Back to Journals » Integrated Pharmacy Research and Practice » Volume 9
Medication Error and Its Contributing Factors Among Pediatric Patients Diagnosed with Infectious Diseases Admitted to Jimma University Medical Center, Southwest Ethiopia: Prospective Observational Study
Authors Feyissa D ![]() , Kebede B
, Kebede B ![]() , Zewudie A
, Zewudie A ![]() , Mamo Y
, Mamo Y
Received 28 May 2020
Accepted for publication 17 August 2020
Published 15 September 2020 Volume 2020:9 Pages 147—153
DOI https://doi.org/10.2147/IPRP.S264941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Desalegn Feyissa, Bezie Kebede, Ameha Zewudie, Yitagesu Mamo
Department of Pharmacy, College of Medicine and Health Science, Mizan-Tepi University, Mizan-Aman, Ethiopia
Correspondence: Desalegn Feyissa Tel +251 917127556
Email [email protected]
Background: Medication errors in pediatric patients are grossly underreported. Pediatric patients are quite susceptible to medication errors. Potential injury by medication error is higher in young children and infants. It results in serious morbidity and mortality. Thus, this study aimed to assess medication error and its contributing factors among pediatric patients diagnosed with infectious diseases admitted to Jimma University Medical Center.
Methods: A prospective observational study was conducted among pediatric patients with infectious diseases admitted from April 1 to June 30, 2018. The patient’s written informed consent was obtained after explaining the purpose of the study. The data were collected by structured questionnaire. Data were entered into EpiData version 4.0.2 and then exported to SPSS version 21.0 for analysis. To identify the predictors of medication error, backward logistic regression analysis was done.
Results: From a total of the 325 study participants, 136 (41.8%) patients had at least one medication error during their hospital stay. A total of 273 medication errors were identified among 136 patients. Medication errors frequently occurred at prescribing stage 94 (34.4%). The most common types of medication errors were wrong dosing 72 (26.4%) and wrong frequency 47 (17.2%). Presence of disease comorbidity (AOR=1.64, 95%CI=1.01– 2.67), being male (AOR=1.79, 95%CI:1.13– 2.86) and presence of two infectious diseases (AOR=1.96, 95%CI: 1.20– 3.23) and more than three infectious diseases (AOR=2.04, 95%CI: 1.03– 4.01) were independent predictors of medication error occurrence.
Conclusion and Recommendation: Medication errors were common in pediatric patients with infectious diseases in the study area. Presence of comorbidities, being male and the number of infectious diseases were associated with the occurrence of medication errors. Therefore, to reduce medication errors in the study setting, e-prescribing, computerized provider order entry, medication reconciliation, and collaboration of clinical pharmacists with other health professionals are needed.
Keywords: medication error, pediatric, infectious disease, Ethiopia
Introduction
Medication error is defined as any preventable event that may lead to inappropriate medication use or patient harm while the medication is in the control of the health-care professional or patient. Such events may be related to professional practice, health-care products, procedures, and systems, including prescribing, order communication, product labeling, compounding, dispensing, administration, monitoring, and use.1 The outcomes of such errors are variable and may range from clinically insignificant to a life-threatening event.2
Children present unique demands in regard to medication ordering, dispensing, administering and monitoring as they often require weight-based dosing calculations, a situation further complicated by a lack of standardized pediatric easy-to-use dosage formulation.3
There are different factors that contribute to the occurrence of medication errors in pediatrics such as ignorance and lack of proper training among professionals, the use of abbreviations in prescriptions, illegible prescriptions, fatigue among professionals, inconsistencies in different formulations of drugs available, language barriers and the lack of good communication skills are some of the major factors that lead to medication errors.4–6
The pediatric medication-use process is complex and error-prone because of the multiple steps required in calculating, verifying, preparing, and administering doses.7 These factors prove that pediatrics are high risk for medication errors. Therefore, all pediatric prescriptions and medication orders must be checked for appropriate dose, route and frequency with a pediatrics dosing reference.8
Medication errors can directly affect patients, parents, and health-care providers by cost implications, prolonged hospital stays, and indirectly, it can have a psychological impact on the public by eroding confidence in health-care services. It can also cause significant mortality and morbidity among children.9,10
The risk of adverse events due to medication errors was higher in children than in adults. Among children, the rate of potentially dangerous medication errors is three times that of adults and wrong dose ordering errors are common because of the complexity of weight-based dosing.11,12 Pharmacists have a important role in the reduction of medication errors. For instance, a study conducted in the pediatric ward showed that the presence of pharmacists in the health-care team reduced the rate of serious medication errors from 29 to 6 per 1000 patient/days.13
The most common class of drugs involved in medication error among pediatric patients was anti-infective drugs.11
Data regarding medication error among pediatric patients with infectious diseases in the study setting were absent. Therefore, this study aimed to assess medication error and its contributing factors among pediatric patients diagnosed with infectious diseases admitted to Jimma University Medical Center, Southwest Ethiopia.
