")
Back to Journals » Clinical Interventions in Aging » Volume 15
Menopausal Symptoms and Associated Social and Environmental Factors in Midlife Chinese Women
Authors Zhang L, Ruan X , Cui Y, Gu M, Mueck AO
Received 26 August 2020
Accepted for publication 8 October 2020
Published 16 November 2020 Volume 2020:15 Pages 2195—2208
DOI https://doi.org/10.2147/CIA.S278976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Lingyan Zhang,1 Xiangyan Ruan,1,2 Yamei Cui,1 Muqing Gu,1 Alfred O Mueck1,2
1Department of Gynecological Endocrinology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, Beijing 100026, People’s Republic of China; 2Department of Women’s Health, University Women’s Hospital and Research Center for Women’s Health, University of Tuebingen, Tuebingen D-72076, Germany
Correspondence: Xiangyan Ruan
Department of Gynecological Endocrinology, Beijing Obstetrics and Gynecology Hospital, Capital Medical University, No. 251, Yaojiayuan Road, Chaoyang District, Beijing 100026, People’s Republic of China
Tel +86-13011215678
Email [email protected]
Objective: To investigate the dependency of menopausal symptoms on age and/or menopausal status and association with social and environmental factors.
Methods: The cross-sectional study was conducted on 4595 women (40– 83 years) coming from 31 provinces during two years to our “Menopause Clinic”, the first official center in China. Menopausal symptoms were assessed: negative mood, cognitive symptoms, sleep disorder, vasomotor symptoms (VMS), urogenital symptoms, autonomic nervous disorder, limb pain/paresthesia. Social and environmental factors were collected; simple and unconditional logistic regression with adjustments by all analyzed factors were used to assess associations.
Results: Urogenital symptoms were the most common and VMS the least common complaints. All symptoms, except cognitive and urogenital symptoms, worsened age-dependently up to 60 years but improved beyond this age. Most symptoms also were associated with menopause, except negative mood and autonomic nervous disorders. Soya-rich diet decreased all symptoms, but only if consumed daily. Exercise was beneficial for some symptoms. Hormone replacement therapy (HRT) was most effective but only with regular use. Increased alcohol consumption aggravated VMS. Higher education was associated with less symptoms; no relationship was found for smoking, gravidity, parity, and menarche.
Conclusion: All symptoms, except cognitive and urogenital symptoms, worsened age-dependently up to 60 years but improved beyond this age; most were also associated with menopause. For the first time in a large study population, it was observed that soy-rich diet is protective but only with daily consumption. Exercising can protect against some of the symptoms. HRT decreased all symptoms, but regular use is necessary. Women with higher education reported less symptoms, but after adjustments no other relationships were observed (ChiCTR2000035047).
Key/words: menopausal symptoms, age, menopause, HRT, associated factors
Introduction
Menopause marks the end of a woman’s reproductive life and is caused by reduced secretion of ovarian hormones.1 With increased life expectancy, it is estimated that the number of postmenopausal women worldwide will reach 1.1 billion by 2025.2 Many symptoms have been attributed to menopause, with substantial effects on quality of life.3 Severe vasomotor symptoms (VMS) and sleep disorders might increase cardiovascular risk; severe VMS and depression may affect cognitive function.3 On average, menopausal symptoms appear between age 48 and 55 years of age, with menopausal transition typically lasting four to eight years.4 However, geographical location, ethnicity, education and lifestyle may influence the prevalence of menopausal symptoms.5 Thus, identifying the factors associated with menopausal symptoms, especially those which are modifiable, may be important to reduce the risk of future chronic illness among postmenopausal women. Smoking has been proved to be linked to depressive mood during the menopausal transition.6 However, the effect of other potential factors involving level of education, lifestyle behavior and soya intake on menopausal symptoms has been studied less, with no universal consensus, and only a few studies have been conducted in Chinese women. In this study, we observed how menopausal symptoms change with age and menopausal status, and examined the association between menopausal symptoms and socio-demographic and environmental factors including treatment possibilities in a large population of midlife women coming from 31 provinces of China to one center, specialized in menopausal issues.
Participants and Methods
Patients and Study Design
This cross-sectional study to analyze baseline information was conducted at the Department of Gynecological Endocrinology in the Beijing Obstetrics and Gynecology Hospital, Capital Medical University, China. In total, 4595 outpatient women who visited our new “Menopause Clinic Center” because of menopausal concerns over a 24-month period met the inclusion and exclusion criteria of a validated questionnaire survey and all attended standardized menopausal examinations, including 2407 perimenopausal (52.38%) and 2188 postmenopausal women (47.62%).
All participants provided written informed consent according to the Declaration of Helsinki, and the study was approved by the Ethics Committee of the Beijing Obstetrics and Gynecology Hospital, Capital Medical University, China (2020-KY-008-01).
Inclusion and Exclusion Criteria
Women were included based on the “2011 Stages of Reproductive Aging Workshop (STRAW+10) staging system”7 Inclusion criteria: (1) Perimenopause: irregular menstrual cycles, with/without perimenopausal symptoms, (2) Postmenopause: ≥12 consecutive months without spontaneous menstruation, or bilateral ovariectomy ≥6 weeks before enrollment (with or without hysterectomy), FSH >40IU/L.
Exclusion criteria: (1) prior/current DSM-5 depression, anxiety, sleep or circadian disorders (other than insomnia), Alzheimer’s disease and other mental illness diagnosed by a neurologist; (2) heart disease, (3) Meniere’s disease; (4) joint pain caused by systemic lupus erythematosus or rheumatoid arthritis.
Assessment of Basic Characteristics, Exposure Variables and Menopausal Symptoms
Certified medical staff collected information on general socio-demographic data using a laptop-based questionnaire (age, nationality, district, marital status), dietary habits (especially consumption of soya products), lifestyle (daily exercise, alcohol, smoking), level of education, HRT, and reproductive characteristics (age at menarche, gravidity, parity). In addition, body weight, height and BMI were assessed, and physicians performed the usual routine examinations before starting any therapy.
A validated research database8–10 was used containing questions with seven domains: negative mood, cognitive symptom, sleep disorder, VMS, urogenital symptom, autonomic nervous disorder, limb pain/paresthesia, and each domain included several specific items with more detailed questions. Our results (see supplementary materials) show excellent internal consistency of this online questionnaire and high criterion validity (Cronbach’s alpha=0.960, Guttman split-half coefficient=0.852) (KMO=0.961, p<0.001; cumulative %=54.994%). Each question was answered on a 0–4 level of severity: none/little, mild, moderate, and severe (corresponding score 0–3). For example, Women were asked if they had been bothered by hot flashes and/or sweating over the previous 2 weeks, and were requested to classify severity (no, light, moderate and heavy, respectively) and frequency (no, 2 times/day, 3–9 times/day, 10 times/day) with a corresponding score of 0–3, which is the same as improved Kupperman Index. The sum of each item divided by the number of items in each domain was defined as one subject’s domain-specific mean value. Similarly, all the subjects’ mean values are the sum of all subject’s domain-specifics divided by the number of subjects. Thus, higher mean scores are indicative of more severe symptoms. Most patients answered the questions themselves, but also could ask a doctor if help was required.
