Back to Journals » Advances in Medical Education and Practice » Volume 14
Medical Student Enrollment in a Voluntary Medical Innovation Course
Received 28 December 2022
Accepted for publication 23 March 2023
Published 17 July 2023 Volume 2023:14 Pages 773—782
DOI https://doi.org/10.2147/AMEP.S402934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
David A Zarrin,1 Li Zhou2
1David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, USA; 2Department of Medicine, University of California, Los Angeles, CA, 90095, USA
Correspondence: David A Zarrin, David Geffen School of Medicine, University of California, Los Angeles, 10833 Le Conte Avenue, Los Angeles, CA, 90095, USA, Tel +1408-438-8127, Email [email protected]
Background: There is an increasing need for medical innovators to help address the growing challenges within health care. Despite this, the rate of adoption of new medical innovation programs at the United States (US) medical schools has been slow. Existing literature explaining this slow rate of adoption is scant. We examined the rate of student enrollment in a voluntary medical innovation course during an unscheduled summer at our institution and the educational backgrounds of these enrollees.
Methods: This mixed qualitative and quantitative survey study comprised consecutive surveys quantifying a two-stage sign-up process for a voluntary summer medical innovation course for Medical Doctorate (MD) candidates at the David Geffen School of Medicine. After a “General interest” survey, interested students completed an “Enrollment” survey to indicate enrollment, educational background, and open-ended comment about motivations for enrollment. Surveys were administered electronically via email listservs. Statistical methods included chi squared testing with statistical significance defined as p < 0.05.
Findings: A total of 12% of UCLA Class of 2024 expressed an interest in participation in the program, and 10.3% ultimately enrolled. Enrollees were motivated primarily by the opportunity to learn about medical innovation (72%) and also shadow (28%). Enrollees were similar in undergraduate degrees and majors to the general medical student class and US MD candidate population.
Conclusion: A lack of medical student willingness to participate may not underlie the observed slow rate of adoption of medical innovation programs at US MD programs given the observed high voluntary enrollment rate. Enrollee educational background did not differ significantly from non-enrollees or the broader US MD candidate population. Educators should be encouraged by these data to explore student willingness to participate in medical innovation education at their institutions.
Keywords: medical innovation education, medical students, educational background
Introduction
In recent decades, there has been a trend towards establishing a culture of medical innovation within medical schools across the United States (US).1 Such efforts aim to equip future physicians better to identify and solve many and formidable ongoing and future challenges that face the US healthcare system, such as rising costs of health care, inequity in healthcare access, physician and nursing shortages, and medical errors, among others.2,3 While trends have been positive in the creation of these programs, according to a recent systematic review of US and Canadian medical school websites and curricula, only 26 of the over 170 medical schools across the United States offer their Medical Doctorate (MD) students the opportunity to participate in innovation and entrepreneurship programs alongside the traditional MD education.4 Despite the importance of physician innovators,5 the rate of adoption of such programs within medical schools has been slow, with the first of these programs being founded in 2007 and an average of only two new innovation programs founded each year across the country.
