Back to Journals » Patient Preference and Adherence » Volume 19
Medication Adherence in Parkinson’s Disease: Longitudinal Changes and the Influence of Depressive Symptoms
Authors Heimrich KG ![]() , Schönenberg A
, Schönenberg A ![]() , Franke GH
, Franke GH ![]() , Prell T
, Prell T
Received 20 March 2025
Accepted for publication 12 August 2025
Published 9 September 2025 Volume 2025:19 Pages 2835—2845
DOI https://doi.org/10.2147/PPA.S529538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Konstantin G Heimrich,1,2 Aline Schönenberg,3 Gabriele Helga Franke,4 Tino Prell3
1Department of Geriatrics, Jena University Hospital, Jena, Germany; 2Department of Neurology, Jena University Hospital, Jena, Germany; 3Department of Geriatrics, Halle University Hospital, Halle, Germany; 4Department of Psychology of Rehabilitation, University of Applied Sciences Magdeburg-Stendal, Magdeburg-Stendal, Germany
Correspondence: Konstantin G Heimrich, Department of Geriatrics, Jena University Hospital, Jena, 07747, Germany, Email [email protected]
Purpose: Parkinson’s disease (PD) is a progressive neurodegenerative disease. As the disease progresses, medication regimens become increasingly complex. The long-term success of PD pharmacotherapy is highly dependent on patient adherence to the prescribed medication regimen. The aim of this study is to investigate how intentional and unintentional non-adherence evolves over time and to identify PD-related factors that influence these longitudinal changes. These findings may be crucial in developing targeted interventions to improve adherence, particularly in patients who have difficulties with intentional or unintentional non-adherence.
Patients and Methods: The sample consisted of 91 people with PD who were initially treated as part of the PD multimodal complex treatment at the Department of Neurology, Jena University Hospital, Germany. They were followed up three and six months after discharge. Medication adherence was assessed using the Stendal Adherence to Medication Score (SAMS) and its three subscores for forgetfulness, knowledge, and modification. Statistical analyses included Wilcoxon signed rank test, Friedman test, and generalized estimating equations to determine longitudinal changes in non-adherence and the influence of PD-related variables.
Results: Analysis of SAMS subscores showed improvement over time in modification and knowledge, whereas forgetfulness did not show significant change. Modification was significantly associated with depressive symptoms.
Conclusion: Medication adherence in PD is a dynamic process and changes over time. The findings suggest that while educational interventions are effective in improving knowledge and reducing intentional non-adherence, addressing depressive symptoms and cognitive impairment is critical to improving overall adherence. Future research should continue to explore the factors that influence adherence behaviors and develop targeted strategies to help people with PD maintain adherence throughout the course of their disease.
Keywords: compliance, cognition, assessment, multimodal treatment, comprehensive health care
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder characterized by motor symptoms such as tremor, bradykinesia, and rigidity, and non-motor symptoms such as cognitive decline, mood, and sleep disturbances.1 The progressive nature of PD requires lifelong treatment, with dopaminergic as well as noradrenergic, glutamatergic, and serotonergic pharmacotherapy playing a decisive role in alleviating variable motor and non-motor symptoms.2 These medications are essential for improving quality of life (QoL) by reducing the motor and non-motor symptoms that interfere with daily functioning. Despite the availability of effective pharmacotherapy, the clinical management of PD is challenging due to the complexity of the disease and its treatment regimen. As PD progresses, medication regimens become increasingly complex, requiring patients to take multiple medications several times a day. The effectiveness of treatment is highly dependent on the patient’s adherence to the prescribed medication regimen.3,4 Poor adherence can lead to suboptimal symptom control, worsening of motor and non-motor symptoms, increased risk of complications, and overall deterioration in QoL.4–6 Therefore, medication adherence is a key determinant of the long-term success of PD pharmacotherapy.
Medication adherence refers to the extent to which a patient’s medication taking behavior is in accordance with the prescribed therapeutic regimen.6 It includes the timing, dosage and frequency of taking medication as agreed with the healthcare provider. Adherence is a critical factor in achieving therapeutic goals, particularly in chronic diseases such as PD that require long-term pharmaceutical treatment.7 However, adherence is not a static behavior and can vary over time due to a number of factors, including disease progression, side effects, cognitive decline and psychosocial influences (eg, depressive symptoms, stressful life events, and individual coping capabilities).
In contrast, non-adherence denotes the inability or unwillingness to adhere to a prescribed regimen, which can be either intentional or unintentional.7 Intentional non-adherence is defined as a conscious decision of a person to deviate from the prescribed regimen. This is often motivated by factors such as perceived side effects, doubts about the efficacy of the treatment, or difficulties with complex regimens.3 Unintentional non-adherence is frequently attributable to factors such as forgetfulness or cognitive impairment, which is of particular relevance in the context of the ageing PD population. In people with PD (PwPD), non-adherence is a prevalent issue, largely due to the complexity of treatment regimens, the cognitive impairments that frequently accompany the disease, and the high prevalence of depressive symptoms.8,9 In particular, depressive symptoms are closely linked to non-adherence, eg through reduced motivation and ability to adhere to treatment, a lack of interest in improving one’s own health, as well as changes in concentration and fatigue, resulting in intentional and unintentional non-adherence.10 Furthermore, as the disease progresses, PwPD may experience motor fluctuations and dyskinesias, which can lead to frustration and deliberate changes in medication intake without consulting a healthcare provider (intentional nonadherence).
The traditional measures of adherence, such as the proportion of days covered (PDC) or the medication possession ratio (MPR), provide a snapshot of overall adherence over a fixed period.11 However, they are unable to capture reasons for longitudinal changes and fluctuations in adherence that are often observed in people with chronic diseases.12 In PD, where disease progression, cognitive changes and fluctuations in symptoms are common, adherence can follow a number of different trajectories over time.
Group-based trajectory modelling was demonstrated to be an effective method for categorizing people into discrete adherence trajectory groups based on their medication-taking behavior over time.13 The utilization of this approach has led to the identification of a number of common adherence trajectories, including consistent high adherence, declining adherence, early and persistent nonadherence, and initial nonadherence followed by improved adherence.13 Although these trajectories demonstrate the intricacy of adherence behavior in chronic diseases such as PD, it remains unclear how different forms of non-adherence (ie, intentional or unintentional) evolve over time.
