Back to Journals » Advances in Medical Education and Practice » Volume 13
Medical Students’ Participation in Extracurricular Activities: Motivations, Contributions, and Barriers. A Qualitative Study
Authors Achar Fujii RN ![]() , Kobayasi R, Claassen Enns S
, Kobayasi R, Claassen Enns S ![]() , Zen Tempski P
, Zen Tempski P
Received 29 January 2022
Accepted for publication 17 May 2022
Published 23 September 2022 Volume 2022:13 Pages 1133—1141
DOI https://doi.org/10.2147/AMEP.S359047
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Renata Nunes Achar Fujii,1,2 Renata Kobayasi,1 Sylvia Claassen Enns,1 Patricia Zen Tempski1
1Centro de Desenvolvimento de Educação Médica (CEDEM), Universidade de São Paulo, São Paulo, SP, Brazil; 2Municipal University of São Caetano do Sul, São Caetano do Sul, SP, Brazil
Correspondence: Sylvia Claassen Enns, Centro de Desenvolvimento de Educação Médica (CEDEM), Universidade de São Paulo, Av. Dr. Arnaldo 455, 2 Floor, Room 2343, São Paulo, SP, Brazil, Tel +55(11) 3061 7472, Email [email protected]
Introduction: Extracurricular activities in medical education are defined as any social, philanthropic, non-mandatory, and unpaid activities. These activities promote interactions between students and the community in ways that both provide care and create learning opportunities and experiences for both students and the community at large. This study elaborates on the motivational aspects, learnings, and barriers that occur when students participate in these activities.
Methods: This is a cross-sectional study of medical students in their first to fifth years. Qualitative analyses have been used to understand the motivation, barriers, and contributions associated with extracurricular activities participation.
Results: Of the 586 students enrolled in the medical course, 462 students agreed to participate in the research. The students reported that they were motivated to participate in contributing to society, support their professional choices, integrate their knowledge, gain life experience, develop communication and leadership skills, learn to work in a team, and become more responsible, empathetic, and resilient. Barriers to participation were the limited number of available positions, selection criteria, lack of support from those involved, personal issues, poor time management, risk of lowered academic performance, and lack of physical and financial resources.
Discussion: Medical students are motivated to participate in Community-based extracurricular activities (CBEA) and this experience leads to improvement in the curriculum and can develop fundamental skills and attitudes such as leadership, commitment, and responsibility. To maximize the benefits of these activities, schools must support students and ensure that they have the time and chance to participate without physical strain, that were barriers mentioned by the academics.
Keywords: quality of life, education, medical, students, medical, community-institutional relationships
Introduction
Medical students have a strong inclination to pursue extracurricular activities.1 Extracurricular activities in Brazil are defined as any social, philanthropic, non-mandatory, and unpaid activities. These include music, physical activities, volunteer work, participating in academic leagues and congresses, and so on.2,3 Community-based extracurricular activities (CBEA) are activities that students perform in the community using the knowledge acquired at graduation, for example, giving lectures to adolescents from schools in the municipality about sexually transmitted diseases, advising mothers in the municipality about breastfeeding, making conversation circles for the community about diabetes and hypertension, training health workers in disease prevention, among countless other actions that students are able to contribute to improve the lives of citizens. They provide learning and developmental experiences for both students and the community at large.
Participating in CBEA can add a human approach to medical training. However, most students primarily focus on updating their scientific knowledge while studying at graduate school. They usually neglect the development of other important skills and attributes required to offer humanized care in the future.4 Thus, it can be stated that teaching should facilitate the reproduction of knowledge, and research should be linked to ongoing developments in science. In addition, CBEA should lead to the execution of knowledge based on research and educational curriculum.5 These activities could be organized by universities or academic leagues and should ideally focus on both the students’ interests and societies’ needs.
The academic leagues at the Municipal University of São Caetano do Sul encourage interaction with the community, in addition to teaching and research. This study identifies and elaborates upon the motivating and demotivating factors that are associated with the academic practice in CBEA. It identifies the contributions of such activities to the students’ overall development.