The reasons underlying slow adoption of medical innovation content into US MD curricula are not well described given the paucity of literature in the field.4 We hypothesize that a number of factors may contribute to the slow rate of adoption, including lack of student willingness to participate, lack of faculty interest, and lack of positive outcomes of such innovation programs for US MD students. Furthermore, the lack of literature on this topic may itself be a reason for the slow adoption of medical innovation curricula in medical schools. Recent research suggests that learning about medical innovation remains elusive task not just for medical students but more broadly for medical trainees.6 The medical education research community has begun to formalize different methods for integrating innovation curricula into the traditional medical education in order to fill this gap. Options such as innovation tracks, workshop series, and targeted skills sessions have been proposed.6 Typical medical innovation courses aim to develop skills which are considered critical for open-ended problem solving inherent to the innovation process, such as clinical ethnography, needs identification, solution landscaping, brainstorming, business and entrepreneurship of medical devices and technology, among others.7,8 Beyond the teachings of core innovation content, leadership competencies have been highlighted as a critical component of the recipe for training physicians capable of tackling even the most complex and seemingly amorphous challenges plaguing modern health care, coined “wicked” problems, by Keijser et al in their recent work.9
Across the country, various local institutional and nationwide organizations have spawned to accelerate innovative solutions to these complex changes. One such example is Sling Health, a national organization with numerous institutional chapters that is focused on training students in medical innovation.10 Sling Health was born out of IDEA Labs, a medical technology incubator founded at Washington University in St. Louis. Our local branch of Sling Health at the David Geffen School of Medicine (DGSOM) at the University of California, Los Angeles (UCLA) sought to shed further insight upon one possible explanation for the slow rate of adoption of medical innovation curricula in US MD programs, namely the level of US MD student willingness to participate in medical innovation education. In this study, which was conducted in January and February of 2021, we aimed to examine the extent of student enrollment in a voluntary medical innovation course during the unscheduled summer of 2021 at the David Geffen School of Medicine at UCLA and the educational backgrounds of these enrollees. This medical innovation course was scheduled during the two-month-long summer vacation after first year in DGSOM’s four-year curriculum and comprised a didactics component focused on learning to identify, evaluate, and solve unmet clinical needs, formulate clinical needs statements, create and select different solution concepts, and understand regulatory and business considerations when developing a solution. A clinically immersive component complimented didactic learning as means of applying didactic concepts in a hands-on manner under close mentorship of clinicians. Such a course would be feasible to host in a large academic medical institution such as that of UCLA, where there are ample clinicians to assume mentorship roles.
Methods
This research was conducted with the approval from our institutional review board (IRB# 21–001608). The study design is a mixed qualitative and quantitative survey study conducted through January and February of 2021. An initial “General Interest” survey was distributed to all 175 members of the DGSOM Class of 2024 (2019–2020 application cycle) to gauge the level of interest in participating in a clinically immersive medical innovation program between the first and second year of MD courses. Participation in the program was strictly voluntary, and no credit towards graduation was offered to enrolled students.
