")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Mediators of Life-Course and Late-Life Financial Strain on Late-Life Health in Japan: Based on a Cross-Sectional Survey
Authors Sugisawa H , Harada K, Sugihara Y, Yanagisawa S, Shinmei M
Received 1 January 2022
Accepted for publication 22 March 2022
Published 26 April 2022 Volume 2022:15 Pages 883—896
DOI https://doi.org/10.2147/JMDH.S356760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hidehiro Sugisawa,1 Ken Harada,2 Yoko Sugihara,3 Shizuko Yanagisawa,4 Masaya Shinmei5
1International Graduate School for Advanced Studies, J. F. Oberlin University, Machida-shi, Tokyo, Japan; 2Department of Humanities and Social Sciences, Jissen Women’s University, Shibuya-ku, Japan; 3Department of Urban Science and Policy, Tokyo Metropolitan University, Hachioji-shi, Japan; 4Department of Oral Health Science and Social Welfare, Institute of Biomedical Sciences, Tokushima University, Tokushima-shi, Japan; 5Faculty of Human Welfare, Den-En Chofu University, Kawasaki Shi, Japan
Correspondence: Hidehiro Sugisawa, International Graduate School for Advanced Studies, J. F. Oberlin University, 3758, Machida-shi, Tokyo, 194-0294, Japan, Tel/Fax +81(0)02-797-9847, Email [email protected]
Purpose: Few studies have examined together the psychosocial mediators of how life-course and late-life socioeconomic status (SES) influence late-life health. This study explored psychosocial mediators of influences of not only life-course but also late-life financial strain on late-life health in Japan, using a cross-sectional survey. It was hypothesized that: 1) both life-course and late-life financial strain will influence late-life health through common mediators, and 2) such mediating influences will be large on health indicators strongly related to psychosocial resources, such as depressive tendencies and self-rated health.
Methods: The participants (N = 739) were aged 65 years and older and lived in metropolitan Tokyo, Japan. Life-course financial strain was measured retrospectively by the number of financially strenuous experiences over the participants’ life-courses. Possible mediators included stressors (life-course and late-life major traumatic life events) and psychosocial resources (self-esteem, sense of control, health literacy, social networks, and social support). Health indicators included multimorbidity, disabled activities of daily living (ADL), depressive tendency, and poorer self-rated health.
Results: Having a sense of control mediated the significant influences of both life-course and late-life financial strain on disabled ADL. Furthermore, self-esteem significantly mediated the influences of both life-course and late-life financial strain on depressive tendencies and poorer self-rated health. All such mediating influences were significant at p < 0.05. Psychosocial resources did not mediate significant influences of life-course and financial strain on multimorbidity.
Conclusion: The results support our hypotheses and make three main contributions on the mechanism through which SES influences late-life health: 1) psychosocial resources mediate the effect of life-course SES on late-life health; 2) the influence differs depending on health type; and 3) these results can generalize to older adults in not only Japan but also Western countries.
Keywords: accumulative effects model, multiple health indicators, multiple mediation, social class, self-concept
Introduction
Differences in certain health indicators, such as physical health, mental health, and mortality by socioeconomic status (SES) have been observed among populations without the consideration of age group.1,2 Also, significant SES influences on a wide range of health indicators have been found in empirical studies on older adults conducted in both Western3,4 and Eastern countries.5–8 In addition, studies have been conducted on the mediators of the links between SES and health to explain the mechanisms underlying SES differences in health. The Stress Process Model9 and the Reserve Capacity Model10 have been used as the theoretical models to explore the mediators. Both models commonly assert that two factors are related to poorer health in people with lower SES: more exposure to stressors and lower levels of resources required to prevent the negative influences of stressors. There have been accumulative studies, mainly in Western countries, which have identified the mediators between SES and health, while participants were not limited to older adults. According to these studies; stressors, such as strains and life events;11–13 psychological resources, such as a sense of control;12,14,15 optimism;15 and good health literacy16,17 were found to be effective mediators.
However, recently, although studies have established associations between life-course SES and adult health,18 only a few studies have explored mediators of links between life-course SES and adult health. Pudrovska et al19 showed that a sense of mastery mediated the links between financial strain in the life-course and health of older adults. Kan et al20 found that the association between childhood SES and Japanese adult health partially depends on the psychological resources of mastery and a sense of coherence. Bosma et al21 showed that influences of the father’s occupation on self-rated health were mediated by locus of control, neuroticism, and coping style. Lehman et al22,23 indicated that low childhood SES was associated with harsh parenting, which in turn was related to poor metabolic functioning and increased blood pressure in adults from the United States. These findings suggest that common psychosocial factors mediate the influences of both current and life-course SES on adult health.
Whereas previous studies have examined such influences, some points remain to be resolved. First, existing studies on mediators between current or life-course SES and health in adults aged 60 years and older, are scarce, and primarily focus on a limited number of potential psychosocial mediators, such as, social relationships,7 mastery/sense of control,19,24,25 and health literacy.26,27. Conflicting findings regarding whether the effect of SES differences on health are reduced over time28 render it unclear whether results from populations under the age of 60 apply to older adults. Second, although influences of both current and life-course SES on health may be mediated through common psychosocial mediators, few studies have examined whether mediators of influences of current and life-course SES on health are common in the same study. Third, only a handful of studies have examined whether mediating influences of current or life-course SES on health differ by types of health indicators. For instance, a study shows that although education and mental health are largely mediated through social resources, associations between education and physical health are only partly mediated through these resources.29 Another study indicates that psychosocial factors contribute to the explanation of socioeconomic inequalities in self-rated health.30 Additionally, it has been suggested that self-rated health reflects a global assessment of health and incorporates perceptions of a range of physical, mental, and social factors.31 Conversely, it has been indicated that adverse social circumstances facilitate biological programs associated with higher risks of diseases in later-life.32 Accordingly, psychosocial factors could mediate the influences of current or life-course SES on mental health and self-rated health.