Methods
Study Design
This qualitative cross-sectional study was conducted in 2018, using the narratives of medical students from the School of Medicine at the Municipal University, São Caetano. Participation was voluntary and anonymity was guaranteed. Moreover, access to the results was also guaranteed. No monetary compensation or incentive was offered for participating. Refusal to participate did not result in loss or damage of any kind. The project was submitted to the Research Ethics Committee (CEP) of São Paulo University (USP) and approved without restrictions (CAAE: 99776718.4.0000.0065).
Participants
All medical students (586) from the School of Medicine, Municipal University, São Caetano, were invited to participate in the study in the end of the class. As the university was new at the time of the data collection, there were only students from the first to the fifth year of graduation. This University adopts the Problem Based Learning (PBL) teaching method. Participants signed the Consent Term authorizing the anonymous publication of responses. Participants were asked to respond to a sociodemographic questionnaire and answer three open questions with no time limit to respond.
Instruments
The sociodemographic questionnaire included questions on the participant’s gender, age, and graduation year. It also inquired about the CBEA in which they had participated as well as whether they were considering specializing in any specific field in the future.
The open-ended questions were as follows: What was your motivation to participate in these activities? What lessons did you learn from these activities? What were the barriers that hindered your participation in these activities?
Data Analysis
Content analysis was used for the qualitative analysis.6 This includes a set of systematic and objective techniques and procedures to describe the contents in a way that allows categorization, elaboration of inferences, and the interpretation of the data. Two of the researchers utilized the traditional content analysis methods to analyze the data. This involved the preparation of the material (typing the answers to the open questions and organization of the data), free reading, highlighting the subjects by relevance and/or repetition, categorization of the emerging categories and derived issues, a discussion with all the members of the research group, and a descriptive presentation of the results using quotes from the responses. The Consolidated Criteria for Reporting Qualitative Studies (COREQ) was used to ensure the study’s quality criteria7 (Supplementary Files).
Results
The initial sample included 586 students (200 males and 386 females) enrolled at the School of Medicine, Municipal University, São Caetano do Sul. Valid responses were received from 462 participants (response rate 78.83%). These included responses from 303 females (65.6%) and 159 males (34.4%). While 110 students were from the first year (23.80%, 29 male students [26.4%] and 81 female students [73.6%]), 91 students were from the second year (19.69%, 37 male students [40.7%] and 54 female students [59.3%]); 90 students were from the third year (19.48%, 31 male students [34.4%] and 59 female students [65.6%]), 89 were from the fourth year (19.26%, 34 male students [38.2%] and 55 female students [61.8%]), and 82 students were from the fifth year (17.74%, 28 male students [34.1%] and 54 female students [65.9%]). The participants’ ages ranged from 17 to 45 years. The average age was 22.72 years.
Out of the total participants, 194 (41.99%, 63 male students and 131 female students) did not participate in any CBEA. Of these 194 students, 98 (89.1%) were first-year students, 37 (40.7%) were second-year students, 20 (22.2%) were third-year students, 10 (11.2%) were fourth-year students, and 29 (35.4%) were fifth-year students.
The questions had three central themes: motivation, learnings, and barriers. Within these themes, the responses were categorized and subdivided into items. The answers were transcribed as examples of each category and item.
The respondents stated that contribution to society, with the possibility of being able to help the community, was the primary motivation for participating in these activities. Students also indicated that these activities assist in increasing professional knowledge as they help develop a better understanding of the different fields in which the students can specialize. CBEA also complements the course. One participant said:
My motivation is to deepen my knowledge on subjects that I believe are not focused upon in the curriculum. (Male, 22 years, 4th year)
Some respondents stated that their motivation was primarily academic development, which was categorized under a personal curriculum. This was primarily due to the impact of CBEA on the medical residence selection process and the requirement to accumulate extracurricular hours for the course. Other respondents mentioned that social interaction is also a motivating factor, as participation in CBEA provides them with the opportunity to connect with teachers and colleagues in the medical program. Table 1 elaborates on these comments.
 |
Table 1 Qualitative Analysis of the Data Produced from the Central Theme: Motivation |
Most of the responses indicated that the participants took part in CBEA because they wanted to know about the different fields they could specialize in. This was followed by the desire to complement the program, help society, gain personal and life experiences, boost personal growth, accumulate credits, and build a network.