This study builds upon previous research by exploring not only how general adherence changes over time, but also how different forms of non-adherence evolve longitudinally.3,14 This study represents the first attempt to differentiate between intentional and unintentional non-adherence and to examine how each form changes over time in PwPD. Thereby, the study focused on PwPD, who were treated within Parkinson’s disease multimodal complex treatment (PD-MCT) and on the months following discharge. PD-MCT is a multidisciplinary inpatients treatment approach for PwPD. In Germany, this treatment approach is integrated in the national health insurance system and lasts at least seven days.15,16 It is carried out according to precise specifications and includes multidisciplinary treatment with the additional involvement of physiotherapists, occupational therapists, speech and language therapists and psychologists, with a treatment duration of at least 7.5 hours per week in addition to standard medical treatment and medication optimization. Previous studies have shown that PD-MCT can effectively improve motor and non-motor symptoms as well as QoL.16–19 However, it is not yet known whether this multimodal therapy can also change patient’s medication adherence.
The aim of this study is 1) to examine how intentional and unintentional non-adherence evolve over time in PwPD following PD-MCT and 2) to determine PD-related factors that influence longitudinal changes in intentional and unintentional non-adherence. By addressing these questions, our objective is to gain a more nuanced understanding of adherence behavior in PwPD and to identify which factors contribute to changes in different types of non-adherence over time. These insights could prove pivotal in the development of targeted interventions to improve adherence, particularly in patients who experience difficulties with intentional or unintentional non-adherence.
Materials and Methods
Study Design and Participants
We performed a prospective monocentric study with a follow-up of six months conducted at the Department of Neurology of the University Hospital Jena, Germany. The study is approved by the Ethics Committee of the University Hospital Jena (registration number 2021–2228-BO). Between July 2021 and March 2023, PwPD who were admitted for PD-MCT were screened, and included if they have a confirmed diagnosis of idiopathic PD in accordance to the Movement Disorder Society (MDS) criteria.20 Exclusion criteria were severe cognitive impairment with the inability to complete a questionnaire. Prior to study inclusion, written informed consent was obtained from all participants (total number of participants, N = 120). Of 120 PwPD who were treated within PD-MCT, N = 91 received two follow-ups by telephone calls at three and six months and were included in data analysis.
Dependent Variable
The primary outcome of this secondary analysis was non-adherence according to the Stendal Adherence to Medication Score (SAMS).21 Briefly, the SAMS is a self-report questionnaire consisting of 18 items. Items are scaled on a 5-point Likert scale (from “0” to “4”, eg, never, rare, sometimes, often, mostly), and added up to a cumulative adherence score, with “0” indicating complete adherence and “72” complete non-adherence. Different subscores can be calculated, namely forgetting to take medication (unintentional non-adherence), modification of medication (intentional non-adherence), and missing knowledge about medication. Modification refers to the adjustment of medications (dosages, time points) without consulting a doctor, while missing knowledge represents people who were unaware of the purpose of their medications and/or dosages. The factor forgetfulness includes people who unintentionally forget to take their medications.3,21,22 The SAMS subscales were calculated as described previously.3
Covariates
The following general and PD-related variables were collected by trained study staff at baseline: Age (years, metric); gender (male/female); disease duration (years, metric); levodopa equivalent daily dose (LEDD, metric);23 number of medications per day (metric); motor symptoms assessed by the MDS sponsored revision of the unified Parkinson’s disease rating scale part II (MDS-UPDRS II, motor experiences of daily living, metric; higher values indicate more impairment) and III (MDS-UPDRS III, motor examination, metric; higher values indicate more impairment)24 and the Hoehn & Yahr stage (multi-nominal, stage I to V; higher values indicate a more severe disease stage);25 the number of non-motor symptoms as assessed by the Non-Motor Symptoms Questionnaire (NMSQ, metric; higher numbers indicate more non-motor symptoms);26 screening for depressive symptoms (Patient Health Questionnaire-9, PHQ-9, metric; higher values indicate more depressive symptoms);27 cognition assessed with the Montreal Cognitive Assessment (MoCA, metric; higher values indicate better cognition);28,29 and finally, the PD-questionnaire (PDQ-8, metric) to determine health-related QoL (lower values indicate better QoL).30,31 At the three and six months follow-up, the MDS-UPDRS II, NMSQ, PHQ-9, and PDQ-8 were determined again.
Statistical Analysis
For statistical analyses, IBM SPSS version 29 and R version 4.3.0 were used. Statistical significance for all tests was set at p < 0.05. Descriptive statistics were used to describe the study population. Mean and standard deviation (SD) were reported for continuous variables, and categorical variables were presented as absolute values and relative frequencies. Missing data were treated according to the pairwise deletion process.32 To compare the variables within groups, the Wilcoxon signed rank test for non-normally distributed data and the Friedman test to test for one-way repeated measures analysis of variance by ranks were used.33 Effect sizes were given as rank biserial correlation coefficient r (> 0.2: low; > 0.5: moderate; > 0.8: large) for the Wilcoxon signed rank test and partial Eta2 (> 0.01: low; > 0.06: moderate; > 0.14: large) for variables in the ANOVA model.34 Generalized Estimating Equations (GEEs) were developed to assess the influence of the PD-related variables (NMSQ, MDS-UPDRS II, PHQ-9, PDQ-8) on SAMS subscales modification, missing knowledge, and forgetting.35 An exchangeable covariance structure was used assuming that every observation (ie, factor score) of a participant is equally correlated with the other factor scores of that participant. Robust standard errors were calculated to ensure consistent inferences from a GEE model.
Results
Characteristics
Table 1 outlines the detailed characteristics of the cohort. PwPD had a mean age of 70 (SD = 9) years. The majority of the cohort (56%, N = 51) were male. With regard to PD severity, 68% (N = 62) of the cohort were classified as Hoehn and Yahr stage 3. The mean number of medications taken per day is 12 (SD = 6), with a mean LEDD of 833 mg (SD = 591). PwPD reported a mean number of different non-motor symptoms according to the NMSQ of 8 (SD = 5). The majority of the participants (67%, N = 60) had no relevant depressive symptoms (PHQ-9 total score <10).