Statistical Analysis
Statistical analysis was performed using SPSS 22.0. Normality of distribution was assessed with the one-sample Kolmogorov–Smirnov test. Normal distributed data were presented as the mean standard deviation (SD). The menopausal symptoms were described with mean (M). Age and BMI between the two groups were performed with T test; nationality, district, HRT, marital status between the two groups were compared using the chi-square test; level of education between the two groups was compared by rank sum test. Simple and unconditional logistic regression were used to assess the relationship between menopausal symptoms and potential confounding factors with odds ratios (OR) and their 95% confidence intervals (CI) with adjustments by all analyzed factors were reported. A p-value of <0.05 was considered to be statistically significant.
Results
Demographic and Menopausal Characteristics of Subjects
The demographic and menopausal characteristics of the subjects are presented in Table 1 comparing perimenopausal and postmenopausal women. Age, level of education, marital status and use of HRT differed significantly between the two groups. There was no significant difference in nationality, district, and BMI between the two groups. Among them, 28% (1307) used HRT at least for six months, the number of hysterectomized women is 215 (16.45%), these women have been treated with estrogen-only, whereby we used oral estradiol, or oral estradiol valerate or transdermal estradiol (patch or gel).
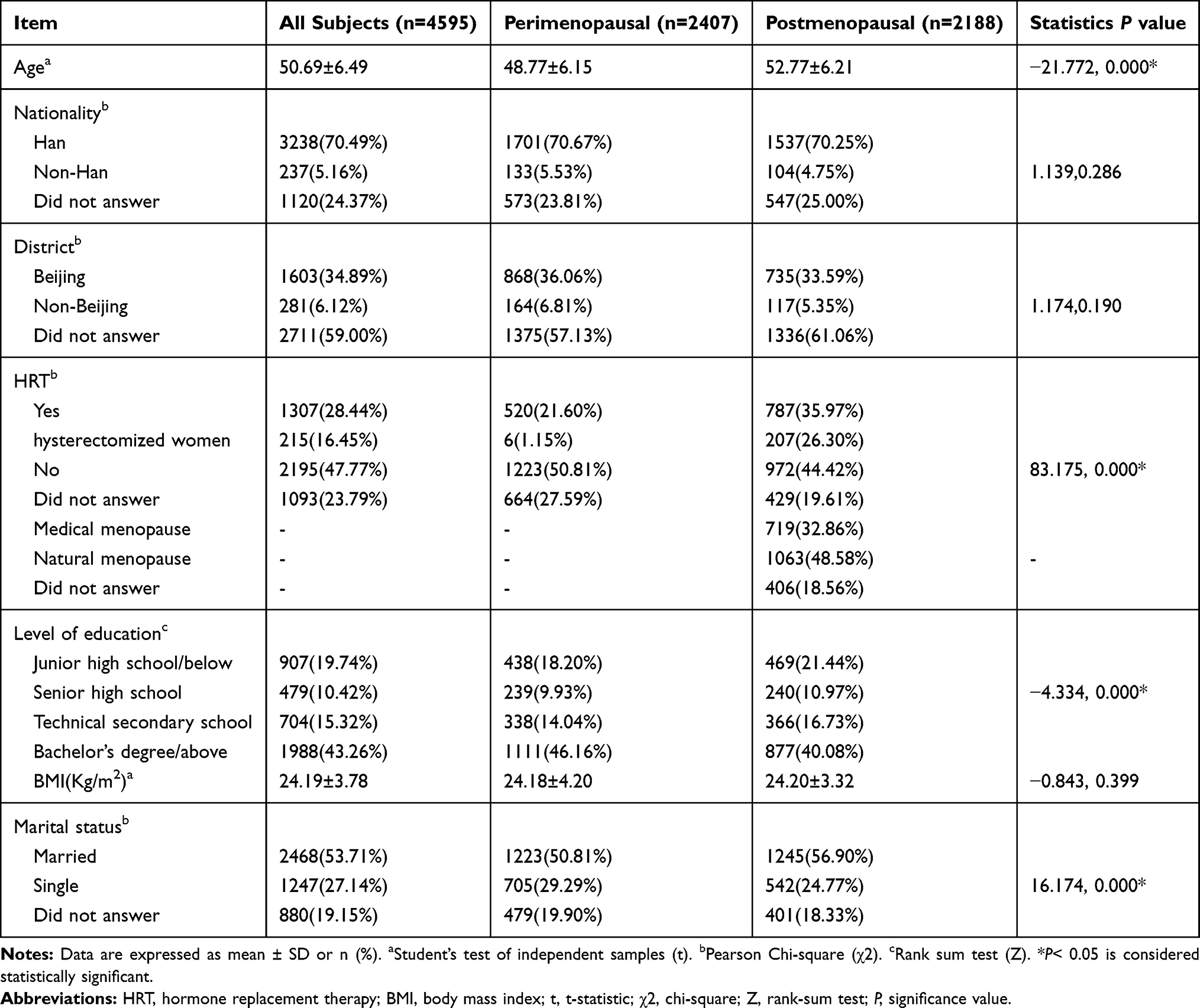 |
Table 1 Demographic Characteristics of Perimenopausal and Postmenopausal Women (n=4595) |
Prevalence of Menopausal Symptoms Comparing Perimenopausal and Postmenopausal Women
As shown in Figure 1, the prevalence of urogenital symptoms was the highest (97.92%) and VMS was the lowest (48.83%) within our patient sample.
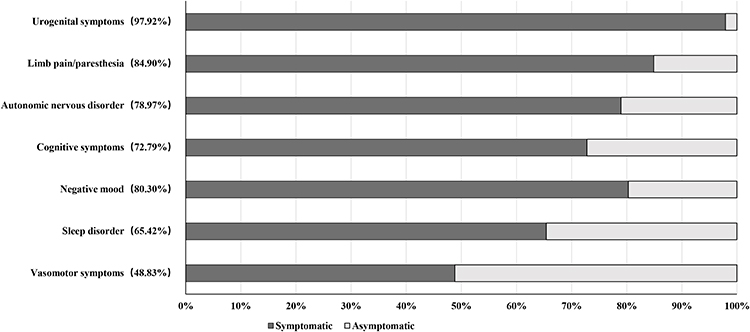 |
Figure 1 Prevalence of menopausal symptoms in midlife women (n=4595). |
Changes in Menopausal Symptoms with Age
The severity of menopausal symptoms increased with age as shown in Figure 2, but decreased after 60 years of age, with the exception of cognitive and urogenital symptoms. However, because there were only 313 women ≥60 years of age, the results in this age-group are not robust.
