Back to Journals » Advances in Medical Education and Practice » Volume 11
Medical Student Attitudes Toward Substance Use Disorders Before and After a Skills-Based Screening, Brief Intervention, and Referral to Treatment (SBIRT) Curriculum
Authors Kidd JD ![]() , Smith JL, Hu MC
, Smith JL, Hu MC ![]() , Turrigiano EM, Bisaga A, Nunes EV
, Turrigiano EM, Bisaga A, Nunes EV ![]() , Levin FR
, Levin FR
Received 26 February 2020
Accepted for publication 13 May 2020
Published 30 June 2020 Volume 2020:11 Pages 455—461
DOI https://doi.org/10.2147/AMEP.S251391
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Jeremy D Kidd, 1, 2 Jennifer L Smith, 1 Mei-Chen Hu, 1 Eva M Turrigiano, 2 Adam Bisaga, 1, 2 Edward V Nunes, 1, 2 Frances R Levin 1, 2
1Department of Psychiatry, Columbia University, New York, NY, USA; 2Division on Substance Use Disorders, New York State Psychiatric Institute, New York, NY, USA
Correspondence: Jeremy D Kidd Email [email protected]
Purpose: Screening, Brief Intervention, and Referral to Treatment (SBIRT) is an evidence-based framework for assessing and addressing risky substance use. This study evaluated the substance-related attitudes of medical students who participated in an Enhanced Pre-Clinical SBIRT Curriculum designed to reduce stigma, help students empathize with the experiences of people using alcohol and drugs, understand substance use in-context, and feel more optimistic about efforts to prevent and treat substance use disorders (SUDs).
Methods: Students (N=118; 73.8% of eligible) completed the Attitudes and Opinions Survey for alcohol and drugs before and after this 2-year, multi-modality curriculum. The authors classified attitudes as “positive” or “negative” and grouped students by pre-post attitudinal change: persistently negative, persistently positive, negative-to-positive, positive-to-negative. Using chi-square tests, the authors assessed differences by sex, race/ethnicity, and whether students had a family member or friend with an SUD.
Results: Most students (> 90%) reported persistently positive attitudes regarding physicians in recovery, societal contributions of patients with SUDs; ability to learn from such patients; and general attitudes toward SUD treatment. This skewed distribution precluded the investigation of subgroup differences. Fewer students reported persistently positive attitudes regarding SUD patients’ healthcare utilization (alcohol 58.5%; drug 57.8%) and impact on other patients’ care (alcohol 73.7%; drug 72.4%), compared to other attitudinal domains (at p-values < 0.0001 in the McNemar’s tests). Approximately, 1 in 5 students reported more negative healthcare utilization attitudes on follow-up. There were no demographic differences in these two attitudinal domains.
Conclusion: Unlike previous studies of medical student attitudes, most students who participated in the Enhanced Pre-Clinical SBIRT Curriculum reported an enduring appreciation for the educational and societal contributions of patients with SUDs. Attitudes toward healthcare utilization and the impact of patients with SUDs on the care of other patients were more resistant to change, possibly due to the predominance of acute-care inpatient settings in clinical training.
Keywords: addiction, alcohol, drugs, screening, brief intervention, medical education
A Letter to the Editor has been published for this article.
