")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Melatonin Receptor 1B Genetic Variants on Susceptibility to Gestational Diabetes Mellitus: A Hospital-Based Case–Control Study in Wuhan, Central China
Authors Liu J , Li W, Liu B, Dai A , Wang Y, She L , Zhang P, Zheng W, Dai Q, Yang M
Received 27 October 2021
Accepted for publication 1 April 2022
Published 20 April 2022 Volume 2022:15 Pages 1207—1216
DOI https://doi.org/10.2147/DMSO.S345036
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Ming-Hui Zou
Jianqiong Liu,1,* Wei Li,1,* Bei Liu,2 Anna Dai,3 Yanqin Wang,1 Lu She,4,5 Pei Zhang,4,5 Wenpei Zheng,1 Qiong Dai,1 Mei Yang4,5
1Maternal and Child Health Hospital of Hubei Province, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 2Technical Guidance Institute, Jinan Family Planning Service Center, Jinan, Shandong Province, People’s Republic of China; 3School of Basic Medicine, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 4School of Medicine, Wuhan University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China; 5Research Center for Health Promotion in Women, Youth and Children, Wuhan University of Science and Technology, Wuhan, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qiong Dai; Mei Yang, Tel +86-13294183249 ; +86-13037149918, Email [email protected]; [email protected]
Purpose: The aim of the study was to find out the associations of Melatonin receptor 1B (MTNR1B) genetic variants with gestational diabetes mellitus (GDM) in Wuhan of central China.
Patients and Methods: A hospital-based case–control study that included 1679 women was carried out to explore the associations of MTNR1B single nucleotide polymorphisms (SNPs) with GDM risk, which were analyzed through logistic regression analysis by adjusting age, pre-pregnancy BMI and family history of diabetes. Multifactor dimensionality reduction was applied to determine gene–gene interactions between SNPs.
Results: MTNR1B SNPs rs10830962, rs10830963, rs1387153, rs7936247 and rs4753426 were significantly associated with GDM risk (P< 0.05). The rs10830962/G, rs10830963/G, rs1387153/T, and rs7936247/T were risk variants, whereas rs4753426/T was protective variant for GDM development. Fasting plasma glucose (FPG) and 1h-plasma glucose (PG) were significantly different among genotypes at rs10830962 and rs10830963, whereas 2h-PG levels were not. Gene–gene interactions were not found among the five SNPs on GDM risk.
Conclusion: MTNR1B genetic variants have significant associations but no gene–gene interactions with GDM risk in central Chinese population. Furthermore, MTNR1B SNPs have significant relationships with glycemic traits.
Keywords: melatonin receptor 1B, gestational diabetes mellitus, single nucleotide polymorphisms, multifactor dimensionality reduction, gene–gene interactions
Introduction
Gestational diabetes mellitus (GDM), characterized by glucose intolerance or hyperglycemia, is one of the most common metabolic disorders in pregnant women.1 It is reported in a meta-analysis that the total incidence of GDM in mainland China is 14.8.2 The adverse outcomes associated with GDM for both pregnant women and their offspring are diverse. Apart from potential adverse pregnant outcomes such as macrosomia, neonatal hypoglycemia, this disorder is also associated with an increased risk of type 2 diabetes (T2D) and cardiovascular disease later in life.3 Therefore, it is essential to identify potential risk factors for GDM.
As a pre-diabetic status, GDM is thought to be associated with hyperinsulinemia and insulin resistance, but the exact underlying pathogenic mechanism of GDM is still unclear. Nevertheless, accumulating evidences reveal that genetic predisposition may play a crucial role in its pathogenesis.4,5 Recently, a genome-wide association study (GWAS) in Korean population concluded that genetic variants near melatonin receptor 1B (MTNR1B) gene were strongly associated with GDM.6 Moreover, another GWAS showed that MTNR1B polymorphism was associated with glycemic levels in both gravid and non-gravid populations.7
MTNR1B, which is strongly expressed in the brain, retina and β-cells, encodes the MT2 protein. Except for regulating circadian rhythm, melatonin can also impact insulin secretion both in vivo and in vitro.8,9 Plasma melatonin level was reversely correlated with insulin level.10 As a melatonin receptor, MT2 regulates blood glucose homeostasis through the regulation of insulin release via the melatonin signaling pathway.11 Hence, it is rational to believe that genetic variants in the MTNR1B might affect pancreatic glucose sensing, insulin secretion and conceivably glucose tolerance.12 Existed studies have predominantly demonstrated the associations of MTNR1B gene polymorphisms with GDM risk and genetic heterogeneity has been observed across ethnic groups.13–19 Nevertheless, these findings were not consistent in Chinese population. Li et al showed that in Chinese women rs10830963 but not rs10830962 was associated with an increased risk of developing GDM.15 However, Xie et al concluded that rs10830962 variant was associated with a higher GDM risk.16 In addition, other candidate single nucleotide polymorphisms (SNPs), such as rs1387153, rs7936247, rs4753426, which were confirmed to be significantly associated with glucose homeostasis, have not been fully elucidated in GDM in Chinese population to date.20–24 Furthermore, few data are available on the associations of MTNR1B SNPs with GDM risk in central Chinese population until now. Thus, the present study was carried out to explore whether these SNPs contributed to GDM risk in Wuhan of central China.
