")
Back to Journals » International Journal of General Medicine » Volume 15
Medication Adherence and Its Influencing Factors Among Inflammatory Bowel Disease Patients in China
Authors Xu F, Tang J, Zhu Z, Chen Y, Hu W, Lu S , Zhou Y, Lin D
Received 23 January 2022
Accepted for publication 5 April 2022
Published 18 April 2022 Volume 2022:15 Pages 4141—4149
DOI https://doi.org/10.2147/IJGM.S359082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Fen Xu,1,* Juping Tang,1,* Zhiping Zhu,2 Yan Chen,3 Wen Hu,4 Sha Lu,5 Yunxian Zhou,6 Ding Lin7
1Department of Nursing, Hangzhou Third Hospital, Hangzhou, People’s Republic of China; 2Department of Vascular Surgery, Hangzhou Third Hospital, Hangzhou, People’s Republic of China; 3Department of Gastroenterology, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 4State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative National Clinical Research Center for Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 5Department of Obstetrics and Gynecology, Hangzhou Women’s Hospital (Hangzhou Maternity and Child Health Care Hospital), Hangzhou, People’s Republic of China; 6School of Nursing, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 7Department of Cardiovascular Medicine, Hangzhou Third Hospital, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yunxian Zhou, School of Nursing, Zhejiang Chinese Medical University, 548 Binwen Road, Binjiang District, Hangzhou, Zhejiang, 310053, People’s Republic of China, Tel +860571-86633121, Email [email protected] Ding Lin, Department of Cardiovascular Medicine, Hangzhou Third Hospital, No. 38 Xihu Road, Hangzhou, Zhejiang Province, 310009, People’s Republic of China, Tel +860571-87827512, Email [email protected]
Purpose: To investigate the current state of medication adherence among patients with inflammatory bowel disease (IBD) in China and analyze the influencing factors.
Patients and Methods: We recruited as many eligible subjects as possible and a total of 105 patients with IBD finished this cross-sectional survey. The General Information Questionnaire and Morisky Medication Adherence Scale were used as measurement instruments. The factors influencing the Morisky score were studied by multiple linear regression analysis.
Results: The average Morisky score was 6.11 ± 1.93. Univariate analysis showed that there were statistically significant differences in Morisky scores among patients with different ages, education levels, disease types, medication administration methods, medication frequencies, disease understanding and knowledge learning frequencies (P < 0.05). Multiple stepwise linear regression analyses showed that medication frequency, medication administration method and disease understanding were important factors influencing the Morisky score (P < 0.001).
Conclusion: Our data confirmed that the medication adherence of IBD patients was poor, especially among patients taking oral medication, those taking medications with a high frequency and those with a low understanding of the disease. To reduce symptom recurrence and control the disease, medical staff should pay attention to the individual patient factors, simplify the medication regimens, formulate effective coping strategies for drug management support.
Keywords: Crohn’s disease, inflammatory bowel disease, medication adherence, ulcerative colitis
Introduction
Inflammatory bowel disease (IBD), which includes ulcerative colitis (UC) and Crohn’s disease (CD), is a chronic idiopathic inflammatory disease with intestinal and extraintestinal features characterized by relapses and periods of remission.1 In the last 20 years, the incidence of IBD has increased rapidly in China, which now has the highest prevalence of IBD of any country in Asia (3.64 per 100,000 people).2 IBD has a long course, is prone to recurrence, and requires long-term medication.3,4 The main drugs currently used for IBD treatment include 5-aminosalicylic acid (5-ASA), corticosteroids, immunomodulators [thiopurines (azathioprine and mercaptopurine) and methotrexate] and biologics [antitumor necrosis factors (infliximab, adalimumab, and certolizumab)] and antiadhesion molecules (monoclonal antibodies).5,6 Medication adherence refers to the process by which patients take their medications as prescribed.7 Currently, the Morisky Medication Adherence Scale (MMAS), which was adapted to the Chinese language by Si et al,8 is commonly used in China to assess medication adherence in patients with IBD. The study showed that the medication adherence of patients with IBD is not ideal. The average treatment nonadherence rate for chronic diseases in developed countries is 50% and even lower in developing countries, and only 20% to 30% among IBD patients in Asia.9 Poor medication adherence can have many adverse consequences. These include increased disease activity,10 relapse,11 loss of response to antitumor necrosis factor drugs,12 increased morbidity and mortality (eg, colorectal cancer), increased health care costs,13 poorer quality of life,14 and higher rates of disability.15 Meanwhile, several studies have shown that good medication adherence among IBD patients plays an important role in improving treatment outcomes and controlling disease recurrence (Gunasekeera, Mendall, Chan, and Kumar, 2016; Holdam et al, 2016; Owczarek, Rodacki, Domagała-Rodacka, Cibor, and Mach, 2016).3,16,17 However, there are few studies on medication compliance among IBD patients in China. The aim of this study was to investigate the current state of medication adherence among IBD patients in China and analyze the factors affecting medication adherence among IBD patients in order to provide a reference point for proposing effective interventions.
