Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 13
Meniscal Root Repair Alone or Combined with Different Procedures After at Least 6 Months of Follow-Up: A Series of Cases
Authors Rocha de Faria JL, Serra Cruz R ![]() , Campos ALS
, Campos ALS ![]() , Souza GGA, Di Cavalcanti YS
, Souza GGA, Di Cavalcanti YS ![]() , Goes RA
, Goes RA
Received 12 November 2021
Accepted for publication 10 March 2022
Published 29 March 2022 Volume 2022:13 Pages 25—34
DOI https://doi.org/10.2147/OAJSM.S348401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Video abstract presented by Jose Leonardo Rocha de Faria.
Views: 232
José Leonardo Rocha de Faria,1,2 Raphael Serra Cruz,1,3,4 André Luiz Siqueira Campos,1,5 Gabriel Garcez Araújo Souza,1 Yuri Sampaio Di Cavalcanti,1 Rodrigo Araujo Goes1
1Instituto Nacional de Traumatologia e Ortopedia (INTO), Rio de Janeiro, RJ, Brazil; 2Albert Sabin Hospital, Juiz de Fora, MG, Brazil; 3Instituto Brasil de Tecnologias da Saúde, Rio de Janeiro, RJ, Brazil; 4Hospital São Vicente de Paulo, Rio de Janeiro, RJ, Brazil; 5Hospital Federal dos Servidores do Estado, Rio de Janeiro, RJ, Brazil
Correspondence: Raphael Serra Cruz, Tel +55 21 972347474, Email [email protected]
Purpose: To analyze clinical and functional outcomes of patients submitted to posterior meniscal root repair of the medial or lateral meniscus in different settings, with at least 6 months of follow-up.
Patients and Methods: Retrospective multicentric study assessing epidemiological characteristics and clinical-functional results of 22 patients who underwent meniscal root reinsertion (MRR) by transtibial technique. This study addressed different settings: isolated medial root repair, medial root repair associated with high tibial osteotomy (HTO) and lateral root repair associated with anterior cruciate ligament (ACL) reconstruction.
Results: Twelve patients had an isolated tear of the posterior root of the medial meniscus and underwent MRR alone. Six patients had a varus axis > 5°, undergoing MRR in addition to HTO in the same surgical procedure. Four patients underwent repair of the posterior root of the lateral meniscus associated with simultaneous reconstruction of the ACL. The main results of the study were observed in the improvement of the IKDC score from 27.7% preoperatively to 69.8% in the postoperative period (p < 0.0001) and the Lysholm score of 44.4 points preoperatively to 88.4 points in the postoperative period (p < 0.0001). Significant clinical and subjective improvements were also reported.
Conclusion: Medial meniscal root repair, associated or not with valgus tibial osteotomy (when indicated) and lateral meniscal root repair associated with ACL reconstruction, improved clinical, functional, and subjective results of the patients presented in this case series in the short term.
Keywords: meniscus, meniscus root tear, root repair, outcomes
Introduction
The menisci are essential structures located inside the knee. Their main functions include the absorption and distribution of loads across the joint, increasing the contact area between the femur and the tibia.1 Each of the menisci have bony fixations in their anterior and posterior extremities, known as meniscal roots, which anchor them firmly to the tibial plateau in the medial and lateral compartments.2 Injuries of the meniscal roots represent potential damage to the maintenance of joint homeostasis by increasing the contact pressure on loading areas, which can lead to premature wear of the cartilage of the femoral condyles and tibial plateau.1
Meniscal root tear (MRT) was first described by Pagnani et al,2 in 1991, when studying the cause of medial meniscus extrusion in a young patient.2 Since then, several studies have focused on this topic and the harmful consequences of a MRT for the knee.3 The anatomy of the meniscal roots have already been depicted by Johannsen et al.4 The posterior root of the medial meniscus is located approximately 9.6mm posterior and 0.7mm lateral to the medial tibial spine. The posterior root of the lateral meniscus is located approximately 1.5mm posteriorly and 4.2mm medially to the lateral tibial spine, approximately 12.7mm from the most proximal part of the insertion of the posterior cruciate ligament (PCL).4
The contribution of meniscal root integrity to impact absorption has been well studied by Allaire et al,1 Schillhamer et al,5 and Bathia et al.6 Such studies have demonstrated the increase in tibiofemoral contact pressure in the context of a posterior MRT, similar to a total meniscectomy. This biomechanical consequence can be reduced by repairing the root using the pull-out technique.1,5,7 In addition, posterior root tear of the lateral meniscus, can increase tibial translation in the setting of an anterior cruciate ligament (ACL) injury, making more evident rotational tests such as pivot-shift. This fact highlights the importance of the lateral meniscus root to the rotational stability of knees with a deficient ACL.8
Currently, treatment options include conservative management, meniscectomy, and meniscal root repair (MRR). In any case, it is paramount to assess patient’s lower limb alignment, since coronal plane deformities could deteriorate clinical results.9 When indicated, tibial or femoral osteotomy must be performed to correct the mechanical axis, whether associated or not with the root repair.10
Krych et al showed low levels of patient satisfaction and rapid progression to osteoarthritis in those treated conservatively.10 Regarding the functional assessment of patients, both meniscectomy and MRR found good results, as measured by Lysholm and IKDC scores.11 However, the repair results in better outcomes in the medium term with regard of osteoarthritis progression (Kellgren and Lawrence) and joint space reduction.11
Despite the better results with meniscus preservation, the reinsertion of the meniscal root is not able to completely prevent the progression of arthrosis, as shown in the study by Chung et al.12 Furthermore, the surgical approach is contraindicated in patients with severe clinical comorbidities or degenerative changes in the ipsilateral compartment classified as Kellgren and Lawrence ≥ 3 or Outerbridge ≥ 3.13,14
Despite recent advances in the study of MRT, more studies are needed to assess the effectiveness of surgical treatment with MRR.15–17 This is particularly important in the setting of concomitants injuries and/or limb malalignment, where other variables may influence the results of the repair. Therefore, it is necessary to understand better the surgical techniques and the management of MRT in different settings.