The survey was administered via a class-wide email listserv in January 2021 of the students first year of medical school and contained a short program description followed by two questions. This “General Interest” survey consisted of a program description and learning objectives, namely to identify, evaluate, and solve unmet clinical needs, list of opportunities for program participants, and two questions gauging interest in enrolling and medical field preference for clinical immersion assuming participation (Figure 1).
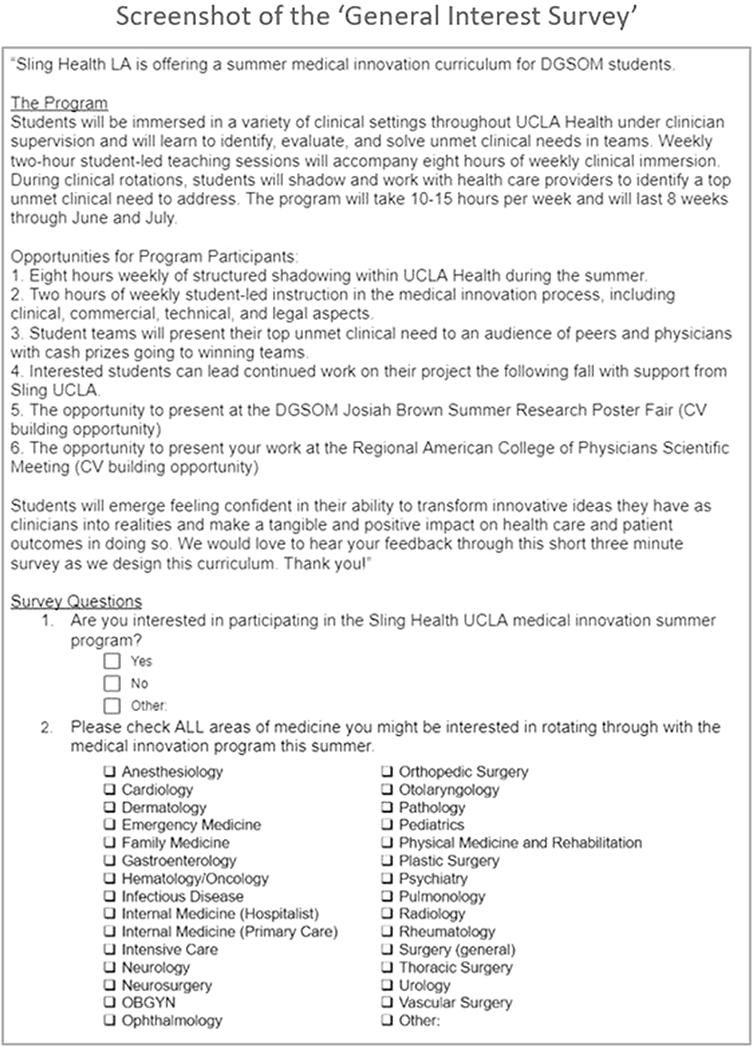 |
Figure 1 Screenshot of the “General Interest Survey” which was distributed electronically via email listserv to the members of David Geffen School of Medicine (DGSOM) Class of 2024 at the beginning of the study. |
After distributing the “General Interest” survey, the same group of students were subsequently provided a course registration survey to determine who would commit to the described medical innovation program, the reasons for enrollment, and information regarding the educational background of each student. The following questions and instructions were included in the survey:
- Please select “yes” to sign up for our program!
- What was your undergraduate major?
- What graduate degree did you receive? If none, select “n/a”.
- What field is your graduate degree in? If none, put “n/a”.
- What drew you to this program?
The responses to question five were analyzed, and similar responses were grouped. Analysis of motivations for signing up was particularly important in this study, given this medical innovation course was one of the first in-person opportunities available to students following restrictions due to the COVID-19 pandemic, which served as a potential confounder to participation rate. All survey responses within 30 days of the date of survey distribution were included. Duplicate responses due to technical errors were eliminated. All data were collected in an anonymized form.
In order to compare educational backgrounds of students who registered for this program with those from the general medical school class, de-identified, class-wide educational background information was then obtained from the DGSOM Admissions Committee. These data consisted of undergraduate majors, undergraduate degrees, undergraduate minors, graduate fields of study, and graduate degrees for all students within DGSOM Class of 2024. To compare the educational backgrounds of those who registered for the innovation course with nationwide medical school matriculants, the educational backgrounds of the 2021–2022 application cycle were extracted from the American Association of Medical Colleges (AAMC) website, because this was the year with publicly available data which were most temporally aligned with DGSOM Class of 2024 (2019–2020 application cycle). All data in this study were analyzed on a device compliant with university encryption standards using Microsoft Excel (Office 16) and MATLAB (R2020b). Tests of significance included chi squared testing with significance defined as p < 0.05 were used to quantitatively compare educational backgrounds of local and national students.
Findings
General Interest Survey Results
Of 175 students, 25 responses (14.3% response rate) were recorded for the initial “General Interest Survey” within the 30-day response window. In response to question #1 (Figure 2), “Are you interested in participating in the Sling Health LA medical innovation program?”: 21 students (12% of all respondents) responded “Yes”, zero students responded “No”, and four students (2% of all respondents) responded “Other” and submitted an explanation indicating an undecided state. In response to question #2 (Figure 3), “Please check ALL areas of medicine you might be interested in rotating through with the medical innovation program this summer”, cardiology (16/18, 89% of respondents), vascular surgery (14/18, 78% of respondents), and general surgery (13/18, 72% of respondents) were the three most voted specialties for rotation.