Materials and Methods
Study Population and Data Collection
The pregnant women who took antenatal examination in Obstetrics and Gynecology Clinic of Maternal and Child Health Hospital of Hubei Province from January 15, 2018 to March 31, 2019 were recruited in the study. All subjects were enrolled at 24–28 weeks’ gestation right after the 75g oral glucose tolerance test (OGTT). The diagnosis of GDM was based upon the criteria of International Association of Diabetes and Pregnancy Study Groups (IADPSG): fasting plasma glucose (FPG) ≥5.1 mmol/L, or 1h-plasma glucose (PG) ≥10.0 mmol/L, or 2h-PG ≥8.5 mmol/L. The non-diabetic controls were randomly selected at the same outpatient clinic matched with testing date and gestation week. Exclusion criteria: age <18 years; ethnic minorities; pre-gestational diabetes; multiple pregnancies; pregnancies complicated with endocrine diseases such as hypertension and polycystic ovary syndrome; any other medical condition that might affect glucose regulation; unable or unwilling to participate in the study. At the genotyping stage, unsuccessful samples were also excluded. After exclusion, 1679 pregnant women (818 GDM patients and 861 non-diabetic controls) were included. All the subjects were unrelated Han Chinese residing in Wuhan of Hubei Province, a central area of China. The method of data collection was reported in previous article.25 The study protocol was approved by the institutional review board of Wuhan University of Science and Technology and was performed in accordance with the Declaration of Helsinki. All subjects provided informed consents for participation.
Selection and Genotyping of SNPs
By tracking the literature, combined with genome-wide association studies of GDM and minor allele frequency (MAF)>0.05 reported in Chinese population, we selected five SNPs in or near MTNR1B gene for assessment. These SNPs were rs10830963, rs10830962, rs1387153, rs7936247 and rs4753426. The method of sample collection was also reported in the previous article.25 The aforementioned five SNPs were genotyped on the Sequenom MassARRAY platform (Sequenom Inc., San Diego, CA, USA). For quality control: (i) case and control samples were mixed on each plate; (ii) genotyping was performed blinded to case or control status; (iii) two water controls were used in each plate as blank controls; (iv) 5% of the samples were randomly selected for repeated genotyping, as blind duplicates, and the reproducibility was 100%. The call rates of rs10830963, rs10830962, rs1387153, rs7936247, rs4753426 were respectively 98%, 99%, 99%, 99%, 96%.
Statistical Analysis