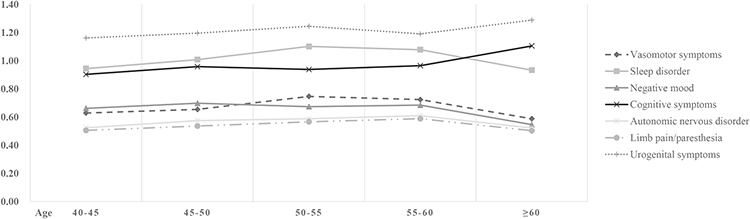 |
Figure 2 Dependence of the severity of the domain menopausal symptoms on age (n=4595). |
Risk Factors for Menopausal Symptoms
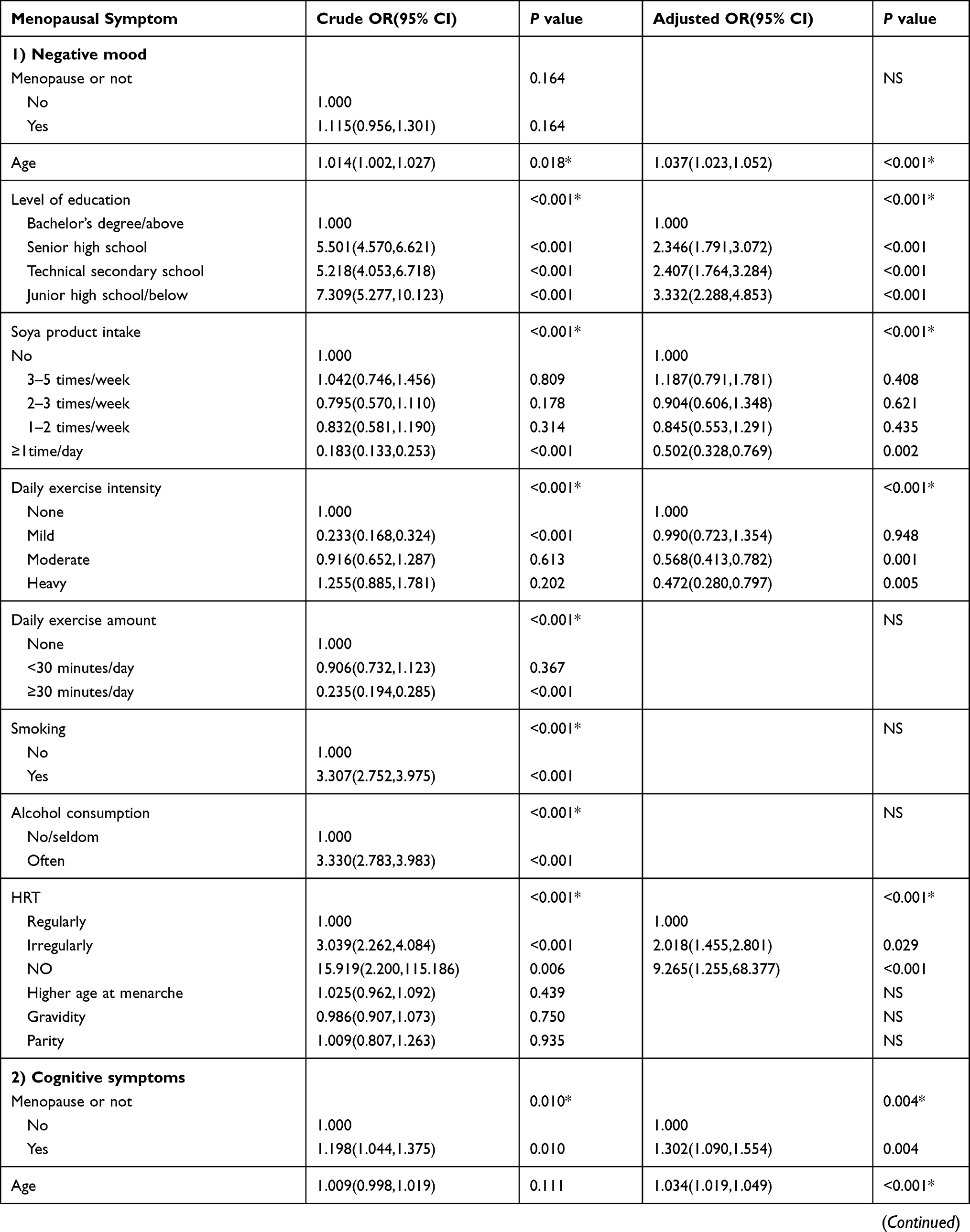
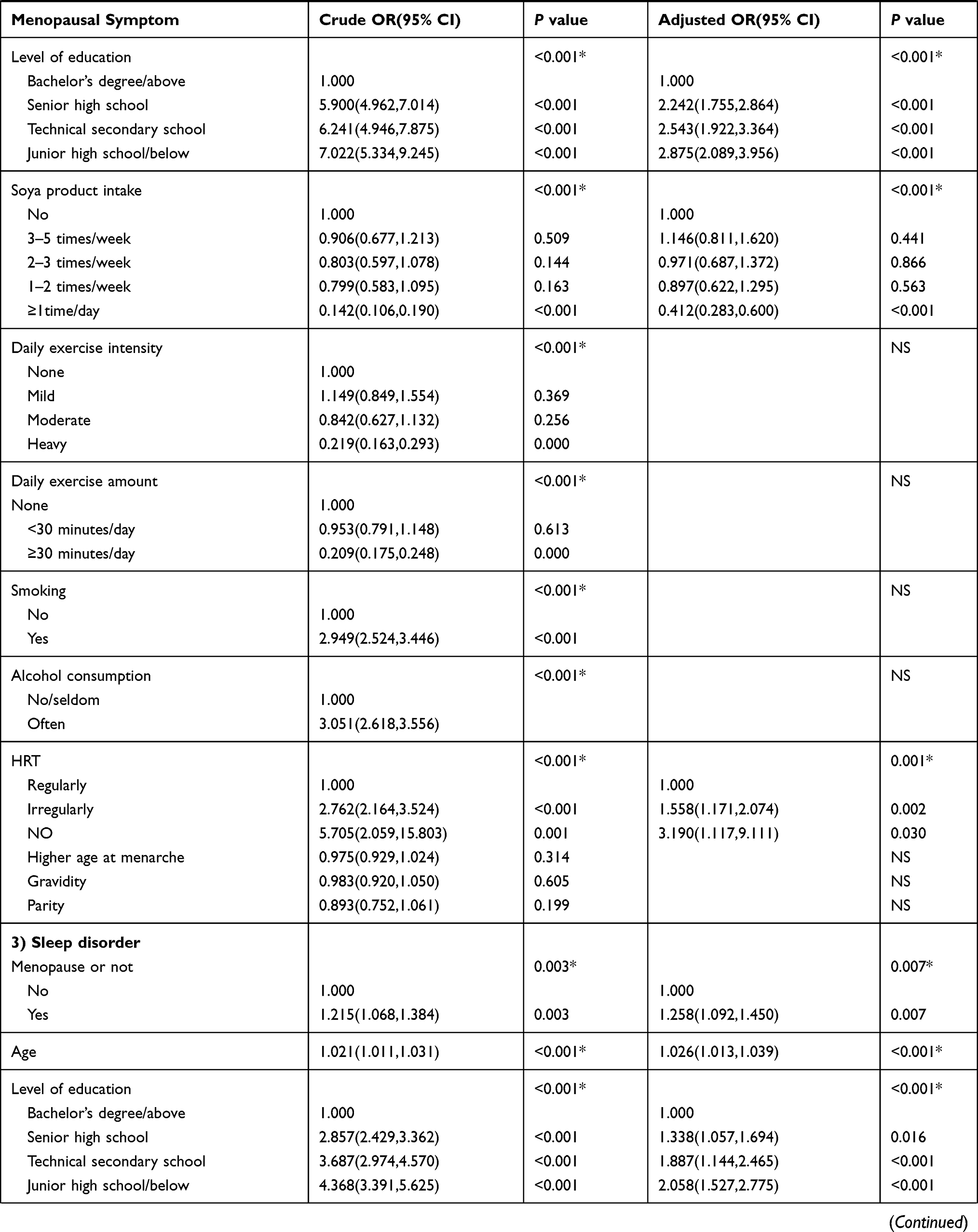
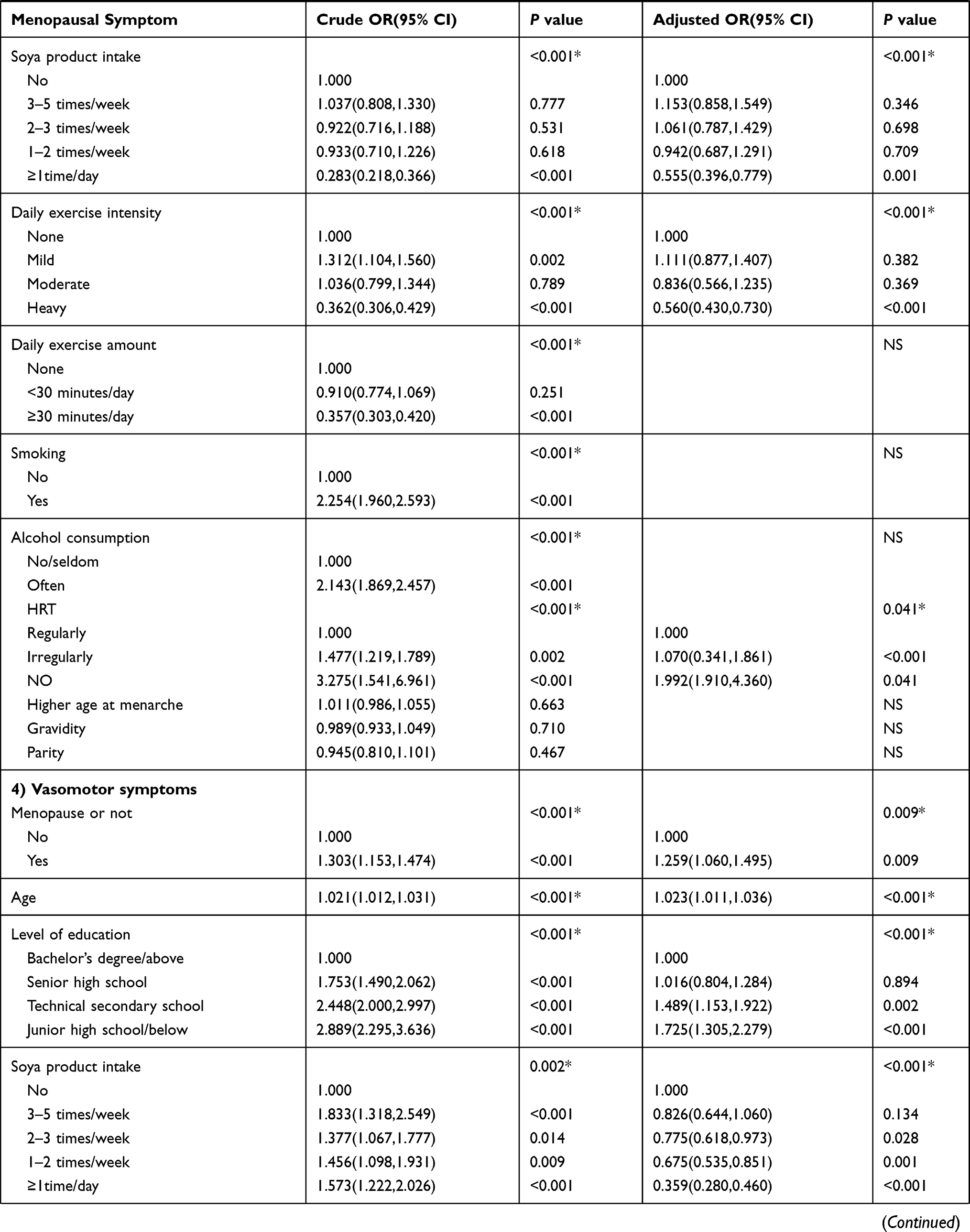
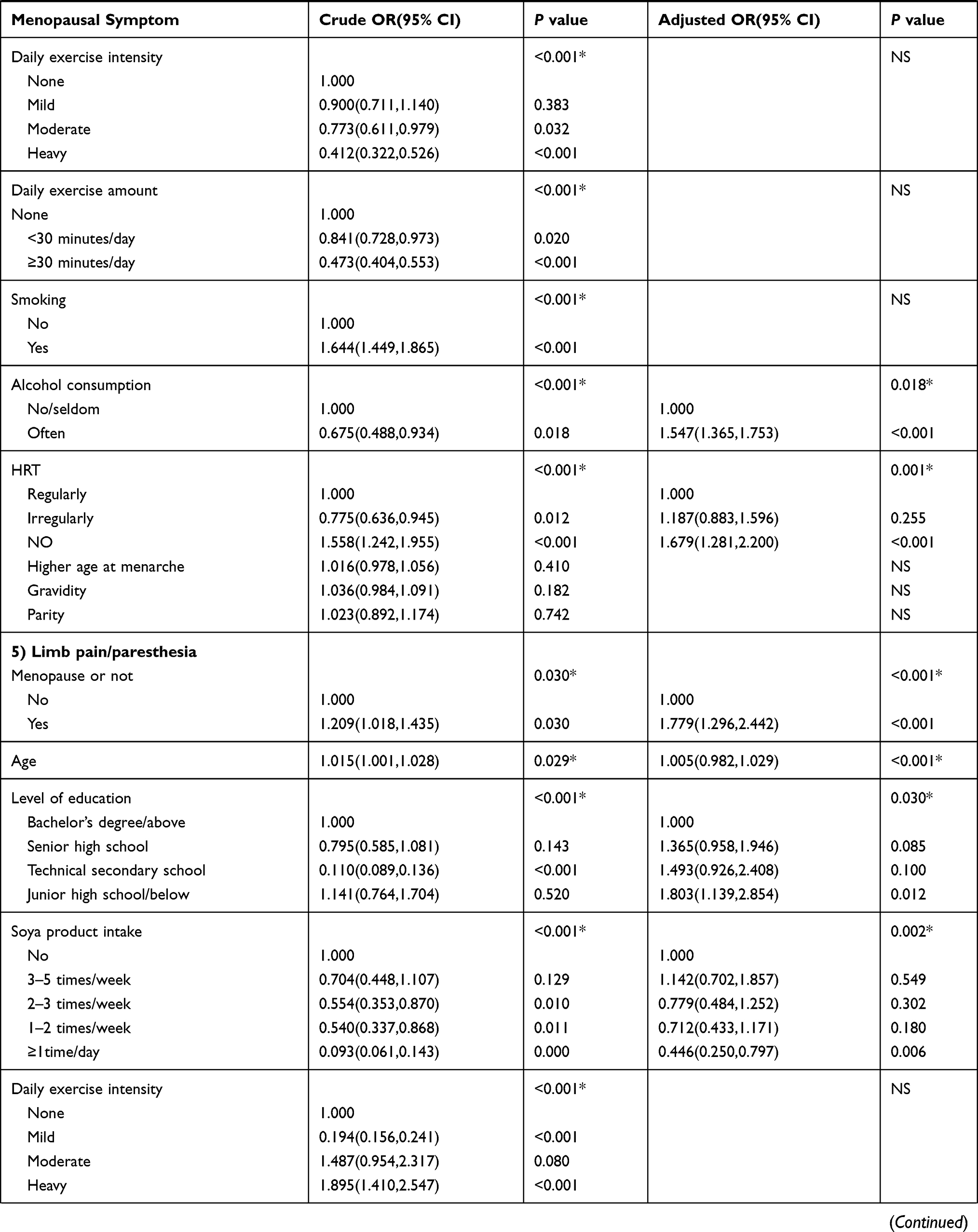