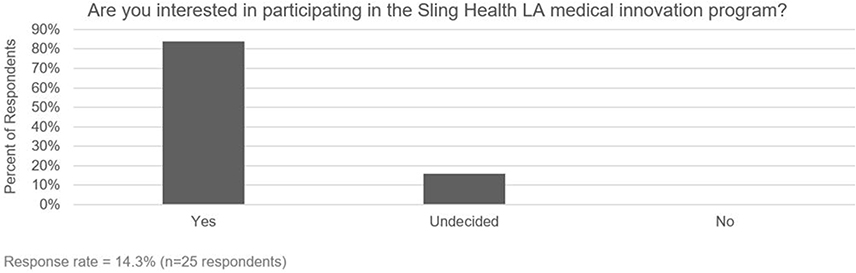 |
Figure 2 Student responses to question #1 of the “General Interest Survey”: “Are you interested in participating in the Sling Health Los Angeles (LA) medical innovation program?”. |
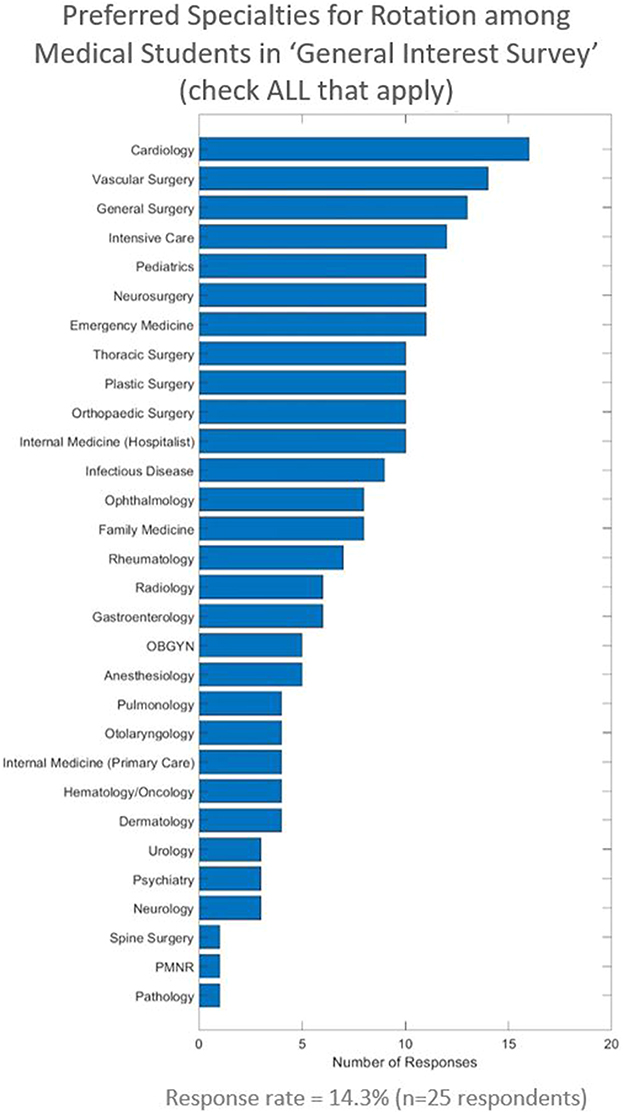 |
Figure 3 Student responses to question #2 of the “General Interest Survey”: “Please check ALL areas of medicine you might be interested in rotating through with the medical innovation program this summer”. |
Course Registration Survey Results
In response to question one of the subsequent Course Registration Survey, “Please select ‘Yes’ to sign up for our program!”, 18 students (10.3% of DGSOM Class of 2024) formally signed up for the medical innovation program by selecting “Yes”.
Undergraduate and Graduate Fields of Study
Questions two (Figure 4a) revealed the composition of the first year DGSOM was not statistically different from the nationwide average of medical school matriculants in the 2021–22 application cycle,11 with the exception of those who majored in majors classified as “other” (15% Nationwide, 6% DGSOM, p = 0.04).