Introduction
According to estimates by the World Health Organization’s Global Burden of Disease Project, substance use is linked to five of the six fastest increasing causes of mortality worldwide.1 In the US, alcohol use disorder (AUD) prevalence increased from 8.5% to 12.7% between 2002 and 2013,2 while the number of opioid overdose deaths continues to rise.3 However, only 10% of individuals with a substance use disorder (SUD) receive evidence-based treatment, a gap driven in-part by provider and patient-level stigma toward SUD treatment.4
Despite increased attention by government and media, medical school curricula often do not reflect the profound impact of SUDs on patients’ lives.5,6 When SUD topics are taught, they are often restricted to pre-clinical psychiatry curricula,5,6 overlooking the relevance of addiction to all specialties. Additionally, numerous studies demonstrate that attitudes of medical trainees toward patients with SUDs trend more negative with increased clinical training,7 possibly reflecting the “hidden curriculum” by which trainees internalize their supervisors’ negative attitudes. Among medical students, positive attitudes toward patients with SUDs are associated with greater recognition of the role of SUD treatment in clinical care and greater self-efficacy in delivering SUD treatment.8
Most SUD attitudinal interventions focus on post-graduate trainees, with far fewer addressing medical students.9,10 In this study, we evaluated the impact of a preclinical curriculum on medical students’ SUD attitudes. This curriculum utilized Screening, Brief Intervention, and Referral to Treatment (SBIRT); an evidence-based framework that combined standardized screening with motivational interviewing principles11 to assess and intervene on risky substance use.12,13 SBIRT is intended for rapid delivery in primary care settings and is associated with reduced tobacco and alcohol use.14,15 Evidence for drug use is less robust,16 but SBIRT has efficacy in some specific clinical settings.17 This curriculum expands on existing SBIRT education by integrating repeated exposure to brief intervention principles across several disciplines. We hypothesized that the majority of medical students who participated would maintain or develop positive attitudes toward patients with SUDs.
Materials and Methods
SBIRT-Focused Curricular Enhancements
Figure 1 illustrates components of the Enhanced Pre-Clinical SBIRT Curriculum. Participation was mandatory for all students. This curriculum involved three existing courses in the second and third semesters of medical school: (1) Foundations of Clinical Medicine (FCM); (2) Psychiatric Medicine (PM); and (3) Body, Health, and Disease (BHD). The curriculum included didactic instruction about SUDs (eg, diagnosis and neurobiology), student field visits to 12-step mutual-support groups, and general instruction about motivational interviewing. Additionally, we incorporated an SBIRT standardized patient small group and an objective structured clinical examination (OSCE), described in more detail below. Through repeated exposure to motivational interviewing and SBIRT, this curriculum was intended to reduce stigma by helping students empathize with the experiences of people who use alcohol and drugs, understand substance use in-context, and develop appropriate optimism about preventing and treating SUDs.
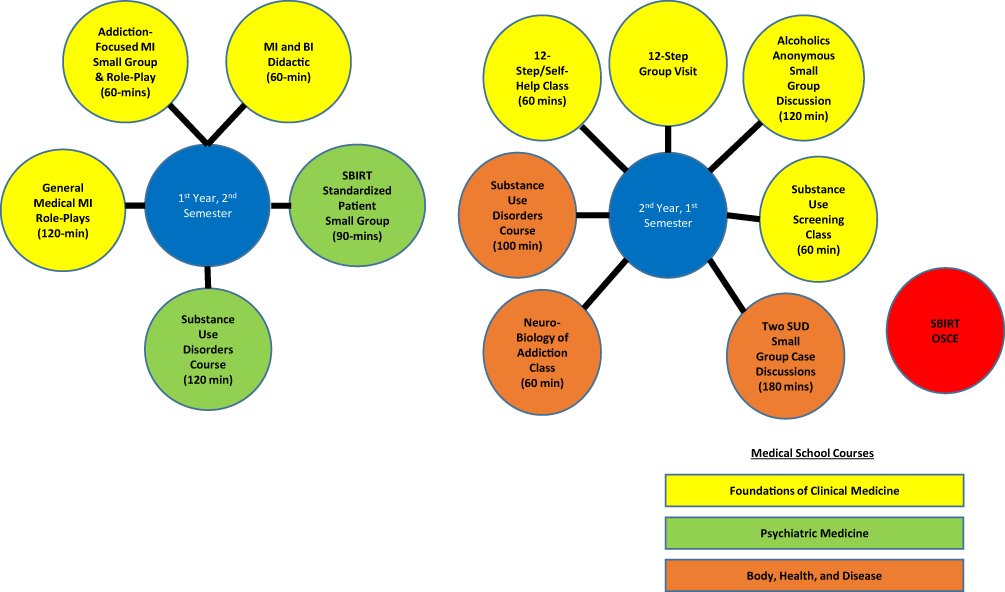 |
Figure 1 Components of the Enhanced Pre-Clinical SBIRT Curriculum. Abbreviations: MI, motivational interviewing; BI, brief intervention; OSCE, Observed Standardized Clinical Exam; SBIRT, Screening, Brief Intervention, and Referral to Treatment; SUD, substance use disorder. |
SBIRT Standardized Patient Small Group
An addiction psychiatry fellow facilitated this 90-mins small-group workshop as part of a weekly small-group series during the first-year, second-semester PM course. Instructional materials were compiled from current research and federal agencies and made available online. Utilizing a flipped classroom design, students reviewed course material prior to the small group, enabling facilitators to focus on experiential learning. During the first half, instructors engaged students in primary care case-based discussions of SBIRT principles. Students referred to “white-coat pocket cards” with NIAAA standard drink measurements, common screening instruments (eg, CAGE, ASSIST), motivational interviewing tools (eg, change ruler) and techniques, and sample questions for each brief-intervention stage. Next, students viewed a video demonstration of primary care brief intervention and identified SBIRT-adherent behaviors. Students were also encouraged to discuss reactions to the patient’s description of substance use and its impact on their life.