Materials and Methods
Study Design and Selection of Participants
This study was reviewed by the hospital ethics committee, and patients from the outpatient of three tertiary general hospitals in Zhejiang, a province located in East China, from September 2020 to June 2021 were selected as study subjects. Data were obtained through questionnaires. Before the questionnaire survey, we screened the patients according to their medical records. Patients were included to questionnaires survey if they met the following criteria: those diagnosed with IBD according to the IBD diagnostic criteria established by the Inflammatory Bowel Disease Group of the Chinese Medical Association Society of Gastroenterology in 2018;18 disease duration ≥ 3 months; age ≥ 18 years; basic reading ability; informed consent provided; and voluntary participation. Patients were excluded if they met the following criteria: patients with concomitant psychiatric disorders, cancer or other serious physical illnesses.
We referred to a rough estimation method with 5–10 times the number of variables to calculate the sample size.19 A total of 20 variables were included in the study; therefore, the required sample size was 100 (20 × 5). Considering a sample loss of 20.0%, the minimum sample size required for this study was 120 participants. We recruited as many eligible subjects as possible.
Data Collection
General Information Questionnaire
Patients’ age, gender, marital status, education level, occupation, length of residence, per capita monthly family income, medical cost payment method, psychological status, family support, doctor-patient relationship, disease type, disease duration, presence of intestinal surgery, medication type, medication administration mode, medication frequency, presence of adverse drug reactions, degree of disease understanding, and frequency of knowledge learning were included.
Morisky Medication Adherence Scale (MMAS)
This questionnaire was developed by Morisky in 2008 based on the original 4-entry Morisky questionnaire to assess patients’ medication adherence.20 The Cronbach’s alpha coefficient of the Chinese version of the MMAS questionnaire was 0.65–0.81, and the intergroup consistency coefficient (ICC) was 0.80–0.92, which had good reliability and validity.8,21 The MMAS has 8 items, 7 of which are closed-ended questions. Questions 1–4 and 6–7 are scored 0 for “yes” and 1 for “no”, question 5 is scored in reverse, and question 8 is scored on a 5-point Likert scale, as follows: 1 for “never”, 0.75 for “occasionally”, 0.5 for “sometimes”, 0.25 for “often”, and 0.25 for “almost always”, and 0 for “always”. A total score of <6 indicates poor adherence, 6–7 indicates moderate adherence, and 8 indicates good adherence.20 We have obtained copyright permission to use MMAS.
Quality Control
The investigators administering the questionnaire received uniform instruction and training to ensure a consistent understanding of the questionnaire content. Uniform instruction language was used to explain to patients the purpose and meaning of the survey and the method of filling out the questionnaire. After the patients completed the questionnaire, it was retrieved on the spot, and timely inquiries were made to ensure the completeness and clarity of the answers if selections had been crossed out or if answers were unclear.