This study aimed to evaluate clinical and functional outcomes, as well as the epidemiology of patients undergoing MRR after a minimum period of 6 months of follow-up in different scenarios, addressing concomitant conditions as patients presented to the office consecutively.
Materials and Methods
This study was approved by the local Ethics and Research Committee (Instituto Nacional de Traumatologia e Ortopedia - Certificate of Presentation of Ethical Appreciation #: 22985819.8.1001.5273) and an informed consent was obtained from each study participant prior to the study commencement. The study was conducted in accordance with the principles set forth in the Helsinki Declaration.18
The evaluations of patients from the private clinic were carried out in the surgeons’ private offices, while the evaluations of patients from the public system were carried out in the outpatient sector of only one hospital. All the patients had the diagnosis of medial or lateral MRT confirmed by magnetic resonance imaging (MRI) and underwent reinsertion surgery between January of 2017 and March of 2019. All of them were 18 years-old or more, and there was no restriction by gender. All patients had a preoperative clinical-functional assessment, which included Lysholm, IKDC, visual analog scale questionnaires (VAS) for pain, subjective perception of function and range of motion (ROM). The same assessment was applied at least six months after the operation. Patients with incomplete pre or postoperative data, with complex meniscal injuries, anterior root injuries, injury to more than one meniscus, and patients with any kind of injury in the contralateral knee were excluded from this study. All of them received the same rehabilitation protocol.19
The surgical procedure is standardized among authors. All surgeries were arthroscopically performed by one of two surgeons (JRFL and RAG) involved in this project. Both used a well-padded tourniquet placed in the upper thigh of the operative leg and set to 100mmHg above the systolic pressure. Two loop stitches using non-absorbable sutures were made in the posterior horn of the injured meniscus with the aid of a specific device (mini scorpion – Arthrex, Naples, FL). Fixation was performed through a single transtibial tunnel in the anterior cortex of the tibia, using a cortical button (Figure 1A). All patients met the same rehab deadlines and goals, regardless of concomitant HTO. Weight bearing was not allowed for the first six weeks, while gaining ROM was stimulated. After this period, weight bearing was allowed as tolerated and non-impact exercises were started, such as low-speed cycling, isometric muscle strengthening, and swimming pool activities.19
 |
Figure 1 Examples of post-operative radiographs for each group. (A) AP view of a left knee after isolated medial meniscal root repair surgery; (B) AP view of a right knee after combined high tibial osteotomy and medial meniscal repair surgery; (C) AP view of a left knee after combined anterior cruciate ligament reconstruction and lateral meniscal root repair surgery. |
HTO was indicated in patients with medial MRT associated with a varus malalignment (defined in this study as a femoral-tibial angle of 5° of varus or greater).20–23 This surgery was performed at the same time of the root reinsertion and fixation was achieved using an osteotomy plate with at least 3 locking screws proximally and 3 locking screws distally (Figure 1B). The aim of post-operative alignment was neutral to 3° of valgus.
All the patients in this sample who presented with lateral MRT had concomitant ACL injury and were submitted to simultaneous root repair and ACL reconstruction (ACLR). ACLR was performed with autologous hamstrings graft. Femoral tunnel was drilled using anatomic transportal technique. Proximal fixation was achieved with a cortical fixation device, whereas distal fixation was made with a bioabsorbable interference screw. Root reinsertion in these cases were made with the same technique as described for the medial side. The transtibial tunnel was drilled independently to the ACL tibial tunnel in a divergent direction to avoid tunnel convergence (Figure 1C). We did not use the ACL tunnel to pass any meniscal suture, as the passage of the interference screw could damage it and put the repair at risk.
Statistical Analysis
In the descriptive analysis, we present the observed data in the form of measures of central tendency for numerical data and by frequency and percentage for categorical data. For the inferential analysis, we used the Shapiro–Wilk test to identify the distribution pattern of the data and non-parametric methods to perform the statistical tests. The criteria for determining the significance adopted was the level of 5%. The evolutionary assessment (preoperative x postoperative) was performed using the Wilcoxon signed-rank test for numerical data and the McNemar test corrected for categorical data. The software used to process the statistical analysis was SPSS version 26.
Results
During the study period, the surgeons performed 30 meniscal root reinsertions. Four patients were not included because of incomplete preoperative data. Two patients were excluded for not willing to participate and other two patients were lost to postoperative follow-up. Twenty-two patients remained for analysis, of which 12 had an isolated tear of the medial meniscus root without varus malalignment and were submitted to isolated MRR (IMR group). Six underwent MRR associated with concomitant medial opening HTO (MR+HTO group). Four patients underwent repair of the posterior root of the lateral meniscus associated with simultaneous reconstruction of the anterior cruciate ligament (LR+ACLR group).
The total sample consisted of 12 men (54.5%) and 10 women (45.5%). Considering the total number of MRT found in this study, 18 (81.81%) occurred in the medial compartment, and 4 (18.18%) in the lateral compartment (all of them, associated to ACL tear). Among the medial tears, one-third (6) occurred in patients with varus axis alignment > 5° and two-thirds (12) in patients without varus malalignment.