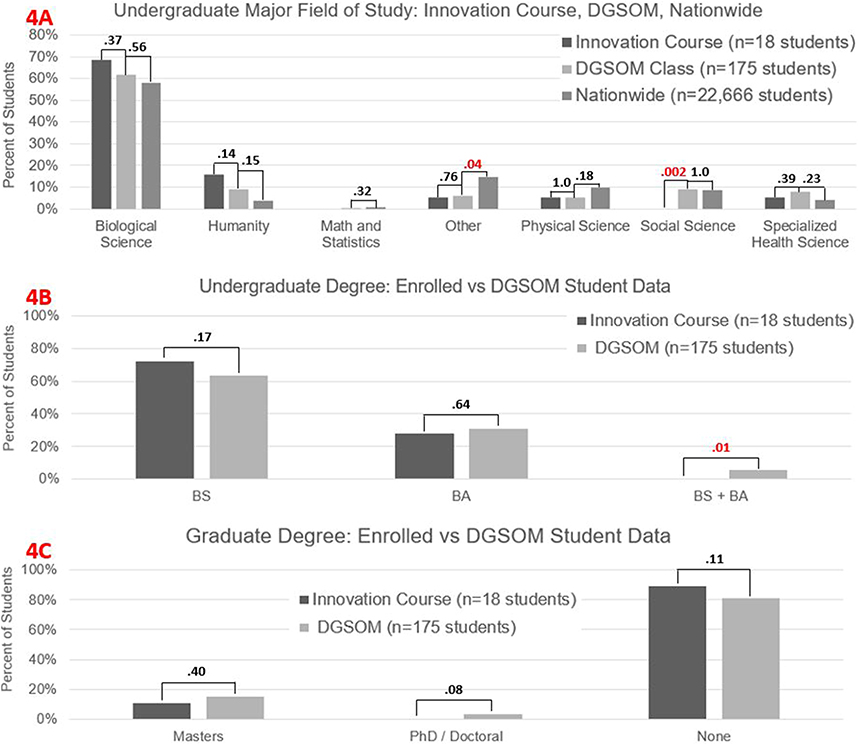 |
Figure 4 Educational backgrounds including (A) Fields of undergraduate majors, (B) Undergraduate degrees, and (C) Graduate degrees of the David Geffen School of Medicine (DGSOM) class, the innovation in course enrollees, and United States (US) Medical Doctorate (MD) matriculants nationwide. Levels of significance as measured by p-values are indicated between groups above each crossbar. Each p-value assesses for a statistically significant difference in fraction of students corresponding to the respective categories. Significant p-values (<0.05) are indicated in red font. |
The large majority of innovation course enrollees majored in a physical or biological science (14/18, 78%) at their undergraduate institution compared with 74% (130/175) across all students in DGSOM Class of 2024. With the exception of social sciences in which no innovation course enrollees obtained their major field of study (0% Innovation Course, 9% DGSOM, P = 0.002), there were no statistically significant differences in the composition of undergraduate majors between those in the innovation course and the general DGSOM first year class.
With regard to undergraduate degrees (Figure 4b), 72% (13/18) of innovation course enrollees compared with 63% of the general first year class earned a Bachelor of Science (BS) from their undergraduate institution. Twenty-eight percent of enrollees (5/18) compared with 31% of the DGSOM first year class earned a Bachelor of Arts (BA) from their undergraduate institution. There were no statistically significant differences between these two groups. However, amongst innovation course enrollees, there were no enrollees who obtained both BS and BA degrees, which was statistically significant compared with 6% of DGSOM first year medical student class who obtained both a BS and a BA (P = 0.01).
With regard to graduate degrees (Figure 4c), 11% (2/18) of innovation course enrollees (vs 15% (27/175) class-wide) had a Master’s Degree, 0% (vs 3% class-wide (6/175)) had a PhD/doctoral degree, and 89% (vs 81% class-wide (142/175)) had no graduate degree. There were no statistically significant differences between these groups.
Motivations for Course Registration
With regard to the survey question about motivations for signing up for the course, 89% of enrollees responded (Figure 5). Student’s qualitative responses were analyzed, and similar responses were grouped: opportunity to learn about medical innovation (9/16, 56%), opportunity to learn about medical innovation and shadow (4/16, 25%), the opportunity to present their findings in a research presentation (2/16, 13%), and the opportunity to shadow clinicians (1/16, 6%). Specific examples of provided responses for motivations to participate include “I am interested in innovation and thinking of practical solutions for real-world problems. I have always envisioned this to be a part of my future career as a physician and I think this program is a good way to start”, and “There aren’t too many opportunities to engage in learning about medical innovation in medical school. I thought that structured and formalized instruction on medical innovation would be super useful in the future as it has a place in any clinical environment”.