In the second half of the workshop, students role-played screening and brief intervention with a standardized patient. Two students volunteered to play outpatient primary care physicians seeing a young adult patient for follow-up management of a shoulder injury and low mood in the setting of heavy drinking. Students were to obtain a focused history of the patient’s chief complaint, use the CAGE questionnaire18 to screen for risky drinking, and deliver a brief intervention if appropriate based on screening. The two students acted together as one physician, with one student beginning the interview and then alternating between sections. Students could “pause” the interview to elicit help from classmates, and instructors could interject to help students overcome difficulties. The standardized patient actor also provided students with feedback from the patient’s perspective to help them maintain a non-judgmental stance and emphasize patient autonomy.
SBIRT Objective Structured Clinical Examination (OSCE)
In the third semester (ie, end of pre-clinical training), each student participated in an SBIRT OSCE. OSCEs are designed to mimic “real-life” patient encounters, occurring in simulated examination rooms with standardized patients trained to evaluate students’ performance. First, students received group orientation to the OSCE format and objectives: (a) prepare them for their clinical clerkship year and (b) assess their ability to perform a focused history and physical examination, demonstrate diagnostic reasoning, make recommendations about clinical management, and display appropriately supportive “bedside manner.” Students then received the following patient information:
(Mr/Ms.) Mann is a 48-year-old (man/woman) presenting to the emergency department for abdominal pain. Vital signs: Temperature 101°F (38°C), Blood Pressure 160/90 mmHg, Heart Rate 104 beats/minute, Respiratory Rate 12 breaths/minute.
Students were to obtain an appropriate focused history, perform a pertinent physical examination, and explain their clinical impression to the patient. If the student used an SBIRT-adherent approach (eg, nonjudgmental, open-ended questions), the patient would disclose previously unrecognized heavy drinking. In prior trainings, students were instructed that this should alert them to engage the patient in further discussion. After the interview, students had 10 mins for reflection and note-writing. Instructors reviewed OSCEs in real-time via video monitoring and debriefed students as a group. Students also completed self-evaluations and received feedback from standardized patient actors.
Curriculum Evaluation Procedures and Outcome Measures
All first-year medical students were required to complete curriculum activities. Research assessments were voluntary and anonymous. The Institutional Review Board reviewed the study protocol, concluding that it did not meet criteria for human subject research. Students assented to study participation at the beginning of each assessment. To link individual-level data, each student generated a unique identification number. Students completed self-report assessments at the beginning of their pre-clinical training (2nd semester) and after the psychiatry clerkship (4th or 5th semester), a period of 1.5–2 years depending on the clinical clerkship schedule to which a student was assigned. For demographic purposes, students reported their sex and race/ethnicity. Students also completed the Attitudes and Opinions Survey (AOS),7 a 6-item questionnaire that separately assesses attitudes toward alcohol and drug use. Students used a 4-point Likert scale (strongly agree, agree, disagree, strongly disagree) to rate their level of agreement with statements about physicians in recovery, the potential societal contributions and appropriateness of healthcare utilization by people with SUDs, the educational value of caring for such patients, and the perceived impact of patients with SUDs on the care of other patients. The six AOS items showed reasonable internal consistency reliability (alpha coefficients = 0.63 for both alcohol and drugs) for students at the beginning of their pre-clinical training. However, in the study by Lindberg et al that established this instrument,7 each item is considered separately as a different dimension of a student’s attitudes toward patients with SUDs. The AOS also asked students if they have had a family member or friend with an alcohol or drug problem.