Methods
Study Area and Period
The study was conducted from April 1, 2018 to June 30, 2018 in the pediatric ward of Jimma University Medical Center (JUMC), which is located in Jimma town, Southwest Ethiopia; 352 km away from Addis Ababa, the capital city of Ethiopia. The hospital has been providing services for approximately 9000 inpatients and 80,000 outpatient clients per year with a catchment population of approximately 15 million people. There were 1584 pediatric patients with infectious diseases admitted to JUMC from September 1, 2017 to August 30, 2017.
Study Design and Population
A prospective observational study design was conducted in the pediatric ward of JUMC to assess medication error and its contributing factors. All pediatric patients admitted to JUMC and diagnosed with infectious diseases during the study period were the source population and all pediatric patients admitted to JUMC and diagnosed with infectious diseases and that fulfilled eligibility criteria were the study population.
Sample Size Determination and Sampling Techniques
The sample size was determined based on a single population proportion formula:  with the assumption of a 95% confidence interval (Zα/2= 1.96), marginal error (d) of 5% and P=50%. By using the correction formula and 5% nonresponse rate, the required sample size was 325. All patients admitted to the pediatric ward and diagnosed with infectious diseases during the data collection period and fulfilled the eligibility criteria were consecutively included in the study.
with the assumption of a 95% confidence interval (Zα/2= 1.96), marginal error (d) of 5% and P=50%. By using the correction formula and 5% nonresponse rate, the required sample size was 325. All patients admitted to the pediatric ward and diagnosed with infectious diseases during the data collection period and fulfilled the eligibility criteria were consecutively included in the study.
Inclusion and Exclusion Criteria
Patients admitted to the pediatric ward of JUMC during the study period, aged less than 16 years old, patient diagnosed with at least one infectious disease, patients’ whom their caregiver or parents signed the informed consent were included in the study whereas, readmitted patients for whom data were previously collected; patients admitted to ICU ward and patients with hospital admission less than 24 hwere excluded from study.
Study Variables
The dependent variable was medication error, whereas the independent variables included number of drugs used, comorbidity, number of infectious diseases, sex, age, place of residence, type of admission, and duration of hospital stay.
Data Collection Tool and Procedure
A multifaceted approach was employed to identify medication errors in the study setting. This approach included chart review, attendance of multidisciplinary meetings, attendance of multidisciplinary rounds, and interviews with the caregiver. The data collection format was prepared by reviewing different studies for important variables that were used to assess medication errors. The main contents of the tool include sociodemographic characteristics, disease and medication-related questionnaires. Daily visits to the ward by supervisor and data collectors involved registering new patients and interviewing mother/patient attendants, reviewing medical records and following the study patients until discharge. During chart review, when there was a dose change, medication discontinuation or a hold order, new order, change in route of administration from previous order, the primary care provider was contacted for clarification. All medications that were prescribed, dispensed and administered among pediatric patients with infectious disease were evaluated. The error types were categorized based up on NCCMERP14 into dose omission, improper dose (dose too high, too low and extra doses), wrong strength/concentration, wrong drug, wrong dosage form, wrong frequency, wrong route of administration, wrong duration, wrong patient, and monitoring error others. When an error was identified, it was recorded in the medication error documentation format.
Data Quality Assurance
Data quality was assured by careful selection and collection of complete and appropriate data. The data collection involved four pharmacists (BSc holders) and supervised by a clinical pharmacist daily. One days training was given for the data collectors and supervisor. Pretesting was conducted on 17 (5%) patients in the Shenan Gibe hospital. The collected data were cleared and checked every day for completeness and consistency. Data were entered into EpiData manager version 4.0.2 and double entry verification was made. Then the data were exported to SPSS version 21.0 for analysis.