Investigators made a timely check of the patients’ completed information, entered the information truthfully, and double-checked the data.
Statistical Analysis
Continuous data were compared by using independent samples t-test and analysis of variance. We took Morisky score as the dependent variable. In advance dummy variables were created for all categorical variables. The statistically significant factors of univariate analysis were selected for multiple linear regression analysis to study the factors affecting the Morisky score. Statistical analysis was performed using SPSS version 22.0 (SPSS, Armonk, NY, USA). P < 0.05 was considered to indicate a significant difference. All tests were two-tailed analyses.
Results
Analysis of Clinical Data of the Study Subjects
A total of 120 questionnaires were distributed in this study, of which 105 were completed and clear (we regarded them as valid), for an effective recovery rate of 87.5%. Among the 105 study subjects, 67 were male and 38 were female; 28 were UC patients and 77 were CD patients; the mean age was 32.79 ± 10.56 years, and the mean Morisky score was 6.11 ± 1.93. The results of this questionnaire revealed that 31.4% (33/105) of IBD patients had low medication adherence, 43.8% (46/105) had moderate adherence, and 24.8% (26/105) had high adherence, respectively.
Univariate Analysis of Factors Influencing Morisky Score Among Patients with IBD
The Morisky scores showed significant differences in characteristics of participants, such as age and education level (P < 0.05). The differences were not statistically significant when compared with Morisky scores among patients with different genders, marital statuses, occupations, long residences, monthly household incomes, payment methods, psychological status, family support and doctor-patient relationships (P > 0.05). The details are shown in Table 1.
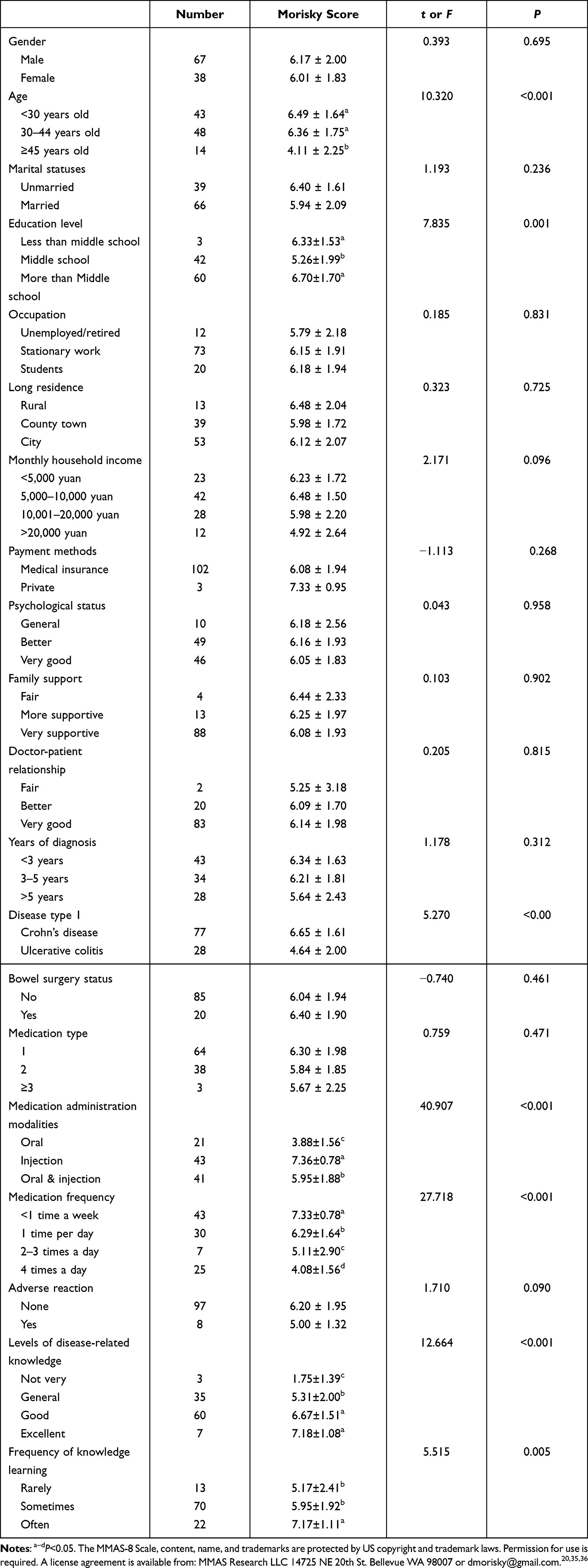 |
Table 1 Univariate Analysis of Factors Influencing Morisky Score Among Patients with IBD |
The Morisky scores showed significant differences in different disease conditions, such as disease types, different medication administration modalities, and medication frequencies (P < 0.05). There was no statistically significant difference in Morisky scores between patients with different years of diagnosis, bowel surgery status, type of medication or adverse reactions (P > 0.05). The details are shown in Table 1.