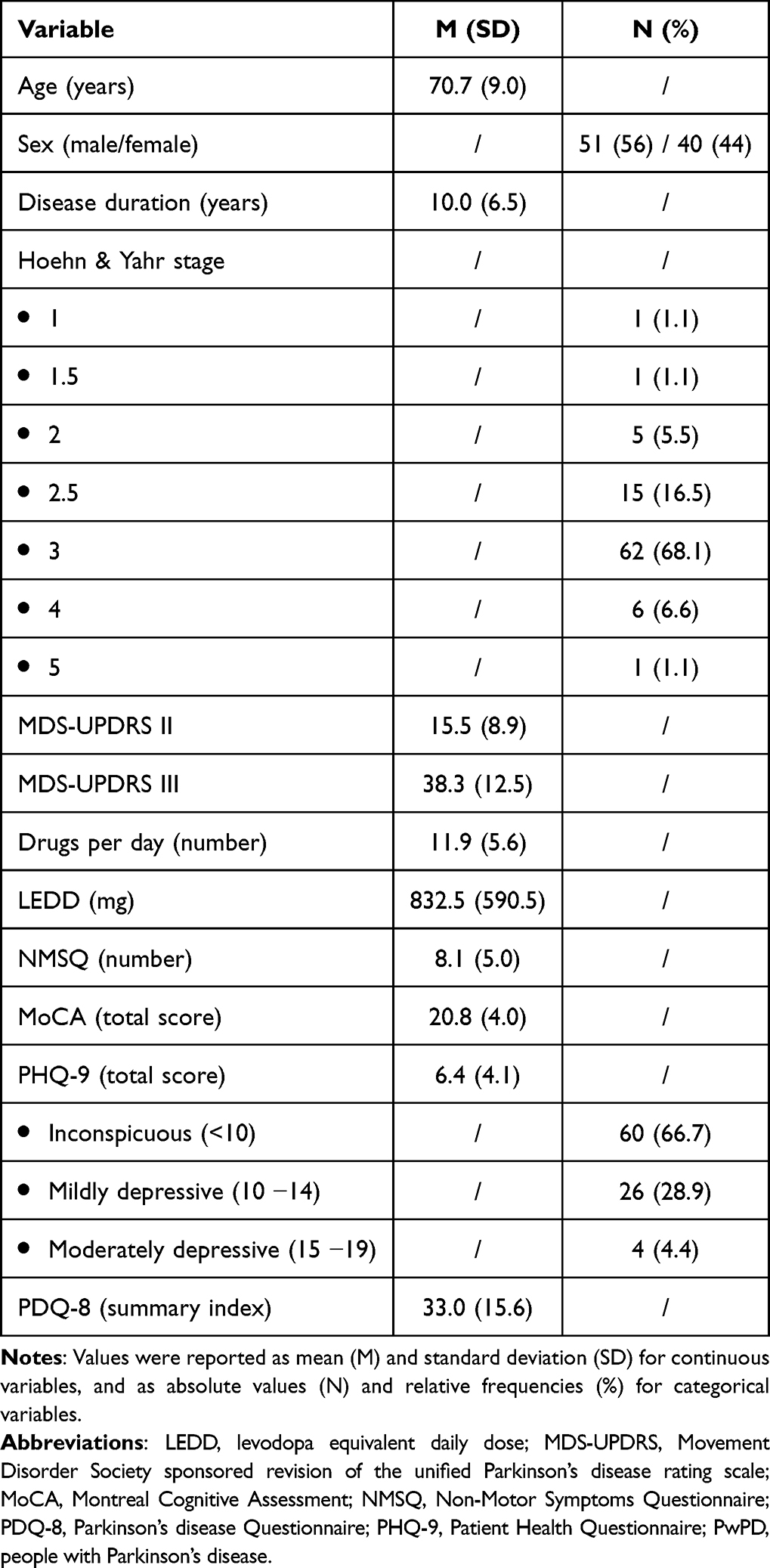 |
Table 1 Characteristics of the Baseline Cohort of PwPD at Hospital Admission (N = 91) |
Changes of PD-Related Characteristics
As shown in Table 2, the longitudinal analysis of the PD-related characteristics showed significant improvements from baseline to both follow-ups regarding motor function (MDS-UPDRS II), the number of non-motor symptoms (NMSQ), and health-related QoL (PDQ-8), and regarding the one follow-up of depressive symptoms (PHQ-9) after six months. The MDS-UPDRS II scores decreased significantly, indicating improved motor aspects of daily living, with a large effect size (p < 0.001, partial eta2 = 0.213). The NMSQ scores also showed a significant reduction in non-motor symptoms, with a large effect size (p < 0.001, partial eta2 = 0.531). Health-related QoL, assessed with the PDQ-8 summary index, improved significantly with a large effect size (p < 0.001, partial eta2 = 0.316). Lastly, depressive symptoms, assessed with the PHQ-9 total score, decreased significantly with a moderate effect size (p < 0.001, r = 0.506).