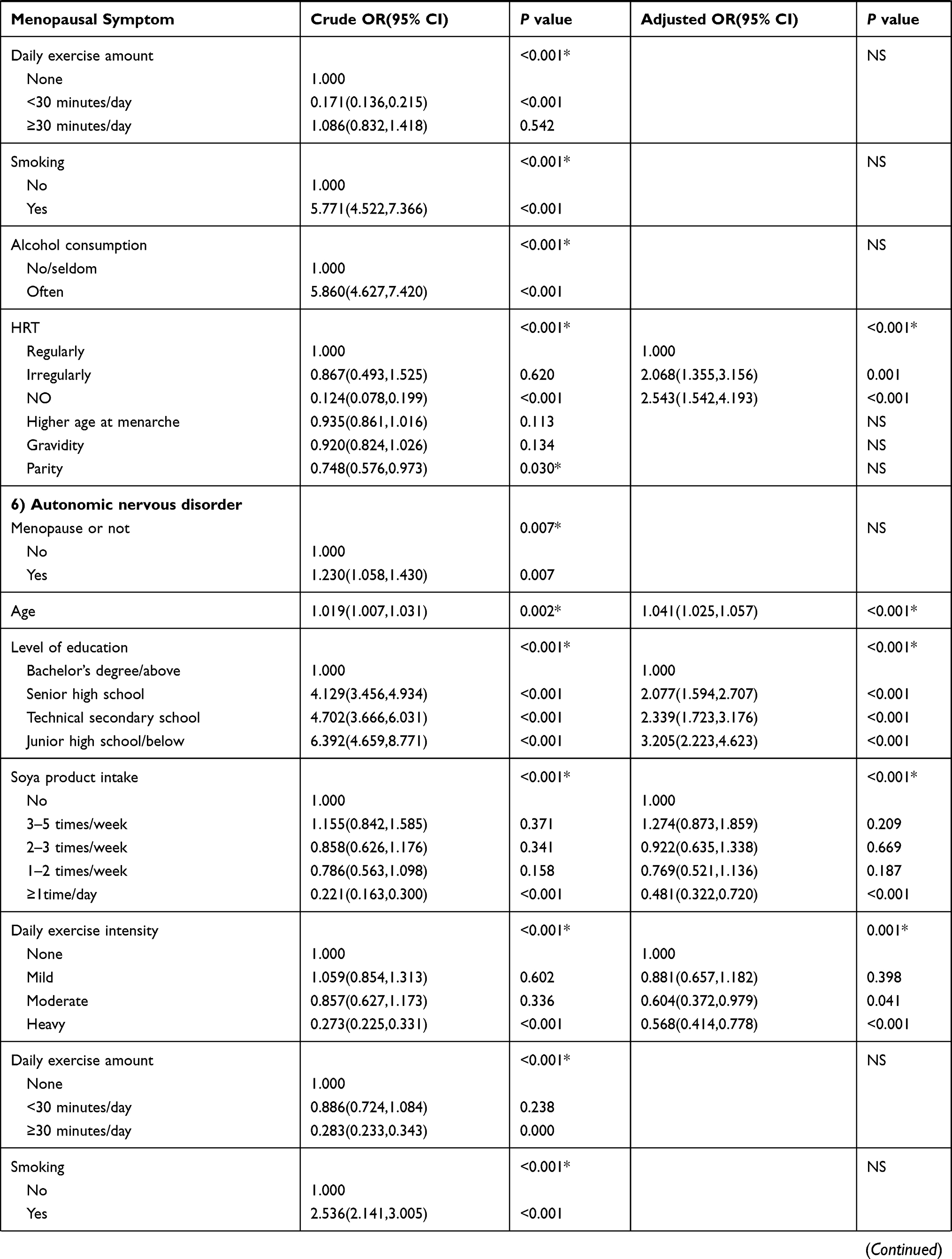
The associations between menopausal symptoms and age, menopausal status, level of education, daily exercise intensity, daily exercise, smoking, alcohol consumption, menarche, gravidity and parity, HRT and consumption of soya products are presented in Table 2 as crude odds ratio (OR) and adjusted OR. The adjustment was made for each analyzed factor for all items. Because of the very large number of women with urogenital symptoms, there was a lack of control for analyzing multiple regression risk factors with urogenital symptoms; therefore, these complaints are not included in Table 2.
