")
Back to Journals » Infection and Drug Resistance » Volume 12
Meningococcal Group B Vaccine For The Prevention Of Invasive Meningococcal Disease Caused By Neisseria meningitidis Serogroup B
Authors Rivero-Calle I , Raguindin PF , Gómez-Rial J , Rodriguez-Tenreiro C, Martinón-Torres F
Received 2 March 2019
Accepted for publication 12 September 2019
Published 9 October 2019 Volume 2019:12 Pages 3169—3188
DOI https://doi.org/10.2147/IDR.S159952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Joachim Wink
Irene Rivero-Calle,1,2 Peter Francis Raguindin,2 Jose Gómez-Rial,2 Carmen Rodriguez-Tenreiro,2 Federico Martinón-Torres1,2
1Translational Pediatrics and Infectious Diseases, Department of Pediatrics, Hospital Clínico Universitario de Santiago de Compostela, Galicia, Spain; 2Genetics, Vaccines and Pediatric Infectious Diseases Research Group (GENVIP), Hospital Clínico Universitario and Universidad de Santiago de Compostela (USC), Galicia, Spain
Correspondence: Federico Martinón-Torres
Translational Pediatrics and Infectious Diseases Section, Pediatrics Department, Hospital Clínico Universitario de Santiago de Compostela, Travesía da Choupana, s/n, Santiago de Compostela 15706, Spain
Email [email protected]
Abstract: Invasive meningococcal disease (IMD) is a major public health concern because of its high case fatality, long-term morbidity, and potential to course with outbreaks. IMD caused by Nesseira meningitidis serogroup B has been predominant in different regions of the world like Europe and only recently broadly protective vaccines against B serogroup have become available. Two protein-based vaccines, namely 4CMenB (Bexsero®) and rLP2086 (Trumenba®) are currently licensed for use in different countries against MenB disease. These vaccines came from a novel technology on vaccine design (or antigen selection) using highly specific antigen targets identified through whole-genome sequence analysis. Moreover, it has the potential to confer protection against non-B meningococcus and against other Neisserial species such as gonococcus. Real-world data on the vaccine-use are rapidly accumulating from the UK and other countries which used the vaccine for control of outbreak or as part of routine immunization program, reiterating its safety and efficacy. Additional data on real-life effectiveness, long-term immunity, and eventual herd effects, including estimates on vaccine impact for cost-effectiveness assessment are further needed. Given the predominance of MenB in Europe and other parts of the world, these new vaccines are crucial for the prevention and public health control of the disease, and should be considered.
Keywords: meningococcal disease, invasive meningococcal disease, meningococcal B, vaccine development, vaccine effectiveness, epidemiology
Introduction
Etiology
Neisseria meningitidis (meningococcus) is a gram-negative encapsulated bacteria which causes invasive meningococcal disease (IMD). The most frequent clinical presentations are meningitis and septicemia, both of which are responsible for significant morbidity and mortality worldwide.1–3 Humans are the only host for the bacteria. Meningococcus is also a common commensal in the nasopharynx, transmitted from person-to-person via respiratory secretions.1 Nasopharyngeal carriage prevalence varies with age, having its peak (23.7%) in adolescents and young adults. It may also be substantially higher (up to 71%) in closed communities like college residences and military camps.4–6
The most common pathogenic groups in humans are A, B, C, W, X, and Y, which can cause endemic disease or seasonal outbreaks.1
Epidemiology And Burden Of Illness
Invasive meningococcal disease remains a public health concern worldwide even with safe and effective available vaccines for use.3,7 More than one million cases are reported annually.3,7 Case fatality rates range from 10% to 40% depending mainly on the clinical presentation and serogroup, despite antibiotic-use and intensive supportive care.7 Furthermore, survivors may suffer debilitating sequelae that reduce the quality of life for the patient and family members.7 Financial burden caused by long-term morbidities has continuously been underestimated. This is commonly due to healthcare costs related to permanent cognitive deficits, psychological stress, and adaptive measures for reintegration into society.7,8 The holistic analysis of burden, including both its financial and social aspects, sums up the real consequences of this debilitating disease.
The incidence of IMD varies with age. The first peak occurs during the first year of life due to immunological immaturity, a second peak appears in adolescence related to an increased carriage, and a third peak in the elderly that is related to multiple comorbidities.1 In 2017, the average incidence of IMD across Europe slightly decreased to 0.6 cases per 100,000 population from the 0.7 cases per 100,000 population reported in 2010.3,9 Countries with the highest number of incidence in 2015 were Lithuania (2.4 cases/100,000), Ireland (1.5), the Netherlands (1.2), and the United Kingdom (1.2).3 Despite the low overall disease incidence, certain serogroups are emerging as a concern in selected areas.3
The introduction of serogroup C meningococcus10-containing vaccine in the routine immunization across Europe has resulted in a significant decline in the proportion of MenC-disease in the region. However, this has minimal to no effect on other serogroups. N. meningitidis serogroup B (MenB) has become the leading cause of meningococcal disease across several regions, including Europe and America.1,11,12 Although the overall incidence is low compared to other vaccine-preventable diseases, MenB disease carries substantial case fatality rate at 3% to 10%.12 It also results in significant morbidity and carries a threat for an outbreak.13–16 Thus, vaccination against MenB serogroup has become an important public health priority.
Treatment And Preventive Strategies
Meningococcal disease can be devastating as it is capable of causing death in a few hours. Antibiotics should be started as soon as the disease is suspected as their use aims to reduce the severity and chances of death14 However, the best way to avoid adverse long-term sequelae is to prevent infection that could be done through immunization. Currently available meningococcal conjugate vaccines contain polysaccharides from one (A or C), two (C and Y), or four (A, C, W, and Y) serogroups, which are chemically conjugated to protein carrier molecules.17
Although conjugated polysaccharide vaccines seem to work for other serogroups (A, C, Y, W), this has not been the case for serogroup B. A polysaccharide-based vaccine was disregarded for two major reasons, its theoretical risk for autoimmunity and its low immunogenicity. First, there is similarity of human endogenous glycopeptide with serogroup B meningococcal capsule.18,19 Although natural infection is not shown to produce cross-reactive antibodies,20 the use of polysaccharide capsule to induce bactericidal antibodies took lesser priority because of its theoretical risk for auto-antibody responses. Second, the polysialic acid nature of MenB capsule has been shown to be poorly immunogenic.21 Initial investigation on the use of capsular components failed to generate adequate antibody responses.22 Likewise, conjugation of the capsular components failed to show adequate responses on rhesus monkeys.23 As such, other vaccine targets and vaccine designs were ventured.