The Morisky scores showed significant differences in IBD patients’ different disease-related knowledge, such as levels of disease-related knowledge and frequency of knowledge learning (P < 0.05) (Table 1).
Multiple Linear Regression Analysis of Factors Influencing Morisky Score Among Patients with IBD
To explore the factors influencing medication adherence among patients with IBD, we performed multiple linear regression analysis for the seven statistically significant variables (age, education level, disease type, medication administration modalities, medication frequency, levels of disease-related knowledge and frequency of knowledge learning) in univariate analysis process.
The stepwise regression method of multiple linear regression analysis was used, and the multiple linear regression equation model was statistically significant (P < 0.001). The linear regression coefficient of determination indicates that the independent variable can explain 55.6% of the variance in the dependent variable (Table 2).
 |
Table 2 Multiple Linear Regression Analysis Model for Factors Influencing Morisky Scores in IBD Patients |
From the standardized regression coefficients, it can be seen that the frequency of medication, disease knowledge, and medication administration modalities are the factors that have a significant impact on Morisky scores, and patients who take medication four times a day have lower Morisky scores than those who take medication less than once a week (P < 0.001); patients with higher disease knowledge also have higher Morisky scores (P < 0.001); Morisky scores were higher in patients who took injectable medication than in those who took oral medication (P < 0.001). The details are shown in Table 3.
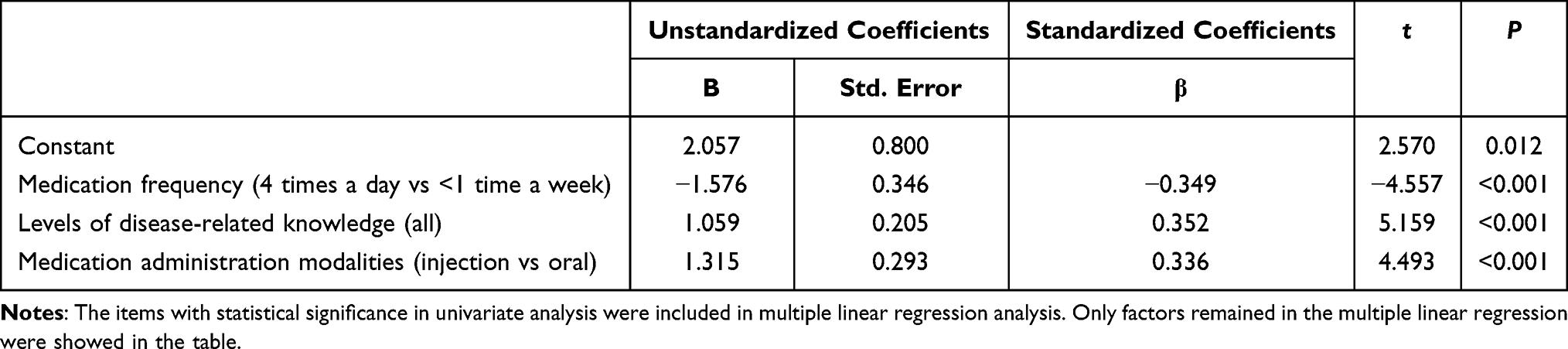 |
Table 3 Multiple Linear Regression Analysis for Factors Influencing Morisky Scores |
Discussion
Through this study, the mean Morisky score of patients with IBD (6.11 ± 1.93) was shown. Morisky et al20 classified medication adherence as low adherence (< 6), moderate adherence (6–7), and high adherence (8) based on the scores derived from the measurement instrument. The results of our study was generally consistent with the low medication adherence rate among Asian IBD patient studies.4 Additionally, the adherence of CD patients in the univariate analysis in this study was better than that of UC patients; the Morisky score of adherence among CD patients (6.65 ± 1.61), was not quite consistent with the results of a cross-sectional survey of medication adherence of CD patients done by a study in which 68.55% were low adherents.22 This may be related to the 6 years between that study and our research and the more widespread use of biologics in recent years or due to that earlier study using the self-reported MAQ medication adherence questionnaire developed by Morisky et al,23 which only contains responses to 4 questions.