Data Analysis
As was done in Lindberg et al,7 we combined the AOS response “strongly agree” with “agree” and “strongly disagree” with “disagree.” We further classified AOS responses as “positive” or “negative” toward patients with SUDs. A student’s response was classified as positive if they disagreed with a stigmatizing statement [eg, A healthcare professional in full, sustained recovery from a substance use disorder (SUD) should not be allowed to practice again.] or agreed with an affirming statement (eg, Patients with SUDs can provide meaningful contributions to society.). Similarly, responses were considered negative if they agreed with a stigmatizing statement or disagreed with an affirming statement. Comparing students’ matched pre- and post-intervention responses, we created a four-level variable to classify each student’s pre-post curriculum attitudinal change: (1) persistently negative, (2) persistently positive, (3) negative-to-positive, and (4) positive-to-negative. First, we examined the percentage of students in each attitudinal change group for each of the six AOS questions, looking separately at alcohol and drug-related attitudes, and used McNemar’s tests to display differences in the changes of these six attitudinal domains. Next, we used chi-square tests to assess differences by sex, race/ethnicity (White vs Non-white), presence of a family member/friend with an alcohol or drug problem. We also compared students who completed follow-up in the first half of the clinical clerkship year to those who completed follow-up in the latter half. Fisher’s exact tests would be applied if expected values of less than 5 occurred in more than 25% of cells in the contingency table.
Results
Sample Characteristics
Of 160 eligible medical students, 118 (73.8%) completed the matched pre- and post-intervention alcohol AOS; 116 (72.5%) completed the drug AOS at both time-points. Of these students, 51.2% were women. The racial/ethnic breakdown was as follows: White 58.4%, Black/African American 9.6%, Hispanic/Latino 1.6%, and Asian/Pacific Islander 20.0% (10.4% left this item blank). Nearly half (47.2%) reported having a family member or friend with an alcohol or drug problem.
Attitudinal Change
Table 1 details pre-post change in attitudes toward patients with alcohol use disorder (AUD) and drug use disorder (DUD). For both AUD and DUD, greater than 90% of students reported persistently positive attitudes regarding healthcare professionals in recovery, the potential societal contributions of patients with AUD/DUD, their ability as students to learn from patients with AUD/DUD, and their general attitude toward providing clinical care to patients with AUD/DUD. Such a skewed distribution precluded the investigation of demographic differences. Fewer students reported persistently positive attitudes regarding the appropriateness of healthcare utilization by people with SUDs (AUD 58.5%; DUD 57.8%) and the impact of such patients on the medical care of others (AUD 73.7%; DUD 72.4%), compared to other attitudinal domains (at p-values < 0.0001 in the McNemar’s tests). In fact, 7.6% of students continued to feel that patients with AUD over-utilize healthcare and 22.0% reported more negative attitudes in this domain at follow-up. Results were similar for DUD, with 9.5% holding persistently negative attitudes about healthcare utilization and 22.4% reporting more negative attitudes at follow-up. For attitudes related to healthcare utilization by patients with SUDs and the impact on other patients’ care, domains, there were no statistically significant differences (at the p<0.05 level of significance) in the percentage of students with persistently positive attitudes by sex (p-values = 0.15–0.80 for alcohol, p-values=0.21–0.80 for drugs); race/ethnicity (p-values = 0.22–1.00 for alcohol, p-values = 0.12–1.00 for drugs), having family/friends with a substance problem (p-values = 0.09–1.00 for alcohol, p-values = 0.27–1.00 for drugs), or whether students completed the follow-up assessment in the first or second half of their clinical clerkship year (p-values = 0.09–1.00 for alcohol, p-values = 0.16–0.76 for drugs).