Fourth, almost all studies have been conducted in Western countries, which exhibit individualistic tendencies. In individualism, people are motivated primarily by their own preferences, needs, and rights.33 Conversely, it is widely accepted that people in East Asia exhibit a more collectivistic culture, relative to those in Western countries.34 In collectivism, individuals are motivated primarily by the norms and duties imposed by the collective population.33 Under East Asia’s cultural conditions, through strong social cohesion, SES could exert a weaker effect on late-life health, relative to that observed in Western countries. However, in East Asia, health differences by SES in not only the general population,35 but also older adults, have been observed.8 Although the influence of SES on health in East Asia’s adults has been shown in previous research, the applicability of theory and findings regarding the mediators provided in Western countries, to the East Asia context remains unknown.
Accordingly, in this study, we examined psychosocial factors mediating the influences of both life-course and late-life financial strain on late-life health in Japan. Based on the Stress Process Model, a wide range of psychosocial factors were established as mediators: three types of factors—stressors, psychological resources, and social resources. Additionally, multiple health indicators of physical and mental health were used. Consequently, we proposed the following hypotheses: 1) Common psychosocial factors will mediate the influences of both late-life and life-course financial strain on late-life health; and 2) such mediating influences will be large on health indicators strongly related to psychosocial resources, such as depressive tendencies and self-rated health.
We selected Japan as the survey field for the following reasons. Japan is an East Asian country, exhibiting a more collectivistic culture relative to Western countries. It is one of the countries in the world with the longest life expectancy at birth for both males and females. The egalitarian characteristics of Japan could have possibly contributed to this ranking.36
We used financial strain as a possible proxy indicator of actual income in this study. Financial strain measures the balance between income and the requirements of people and provides useful information in addition to income, as people with low incomes do not always report financial strain.4,37 Also, financial strain is likely to affect a wide range of health-related indicators, such as self-rated health, physical function, hypertension, life satisfaction, and mortality, after controlling for actual income.4,38 Further, including financial strain as a measure of financial conditions in childhood is useful because it is difficult to collect actual childhood income information. Although it is a subjective measure, participants can more easily identify experiences of financial strain than actual family income during childhood.39,40 Thus, financial strain is a useful construct that facilitates evaluating life-course SES at several points using the same measure.
We relied on the accumulative effect model, which can describe the influences of life-course SES on later-life health, considering two important points: (1) this model synthesizes elements from the stress process, cumulative disadvantage, and life-course perspectives and emphasizes the accumulation of inequality over the life-course;41 and, (2) studies that compared the effectiveness of models describing influences of life-course SES on health in older adults among several models reported an advantage of the accumulative effective model.42,43
Materials and Methods
Analytic Framework
The analytic framework is shown in Figure 1. Psychosocial mediators included stressors (life-course and late-life major traumatic life events), psychological resources (self-esteem, a sense of control, and health literacy), and social resources (social networks and social support). a*c indicates indirect influences of life-course financial strain on late-life health through mediators. b*c indicates indirect influences of late-life financial strain on late-life health through mediators. Mediating influences of life-course and financial strain on late health were evaluated using health indicators in older adults: multimorbidity, depressive tendencies, disabled activities daily living (ADL), depressive symptoms, and poor self-rated health.
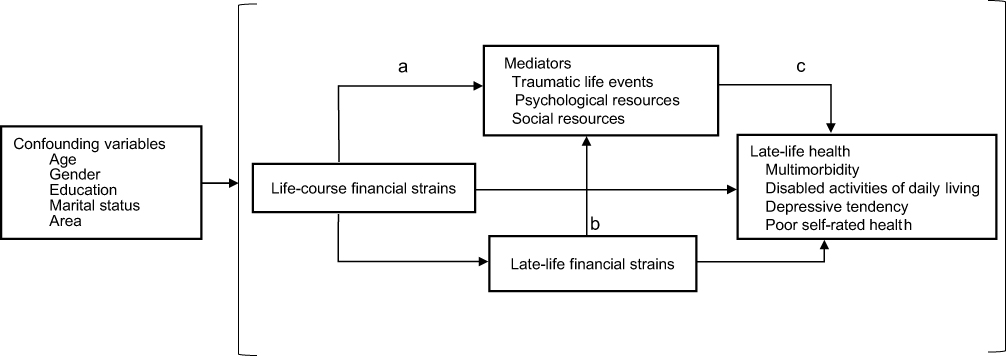 |
Figure 1 Analytic framework. Notes: a*c indicates indirect influences of life-course financial strain on late-life health through mediators. b*c indicates indirect influences of late-life financial strain on late-life health through mediators. |
Participants
One thousand people aged 65 years or older from each of two cities (Sumida-City and Setagaya-City) in the Tokyo metropolitan area were selected via systematic sampling, for a total of 2000 participants. The required sample size differed by estimation methods. For the multiple regression model, applicable for continuous health indicators (multimorbidity in this study), we obtained a sample size of 135 as a result of calculation using G*power.44 To calculate the required sample size for multiple logistic regression for the dummy health indicators (disabled ADL, depressive tendencies, and poor self-rated health in this study) using G*Power, we needed additional information, such as the coefficient of determination of the main predictor with other predictors, which is often unavailable in practice.45 As an alternative, we calculated the required sample size by using a convenient method (Sample size = 10*(k/p); k, number of independent variables; p, proportion for the outcome in the least categories) developed by Peduzzi et al.46 By entering k = 14 and p = 9.6% into the above formula, we estimated 1458 to be the required sample size. The proportion for the outcome in the lowest number of categories was obtained from the following data: According to National Life Survey in 2013,47 each rate of depressive tendency, ADL disability, and poor self-rated health, used as outcome health indicators in this study, was 9.6%, 12.5%, and 24.1%, respectively. As 9.6% of depressive tendency was induced in the largest sample size, we used this value to calculate the sample size. Furthermore, a sample size with 500 and above yielded statistics for logistic regression, which represented the parameters in the targeted population.48 To obtain a sample size of 1000 which was the approximate intermediate size between two calculations, we decided upon a sample size of 2000 (expecting a response rate of 50%).