Regarding the theme and learning area, the respondents stated that participating in CBEA enabled them to further expand and integrate their knowledge of medicine. They also stated that CBEA helped them acquire time management skills and enhance their communication abilities. One student said:
We learned how to communicate information in a clearer manner to a population that does not understand technical language. (Male, 25 years, 3rd year)
Since academic leagues’ CBEA are organized by students, the participants stated that the experience helped them develop organizational skills and the ability to work in a team. They stated that these activities contribute toward improving leadership skills and teach commitment and responsibility. They also stated that these activities enable the development of emotional skills, such as empathy and resilience.
Table 2 shows some of the statements made regarding learning at the hospital and in the community.
 |
Table 2 Qualitative Analysis of the Data Produced from the Central Theme: Learning |
The majority of the responses implied that the respondents wanted to expand their knowledge and familiarize themselves with their community. They also wanted to acquire communication skills and empathy, learn to work in a team, and develop an understanding of the hospital environment, besides integrating their knowledge and developing their organizational, leadership, and time management skills. Additionally, they sought to understand the commitment and build on their resilience.
Within the theme of barriers, students understood that the limited number of participants in each program was a demotivating factor. This also applies to the availability of tests for the selection of members and the failure to organize some activities. Other barriers indicated by the students included a lack of support from the college, community, partner institutions, and other students.
The main barrier is when the group that participates does not do the work they were supposed to, while the other members are overloaded. (Female, 25 years, 5th year)
Institutions do not accept our projects or create unsustainable conditions (for example, an unviable number of weekly visits). (Male, 32 years, 3rd year)
Teachers were also concerned about the possible losses in academic performance. This is because students would require time for CBEA and thus spend less time studying. Students were also concerned about the money they spent on transportation to CBEA and eating before they attended classes; they also expressed concerns regarding working during their spare time.
Students described that physical exhaustion, such as tiredness and lack of sleep, also make participation difficult. A student stated:
Due to extracurricular activities, I am constantly rushing, and [I] do not have time for my meals or to sleep. (Female, 23 years, 3rd year)
Other barriers mentioned by students included personal difficulties associated with self-displacement and a lack of knowledge regarding the activities. First-year students also stated that they did not participate because they needed time to adapt to the medical school and the problem-based learning approach.