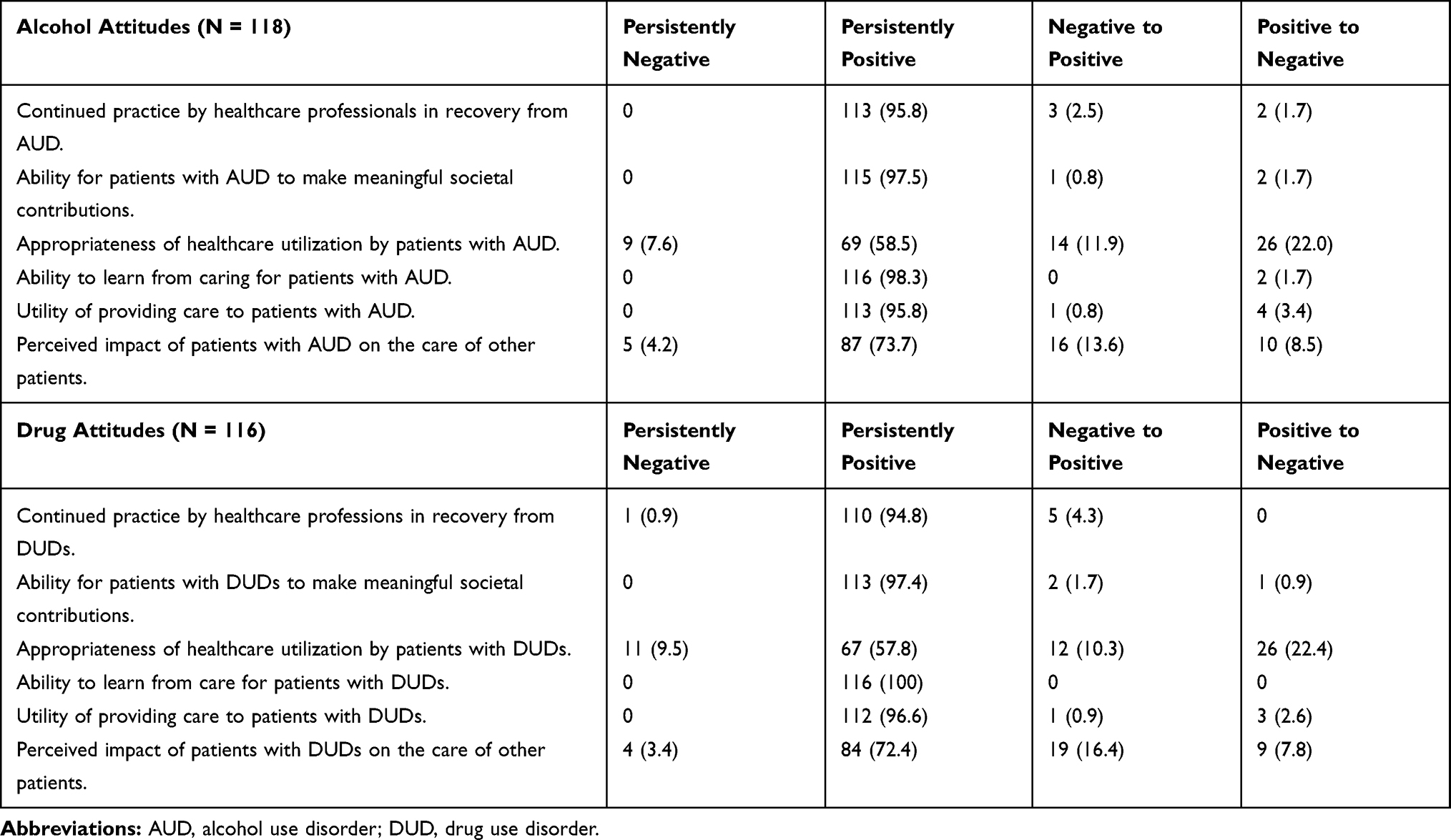 |
Table 1 Trajectory of Medical Student Attitudes Before and After Participation in the Enhanced Pre-Clinical Screening, Brief Intervention, and Referral to Treatment (SBIRT) Curriculum |
Discussion
After participating in this multi-year skills-based SBIRT curriculum, nearly all students reported persistently positive SUD attitudes in several domains. Most felt that patients with SUDs could contribute to their education and to society. Students in our sample held more positive baseline attitudes than previous studies.9,10 One possible explanation is that this cohort of students completed high school and undergraduate education during the current opioid epidemic, a period of heightened attention to SUDs and the negative impact of stigma. This contrasts with medical students raised in the 1980s and 1990s when “Just Say No” was the predominant public health message, casting addiction as wholly volitional. The preservation of such positive attitudes throughout clerkship training is an improvement over previous studies, which showed more global attitudinal deterioration of medical student beliefs with increased clinical training.7
Students reported more discrepant opinions regarding the appropriateness of healthcare utilization by patients with SUDs. For approximately 1 in 5 students, this included movement toward a negative perception of over-utilization. This resembles findings from other studies7 and may reflect the reality that healthcare expenditures are greater for patients with untreated SUDs, compared to patients without an SUD.19 This may also be influenced by clerkship sites, which are predominately inpatient settings where patients are not typically seeking SUD treatment. Training likely focuses on acute medical or psychiatric problems secondary to SUDs rather than offering students the opportunity to witness successful SUD treatment. The over-representation of inpatient training also conflicts with the reality that most evidence-based SUD treatment is delivered outpatient. Further research is needed to understand how to structure training to better promote optimistic, non-stigmatizing attitudes regarding healthcare utilization.