Vaccines Licensed For Use Against Meningococcus Serogroup B (MenB)
Currently licensed vaccines, 4CMenB (Bexsero®, GSK) and rLP2086 (Trumenba®, Pfizer) (see Table 1), used subcapsular proteins that were widely present not only in serogroup B strains but also across different meningococcus serogroups.4,24–47 These protein candidates used for vaccines are summarized in Table 2.
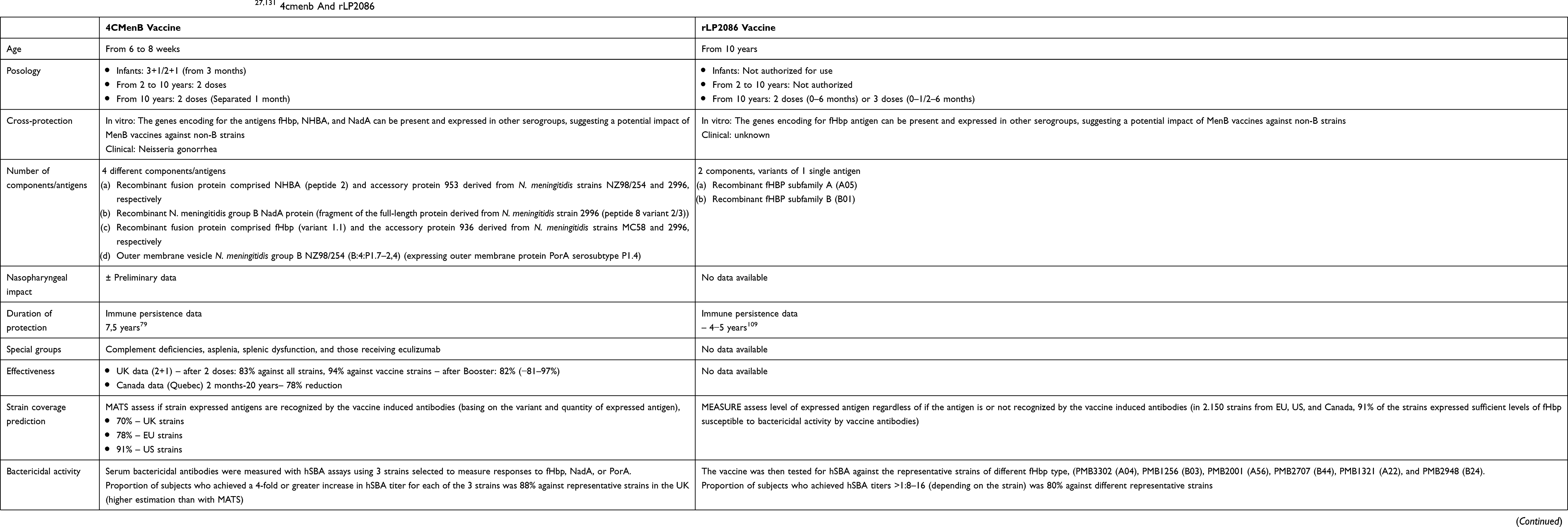 |
Table 1 Main Characteristics Of Available MenB Vaccines:27,131 4cmenb And rLP2086 |
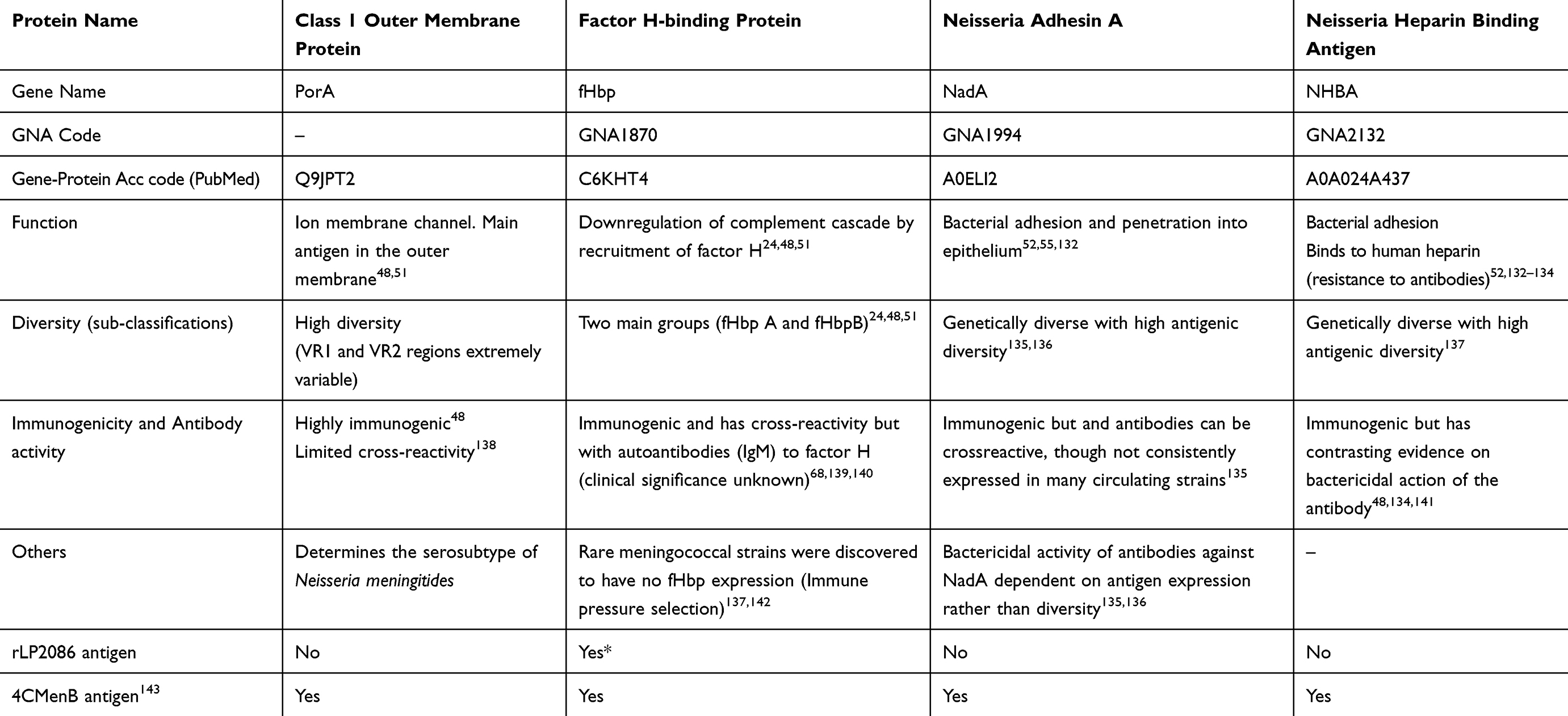 |
Table 2 Protein Targets Of Currently Licensed Vaccines |
Development Of The 4cMenB Vaccine
The 4CMenB vaccine contains subcapsular protein antigens intended to induce the production of bactericidal antibodies against 4 vaccine antigens, namely NHBA, NadA, fHbp, and Porin A (details summarized in Table 2).48 Multiple subcapsular components are thought to enable comprehensive coverage across a number of strains via their respective different mechanisms of action and thus, also prevent eventual “escape” strains.19,25
Suitable subcapsular protein targets were first identified via the process known as “Reverse Vaccinology”. This technology used the complete genome sequence of a pathogenic reference strain of MenB (MC58 strain)49 to identify proteins suitable for further investigation as vaccine candidates.49–52 Of the 2158 genes present in the complete genome of the reference strain,49 the group selected 570 that were predicted in-silico to encode for secreted or surface proteins. Of these, only 350 were successfully expressed as recombinant proteins, of which only 28 were found to induce a functional serum bactericidal antibody (SBA) response.48,53 The selection of proteins to be included was based on its ability to induce bactericidal antibodies, its prevalence across different B strains, and its capacity to confer protection in an infected mouse model.53 The three genome-derived Neisseria antigens (GNA) meeting these criteria were Neisserial heparin binding antigen (NHBA or GNA 2132),52 factor-H binding protein (fHbp or GNA 1870),54 and Neisseria adhesin A (NadA or GNA 1994).55 The three proteins, fHbp, NadA, and NHBA, were observed to have epitopes which elicit protective antibodies.56 Thus, the practice of combining different protein targets in a single vaccine will theoretically result in an enhanced bactericidal response through synergism. A study has shown that some antibodies directed against fHbp and NHBA may work in a cooperative manner for their bactericidal effect.57
A mixture of soluble outer membrane vesicles (OMVs) obtained after detergent extraction was fractionated and purified, and the resulting formulation was used to immunize mice to identify proteins capable of inducing SBA against a range of meningococcal strains.26,58
Development Of The rLP2086 Vaccine
An analysis of 2150 strains has shown that fHBP expression was detected above the limit of detection in >95% of the investigated isolates, proving the ability to induce a protective immune response and thus was considered a reasonable choice for a vaccine antigen.39,58,59 Extensive molecular epidemiology of MenB clinical isolates collected from European meningococcal reference laboratories demonstrated that meningococcal fHBP gene sequences segregate into two subfamilies, designated A and B.60 Protein variants within subfamilies share ≥83% amino acid sequence identity, but only 60–75% identity between subfamilies.61 The rLP2086 vaccine contains two lipidated fHbp variants, one from each subfamily A and B, and aims to broaden cross-protection through a nearly complete coverage of a single antigen.26 The lipidation of fHbp facilitates antigen presentation during MenB infection and acts as an adjuvant.62 The selection of fHbp variants included in rLP2086 vaccine is derived from the phylogenetic analysis of IMD isolates from the US and Europe to cover two of the most prevalent variants from both fHbp subfamilies.59,61,63 The current vaccine formulation contains A05 and B01 variants of the fHbp, with the addition of aluminium salt as an adjuvant.64
Clinical Studies On Meningococcal B Vaccines
Due to the low incidence of invasive meningococcal disease in some countries or the unpredictability of the emergence of an outbreak, study designs with clinical endpoints are almost impossible to conduct.65–67 Thus, a correlate of protection is being used on all meningococcal vaccines in development. The correlate of protection is an immunologic outcome that is used as a surrogate measure for efficacy. For serogroups A, C, W, X, and Y both rabbit (rSBA) and human serum bactericidal assays (hSBA), which measure levels of functional antibody, are an accepted correlate of protection (although baby rabbit serum is recommended); whereas human serum bactericidal assays (hSBA), is the only currently accepted correlate of protection used for the development of MenB vaccines.34,68 However, due to the inherent difference of the two MenB vaccines, each product used a different assay to measure the correlate of protection and thus, direct comparison of efficacy is not feasible. Tables 3 and 4 summarize the available data on efficacy and safety of 4CMenB28–30,69–71 and rLP2086,31–33,72 respectively.
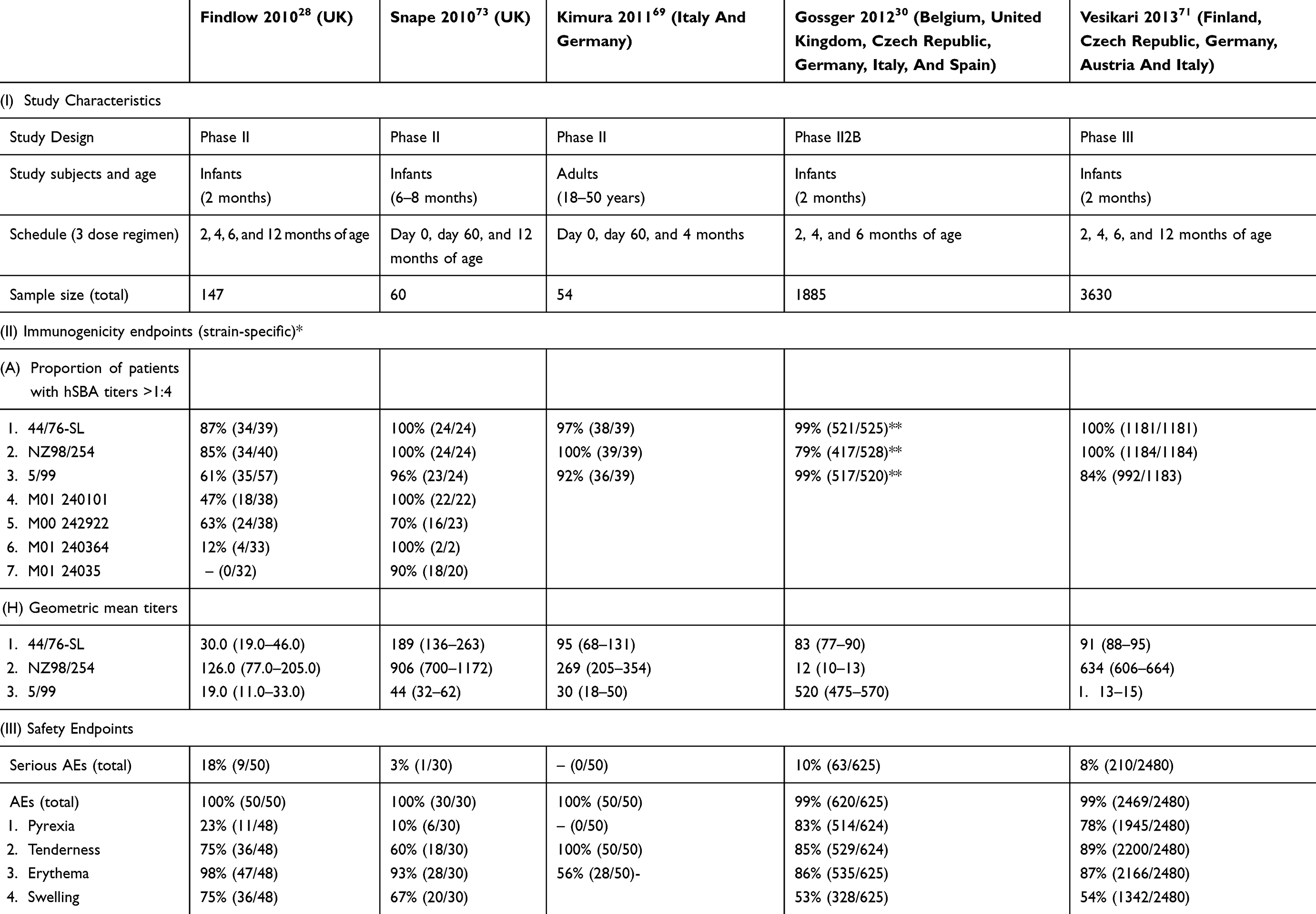 |
Table 3 Key Clinical Trials On 4cmenb Vaccine |
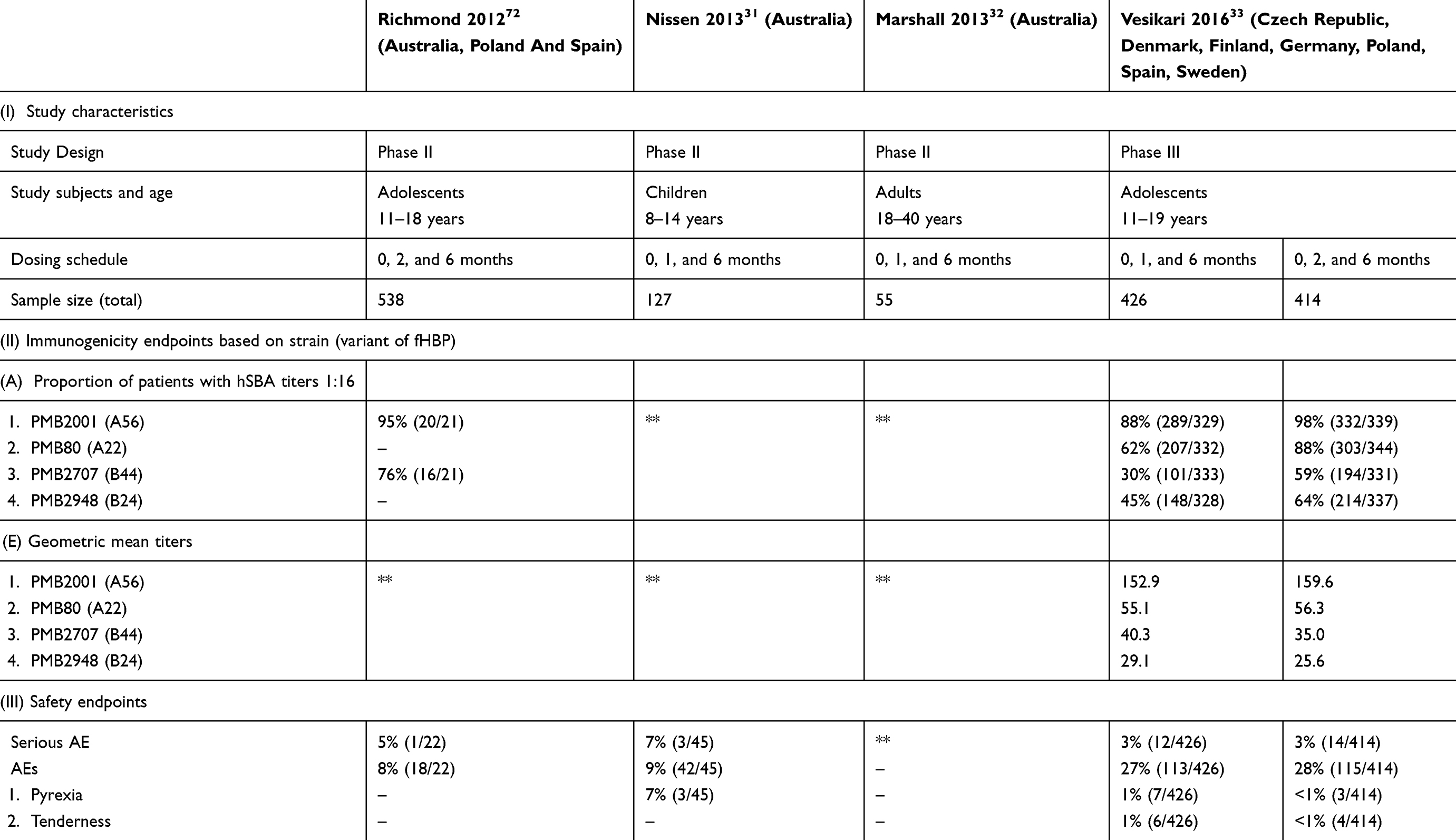 |
Table 4 Key Clinical Trials On rLP2086 Vaccine |
Furthermore, the clinical vaccine development program of the two vaccines was planned for introduction in different age groups, with the 4CMenB for individuals from 2 months of age and older and the rLP2086 for adolescents from 10 years of age. However, trials have been ongoing on both vaccines to expand their use among age groups beyond their current marketing approval.
Immunogenicity Of The 4cMenB Vaccine
4CMenB was shown to elicit good immunogenicity in infants using 3 doses. Although initial clinical trials were performed with a total of 4 doses, results from later trials allowed dose reduction.28,30,69,71,73 Furthermore, concomitant administration of MenC CRM-conjugated vaccine (MenC-CRM) and 4CMenB in infants was found to be immunogenic, resulting in a sufficient immune response against MenB after primary and booster vaccination.38
The immunogenicity of 4CMenB in adolescents was studied in four clinical studies as part of the clinical vaccine development program and eventual planned marketing authorization in the similar age group.35–37,74 hSBA was assessed against three indicator strains (strain 44/76-SL for fHbp, strain 5/99 for NadA, and strain NZ98/254 for PorA P1.4) to determine the immunogenicity of individual vaccine components.35,37 A suitable strain for assessing bactericidal activity of NHBA-specific antibodies was not available at that time, and was later performed using strain M10713. The primary immunogenicity endpoints in the four 4CMenB clinical trials were different.35–37,74 The hSBA titers of ⩾1:4 were used in two studies,37,74,75 but to ensure a higher assurance of reaching the immunological endpoint, the subsequent studies have used higher titers as a cut-off (see Table 3).