Furthermore, the inability to decide on the extracurricular activity in which to participate was a barrier. The participants also stated that they had difficulty in time management. A student elaborated:
The main barrier is the personal difficulty associated with time management, as sometimes I cannot fully benefit from the activity that I participated in because I have not organized my time properly. (Female, 23 years, 3rd year)
Table 3 elaborates on the comments pertaining to the barriers.
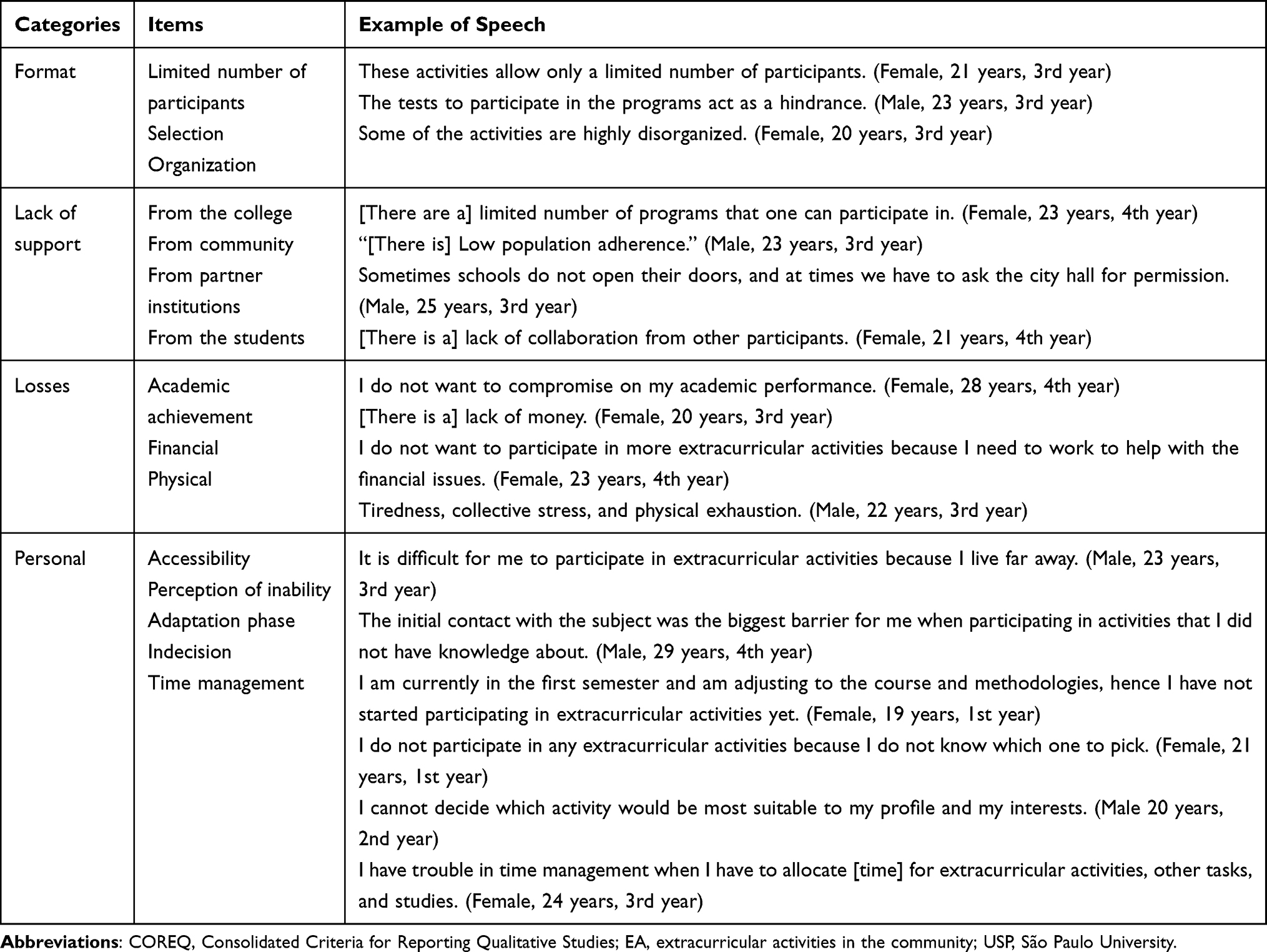 |
Table 3 Qualitative Analysis of the Data Produced from the Central Theme: Barriers |
Most of the responses demonstrated that the participants were concerned about time management. This was followed by the distance that they needed to travel to participate, their physical limitations, and the limit on the number of participants by the type of activity. Further barriers included perception of their lack of skill, the time required to adapt to the school, experiencing financial problems, lack of support from institutions and organizations, the pressure of maintaining their academic achievement, and their indecision on which activity to choose.
Discussion
Most students (58%) stated that they were interested in participating in CBEA. However, the participation was lowest among students in their first year (10.9%). Participation increased with each year. The participation of fourth-year students was 88.8%.
This study reiterates that medical students are motivated to participate in CBEA as this experience adds to their credits and leads to improvement in the curriculum.1,3,8–12 Students also expressed that their desire to help society is a motivating factor to participate in these activities. It is noteworthy that the desire to help people is the reason that many students choose medicine as a profession. However, while their subject matter expertise develops, they often lose sight of their primary motivation.13 Community-based CBEA allows for a curriculum balance. This teaches students to develop an understanding of their patients.
Other important motivations stated are the opportunities to gain experiences and personal learning that might help students develop as individuals and professionals. These experiences allow students to see beyond their own universe, reflect on their values and internalize, adopt, and practice values that are important for their future. Da Silveira et al14 stated that students who participate in CBEA display high levels in the affective domain, indicating that they could internalize new experiences and change how they were living. Additionally, these students also had high cognitive levels that corresponded to the synthesis capacity, while students who did not participate in these activities remained in the lowest taxonomy,15 strictly pertaining to knowledge. Lins et al16 mentioned that CBEA promotes the integration between teachers, students, and the community and allows them to share and exchange knowledge.
According to Cohen and Sherif,17 human values include honesty, integrity, care, compassion, altruism, empathy, and respect for oneself, patients, peers, and other professionals involved in medical care. A number of these skills and competencies are mentioned as learnings that are acquired through participation in CBEA.