Mechanism of Injury
A story of mild sprain was observed in 50% of cases and severe sprain in 27.3%. In 13.6% of the cases, there was no history of trauma, and 9.1% reported a fall. When analyzing the etiology according to the aforementioned groups, we found that, in the IMR group, 58.3% of the patients suffered a mild sprain, 25.1% reported a severe sprain, 8.3% reported a fall, and 8.3% did not remember any event that could have led to the injury. In the MR+HTO group, the etiology was equally distributed (33.3%) between a non-traumatic, mild sprain, and severe sprain. No patient in this group reported fall as injury mechanism. In the LR+ACLR group, 50% reported a mild sprain, 25% a severe sprain, and 25% a fall. There was no atraumatic etiology in this group.
Epidemiology by Gender
Among male patients, 5 (41.66%) had a medial root tear associated with varus alignment of the lower limb greater than 5°, being submitted to concomitant HTO; 4 (33.3%) had less than 5° of varus alignment, and 3 (25%) had lateral meniscus injury concomitant with an ACL injury. Among women, only 1 (10%) had varus alignment of the lower limb greater than 5°, requiring concomitant HTO. Eight patients (80%) had an isolated lesion of the medial MRT without axis deviation greater than 5°, and 1 (10%) underwent lateral root repair associated with ACL reconstruction.
Obesity
Considering obesity as a BMI > 30 kg/m2, we observed 3 obese patients (13.6%) in this sample. One (33.3%) was located in the IMR group and two (66 0.6%) in the MR+HTO group. There were no obese patients in the LR+ACLR group. Table 1 presents a full description of the demographics found in this population.
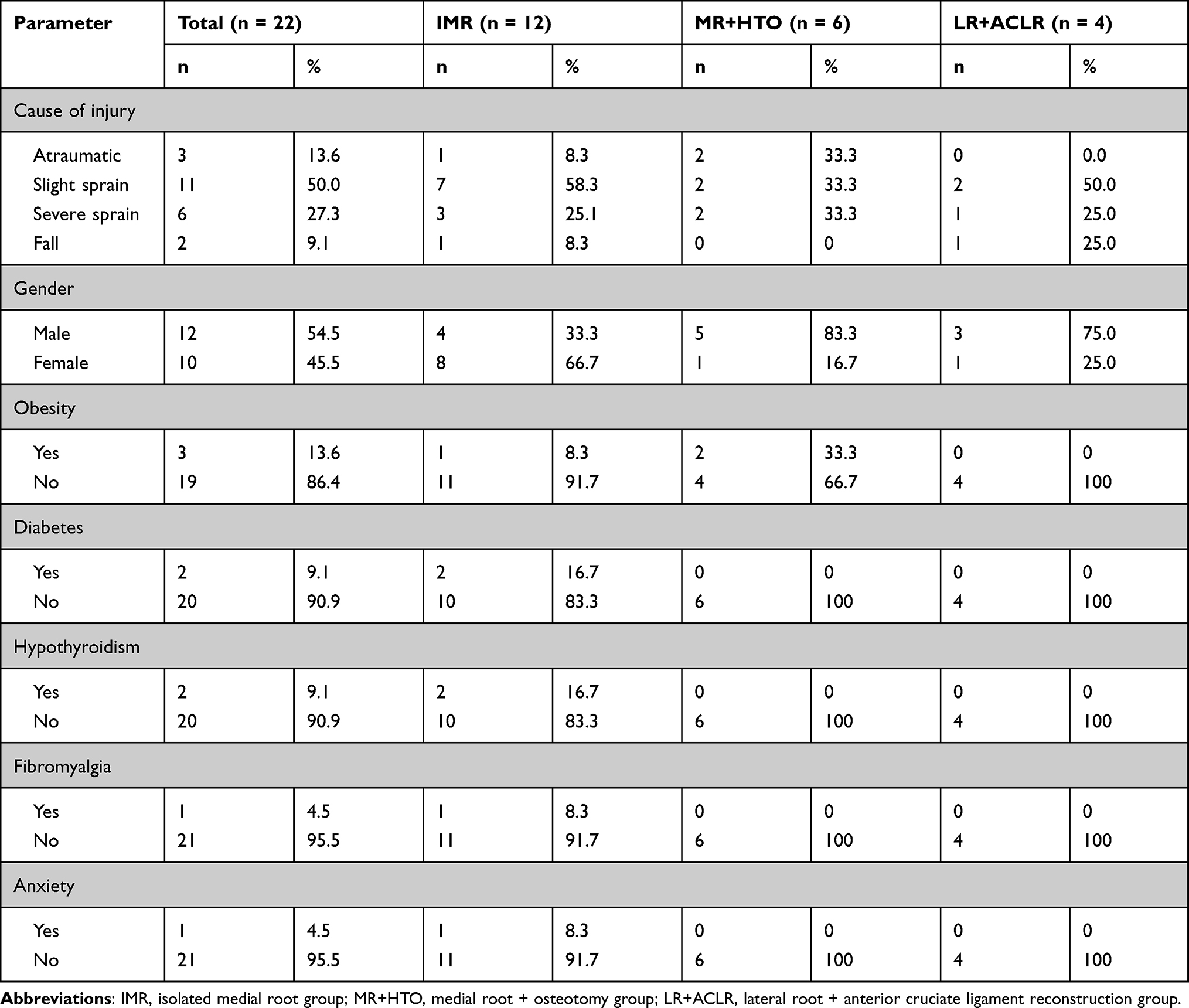 |
Table 1 Etiology of Injuries and Patient Demographics |
Age
The overall age mean of the patients in this study was 53.1 years. It was higher in patients in the IMR group (61.5 years) and lower in the LR+ACLR group (33.3). Patients in the MR+HTO group had a mean age of 49.5 years.