 |
 |
 |
 |
 |
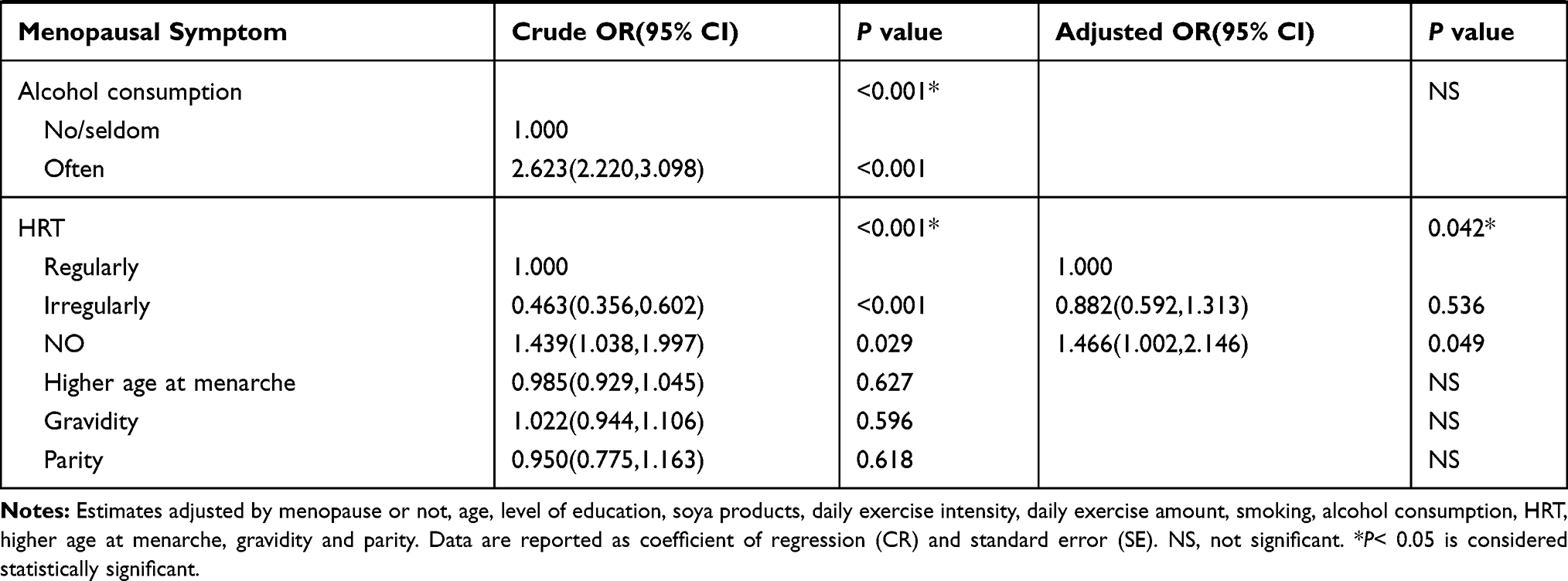 |
Table 2 Factors Influencing Menopausal Symptoms Analyzed by Simple and Unconditional Logistic Regression Analysis (n=4595) |
Besides the relationship to age (Figure 2), menopausal symptoms also were dependent on menopause, except negative mood and autonomic nervous disorders, which only showed an age-dependent increase (up to 60 years). Proper physical activity was beneficial for controlling negative mood, insomnia, and autonomic nervous disorders, but showed no significant association with VMS, cognitive symptoms and limb pain/paresthesia.
A soya-rich diet could decrease all symptoms, but daily consumption was needed, and less than daily intake was not effective for any symptom. Likewise, HRT could decrease all symptoms, but regular use with daily administration for at least 6 months was necessary. Regarding the association with other factors, only a higher level of education was positively associated with decreased odds of menopausal symptoms. Current smoking, gravidity and parity showed no relationship, but we found that increased alcohol consumption could aggravate VMS.
Discussion
This is the largest cross-sectional study in Chinese women coming from all over China to one specialized center to evaluate menopausal symptoms and their variability with age and menopausal status, and to comprehensively assess their relationship with various social and environmental factors which could have an effect on menopausal complaints. Possible associations were assessed after rigorous multiple adjustments of all analyzed factors.
Prevalence of Menopausal Symptoms and Dependency on Menopausal Status
All symptoms, except cognitive and urogenital symptoms, worsened age-dependently up to 60 years, but improved beyond this age and most, but not all, were also dependent on menopausal status, ie, with different risk in women who had experienced menopause. Regarding the time of menopausal transition, a meta-analysis of 36 studies evaluating age at natural menopause reported an overall mean of 48.8 years, with a range of 46 to 52 years.11 Menopausal symptoms usually begin four to six years before cessation of menses.12
One of the main results of our study is that urogenital symptoms had the highest prevalence (97.9%) (Figure 1). The lowest prevalence was found for VMS (48.8%). This is in sharp contrast to the literature concerning menopausal women in most Western countries, where up to 75% present with VMS as the main complaints.13 Similar to reports from Western countries, the prevalence of negative mood in midlife women was also very high in our study (at 80.3%) and was the third most common symptom after urogenital complaints and limb pain/paresthesia (84.9%), beginning during menopausal transition and persisting beyond 60 years of age.
An increased risk of negative psychological symptoms during menopausal transition, such as anxiety and emotional distress, has been observed in many studies such as SWAN14 and the Seattle Midlife Women’s Health Study.15 Furthermore, about 30% of women in SWAN experienced a worsening of depressive mood.14 The risk of depressive symptoms and impairment of cognitive performance were significantly higher in women during the menopausal transition, with a lower risk after the final menstrual period (FMP).16 However, in our previous study, we found that the prevalence and severity of depression was significantly higher in postmenopausal compared to perimenopausal women,17 so there may be differences between study populations.
The SWAN study reported cognitive performance impairment during the menopausal transition, with subsequent improvement to premenopausal levels in the postmenopausal period.18 However, in our study, decreased cognitive performance began during menopausal transition, lasted up to the age of 60 and then worsened during the following years.
Sleep difficulties often begin during menopausal transition, and the prevalence increases in post-menopausal life (31% vs 40%-56%).19 This is in line with our previous study, where we found that the prevalence and severity of insomnia was significantly higher in postmenopausal compared to perimenopausal women.17 In the present study, complaints about insomnia also started in the menopausal transition and increased after menopause to a prevalence of 65.4%.
One study revealed that VMS can begin as early as two years before the FMP, peaks one year after the FMP and tapers off within a median time of 7.4 years in approximately half of women.20 Approximately 12% of women will continue reporting symptoms as long as 11–12 years after the FMP.21 In our study, VMS started during the menopausal transition and persisted even beyond the age of 60.
Women exhibit a decrease in sexual desire and an increase in painful intercourse beginning in the late perimenopause.22 It was found that sexual dysfunction showed a steep decline in women 46 to 48 years of age, partly increased in the 49 to 51 years age group and declined at age 52 to 55 years.23 In our previous study, we found that the prevalence and severity of sexual dysfunction was significantly higher in postmenopausal compared with perimenopausal women.17 In our present study, we did not differentiate between urogenital symptoms and sexual dysfunction, ie, both symptoms were collected within the same group. We found that urogenital symptoms started during menopausal transition, increased in the 50–55 years age group, and further worsened after 60 years of age. To obtain more insight regarding the prevalence of sexual function would require more sophisticated evaluations, such as the use of special validated scores.
Women in different stages of reproductive life may have altered autonomic nervous system (ANS) function due to the different hormonal environment.24 The ANS plays a key role in all cardiac regulatory mechanisms, exerting a tonic and reflexive influence on the main variables of the cardiovascular system, and an imbalance in ANS functioning leads to disease and mortality.25 Estradiol is cardio-protective, associated with higher vagal activity and lower sympathetic nervous system (SNS) activity.26 Progesterone is associated with higher SNS activity.27 Therefore, not only dependency on age (Figure 2), but also dependency on the menopausal status should be expected, which, however, was not the result in our study (Table 2). However, in general, data on the issue of ANS are very rare and need more research. To our knowledge, our results are the first to be published using a large population.