In our study, it was concluded that medication frequency had a significant influence on Morisky scores, with patients who took medication four times daily having lower scores than those who took medication less frequently than once daily. This is consistent with the study by Claxton et al.:24 more frequent dosing was associated with lower adherence rates, with significantly higher adherence for once-daily dosing than for four-times-daily dosing (P < 0.001), and higher adherence for twice-daily dosing than for four-times-daily dosing (P = 0.001), although there were no significant differences in adherence between the once daily and twice-daily regimens or between the twice-daily and three-times-daily regimens. Similarly, Devlen et al25 concluded from focus groups and one-on-one interviews with 27 patients with IBD that frequency of dosing was one of the factors influencing the use of mesalazine in patients with IBD, and that placing the medication in multiple containers for dispensing was a way to increase accessibility of the medication, which may prevent situations such as forgetfulness or insufficient medication due to the high frequency of dosing. It has also been shown that after one year of maintenance treatment with grouped administration of mesalazine, either 2.4 g once daily or 1.2 g twice daily, the rates of maintenance remission and relapse were roughly similar in both groups.26 Therefore, simplifying the dosing regimen and minimizing the frequency of dosing may improve patients’ medication adherence.
The results of this study showed that patients’ knowledge of the disease was a factor influencing their medication adherence, and the more comprehensive the patients’ knowledge of the disease, the better their adherence. A prospective study found that poor medication adherence among patients with IBD was associated with a lack of knowledge about the prescribed medication.27 This study also showed that patients with poor adherence had a significantly higher risk of relapse and that having knowledge of the disease and the medication used to treat it was effective in improving disease prognosis.27 Several studies on medication compliance among IBD patients in China also show that lack of knowledge was an important factor.28–30 Patients in our study were generally highly educated, but regression analysis of the variable of different literacy levels showed no statistically significant effect on medication adherence scores. This may be related to the mean age of the patients in our study (32.79 ± 10.56) years, their generally young age, and their high level of education. Although these patients are more knowledgeable about the disease, they may also be more autonomous, less willing to fully comply with treatment recommendations, more likely to change medications frequently and to increase or decrease doses at will, or to feel confident in their control of the disease and medications and therefore more likely to experience nonadherence. This is also consistent with the study by Coenen et al, who found that nonadherence among IBD patients accounted for 1/3 of cases less than 40 years of age, higher education, and use of mesalazine as predictors of low adherence.31 For patients who know more about the disease but have a higher sense of autonomy, we need to pay more attention to their medication adherence. The “knowing, believing, acting” model is a model that influences patients’ beliefs and behaviors by enhancing their awareness, which has a positive effect on patients’ treatment confidence and behaviors.32 The premise and foundation of medication adherence are disease awareness, correct understanding of the disease, knowledge of long-term medication as an essential tool for the treatment and control of IBD, and guidance offered to patients on the correct use of medication, knowledge of medication, and understanding of the possible adverse effects of medication and the importance of adherence to medication during remission.