Return to Physical Activities
The total average time to return to physical activities was 142 days. The longest time was observed in the LR+ACLR group (157.5 days), while the shortest time was observed in the IMR group (135.8 days). The average time in the MR+HTO group was 145 days. Table 2 shows these data and time elapsed between injury and surgery and between surgery and the latest reassessment.
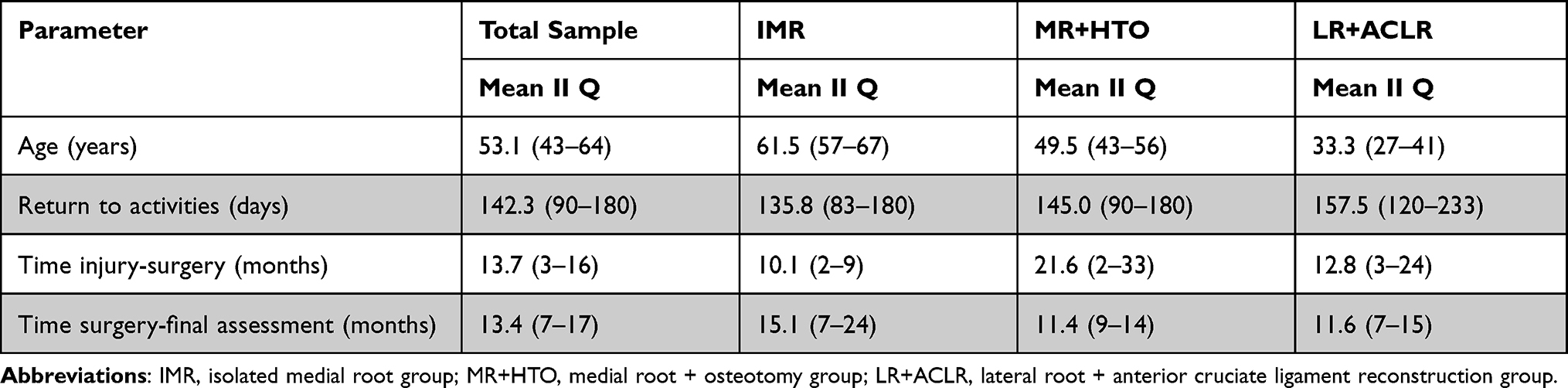 |
Table 2 Age and Times for Each Group |
Clinical-Functional Outcomes
The functional scores (IKDC and Lysholm), range of motion (ROM), pain, and subjective perception of function in the pre-and postoperative periods are presented in Table 3. A significant increase in function scores and ROM was observed, in addition to a significant decrease in the pain scale in the total sample and in the IMR and MR+HTO groups. The results obtained by the LR+ACLR group, did not reach statistical difference, at the level of 5% of significance. When we applied the Kruskal–Wallis ANOVA test to assess the difference between the groups, we found statistical relevance in the ROM (p=0.027) and the total Lysholm score (p=0.033). The p-values for the differences observed in the items pain, knee functionality, and IKDC were respectively 0.14, 0.56, and 0.073.