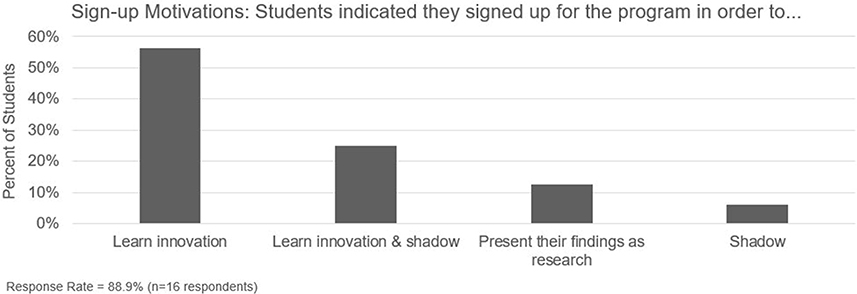 |
Figure 5 Responses to question #5 from the Course Registration Survey: “What drew you to this program?” grouped by similarity in response. |
Discussion
This study conducted by Sling Health10 LA is the first to characterize the rate of enrollment among US MD candidates in a voluntary medical innovation curriculum, to assess learner motivations for program enrollment, and to examine the educational backgrounds of enrollees at a US-based medical school. The described medical innovation curriculum was modeled after existing and well-established medical innovation programs which are offered primarily to engineering students.7,8 Overall, this study revealed an unexpectedly high degree of voluntary participation in the voluntary medical innovation course which was attributable to the desire to specifically learn medical innovation, and further analysis revealed that enrollees shared a similar educational background to the entire DGSOM class and the average US MD matriculant.
Degree of Voluntary Student Participation in Medical Innovation Course
Overall, 25 students (14.3%) of first-year medical students expressed an interest in participating in the summer medical innovation program, and 18 students (10.3% of students) ultimately enrolled. An enrollment rate exceeding 10% of the class was unexpectedly high given the innovation course provided no graduation credit to students and participation was strictly voluntary. There are more than 10 sub-fields within medicine which medical students can focus their extracurricular learning in modern medical education. Some examples include basic science research, clinical research, translational research, global health, social sciences and medical humanities, health justice and policy, medical education, medical leadership, quality improvement, among others. Medical innovation is just one such sub-field, yet the described course drew a greater than 10% voluntary participation rate, suggesting a high degree of underlying interest in this sub-field.
Motivations for Enrollment
The students’ motivations for signing up for this course help to explain the reasons for the relatively high enrollment rate. According to student survey responses, the most common reason for enrolling in this curriculum was the opportunity to learn about medical innovation in a setting that previously did not have such curricular opportunities (Figure 5). Indeed, students qualitative responses indicated that they had few prior opportunities to learn about or participate in medical innovation and were therefore motivated to participate in the described course as it was perceived to be a rare opportunity to learn something new. Indeed, medical trainees interested in medical innovation have been shown to lack the resources to pursue education within this realm.6 These sentiments align with those reported by our respondents, and further support the argument for integrating medical innovation courses more closely with traditional medical education.
A potential confounding factor to student motivations for participation relates to the COVID-19 restrictions, which spanned most of the academic year preceding the summer of 2021, both at UCLA and other medical schools. During this time, students had little opportunity to attend in-person clinical experiences.12 Given that this program was one of the first opportunities to return to an in-person clinical environment at UCLA, it was important to distinguish between students who signed up to learn about medical innovation rather than solely have an opportunity to shadow clinically. In total, only one student indicated a sole interest in shadowing, while four expressed interest in both the opportunity to learn about medical innovation and shadow. This suggests that most students were interested in participating in this curriculum primarily out of interest for learning about medical innovation instead of solely out of desire for an in-person clinical experience. Nonetheless, the opportunity to shadow clinically may have been an incentive regardless of the timing relative to pandemic restrictions.
Although the authors of the survey had anticipated that opportunities for CV building would be a strong motivator for enrollment, very few students were motivated (2/18) by the opportunity to present their research findings.