The two cities were selected as locations for the survey to ensure the sample included participants with a wide range of SES-related factors, including income and educational attainment. The average annual income per taxpayer in 2014 was 3.60 million Yen in Sumida-City and 5.36 million Yen in Setagaya-City, and the proportion of university graduates in 2010 was 16.6% and 25.3%, respectively.49 Face-to-face interviews were conducted with each participant at home in March 2016. To increase participation rates, we re-visited those who could not be interviewed because of temporary unavailability or they had no time to be interviewed during at least three interviewer visits. A total of 761 participants ultimately completed the survey, for an overall participation rate of 38.1%. Non-participation reasons included refusal (41.3%), absence (13.3%), poor health (3.4%), relocation (2.4%), death (0.6%), and other (0.9%). The final number of participants included in the analysis was 739 after those with a high possibility of cognitive impairment were excluded. Cognitive impairment was measured using the Short Portable Mental Status Questionnaire,50 modified to exclude the “name of this place” item because it duplicated the “your street address” item, since interviews took place at home for nearly all participants. Using the original item cut-offs,51 we excluded those with more than three errors based on their answers to the Short Portable Mental Status Questionnaire.
Measurements
Life-Course and Late-Life Financial Strain
Life-course financial strain was evaluated using a retrospective method that applied life-course benchmark periods: <18 years (childhood), 18–35 years (young adults), and 35–50 years (middle age). Items that evaluated financial strain were developed by Kahn and Pearlin.42 The validity of retrospective self-reported financial strain has been confirmed by Kahn and Pearlin42 and others43,52 who found that factors defined by retrospective self-reported financial strain over a lifetime have a significant influence on adults’ health. Financial strain in the period younger than 18 years old was evaluated by asking participants: “Did your family have trouble covering expenditures for necessities, such as food, clothes, and housing?” Choices of answers included “a lot of trouble,” “some trouble,” “a little trouble,” and “no trouble.” For the groups aged 18–35 and 35–50 years old, we changed “your family,” in the question, to “you.” When the data were finally analyzed, participants who chose “a lot of trouble” or “some trouble” were defined as the group with exposure to financial strain, and participants who chose “a little trouble” or “no trouble” were defined as the group without exposure to financial strain. Therefore, the accumulation indicator reflected the frequency of exposure to financial strain over the life-course, regardless of the age periods in which participants were exposed to financial strain. The maximum score was three and the minimum was zero. The level of current financial strain in late-life was measured by asking “How do you rate your family’s household finances at the present time?” Choices of answers included “very difficult” (4), “somewhat difficult” (3), “neither” (2), “a little difficult” (1), and “absolutely not difficult” (0), using a 5-point scale.
Stressors
Life-Course Major Traumatic Life Events
This was created using two scales. Both were for the number of major traumatic life events participants experienced; one for before the age of 18, and the other before the age of 65. The number of major traumatic life events before the age of 18 was measured using a five-item scale: repeating the same year at a school, getting into trouble with the police, being physically abused by parents, dealing with a parent’s drug or alcohol addiction which badly affected the family, and maltreatment and bullying in school. The first four items came from a psychological and lifestyle questionnaire from the 2006–2020 Health and Retirement Study.53 The fifth item, “Maltreatment and bullying in school,” was added because a study indicated that this event strongly influenced an adult’s well-being.54 Participants provided the age period when they experienced each life event: <6 years, 6–11 years, or 12–18 years. Those who experienced the same life events multiple times were asked to choose the nearest age period when they were exposed to the event.
The number of lifetime major traumatic life events before the age of 65 included the following five items: losing a child, dealing with the drug or alcohol addiction of family members, being physically abused, experiencing a life-threatening accident, and family members facing a life-threatening accident. This also came from the psychological and lifestyle questionnaire in the 2006–2020 Health and Retirement Study.53 Participants indicated whether they experienced each life-course major traumatic life events and the age periods during which they experienced them; <6 years, 6–11 years, 12–17 years, 18–30 years, and 31–64 years. Those who experienced the same traumatic life events multiple times were asked to choose the nearest age period in which they experience them. Although the original scale was composed of seven items, we deleted two items: “encountering a natural disaster” and “using weapons or getting injured in war.” This was done because of the low possibility of these events being caused by financial strain. This measure was scored by calculating a simple sum of both the number of traumatic life events before the age of 18 years and the number of major traumatic life events before the age of 65 years. However, both scales included two similar events: “being physically abused by parents” and “dealing with a parent’s drug or alcohol addiction which negatively impacted the family.” We did not count participants who experienced both traumatic events before the age of 18 years in the second scale to avoid double counting.
Late-Life Major Traumatic Life Events
This was measured by using the same five items of the second scale which was used to measure major traumatic life events before the age of 65 years.
Psychosocial Resources
We used three psychological indicators (self-esteem, a sense of control, and health literacy) and two social indicators (social networks and social support).
Self-Esteem
This was measured by a seven-item scale extracted from Rosenberg’s self-esteem scales used in the Survey of Midlife Development in Japan (MIDJA).55 Responses were scored on a 7-point scale ranging from 1 (agree strongly) to 7 (disagree strongly). The internal consistency reliability of the scale in this study (Cronbach’s alpha) was 0.485. Recognizing that this scale did not show high reliability, we interpreted our results with caution.
A Sense of Control
This was measured using the sum of two scales from the Survey of MIDJA.55 Each scale scored items on a 7-point scale that ranged from 1 (agree strongly) to 7 (disagree strongly). In this study, the internal consistency reliability of the combined scale was 0.750.
Health Literacy
We used a health literacy scale by Ishikawa, et al56 for this study. All items were scored on a 5-point Likert scale from 1 (totally disagree) to 5 (strongly agree), and the scores were summed to obtain a total score. The internal consistency reliability of the combined scale was 0.942.
Social Networks
These were measured by summing the frequency of contact with people/organizations in two categories: friends/neighbors and community organizations. Response choices included “more than or equal to two times a week,” “approximately once a week,” “two or three times a month,” “approximately once a month,” “less than once a month,” and “almost no contact” for each type of social network. The midpoint of each choice (10, 4, 2.5, 1, 0.5, and 0, respectively) was assigned to each category to quantify the responses.