We used t-test or analysis of variance (ANOVA) for normally distributed data and Chi-square test for non-normally distributed data. The exact Chi-square test was used to detect Hardy–Weinberg equilibrium (HWE). Logistic regression adjusted by age, pre-pregnancy BMI and family history of diabetes was performed to evaluate the associations with GDM risk. No Bonferroni correction was applied, in the case of replication studies, as it is unlikely to detect effects due to statistical fluctuation only.26 P<0.05 was considered statistically significant. Post hoc power calculations were performed giving the power to detect a given effect which could be estimated. All the statistical analyses were performed through SPSS 24.0 (SPSS Inc., Chicago, IL, USA). Multifactor dimensionality reduction (MDR) method, proposed by Ritchie et al27 as a new statistical and computational method to analyze gene–gene interactions in genetic studies and shown to have good power in case–control studies,28 was applied to determine gene–gene interactions.
Results
Demographic and Clinical Characteristics
Table 1 presented the demographic and clinical characteristics of subjects. Differences in age, pre-pregnancy BMI, family history of diabetes, FPG, 1h-PG and 2h-PG between the case and control groups were statistically significant (P<0.05). There were no significant differences in gravidity and parity between the two groups.
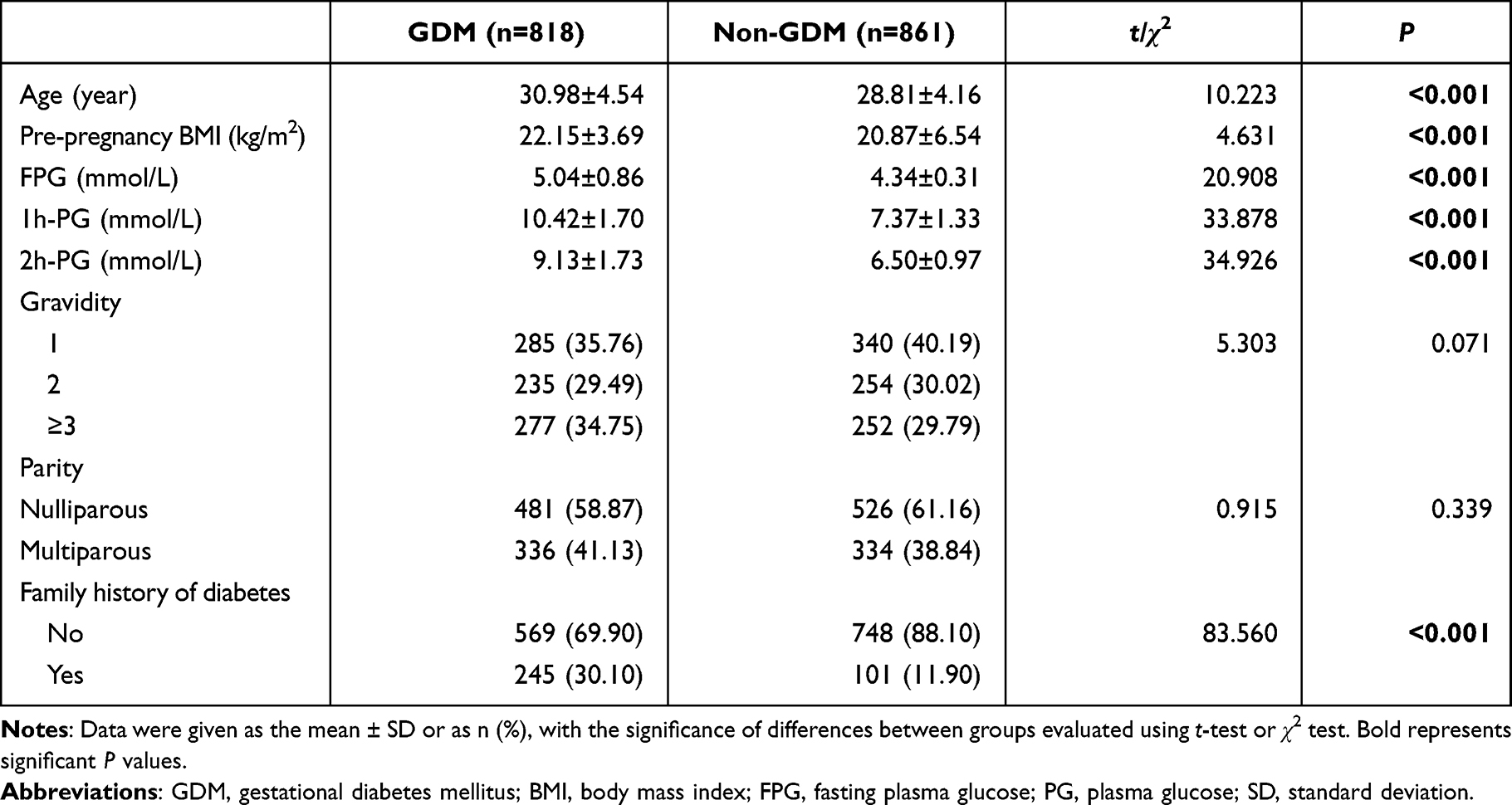 |
Table 1 Demographic and Clinical Characteristics of Subjects |
Association of MTNR1B Gene SNPs with GDM
The distributions of rs10830962, rs10830963, rs1387153, rs4753426 and rs7936247 in the control group were all in HWE. Table 2 showed that the allele and genotype distributions of the five SNPs were significantly different between GDM women and controls (P<0.05). The rs10830962/G, rs10830963/G, rs1387153/T and rs7936247/T led to a higher risk whereas the rs4753426/T led to a lower risk for GDM. The associations of the five SNPs with GDM were all statistically significant (P<0.05). The MTNR1B rs10830962 CG genotype was significantly associated with an increased GDM risk compared with CC genotype (OR=1.423, 95% CI: 1.059–1.912), and the risk of developing GDM with GG genotype was twofold than that of the CC genotype (OR=2.056, 95% CI: 1.444–2.927). The SNPs rs10830963, rs1387153 and rs7936247 could increase the GDM risk with a similar effect as rs10830962. In contrast, rs4753426 TT genotype was significantly associated with a decreased GDM risk compared with CC genotype (OR=0.466, 95% CI: 0.283–0.769).
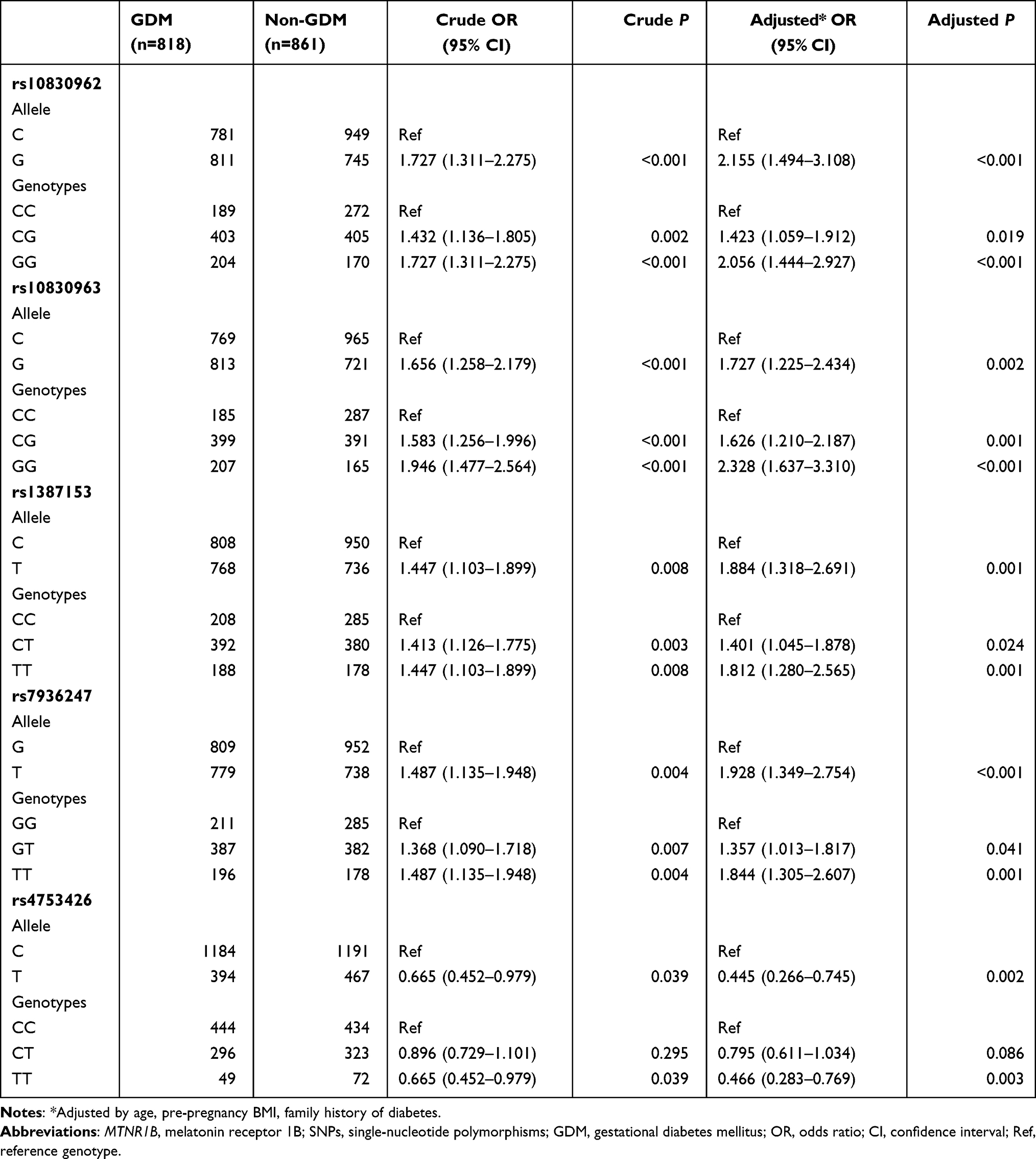 |
Table 2 Associations Between MTNR1B Gene SNPs and the Risk of GDM |
Relationships Between MTNR1B Gene Polymorphism and Glycemic Traits
Table 3 showed that FPG and 1h-PG levels were significantly different among genotypes at rs10830962 and rs10830963.