In terms of long-term immunogenicity, the primary course is sufficient to achieve a satisfactory immune response within 30 days of vaccination for both infants and adolescents.29,76 A booster dose at 12 months with 4CMenB improved bactericidal responses and facilitated immune persistence in infants until 28 months of age.29 On the other hand, an additional dose at 40–44 months old in those who had previously completed the primary course showed an anamnestic response.77 However, antibody persistence, booster responses, and safety profiles were similar between vaccination schedules using 2 primary doses and 3 primary doses.78 Among adolescents, hSBA declined at 4.5 years and 7 years after primary immunization although remained to be higher compared to the vaccine-naïve population.76,79
Immunogenicity Of The rLP2086 Vaccine
The clinical trials on rLP2086 are peculiar as they used strains of meningococcus that expressed fHBP variant that is different from what the vaccine contains (A05 and B01). This alternative strategy aims to provide an immunologic proof that the vaccine can induce protective antibodies against a broader range of meningococcal strains. The vaccine was then tested for hSBA against the representative strains of different fHbp type, namely PMB3302 (A04), PMB1256 (B03), PMB2001 (A56), PMB2707 (B44), PMB1321 (A22), and PMB2948 (B24).4,80 A higher threshold value was also set to ensure high titers when the vaccine is used in humans (>1:8–16, depending on the strain).4,81
rLP2086 has shown to elicit robust hSBA responses to MenB strains expressing different fHBP variants on adolescents at 2 or 3 doses.39 Co-administration with adolescent immunizations and rLP2086 was also evaluated in some studies. The non-inferiority criteria were met for all immunogenicity endpoints for MenB strains, MCV4, and Tdap antigens, as well as for HPV antigens, except HPV18.82,83 Seroconversion for all 4 HPV antigens was achieved by ≥99% of subjects in the groups that received quadrivalent HPV vaccine.83
After three doses of rLP2086, protective hSBA titers above the correlate of protection (≥1:4) were elicited after a 4-year follow-up in more than 50% of the children for the three out of four representative meningococcal strains expressing the vaccine-heterologous antigens.84 However, serum titers declined to <1:4 by 9 to 11 months for some strains, raising concerns by some on the strain-specificity of the long-term protection.85
Vaccination In Special Groups
The major bactericidal action of antibodies against meningococcus is mediated by the complement system. Thus, children with complement deficiencies, asplenia, and splenic syndromes, and children receiving drugs against the complement proteins (i.e., eculizumab) are at high-risk for the development of invasive meningococcal diseases.86–89 4CMenB is recommended for children with complement deficiencies, asplenia, splenic dysfunction, and those receiving the monoclonal antibody eculizumab.86 However, data on the safety and immunogenicity in these patients are scarce.87–89
In a clinical study enrolling children with asplenia or splenic dysfunction, giving 2 doses of 4CMenB has been shown to induce bactericidal antibodies as compared to healthy controls.86 Also, the 4CMenB vaccine was able to generate bactericidal activity, albeit lower, in the presence of exogenous complement on the majority of children with complement deficiency86 The significance of the inferior responses of SBA titers in complement-deficient children and those undergoing complement-inhibitor therapy must be further analyzed and compared with ongoing surveillance on vaccine failures. Schedules in this subgroups of children could be revised to accommodate additional dose, the inclusion of a booster, or different dose intervals.86 There is no data available for special groups with rLP2086 vaccine.
Cross-Protection Against Other Meningococcal Serogroups
The genes encoding for the antigens fHbp, NHBA, and NadA can be present and expressed in other serogroups, suggesting a potential impact of MenB vaccines against non B strains.42 Thus, the vaccine has a theoretical effect against all serogroups becoming a true universal anti-meningococcal vaccine. The first investigation was done on the possible cross-protection against serogroup × causing outbreaks in Africa in a pooled sera of infants immunized with 4CMenB.43 Although with small sample size, the sera revealed bactericidal antibodies against the other serogroup. Further studies have explored the potential impact of MenB vaccination against non-B meningococcal disease in Australia, Europe, and Brazil.42,44,90 The results showed that sera of 4CMenB immunized subjects induced complement-mediated killing of MenC, MenW, and MenY in a range from 45% to 90%, suggesting that 4CMenB vaccine could potentially have an impact on non-B meningococcal disease.42–44,90
Immunological responses have been assessed with non-B meningococcal disease-causing strains from Europe, Africa, and the United States using rLP2086.39 After 2 or 3 doses of the vaccine, 53% to 100% of individuals had bactericidal responses against meningococcal serogroup C, W, Y, and X strains, and 20% to 28% had bactericidal responses against serogroup A strains.81 In fact, these bactericidal responses were higher than the serological correlate of protection for meningococcal disease (hSBA titers ≥ 1:8 vs hSBA titers ≥ 1:4).91 These results suggest that rLP2086 could confer protection against meningococcal disease, regardless of serogroup.91
Cross-Protection Against Neisseria gonorrhoeae (gonococcus)
Neisseria gonorrhoeae and N. meningitidis are closely related to bacteria. Although vaccines are routinely used for N. meningitidis, there is currently no vaccine available for N. gonorrhoeae (gonococcus). The target epitopes of the currently licensed vaccines for meningococcus are similarly found in gonococcus. Recent studies have proven that N. gonorrhoeae shares a high level of sequence identity with OMV antigens in serogroup B meningococcal vaccines, MeNZB, and 4CMenB.92–94 Antibodies in the serum of 4CMenB vaccines are able to recognize several gonococcal proteins, including the gonococcal NHBA homologue.94 Theoretically, the high level of anti-gonococcal-NHBA antibodies generated by the MenB vaccines may result in additional cross-protection against gonorrhea. It was estimated that an OMV-based vaccine has an effectiveness estimate of 31% (95% CI 21–39) against gonococcus.92,94
Vaccine Coverage Of Invasive Meningococcal Group B Isolates
To predict the strain coverage of the vaccine across different meningococcal strains, a large panel of bacterial isolates representative of invasive disease would need to be tested for hSBA using a huge number of samples. A large volume of serum is also needed per participant which would pose ethical problems in pediatric studies.95 Furthermore, the SBA assay with human complement is difficult to standardize from varying sources for different meningococcal strains. Thus, estimation of strain coverage of the current vaccines using conventional laboratory methods proves cumbersome and impractical. This leads to the development of alternative assays to measure surface antigens and theoretical strain coverage of the vaccine. However, these novel assays are vaccine-specific as they detect different proteins that are distinct to the vaccine product, thereby limiting its cross-platform utility and comparability.