There are likely to be reasons for student enrollment in the program that were not captured in this survey. Given enrollment in this program required only 10 hours of commitment per week, the flexibility of this curriculum’s schedule may have been appealing to students who were enrolled in other formal summer research programs.
It should be noted that although we know at least 10% of the UCLA class had an interest in medical innovation based on the enrollment rate, this study does not directly assess level of interest across all students, because those who did not enroll may have not enrolled for reasons other than lack of interest (other commitments, not in town, etc). “Students in this study were being asked to formally commit to a summer course”, rather than simply complete a traditional survey with no further engagement. This explains the apparently low response rate of 18/175 (10.3%), which may be better termed an “enrollment” rate. Indeed, this study was not meant to assess reasons for not enrolling among those who did not enroll, but rather to measure the rate of voluntary enrollment in a medical innovation course. Given that 10.3% of students voluntarily committed approximately 70 hours of their summer vacation to learn medical innovation, while receiving no credits towards graduation, this suggests that there is considerable interest in this particular sub-field of medicine, namely medical innovation. These findings are in alignment with prior work, which has focused on gauging general level of interest in innovation curricula, as opposed to gauging extent of voluntary enrollment. For example, Scott et al reported high rates of interest (ranging between 67% and 88%) across undergraduates, medical students, and post-baccalaureates in having innovation incorporated into medical school curricula.13
Educational Backgrounds of Enrollees
In evaluating the characteristics of students who enrolled in this class, we found the educational background did not differ significantly from the general class with the exception of an underrepresentation of social sciences (Figure 3). This suggests that medical students from a variety of educational backgrounds may be interested in learning about medical innovation. There are many possibilities for why those who studied social science were underrepresented amongst the innovation course enrollees, including competing opportunities during the summer or lack of interest. However, larger studies are needed to validate this discrepancy and further understand its possible causes.
Groups did not significantly differ in the types of undergraduate degrees earned with the exception of dual BS/BA, which represented only a small portion of the first year medical student class. Similarly, innovation course enrollees did not differ significantly in the type of advanced degrees earned.
The undergraduate majors of first year students at DGSOM were very similar to those from the nationwide survey of medical school matriculants by the AAMC, with the exception of an undergraduate major categorized as “other”. This suggests that the DGSOM medical school class may be relatively representative of nationwide medical school matriculants with regard to educational backgrounds.
Clinical Interests of Enrollees
Similarly, we found that students who were interested in this program were interested in a broad range of specialties (Figure 2). The top seven specialties in which the students were interested for the innovation curriculum include two medicine specialties (intensive care and cardiology), 3 surgical specialties (general surgery and vascular surgery, neurosurgery), emergency medicine, and pediatrics. It is therefore apparent that students who registered for the medical innovation curriculum had a variety of clinical interests.
Limitations
The limitations of this study include those inherent to single-institution and observational studies. Multicenter studies are needed to generalize the results of this study. Although our data suggest that the educational backgrounds of our school are very similar to that of the nationwide first year medical school matriculants, other demographic factors such as race, gender, and socioeconomic backgrounds were not assessed. There is the potential that social desirability bias influenced qualitative responses of enrollees with regard to their motivations for participating; however, this was likely lessened by the assurance that all responses were anonymized. Additionally, the class-wide analysis included innovation course enrollees because these data could not be separated given all collected data were anonymized. Finally, this study was designed to investigate the population of students who voluntarily enrolled in the innovation course but did not analyze reasoning among students who did not enroll. Thus, findings are limited to enrollees, who comprised 10.3% of the original student body.
Conclusion
While a need for physician innovators exists, the rate of adoption of medical innovation curricula in US medical schools remains slow. In this study, we examined the extent of student enrollment in a voluntary medical innovation course, their motivations for participation, and their educational backgrounds to better understand the reason for this slow adoption.
We concluded that at our institution, US MD students demonstrated a high willingness to participate (10.3% of students) in a voluntary, clinically immersive medical innovation education curriculum. Furthermore, we find that most students were truly interested in learning about medical innovation and not strictly using the course as an opportunity to shadow. These findings suggest that a lack of student willingness to participate may not underlie the observed slow rate of adoption of medical innovation programs at US MD programs.