Social and Environmental Factors Influencing Menopausal Symptoms
Regarding the possible etiology of menopausal symptoms, hormonal changes are well known to be responsible for these symptoms in type and severity,17 as also published by our group elsewhere.17 However, little is known about the relationship between menopausal symptoms and socio-demographic data, lifestyle, and dietary changes. Since BMI has been found to be positively related to the intensity of menopausal symptoms,12 lifestyle and dietary changes may elicit indirect negative effects. Our study did have a relatively low BMI (24) in contrast to most Western studies, so the results of our study may not be extrapolated to other studies. Indeed, this should be also an argument, that it is necessary to perform studies especially for Chinese women, despite similar studies may already exist in Western world. There is increasing evidence that socio-demographic and environmental factors including childhood nutrition, disease exposure, energy expenditure, parity and smoking habits may exert a tremendous influence on menopausal symptoms.9 The menopausal symptoms which we investigated in our study regarding possible associations are listed in Table 2, in terms of the different influencing factors and “crude” and adjusted OR values.
From our results it is notable that women with a higher level of education are less likely to have menopausal symptoms, in line with previous studies.28 Level of education is suggested as being a good indicator of socio-economic status and may affect menopausal symptoms by physiological effects on lifestyle behavior and reproductive health.29 However, it may also be that women with higher education simply better cope with their VMS, for example by avoiding drinking too much coffee and alcoholic beverages and using suitable clothing.
Regular exercise can mitigate some menopausal symptoms and improve sleep quality.30 In our study, we found protective effects on negative mood, insomnia, and autonomic nervous disorders, but no significant association with VMS, cognitive symptoms and limb pain/paresthesia. There may be some explanations for these negative results: Regarding VMS, it was demonstrated that increased physical activity leading to increased sweating and higher body temperatures is associated with higher rates of VMS.3 Regarding cognitive performance, it was hypothesized that there may be neuroprotection mediated through brain-derived neurotrophic factors and reduction of pro-inflammatory cytokines,31 or reduction in cardiovascular risk through exercise may have a general health benefit.32 However, in a randomized controlled trial, the effect of physical exercise on cognition was largely negative,33 consistent with our results. Regarding limb pain/paresthesia, high-intensity exercise can induce collagen growth, but may also cause injuries to tendons and other soft tissue.34
Despite these negative results in our study and in other studies, adequate physical activity should be recommended also for menopausal women since it undoubtedly has many beneficial effects, not only for decreasing some of the menopausal symptoms, but particularly for postural stability, prevention of cardiovascular and bone disease.
Hormone replacement therapy (HRT) is well known to be the most effective way of relieving menopausal symptoms and preventing or reducing the occurrence of various chronic diseases.35,36 However, because of risks such as breast cancer and thromboembolic diseases, patients and many doctors dislike using HRT or do not use HRT on a regular basis. Our study showed a decrease in all menopausal symptoms with HRT, which also clearly confirms that if there is a decision for HRT, it should be used at least for six months every day (Table 2) to achieve the benefits of estrogen replacement.
For patients with contraindications for HRT or who refuse hormonal therapy, there is broad consensus that soya products (eg, isoflavones in tablets) can be used because they contain phytoestrogens.37 However, our study shows that if using a soya-rich diet, daily consumption is necessary to improve symptoms. Consumption only 2–3 times/week was mostly not effective (Table 2). To our knowledge, this was shown here for the first time in a large population study. To explain the different results of studies from Western countries, it must be considered that the amount of isoflavones in the normal Chinese diet (about 200 mg/day) is much higher than in “food supplements” offered in pharmacies (50 mg/day).37
It should be mentioned that we use instead of HRT also tibolone particularly in women with sexual complaints or negative mood, because of the well-known additional androgenic effects due to the progestational metabolite and because SHBG is decreased. Besides soy, we use alternatives for the treatment of VMS like hot flashes, especially if HRT is contraindicated, with good experience using black cohosh for example in patients with breast cancer history. About this, we have published elsewhere.38
Regarding a possible association between menopausal symptoms and other related factors, which were investigated in our study, we found that current smoking, gravidity, parity, and menarche are not related to menopausal symptoms. We only found that alcohol consumption (≥3times/week) could aggravate VMS. This is in line with the results of Freeman et al, who found a significant positive association between alcohol intake and hot flashes.38 However, the results in the SWAN study did not detect any effects of alcohol consumption on VMS.39
This and other differences can be explained as we performed simple and unconditional logistic regression methods with rigorous adjustment of all analyzed factors, with the consequence that we obtained similar results to other studies for some of those single factors in the “Crude OR”, ie, significant relationships, but not after multiple adjustments.
Conclusion
All symptoms, except cognitive and urogenital symptoms, worsened age-dependently up to 60 years, but improved beyond this age, the strongest effect being the prevalence and severity of urogenital complaints. The prevalence of most menopausal symptoms, except negative mood and autonomic nervous disorders, is also dependent on the menopausal status, ie, increasing in postmenopausal compared to perimenopausal patients. Complex relationships with social/environmental factors may explain the fact that after rigorous adjustments, we only found an association between a higher level of education and less menopausal symptoms, and increase in VMS in women with increased alcohol consumption, but no relationship with age at menarche, gravidity, parity and smoking. Regular exercise was beneficial only for some of the symptoms, but it is recommended for maintaining general health. As expected, HRT can decrease frequency and severity of all complaints investigated in our study, but must be used regularly. Nutritional soya products are an effective alternative, but only with daily consumption. We should pay more attention to diet and lifestyle, as this may contribute to the control of menopausal symptoms.
Strengths and Limitations
To our knowledge, this is the largest cross-sectional study on menopausal symptoms and associated social and environmental factors in midlife Chinese women. Because the women came from 31 provinces, the results should be credible throughout China. It also is a strength that all women were patients from one center where data were collected and all clinical examinations were performed, and that this center is specialized in the field of menopause, being the first “Menopause Clinic Center” in China to be officially acknowledged by the health authorities.
Limitations are that there may be selection bias suggesting that more women with symptoms would come to our hospital and participate in this study. Another limitation is that our results are based on the baseline data of a prospective cohort study, more robust results need long-term follow-up. Another limitation is related to the very large number of women with urogenital symptoms, leading to a lack of control for analyzing multiple regression risk factors with urogenital symptoms.
Data Sharing Statement
Because this cohort study is ongoing, the data is not available for readers.
Acknowledgment
This study received statistical support from Xingming Li, a statistical expert of the Capital Medical University, Beijing, China.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Beijing Municipal Health Commission [No. (2017)35]; Beijing Municipal Administration of Hospitals’ Ascent Plan [No. DFL20181401]; and Beijing Municipality Health Technology High-level Talent [No. 2014-2-016].