It is important to consider that practical experience is required to develop the right skills and attitudes. Therefore, after the completion of the medical degree, without the practical experience of these activities, practitioners should not be expected to possess the appropriate skills.18,19 It is necessary to complement technical training with practical experience.12 By participating in CBEA, professionals will be able to comprehend that solely theoretical knowledge is not sufficient to develop the skills required for coping with social complexities.19
Community-based CBEA provides exposure to real-life in higher education and creates the right skill set for the benefit of the community.5 Thus, professionals will understand that health does not merely imply the absence of disease and a vision that is restricted to biological functioning. It is an integration of the biological, social, cultural, economic, political, and historical dimensions of an individual.
Paulo Freire, an educator and philosopher recognized for his work in adult education, stated, “Nobody educates anyone, nobody educates themselves, men educate themselves, mediated by the world”20 [pp. 78]. This statement implies that before someone can teach something to another person, they must first learn about the other person to understand their situation.
According to Lins et al16 the confrontation with reality allows students to learn, for example, that the lack of information regarding the prevention of certain pathological problems leads to a higher incidence of their occurrence. Therefore, CBEA can contribute to the democratization of knowledge. Students can act as facilitators of knowledge. Consequently, this can have an impact on public health through the association between the learned theory and the experience.16 Evidently, these activities contribute to the advancement of local education because they assist students in uncovering gaps in their community’s knowledge.
Emotional skills such as empathy and resilience can be developed through CBEA. De Almeida and Barbosa19 reinforced that empathy is the social aptitude to understand the feelings of others and the adoption of their perspective with respect to the differences in the way people deal with the situations they experience. The responses indicated that these activities allow students to experience emotions when they observe others, reflect on their own privileges, or are surprised by the unexpected events of daily life.
If the emotions and rationales contribute to the culture of a society, new practices can be introduced based on the same.21 Developing a humane attitude is easier during education than after a professional has developed his or her method of conduct.13 The empathy arising from social contact also encourages students to work in favor of a more just and egalitarian society.16 This will solidify the desire for a democratic public health system that is capable of ensuring services for all segments of society.22
The participants also mentioned that CBEA made it possible to integrate their accumulated knowledge. These activities assist in integrating all areas of health and may include several university courses. They are extremely beneficial in the context of professional training for ensuring interdisciplinarity.23 However, activities that focus only on providing medical assistance may be ineffective for comprehensive training as the students are not usually required to learn how to provide assistance in terms of the community’s social reality and the integration of health activities.23 When detached from the social perspective, these activities remain locked in a biological perspective. The individuals of a community are the only recipients of the university.5
Students reported that these activities provided a more mature outlook and offered the possibility of enhancing the knowledge garnered from their classes. They also provided a realistic view regarding the socioeconomic difficulties and other social differences existing within the community.
The literature establishes the relevance of these activities for the development of communication skills.10,13,24–27 The ability to communicate technical knowledge in a simple manner that can be understood by others requires practice. Practitioners may also need to learn the regional language at times to establish a productive relationship between themselves and their patients.28 De Almeida and Barbosa19 state that these activities also enhance the student’s ability to listen and understand.
However, to enable students to participate in CBEA, it is necessary to remove these barriers. An important barrier mentioned by the respondents is the lack of support from the different segments involved in these activities. This reinforces the proposal by Cohen and Sherif17 regarding the need to ensure that a joint effort is made by the teachers, institution directors, health managers, preceptors, and students. These activities can be conducted efficiently only if all the sectors involved are cooperative and engaged.
Another barrier mentioned exclusively by the first-year students was related to their perception of the inability to enter the programs. To address this, activities such as play therapy, clown therapy, and music therapy could allow students to participate. Additionally, tests for entering the extension programs were also mentioned as a demotivating factor. Amorim and Bedaque10 stated that students could be motivated to participate in activities that only require the demonstration of will and responsibility through a letter of interest.
Community-based CBEA contributes to the accumulation of knowledge, skills, and competencies that are essential for complete medical education. Based on an understanding of the barriers that hinder students’ participation, medical schools can work with academic centers to minimize these factors. Students can then be assimilated into a wholesome extracurricular experience.
This study achieved a good response rate with a balanced sample between the genders. A limitation of the study was the absence of students in the sixth year of medicine, which would allow an even more detailed analysis comparing the years of graduation.
Conclusion
This study analyzes the motivation of medical students to participate in CBEA to contribute to society, support their professional choices, and improve their learning.
