OR, odds ratio; 95% CI, 95% confidence intervals. |
Discussion
We retrospectively assessed the relationship between men’s sleep quality and treatment outcomes in their partners who underwent ART. We found that a higher global PSQI score was related to lower fertilization rate, birth weight, and live birth rate. However, men’s subjective sleep quality was unrelated to good quality embryos rate, implantation rate, positive pregnancy rate, clinical pregnancy rate, or miscarriage rate.
Previous studies mostly focused on the potential effect of sleep quality on male reproduction and its relation with semen quality. We found that men with poor sleep quality had fewer spermatozoa with lower motility and lower normal sperm morphology than men who slept well.16 However, sleep quality was unrelated to ejaculate volume in a cross-sectional analysis among men from the Reproductive Medicine Center in Zhejiang. Chen HG et al17 studied the sperm samples from 842 healthy potential sperm donors and reported that poor sleep quality was associated with lower total sperm count, total motility, and progressive motility. Furthermore, Jensen et al28 reported that sleep disturbance was negatively related to sperm concentration, total sperm count, and percentage of normal sperm morphology in a 953 Danish men’s case-control study. These three findings are in accordance with our analysis and infer strong associations between sleep quality and semen quality.
This study illustrates an inverse relationship between the global PSQI score and outcomes in ART cycles and supports the previous reports of a negative association between the general PSQI scores and sperm morphology.16 Such a relationship was expected since sperm morphology is associated with ART outcomes.29 However, whether sleep quality has an impact on semen quality has yet to be elucidated.
Notably, few previous studies have evaluated the association between men’s sleep and infertility treatment outcomes. Interestingly, a study examined the association between male sleep and fecundability ratios (FRs) in a population-based cohort of 1176 couples who were attempting to conceive without using contraception or fertility treatment.21 In this study, multivariable-adjusted FRs for participants with <6 hours of sleep per night were 0.62 (95% CI 0.42–0.87) when compared to peers with 8 hours of sleep per night. This study reached a similar conclusion as our findings, that is, compared with men who had no trouble sleeping, the FRs for men who had difficulty sleeping less than half the time was 1.06 (95% CI 0.85–1.31), and the FRs for men who had trouble sleeping more than half the time was 0.93 (95% CI 0.72–1.20).
The mechanisms by which poor sleep quality can reduce male fertility remain unclear. Several studies support the testosterone hypothesis; Andersen ML et al, Leproult R et al, and Jankowski KS et al30–32 found that poor sleep quality was associated with lower semen quality and/or lower testosterone levels. However, Jensen et al, Chen Q et al, Du CQ et al, and Morten Ruge et al16,28,33,34 found little connection between sleep quality and testosterone in their studies. The discrepancy in the results from various studies may reflect the complexity of the involved mechanisms. The circadian rhythm system may partially account for our observations. This system, regulated by the solar light and dark cycle, controls vital aspects of our physiology, including body temperature, heart rate, hormone secretion and cellular metabolism.7,35 Therefore, the circadian rhythm plays an essential role in the mature sperm production process.36–39 Unhealthy sleep habits disrupt the expression of circadian rhythm genes and have adverse effects on the male reproductive system.40,41 Since melatonin regulates the sleep-wake cycle of the circadian rhythm, the inhibition of melatonin and cortisol production by endogenous circadian rhythm disorders may cause a disruption of the cycle.42 Additional functions of melatonin include the regulation of gonadotropin and testosterone secretion, promotion of testicular maturation and free radical scavenging, thus preventing testicular injury.43 Therefore, the potential impact of sleep on male fertility deserves further investigation.