Furthermore, examination of educational backgrounds of student enrollees suggests that the average student at DGSOM who is interested in learning about medical innovation is diverse and not limited to a subgroup of medical students of a certain educational background or with a subset of clinical interests.
Finally, our study may provide insights into the broader trend of interests in medical innovation across the country given the similarity of educational background between our student body and the nationwide MD matriculants. These results should encourage educators to reach out to their own student bodies to assess the level of interest in creating such a curriculum.
Data Sharing Statement
The manuscript as it is currently written contains all associated data. If there is any additional information regarding the data a reader would like to see, the authors will be happy to provide access.
Ethics Approval and Informed Consent
This research was conducted with the approval from the UCLA institutional review board (IRB# 21-001608).
Acknowledgments
We would like to the UCLA Deans Office for providing data regarding the educational background of DGSOM Class of 2024.
Funding
Neither this study nor any authors received financial support for the research presented in this manuscript.
Disclosure
The authors have no financial competing interests or disclosures relevant to the research presented herein.
References
1. Suryavanshi T, Lambert S, Lal S, Chin A, Chan TM. Entrepreneurship and innovation in health sciences education: a scoping review. Med Sci Educ. 2020;30(4):1797–1809. doi:10.1007/S40670-020-01050-8
2. Dieleman JL, Cao J, Chapin A, et al. US health care spending by payer and health condition, 1996–2016. JAMA. 2020;323(9):863–884. doi:10.1001/JAMA.2020.0734
3. Buntin MB. Confronting challenges in the US health care system: potential opportunity in a time of crisis. JAMA. 2021;325(14):1399–1400. doi:10.1001/JAMA.2021.1471
4. Arias J, Scott KW, Zaldivar JR, et al. Innovation-oriented medical school curricula: review of the literature. Cureus. 2021;13(10). doi:10.7759/CUREUS.18498
5. Majmudar MD, Harrington RA, Brown NJ, Graham G, McConnell MV. Clinician innovator: a novel career path in academic medicine a presidentially commissioned article from the American heart association. J Am Heart Assoc. 2015;4(10). doi:10.1161/JAHA.115.001990
6. Boms O, Shi Z, Mallipeddi N, et al. Integrating innovation as a core objective in medical training. Nat Biotechnol. 2022;40(3):434–437. doi:10.1038/s41587-022-01253-x
7. Yock PG, Brinton TJ, Zenios SA. Teaching biomedical technology innovation as a discipline. Sci Transl Med. 2011;3(92):92cm18. doi:10.1126/scitranslmed.3002222
8. Yazdi Y, Acharya S. A new model for graduate education and innovation in medical technology. Ann Biomed Eng. 2013;41(9):1822–1833. doi:10.1007/s10439-013-0869-4
9. Keijser W, Huq JL, Reay T. Enacting medical leadership to address wicked problems. BMJ Lead. 2020;4(1):12–17. doi:10.1136/leader-2019-000137
10. Linderman SW, Appukutty AJ, M V R, Shah AP, Javaherian K. Advancing healthcare technology education and innovation in academia. Nat Biotechnol. 2020;38(10):1213–1217. doi:10.1038/s41587-020-0689-7
11. 2021 FACTS: Applicants and Matriculants Data | AAMC. MCAT and GPAs for applicants and matriculants to U.S. medical schools by primary undergraduate major, 2021–2022; 2022. Available from: https://www.aamc.org/data-reports/students-residents/interactive-data/2021-facts-applicants-and-matriculants-data.
12. Arja SB, Wilson L, Fatteh S, Kottathveetil P, Fateh A, Arja SB. Medical education during COVID-19: response at one medical school. J Adv Med Educ Prof. 2021;9(3):176. doi:10.30476/JAMP.2020.88744.1351
13. Scott KW, Trumbull D, Zaldivar J, et al. Bridging the gap between innovation and medical curricula. MedEdPublish. 2021;10(1). doi:10.15694/mep.2021.000013.1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.