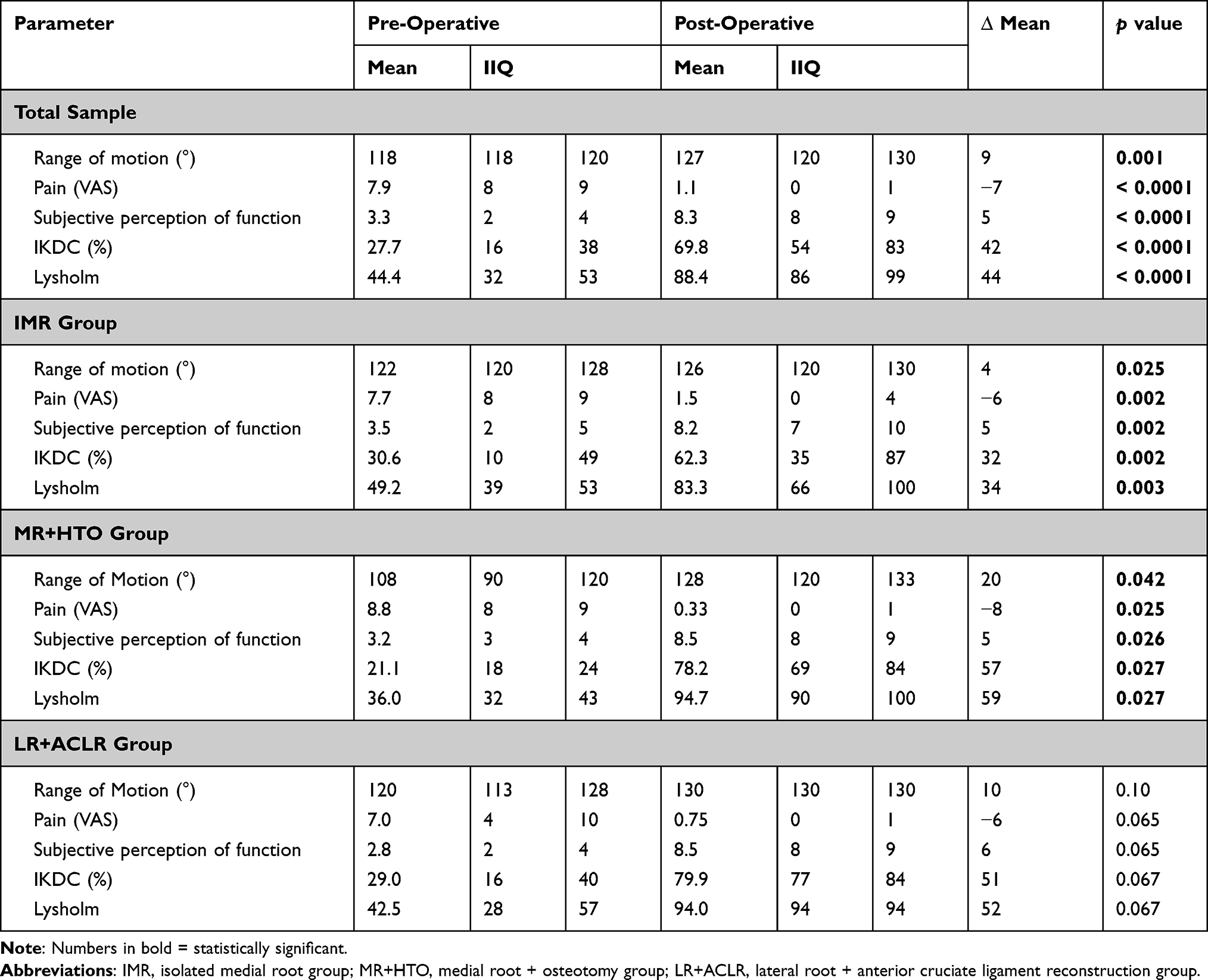 |
Table 3 Clinical-Functional Parameters Before and After the Operation by Treatment Group and in the Total Sample |
Of the 22 patients in this sample, only three (13.6%) presented a poor result after the surgical intervention, according to the Lysholm score. All of them were allocated in the IMR group, corresponding to 25% of the patients in this group. Amongst patients undergoing HTO and those affected by injury to the posterior root of the lateral meniscus, none had an outcome classified as poor in the postoperative evaluation (Table 4).
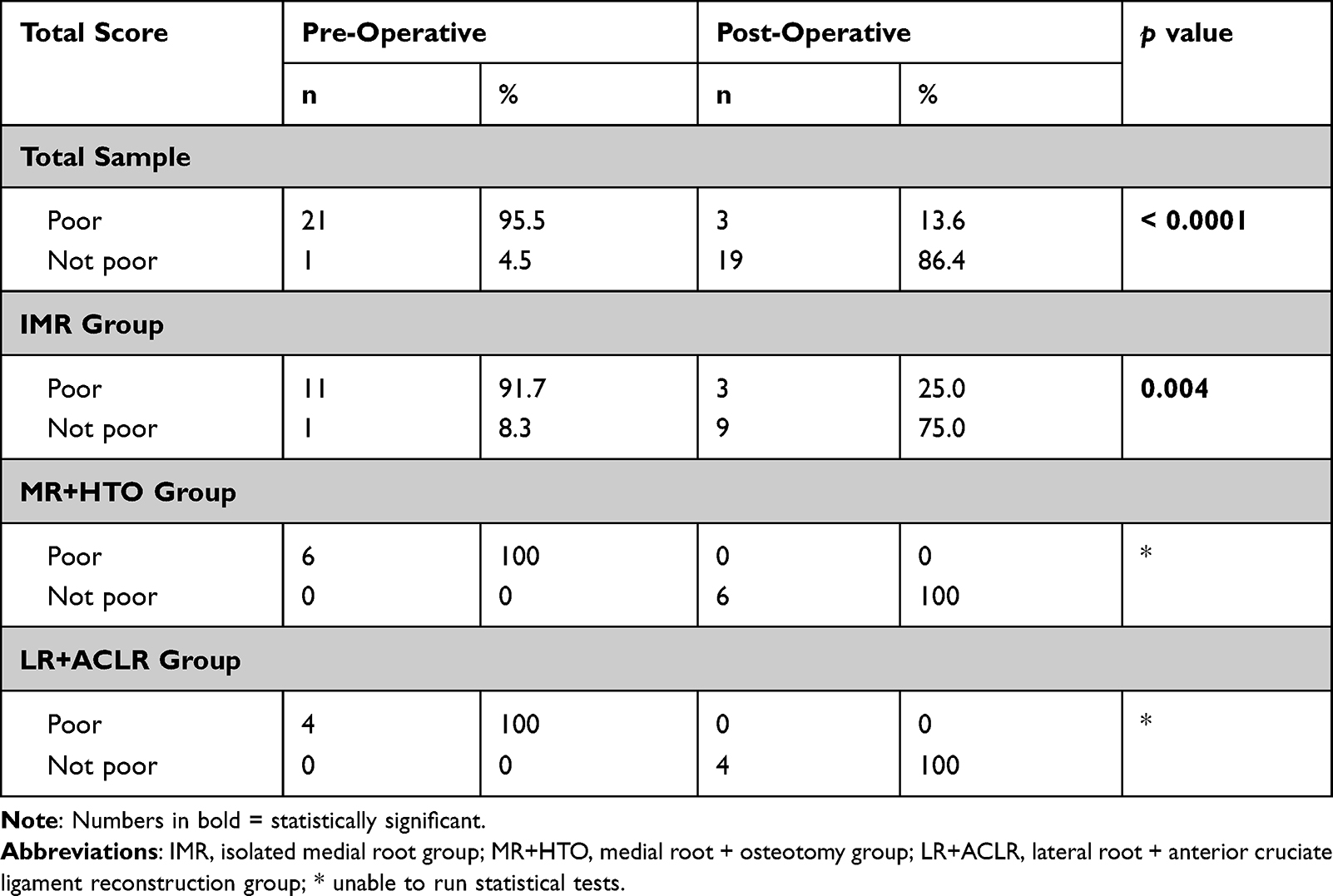 |
Table 4 Lysholm Score Evolution by Treatment Group and in the Total Sample |
Discussion
The most important findings of this study are the clinical, functional, and subjective improvements found in patients undergoing MRR in different settings. Overall, patients included in this study evolved with improved range of motion, pain, subjective perception of joint function, and functional scores (IKDC and Lysholm).