Social Support
This measure was based on the perceived availability of four types of social support: instrumental, emotional, informational, and companionship. Participants who could receive either of the four support types were assigned a score of 1 and those who could not, scored zero, and the scores were summed for a total score.
Health Outcomes
Health indicators included multimorbidity, disabled ADL, depressive tendency, and self-rated health.
Multimorbidity
This was measured by the existence of serious and chronic illnesses,57 such as cancer, diabetes, heart failure, hypertension, and stroke. Multimorbidity indices comprised the total number of serious and chronic illnesses participants had during the survey.
Disabled ADL
This was measured by five activities, such as taking a bath and putting on/taking off clothes for which aid was either required or not required. Responses were scored on a 4-point scale from “can do without difficulty” to “require total assistance.” Participants with one or more items rated below the “can do without difficulty” response were categorized as disabled ADL.
Depressive Tendency
This was measured with the Japanese version of the Geriatric Depression Scale.58–60 Participants with more than five points were defined as having a depressive tendency.
Poorer Self-Rated Health
This was measured by the question “In general, how would you rate your health today?” Response choices were “excellent,” “very good,” “good,” “fair” and “poor.” Participants who selected “fair” or “poor” were categorized as having poorer self-rated health.
Confounding Variables
Demographic Variables
These included age, sex (1 = male, 0 = female), marital status (1 = having a spouse, 0 = not having a spouse), and city of residence (1 = city with high SES residents, 0 = city with low SES residents).
Educational Attainment
This was measured by asking participants to indicate their highest academic qualification from the following list: “junior high school graduate,” “high school graduate,” “vocational school graduate,” “junior college graduate,” “university graduate” or “university post-graduate.” The corresponding number of years of education according to the Japanese educational system, 9, 12, 13, 14, 16, and 18, respectively, were assigned to each category to quantify the responses. We performed a preliminary analysis to examine whether the relationships between educational attainment and the three health behaviors were linear. The results indicated almost linear relationships.
Participants who completed at least 70% of the items for each scale were included in the analyses by substituting the participants’ mean of the completed scale items for the missing values. Shrive et al61 and Siddiqui62 suggested that this is the desirable method for inputting both random and non-random missing items in psychometric scale constructions.
Statistical Analysis
Mplus version 8.163 was used for data analyses. Multiple mediation analysis, proposed by Preacher and Hayes,64 was used to estimate total and specific indirect effects in a multiple-factor model. All variables in the model were standardized to compare the indirect effect sizes produced by each mediator. Bootstrapping was used to estimate the total and specific indirect effects of the mediators. Point estimates and 95% confidence intervals were determined according to the null hypothesis. A full information maximum likelihood approach to handling missing data was employed in the analysis.63 Overall model fit was assessed using root mean square error of approximation (RMSEA) and comparative fit index (CFI). For good model fit, the most widely used cut-offs for RMSEA include values less than 0.05 or 0.06 that suggest good fit, and values between 0.05 and 0.10, that suggest acceptable fit. Furthermore, CFI values above 0.95 are commonly considered to suggest good fit, and values between 0.90 and 0.95 are considered acceptable.65
Ethical Considerations
The study complied with the guidelines of the Declaration of Helsinki. All procedures were approved by the research ethics board at J. F. Oberlin University (Approval Number:15040). A letter of invitation that explained the aims and content of the entire study project, including the present study, was provided to each potential participant; only those who verbally consented to participate were interviewed. Data collection procedures and storage management were followed to ensure confidentiality. Participation was entirely voluntary, and confidentiality was fully guaranteed.
Results
Participant Characteristics
Table 1 displays the distribution of participants’ health, life-course, late-life financial strain, and other measures. The participants’ mean age was 74.9 years, and women accounted for 55.2% of the total sample. The average number of multimorbidity was 1.3. Rates of disabled ADL, depressive tendency, and poorer self-rated health were 6.5%, 24.3%, and 15.2%, respectively. Rates for each category of financial strain over the life-course were 71.0% for zero, 16.3% for one, 8.2% for two, and 4.5% for three. Regarding late-life major traumatic life events, as the average number of the experiences was very small (0.04), this variable was deleted from the analytic model which explored mediators between late-life financial strain and late-life health.