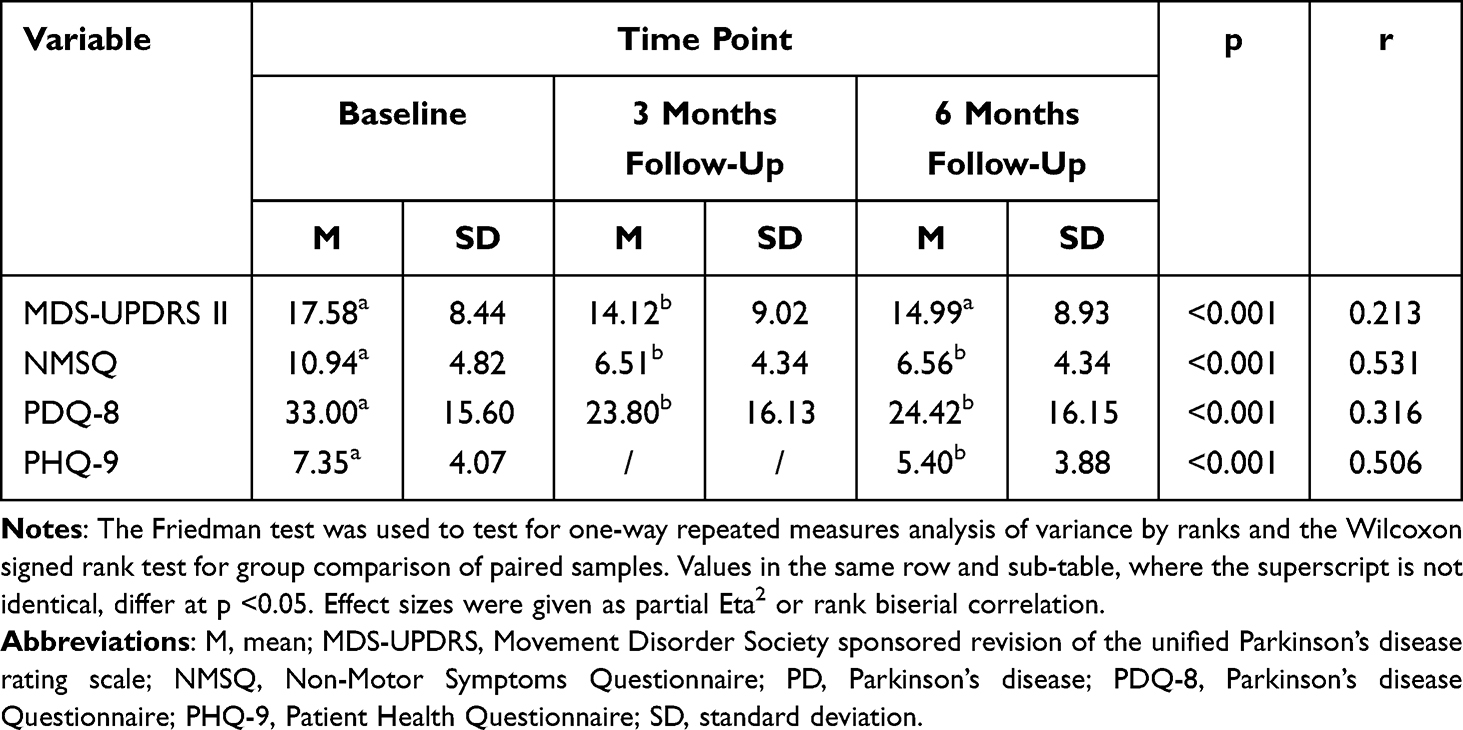 |
Table 2 Longitudinal Changes of PD-Related Characteristics (N = 91) |
Changes of SAMS
The SAMS score demonstrated notable fluctuations across the three time points (Table 3). At the initial measurement point, the mean SAMS score was 8.92 (SD = 7.56). By the first follow-up after three months, the score had decreased to 5.19 (SD = 4.47), indicating an improvement in adherence. This reduction was statistically significant (p < 0.001). By the second follow-up after six months, the SAMS score exhibited a further reduction to 4.21 (SD = 4.41), again, demonstrating a statistically significant improvement in comparison to baseline (p < 0.001). However, the change between the two follow-ups after three and six months was not statistically significant (p = 0.190), indicating that the majority of the improvement occurred within the first three months, and with a minimal further change thereafter.
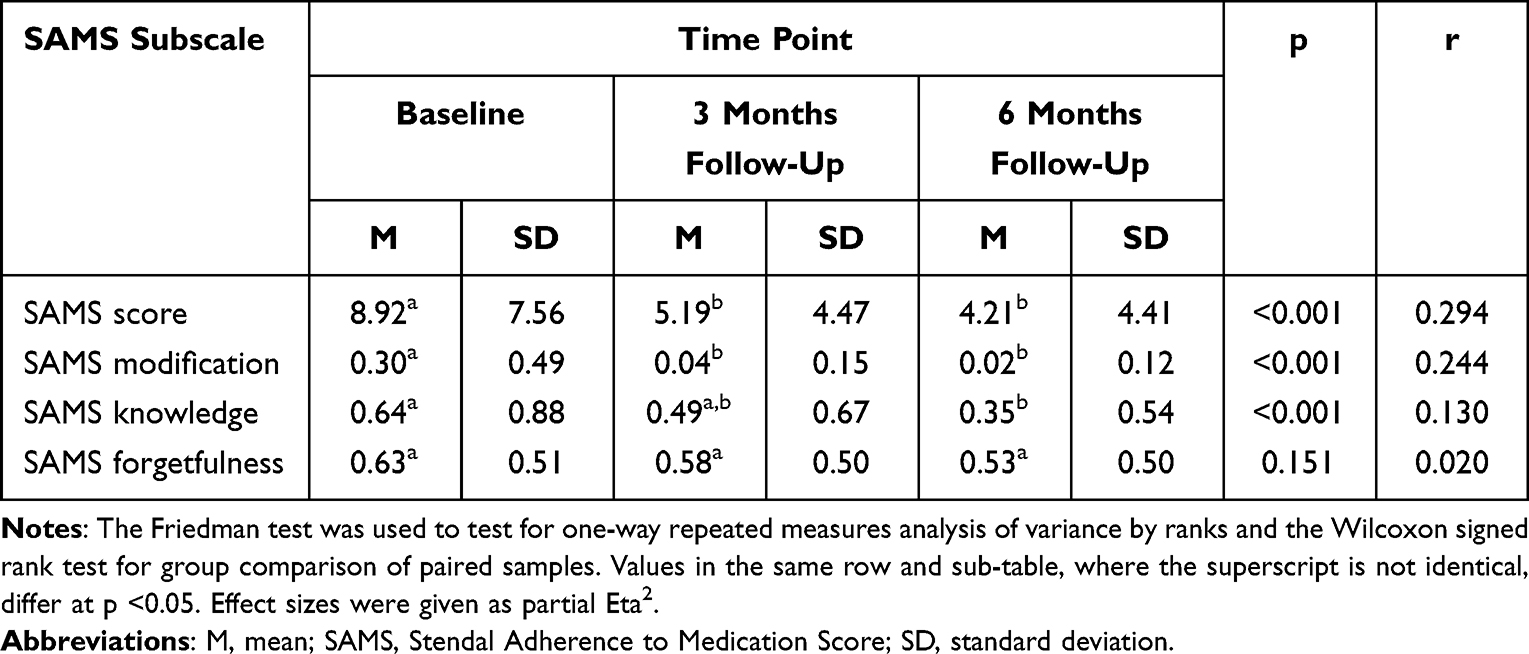 |
Table 3 Longitudinal Changes of SAMS Subscales in PwPD (N = 91) |
The analysis of SAMS subscores across three assessment points revealed significant changes in SAMS modification and SAMS knowledge subscales, while SAMS forgetfulness remained stable (Table 3). For the SAMS modification subscore, PwPD demonstrated a significant decrease in their scores from baseline to the first follow-up at 3 months, with a further slight non-significant decrease to the second follow-up at 6 months. The SAMS knowledge subscore decreased significantly from baseline to the second follow-up after 6 months. In contrast, the SAMS forgetfulness subscore did not exhibit any significant changes over time.