The Meningococcal Antigen Typing System (MATS) assess if strain expressed antigens are recognized by the vaccine-induced antibodies (basing on the variant and quantity of expressed antigen). MATS is an ELISA test designed specifically to measure the immunologic cross-reactivity and quantity of antigen expression of three 4CMenB protein antigens (fHbp, NadA, and NHBA).25,96 The results are correlated with the lysis of the meningococcal strains in the hSBA assays upon exceeding the positive bacterial threshold (PBT) for any one of the 3 antigens of the vaccine with ≥80% chance of being neutralized in a serum of the immunized person. Those strains that are positive for 2 or more antigens are more likely to be neutralized at 96%.25,96
The theoretical strain coverage of the vaccine could be defined as the proportion of circulating strains in a given country or region with scores (RP: relative potency) above the bactericidal threshold (PBT) for at least one of the three antigens. MATS has estimated strain coverage in different countries for 4CMenB vaccine which ranges from 66% in Canada (95% CI, 43–78%) to 91% in the US (95% CI, 72–96%).97,98 In a study conducted using 1052 strains of MenB from 5 European countries (Germany, France, UK, Italy, and Norway), MATS predicted that 4CmenB strain coverage would range from 73% (95% CI, 57–87%) in the UK to 87% (95% CI, 70–93%) in Italy.45 MATS coverage increases with age, varies by geographical region, and is associated with more severe disease.46 Temporal changes in circulating strains underscore the need for continued monitoring of antigen expression and diversity, particularly in countries using 4CMenB vaccines in their respective immunization programmes.46
The Meningococcal Antigen Surface Expression (MEASURE, Pfizer Inc.) assay was developed to assess surface expression levels of fHbp on meningococcal strains and prediction of complement-mediated killing by hSBA in an immunized serum. MEASURE assesses level of expressed antigen regardless of if the antigen is or not recognized by the vaccine-induced antibodies. MEASURE is a flow cytometry platform that uses a monoclonal antibody specific to an epitope common to both fHBP variants, thereby allowing a phenotypic assessment of expression and quantification of surface-expression on meningococcus strains prepared via hSBA assay. Unlike some other meningococcal epidemiologic markers, fHBP surface expression levels determined by the flow cytometric-based MEASURE assay were predictive of strain susceptibility in the hSBA assay.99 In a large, prevalence-based collection of invasive MenB isolates from national reference laboratories in the United States and Europe, 95.8% of them demonstrated fHBP expression levels greater than the limit of detection of the assay.26,60
Safety Of Meningococcal B Vaccines
4cMenB Vaccine
Some commonly observed vaccine-induced reactions have been reported when administering 4CMenB in both adolescents37 and infants.47 The most frequent among adolescents and adults were pain at the injection site37 while injection-site tenderness, erythema, and fever >38.5ºC were more frequently observed in infants (especially when 4CMenB was concomitantly administered with routine immunization).47,100 This reactogenicity can be prevented with the prophylactic use paracetamol provided with the vaccine without interferences in the immunogenicity.47 For this reason, UK Joint Committee on Vaccination and Immunisation advised the use of paracetamol when 4CmenB is administered to infants concomitantly with other routine vaccines.47
Two large observational cohort studies investigated the national MenB immunization programmes for infants (2–4 months) in the UK101 and in individuals (2 months to 20 years) in Quebec.102,103 After the administration of 3 million doses of 4CMenB in the UK, 366 (41%) reports were received related to local reactions and 364 (40%) related to fever.104 To note, 160 reported of a persistent nodule at the site of injection, three (<1%) reported of Kawasaki disease, and another three reported (<1%) of sudden infant death syndrome.104 There were no significant safety concerns.104 On the other hand, among approximately 43,000 vaccinated individuals at Quebec, only two possibly vaccine-related serious adverse events (bronchospasm) were reported. However, the reported prevalence of local pain (97%) and fever (44%) was high.103,105
Healthcare-associated costs of vaccine-related adverse events or increased reactogenicity might be eventually significant. However, its low incidence in real-life practice and the protection the vaccine confers against the disease overwhelmingly outweigh the risks.106 Vaccine reactogenicity could potentially raise concerns in the immunization campaigns, but accumulated experience shows that it has not had a significant impact on the immunization program.107
rLP2086 Vaccine
Safety and immunogenicity of the vaccine were established in several clinical trials (see Table 4).31–33,72 Localized reactogenicity was mainly observed in adolescent trials. Only few systemic reactions, such as fever or headache, were attributed to the vaccine.84,108,109 rLP2086 appears to be well tolerated in younger children. Fever occurred in 0–40.9% of toddlers receiving any rLP2086 vaccine dose, but was mostly mild or moderate in severity.110 By comparison, 9.7–18.8% of participants receiving HAV reported some fever.110 Four cases of fever >40.0°C were reported (3 in the 200 μg group and 1 in the 60 μg group), each of which lasted for 1 to 2 days.110
Post-marketing safety data of rLP2086 through the Vaccine Adverse Event Reporting System (VAERS) analysis showed very few serious adverse events and no new safety concerns.111 The first real-world experience to examine adverse events of bivalent rLP2086 was at Rhode Island (US) where more than 90% of a college-age population was vaccinated.112 The most commonly reported adverse event was injection site pain, followed by fatigue, myalgia, and fever, similar to those reported in clinical trials, while headache rates were lower than previously reported.112
Potential For Herd Immunity Through The Impact On Carriage
Adolescents have the highest rates of meningococcal carriage and transmission rates.11 Interrupting carriage acquisition of invasive MenB strains in adolescents is crucial in the control of meningococcal disease by reducing the transmission to other age groups through herd immunity.4,24 A strategy focused on adolescents may have more profound and long-lasting indirect impact, and may be more cost-effective. Furthermore, the increasing focus of different countries in improving adolescent health can be used as a platform to include newer vaccines in the routine immunization program targeting this age-group. However, limited data exist on the impact of both MenB vaccines on meningococcal carriage and herd protection.113
A clinical trial evaluated meningococcal carriage among university students in England after MenACWY or 4CMenB vaccination. It revealed reduction in carriage observed after 3 months of the second vaccine dose.36 Another study which evaluated carriage in high school students in the US after MenACWY immunization concluded that carriage rates were lower than expected, with nongroupable strains accounting for almost 90% of isolates.36 In contrast, another study assessed meningococcal carriage after MenB vaccination in response to a university outbreak in 2015.114 Total MenB carriage prevalence among sampled students was stable with eradication of the outbreak strain.114 Neither 1–3 doses of rLP2086 nor 1–2 doses of 4CMenB were associated with decreased total or MenB carriage prevalence and are unlikely to provide herd protection in the context of an outbreak response.114
Three studies evaluated MenB carriage in university students after vaccination with MenB OMV in France115 and in the US using rLP208614 or 4CMenB.36 Only one individual vaccinated with MenB OMV was a carrier (serogroup not determined), whereas 16 children in the unvaccinated group were carriers (5 carried MenB).13,14,36,114–116 Four percent (n=31) of the university students immunized with rLP2086 were carriers of MenB at baseline. Those receiving 4CMenB had lower carriage prevalence, that is, only at 3 months after the second vaccine dose, and applied to capsular groups B, C, W, and Y, rather than solely to group B.14,36,114,115 Current evidence on disease prevention is still inconclusive owing to the small number of cases.
To provide more evidence on the effects on meningococcal carriage and prospects on generating herd immunity, a cluster-randomized controlled trial enrolled 24,269 school students ≥14 years of age which used 4CMenB (ACTRN12617000079347 and NCT03089086).117,118 Preliminary results showed that among the enrolled patients with nasopharyngeal carriage, vaccination did not reduce disease causing meningococcus serogroup, including MenB.119 Similarly, no reduction was seen among non-groupable meningococcus carriage.119 As such, the 4CMenB was hypothesized to have no indirect effect.
Another meningococcal carriage trial, led by the Oxford Vaccine Group at the University of Oxford, is ongoing using two licensed MenB vaccines on teenagers 16–18 years old (EUDRACT 2017-004609-42).120 One group will receive 4CMenB while another will receive rLP2086. The vaccines will be given at the beginning of the study and after six months. Two throat swabs will be taken 12 months apart. A further control group will receive 4CMenB vaccine 12 months into the study. The trial will be recruiting students in the UK for 18 months which started in April 2018. Both studies will hopefully provide a better understanding of the effects of the vaccines on the nasopharyngeal carriage in adolescents.
Real-World Experience On Vaccination Against Meningococcal B
Both 4CMenB and rLP2086 vaccines have gained marketing approval in several countries. 4CMenB is approved for use in 39 countries including EU/EEA countries, Australia, Canada, Chile, Colombia, Uruguay, and the US, and has been included in the immunization calendar in Austria, Czech Republic, Andorra, Lithuania, UK, Ireland, Italy, Australia, Canada, and the US.26,121 rLP2086 is approved for use in EU/EEA and the US in individuals 10 years of age and older. We summarized in Table 5 the experiences of the US, the UK, Canada, and Spain on the use of the MenB vaccines in a public health setting.
 |
Table 5 Real-World Data Of MenB Vaccination In Different Countries |
Experience In A Nationwide Routine Infant Immunization (UK)
4CMenB was first licensed in Europe in 2013122 and was included in the UK’s immunization program as part of the routine infant schedule in September 2015.123 During this immunization program, the vaccine was administered to infants as a reduced 2-dose primary series at 2 and 4 months of age with a booster dose at 12 months, alongside their routine immunizations. The resulting coverage in eligible infants was 95.5% for the first dose and 88.6% for the second dose in the primary series.101 Catch-up vaccination was offered to infants attending their routine immunization at 3 months of age with 2 primary doses at 3 and 4 months (coverage was 88.8% and 75.2%, respectively), or at 4 months of age with a single dose (coverage was 76.6%).101
The vaccine effectiveness of the 2-dose primary series was 82.9% against all Men B cases during the first 10 months of the program. Compared with the pre-vaccine period, there was a 50% reduction of the incidence rate ratio of Men B cases among the vaccine-eligible cohort for 4CMenB vaccine, as against a non-significant 14% reduction in the unvaccinated cohort.101
During the surveillance period from September 1, 2015 until May 31, 2017, approximately 1.29 million children aged between 2 and 18 months received more than 3 million doses of 4CMenB vaccine. Nine hundred two (902) reports of suspected adverse events were collected from the UK Yellow Card Scheme, of which 366 (41%) were related to local reactions and 364 (40%) related to fever.104 There were no safety signals related to pre-specified adverse events of interests as the occurrence of these events was similar to background rates.104 There was no indication of reduced compliance with doses of other routine vaccinations. This study is the most comprehensive assessment of 4CMenB vaccine’s safety to date.