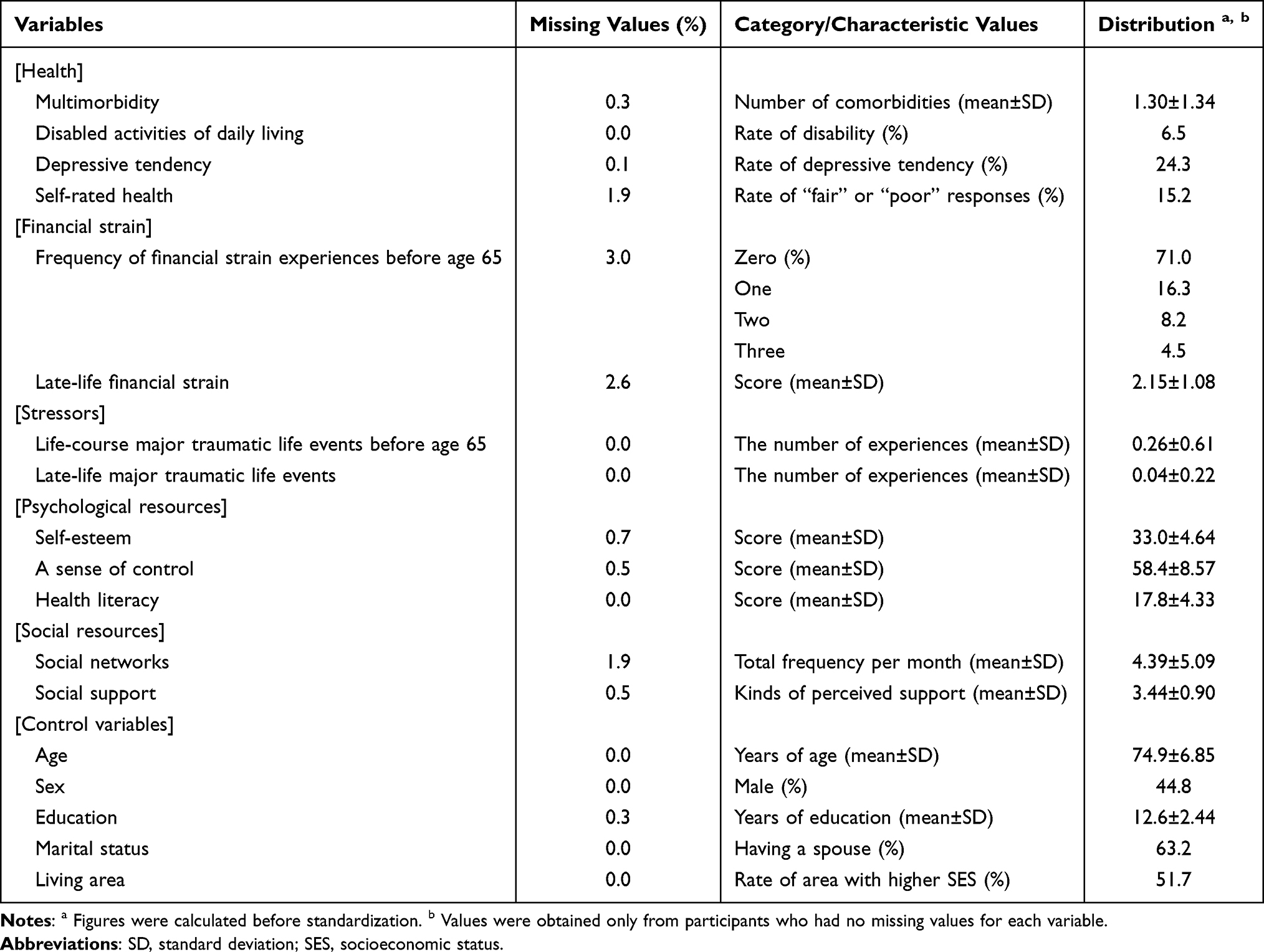 |
Table 1 Distribution of Participant Health, Late-Life and Life-Course Financial Strain, and Control Variables |
Multiple Mediation Analysis
Table 2 shows the results of the multiple mediation analyses on the relationships between life-course and late-life financial strain and four health indicators. Based on values for RMSEA and CFI as model fit indices, the model fit for each of the four indicators was acceptable.
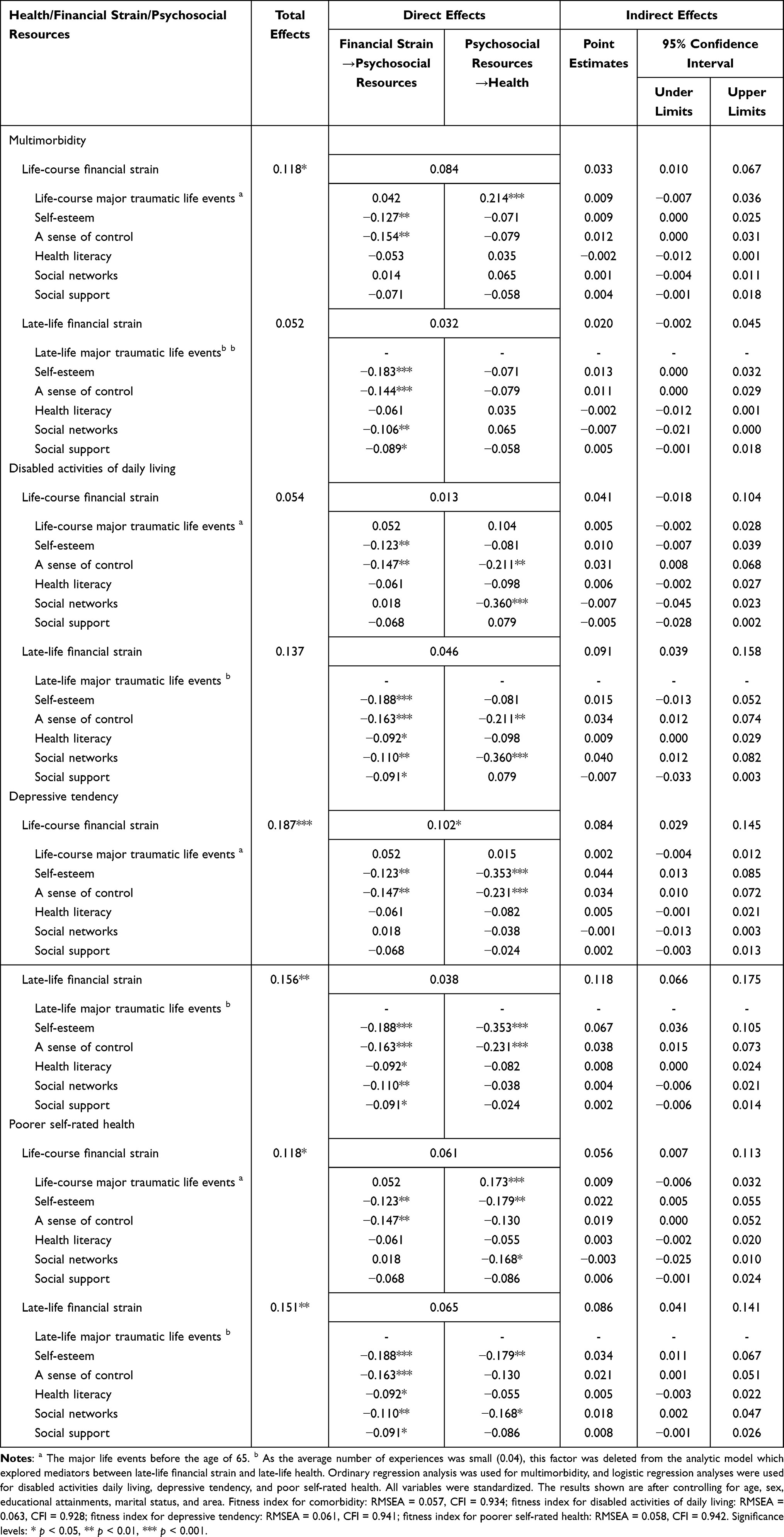 |
Table 2 Mediating Influences of Psychosocial Factors Between Financial Strain and Health |
For a psychosocial factor to be regarded as a mediator, the following paths all needed to be statistically significant: from financial strain to the psychological factor; from the psychological factor to health; and from financial strain to health via the psychological factor (indirect influence). Based on these criteria, self-esteem and a sense of control were significant mediators of the influences of both late-life and life-course financial strain on depressive tendency (p < 0.05). In addition, a sense of control significantly mediated the influences of both late-life and life-course financial strain on disabled ADL (p < 0.05), and self-esteem significantly mediated the influences of both late-life and life-course financial strain on poorer self-rated health. Meanwhile, social networks significantly mediated the influence of late-life financial strain on disabled ADL and poorer self-rated health. No psychosocial factors significantly mediated the influences of life-course and late-life financial strain on multimorbidity.