Finally, we determined which PD-related variables (MDS-UPDRS II, NMSQ, PDQ-8, PHQ-9) influence changes of SAMS subscores over time. The results of the three GEE models for the SAMS subscores (forgetfulness, knowledge, modification) show the following (see Table 4).
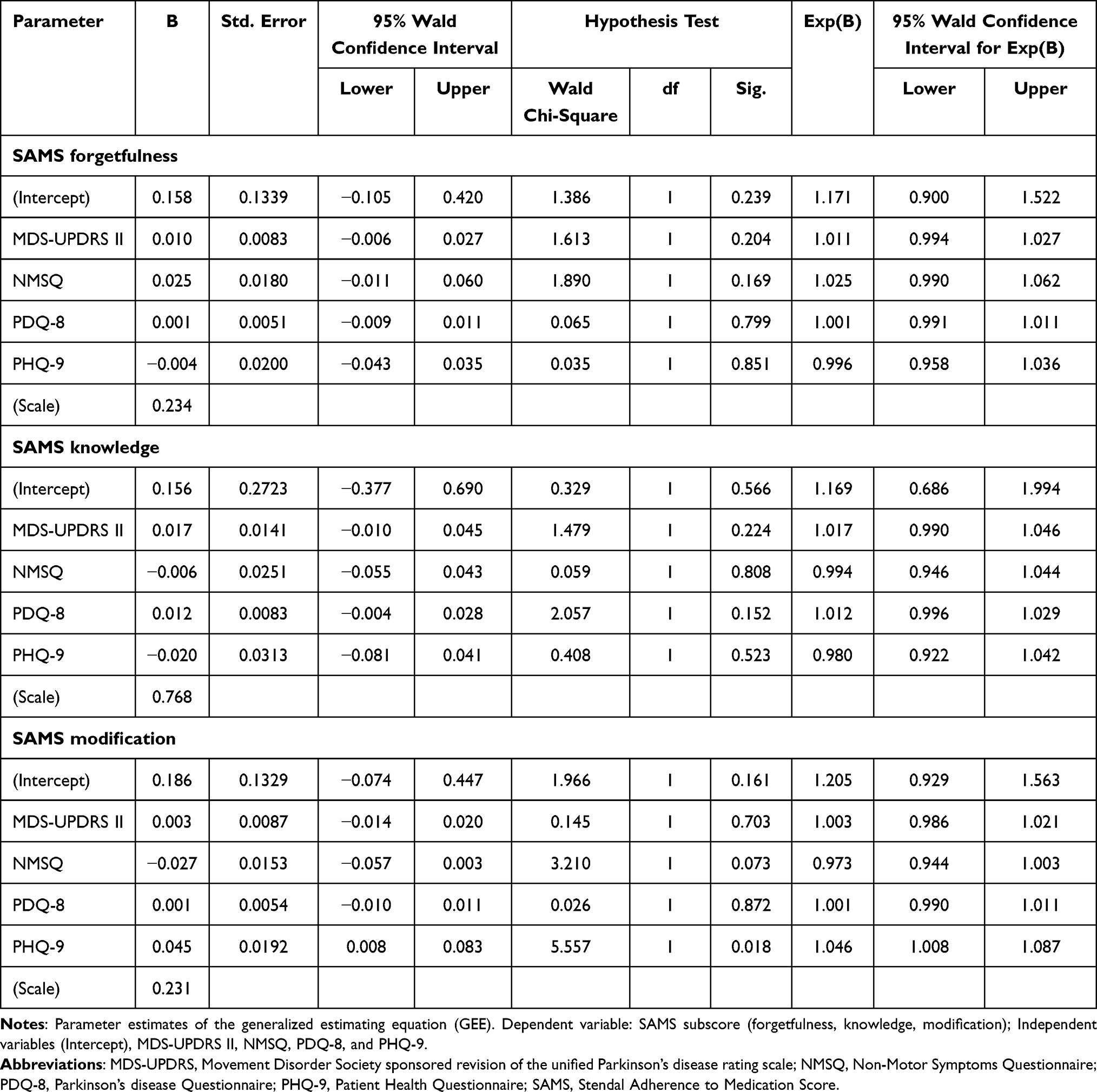 |
Table 4 Predictors of SAMS Subscales, GEE Analysis (N = 91) |
The forgetfulness subscore shows no significant influence of the PD-related variables (MDS-UPDRS II: p = 0.204; NMSQ: p = 0.169; PDQ-8: p = 0.799; PHQ-9: p = 0.851). For the knowledge subscore, the PD-related variables also do not show a significant influence (MDS-UPDRS II: p = 0.224; NMSQ: p = 0.808; PDQ-8: p = 0.152; PHQ-9: p = 0.523). In contrast, the model for the modification subscore shows a significant effect of PHQ-9 (p = 0.018), suggesting that depressive symptoms significantly influence this subscore. Again, no significant effect was determined for MDS-UPDRS II (p = 0.703), NMSQ (p = 0.073), and PDQ-8 (p = 0.872). Overall, the results suggest that the forgetfulness and knowledge subscores are not strongly influenced by the examined PD-related variables. However, the modification subscore shows a significant association with depressive symptoms, indicating a potential psychosocial component.