This study features a number of notable aspects. Our study was retrospectively designed and used a previously validated PSQI, and the participating couples were followed up during pregnancy until the babies were born. Furthermore, we examined multiple factors that could affect semen quality and ART outcomes, such as paternal age, paternal BMI, smoking, alcohol drinking, and maternal age, maternal BMI, global PSQI score, duration of sleep (categorical variable), duration of infertility, type of ovarian stimulation protocol, the number of retrieved oocytes, oocyte insemination technique (IVF/ICSI), endometrial thickness, number of embryos transferred, and embryo transfer day. Moreover, direct and objective measures of male fertility were selected, including fertilization rate, good quality embryos rate, implantation rate, live birth rate, and miscarriage rate. This is a novel approach that improves on the traditional semen quality parameters to assess male fertility. However, the present research also has some limitations. Firstly, sleep quality is a self-reported subjective indicator, and measurement errors cannot be completely excluded. Secondly, the participants were recruited from a single fertility clinic and were limited in number, raising the possibility of selection bias. Lastly, we only investigated the sleep quality before entering the ART cycle, without dynamically detecting the sleep quality, without considering the influences of anxiety and obstructive sleep apnea (OSA) on sleep quality, and only selected the data of the fresh embryo transfer cycle, which may cause some deviations in the results.
Sleep is closely related to quality of life and mental health. Some researchers have proposed that psychological stress negatively affects sperm parameters.44–46 Furthermore, psychological stress is associated with sleep disturbance and is more common in infertile couples than in fertile couples.47 So, it should be emphasized that the relationship between sleep disturbances and male fertility may be bidirectional. Therefore, it will be interesting to include these confounding factors in future studies. Efforts to improve sleep can also be incorporated into global and individualized preconception care plans for infertile couples.48
Conclusion
In this retrospective study, we present evidence that poor sleep quality is correlated with adverse pregnancy outcomes. This suggests a greater male reproductive potential with better sleep quality. Our study extends the current literature on the relationship between sleep quality and male fertility. In view of the growing global evidence that human semen quality is declining, and poor sleep quality is becoming more common, further research is needed to explore the underlying mechanisms and confirm our findings.
Acknowledgments
The authors are grateful to colleagues from Reproductive Medicine Center of The First Affiliated Hospital, College of Medicine, Zhejiang University for providing direct assistance and constructive suggestions for this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship and publication of this article.
References
1. Brinster RL. Male germline stem cells: from mice to men. Science. 2007;316(5823):404–405. doi:10.1126/science.1137741
2. Kumar N, Singh AK. Trends of male factor infertility, an important cause of infertility: a review of literature. J Hum Reprod Sci. 2015;8(4):191–196. doi:10.4103/0974-1208.170370
3. Sermondade N, Huberlant S, Bourhis-Lefebvre V, et al. Female obesity is negatively associated with live birth rate following IVF: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(4):439–451. doi:10.1093/humupd/dmz011
4. Sermondade N, Faure C, Fezeu L, et al. BMI in relation to sperm count: an updated systematic review and collaborative meta-analysis. Hum Reprod Update. 2013;19(3):221–231. doi:10.1093/humupd/dms050
5. Waylen AL, Metwally M, Jones GL, Wilkinson AJ, Ledger WL. Effects of cigarette smoking upon clinical outcomes of assisted reproduction: a meta-analysis. Hum Reprod Update. 2009;15(1):31–44. doi:10.1093/humupd/dmn046
6. Bin YS. Is Sleep Quality More Important Than Sleep Duration for Public Health? Sleep. 2016;39(9):1629–1630. doi:10.5665/sleep.6078
7. Gentry NW, Ashbrook LH, Fu YH, Ptáček LJ. Human circadian variations. J Clin Invest. 2021;131(16):5347. doi:10.1172/JCI148282