Data Processing and Statistical Analysis
The data were explored to check for outliers, missing data and assumptions. During analysis, frequencies and percentages were used to describe categorical variables, while means and standard deviations were used to describe continuous variables. Bivariate logistic regression was run for all independent variables to assess the association between the study outcomes and the independent variables. Variables with a P-value <0.25 in the bivariate analysis were included in the multivariable logistic model to identify the predictors of medication error. A P-value of less than 0.05 was considered statistically significant.
Ethical Consideration
Ethical clearance was obtained from the Jimma University Research Ethical Board. Then the letter was given to the chief executive officer of the hospital and head of the pediatric department. This study was conducted in accordance with the Declaration of Helsinki. In line with this, caregivers/parents were requested to provide written informed consent. The name and address of the patient was excluded from data collection format to ensure the patient’s confidentiality.
Operational Definition
Medication Errors
Medication errors were defined as errors during drug prescribing, transcribing, administering, dispensing, and monitoring.1
Prescription Error
Prescription error was an error that occurred during the choice of drugs for patients. This includes incorrect dose, incorrect medicine, incorrect frequency, incorrect route of administration, or wrong patient.6
Administration Error
An administration error was any difference between what the patient received or was supposed to receive and what the prescriber intended in the original order.
Transcribing Error
A transcribing error was any discrepancy between the physician medication order and medication order transcription onto patient medical record.
Dispensing Error
Dispensing error was an error that occurred during drug dispensing.
Monitoring Error
This accounts for the untended failure in treatment process that leads to potentially cause harm to the patient.
Route Error
When a medication is given in a wrong route of administration.6
Omitted Drug Error
Omitted drug error is when there is failure to administer a prescribed medication.
Dose Error
Dose error is when the medication dose is different from the standard dose.
Results
Sociodemographic and Clinical Characteristics of the Study Participants
Among the 325 study participants, 184 (56.6%) were male. One hundred and twenty-two (37.5%) of them were infants with the mean (±SD) age of 3.22±1.53 years. The mean (±SD) weight of patients was 11.13± 8.2 kg (Table 1). From 325 studied patients, two thirds of them had comorbidity 212 (65.2%). One hundred and thirty-three (40.9%) patients stayed in hospital between six and ten days with a mean duration of 9.25±5.00 days. Two hundred and twenty-six (69.5%) patients were admitted to the pediatric ward of JUMC by transferring from different health facilities and 130 (40%) study participants had taken more than five drugs (Table 2).
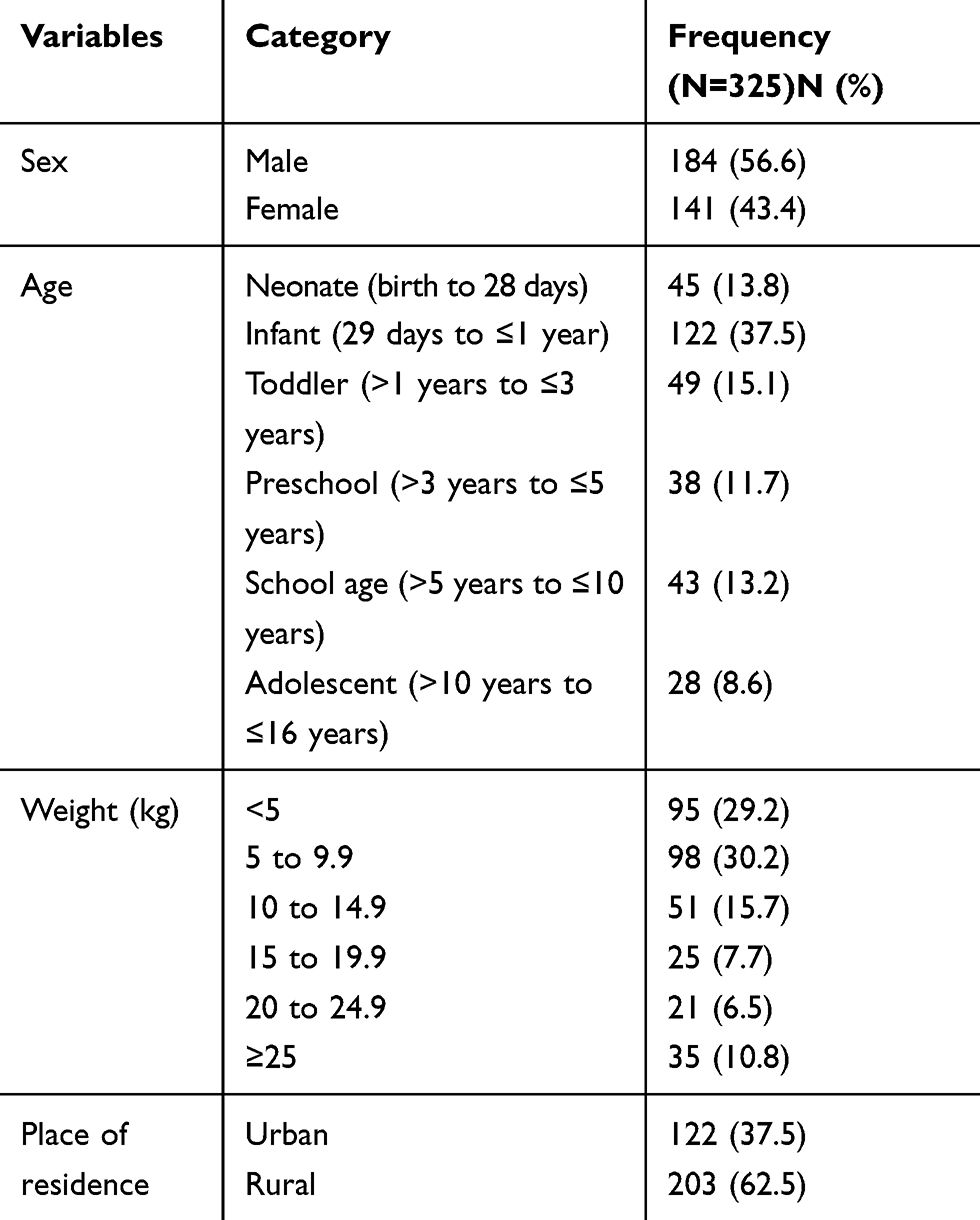 |
Table 1 Sociodemographic Characteristics of Study Participants in the Pediatric Ward of JUMC, Southwest Ethiopia, 2018 |
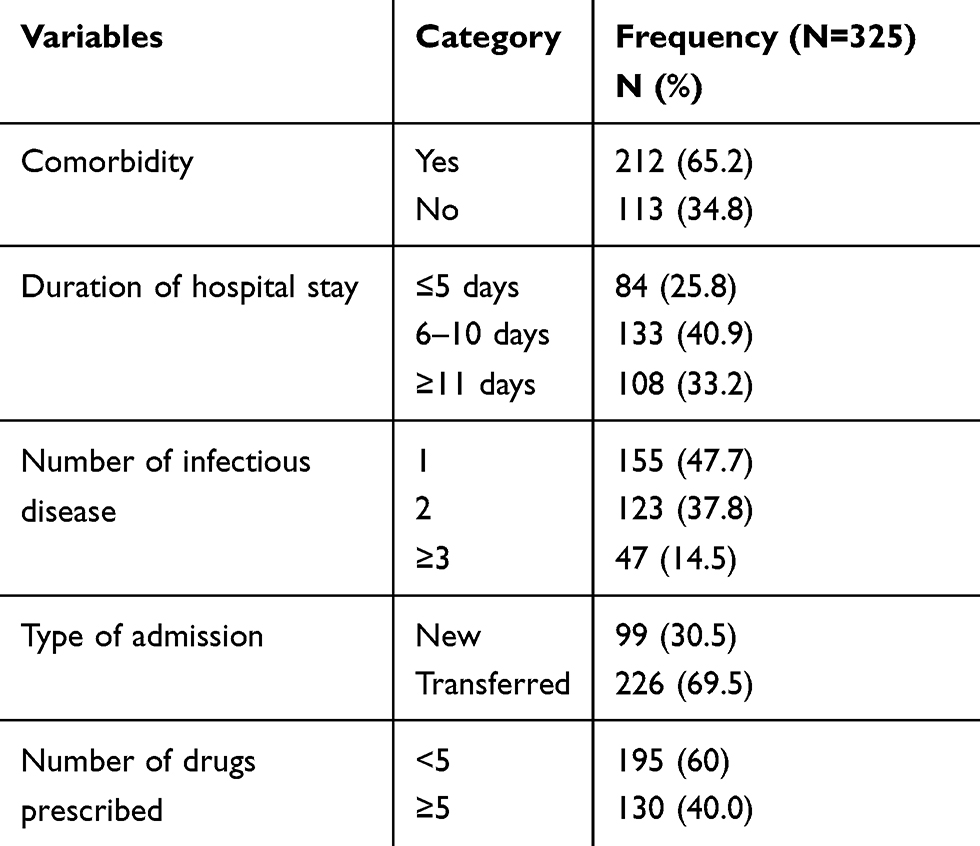 |
Table 2 Clinical Characteristics of Study Participants in the Pediatric Ward of JUMC, Southwest Ethiopia, 2018 |