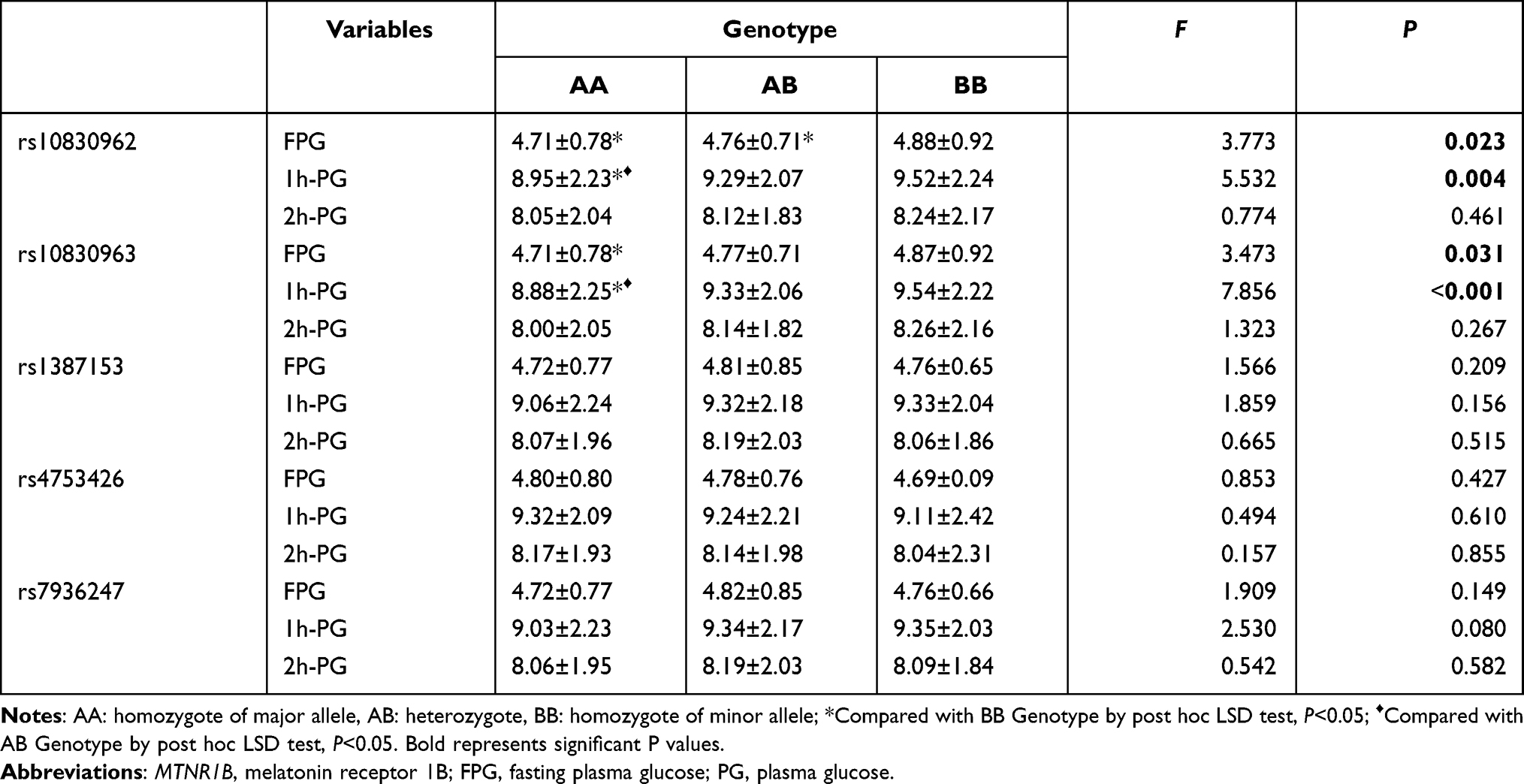 |
Table 3 Relationships Between MTNR1B Gene Polymorphisms and Glycemic Traits |
For rs10830962, FPG levels of GG genotype carriers were significantly higher than those of CC and CG genotype carriers, and the 1h-PG levels of CG and GG genotype carriers were significantly higher than those of CC genotype carriers.
For rs10830963, FPG levels of GG genotype carriers were significantly higher than those of CC genotype carriers, and the 1h-PG levels of CG and GG genotype carriers were significantly higher than those of CC genotype carriers.
Gene–Gene Interactions to GDM
The results in Table 4 showed that both one-factor model (rs10830963) and three-factor model (rs10830963, rs1387153 and rs4753426) had good cross-validation consistency at 10/10, but the test accuracy of the one-factor model (0.5536) was higher than that of the three-factor model (0.5528). After further analysis, none of the results were statistically significant (P>0.05). Hence, we could infer that there were no gene–gene interactions among the five MTNR1B gene SNPs on the GDM risk.
 |
Table 4 Analysis of Gene–Gene Interactions |
Discussion
Up to now, several studies have explored associations of MTNR1B with GDM risk.16,29–33 However, these studies with diverse sample sizes in different populations reported that there are controversial associations of MTNR1B with GDM risk. Furthermore, most analyses only examined one or two SNPs and the gene–gene interactions were commonly neglected. In the present study, we explored the associations with GDM risk and gene–gene interactions among the selected five MTNR1B SNPs. The results revealed that MTNR1B SNPs had significant associations but no gene–gene interactions with GDM risk in Wuhan of China. As far as we know, this is the first study that examines associations of several MTNR1B SNPs with GDM risk in genetic models as well as interactions between genetic polymorphisms in Central Chinese population.