Discussion
In this study, we examined the longitudinal changes in different types of self-reported medication adherence in PwPD following an interdisciplinary inpatient treatment (PD-MCT). Specifically, we sought to differentiate between intentional and unintentional forms of non-adherence and investigate the factors that may influence changes in these behaviors over time. Our findings highlight the dynamic nature of adherence in PD, revealing that while some aspects of non-adherence improve after discharge from PD-MCT, others remain stable. In this context, the study provides important insights into the limited role that PD-related factors play in explaining these changes.
Our results showed that medication adherence in PD is not a fixed behavior, but changes over time. More specifically, forgetfulness (a form of unintentional nonadherence) remained stable throughout the follow-up period, indicating that forgetfulness does not fluctuate significantly after discharge. In contrast, both modification of medication (intentional non-adherence) and knowledge about medication improved significantly during the follow-up period, with notable reductions in non-adherence in these areas. These improvements suggest that PwPD were better informed and adhered more closely to their prescribed regimens after discharge from PD-MCT. Whether these changes are a consequence of PD-MCT or can also be observed after inpatient treatments of shorter duration or without interdisciplinary care requires further investigation.
Interestingly, the PD-related factors we investigated—such as motor and non-motor symptoms—explained only a small portion of the variance in the observed changes in adherence. Among these factors, only depressive symptoms (PHQ-9) were significantly associated with changes in one form of non-adherence, specifically modification of medication. The associations between depression and non-adherence,36 as well as mood disorders and non-adherence, especially in PD are already known.37 However, our study provided a more detailed analysis of this association. Accordingly, PwPD with higher depressive symptoms were more likely to modify their medication regimens without consulting their healthcare providers, indicating that psychosocial factors may play a more substantial role in influencing intentional non-adherence than clinical variables such as motor and non-motor symptoms as assessed by the MDS-UPDRS II or NMSQ.
Our study supports the growing recognition that adherence is a highly dynamic phenomenon, particularly in chronic conditions like PD.12 Traditional cross-sectional measures of adherence provide only a static snapshot and fail to capture the temporal fluctuations and behavioral changes that occur over time. In contrast, our longitudinal approach revealed distinct trajectories of adherence behavior, especially regarding intentional and unintentional non-adherence. This distinction is critical because the factors driving intentional and unintentional non-adherence are likely to differ, requiring tailored strategies to address each form.
In general, educational and behavioral interventions may improve the proportion of older adults who satisfactorily adhere to their prescribed medications.38 However, further research is necessary to assess the effect of targeted interventions on the subfactors of medication adherence. For example, the stability of forgetfulness implies that interventions aimed at reducing forgetfulness, such as the use of pill organizers, reminders, or caregiver support, should be a consistent part of the treatment plan and not limited to the period immediately following discharge after PD-MCT. On the other hand, the observed improvement in medication knowledge and the reduction in intentional non-adherence after discharge suggest that patient education and counseling during the hospital stay are effective in addressing knowledge gaps. In this regard, further research is necessary to investigate these relationships in more detail. However, the finding that intentional non-adherence (ie, modification of medication) was influenced by depressive symptoms underscores the complexity of adherence behavior. While PwPD may become more knowledgeable about their medications, emotional and psychological factors, such as depression, can undermine their willingness to follow the prescribed regimen. Depression is common in PD and known to affect motivation and decision-making,39,40 which could explain why PwPD with higher levels of depressive symptoms are more likely to modify their medication without consulting a healthcare provider. This highlights the need for mental health interventions alongside educational strategies to improve adherence, particularly for PwPD at risk of intentional non-adherence.37,38
One of the key implications of our findings is that the hospital discharge period appears to be a critical time for interventions aimed at improving adherence. Both modification of and knowledge about medication improved after discharge, suggesting that patients may benefit from the structured environment and increased attention to their care during their hospital stay. However, once PwPD return to the outpatient setting, the support and oversight they received in the hospital may diminish, leading to potential declines in adherence if appropriate follow-up interventions are not in place.
The differences between adherence behaviors in the hospital and after discharge raise important considerations for designing interventional trials. Measures of adherence taken during a hospital stay may not accurately reflect patients’ long-term behavior once they return to their normal routines. Therefore, interventions aimed at improving adherence should be tailored to the outpatient setting, where PwPD are more likely to face challenges related to medication management, such as reduced access to healthcare professionals, lack of caregiver support, or increased burden from managing multiple medications.
The findings from this study have important implications for developing tailored interventions to improve medication adherence in PwPD:
First, our results suggest that educational interventions (eg, as part of PD-MCT) that focus on improving patients’ knowledge about their medications can often be effective and should be a key component of general discharge planning. These interventions should emphasize the importance of following the prescribed regimen and address any misconceptions PwPD may have about their medications.37 Given the significant improvement in knowledge after discharge, continuing education in the outpatient setting through follow-up appointments or telemedicine could help sustain these gains over time.
Second, addressing depressive symptoms is critical for improving adherence, particularly for intentional non-adherence. Depression-specific interventions, such as counseling, psychotherapy, or antidepressant medications, should be integrated into the care plan for PwPD, especially those who show signs of depressive symptoms. By improving mood and motivation, these interventions may reduce the likelihood of PwPD modifying their medication regimens without consulting their healthcare providers.37
Finally, the persistence of forgetfulness as a form of non-adherence highlights the need for practical strategies to support medication-taking behavior in PwPD with cognitive impairments. Interventions such as the use of assistive technologies (eg, medication reminder apps), involvement of caregivers in medication management, and simplifying medication regimens (eg, using long-acting formulations) could help mitigate the impact of forgetfulness on adherence.37 It is therefore important to adopt a medication regime that is tailored to the individual needs of those affected, and which they can realistically take on a regular basis. In order to achieve this objective, it is imperative to consider both the PD-specific medication and the plethora of medications prescribed for individual comorbidities. Reducing polypharmacy is a key factor in improving medication adherence.37,41
The main strength of our study is that it investigated different forms of medication adherence longitudinally in PwPD. This study is the first that differentiates between intentional and unintentional non-adherence and examines how each form changes over time in PwPD. However, despite the valuable insights gained from this study, there are several limitations that should be acknowledged: First, the study relied on self-reported measures of adherence, which are subject to biases such as social desirability and recall bias. PwPD may have underreported their non-adherence due to the desire to appear compliant, or they may have difficulty accurately recalling their medication-taking behavior, particularly if they have cognitive impairments. Second, while we explored the influence of several PD-related factors on adherence, we did not investigate other potentially important variables that could affect adherence, such as certain life circumstances (eg, stressful life events, lifestyle), other relevant medical conditions or diagnoses, social support, access to healthcare, or the complexity of the medication regimen. These factors may play a significant role in adherence behavior, particularly in the outpatient setting, and should be included in future studies. Third, the follow-up period in this study was limited to six months, which may not be sufficient to capture long-term changes in adherence. Future studies should include longer follow-up periods to examine whether the improvements observed after discharge are sustained over time or whether adherence begins to decline as PwPD adjust to life outside the hospital. Finally, our study population consisted of PwPD who were initially admitted to the hospital for PD-MCT, which may limit the generalizability of our findings to other populations. PwPD with less severe disease or those who do not receive such intensive treatment may exhibit different adherence behaviors, and future research should explore adherence trajectories in a broader range of PwPD.