The Types and Prevalence of Medication Error
From a total of 325 patients, 136 patients experienced medication errors, with overall prevalence of 41.8%. During the study period, a total of 273 medication errors were identified. One third of the medication errors were identified at prescribing 94 (34.4%) and administration stage 81 (29.7%). The most common type of medication error was wrong dosing 72 (26.4) followed by wrong frequency 47 (17.2%) (Table 3).
 |
Table 3 Prevalence, Stage and Type of Medication Errors Identified Among Study Participants in the Pediatric Ward of JUMC, Southwest Ethiopia, 2018 |
Class of Drugs Involved in Medication Errors
Different classes of drugs were involved with medication errors. The main class of drugs involved in medication errors were systemic anti-infective 192 (70.3%) (Table 4).
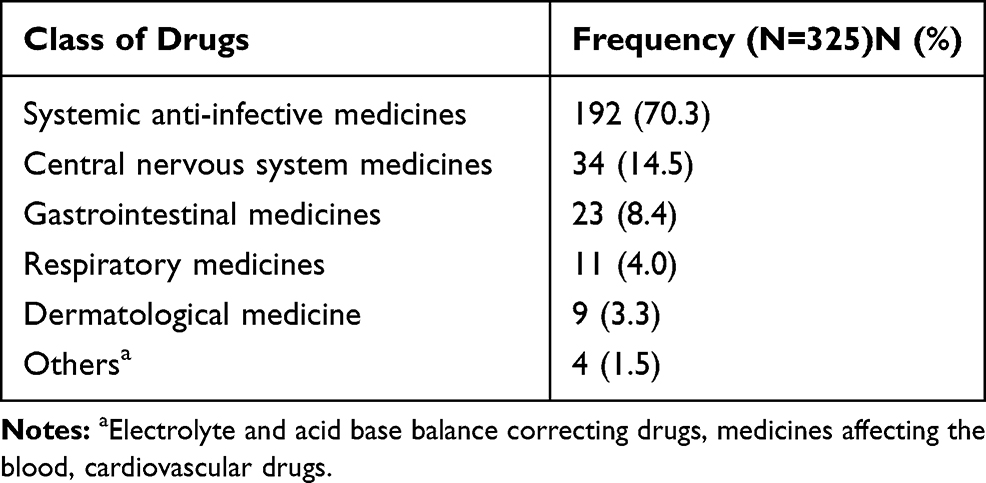 |
Table 4 Class of Drugs Involved in Medication Errors in the Pediatric Ward of JUMC, Southwest Ethiopia, 2018 |
Predictors of Medication Error Among Study Participants
Multiple logistic regression analysis showed that comorbidity, number of infectious disease and sex (male) were found to be independent predictors of medication errors among study participants. Patients with two diseases were 1.96 times more likely to have medication errors (AOR=1.96, 95%CI: 1.20–3.23) whereas,those who had more than three infectious diseases were 2.04 times more likely to have medication errors (AOR=2.04, 95%CI: 1.03–4.01) compared to those who had one infectious disease. Similarly, patients with comorbidity were 1.64 times more likely to experience medication errors (AOR=1.64, 95%CI: 1.01–2.67) than patients without comorbidity (Table 5).