8. Lanza G, DelRosso LM, Ferri R. Sleep and homeostatic control of plasticity. Handb Clin Neurol. 2022;184:53–72.
9. Wang C, Bangdiwala SI, Rangarajan S, et al. Association of estimated sleep duration and naps with mortality and cardiovascular events: a study of 116 632 people from 21 countries. Eur Heart J. 2019;40(20):1620–1629. doi:10.1093/eurheartj/ehy695
10. Domínguez F, Fuster V, Fernández-Alvira JM, et al. Association of Sleep Duration and Quality With Subclinical Atherosclerosis. J Am Coll Cardiol. 2019;73(2):134–144. doi:10.1016/j.jacc.2018.10.060
11. Kim CW, Chang Y, Kang JG, Ryu S. Changes in sleep duration and subsequent risk of hypertension in healthy adults. Sleep. 2018;41(11):638. doi:10.1093/sleep/zsy159
12. Shan Z, Ma H, Xie M, et al. Sleep duration and risk of type 2 diabetes: a meta-analysis of prospective studies. Diabetes Care. 2015;38(3):529–537. doi:10.2337/dc14-2073
13. Palnitkar G, Phillips CL, Hoyos CM, Marren AJ, Bowman MC, Yee BJ. Linking sleep disturbance to idiopathic male infertility. Sleep Med Rev. 2018;42:149–159. doi:10.1016/j.smrv.2018.07.006
14. Caetano G, Bozinovic I, Dupont C, Léger D, Lévy R, Sermondade N. Impact of sleep on female and male reproductive functions: a systematic review. Fertil Steril. 2021;115(3):715–731. doi:10.1016/j.fertnstert.2020.08.1429
15. Goldstein CA, Lanham MS, Smith YR, O’Brien LM. Sleep in women undergoing in vitro fertilization: a pilot study. Sleep Med. 2017;32:105–113. doi:10.1016/j.sleep.2016.12.007
16. Du CQ, Yang YY, Chen J, Feng L, Lin WQ. Association Between Sleep Quality and Semen Parameters and Reproductive Hormones: a Cross-Sectional Study in Zhejiang, China. Nat Sci Sleep. 2020;12:11–18. doi:10.2147/NSS.S235136
17. Chen HG, Sun B, Chen YJ, et al. Sleep duration and quality in relation to semen quality in healthy men screened as potential sperm donors. Environ Int. 2020;135:105368. doi:10.1016/j.envint.2019.105368
18. Shi X, Chan CPS, Waters T, Chi L, Chan DYL, Li TC. Lifestyle and demographic factors associated with human semen quality and sperm function. Syst Biol Reprod Med. 2018;64(5):358–367. doi:10.1080/19396368.2018.1491074
19. Wogatzky J, Wirleitner B, Stecher A, et al. The combination matters–distinct impact of lifestyle factors on sperm quality: a study on semen analysis of 1683 patients according to MSOME criteria. Reprod Biol Endocrinol. 2012;10:115. doi:10.1186/1477-7827-10-115
20. Pokhrel G, Yihao S, Wangcheng W, et al. The impact of sociodemographic characteristics, lifestyle, work exposure and medical history on semen parameters in young Chinese men: a cross-sectional study. Andrologia. 2019;51(8):e13324. doi:10.1111/and.13324
21. Wise LA, Rothman KJ, Wesselink AK, et al. Male sleep duration and fecundability in a North American preconception cohort study. Fertil Steril. 2018;109(3):453–459. doi:10.1016/j.fertnstert.2017.11.037
22. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Colaci DS, Afeiche M, Gaskins AJ, et al. Men’s body mass index in relation to embryo quality and clinical outcomes in couples undergoing in vitro fertilization. Fertil Steril. 2012;98(5):1193–1199.e1191. doi:10.1016/j.fertnstert.2012.07.1102
24. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual Life Res. 2005;14(8):1943–1952. doi:10.1007/s11136-005-4346-x
25. Aloba OO, Adewuya AO, Ola BA, Mapayi BM. Validity of the Pittsburgh Sleep Quality Index (PSQI) among Nigerian university students. Sleep Med. 2007;8(3):266–270. doi:10.1016/j.sleep.2006.08.003
26. Curcio G, Tempesta D, Scarlata S, et al. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol Sci. 2013;34(4):511–519. doi:10.1007/s10072-012-1085-y
27. Benjamini Y, Hochberg Y. Controlling the False Discovery Rate: a Practical and Powerful Approach to Multiple Testing. Int J Med. 1995;57(1):289–300.