Experience In A Selective (US) And Subnational Immunization
In the US, outbreaks of MenB disease occur at universities and other organizations. However, until October 2014, there were no licensed MenB vaccines available for outbreak control. A MenB disease outbreak occurred in 2013–2014 among persons linked to a university in New Jersey.13 This prompted the US Food and Drug Administration to authorize the use of an investigational MenB vaccine to control the outbreak.124 The attack rate among undergraduate students was 134 cases/100,000 and was more than 1400 times greater than the national incidence in this age group. Since cases occurred among students of four undergraduate class years, the entire undergraduate population was targeted for vaccination. Over 5000 students received the first-dose of 4CMenB during the vaccination campaign, achieving 89.1% coverage with the two-dose vaccination series. No MenB cases were reported in vaccinated population regardless of the number of doses administered. However, the rarity of the case precluded the estimation of vaccine effectiveness.
In Canada, to address the high incidence serogroup B, the Saguenay-Lac-Saint-Jean region in Quebec conducted a mass vaccination campaign on individuals ≤20 years old from May 2014 to July 2015.124,103 4CMenB vaccine was given targeting 59,098 individuals, achieving 83% coverage for 1 dose. For the vaccine target age group (0–20 years old), the disease incidence declined by 96% from 11.4 to 0.4 cases/100,000. For non-vaccine targets (>21 years), disease incidence declined by 56% from 1.1 to 0.5 cases/100,000.125 Furthermore, vaccine safety surveillance reports demonstrated an acceptable safety and risk-benefit profile in a large-scale, population-based study.103
While the number of sporadic cases of MenB disease occurring in each year in both the US and Canada was highly varied, the potential impact of MenB vaccines on both sporadic disease and outbreaks is an important consideration in the development of recommendations for the use of licensed MenB vaccines.
Experience In A Limited Release Of The Vaccine For Private Market Use In Spain
The official meniningococal B vaccine recommendation in Spain since 2013 is limited for use in high-risk population126 However, the Spanish Pediatric Association recommends universal vaccination of all infants with this vaccine127 As a result, moderate immunization coverages were achieved as vaccines were only made available in the private market without reimbursements from the national government.128
Based on the data by the Spanish Health Ministry on the utilization of 4CMenB in private setting, 33.55% of the infants (2015–2016 birth cohorts) received at least 2 doses of the vaccine129 Older birth cohorts obtained 19.2% (207–2015) and 6.85% (2003–2006) coverage rates. The highest coverage rate was seen in Galicia and Castilla y Leon region with 58.92% and 54.61% in the youngest birth cohort, respectively. Since the vaccine was not included in the routine immunization program, children may have obtained the vaccine with varying schedules. Vaccine supply was also inconsistent across the observation period.
To estimate the vaccine impact in Spain, the decrease in the number of cases was roughly compared from pre-vaccination period (2013 to 2014 period) to subsequent post-vaccination period (2015-onwards). A decline in cases was observed at 41.7% for 0–5 months and 65.4% for 6–11 months comparing 2013–2014 season (baseline, prior to immunization) and 2017–2018 season (after limited immunization in private market).129,130 There are ongoing efforts to assess effectiveness of the 4CMenB vaccine in Spain using a case–control design.
Conclusion
The global burden of invasive meningococcal disease remains substantial, lingering, and unpredictable. Considering that most cases occur in otherwise healthy subjects, the most effective strategy in the fight against meningococcal disease is prevention through immunization. The immunogenicity, effectiveness, and safety profiles of 4CMenB and rLP2086 have been demonstrated in clinical trials and population-based surveillance studies. Available data indicate that new MenB vaccines have the potential to have a huge impact on the global burden of meningococcal disease. Real-world evidence, although limited, is rapidly accumulating and is encouraging. Post-licensure safety data are reassuring for both vaccines. The preliminary effectiveness assessment for 4CMenB in the UK, Canda, or Spain, looks positively promising. Likewise, as with any new vaccine, we still have knowledge gaps on the ideal age groups to be immunized, the long-term duration of clinical efficacy, or the impact on the nasopharyngeal carriage and eventual herd effect. Universal vaccination programs such as those undertaken in the United Kingdom will provide crucial information in this regard. Furthermore, the potential for MenB vaccines to prevent infection by non-B serogroups appears promising, and the impact on other pathogenic Neisserial species with homologous surface proteins warrants further investigation. Overall, with the remaining burden of invasive meningococcal disease across Europe and other parts of the world, mostly of serogroup B meningococcus, new vaccines should highly be considered for broad use.
Disclosure
FMT has received research grants and/or honoraria as a consultant/advisor and/or speaker and for conducting vaccine trials from GlaxoSmithKline, Sanofi Pasteur MSD, Merck, Sanofi Pasteur, Pfizer, Novartis, and MedImmune Inc. IRC has received research grants and honoraria as an advisor and speaker, and for attending conferences and practical courses from GlaxoSmithKline, Sanofi Pasteur MSD, Merck, Sanofi Pasteur, Novartis, and Pfizer. JGR has received honoraria as advisor and speaker from GlaxoSmithKline, Merck Sharp & Dohme and Pfizer. The authors report no other conflicts of interest in this work.
References
1. Jafri RZ, Ali A, Messonnier NE, et al. Global epidemiology of invasive meningococcal disease. Popul Health Metr. 2013;11(1):17. doi:10.1186/1478-7954-11-17
2. Martinón-Torres F, Salas A, Rivero-Calle I, et al. Life-threatening infections in children in Europe (the EUCLIDS Project): a prospective cohort study. Lancet Child Adolesc Health. 2018;2(6):404–414. doi:10.1016/S2352-4642(18)30113-5
3. Rivero-Calle I, Vilanova-Trillo L, Pardo-Seco J, et al. The burden of pediatric invasive meningococcal disease in Spain (2008–2013). Pediatr Infect Dis J. 2016;35(4):407–413. doi:10.1097/INF.0000000000001048
4. Vetter V, Baxter R, Denizer G, et al. Routinely vaccinating adolescents against meningococcus: targeting transmission & disease. Expert Rev Vaccines. 2016;15(5):641–658. doi:10.1586/14760584.2016.1130628
5. Soriano-Gabarro M, Wolter J, Hogea C, Vyse A. Carriage of Neisseria meningitidis in Europe: a review of studies undertaken in the region. Expert Rev Anti Infect Ther. 2011;9(9):761–774. doi:10.1586/eri.11.89
6. Christensen H, May M, Bowen L, Hickman M, Trotter CL. Meningococcal carriage by age: a systematic review and meta-analysis. Lancet Infect Dis. 2010;10(12):853–861. doi:10.1016/S1473-3099(10)70251-6
7. Martinon-Torres F. Deciphering the burden of meningococcal disease: conventional and under-recognized elements. J Adolesc Health. 2016;59(2 Suppl):S12–S20. doi:10.1016/j.jadohealth.2016.03.041
8. Pace D, Pollard AJ. Meningococcal disease: clinical presentation and sequelae. Vaccine. 2012;30 Suppl 2:B3–B9. doi:10.1016/j.vaccine.2011.12.062
9. Serra LC, York LJ, Gamil A, Balmer P, Webber C. A Review of meningococcal disease and vaccination recommendations for travelers. Infect Dis Ther. 2018;7(2):219–234. doi:10.1007/s40121-018-0196-z
10. Grupo de trabajo MenCC 2012. Ministerio de Sanidad SSeI. Revisión del programa de vacunación frente a enfermedad meningocócica por serogrupo C: Ponencia de Programa y Registro de Vacunaciones. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualidad; 2013.
11. Pelton SI. The global evolution of meningococcal epidemiology following the introduction of meningococcal vaccines. J Adolesc Health. 2016;59 2 Suppl:S3–S11. doi:10.1016/j.jadohealth.2016.04.012
12. Sridhar S, Greenwood B, Head C, et al. Global incidence of serogroup B invasive meningococcal disease: a systematic review. Lancet Infect Dis. 2015;15(11):1334–1346. doi:10.1016/S1473-3099(15)00217-0
13. McNamara LA, Shumate AM, Johnsen P, et al. First use of a serogroup B meningococcal vaccine in the US in response to a university outbreak. Pediatrics. 2015;135(5):798–804. doi:10.1542/peds.2014-4015
14. Soeters HM, McNamara LA, Whaley M, et al. Serogroup B meningococcal disease outbreak and carriage evaluation at a college – Rhode Island, 2015. MMWR Morb Mortal Wkly Rep. 2015;64(22):606–607.
15. Schildkamp RL, Lodder MC, Bijlmer HA, Dankert J, Scholten RJ. Clinical manifestations and course of meningococcal disease in 562 patients. Scand J Infect Dis. 1996;28(1):47–51. doi:10.3109/00365549609027149
16. Ruth A, McCracken CE, Fortenberry JD, Hall M, Simon HK, Hebbar KB. Pediatric severe sepsis: current trends and outcomes from the Pediatric Health Information Systems database. Pediatr Crit Care Med. 2014;15(9):828–838. doi:10.1097/PCC.0000000000000254
17. Rivero Calle I, Rodriguez-Tenreiro Sanchez C, Martinon-Torres F. [Meningococcal vaccines. Global epidemiological situation and strategies for prevention by vaccination]. Enferm Infecc Microbiol Clin. 2015;33(4):257–267. doi:10.1016/j.eimc.2015.03.001
18. Finne J, Leinonen M, Makela PH. Antigenic similarities between brain components and bacteria causing meningitis: implications for vaccine development and pathogenesis. Lancet. 1983;2(8346):355–357. doi:10.1016/s0140-6736(83)90340-9
19. Hayrinen J, Jennings H, Raff HV, et al. Antibodies to polysialic acid and its N-propyl derivative- binding properties and interaction with human embryonal brain glycopeptides. J Infect Dis. 1995;171:1481–1490. doi:10.1093/infdis/171.6.1481
20. Montero-Martin M, Inwald DP, Carrol ED, Martinon-Torres F. Prognostic markers of meningococcal disease in children: recent advances and future challenges. Expert Rev Anti Infect Ther. 2014;12(11):1357–1369. doi:10.1586/14787210.2014.966079
21. Mayr FB, Yende S, Angus DC. Epidemiology of severe sepsis. Virulence. 2014;5(1):4–11. doi:10.4161/viru.27372
22. Martinon-Torres F, Png E, Khor CC, et al. Natural resistance to Meningococcal Disease related to CFH loci: meta-analysis of genome-wide association studies. Sci Rep. 2016;6:35842. doi:10.1038/srep35842
23. Martin NG, Sadarangani M, Pollard AJ, Goldacre MJ. Hospital admission rates for meningitis and septicaemia caused by Haemophilus influenzae, Neisseria meningitidis, and Streptococcus pneumoniae in children in England over five decades: a population-based observational study. Lancet Infect Dis. 2014;14(5):397–405. doi:10.1016/S1473-3099(14)70027-1
24. Wang NY, Pollard AJ. The next chapter for group B meningococcal vaccines. Crit Rev Microbiol. 2018;44(1):95–111. doi:10.1080/1040841X.2017.1329276
25. Donnelly J, Medini D, Boccadifuoco G, et al. Qualitative and quantitative assessment of meningococcal antigens to evaluate the potential strain coverage of protein-based vaccines. Proc Natl Acad Sci U S A. 2010;107(45):19490–19495. doi:10.1073/pnas.1013758107
26. Toneatto D, Pizza M, Masignani V, Rappuoli R. Emerging experience with meningococcal serogroup B protein vaccines. Expert Rev Vaccines. 2017;16(5):433–451. doi:10.1080/14760584.2017.1308828
27. Europeans Medicines Agency. European public assessment report - Bexsero product information. 2018. Available from: https://www.ema.europa.eu/documents/product-information/bexsero-epar-product-information_en.pdf.