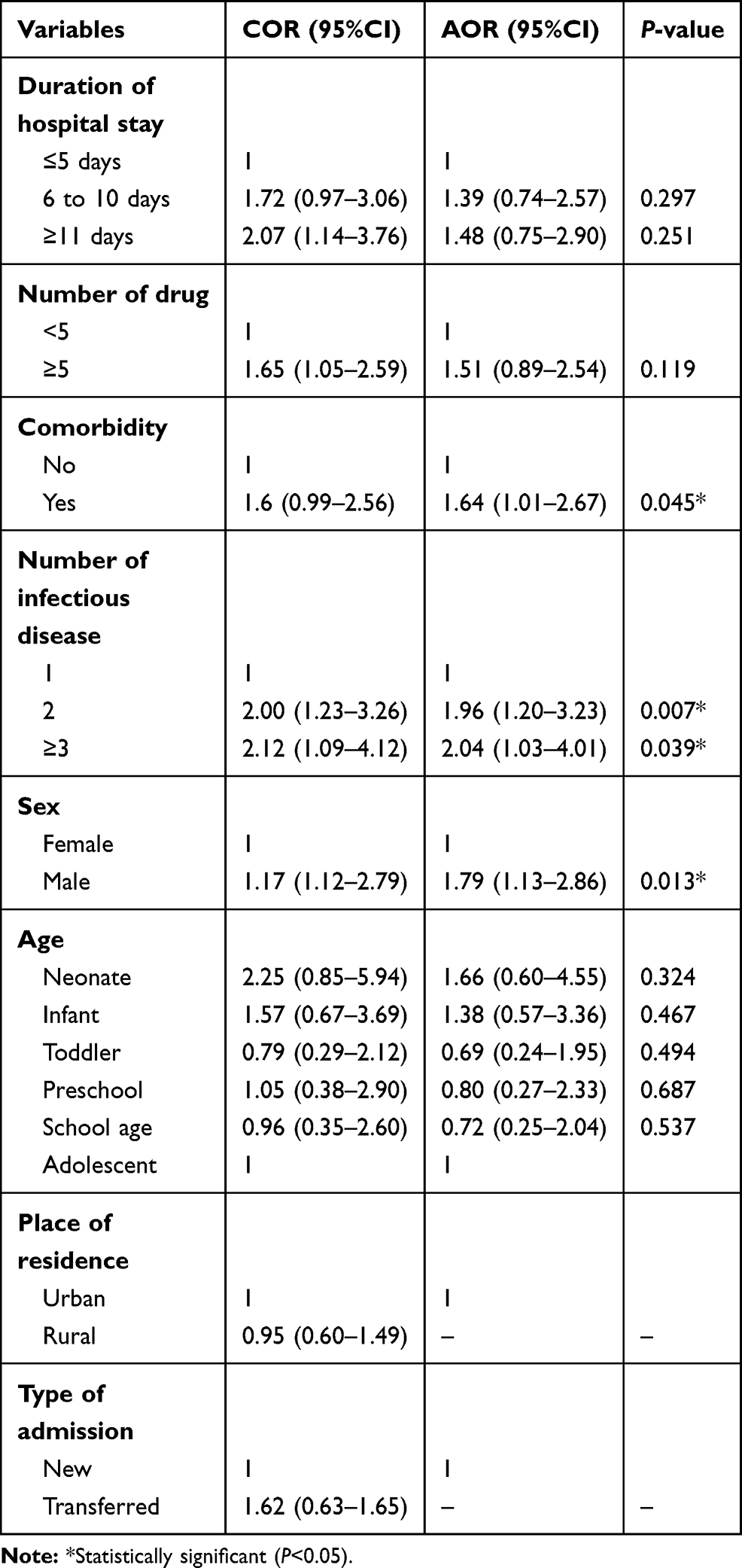 |
Table 5 Multiple Logistic Regression Analysis of Medication Error Among Study Participants in the Pediatric Ward of JUMC, Southwest Ethiopia, 2018 |
Discussion
Errors are possible at any step of the process from medication selection and ordering, order transcription, drug formulation, and drug dispensing, to drug administration.15 Pediatrics are more susceptible to medication errors than are adults because of childhood development and the different epidemiology of medical conditions.16
The present study showed that the prevalence of medication errors in the study area was found to be 41.8%. This is higher than the finding reported by Otero et al, where the prevalence of medication errors in pediatric was 7.3%.17 This discrepancy might be due to the difference in setting, staff experience, knowledge, skill, and lack of electronic prescribing in the study setting.