According to the literature, MRT is more common in women around the sixth decade.3,12,24 However, in our study, more than half of the patients (54.5%) were male. A possible explanation is that most articles report MRT of the medial meniscus without considering the need for osteotomy. When we isolated patients with these characteristics in our sample (IMR group), we also found a predominance of females (66.7%) over males (33.3%). On the other hand, posterior root tear of the lateral meniscus is more common in male patients and around the third and fourth decades of life.25 We found similar results in the demographic data of our study.
Regarding the age, the mean found in our total sample (53.1 years) is in accordance with that reported in the literature.3,13,17,26 When we isolate patients with lateral MRT associated with an ACL injury, there was a reduction in the mean age (32 years), which is also observed in most previously published article.25,26 Among patients with medial MRT, the mean age of those who had a varus malalignment (49.5 years) was lower than the one of patients who had solely medial MRT (61.5 years), suggesting that the axis deviation and the consequent mechanical overload may influence the degeneration of the medial compartment, including the meniscus itself.27
The measurement of the limb alignment is considered crucial when evaluating patients with suspected MRT.22 It may be even more critical than the meniscal procedure itself, when considering the clinical-radiological progression to arthrosis.20 Lee et al, found, in patients with axis deviation, a higher healing rate of the repair of the posterior root of the medial meniscus when associated with valgus HTO compared to isolated osteotomy, but did not find differences when evaluating progression to arthrosis.20 In this study, every patient who had a varus alignment greater than 5° underwent concomitant HTO,20–23 which probably contributed to the clinical and functional improvement observed during the follow-up period. However, it was not possible to differentiate which procedure (osteotomy or root repair) had the most significant influence on the final result.
Differently from what is commonly reported in the literature regarding the injury mechanism,28 most patients in the present sample mentioned some trauma, even if mild, as the cause of the injury. The majority (50%) reported a mild sprain, and 27.3% a severe sprain. Only 13.6% of patients were not able to correlate the onset of symptoms with a traumatic event.
Three patients had a BMI > 30 kg/m2, representing 13.6% of the total sample. All of them had a medial MRT and two of them required HTO. Only the patient who did not undergo HTO evolved with a Lysholm score classified as poor postoperatively, despite an improvement in pain and the subjective perception of function. This patient was also the only one over 60 years old among the three obese patients. The other two obese patients evolved with results considered good and excellent. Other studies that evaluated clinical results in obese patients also did not demonstrate obesity as a poor prognostic factor for MRR.21
Regarding clinical and functional results, despite the overall progress, the improvement observed in the LR+ACLR group did not reach statistical significance. We believe the small number of patients in this group (n=4) was responsible for the lack of statistical difference. Considering the total sample, there was a 9° improvement in range of motion, 7 points on the VAS pain scale, 5 points on the subjective perception of function (range 0–10), 42 points on IKDC, and 44 points on Lysholm score. In all variables, the MR+HTO group showed the most expressive improvement, confirming the benefit of the procedures performed in these patients.