We found that MTNR1B rs10830962 GG genotype increased GDM risk compared with CC genotype, which was consistent with findings of Xie et al16 but differed from those of Li et al.29 Moreover, we also found that the G allele of rs10830963 lead to a higher risk for GDM. Consistent with our findings, studies in Caucasian populations17,18 as well as in Chinese15 and South Korean34 populations confirmed the robust association of MTNR1B rs10830963/G variant with GDM. However, Wang et al observed that rs10830963 was not associated with GDM in Beijing.35 For rs1387153, we also detected a significant association with GDM risk, which was consistent with all the previous studies.13,26,34,36 The SNP rs10830963, maps within the single 11.5kb intron of MTNR1B. The association signal is bounded by recombination hot spots defining a ~60-kb interval within which all our strongly associated SNPs lie and the causal variant is likely to reside.37 As for SNP rs1387153, it maps within a 62.1-kb linkage disequilibrium (LD) block on chromosome 11 and is located in the 5′ region of MTNR1B, encoding the MTNR1B.20 A recent bioinformatics analysis reveals that rs10830962 is located in the functional elements of pancreatic islets and alters motif binding.16 Thus, it is biologically plausible that these SNPs may affect the expression of genes and be involved in the pathogenesis of GDM. However, due to controversial LD analyses among MTNR1B SNPs,13,23,34,36,38–40 further large-scale research is expected to analyze related molecular pathways combining multi-racial GWAS results by bioinformatics.
So far, remarkably, few studies have reported the associations between SNPs rs7936247, rs4753426 and GDM risk. Our study revealed that T allele of rs7936247 lead to a higher risk for GDM. Up to now, only one Chinese study had focused on the relationship between rs7936247 and GDM, indicating that the SNP rs7936247 was located in the region of histone modifications and regulated small nucleolar RNA, H/ACA box 8 (SNORA8) expression in pancreatic tissue,16 which makes the association of this SNP with GDM risk biologically plausible. Outstandingly, we found that rs4753426/T lead to a lower risk for GDM, which was consistent with findings of Shen et al26 but differed from those of Tarnowski et al.17 Qiu et al in 2007 detected a potential transcription factor of SNP rs4753426 and found a nearby transcription factor-binding site for v-Myb.41 Moreover, they also found SNP rs4753426 was located in the regulatory region of MTNR1B and could result in variation of MTNR1B expression level. Those findings suggested the MTNR1B SNP rs4753426 might be a susceptibility gene locus for GDM. However, functional studies are needed to confirm this.
Interestingly, FPG and 1h-PG levels were significantly different among genotypes at rs10830963 and rs10830962, whereas 2h-PG levels were not. The FPG and 1h-PG levels of GG genotype carriers were significantly higher than those of CC genotype carriers at rs10830963 and rs10830962. Numerous studies in ethnically diverse populations indicated that the G allele of rs10830963 was associated with FPG levels and impaired insulin secretion, as well as increased risk of T2D or GDM.18,23,34,37,42–44 The risk G allele of rs10830963 in MTNR1B preferentially binds NEUROD1 in islet-derived cells in vitro, and increases FOXA2-bound enhancer activity in human islet and liver-derived cells.43 In addition, the risk allele has also been associated with increased expression of MTNR1B in pancreatic beta cells, thereby possibly enhancing the effects of impaired early insulin secretion and elevated FPG levels.42 With respect to postprandial PG levels, Liao S et al found the association of rs10830963 with the increased 1h-PG levels in Chinese population, while Rosta et al demonstrated the association of rs10830963/G with 2h-PG values in Caucasian population. Our study found that 1h-PG levels but not 2h-PG levels were significantly different among genotypes of rs10830963. We speculate that there might be a timing effect on the association of MTNR1B rs10830963 with glycemic changes. Lane et al revealed that carriers of the rs10830963 might extend the duration of endogenous melatonin secretion later to morning and that early wake time might magnify the diabetes risk caused by the risk allele.45 They suggested that because melatonin inhibited glucose stimulated insulin secretion, it was plausible that a longer duration of melatonin production and delayed melatonin offset in the morning, in concurrence with an earlier waking, might lead to melatonin suppressing insulin secretion during times of raised glucose intake. A recent study indicated that rs10830963 variant was a marker for the initiation of antenatal insulin therapy in GDM, which also proposed clinical value of MTNR1B in the prevention and treatment of GDM.31 If our speculations are confirmed in large-scale prospective cohort studies, it would be advisable in the general population to avoid concurrence of food intake with elevated melatonin levels, which is of great importance for the human to improve health. As for rs10830962, because it might have a high LD with rs10830963 and thus the effect observed for rs10830962 might be due to rs10830963,46 the findings of rs10830962 should be dealt with cautiously and needed to be verified in large-scale genomic studies.
There were several similarities between this study and the previous research. They used similar methods to explore the associations of gene polymorphisms with GDM. The present but not the previous one found significant associations of gene polymorphisms with GDM. In addition, they both found no interactions amongst the examined SNPs. And unfortunately, the present study has some similar limitations with the previous research. First, the information regarding environmental and lifestyle factors, recently reported to be important determinants of GDM development,47,48 was not collected. Second, considerable controversies remain regarding the screening timing of GDM.49 Third, the level of melatonin was not tested because of practical reasons. We will carry out further study to explore the relation of melatonin and other possible biomarkers50 with GDM. Moreover, additional studies concerning other above-mentioned factors will be required in future to validate the findings of the study.