The results of this study showed that patients’ medication adherence was influenced by the medication administration modalities, with injectable medication having better adherence than oral medication. This may be related to the fact that oral medication is mostly mesalazine, which is taken frequently, easily forgotten, and delayed by work and life chores, while injectable medication is mostly biologic, mostly administered once every 8 weeks, with less frequency and fewer adverse effects, so patients are relatively more likely to comply. This is consistent with Rapport et al’s study, in which patients were more positive in their acceptance of infliximab because they felt it required only returning to the hospital once every few weeks for dosing, rather than having to remember to take the drug every day.33 There are also studies that have found statistically and clinically significant improvements in quality of life for patients with IBD treated with biologic therapies.3 It is evident that patients are more likely to comply with biologic therapy because of its ease of use and relative efficacy. In the present study, we found that patients who took oral medication along with an injection had better compliance than those who took oral medication only; this is probably because the only oral medication in this study was mostly mesalazine, usually 3–4 times a day, while patients who took oral medication along with a biologic injection were mostly receiving immunologic or biologic agents, and the oral frequency was usually once a day or once a week, so their compliance was better than for oral medication only. This is also consistent with the inference from this study, that the frequency of dosing is an important factor influencing patients’ medication compliance. In addition to oral and injectable dosing, a survey on the use of mesalazine rectal suppositories among patients with IBD showed that intentional nonadherence was common among patients using mesalazine rectal suppositories, with only 26% of subjects achieving full adherence, and patients with IBD who were nonadherent to mesalazine rectal suppositories often cited the mode of administration as the reason for nonadherence.34 Therefore, improving the dosing regimens may be a factor in improving medication adherence among IBD patients. Selecting the appropriate dosing regimen for different population characteristics may improve patient adherence.
Some limitations remain to be discussed. First, because of the COVID-19 epidemic, the sample size was limited, and it could be further expanded. Second, to further understand the deep-seated causes of medication nonadherence among IBD patients, it is necessary to conduct further qualitative research by purposeful sampling.
Conclusion
In conclusion, the state of medication adherence among patients with IBD is not optimistic, and patients with high medication frequency, low understanding of the disease, and oral medications show generally poor adherence. In addition to good disease education and effective communication, health care professionals should also pay attention to individualized patient factors, simplify medication regimens, develop effective response strategies supported by medication management, emphasize the importance of standardized medication use in IBD patients, and improve patient medication adherence to achieve the goal of reducing relapse and controlling the disease.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Considerations
Ethical approval for this study was obtained from the ethics committee of Hangzhou Third Hospital (written permission with approval number 2021KA022), and written informed consent (electronic form) was obtained from each participant. This study was performed in accordance with the Declaration of Helsinki.