These findings are in agreement with recent literature. Ahn et al compared 25 patients undergoing medial MRR with 13 patients treated conservatively and observed better functional scores in the operated group.24 Zheng et al recently carried out a systematic review including clinical studies that evaluated reconstruction of the anterior cruciate ligament associated with the repair of the posterior root of the lateral meniscus. No randomized clinical trials were found. The nine studies included had a low level of evidence (five retrospective cohorts and four case series). Heterogeneity between studies was also found. The results showed improvement in functional scores and a high meniscal healing rate. On the other hand, the radiological and arthroscopic findings (second look) were inconsistent, and they could not conclude that the repair can completely restore the function of the lateral meniscus.25
Chung et al compared the repair of the posterior root of the medial meniscus with partial meniscectomy with a minimum follow-up of 5 years. They had better functional scores, less progression of arthrosis, and less narrowing of the joint space in the group where the meniscus was preserved. While no patient in the repair group was converted to arthroplasty, 35% of the patients who underwent meniscectomy were reoperated for joint replacement by the end of the study. The 5-year success rate was 75% in the meniscectomy group and 100% in the repair group.12
Feucht et al carried out a systematic review and evaluated the results of the repair performed using the pull-out technique. In addition to the overall improvement in postoperative functional scores, at the end of the mean follow-up of 30 months, 84% of patients had no radiographic progression of arthrosis, 82% had no progression of chondral degeneration, and 56% had reduced meniscal extrusion on magnetic resonance imaging. Assessment by arthroscopic second look showed a complete healing rate of 62% and a partial healing rate of 34%.3
In the present study, the comparison of improvements amongst groups only revealed statistically significant differences when analyzing the range of motion and the Lysholm score. In both cases, the patients in the MR+HTO group showed the most expressive improvement, suggesting that the associated osteotomy may have contributed for a considerable amount of the improvement effect in these patients, as already described in the literature.22,27
Finally, after the surgical procedures performed, we observed that only 3 (13.6%) of the 22 patients had results classified as poor, according to the Lysholm scale. When depicting these patients’ data, looking for common characteristics that could indicate poor prognostic factors, we found that all of them were allocated in the IMR group (medial MRT with limb alignment less than 5° of varus), were female and were older than 62 years old. However, due to the small sample size, this study did not reach enough statistical power to consider these characteristics as risk factors. In a systematic review, Jiang et al, found that pre-existing chondral lesions (Outerbridge >3) and varus alignment > 5° were associated with a worse prognosis of posterior MRR of the medial meniscus.21 LaPrade et al, in a cohort of 49 patients who underwent medial MRR using a pull-out technique, observed that neither laterality nor age over 50 years had a relationship with a poor prognosis.29
This study has some limitations. It is a retrospective analysis of a series of cases operated by two different surgeons, mixing patients from both public and private clinic. However, due to the fact that MRT is a pathology that is still poorly studied and perhaps even under-diagnosed in our country, this strategy allowed us to gather more patients and reach statistical relevance in several aspects addressed. In addition, both surgeons received their training at the same hospital and used the same previously published rehabilitation protocol.19 Another limitation that we acknowledge is the heterogeneity of patients when considering the analysis of the total sample. However, this study was not intended to compare the superiority between methods, but to present the results obtained with MRR in the different situations reported. We also acknowledge the short follow-up time, which could have overestimated our results as they will probably decrease with time. Finally, variations in time between injury and surgery, as well as between surgery and postoperative evaluation, may have a negative influence on the results obtained in patients whose times were longer. Certainly, randomized controlled trials, with a larger sample size and isolating potential biases, are needed to better understand the clinical outcomes of patients undergoing MRR. However, by approaching a pathology and treatments that are relatively little studied, the key point of this study was to contribute with the authors’ experience to the scientific community, revealing the results obtained with the conducts presented hereby and providing important data that can be compiled in the future by other studies as meta-analyses, in order to reach a higher level of evidence on this topic.
Conclusion
Meniscal root repair whether isolated or in combination with valgus HTO or ACL reconstruction, when indicated, was able to improve the clinical, functional and subjective results of the patients presented in this case series. These results reveal that, since all the variables and possible concomitant injuries are investigated and addressed, MRR can achieve good results in in patients with 6 months of postoperative follow-up. More studies with a high level of evidence and controlled variables are needed to understand better the interventions performed for the treatment of this pathology.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allaire R, Muriuki M, Gilbertson L, Harner CD. Biomechanical consequences of a tear of the posterior root of the medial meniscus: similar to total meniscectomy. J Bone Jt Surg Ser A. 2008;90(9):1922–1931. doi:10.2106/JBJS.G.00748
2. Pagnani MJ, Cooper DE, Warren RF. Extrusion of the medial meniscus. Arthrosc J Arthrosc Relat Surg. 1991;7(3):297–300. doi:10.1016/0749-8063(91)90131-G
3. Feucht MJ, Kühle J, Bode G, et al. Arthroscopic transtibial pullout repair for posterior medial meniscus root tears: a systematic review of clinical, radiographic, and second-look arthroscopic results. Arthrosc J Arthrosc Relat Surg. 2015;31(9):1808–1816. doi:10.1016/j.arthro.2015.03.022
4. Johannsen AM, Civitarese DM, Padalecki JR, Goldsmith MT, Wijdicks CA, Laprade RF. Qualitative and quantitative anatomic analysis of the posterior root attachments of the medial and lateral menisci. Am J Sports Med. 2012;40(10):2342–2347. doi:10.1177/0363546512457642
5. Schillhammer CK, Werner FW, Scuderi MG, Cannizzaro JP. Repair of lateral meniscus posterior horn detachment lesions: a biomechanical evaluation. Am J Sports Med. 2012;40(11):2604–2609. doi:10.1177/0363546512458574
6. Bhatia S, Laprade CM, Ellman MB, Laprade RF. Meniscal root tears: significance, diagnosis, and treatment. Am J Sports Med. 2014;42(12):3016–3030. doi:10.1177/0363546514524162
7. LaPrade CM, Jansson KS, Dornan G, Smith SD, Wijdicks CA, LaPrade RF. Altered tibiofemoral contact mechanics due to lateral meniscus posterior horn root avulsions and radial tears can be restored with in situ pull-out suture repairs. J Bone Jt Surg Ser A. 2014;96(6):471–479. doi:10.2106/JBJS.L.01252
8. Shybut TB, Vega CE, Haddad J, et al. Effect of lateral meniscal root tear on the stability of the anterior cruciate ligament-deficient knee. Am J Sports Med. 2015;43(4):905–911. doi:10.1177/0363546514563910
9. LaPrade RF, Ho CP, James E, Crespo B, LaPrade CM, Matheny LM. Diagnostic accuracy of 3.0 T magnetic resonance imaging for the detection of meniscus posterior root pathology. Knee Surg Sport Traumatol Arthrosc. 2015;23(1):152–157. doi:10.1007/s00167-014-3395-5
10. Krych AJ, Reardon PJ, Johnson NR, et al. Non-operative management of medial meniscus posterior horn root tears is associated with worsening arthritis and poor clinical outcome at 5-year follow-up. Knee Surg Sport Traumatol Arthrosc. 2017;25(2):383–389. doi:10.1007/s00167-016-4359-8
11. Kim SB, Ha JK, Lee SW, et al. Medial meniscus root tear refixation: comparison of clinical, radiologic, and arthroscopic findings with medial meniscectomy. Arthrosc J Arthrosc Relat Surg. 2011;27(3). doi:10.1016/j.arthro.2010.08.005
12. Chung KS, Ha JK, Yeom CH, et al. Comparison of clinical and radiologic results between partial meniscectomy and refixation of medial meniscus posterior root tears: a minimum 5-year follow-up. J Arthrosc Relat Surg. 2015;31(10):1941–1950. doi:10.1016/j.arthro.2015.03.035
13. Serra Cruz R, Ferrari MB, Metsavaht L, Laprade RF Revista Brasileira de Ortopedia - Compreendendo as lesões das raízes posteriores dos meniscos: da ciência básica ao tratamento. Compreendendo as lesões das raízes posteriores dos meniscos: da ciência básica ao tratamento; 2017. Available from: http://rbo.org.br/detalhes/2508/pt-BR/compreendendo-as-lesoes-das-raizes-posteriores-dos-meniscos–da-ciencia-basica-ao-tratamento.