Nevertheless, there were still some strengths in the present study. First, MDR method was employed. The MDR method was developed for detecting and characterizing gene–gene interactions and was widely employed in genetic studies.51–54 The main principle of MDR is to reduce multidimensional genotypes into one-dimensional binary attributes, in which multi-level genotypes of SNPs are classified into either high-risk or low-risk groups, using a ratio of cases and controls in case–control studies.55 It was also applied in our previous study for detecting gene–gene interactions and found to be effective. Second, the interrelations of MTNR1B SNPs were considered and potential confounding factors including age, pre-pregnancy BMI and family history of diabetes were adjusted. Last but not least, a relatively large sample size was used in our study. Although post hoc analyses are debated and should be dealt with cautiously, the relatively large sample size might achieve adequate statistical power for the credibility.
Conclusions
In conclusion, MTNR1B SNPs rs10830962, rs10830963, rs1387153, rs7936247 and rs4753426 are associated with GDM risk in central Chinese population. There are no gene–gene interactions among the examined MTNR1B SNPs on GDM risk. FPG and 1h-PG levels but not 2h-PG levels are significantly different at MTNR1B SNPs rs10830962 and rs10830963, which inspire us to speculate that there might be a timing effect on the association of MTNR1B SNPs with glycemic changes. The findings of the study may provide a novel perspective for the prevention and treatment of GDM in the future. Additional studies are warranted to validate the findings and clarify the underlying mechanism.
Abbreviations
GDM, gestational diabetes mellitus; T2D, type 2 diabetes; GWAS, genome-wide association study; MTNR1B, melatonin receptor 1B; SNPs, single nucleotide polymorphisms; OGTT, oral glucose tolerance test; IADPSG, International Association of Diabetes and Pregnancy Study Groups; FPG, fasting plasma glucose; PG, plasma glucose; MAF, minor allele frequency; ANOVA, analysis of variance; HWE, Hardy–Weinberg Equilibrium; MDR, multifactor dimensionality reduction; LD, linkage disequilibrium; BMI, body mass index; SD, standard deviation; OR, odds ratio; CI, confidence interval; LSD, least significant difference.
Data Sharing Statement
The datasets of this study are available from the corresponding authors on reasonable request.
Ethics Approval and Informed Consent
The study was approved by the institutional review board of Wuhan University of Science and Technology. Informed consent was obtained from all subjects of the study.
Acknowledgments
The authors thank the study participants, hospital staff, research workers and students who participated in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by The National Natural Science Fund of China (81703239), Chinese Center for Disease Control and Prevention (2018FYH014) and Health Commission of Hubei Province (WJ2018H0134; WJ2018H0145).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships or conflicts of interest that could have appeared to influence the work reported in this paper.
References
1. Guariguata L, Linnenkamp U, Beagley J, Whiting DR, Cho NH. Global estimates of the prevalence of hyperglycaemia in pregnancy. Diabetes Res Clin Pract. 2014;103(2):176–185. doi:10.1016/j.diabres.2013.11.003
2. Gao C, Sun X, Lu L, Liu F, Yuan J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J Diabetes Investig. 2019;10(1):154–162. doi:10.1111/jdi.12854
3. Hammoud NM, Visser GHA, van Rossem L, Biesma DH, Wit JM, de Valk HW. Long-term BMI and growth profiles in offspring of women with gestational diabetes. Diabetologia. 2018;61(5):1037–1045. doi:10.1007/s00125-018-4584-4
4. Wu L, Cui L, Tam WH, Ma RC, Wang CC. Genetic variants associated with gestational diabetes mellitus: a meta-analysis and subgroup analysis. Sci Rep. 2016;6:30539. doi:10.1038/srep30539
5. Dalfrà MG, Burlina S, Del Vescovo GG, Lapolla A. Genetics and epigenetics: new insight on gestational diabetes mellitus. Front Endocrinol. 2020;11:602477. doi:10.3389/fendo.2020.602477
6. Kwak SH, Kim SH, Cho YM, et al. A genome-wide association study of gestational diabetes mellitus in Korean women. Diabetes. 2012;61(2):531–541. doi:10.2337/db11-1034
7. Hayes MG, Urbanek M, Hivert MF, et al. Identification of HKDC1 and BACE2 as genes influencing glycemic traits during pregnancy through genome-wide association studies. Diabetes. 2013;62(9):3282–3291. doi:10.2337/db12-1692
8. Peschke E. Melatonin, endocrine pancreas and diabetes. J Pineal Res. 2008;44(1):26–40. doi:10.1111/j.1600-079X.2007.00519.x
9. Garaulet M, Qian J, Florez JC, Arendt J, Saxena R, Scheer F. Melatonin effects on glucose metabolism: time to unlock the controversy. Trends Endocrinol Metab. 2020;31(3):192–204. doi:10.1016/j.tem.2019.11.011
10. Lardone PJ, Alvarez-Sanchez SN, Guerrero JM, Carrillo-Vico A. Melatonin and glucose metabolism: clinical relevance. Curr Pharm Des. 2014;20(30):4841–4853. doi:10.2174/1381612819666131119101032