Conclusion
In conclusion, this study highlights the dynamic nature of medication adherence in PwPD and provides important insights into how different forms of non-adherence change over time. The findings suggest that while educational interventions are effective in improving knowledge and reducing intentional non-adherence, addressing depressive symptoms and cognitive impairments is crucial for improving overall adherence. Tailored interventions that combine education, mental health support, and practical strategies for managing cognitive impairments are likely to be most effective in promoting long-term adherence in PwPD. In addition to the ongoing efforts to optimize the medication regimen, future research should continue to explore the factors influencing adherence behavior and develop targeted strategies to support PwPD in maintaining adherence throughout the course of their disease.
Abbreviations
GEE, Generalized Estimating Equation; LEDD, levodopa equivalent daily dose; MDS, Movement Disorder Society; MDS-UPDRS, Movement Disorder Society sponsored revision of the unified Parkinson’s disease rating scale; MoCA, Montreal Cognitive Assessment; NMSQ, Non-Motor Symptoms Questionnaire; PD, Parkinson’s disease; PD-MCT, Parkinson’s disease multimodal complex treatment; PDQ-8, Parkinson’s disease questionnaire-8; PHQ-9, Patient Health Questionnaire-9; PwPD, people with Parkinson’s disease; QoL, quality of life; SAMS, Stendal Adherence to Medication Score; SD, standard deviation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was conducted in line with the Declaration of Helsinki and approved by the ethics committee of the University Hospital Jena (registration number 2021-2228-BO). Written informed consent was obtained from all individual participants before study inclusion.
Acknowledgments
We thank Eric Winter for his help with thorough data acquisition and management during the course of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
TP is supported by Federal Ministry of Education and Research (BMBF, Bundesministerium für Bildung und Forschung) grants (01GY1804, 01GY2301). The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Disclosure
The authors have no relevant financial or non-financial interests to disclose for this work.
References
1. Bloem BR, Okun MS, Klein C. Parkinson’s disease. Lancet. 2021;397(10291):2284–2303. doi:10.1016/S0140-6736(21)00218-X
2. Jankovic J, Tan EK. Parkinson’s disease: etiopathogenesis and treatment. J Neurol Neurosurg Psychiatry. 2020;91(8):795–808. doi:10.1136/jnnp-2019-322338
3. Mendorf S, Witte OW, Grosskreutz J, Zipprich HM, Prell T. What predicts different kinds of nonadherent behavior in elderly people with parkinson’s disease? Front Med Lausanne. 2020;7:103. doi:10.3389/fmed.2020.00103
4. Straka I, Minár M, Gažová A, Valkovič P, Kyselovič J. Clinical aspects of adherence to pharmacotherapy in Parkinson disease: a PRISMA-compliant systematic review. Medicine. 2018;97(23):e10962. doi:10.1097/MD.0000000000010962
5. DiMatteo MR, Giordani PJ, Lepper HS, Croghan TW. Patient adherence and medical treatment outcomes: a meta-analysis. Med Care. 2002;40(9):794–811. doi:10.1097/00005650-200209000-00009
6. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
7. Brown MT, Bussell J, Dutta S, Davis K, Strong S, Mathew S. Medication Adherence: truth and Consequences. Am J Med Sci. 2016;351(4):387–399. doi:10.1016/j.amjms.2016.01.010
8. Weintraub D, Aarsland D, Chaudhuri KR, et al. The neuropsychiatry of Parkinson’s disease: advances and challenges. Lancet Neurol. 2022;21(1):89–102. doi:10.1016/S1474-4422(21)00330-6
9. Straka I, Minár M, Škorvánek M, et al. Adherence to pharmacotherapy in patients with parkinson’s disease taking three and more daily doses of medication. Front Neurol. 2019;10:799. doi:10.3389/fneur.2019.00799
10. Schönenberg A, Heimrich KG, Prell T. Impact of depressive symptoms on medication adherence in older adults with chronic neurological diseases. BMC Psychiatry. 2024;24(1):131. doi:10.1186/s12888-024-05585-7
11. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
12. Chen Y, Gao J, Lu M. Medication adherence trajectory of patients with chronic diseases and its influencing factors: a systematic review. J Adv Nurs. 2024;80(1):11–41. doi:10.1111/jan.15776
13. Alhazami M, Pontinha VM, Patterson JA, Holdford DA. Medication adherence trajectories: a systematic literature review. J Manag Care Spec Pharm. 2020;26(9):1138–1152. doi:10.18553/jmcp.2020.26.9.1138
14. Schönenberg A, Mühlhammer HM, Lehmann T, Prell T. Adherence to medication in neurogeriatric patients: insights from the NeuroGerAd study. J Clin Med. 2022;11(18):5353. doi:10.3390/jcm11185353
15. Richter D, Bartig D, Muhlack S, et al. Dynamics of Parkinson’s disease multimodal complex treatment in Germany from 2010–2016: patient characteristics, access to treatment, and formation of regional centers. Cells. 2019;8(2):151. doi:10.3390/cells8020151
16. Heimrich KG, Prell T. Short- and long-term effect of parkinson’s disease multimodal complex treatment. Brain Sci. 2021;11(11):1460. doi:10.3390/brainsci11111460
17. Müller T, Öhm G, Eilert K, et al. Benefit on motor and non-motor behavior in a specialized unit for Parkinson’s disease. J Neural Transm. 2017;124(6):715–720. doi:10.1007/s00702-017-1701-3
18. Scherbaum R, Hartelt E, Kinkel M, Gold R, Muhlack S, Tönges L. Parkinson’s disease multimodal complex treatment improves motor symptoms, depression and quality of life. J Neurol. 2020;267(4):954–965. doi:10.1007/s00415-019-09657-7
19. Hartelt E, Scherbaum R, Kinkel M, Gold R, Muhlack S, Tönges L. Parkinson’s disease multimodal complex treatment (PD-MCT): analysis of therapeutic effects and predictors for improvement. J Clin Med. 2020;9(6):1874. doi:10.3390/jcm9061874
20. Postuma RB, Berg D, Stern M, et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov Disord. 2015;30(12):1591–1601. doi:10.1002/mds.26424
21. Franke GH, Nentzl J, Jagla-Franke M. Stendal Adherence to Medication Score, SAMS. 2020. Available from: https://psychometrikon.de/test/?id=ff32ee9ea015021c3fb047e505e2bc45.