Acknowledgments
The authors thank all the staff and patients who participated in this study. The MMAS-8 Scale, content, name, and trademarks are protected by US copyright and trademark laws. Permission for use is required. A license agreement is available from: MMAS Research LLC 14725 NE 20th St. Bellevue WA 98007 or dmorisky@gmail.com.20,35,36
Author Contributions
Conceptualization: F Xu, Y Zhou, D Lin; Data curation: F Xu, J Tang, Y Chen, W Hu, S Lu, Z Zhu; Data analysis: F Xu, J Tang, D Lin; Study supervision: D Lin, Y Zhou; Manuscript writing: F Xu, J Tang, Y Zhou. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Social Development Scientific Research Projects of the Science and Technology Bureau of Hangzhou (Grant 20201231Y029).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chan W, Chen A, Tiao D, Selinger C, Leong R. Medication adherence in inflammatory bowel disease. Intest Res. 2017;15(4):434–445. doi:10.5217/ir.2017.15.4.434
2. Ng SC, Kaplan GG, Tang W, et al. population density and risk of inflammatory bowel disease: a prospective population-based study in 13 countries or regions in Asia-Pacific. Am J Gastroenterol. 2019;114(1):107–115. doi:10.1038/s41395-018-0233-2
3. Holdam AS, Bager P, Dahlerup JF. Biological therapy increases the health-related quality of life in patients with inflammatory bowel disease in a clinical setting. Scand J Gastroenterol. 2016;51(6):706–711. doi:10.3109/00365521.2015.1136352
4. Jackson CA, Clatworthy J, Robinson A, Horne R. Factors associated with non-adherence to oral medication for inflammatory bowel disease: a systematic review. Am J Gastroenterol. 2010;105(3):525–539. doi:10.1038/ajg.2009.685
5. Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 2: current management. J Crohns Colitis. 2012;6(10):991–1030. doi:10.1016/j.crohns.2012.09.002
6. Mowat C, Cole A, Windsor A, et al. Guidelines for the management of inflammatory bowel disease in adults. Gut. 2011;60(5):571–607. doi:10.1136/gut.2010.224154
7. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
8. Si Z, Guo L, Zhou M. Reliability and validity of the modified morisky medication adherence scale applied to patients on warfarin therapy after mechanical heart-valve replacement. J Nurs Sci. 2012;27(22):23–26. doi:10.3870/hlxzz.2012.22.023
9. De Geest S, Sabaté E. Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs. 2003;2(4):323. doi:10.1016/S1474-5151(03)00091-4
10. Kane S, Huo D, Aikens J, Hanauer S. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis. Am J Med. 2003;114(1):39–43. doi:10.1016/S0002-9343(02)01383-9
11. Khan N, Abbas AM, Koleva YN, Bazzano LA. Long-term mesalamine maintenance in ulcerative colitis: which is more important? Adherence or daily dose. Inflamm Bowel Dis. 2013;19(6):1123–1129. doi:10.1097/MIB.0b013e318280b1b8
12. van der Have M, Oldenburg B, Kaptein AA, et al. Corrigendum: non-adherence to anti-TNF therapy is associated with illness perceptions and clinical outcomes in outpatients with inflammatory bowel disease: results from a prospective multicentre study. J Crohns Colitis. 2018;12(11):1381. doi:10.1093/ecco-jcc/jjy083
13. Lenti MV, Selinger CP. Medication non-adherence in adult patients affected by inflammatory bowel disease: a critical review and update of the determining factors, consequences and possible interventions. Expert Rev Gastroenterol Hepatol. 2017;11(3):215–226. doi:10.1080/17474124.2017.1284587
14. Varni JW, Shulman RJ, Self MM, et al. Perceived medication adherence barriers mediating effects between gastrointestinal symptoms and health-related quality of life in pediatric inflammatory bowel disease. Qual Life Res. 2018;27(1):195–204. doi:10.1007/s11136-017-1702-6
15. Perry J, Chen A, Kariyawasam V, et al. Medication non-adherence in inflammatory bowel diseases is associated with disability. Intest Res. 2018;16(4):571–578. doi:10.5217/ir.2018.00033
16. Gunasekeera V, Mendall MA, Chan D, Kumar D. Treatment of crohn’s disease with an Igg4-guided exclusion diet: a randomized controlled trial. Dig Dis Sci. 2016;61(4):1148–1157. doi:10.1007/s10620-015-3987-z
17. Owczarek D, Rodacki T, Domagała-Rodacka R, Cibor D, Mach T. Diet and nutritional factors in inflammatory bowel diseases. World J Gastroenterol. 2016;22(3):895–905. doi:10.3748/wjg.v22.i3.895
18. The Inflammatory Bowel Disease Group of the Chinese Medical Association Digestive Diseases Branch. Consensus on diagnosis and treatment of inflammatory bowel disease (Beijing, 2018), Chin J Dig. 2018;38(5):292–311. Chinese. doi:10.3760/cma.j.issn.0254-1432.2018.05.002
19. Ni P, Chen J, Liu N. The sample size estimation in quantitative nursing research. Chin J Nurs. 2010;45(4):378e80. Chinese. doi:10.3761/j.issn.0254-1769.2010.04.037
20. Morisky DE, Ang A, Krousel-Wood M, Ward HJ. Predictive validity of a medication adherence measure in an outpatient setting. J Clin Hypertens. 2008;10(5):348–354. doi:10.1111/j.1751-7176.2008.07572.x
21. Wang J, Mo Y, Bian R. Evaluation of reliability and validity of application of the Chinese version of 8-item morisky medication adherence scale in patients with type 2 diabetes. Chin J Diabetes. 2013;21(12):1101–1104. doi:10.3969/j.issn.1006-6187.2013.12.013s
22. Xu W. Investigation and influencing factors of drug compliance in patients with Crohn’s disease. Zhejiang Univ. 2014:23–24. Chinese.
23. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
24. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther. 2001;23(8):1296–1310. doi:10.1016/S0149-2918(01)80109-0
25. Devlen J, Beusterien K, Yen L, Ahmed A, Cheifetz AS, Moss AC. Barriers to mesalamine adherence in patients with inflammatory bowel disease: a qualitative analysis. J Manag Care Spec Pharm. 2014;20(3):309–314. doi:10.18553/jmcp.2014.20.3.309
26. Wang Y, Parker CE, Feagan BG, MacDonald JK. Oral 5-aminosalicylic acid for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2016;2016(5):CD000544. doi:10.1002/14651858.CD000544.pub4
27. Tae CH, Jung SA, Moon HS, et al. Importance of patients’ knowledge of their prescribed medication in improving treatment adherence in inflammatory bowel disease. J Clin Gastroenterol. 2016;50(2):157–162. doi:10.1097/mcg.0000000000000431
28. Li W, Gao X, Liu M. Influencing factors and nursing countermeasures of medication compliance in patients with Crohn’s disease. Nurs Pract Res. 2019;16(13):32–34. Chinese. doi:10.3969/j.issn.1672-9676.2019.13.013
29. Fei H, Li W, Guo W. Study on influencing factors of treatment compliance of oral medication for ulcerative colitis. Chin Pharm. 2018;5:87–90. Chinese. doi:10.3969/j.issn.1006-4931.2018.05.027
30. Bai Y, Song Y, Bian Q, et al. Medication adherence and its influencing factors among inflammatory bowel disease patients. Chin Gen Prac. 2019;32:4018–4022. Chinese. doi:10.3969/j.issn.1007-9572.2017.00.043
31. Coenen S, Weyts E, Ballet V, et al. Identifying predictors of low adherence in patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol. 2016;28(5):503–507. doi:10.1097/meg.0000000000000570
32. Sun G, Tian Y, Zhang M, Men M, Li D. The effect of knowledge belief and behavior model on the compliance of patients in special ward. China Med. 2019;15(5):730–732. Chinese. doi:10.3760/j.issn.1673-4777.2020.05.022
33. Rapport F, Clement C, Seagrove AC, Alrubaiy L, Hutchings HA, Williams JG. Patient views about the impact of ulcerative colitis and its management with drug treatment and surgery: a nested qualitative study within the CONSTRUCT trial. BMC Gastroenterol. 2019;19(1):166. doi:10.1186/s12876-019-1085-y
34. Boyle M, Ting A, Cury DB, Nanda K, Cheifetz AS, Moss A. Adherence to rectal mesalamine in patients with ulcerative colitis. Inflamm Bowel Dis. 2015;21(12):2873–2878. doi:10.1097/mib.0000000000000562
35. Krousel-Wood MA, Islam T, Webber LS, Re RS, Morisky DE, Muntner P. New Medication Adherence Scale Versus Pharmacy Fill Rates in Seniors with Hypertension. Am J Manag Care. 2009;15(1):59–66.
36. Morisky DE, DiMatteo MR. Improving the measurement of self- reported medication nonadherence: Rnal response. J Clin Epidemi. 2011;64:258–263.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.