11. Claustrat B, Leston J. Melatonin: physiological effects in humans. Neurochirurgie. 2015;61:77–84. doi:10.1016/j.neuchi.2015.03.002
12. Karamitri A, Jockers R. Melatonin in type 2 diabetes mellitus and obesity. Nat Rev Endocrinol. 2019;15(2):105–125. doi:10.1038/s41574-018-0130-1
13. Alharbi KK, Al-Sulaiman AM, Shedaid KMB, et al. MTNR1B genetic polymorphisms as risk factors for gestational diabetes mellitus: a case-control study in a single tertiary care center. Ann Saudi Med. 2019;39(5):309–318. doi:10.5144/0256-4947.2019.309
14. De Luis DA, Izaola O, Primo D, Aller R. Association of the rs10830963 polymorphism in MTNR1B with fasting glucose, serum adipokine levels and components of metabolic syndrome in adult obese subjects. Nutr Hosp. 2019;36(1):60–65. doi:10.20960/nh.2013
15. Li C, Zhou Y, Qiao B, Xu L, Li Y, Li C. Association between a melatonin receptor 1B genetic polymorphism and its protein expression in gestational diabetes mellitus. Reprod Sci. 2019;26(10):1382–1388. doi:10.1177/1933719118765983
16. Xie K, Chen T, Zhang Y, et al. Association of rs10830962 polymorphism with gestational diabetes mellitus risk in a Chinese population. Sci Rep. 2019;9(1):5357. doi:10.1038/s41598-019-41605-3
17. Tarnowski M, Malinowski D, Safranow K, Dziedziejko V, Pawlik A. MTNR1A and MTNR1B gene polymorphisms in women with gestational diabetes. Gynecol Endocrinol. 2017;33(5):395–398. doi:10.1080/09513590.2016.1276556
18. Rosta K, Al-Aissa Z, Hadarits O, et al. Association study with 77 SNPs confirms the robust role for the rs10830963/G of MTNR1B variant and identifies two novel associations in gestational diabetes mellitus development. PLoS One. 2017;12(1):e0169781. doi:10.1371/journal.pone.0169781
19. Jia G, Gao Y, Li C, Zhang Y. Effects of MTNR1B genetic variants on individual susceptibility to gestational diabetes mellitus: a meta-analysis. Am J Perinatol. 2020;37(6):607–612. doi:10.1055/s-0039-1685446
20. Bouatia-Naji N, Bonnefond A, Cavalcanti-Proença C, et al. A variant near MTNR1B is associated with increased fasting plasma glucose levels and type 2 diabetes risk. Nat Genet. 2009;41(1):89–94. doi:10.1038/ng.277
21. Plengvidhya N, Chanprasert C, Chongjaroen N, Yenchitsomanus PT, Homsanit M, Tangjittipokin W. Impact of KCNQ1, CDKN2A/2B, CDKAL1, HHEX, MTNR1B, SLC30A8, TCF7L2, and UBE2E2 on risk of developing type 2 diabetes in Thai population. BMC Med Genet. 2018;19(1):93. doi:10.1186/s12881-018-0614-9
22. Mazzoccoli G, Dagostino MP, Paroni G, et al. Analysis of MTNR1B gene polymorphisms in relationship with IRS2 gene variants, epicardial fat thickness, glucose homeostasis and cognitive performance in the elderly. Chronobiol Int. 2017;34(8):1083–1093. doi:10.1080/07420528.2017.1340894
23. Staiger H, Machicao F, Schäfer SA, et al. Polymorphisms within the novel type 2 diabetes risk locus MTNR1B determine beta-cell function. PLoS One. 2008;3(12):e3962. doi:10.1371/journal.pone.0003962
24. Matuszek MA, Anton A, Thillainathan S, Armstrong NJ, Rodella LF. Increased insulin following an oral glucose load, genetic variation near the melatonin receptor MTNR1B, but no biochemical evidence of endothelial dysfunction in young Asian men and women. PLoS One. 2015;10(7):e0133611. doi:10.1371/journal.pone.0133611
25. Liu J, Dai Q, Li W, et al. Association of vitamin D receptor gene polymorphisms with gestational diabetes mellitus-A case control study in Wuhan, China. BMC Pregnancy Childbirth. 2021;21(1):142. doi:10.1186/s12884-021-03621-y
26. Shen Y, Jia Y, Li Y, et al. Genetic determinants of gestational diabetes mellitus: a case-control study in two independent populations. Acta Diabetol. 2020;57(7):843–852. doi:10.1007/s00592-020-01485-w
27. Ritchie MD, Hahn LW, Roodi N, et al. Multifactor-dimensionality reduction reveals high-order interactions among estrogen-metabolism genes in sporadic breast cancer. Am J Hum Genet. 2001;69(1):138–147. doi:10.1086/321276
28. Ritchie MD, Hahn LW, Moore JH. Power of multifactor dimensionality reduction for detecting gene-gene interactions in the presence of genotyping error, missing data, phenocopy, and genetic heterogeneity. Genet Epidemiol. 2003;24(2):150–157. doi:10.1002/gepi.10218
29. Li C, Qiao B, Zhan Y, et al. Association between genetic variations in MTNR1A and MTNR1B genes and gestational diabetes mellitus in Han Chinese women. Gynecol Obstet Invest. 2013;76(4):221–227. doi:10.1159/000355521
30. Grotenfelt NE, Wasenius NS, Rönö K, et al. Interaction between rs10830963 polymorphism in MTNR1B and lifestyle intervention on occurrence of gestational diabetes. Diabetologia. 2016;59(8):1655–1658. doi:10.1007/s00125-016-3989-1
31. Firneisz G, Rosta K, Rigó J, et al. Identification and potential clinical utility of the MTNR1B rs10830963 core gene variant associated to endophenotypes in gestational diabetes mellitus. Front Genet. 2020;11:332. doi:10.3389/fgene.2020.00332
32. Lu X, Yao X, Liu X, et al. Melatonin receptor 1B gene polymorphism rs10830963 and gestational diabetes mellitus among a Chinese population—a meta-analysis of association studies. Endokrynol Pol. 2017;68(5):550–560. doi:10.5603/EP.a2017.0045