22. Prell T, Grosskreutz J, Mendorf S, Franke GH, Witte OW, Kunze A. Clusters of non-adherence to medication in neurological patients. Res Social Adm Pharm. 2019;15(12):1419–1424. doi:10.1016/j.sapharm.2019.01.001
23. Schade S, Mollenhauer B, Trenkwalder C. Levodopa equivalent dose conversion factors: an updated proposal including opicapone and safinamide. Mov Disord Clin Pract. 2020;7(3):343–345. doi:10.1002/mdc3.12921
24. Goetz CG, Fahn S, Martinez-Martin P, et al. Movement disorder society-sponsored revision of the unified parkinson’s disease rating scale (MDS-UPDRS): process, format, and clinimetric testing plan. Mov Disord. 2007;22(1):41–47. doi:10.1002/mds.21198
25. Goetz CG, Poewe W, Rascol O, et al. Movement disorder society task force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord. 2004;19(9):1020–1028. doi:10.1002/mds.20213
26. Romenets SR, Wolfson C, Galatas C, et al. Validation of the non-motor symptoms questionnaire (NMS-Quest). Parkinsonism Relat Disord. 2012;18(1):54–58. doi:10.1016/j.parkreldis.2011.08.013
27. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
28. Carson N, Leach L, Murphy KJ. A re-examination of montreal cognitive assessment (MoCA) cutoff scores. Int J Geriatr Psychiatry. 2018;33(2):379–388. doi:10.1002/gps.4756
29. Nasreddine ZS, Phillips NA, Bédirian V, et al. The montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
30. Jenkinson C, Fitzpatrick R, Peto V, Greenhall R, Hyman N. The PDQ-8: development and validation of a short-form Parkinson’s disease questionnaire. Psychol Health. 1997;12(6):805–814. doi:10.1080/08870449708406741
31. Jenkinson C, Fitzpatrick R, Peto V, Harris R, Saunders P. PDQ-39 user manual (including PDQ-8 and PDQ summary index). The parkinson’s disease questionnaire. 2008.
32. Kang H. The prevention and handling of the missing data. Korean J Anesthesiol. 2013;64(5):402–406. doi:10.4097/kjae.2013.64.5.402
33. Friedman M. The use of ranks to avoid the assumption of normality implicit in the analysis of variance. J Am Stat Assoc. 1937;32(200):675–701. doi:10.1080/01621459.1937.10503522
34. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
35. Liang KY, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73(1):13–22. doi:10.1093/biomet/73.1.13
36. Lassen RH, Gonçalves W, Gherman B, et al. Medication non-adherence in depression: a systematic review and metanalysis. Trends Psychiatry Psychother. 2024. doi:10.47626/2237-6089-2023-0680
37. Daley DJ, Myint PK, Gray RJ, Deane KHO. Systematic review on factors associated with medication non-adherence in Parkinson’s disease. Parkinsonism Relat Disord. 2012;18(10):1053–1061. doi:10.1016/j.parkreldis.2012.09.004
38. Cross AJ, Elliott RA, Petrie K, Kuruvilla L, George J. Interventions for improving medication-taking ability and adherence in older adults prescribed multiple medications. Cochrane Database Syst Rev. 2020;5(5):CD012419. doi:10.1002/14651858.CD012419.pub2
39. Reijnders JSAM, Ehrt U, Weber WEJ, Aarsland D, Leentjens AFG. A systematic review of prevalence studies of depression in Parkinson’s disease. Mov Disord. 2008;23(2):
40. Marsh L. Depression and Parkinson’s disease: current knowledge. Curr Neurol Neurosci Rep. 2013;13(12):409. doi:10.1007/s11910-013-0409-5
41. Zhou D, Chen Z, Tian F. Deprescribing interventions for older patients: a systematic review and meta-analysis. J Am Med Dir Assoc. 2023;24(11):1718–1725. doi:10.1016/j.jamda.2023.07.016
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Telemedicine as a Tool to Improve Medicine Adherence in Patients with Affective Disorders – A Systematic Literature Review
Leiz M, Pfeuffer N, Rehner L, Stentzel U, van den Berg N
Patient Preference and Adherence 2022, 16:3441-3463
Published Date: 30 December 2022
Clinical Assessment Tools for the Detection of Cognitive Impairment and Hearing Loss in the Ageing Population: A Scoping Review
Ferguson MA, Nakano K, Jayakody DM
Clinical Interventions in Aging 2023, 18:2041-2051
Published Date: 7 December 2023
Relationship of Glymphatic Function with Cognitive Impairment, Sleep Disorders, Anxiety and Depression in Patients with Parkinson’s Disease
Gui Q, Meng J, Shen M, Feng H, Dong X, Xu D, Zhu W, Cheng Q, Wang L, Wu G, Lu Y
Neuropsychiatric Disease and Treatment 2024, 20:1809-1821
Published Date: 25 September 2024