Health literacy and social support were significantly influenced by late-life financial strain but did not significantly influence any of the four health indicators. Finally, major traumatic life events were not significantly influenced by life-course financial strain.
Discussion
Previous studies that partly included older adults have focused on only limited types of mediators between life-course SES and late-life health. According to them, psychological resources, such as mastery,19,20 a sense of control,20,21 hostility, and hopelessness66 were significantly effective as mediators. This study examined how levels of psychological and social factors mediate the links not only between late-life financial strain but also life-course financial strain and late-life health. Consequently, we found that psychological resources, such as self-esteem and a sense of control significantly (1) mediated the links between life-course financial strain and disabled ADL, depressive tendency, or poorer self-rated health, and (2) mediated the links between late-life financial strain and depressive tendency, or poorer self-rated health. These results suggest that psychological resources have a mediating influence between life-course SES and late-life health. Our hypothesis (1), induced from the theory and findings in the context of Western countries, was supported in this study for Japanese older adults. Regarding hypothesis (2), that mediating influences will be large on health indicators strongly related to psychosocial resources, such as depressive tendency and self-rated health, it was found that psychological resources significantly mediated the influences of financial strain on both depressive tendency and poorer self-rated health, but not on multimorbidity. Thus, hypothesis (2) is supported. This study also showed that psychological resources significantly mediated the influences of financial strain on disabled ADL. According to review articles,67,68 risk factors of ADL decline include social relations and depression related to psychosocial factors. In line with previous studies’ findings that psychosocial resources strongly influence ADL, the results in this study support hypothesis (2).
Health literacy, which was included in psychological resources in this study, was significantly influenced by late-life financial strain. However, it did not influence any of the four health indicators and thus does not work as a mediator. In a review article, health literacy partially mediated the effect that SES exerts on health status and on several health-related outcomes with participants that were not just limited to older adults.69 In this study, health literacy significantly influenced health indicators on disabled ADL, depressive tendency, and poorer self-rated health before controlling self-esteem and a sense of control although these results have not been depicted in the “Results” section. Few previous studies that investigate mediators of health literacy on SES health disparities consider influences of other psychological resources.16 It is possible that the influence of health literacy as a mediator is explained by self-esteem and a sense of control.
Social networks were significantly influenced by late-life financial strain but not by life-course financial strain. One study found that social network size in late-life was influenced by occupational status, and not directly affected by father’s occupational or educational status which indicated childhood SES.70 Social networks in late-life may be indirectly influenced by life-course financial strain; thus, only through late-life financial strain, it is possible that influences of life-course financial strain on late-life health could not be mediated through late-life social networks. In addition, this study found that social support did not work as a significant mediator. In fact, we found no differences in health indicators by social support. However, previous studies have found that social support influences the maintenance of some types of health indicators in older adults: ADL,38 mental health,71 cognitive function,72 and self-rated health.73 As some studies empirically explore a sense of control74 and self-esteem75 as mediators between social support and health or well-being, we examined influences of social support on health indicators before controlling for influences of a sense of control and self-esteem. As a result, we obtained results that showed that social support significantly mediated between late-life financial strain and poorer self-rated health, although these findings have not been depicted in the “Results” section. It is possible that the influence of social support as a mediator is explained by self-esteem and a sense of control.
In this study, the reason for using major traumatic life events as stressors in the life-course of an individual, which were ineffective mediators, is related to their insignificant influence on the effects of life-course financial strain on this indicator. In a review article by Hatch and Dohrenwend,76 some studies indicate that the distribution of traumatic life events differ by SES. However, Hatch and Dohrenwend76 asserted that it is puzzling that the prevalence of reported traumatic and other stressful events over the life-course tend to be higher in younger adults than older adults, because cumulative exposure should increase with longevity if other things are equal. According to Norris,77 there is one possible explanation for this: problems related to an increasingly imperfect recall with increasing length of the recall period for older participants. These problems of increasingly imperfect recall and attrition from the analytic sample, because of bad health, may contribute to reduced differences in life events by life-course financial strain.
Some limitations of the study need to be considered when interpreting the results. First, the response rate of the survey used by this study was low. Response rates of face-to-face interview surveys using 2002–2006 cumulative data of the Japanese General Social Survey for people aged 20–89 years across Japan were provided by city size and age categories.78 This report indicates that the response rate in people aged 65–89 years living in Tokyo was 45.3%. The response rate of this survey, which was conducted in 2016, does not seem low.
Second, we were unable to explore the causal links between financial strain, especially late-life financial strain and health, because we examined only cross-sectional data. Poorer health could influence financial strain by reducing labor wages and increasing medical expenses. Furthermore, although life-course financial strain did not influence major traumatic life events in this study, financial strain caused by major traumatic life events influenced health, possibly showing reverse causation. Therefore, an analysis of longitudinal data to determine causal links between financial strain and health is required. Third, recall bias associated with aggregate self-report measures can lead to under- or over-estimates of associations.79 Longitudinal studies that track the same participants from childhood to old age are required to examine the influence of life-course SES on later-life health. This approach would allow us to identify causal links between life-course SES and later-life health and would prevent recall bias, which is a concern in retrospective studies of life-course SES.