The results of this study revealed that 34.4% of medication errors commonly occurred at the prescribing stage. This is lower than the study done in Nekemte, Western Ethiopia, which showed that 48.6% of medication errors were at the prescribing stage.18 In addition, in the present study, 29.7% of medication errors occurred at the drug administration stage. This is higher than previous in a study done in pediatric inpatients, Ethiopia, where 13% of medication errors were at the administration stage.19
The present study found that the most common type of medication error was wrong dosing (26.4%). This is comparable with results of a study done in Northeast Ethiopia (31.39%) and USA (28%), where dosing error was the most common type of error.20,21 This showed that inappropriate doses are more common in pediatrics, which might be due to weight-based dose calculation, fractional dosing, and incorrect recording of patients’ weights and prescribing error.
The main class of drugs involved in medication errors in study setting was systemic anti-infective 192 (70.3%). This is in agreement with a study done in Northeast Ethiopia and Western Ethiopia, where antibiotics were the main class of drugs responsible for medication errors.18,21 The possible reason might be due to the fact that infectious diseases are the top diagnosis in pediatric wards of developing countries that require anti-infective medication for management.
Multiple logistic regression analysis of this study showed that comorbidity, number of infectious diseases and sex (male) were associated with medication errors among study participants. In our study, patients with two or more infectious diseases were more likely to have medication errors compared to those who had one disease. This is in line with a study done in West Ethiopia.22 This might be as the number of infectious diseases increases the more medications are required. This causes the medication regimen to be complex, which further contributes to occurrence of medication errors.
In our finding, patients with comorbidity were more likely to experience medication errors than patients without comorbidity. This is similar to the finding reported by Leendertse et al.23 This might be due to the presence of another comorbid condition requiring new drugs, which increases the number of drugs prescribed that in turn increases the likelihood of experiencing medication errors in the study setting. The present study finding showed that male patients were more likely to experience medication errors than female patients. This is in contrast to the analysis reported by Bresnick, where female patients are also slightly more likely to experience medication error than male.24
Conclusion
Medication error was common in pediatric patients with infectious diseases in the study area. In the study setting medication errors commonly occurred at prescribing and drug administration stage. Wrong dosing and wrong frequency were the most common types of medication errors identified among study participants. The main class of drugs involved in medication errors was systemic anti-infective drugs. Presence of comorbidity, being male and number of infectious diseases were the predictors of medication errors in the study area. Therefore, to reduce medication errors, computer-assisted prescribing software with updated references of the drug doses, name, strength, dosage form, and drug interaction is needed.
Abbreviations
AOR, adjusted odd ratio; COR, crude odds ratio; ICU, intensive care unit; JUMC, Jimma University Medical Center; NCCMERP, National Coordinating Council for Medication Error Reporting and Prevention.
Data Sharing Statement
All relevant data are within the paper.
Acknowledgments
We extend our gratitude to all individuals who were involved in data collection and also the participants who genuinely provided us all necessary information.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. National Coordinating Council for Medication Error Reporting and Prevention. What is a medication error? New York, NY: National Coordinating Council for Medication Error Reporting and Prevention; 2015.Available from: http://www.nccmerp.org/.
2. Mehndiratta S. Strategies to reduce medication errors in pediatric ambulatory settings. J Postgrad Med. 2012;58(1):47–53. doi:10.4103/0022-3859.93252
3. Giacoia GP, Taylor-Zapata P, Mattison D. Need for appropriate formulations for children: the national institute of child health and human development- pediatric formulations initiative. Int J Pharm Compd. 2007;11(1):5–8.
4. Slight SP, Howard R, Ghaleb M, Barber N, Franklin BD, Avery AJ. The causes of prescribing errors in english general practices. Br J Gen Pract. 2013;63(615):e713–20. doi:10.3399/bjgp13X673739
5. Avery AA, Barber N, Ghaleb M, et al. Investigating the Prevalence and Causes of Prescribing Errors in General Practice: The Practice Study. General Medical Council; 2012:227.