28. Findlow J, Borrow R, Snape MD, et al. Multicenter, open-label, randomized phase II controlled trial of an investigational recombinant Meningococcal serogroup B vaccine with and without outer membrane vesicles, administered in infancy. Clin Infect Dis. 2010;51(10):1127–1137. doi:10.1086/656741
29. Snape MD, Saroey P, John TM, et al. Persistence of bactericidal antibodies following early infant vaccination with a serogroup B meningococcal vaccine and immunogenicity of a preschool booster dose. Can Med J Assoc. 2013;185(15):715–724. doi:10.1503/cmaj.130257
30. Gossger N, Snape MD, Yu LM, et al. Immunogenicity and tolerability of recombinant serogroup B meningococcal vaccine administered with or without routine infant vaccinations according to different immunization schedules. J Am Med Assoc. 2012;307(6):573–582. doi:10.1001/jama.2012.85
31. Nissen MD, Marshall HS, Richmond PC, et al. A randomized, controlled, phase 1/2 trial of a Neisseria meningitidis serogroup B bivalent rLP2086 vaccine in healthy children and adolescents. Pediatr Infect Dis J. 2013;32(4):364–371. doi:10.1097/INF.0b013e31827b0d24
32. Marshall HS, Richmond PC, Nissen MD, et al. A phase 2 open-label safety and immunogenicity study of a meningococcal B bivalent rLP2086 vaccine in healthy adults. Vaccine. 2013;31(12):1569–1575. doi:10.1016/j.vaccine.2013.01.021
33. Vesikari T, Ostergaard L, Diez-Domingo J, et al. Meningococcal serogroup B bivalent rLP2086 vaccine elicits broad and robust serum bactericidal responses in healthy adolescents. J Pediatric Infect Dis Soc. 2016;5(2):152–160. doi:10.1093/jpids/piv039
34. Giuliani MM, Biolchi A, Serruto D, et al. Measuring antigen-specific bactericidal responses to a multicomponent vaccine against serogroup B meningococcus. Vaccine. 2010;28(31):5023–5030. doi:10.1016/j.vaccine.2010.05.014
35. Perrett KP, McVernon J, Richmond PC, et al. Immune responses to a recombinant, four-component, meningococcal serogroup B vaccine (4CMenB) in adolescents: a phase III, randomized, multicentre, lot-to-lot consistency study. Vaccine. 2015;33(39):5217–5224. doi:10.1016/j.vaccine.2015.06.103
36. Read RC, Baxter D, Chadwick DR, et al. Effect of a quadrivalent meningococcal ACWY glycoconjugate or a serogroup B meningococcal vaccine on meningococcal carriage: an observer-blind, phase 3 randomised clinical trial. Lancet. 2014;384(9960):2123–2131. doi:10.1016/S0140-6736(14)60842-4
37. Santolaya ME, O’Ryan ML, Valenzuela MT, et al. Immunogenicity and tolerability of a multicomponent meningococcal serogroup B (4CMenB) vaccine in healthy adolescents in Chile: a phase 2b/3 randomised, observer-blind, placebo-controlled study. Lancet. 2012;379(9816):617–624. doi:10.1016/S0140-6736(11)61713-3
38. Safadi P. MA, Martinon-Torres F, Weckx LY, et al. Immunogenicity and safety of concomitant administration of meningococcal serogroup B (4CMenB) and serogroup C (MenC-CRM) vaccines in infants: A phase 3b, randomized controlled trial. Vaccine. 2017;35(16):2052–2059. doi:10.1016/j.vaccine.2017.03.002
39. Harris SL, Donald RG, Hawkins JC, et al. Neisseria meningitidis Serogroup B Vaccine, Bivalent rLP2086, Induces Broad Serum Bactericidal Activity Against Diverse Invasive Disease Strains Including Outbreak Strains. Pediatr Infect Dis J. 2017;36(2):216–223. doi:10.1097/INF.0000000000001399
40. Martinon-Torres F, Safadi MAP, Martinez AC, et al. Reduced schedules of 4CMenB vaccine in infants and catch-up series in children: immunogenicity and safety results from a randomised open-label phase 3b trial. Vaccine. 2017;35(28):3548–3557. doi:10.1016/j.vaccine.2017.05.023
41. Kuhdari P, Stefanati A, Lupi S, Valente N, Gabutti G. Meningococcal B vaccination: real-world experience and future perspectives. Pathog Glob Health. 2016;110(4–5):148–156. doi:10.1080/20477724.2016.1195072
42. Bianchi A, Fantoni S, Prugnola A. Meningococcal B vaccine and the vision of a meningitis free world. J Prev Med Hyg. 2015;56:e140–e143.
43. Hong E, Giuliani MM, Deghmane AE, et al. Could the multicomponent meningococcal serogroup B vaccine (4CMenB) control Neisseria meningitidis capsular group X outbreaks in Africa?. Vaccine. 2013;31(7):1113–1116. doi:10.1016/j.vaccine.2012.12.022
44. Gloria MCO, Lemos APS, Biolchi A. Impact vaccination with the Novartis meningococcal serogroup B vaccine 4CMenB (BEXSERO®) on non-serogroup B disease burden in Brazil.
45. Vogel U, Stefanelli P, Vazquez J, Taha MK, Claus H, Donnelly J. The use of vaccine antigen characterization, for example by MATS, to guide the introduction of meningococcus B vaccines. Vaccine. 2012;30 Suppl 2:B73–B77. doi:10.1016/j.vaccine.2011.12.061
46. Parikh SR, Newbold L, Slater S, et al. Meningococcal serogroup B strain coverage of the multicomponent 4CMenB vaccine with corresponding regional distribution and clinical characteristics in England, Wales, and Northern Ireland, 2007–08 and 2014–15: a qualitative and quantitative assessment. Lancet Infect Dis. 2017;17(7):754–762. doi:10.1016/S1473-3099(17)30170-6
47. Carter NJ. Multicomponent meningococcal serogroup B vaccine (4CMenB; Bexsero((R))): a review of its use in primary and booster vaccination. BioDrugs. 2013;27(3):263–274. doi:10.1007/s40259-013-0029-2
48. Giuliani MM, Adu-Bobie J, Comanducci M, et al. A universal vaccine for serogroup B meningococcus. Proc Natl Acad Sci U S A. 2006;103(29):10834–10839. doi:10.1073/pnas.0603940103
49. Tettelin H, Saunders NJ, Heidelberg J, et al. Complete genome sequence of Neisseria meningitidis serogroup B strain MC58. Science. 2000;287(5459):1809–1815. doi:10.1126/science.287.5459.1809
50. Rappuoli R, Bottomley MJ, D’Oro U, Finco O, De Gregorio E. Reverse vaccinology 2.0: human immunology instructs vaccine antigen design. J Exp Med. 2016;213(4):469–481. doi:10.1084/jem.20151960
51. Seib KL, Zhao X, Rappuoli R. Developing vaccines in the era of genomics: a decade of reverse vaccinology. Clin Microbiol Infect. 2012;18 Suppl 5:109–116. doi:10.1111/j.1469-0691.2012.03939.x
52. Serruto D, Bottomley MJ, Ram S, Giuliani MM, Rappuoli R. The new multicomponent vaccine against meningococcal serogroup B, 4CMenB: immunological, functional and structural characterization of the antigens. Vaccine. 2012;30 Suppl 2:B87–B97. doi:10.1016/j.vaccine.2012.01.033
53. Pizza M, Scarlato V, Masignani V, et al. Identification of vaccine candidates against serogroup B meningococcus by whole-genome sequencing. Science. 2000;287:1816–1820. doi:10.1126/science.287.5459.1816
54. Masignani V, Comanducci M, Giuliani MM, et al. Vaccination against Neisseria meningitidis using three variants of the lipoprotein GNA1870. J Exp Med. 2003;197(6):789–799. doi:10.1084/jem.20021911
55. Capecchi B, Adu-Bobie J, Di Marcello F, et al. Neisseria meningitidis NadA is a new invasin which promotes bacterial adhesion to and penetration into human epithelial cells. Mol Microbiol. 2005;55(3):687–698. doi:10.1111/j.1365-2958.2004.04423.x
56. Giuliani M, Bartolini E, Galli B, et al. Human protective response induced by meningococcus B vaccine is mediated by the synergy of multiple bactericidal epitopes. Sci Rep. 2018;8(1):3700. doi:10.1038/s41598-018-22057-7
57. Vu DM, Wong TT, Granoff DM. Cooperative serum bactericidal activity between human antibodies to meningococcal factor H binding protein and neisserial heparin binding antigen. Vaccine. 2011;29(10):1968–1973. doi:10.1016/j.vaccine.2010.12.075
58. McNeil LK, Zagursky RJ, Lin SL, et al. Role of factor H binding protein in Neisseria meningitidis virulence and its potential as a vaccine candidate to broadly protect against meningococcal disease. Microbiol Mol Biol Rev. 2013;77(2):234–252. doi:10.1128/MMBR.00056-12
59. Zlotnick GW, Jones TR, Liberator P, et al. The discovery and development of a novel vaccine to protect against Neisseria meningitidis Serogroup B Disease. Hum Vaccin Immunother. 2015;11(1):5–13. doi:10.4161/hv.34293
60. McNeil LK, Donald RGK, Gribenko A, et al. Predicting the Susceptibility of Meningococcal Serogroup B Isolates to Bactericidal Antibodies Elicited by Bivalent rLP2086, a Novel Prophylactic Vaccine. mBio. 2018;9(2):e00036–e00018. doi:10.1128/mBio.00036-18
61. Murphy E, Andrew L, Lee KL, et al. Sequence diversity of the factor H binding protein vaccine candidate in epidemiologically relevant strains of serogroup B neisseria meningitidis. J Infect Dis. 2009;200(3):379–389. doi:10.1086/600141
62. Luo Y, Friese OV, Runnels HA, et al. The dual role of lipids of the lipoproteins in trumenba, a self-adjuvanting vaccine against meningococcal meningitis B disease. AAPS J. 2016;18(6):1562–1575. doi:10.1208/s12248-016-9979-x
63. Rosenstein NE, Perkins BA, Stephens DS, Popovic T, Hughes JM. Meningococcal disease. N Engl J Med. 2001;344(18):1378–1388. doi:10.1056/NEJM200105033441807
64. Gandhi A, Balmer P, York LJ. Characteristics of a new meningococcal serogroup B vaccine, bivalent rLP2086 (MenB-FHbp; Trumenba(R)). Postgrad Med. 2016;128(6):548–556. doi:10.1080/00325481.2016.1203238
65. Bjune G, Høiby EA, Grønnesby JK, et al. Effect of outer membrane vesicle vaccine against group B meningococcal disease in Norway. Lancet. 1991;338(8775):1093–1096. doi:10.1016/0140-6736(91)91961-s
66. Sierra GV, Campa HC, Varcacel NM, et al. Vaccine against group B Neisseria meningitidis: protection trial and mass vaccination results in Cuba. NIPH Ann. 1991;14(2):
67. van Alphen L, van den Dobbelsteen G. Meningococcal B vaccine development and evaluation of efficacy. Hum Vaccines. 2014;4(2):158–161. doi:10.4161/hv.4.2.4871