28. Jensen TK, Andersson AM, Skakkebaek NE, et al. Association of sleep disturbances with reduced semen quality: a cross-sectional study among 953 healthy young Danish men. Am J Epidemiol. 2013;177(10):1027–1037. doi:10.1093/aje/kws420
29. Zhang K, Zhu W, Fan L, Gong F. [Human normal sperm morphology rate and in vitro fertilization outcome]. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2010;35(7):738–742. Chinese. doi:10.3969/j.issn.1672-7347.2010.07.015
30. Andersen ML, Alvarenga TF, Mazaro-Costa R, Hachul HC, Tufik S. The association of testosterone, sleep, and sexual function in men and women. Brain Res. 2011;1416:80–104. doi:10.1016/j.brainres.2011.07.060
31. Leproult R, Van Cauter E. Effect of 1 week of sleep restriction on testosterone levels in young healthy men. JAMA. 2011;305(21):2173–2174. doi:10.1001/jama.2011.710
32. Jankowski KS, Fajkowska M, Domaradzka E, Wytykowska A. Chronotype, social jetlag and sleep loss in relation to sex steroids. Psychoneuroendocrinology. 2019;108:87–93. doi:10.1016/j.psyneuen.2019.05.027
33. Chen Q, Yang H, Zhou N, et al. Inverse U-shaped Association between Sleep Duration and Semen Quality: longitudinal Observational Study (MARHCS) in Chongqing, China. Sleep. 2016;39(1):79–86. doi:10.5665/sleep.5322
34. Ruge M, Skaaby T, Andersson AM, Linneberg A. Cross-sectional analysis of sleep hours and quality with sex hormones in men. Endocrine Connections. 2019;8(2):141–149. doi:10.1530/EC-18-0548
35. Eckel-Mahan K, Sassone-Corsi P. Metabolism and the circadian clock converge. Physiol Rev. 2013;93(1):107–135. doi:10.1152/physrev.00016.2012
36. Alvarez JD, Hansen A, Ord T, et al. The circadian clock protein BMAL1 is necessary for fertility and proper testosterone production in mice. J Biol Rhythms. 2008;23(1):26–36. doi:10.1177/0748730407311254
37. Beaver LM, Gvakharia BO, Vollintine TS, Hege DM, Stanewsky R, Giebultowicz JM. Loss of circadian clock function decreases reproductive fitness in males of Drosophila melanogaster. Proc Natl Acad Sci U S A. 2002;99(4):2134–2139. doi:10.1073/pnas.032426699
38. Tobback J, Boerjan B, Vandersmissen HP, Huybrechts R. Male reproduction is affected by RNA interference of period and timeless in the desert locust Schistocerca gregaria. Insect Biochem Mol Biol. 2012;42(2):109–115. doi:10.1016/j.ibmb.2011.11.003
39. Peterlin A, Kunej T, Peterlin B. The role of circadian rhythm in male reproduction. Curr Opin Endocrinol Diabetes Obes. 2019;26(6):313–316. doi:10.1097/MED.0000000000000512
40. Boden MJ, Varcoe TJ, Kennaway DJ. Circadian regulation of reproduction: from gamete to offspring. Prog Biophys Mol Biol. 2013;113(3):387–397. doi:10.1016/j.pbiomolbio.2013.01.003
41. Gamble KL, Resuehr D, Johnson CH. Shift work and circadian dysregulation of reproduction. Front Endocrinol (Lausanne). 2013;4:92. doi:10.3389/fendo.2013.00092
42. Eckel-Mahan K, Sassone-Corsi P. Metabolism and the Circadian Clock Converge. Physiological Reviews. 2013;93(1):107–135.
43. Li C, Zhou X. Melatonin and male reproduction. Clin Chim Acta. 2015;446:175–180. doi:10.1016/j.cca.2015.04.029
44. Gollenberg AL, Liu F, Brazil C, et al. Semen quality in fertile men in relation to psychosocial stress. Fertil Steril. 2010;93(4):1104–1111. doi:10.1016/j.fertnstert.2008.12.018
45. Nordkap L, Jensen TK, Hansen ÅM, et al. Psychological stress and testicular function: a cross-sectional study of 1215 Danish men. Fertil Steril. 2016;105(1):
46. Nordkap L, Priskorn L, Bräuner EV, et al. Impact of psychological stress measured in three different scales on testis function: a cross-sectional study of 1362 young men. Andrology. 2020;8(6):1674–1686. doi:10.1111/andr.12835
47. Nargund VH. Effects of psychological stress on male fertility. Nat Rev Urol. 2015;12(7):373–382. doi:10.1038/nrurol.2015.112
48. Dupont C, Aegerter P, Foucaut AM, et al. Effectiveness of a therapeutic multiple-lifestyle intervention taking into account the periconceptional environment in the management of infertile couples: study design of a randomized controlled trial - The PEPCI study. BMC Pregnancy Childbirth. 2020;20(1):322. doi:10.1186/s12884-020-2855-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.