CBEA enable medical students to expand their knowledge of medicine and help them to acquire skills, such as time management and communication abilities. Furthermore, students develop the necessary competencies required to work with an organization and to collaborate with others. Through these activities, academics can improve their attitude regarding leadership, commitment, and responsibility. These activities allow students to gain experience and develop emotional skills, such as empathy and resilience. Unfortunately, the literature lacks studies with the same structure of extracurricular activity or that analyze the CBEA in a qualitative perspective.
Acknowledgments
We wish to thank the students who participated in the study and gave their time and views willingly and gratefully. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) -Finance Code 001.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Evans DV, Krasin B, Brown K, Dobie S, Kost A. Student perceptions about benets from an extracurricular curriculum: a qualitative study of the underserved pathway. PRiMER. 2017;1:1–13. doi:10.22454/PRiMER.2017.153424
2. Fares J, Al Tabosh H, Saadeddin Z, El Mouhayyar C, Aridi H. Stress, burnout and coping strategies in preclinical medical students. N Am J Med Sci. 2016;8:75–81. doi:10.4103/1947-2714.177299
3. Almasry M, Kayali Z, Alsaad R, et al. Perceptions of preclinical medical students towards extracurricular activities. Int J Med Educ. 2017;8:285–289. doi:10.5116/ijme.5973.297a
4. Cruz MLS, Torres Peixotoet M, Lima da Silva CA, Galvão Damas W, Menezes de Oliveira AB. Perfil das atividades complementares dos graduandos em medicina pela Universidade Estadual de Feira de Santana, 2009–2017 [Profile of Complementary Activities of Last-Year Medical Students at the State University of Feira de Santana, 2009–2017]. Rev Bras Educ Med. 2019;43:265–275. doi:10.1590/1981-5271v43suplemento1-20190026
5. De Almeida LE, Pereira MN, Oliviera V. Governador Valadares (MG) em Extensão: interfaces para a dinamização e instrumentalização do cenário extensionista em um campus recém-Implantado [Governador Valadares (MG) in extension: interfaces for the promotion and exploitation of the extension scenario in a newly deployed campus]. Rev Bras Educ Med. 2016;40:743–750. doi:10.1590/1981-52712015v40n4e00622015
6. Bardin L. Content Analysis. Lisboa: Edições; 1995:70.
7. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19:349–357. doi:10.1093/intqhc/mzm042
8. Tavares AP, Ferreira RA, Barboza França E, et al. O “Currículo Paralelo” dos estudantes de medicina da Universidade Federal de Minas Gerais [The “parallel curriculum” of medical students of the Federal University of Minas Gerais (UFMG)]. Ver Bras Educ Med. 2007;31:254–265. doi:10.1590/S0100-55022007000300008
9. Yengo-Kahn AM, Baker CE, Lomis KD. Medical students’ perspectives on implementing a curriculum change at one institution. Acad Med. 2017;92:455–461. doi:10.1097/ACM.0000000000001569
10. Amorim KP, Bedaque HP. A percepção dos estudantes de medicina sobre a influência do Mediarte na educação médica [The medical student’s view on Mediarte’s influence on medical education]. Rev Bras Educ Med. 2018;42:54–62. doi:10.1590/1981-52712015v42n2rb20170027
11. Moreira LM, Petroni Mennin RH, de Castro Lacaz FA, Campos Bellini V. Ligas acadêmicas e formação médica: estudo exploratório numa tradicional Escola de medicina [Academic leagues and medical training: an exploratory study in a traditional school of medicine]. Rev Bras Educ Med. 2019;43:115–125. doi:10.1590/1981-52712015v43n1rb20170141
12. Da Silva Rios DR, Caputo MC. Beyond traditional health training: experience of popular education in medical training. Rev Bras Educ Med. 2019;43:184–195. doi:10.1590/1981-52712015v43n3RB20180199
13. Rosevics L, Assunção Aguiar D, Borges CR, et al. ProCura - a arte da vida: um projeto pela humanização na saúde [ProCura - the art of living: a project for the humanization of health care]. Rev Bras Educ Med. 2014;38:486–492. doi:10.1590/S0100-55022014000400010
14. Da Silveira JL, Rodrigues KF, Shishido M, Moraes P. Pesquisa e extensão em saúde e a aprendizagem nos níveis cognitivo e afetivo [Research and Extension in Health and Cognitive and Affective Learning Levels]. Rev Bras Educ Med. 2015;39:550–557. doi:10.1590/1981-52712015v39n4e02852014