This study has several limitations. First, generalizability is limited because data come from one medical school associated with a large, urban medical center. This school utilizes a 3-semester preclinical curriculum, which may not generalize to four-semester pre-clinical curricula. Second, lack of a control group precludes us from drawing conclusions about causality and limits our ability to control for outside factors that may have influenced students’ attitudes. The AOS instrument asks about drugs as a single category, precluding investigation of possible differences in attitudes by drug type. This study focused on medical students’ attitudes toward patients with SUDs. Therefore, we cannot draw conclusions about students’ skills in delivering SBIRT to patients. Finally, social desirability bias is possible. We attempted to mitigate this through anonymous data collection.
Conclusion
While students who participated in the Enhanced SBIRT Curriculum did not show improved attitudes (likely due to a ceiling effect), our findings indicate that this type of curricular enhancement may help preserve positive medical student attitudes toward SUD treatment and patients with SUDs. This can inform future research to develop and evaluate strategies for promoting positive attitudes among students with more stigmatizing attitudes at baseline. Additionally, by grounding pre-clinical addiction training in the primary care context, this longitudinal curriculum emphasizes that addiction is relevant for all physicians regardless of specialty.
Acknowledgments
The authors wish to thank the following faculty at Columbia University College of Physicians and Surgeons (P&S) for their support throughout the development and implementation of the Enhanced SBIRT Curriculum: Drs. Jonathan Amiel, Beth Barron, Janis Cutler, Ronald Drusin, and Prantik Saha. We also thank research team members Analia Gutierrez, Dr. Roberto Lewis-Fernández, Jennifer Lima, Andrew Tuck, and Kelly Granger for their contributions. Finally, we are grateful to the medical students at Columbia P&S for their engagement in the curriculum and participation in this study.
Disclosure
Dr Frances R Levin reports grants from NIDA and SAMHSA; salary support from New York State Psychiatric Institute; a consulting income from Major League Baseball, and non-financial support from US WorldMEDS, outside the submitted work. Dr. Levin was an unpaid member of a Scientific Advisory Board for Alkermes and US WorldMeds but did not personally receive any compensation in the form of cash payments (honoraria/consulting fees) or food/beverage (she declined food/beverages in both circumstances) nor receive compensation in the form of travel reimbursement. Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award number T32DA007294. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors report no other possible conflicts of interest in this work.