14. Cinque ME, Chahla J, Moatshe G, Faucett SC, Krych AJ, LaPrade RF. Meniscal root tears: a silent epidemic. Br J Sports Med. 2018;52(13):872–876. doi:10.1136/bjsports-2017-098942
15. Lau BC, Conway D, Mulvihill J, Zhang AL, Feeley BT. Biomechanical consequences of meniscal tear, partial meniscectomy, and meniscal repair in the knee. JBJS Rev. 2018;6(4):e3–e3. doi:10.2106/JBJS.RVW.17.00125
16. Moon HS, Choi CH, Jung M, Lee DY, Hong SP, Kim SH. Early surgical repair of medial meniscus posterior root tear minimizes the progression of meniscal extrusion: 2-year follow-up of clinical and radiographic parameters after arthroscopic transtibial pull-out repair. Am J Sports Med. 2020;48(11):2692–2702. doi:10.1177/0363546520940715
17. Kodama Y, Furumatsu T, Masuda S, et al. Transtibial fixation for medial meniscus posterior root tear reduces posterior extrusion and physiological translation of the medial meniscus in middle-aged and elderly patients. Knee Surg Sport Traumatol Arthrosc. 2020;28(11):3416–3425. doi:10.1007/s00167-019-05810-x
18. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human sub- jects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
19. Rocha de Faria JL, Pavão DM, Moreirão MDC, et al. Posterior root repair of medial meniscus combined with valgus opening wedge tibial osteotomy. Arthrosc Tech. 2021;10(5):e1373–e1382. doi:10.1016/j.eats.2021.01.042
20. Lee DW, Lee SH, Kim JG. Outcomes of medial meniscal posterior root repair during proximal tibial osteotomy: is root repair beneficial? J Arthrosc Relat Surg. 2020;36(9):2466–2475. doi:10.1016/j.arthro.2020.04.038
21. Jiang EX, Abouljoud MM, Everhart JS, et al. Clinical factors associated with successful meniscal root repairs: a systematic review. Knee. 2019;26(2):285–291. doi:10.1016/j.knee.2019.01.005
22. Gelber PE, Barenius B, Perelli S. Role of alignment and osteotomy in meniscal injuries. Clin Sports Med. 2020;39(1):211–221. doi:10.1016/j.csm.2019.08.006
23. Jing L, Liu K, Wang X, et al. Second-look arthroscopic findings after medial open-wedge high tibial osteotomy combined with all-inside repair of medial meniscus posterior root tears. J Orthop Surg. 2020;28(1):2309499019888836. doi:10.1177/2309499019888836
24. Ahn JH, Il KK, Wang JH, Kyung BS, Seo MC, Lee SH. Arthroscopic repair of bucket-handle tears of the lateral meniscus. Knee Surg Sport Traumatol Arthrosc. 2015;23(1):205–210. doi:10.1007/s00167-013-2764-9
25. Zheng T, Song G, Li Y, et al. Clinical, radiographic, and arthroscopic outcomes of surgical repair for radial and avulsed lesions on the lateral meniscus posterior root during ACL reconstruction: a systematic review. Orthop J Sport Med. 2021;9(3):232596712198967. doi:10.1177/2325967121989678
26. Jiang EX, Everhart JS, Abouljoud M, et al. Biomechanical properties of posterior meniscal root repairs: a systematic review. Arthrosc J Arthrosc Relat Surg. 2019;35(7):2189–2206.e2. doi:10.1016/j.arthro.2019.01.018
27. Primeau CA, Birmingham TB, Leitch KM, Appleton CT, Giffin JR. Degenerative meniscal tears and high tibial osteotomy: do current treatment algorithms need to be realigned? Clin Sports Med. 2019;38(3):471–482. doi:10.1016/j.csm.2019.02.010
28. Strauss EJ, Day MS, Ryan M, Jazrawi L. Evaluation, treatment, and outcomes of meniscal root tears a critical analysis review. JBJS Rev. 2016;4(8). doi:10.2106/JBJS.RVW.15.00082
29. LaPrade RF, Matheny LM, Moulton SG, James EW, Dean CS. Posterior meniscal root repairs: outcomes of an anatomic transtibial pull-out technique. Am J Sports Med. 2017;45(4):884–891. doi:10.1177/0363546516673996
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.