15. Bloom BS. Taxonomy of educational objectives. Porto Alegre: Globo; 1972.
16. Lins L, de Oliveira MMV, Cattony ACE, et al. Extensão universitária e inclusão social de estudantes do ensino médio público [University extension and the social inclusion of public high school students]. Trab Educ Saúde. 2014;12:679–694. doi:10.1590/1981-7746-sip00003
17. Cohen LG, Sherif YA. Twelve tips on teaching and learning humanism in medical education. Med Teach. 2014;36:680–684. doi:10.3109/0142159X.2014.916779
18. Amorim KPC, Rocha AKC, Dos Santos Silva IC, De Melo LMB, De Araújo MAA. Mediarte com amor e humor: uma experiência a partir do olhar dos participantes [Mediarte with Love and Humor: an experience from the participants’ point of View]. Rev Bras Educ Med. 2015;39:294–301. doi:10.1590/1981-52712015v39n2e01132014
19. De Almeida SMV, Barbosa LMV. Curricularização da extensão universitária no ensino médico: o encontro das gerações para humanização da formação [Curricularisation of university community outreach in medical education: meeting of generations for a humanized training]. Rev Bras Educ Med. 2019;43:672–680. doi:10.1590/1981-5271v43suplemento1-20190013
20. Freire P. Pedagogia Do Oprimido [Pedagogy of the Oppressed]. Rio de Janeiro: Paz e Terra; 1987.
21. Mourthé CA, Lima VV, Padilha RQ. Integrando emoções e racionalidades para o desenvolvimento de competência nas metodologias ativas de aprendizagem [Integrating emotions and rationalities for the development of competence in active learning methodologies]. Interface. 2018;22:577–588. doi:10.1590/1807-57622016.0846
22. Da Cunha ATR, Silva JI, da Silva Oliveira G, Souto RD, de França Souza LF, da Cruz Solano L. População em situação de rua: o papel da educação médica ante a redução de iniquidades [The homeless population: the role of medical education to reducing health disparities]. Rev Bras Educ Med. 2020;44:e136. doi:10.1590/1981-5271v44.supl.1-20200376
23. Dos Santos RN, Silva Ribeiro KSQ, Dos Anjos UU, de Farias DN, de Freitas Lucena EM. Integralidade e interdisciplinaridade na formação de estudantes de medicina [Comprehensive and interdisciplinary medical training]. Rev Bras Educ Med. 2015;39:378–387. doi:10.1590/1981-52712015v39n3e02412014
24. Bulcão LG. O ensino médico e os novos cenários de ensino-aprendizagem [Medical education and new scenarios for teaching/learning]. Rev Bras Educ Med. 2004;28:61–72. doi:10.1590/1981-5271v28.1-009
25. Melo RV, Felipe MCP, da Cunha ATR, et al. Roda de conversa: uma articulação solidária entre ensino, serviço e comunidade [Round table: a partnership between education, service and community]. Rev Bras Educ Med. 2016;40:301–309. doi:10.1590/1981-52712015v40n2e01692014
26. Luna WF, de Almeida Nordi AB, Rached KS, de Carvalho ARV. Projeto de extensão iandé guatá: vivências de estudantes de medicina com indígenas potiguara [The Iandé Guatá Extension Project: the experiences of medical students with the Potiguara indigenous community]. Interface. 2019;23:e180576. doi:10.1590/interface.180576
27. Chung MC, Marangon MB, Luna WF, Bettini RV, Watanabe RK, Shiroma MM. Desafios do Brincar com Idosos: narrativas de estudantes de medicina do Programa Amigos do Sorriso [Challenges of playing with the elderly: medicine student’s narratives of the Amigos do Sorriso program]. Rev Bras Educ Med. 2020;44:e170. doi:10.1590/1981-5271v44.4-20200217
28. Martins AC, Schlosser AR, de Arruda RA, et al. Ensino médico e extensão em áreas Ribeirinhas da Amazônia [Medical teaching and community outreach in Amazonian Riverside areas]. Rev Bras Educ Med. 2013;37:566–572. doi:10.1590/S0100-55022013000400012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.