68. Beernink PT, Shaughnessy J, Pajon R, Braga EM, Ram S, Granoff DM. The effect of human factor H on immunogenicity of meningococcal native outer membrane vesicle vaccines with over-expressed factor H binding protein. PLoS Pathog. 2012;8(5):e1002688. doi:10.1371/journal.ppat.1002688
69. Kimura A, Toneatto D, Kleinschmidt A, Wang H, Dull P. Immunogenicity and safety of a multicomponent meningococcal serogroup B vaccine and a quadrivalent meningococcal CRM197 conjugate vaccine against serogroups A, C, W-135, and Y in adults who are at increased risk for occupational exposure to meningococcal isolates. Clin Vaccine Immunol. 2011;18(3):483–486. doi:10.1128/CVI.00304-10
70. Toneatto D, Ismaili S, Ypma E, Vienken K, Oster P, Dull P. The first use of an investigational multicomponent meningococcal serogroup B vaccine (4CMenB) in humans. Hum Vaccines. 2014;7(6):646–653. doi:10.4161/hv.7.6.15482
71. Vesikari T, Esposito S, Prymula R, et al. Immunogenicity and safety of an investigational multicomponent, recombinant, meningococcal serogroup B vaccine (4CMenB) administered concomitantly with routine infant and child vaccinations: results of two randomised trials. Lancet. 2013;381(9869):825–835. doi:10.1016/S0140-6736(12)61961-8
72. Richmond PC, Marshall HS, Nissen MD, et al. Safety, immunogenicity, and tolerability of meningococcal serogroup B bivalent recombinant lipoprotein 2086 vaccine in healthy adolescents: a randomised, single-blind, placebo-controlled, phase 2 trial. Lancet Infect Dis. 2012;12(8):597–607. doi:10.1016/S1473-3099(12)70087-7
73. Van den Bruel A, Thompson MJ, Haj-Hassan T, et al. Diagnostic value of laboratory tests in identifying serious infections in febrile children: systematic review. BMJ. 2011;342:d3082. doi:10.1136/bmj.d3082
74. Block SL, Szenborn L, Daly W, et al. A comparative evaluation of two investigational meningococcal ABCWY vaccine formulations: results of a phase 2 randomized, controlled trial. Vaccine. 2015;33(21):2500–2510. doi:10.1016/j.vaccine.2015.03.001
75. Goldschneider I, Gotschlich EC, Artenstein MS. Human immunity to the meningococcus. I. The role of humoral antibodies. J Exp Med. 1969;129(6):1307–1326. doi:10.1084/jem.129.6.1307
76. Martinon-Torres F, Nolan T, Toneatto D, Banzhoff A. Persistence of the immune response after 4CMenB vaccination, and the response to an additional booster dose in infants, children, adolescents, and young adults. Hum Vaccin Immunother. 2019;1–12. doi:10.1080/21645515.2019.1627159
77. Flacco ME, Manzoli L, Rosso A, et al. Immunogenicity and safety of the multicomponent meningococcal B vaccine (4CMenB) in children and adolescents: a systematic review and meta-analysis. Lancet Infect Dis. 2018;18(4):461–472. doi:10.1016/S1473-3099(18)30048-3
78. Martinon-Torres F, Carmona Martinez A, Simko R, et al. Antibody persistence and booster responses 24–36 months after different 4CMenB vaccination schedules in infants and children: A randomised trial. J Infect. 2018;76(3):258–269. doi:10.1016/j.jinf.2017.12.005
79. Nolan T, Santolaya ME, de Looze F, et al. Antibody persistence and booster response in adolescents and young adults 4 and 7.5 years after immunization with 4CMenB vaccine. Vaccine. 2019;37(9):1209–1218. doi:10.1016/j.vaccine.2018.12.059
80. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
81. Schlapbach LJ, Straney L, Alexander J, et al. Mortality related to invasive infections, sepsis, and septic shock in critically ill children in Australia and New Zealand, 2002–13: a multicentre retrospective cohort study. Lancet Infect Dis. 2015;15(1):46–54. doi:10.1016/S1473-3099(14)71003-5
82. Muse D, Christensen S, Bhuyan P, et al. A Phase 2, Randomized, Active-controlled, Observer-blinded Study to Assess the Immunogenicity, Tolerability and Safety of Bivalent rLP2086, a Meningococcal Serogroup B Vaccine, Coadministered With Tetanus, Diphtheria and Acellular Pertussis Vaccine and Serogroup A, C, Y and W-135 Meningococcal Conjugate Vaccine in Healthy US Adolescents. Pediatr Infect Dis J. 2016;35(6):673–682. doi:10.1097/INF.0000000000001124
83. Senders S, Bhuyan P, Jiang Q, et al. Immunogenicity, tolerability and safety in adolescents of bivalent rLP2086, a meningococcal serogroup B vaccine, coadministered with quadrivalent human papilloma virus vaccine. Pediatr Infect Dis J. 2016;35(5):548–554. doi:10.1097/INF.0000000000001072
84. Marshall HS, Richmond PC, Beeslaar J, et al. Meningococcal serogroup B-specific responses after vaccination with bivalent rLP2086: 4 year follow-up of a randomised, single-blind, placebo-controlled, phase 2 trial. Lancet Infect Dis. 2017;17(1):58–67. doi:10.1016/S1473-3099(16)30314-0
85. Lujan E, Partridge E, Giuntini S, Ram S, Granoff DM. Breadth and duration of meningococcal serum bactericidal activity in health care workers and microbiologists immunized with the MenB-FHbp vaccine. Clin Vaccine Immunol. 2017;24:8. doi:10.1128/CVI.00121-17
86. Martinón-Torres F, Bernatowska E, Shcherbina A, et al. Meningococcal B vaccine immunogenicity in children with defects in complement and splenic function. Pediatrics. 2018;141(6):e20174250. doi:10.1542/peds.2017-4250
87. Hernando Real S, Vega Castano S, Pajares Garcia R. Meningococcemia in vaccinated patient under treatment with eculizumab. Enferm Infecc Microbiol Clin. 2017;35(3):200–201. doi:10.1016/j.eimc.2016.02.015
88. McNamara LA, Topaz N, Wang X, Hariri S, Fox L, MacNeil JR. High risk for invasive meningococcal disease among patients receiving eculizumab (Soliris) despite receipt of meningococcal vaccine. Am J Transplant. 2017;17(9):2481–2484. doi:10.1111/ajt.2017.17.issue-9
89. Parikh SR, Lucidarme J, Bingham C, et al. Meningococcal B vaccine failure with a penicillin-resistant strain in a young adult on long-term eculizumab. Pediatrics. 2017;140:3. doi:10.1542/peds.2017-0685
90. Tozer SJ, Whiley DM, Smith HV The use of the Meningococcal Antigen Typing System (MATS) to assess Australian epidemiology and meningococcal strain coverage with multicomponent serogroup B vaccine.
91. Harris SL, Tan C, Andrew L, et al. The bivalent factor H binding protein meningococcal serogroup B vaccine elicits bactericidal antibodies against representative non-serogroup B meningococci. Vaccine. 2018;36(45):6867–6874. doi:10.1016/j.vaccine.2018.05.081
92. Petousis-Harris H, Paynter J, Morgan J, et al. Effectiveness of a group B outer membrane vesicle meningococcal vaccine against gonorrhoea in New Zealand: a retrospective case-control study. Lancet. 2017;390(10102):1603–1610. doi:10.1016/S0140-6736(17)31449-6
93. Seib KL. Gonorrhoea vaccines: a step in the right direction. Lancet. 2017;390(10102):1567–1569. doi:10.1016/S0140-6736(17)31605-7
94. Semchenko EA, Tan A, Borrow R, Seib KL. The serogroup B meningococcal vaccine Bexsero elicits antibodies to Neisseria gonorrhoeae. Clin Infect Dis. 2018.
95. Rajam G, Stella M, Kim E, et al. Meningococcal antigen typing system (MATS)-based neisseria meningitidis serogroup B coverage prediction for the MenB-4C vaccine in the United States. mSphere. 2017;2(6). doi:10.1128/mSphere.00261-17
96. Plikaytis BD, Stella M, Boccadifuoco G, et al. Interlaboratory standardization of the sandwich enzyme-linked immunosorbent assay designed for MATS, a rapid, reproducible method for estimating the strain coverage of investigational vaccines. Clin Vaccine Immunol. 2012;19(10):1609–1617. doi:10.1128/CVI.00202-12
97. Vernikos G, Medini D. Bexsero(R) chronicle. Pathog Glob Health. 2014;108(7):305–316. doi:10.1179/2047773214Y.0000000162
98. Medini D, Stella M, Mats: WJ. Global coverage estimates for 4CMenB, a novel multicomponent meningococcal B vaccine. Vaccine. 2015;33(23):2629–2636. doi:10.1016/j.vaccine.2015.04.015
99. Jiang HQ, Hoiseth SK, Harris SL, et al. Broad vaccine coverage predicted for a bivalent recombinant factor H binding protein based vaccine to prevent serogroup B meningococcal disease. Vaccine. 2010;28(37):6086–6093. doi:10.1016/j.vaccine.2010.06.083
100. Prymula R, Esposito S, Zuccotti GV, et al. A phase 2 randomized controlled trial of a multicomponent meningococcal serogroup B vaccine (I). Hum Vaccin Immunother. 2014;10(7):1993–2004. doi:10.4161/hv.28666
101. Parikh SR, Andrews NJ, Beebeejaun K, et al. Effectiveness and impact of a reduced infant schedule of 4CMenB vaccine against group B meningococcal disease in England: a national observational cohort study. Lancet. 2016;388(10061):2775–2782. doi:10.1016/S0140-6736(16)31921-3
102. De Wals P, Deceuninck G, Lefebvre B, et al. Impact of an Immunization Campaign to Control an Increased Incidence of Serogroup B Meningococcal Disease in One Region of Quebec, Canada. Clin Infect Dis. 2017;64(9):1263–1267. doi:10.1093/cid/cix154
103. De Serres G, Billard MN, Gariepy MC, et al. Short-term safety of 4CMenB vaccine during a mass meningococcal B vaccination campaign in Quebec, Canada. Vaccine. 2018;36(52):8039–8046. doi:10.1016/j.vaccine.2018.10.095
104. Bryan P, Seabroke S, Wong J, et al. Safety of multicomponent meningococcal group B vaccine (4CMenB) in routine infant immunisation in the UK: a prospective surveillance study. Lancet Child Adolesc Health. 2018;2(6):395–403. doi:10.1016/S2352-4642(18)30103-2
105. De Serres G, Billard MN, Gariepy MC, Rouleau I, Toth E, Landry M. Rapport final de surveillance de la sécurité de la vaccination des jeunes de 20 ans et moins contre le méningocoque de sérogroupe B au Saguenay–Lac-Saint-Jean. Quebec (Canada): Institut National de Santé Publique du Québec; 2016.