Conclusions
This study explored psychosocial factors mediating the influences of not only life-course but also late-life financial strain on late-life health in Japan, using a cross-sectional survey. Results showed that two psychological resources (self-esteem and a sense of control) significantly mediated the links between life-course/late-life financial strain and disabled ADL, depressive tendency, or poorer self-rated health. Psychosocial resources did not work as mediators between financial strain and multimorbidity. Thus, hypotheses (1) and (2) were supported. Our results make three main contributions on the mechanism through which SES influences late-life health: 1) psychosocial resources mediate the effect of life-course SES on late-life health; 2) the influence differs depending on health type; and 3) these results can generalize to older adults in not only Japan but also Western countries.
Funding
This work was supported by Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Number 18H03651 (PI: Sugisawa).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Lorant V, Deliege D, Eaton W, et al. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol. 2003;157:98–112.
2. Mackenbach JP, Kunst AE, Cavelaars AE, et al. Socioeconomic inequalities in morbidity and mortality in Western Europe. The EU Working Group on Socioeconomic Inequalities in Health. Lancet. 1997;349:1655–1659.
3. Huisman M, Read S, Towriss CA, et al. Socioeconomic inequalities in mortality rates in old age in the World Health Organization Europe Region. Epidemiol Rev. 2013;35:84–97.
4. Szanton SL, Allen JK, Thorpe RJ, et al. Effect of financial strain on mortality in community-dwelling older women. J Gerontol B, Psychol Sci Soc Sci. 2008;63:S369–S374.
5. Jeon GS, Jang SN, Rhee SJ, et al. Gender differences in correlates of mental health among elderly Koreans. J Gerontol B Soc Sci. 2007;62:S323–S329.
6. Liang J, McCarthy JF, Jain A, et al. Socioeconomic Gradient in old age mortality in Wuhan, China. J Gerontol B, Soc Sci. 2000;55B:S222–S233.
7. Liu X, Hermalin AI, Chuang YL. The effect of education on mortality among older Taiwanese and its pathway. J Gerontol B, Soc Sci. 1998;53B:S71–S82.
8. Sugisawa H, Harada K, Sugihara Y, et al. Socioeconomic status disparities in late-life disability based on age, period, and cohort in Japan. Arch Gerontol Geriatr. 2018;75:6–15.
9. Pearlin LI. The sociological study of stress. J Health Soc Behav. 1989;30:241–256.
10. Gallo LC, Matthews KA. Understanding the association between socioeconomic status and physical health: do negative emotions play a role? Psychol Bull. 2003;129:10–51.
11. Businelle MS, Mills BA, Chartier KG, et al. Do stressful events account for the link between socioeconomic status and mental health? J Public Health. 2013;36:205–212.
12. Gallo LC, Smith TW, Cox CM. Socioeconomic status, psychosocial processes, and perceived health: an interpersonal perspective. Ann Behav Med. 2006;31:109–119.
13. Orpana HM, Lemyre L, Kelly S. Do stressors explain the association between income and declines in self-rated health? A longitudinal analysis of the National Population Health Study. Int J Behav Med. 2007;14:40–47.
14. Ing JD, Reutter L. Socioeconomic status, sense of coherence and health in Canadian women. Can J Public Health. 2003;94:224–228.
15. Kan C, Kawakami N, Karasawa M, et al. Psychological resources as mediators of the association between social class and health: comparative findings from Japan and the U.S. Int J Behav Med. 2014;21:53–65.
16. Lastrucci V, Lorini C, Caini S, et al. Health literacy as a mediator of the relationship between socioeconomic status and health: a cross-sectional study in a population based sample in Florence. PLoS One. 2019;14:e0227007.
17. van der Heide I, Wang J, Droomers M, et al. The relationship between health, education, and health literacy: results from the Dutch Adult Literacy and Life Skills Survey. J Health Commun. 2013;18(Suppl 1):172–184.
18. Larson K, Russ SA, Kahn RS, et al. Health disparities: a life course health development perspective and future Research directions. In: Halfon N, Forrest CB, Lerner RM, et al. editors. Handbook of Life Course Health Development. Cham, Switzerland: Springer International Publishing AG; 2018:499–520.
19. Pudrovska T, Schieman S, Pearlin LI, et al. The sense of mastery as a mediator and moderator in the association between economic hardship and health in late life. J Aging Health. 2005;17:634–660.
20. Kan C, Kawakami N, Umeda M. Mediating role of psychological resources on the association between childhood socioeconomic status and current health in the community adult population of Japan. Int J Behav Med. 2015;22:764–774.
21. Bosma H, van de Mheen HD, Mackenbach JP. Social class in childhood and general health in adulthood: questionnaire study of contribution of psychological attributes. BMJ. 1999;318:18–22.
22. Lehman BJ, Taylor SE, Kiefe CI, et al. Relation of childhood socioeconomic status and family environment to adult metabolic functioning in the CARDIA Study. Psychosom Med. 2005;67:846–854.
23. Lehman BJ, Taylor SE, Kiefe CI, et al. Relationship of early life stress and psychological functioning to blood pressure in the CARDIA Study. Health Psychol. 2009;28:338–346.
24. Bosma H, Van Jaarsveld CHM, Tuinstra J, et al. Low control beliefs, classical coronary risk factors, and socioeconomic differences in heart disease in older persons. Soc Sci Med. 2005;60:737–745.
25. Chi I, Chou KL. Financial strain and depressive symptoms among Hong Kong Chinese elderly: a longitudinal study. J Gerontol Soc Work. 2000;32:41–60.
26. Bennett IM, Chen J, Soroui JS, et al. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann Fam Med. 2009;7:204–211.
27. Howard DH, Sentell T, Gazmararian JA. Impact of health literacy on socioeconomic and racial differences in health in an elderly population. J Gen Intern Med. 2006;21:857–861.