Disclosure
The authors report no conflicts of interest for this work and declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Jehan S, Masters-Isarilov A, Salifu I, et al. Sleep disorders in postmenopausal women. J Sleep Disord Ther. 2015;4:1000212.
2. Al-Safi ZA, Santoro N. Menopausal hormone therapy and menopausal symptoms. Fertil Steril. 2014;101:905–915.
3. Monteleone P, Mascagni G, Giannini A, et al. Symptoms of menopause – global prevalence, physiology and implications. Nat Rev Endocrinol. 2018;14:199–215.
4. Nelson HD. Menopause. Lancet. 2008;371:760–770.
5. Moilanen J, Aalto AM, Hemminki E, et al. Prevalence of menopause symptoms and their association with lifestyle among Finnish middle-aged women. Maturitas. 2010;67:368–374.
6. Santoro N, Epperson CN, Mathews SB. Menopausal symptoms and their management. Endocrin Metab Clin. 2015;44:497–515.
7. Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19:387–395.
8. Portman DJ, Gass MLS. Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and The North American Menopause Society. J Sex Med. 2014;11:2865–2872.
9. Cohen L, Soares C, Vitonis A, et al. Risk for new onset of depression during the menopausal transition. Arch Gen Psychiat. 2006;63:385–390.
10. Heinemann K, Ruebig A, Potthoff P, et al. The Menopause Rating Scale (MRS) scale: a methodological review. Health Qual Life Out. 2004;2:45.
11. Schoenaker DAJM, Jackson CA, Rowlands JV, et al. Socioeconomic position, lifestyle factors and age at natural menopause: a systematic review and meta-analyses of studies across six continents. Int J Epidemiol. 2014;43(5):1542–1562. doi:10.1093/ije/dyu094
12. Gava G, Orsili I, Alvisi S, et al. Cognition, mood and sleep in menopausal transition: the role of menopause hormone therapy. Medicina. 2019;55:668.
13. Woods NF, Mitchell ES. Symptoms during the perimenopause: prevalence, severity, trajectory, and significance in women’s lives. Menopause. 2005;118:0–24.
14. Bromberger JT, Kravitz HM, Youk A, et al. Patterns of depressive disorders across 13 years and their determinants among midlife women: SWAN mental health study. J Affect Disorder. 2016;206:31–40. doi:10.1016/j.jad.2016.07.005
15. Woods NF, Mariella A, Mitchell ES. Depressed mood symptoms during the menopausal transition: observations from the Seattle Midlife Women’s Health Study. Climacteric. 2008;15:
16. Freeman EW, Sammel MD, Boorman DW, et al. Longitudinal pattern of depressive symptoms around natural menopause. JAMA Psychiatry. 2014;71(1):36–43. doi:10.1001/jamapsychiatry.2013.2819
17. Ruan X, Cui Y, Du J, et al. Prevalence of climacteric symptoms comparing perimenopausal and postmenopausal Chinese women. J Psychosom Obstgyn. 2017;38(3):161–169. doi:10.1080/0167482X.2016.1244181
18. Greendale GA, Huang M, Wight RG, et al. Effects of the menopause transition and hormone use on cognitive performance in midlife women. Neurology. 2009;72:1850.
19. Kravitz HM, Ganz PA, Bromberger J, et al. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10:19.
20. Politi M, Schleinitz M, Col N. Revisiting the duration of vasomotor symptoms of menopause: a meta-analysis. J Gen Intern Med. 2008;23:1507–1513.
21. Freeman E, Sammel M, Lin H, et al. Duration of menopausal hot flushes and associated risk factors. Obstet Gynecol. 2011;117:1095–1104.
22. Avis NE. Change in sexual functioning over the menopausal transition: results from the study of women’s health across the nation. Menopause. 2017;4:379–390.
23. Cagnacci AVMXASA. Female sexuality and vaginal health across the menopausal age. Am J Med. 2020;1:14–19.
24. De Zambotti M, Trinder J, Colrain IM, et al. Menstrual cycle-related variation in autonomic nervous system functioning in women in the early menopausal transition with and without insomnia disorder. Psychoneuroendocrino. 2016;75:44–51.
25. Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int J Cardiol. 2010;141:131.
26. Saleh TM, Connell BJ. Role of oestrogen in the central regulation of autonomic function. Clin Exp Pharmacol P. 2007;34:827–832.
27. Laboratory FR. Ambulatory monitoring of menopausal hot flashes. Psychophysiology. 2010;26:573–579.
28. Dhanoya T, Sievert LL, Muttukrishna S, et al. Hot flushes and reproductive hormone levels during the menopausal transition. Maturitas. 2016;89:43–51.
29. Meng W, Gong WW, Hu RY, et al. Age at natural menopause and associated factors in adult women: findings from the China Kadoorie Biobank study in Zhejiang rural area. PLoS One. 2018;13:e195658.
30. Caretto M, Giannini A, Simoncini T. An integrated approach to diagnosing and managing sleep disorders in menopausal women. Maturitas. 2019;128:1–3.
31. Nascimento CMPJDA. Physical exercise in MCI elderly promotes reduction of pro-inflammatory cytokines and improvements on cognition and BDNF peripheral levels. Curr Alzheimer Res. 2014;11:799–805.
32. Weuve J, Kang JH, Manson JE, et al. Physical activity, including walking, and cognitive function in older women. JAMA. 2004;292:1454–1461.
33. Hoffmann K, Sobol NA, Frederiksen KS, et al. Moderate-to-high intensity physical exercise in patients with Alzheimer’s disease: a randomized controlled trial. J Alzheimers Dis. 2016;50:443–453.
34. Miller BF, Olesen JL, Hansen M, et al. Coordinated collagen and muscle protein synthesis in human patella tendon and quadriceps muscle after exercise. J Physiol. 2005;567:1021–1033.
35. Stuenkel CADSGA. Treatment of symptoms of the menopause: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2015;100:3975–4011.
36. Baber RJ PNFA, Group. IW. 2016 IMS Recommendations on women’s midlife health and menopause hormone therapy. Climacteric. 2016;19:109–150.
37. Schmidt M, Arjomand-Wölkart K, Birkhäuser MH, et al. Consensus: soy isoflavones as a first-line approach to the treatment of menopausal vasomotor complaints. Gynecol Endocrinol. 2016;32:427–430.
38. Ruan X, Mueck AO, Beer AM, et al. Benefit–risk profile of black cohosh (isopropanolic Cimicifuga racemosa extract) with and without St.John’s wort in breast cancer patients. Climacteric. 2019;22:339–347.
39. Gold EB, Block G, Crawford S, et al. Lifestyle and demographic factors in relation to vasomotor symptoms: baseline results from the study of women’s health across the nation. Am J Epidemiol. 2004;159:1189–1199.
40. Freeman EW, Sammel MD, Grisso JA, et al. Hot flashes in the late reproductive years: risk factors for African American and Caucasian women. J Women Health Gend Based Med. 2001;10:67–76.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.