106. Jones R. Costs of pediatric assessment. Br J Healthcare Manage. 2013;17(2):57–63. doi:10.12968/bjhc.2011.17.2.57
107. Marshall HS, Chen G, Clarke M, Ratcliffe J. Adolescent, parent and societal preferences and willingness to pay for meningococcal B vaccine: A Discrete Choice Experiment. Vaccine. 2016;34(5):671–677. doi:10.1016/j.vaccine.2015.11.075
108. Ostergaard L, Lucksinger GH, Absalon J, et al. A phase 3, randomized, active-controlled study to assess the safety and tolerability of meningococcal serogroup B vaccine bivalent rLP2086 in healthy adolescents and young adults. Vaccine. 2016;34(12):1465–1471. doi:10.1016/j.vaccine.2016.01.044
109. Vesikari T, Ostergaard L, Beeslaar J, et al. Persistence and 4-year boosting of the bactericidal response elicited by two- and three-dose schedules of MenB-FHbp: A phase 3 extension study in adolescents. Vaccine. 2019;37(12):1710–1719. doi:10.1016/j.vaccine.2018.11.073
110. Marshall HS, Richmond PC, Nissen MD, et al. Safety and immunogenicity of a meningococcal B bivalent rLP2086 vaccine in healthy toddlers aged 18–36 months: a phase 1 randomized-controlled clinical trial. Pediatr Infect Dis J. 2012;31(10):1061–1068. doi:10.1097/INF.0b013e31826327e4
111. Ahluwalla J. Trumenba pediatric safety and utilization review for the pediatric advisory committee (PAC). 2018. Available from: https://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/PediatricAdvisoryCommittee/UCM599285.pdf.
112. Fiorito TM, Baird GL, Alexander-Scott N, et al. Adverse events following vaccination with bivalent rLP2086 (Trumenba(R)): an observational, longitudinal study during a college outbreak and a systematic review. Pediatr Infect Dis J. 2018;37(1):e13–e19. doi:10.1097/INF.0000000000001742
113. Balmer P, Burman C, Serra L, York LJ. Impact of meningococcal vaccination on carriage and disease transmission: a review of the literature. Hum Vaccin Immunother. 2018;14(5):1118–1130. doi:10.1080/21645515.2018.1454570
114. McNamara LA, Thomas JD, MacNeil J, et al. Meningococcal carriage following a vaccination campaign with MenB-4C and MenB-FHbp in response to a university serogroup B meningococcal disease outbreak-Oregon, 2015–2016. J Infect Dis. 2017;216(9):1130–1140. doi:10.1093/infdis/jix446
115. Delbos V, Lemee L, Benichou J, et al. Impact of MenBvac, an outer membrane vesicle (OMV) vaccine, on the meningococcal carriage. Vaccine. 2013;31(40):4416–4420. doi:10.1016/j.vaccine.2013.06.080
116. Soeters HM, Whaley M, Alexander-Scott N, et al. Meningococcal carriage evaluation in response to a serogroup B meningococcal disease outbreak and mass vaccination campaign at a college-Rhode Island, 2015–2016. Clin Infect Dis. 2017;64(8):1115–1122. doi:10.1093/cid/cix091
117. University of Adelaide. South Australian meningococcal B vaccine herd immunity study (B Part of It). clinicaltrialsgov. 2017. Available from: https://clinicaltrials.gov/ct2/show/record/NCT03089086. NLM identifier: NCT03089086.
118. University of Adelaide. A cluster randomised controlled trial to assess the impact of meningococcal B vaccine 4CMenB on nasopharyngeal carriage of N. Meningitidis in adolescents in South Australia. Australian New Zealand Clinical Trials Registry. 2017. Available from: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=371948.
119. Mcmillan M, Walters L, Koehler A, et al. Impact of 4cmenb vaccine on meningococcal carriage density in adolescents.
120. University of Oxford. Evaluating the effect of immunisation with group B meningococcal vaccines on meningococcal carriage. EU Clinical Trials Register. 2018. Available from: www.clinicaltrialsregister.eu.
121. World Health Organization. WHO vaccine-preventable diseases: monitoring system. 2018 global summary. 2018. Available from: http://apps.who.int/immunization_monitoring/globalsummary.
122. European Medicines Agency. Bexsero authorization details and assessment history. 2018. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/bexsero#authorisation-details-section.
123. Public Health England. Introduction of MenB vaccination for infants. 2015. Available from: https://www.gov.uk/government/publications/menb-vaccination-introduction-from-1-september-2015.
124. Cohn AC, MacNeil JR, Clark TA, et al. Prevention and control of meningococcal disease: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2013;62(Rr–2):1–28.
125. Institut national de santé publique. Impact épidémiologique de la campagne de vaccination contre le méningocoque de sérogroupe B dans la région du Saguenay-Lac-Saint-Jean, en 2014: rapport au 30 Juin 2018. Quebec (Canada): Institut national de santé publique; 2018.
126. Grupo de trabajo MenB Ponencia de Programa y Registro de Vacunaciones. Vacuna frente a enfermedad meningocócica invasora por serogrupo B y su posible utilización en salud pública, Junio de 2013. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualidad; 2015.
127. Moreno-Pérez D, Álvarez García FJ, Arístegui Fernández J, et al. Vaccination against meningococcal B disease. public statement of the advisory committee on vaccines of the Spanish Association of Paediatrics (CAV-AEP). An Pediatr. 2015;82(3):
128. Martinon-Torres F, Trilla A. Meningococcal disease: can we predict the unpredictable? Med Clin. 2019.
129. Pearson GA, Ward-Platt M, Kelly D. How children die: classifying child deaths. Arch Dis Child. 2011;96(10):922–926. doi:10.1136/adc.2009.177089
130. Vila Perez D, Jordan I, Esteban E, et al. Prognostic factors in pediatric sepsis study, from the Spanish Society of Pediatric Intensive Care. Pediatr Infect Dis J. 2014;33(2):152–157. doi:10.1097/01.inf.0000435502.36996.72
131. Sumpter R, Brunklaus A, McWilliam R, Dorris L. Health-related quality-of-life and behavioural outcome in survivors of childhood meningitis. Brain Inj. 2011;25(13–14):1288–1295. doi:10.3109/02699052.2011.613090
132. Delany I, Rappuoli R, Seib KL. Vaccines, reverse vaccinology, and bacterial pathogenesis. Cold Spring Harb Perspect Med. 2013;3(5):a012476. doi:10.1101/cshperspect.a015511
133. Vacca I, Del Tordello E, Gasperini G, et al. Neisserial heparin binding antigen (NHBA) contributes to the adhesion of neisseria meningitidis to human epithelial cells. PLoS One. 2016;11(10):e0162878. doi:10.1371/journal.pone.0162878
134. Serruto D, Spadafina T, Ciucchi L, et al. Neisseria meningitidis GNA2132, a heparin-binding protein that induces protective immunity in humans. Proc Natl Acad Sci U S A. 2010;107(8):3770–3775. doi:10.1073/pnas.0915162107
135. Viner RM, Booy R, Johnson H, et al. Outcomes of invasive meningococcal serogroup B disease in children and adolescents (MOSAIC): a case-control study. Lancet Neurol. 2012;11(9):774–783. doi:10.1016/S1474-4422(12)70180-1
136. Comanducci M, Bambini S, Brunelli B, et al. NadA, a Novel Vaccine Candidate ofNeisseria meningitidis. J Exp Med. 2002;195(11):1445–1454. doi:10.1084/jem.20020407
137. Bambini S, Piet J, Muzzi A, et al. An analysis of the sequence variability of meningococcal fHbp, NadA and NHBA over a 50-year period in the Netherlands. PLoS One. 2013;8(5):e65043. doi:10.1371/journal.pone.0065043
138. Granoff DM. Review of meningococcal group B vaccines. Clin Infect Dis. 2010;50 Suppl 2:S54–S65. doi:10.1086/648966
139. Costa I, Pajon R, Granoff DM. Human factor H (FH) impairs protective meningococcal anti-FHbp antibody responses and the antibodies enhance FH binding. MBio. 2014;5(5):e01625–e01614. doi:10.1128/mBio.01625-14
140. Foltyn Zadura A, Zipfel PF, Bokarewa MI, et al. Factor H autoantibodies and deletion of Complement Factor H-Related protein-1 in rheumatic diseases in comparison to atypical hemolytic uremic syndrome. Arthritis Res Ther. 2012;14(4):R185. doi:10.1186/ar4016
141. Partridge E, Lujan E, Giuntini S, Vu DM, Granoff DM. The role of anti-NHba antibody in bactericidal activity elicited by the meningococcal serogroup B vaccine, MenB-4C. Vaccine. 2017;35(33):4236–4244. doi:10.1016/j.vaccine.2017.06.020
142. Lucidarme J, Tan L, Exley RM, Findlow J, Borrow R, Tang CM. Characterization of Neisseria meningitidis isolates that do not express the virulence factor and vaccine antigen factor H binding protein. Clin Vaccine Immunol. 2011;18(6):1002–1014. doi:10.1128/CVI.00055-11
143. Rappuoli R, Pizza M, Masignani V, Vadivelu K. Meningococcal B vaccine (4CMenB): the journey from research to real world experience. Expert Rev Vaccines. 2018;17(12):1111–1121. doi:10.1080/14760584.2018.1547637
144. Grupo de Trabajo de “uso de 4CMenB en situaciones especiales”. Recomendaciones de utilización de la vacuna frente a enfermedad meningocócica por serogrupo B. Madrid: Ministerio de Sanidad, Servicios Sociales e Igualidad; 2015.
145. Fisher EA, Poissant T, Luedtke P, Leman R, Young C, Cieslak P. Evaluation of mass vaccination clinics in response to a serogroup B meningococcal disease outbreak at a large, public university-Oregon, 2015. J Adolesc Health. 2018;63(2):151–156. doi:10.1016/j.jadohealth.2018.03.018
146. Abad R, Orlando L, Rigat F, Boccadifuoco G, Comanducci M, Muzzi A. Strain coverage of a meningococcal multicomponent (4CMenB) vaccine in Spain.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.