6. World health organization. Medication errors:TechnicalSeries on Safer Primary Care. 2016.
7. Richard K, Marjorie A, Glenn D, Sidney C, Linda E, Jan F. Pediatrics. Merck Manual of Diagnosis and Therapy.
8. Milap C, Taketomo C. Pediatrics. In: Joseph T, Robert L, Gary C, Gary R, Barbara G, editors. Pharmacotherapy a Pathophysiologic Approach.
9. Agalu A, Ayele Y, Bedada W, et al. Medication administration errors in an intensive care unit in Ethiopia. Int Arch Med. 2012;5(15):15. doi:10.1186/1755-7682-5-15
10. Zakharov S, Tomas N, Pelclova D. Medication errors–an enduring problem for children and elderly patients. Ups J Med Sci. 2012;117(3):309–317. doi:10.3109/03009734.2012.659771
11. Kaushal R, Bates DW, Landrigan C, et al. Medication errors and adverse drug events in pediatric inpatients. JAMA. 2001;285(16):2114–2120. doi:10.1001/jama.285.16.2114
12. Ruano M, Villamañán E, Pérez E, Herrero A, Álvarez-Sala R. New technologies as a strategy to decrease medication errors: how do they affect adults and children differently? World J Pediatr. 2016;12(1):28–34. doi:10.1007/s12519-015-0067-6
13. Wang JK, Herzog NS, Kaushal R, Park C, Mochizuki C, Weingarten SR. Prevention of pediatric medication errors by hospital pharmacists and the potential benefit of computerized physician order entry. Pediatrics. 2007;119(1):77–85. doi:10.1542/peds.2006-0034
14. National Coordinating Council for Medication Error Reporting and Prevention. Taxonomy and index category of medication errors; 2020 Available from: http://www.nccmerp.org.
15. Stucky ER. American academy of pediatrics committee on drugs; American academy of pediatrics committee on hospital care. Prevention of medication errors in the pediatric inpatient setting. Pediatrics. 2003;112(2):431–436. doi:10.1542/peds.112.2.431
16. Santell JP, Hicks R. Medication errors involving pediatric patients. Jt Comm J Qual Patient Saf. 2005;31(6):348–353. doi:10.1016/s1553-7250(05)31046-4
17. Otero P, Leyton A, Mariani G, Ceriani CJM. Patient safety committee. Medication errors in pediatric inpatients: prevalence and results of a prevention program. Pediatrics. 2008;122(3):e737–e743. doi:10.1542/peds.2008-0014
18. Fekadu G, Abdisa E, Fanta K. Medication prescribing errors among hospitalized pediatric patients at Nekemte Referral Hospital, western Ethiopia: cross-sectional study. BMC Res Notes. 2019;12(1):421. doi:10.1186/s13104-019-4455-1
19. Feleke Y, Girma B. Medication administration errors involving paediatric in-patients in a hospital in Ethiopia. Trop J Pharm Res. 2010;9(4):401–407. doi:10.4314/tjpr.v9i4.58942
20. Fortescue EB, Kaushal R, Landrigan CP, et al. Prioritizing strategies for preventing medication errors and adverse drug events in pediatric inpatients. Pediatrics. 2003;111(4 Pt 1):722–729. doi:10.1542/peds.111.4.722
21. Zeleke A, Chanie T, Woldie M. Medication prescribing errors and associated factors at the pediatric wards of Dessie Referral Hospital, Northeast Ethiopia. Int Arch Med. 2014;7(1):18. doi:10.1186/1755-7682-7-18
22. Dedefo MG, Mitike AH, Angamo MT. Incidence and determinants of medication errors and adverse drug events among hospitalized children in West Ethiopia. BMC Pediatr. 2016;16(1):81. doi:10.1186/s12887-016-0619-5
23. Leendertse AJ, Egberts AC, Stoker LJ, van den Bemt PM, HARM Study Group. Frequency of and risk factors for preventable medication-related hospital admissions in the Netherlands. Arch Intern Med. 2008;168(17):1890–1896. doi:10.1001/archinternmed.2008.3
24. Bresnick J. Big data shows gender-based medical error, patient safety patterns. Health IT analytics; 2016. Available from: https://healthitanalytics.com/news/big-data-shows-gender-based-medical-error-patient-safety-patterns.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.