33. Zhang Y, Sun C-M, Hu X-Q, Zhao Y. Relationship between melatonin receptor 1B and insulin receptor substrate 1 polymorphisms with gestational diabetes mellitus: a systematic review and meta-analysis. Sci Rep. 2014;4(1):1–7. doi:10.1038/srep06113
34. Kim JY, Cheong HS, Park BL, et al. Melatonin receptor 1 B polymorphisms associated with the risk of gestational diabetes mellitus. BMC Med Genet. 2011;12:82. doi:10.1186/1471-2350-12-82
35. Wang Y, Nie M, Li W, et al. Association of six single nucleotide polymorphisms with gestational diabetes mellitus in a Chinese population. PLoS One. 2011;6(11):e26953. doi:10.1371/journal.pone.0026953
36. Liao S, Liu Y, Tan Y, et al. Association of genetic variants of melatonin receptor 1B with gestational plasma glucose level and risk of glucose intolerance in pregnant Chinese women. PLoS One. 2012;7(7):e40113. doi:10.1371/journal.pone.0040113
37. Prokopenko I, Langenberg C, Florez JC, et al. Variants in MTNR1B influence fasting glucose levels. Nat Genet. 2009;41(1):77–81. doi:10.1038/ng.290
38. Salman M, Dasgupta S, Cholendra A, et al. MTNR1B gene polymorphisms and susceptibility to type 2 diabetes: a pilot study in South Indians. Gene. 2015;566(2):189–193. doi:10.1016/j.gene.2015.04.064
39. Kwak SH, Kim S-H, Cho YM, et al. A genome-wide association study of gestational diabetes mellitus in Korean women. Diabetes. 2012;61(2):531–541. doi:10.2337/db11-1034
40. Patel R, Rathwa N, Palit SP, Ramachandran A, Begum R. Association of melatonin & MTNR1B variants with type 2 diabetes in Gujarat population. Biomed Pharmacother. 2018;103:429–434. doi:10.1016/j.biopha.2018.04.058
41. Qiu XS, Tang NL, Yeung HY, et al. Melatonin receptor 1B (MTNR1B) gene polymorphism is associated with the occurrence of adolescent idiopathic scoliosis. Spine. 2007;32(16):1748–1753. doi:10.1097/BRS.0b013e3180b9f0ff
42. Lyssenko V, Nagorny CL, Erdos MR, et al. A common variant in the melatonin receptor gene (MTNR1B) is associated with increased risk of future type 2 diabetes and impaired early insulin secretion. Nat Genet. 2009;41(1):82–88. doi:10.1038/ng.288
43. Gaulton KJ, Ferreira T, Lee Y, et al. Genetic fine mapping and genomic annotation defines causal mechanisms at type 2 diabetes susceptibility loci. Nat Genet. 2015;47(12):1415–1425. doi:10.1038/ng.3437
44. Tam CH, Ho JS, Wang Y, et al. Common polymorphisms in MTNR1B, G6PC2 and GCK are associated with increased fasting plasma glucose and impaired beta-cell function in Chinese subjects. PLoS One. 2010;5(7):e11428. doi:10.1371/journal.pone.0011428
45. Lane JM, Chang AM, Bjonnes AC, et al. Impact of common diabetes risk variant in MTNR1B on sleep, circadian, and melatonin physiology. Diabetes. 2016;65(6):1741–1751. doi:10.2337/db15-0999
46. Van Poppel MNM, Corcoy R, Hill D, et al. Interaction between rs10830962 polymorphism in MTNR1B and lifestyle intervention on maternal and neonatal outcomes: secondary analyses of the DALI lifestyle randomized controlled trial. Am J Clin Nutr. 2022;115:388–396. doi:10.1093/ajcn/nqab347
47. Carroll X, Liang X, Zhang W, et al. Socioeconomic, environmental and lifestyle factors associated with gestational diabetes mellitus: a matched case-control study in Beijing, China. Sci Rep. 2018;8(1):8103. doi:10.1038/s41598-018-26412-6
48. He JR, Yuan MY, Chen NN, et al. Maternal dietary patterns and gestational diabetes mellitus: a large prospective cohort study in China. Br J Nutr. 2015;113(8):1292–1300. doi:10.1017/s0007114515000707
49. Johns EC, Denison FC, Norman JE, Reynolds RM. Gestational diabetes mellitus: mechanisms, treatment, and complications. Trends Endocrinol Metab. 2018;29(11):743–754. doi:10.1016/j.tem.2018.09.004
50. Giglio RV, Lo Sasso B, Agnello L, et al. Recent updates and advances in the use of glycated albumin for the diagnosis and monitoring of diabetes and renal, cerebro- and cardio-metabolic diseases. J Clin Med. 2020;9(11):3634. doi:10.3390/jcm9113634
51. Hahn LW, Ritchie MD, Moore JH. Multifactor dimensionality reduction software for detecting gene-gene and gene-environment interactions. Bioinformatics. 2003;19(3):376–382. doi:10.1093/bioinformatics/btf869
52. Cho YM, Ritchie MD, Moore JH, et al. Multifactor-dimensionality reduction shows a two-locus interaction associated with type 2 diabetes mellitus. Diabetologia. 2004;47(3):549–554. doi:10.1007/s00125-003-1321-3
53. Milenkovic J, Milojkovic M, Mitic D, et al. Interaction of thrombophilic SNPs in patients with unexplained infertility-multifactor dimensionality reduction (MDR) model analysis. J Assist Reprod Genet. 2020;37(6):1449–1458. doi:10.1007/s10815-020-01808-4
54. Park M, Jeong HB, Lee JH, Park T. Spatial rank-based multifactor dimensionality reduction to detect gene-gene interactions for multivariate phenotypes. BMC Bioinform. 2021;22(1):480. doi:10.1186/s12859-021-04395-y
55. Lee JW, Lee S. A comparative study on the unified model based multifactor dimensionality reduction methods for identifying gene-gene interactions associated with the survival phenotype. BioData Min. 2021;14(1):17. doi:10.1186/s13040-021-00248-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.