References
1. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
2. Cheng HG, Kaakarli H, Breslau J, et al. Assessing changes in alcohol use and alcohol use disorder prevalence in the United States: evidence from national surveys from 2002 through 2014. JAMA Psychiatry. 2018;75(2):211–213. doi:10.1001/jamapsychiatry.2017.4008
3. Centers for Disease Control and Prevention [homepage on the Internet]. Underlying cause of death 1999–2018 on CDC WONDER online database; 2018. Available from: http://wonder.cdc.gov/ucd-icd10.html.
4. Center for Behavioral Health Statistics and Quality. Results from the 2015 National Survey on Drug Use and Health: Detailed Tables. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2016.
5. Rasyidi E, Wilkins JN, Danovitch I. Training the next generation of providers in addiction medicine. Psychiatr Clin North Am. 2012;35(2):461–480. doi:10.1016/j.psc.2012.04.001
6. Miller NS, Sheppard LM, Colenda C. Why physicians are unprepared to treat patients who have alcohol- and drug-related disorders. Acad Med. 2001;76(5):410–418. doi:10.1097/00001888-200105000-00007
7. Lindberg M, Vergara C, Wild-Wesley R, et al. Physicians-in-training attitudes toward caring for and working with patients with alcohol and drug abuse diagnoses. South Med J. 2006;99(1):28–35. doi:10.1097/01.smj.0000197514.83606.95
8. van Boekel LC, Brouwers EPM, van Weeghel J, et al. Healthcare professionals’ regard towards working with patients with substance use disorders: comparison of primary care, general psychiatry and specialist addiction services. Drug Alcohol Depend. 2014;134:92–98. doi:10.1016/j.drugalcdep.2013.09.012
9. Crapanzano K, Vath RJ, Fisher D. Reducing stigma towards substance users through an educational intervention: harder than it looks. Acad Psychiatry. 2014;38(4):420–425. doi:10.1007/s40596-014-0067-1
10. Cape G, Hannah A, Sellman D. A longitudinal evaluation of medical student knowledge, skills and attitudes to alcohol and drugs. Addiction. 2006;101:841–849. doi:10.1111/j.1360-0443.2006.01476.x
11. Miller WR, Rose GS. Toward a theory of motivational interviewing. Am Psychol. 2009;64(6):527–537. doi:10.1037/a0016830
12. Kaner EF, Beyer FR, Muirhead C, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. 2018;24(2):CD004148.
13. Madras BK, Compton WM, Avula D, et al. Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug Alcohol Depend. 2009;99(1–3):280–295. doi:10.1016/j.drugalcdep.2008.08.003
14. Barata IA, Shandro JR, Montgomery M, et al. Effectiveness of SBIRT for alcohol use disorders in the emergency department: a systematic review. West J Emerg Med. 2017;18(6):1143–1152. doi:10.5811/westjem.2017.7.34373
15. Bernstein SL, D’Onofrio G. Screening, treatment initiation, and referral for substance use disorders. Addict Sci Clin Pract. 2017;12(1):18. doi:10.1186/s13722-017-0083-z
16. Saitz R, Palfai TP, Cheng DM, et al. Screening and brief intervention for drug use in primary care: the ASPIRE randomized clinical trial. JAMA. 2014;312(5):502–513. doi:10.1001/jama.2014.7862
17. Martino S, Ondersma SJ, Forray A, et al. A randomized controlled trial of screening and brief interventions for substance misuse in reproductive health. Am J Obstet Gynecol. 2018;218(3):
18. Ewing JA. Detecting alcoholism: the CAGE questionnaire. JAMA. 1984;252(14):1905–1907. doi:10.1001/jama.1984.03350140051025
19. Cherpitel CJ, Ye Y. Drug use and problem drinking associated with primary care and emergency room utilization in the US general population: data from the 2005 national alcohol survey. Drug Alcohol Depend. 2008;97(3):226–230. doi:10.1016/j.drugalcdep.2008.03.033
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.