28. Dupre MA. Educational differences in age-related patterns of disease: reconsidering the cumulative disadvantage and age-as-leveler hypotheses. J Health Soc Behav. 2007;48:1–15.
29. Zhang W, Chen Q, McCubbin H, et al. Predictors of mental and physical health: individual and neighborhood levels of education, social well-being, and ethnicity. Health Place. 2011;17:238–247.
30. Moor I, Spallek J, Richter M. Explaining socioeconomic inequalities in self-rated health: a systematic review of the relative contribution of material, psychosocial and behavioural factors. J Epidemiol Community Health. 2017;71:565–575.
31. Mavaddat N, Kinmonth AL, Sanderson S, et al. What determines Self-Rated Health (SRH)? A cross-sectional study of SF-36 health domains in the EPIC-Norfolk cohort. J Epidemiol Community Health. 2011;65:800–806.
32. Kuh D, Ben-Shlomo Y, Lynch J, et al. Life course epidemiology. J Epidemiol Community Health. 2003;57:778–783.
33. Triandis HC. Individualism & Collectivism. New York, NY: Westview Press; 1995.
34. Kitayama S, Park H, Sevincer TA, et al. A cultural task analysis of implicit Independence: comparing North America, Western Europe, and East Asia. J Pers Soc Psychol. 2009;97:236–255.
35. Sugisawa H, Harada K, Sugihara Y, et al. Socioeconomic status and self-rated health of Japanese people, based on age, cohort, and period. Popul Health Metr. 2016;14:27.
36. Wilkinson R, Picket K. The Spirit Level: Why More Equal Societies Almost Always Do Better. London: Allen Lane; 2009.
37. Mirowsky J, Ross C. Economic hardship across the life course. Am Sociol Rev. 1999;64:548–569.
38. Krause N, Newsom JT, Rook KS. Financial strain, negative social interaction, and self-rated health: evidence from two United States nationwide longitudinal surveys. Ageing Soc. 2008;28:1001–1023.
39. Batty GD, Lawlor DA, Macintyre S, et al. Accuracy of adults’ recall of childhood social class: findings from the Aberdeen children of the 1950s study. J Epidemiol Commun Health. 2005;59:898–903.
40. Berney LR, Blane DB. Collecting retrospective data: accuracy of recall after 50 years judged against historical records. Soc Sci Med. 1997;45:1519–1525.
41. Shippee TP, Wilkinson LR, Ferraro KF. Accumulated financial strain and women’s health over three decades. J Gerontol B, Psychol Sci Soc Sci. 2012;67:585–594.
42. Kahn JR, Pearlin LI. Financial strain over the life course and health among older adults. J Health Soc Behav. 2006;47:17–31.
43. Sugisawa H, Sugihara Y, Kobayashi E, et al. The influence of lifecourse financial strains on the later-life health of the Japanese as assessed by four models based on different health indicators. Ageing Soc. 2019;39:2631–2652.
44. Faul F, Erdfelder E, Buchner A, et al. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41:1149–1160.
45. Kim S, Heath E, Heilbrun L. Sample size determination for logistic regression on a logit-normal distribution. Stat Methods Med Res. 2017;26:1237–1247.
46. Peduzzi P, Concato J, Kemper E, et al. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49:1373–1379.
47. Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions 2013. Ministry of Health, Labour and Welfare; 2014.
48. Nemes S, Jonasson JM, Genell A, et al. Bias in odds ratios by logistic regression modelling and sample size. BMC Med Res Methodol. 2009;9:56.
49. Statistics Bureau, Ministry of Internal Affairs and Communications. Regional statistics database, portal site of official statistics of Japan; 2016. Available from: http://www.e-stat.go.jp/SG1/chiiki/ToukeiDataSelectDispatchAction.do.
50. Pfeiffer E. A short portable mental status questionnaire for the assessment of organic brain deficits in elderly patients. J Am Geriatr Soc. 1975;23:433.
51. Liang J, Borawski-Clark E, Liu X, et al. Transitions in cognitive status among the aged in Japan. Soc Sci Med. 1996;43:325–337.
52. Szanton SL, Thorpe RJ, Whitfield K. Life course financial strain and health in African-Americans. Soc Sci Med. 2010;71:259–265.
53. Smith J, Fisher G, Ryan L, et al. Health and Retirement Study Psychosocial and Lifestyle Questionnaire 2006-2010: Documentation Report. Ann Arber, Michigan: University of Michigan; 2013.
54. Oshio T, Umeda M, Kawakami N. Childhood adversity and adulthood subjective well-being: evidence from Japan. J Happiness Stud. 2013;14:843–860.
55. Ryff CD, Kitayam S, Karasawa M, et al. Survey of Midlife Development in Japan (MIDJA), April-September 2008 (ICPSR 30822). Ann Arber, Michigan: Inter-university Consortium for Political and social Research; 2022.
56. Ishikawa H, Nomura K, Sato M, et al. Developing a measure of communicative and critical health literacy: a pilot study of Japanese office workers. Heath Promot Int. 2008;23:269–274.
57. Ferraro KF, Farmer MM. Utility of health data from social surveys: is there a gold standard for measuring morbidity? Am Sociol Rev. 1999;64:303–315.
58. Niino N, Imaizumi T, Kawakami N. A Japanese translation of the Geriatric Depression Scale. Clin Gerontol. 1991;2:85–87.
59. Yesavage J, Brink T, Rose T, et al. Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. 1983;17:37–49.
60. Montorio I, Izal M. The geriatric depression scale: a review of its development and utility. Int Psychogeriatr. 1996;8:103–112.
61. Shrive FM, Stuart H, Quan H, et al. Dealing with missing data in a multi-question depression scale: a comparison of imputation methods. BMC Medical Res Methodol. 2006;6:57.
62. Siddiqui OI. Methods for computing missing item response in psychometric scale construction. Am J Biostat. 2015;5:1–6.
63. Muthén LK, Muthén BO. Mplus User’s Guide.
64. Preacher KJ, Hayes AJ. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. 2008;40:879–891.
65. Lai K, Green SB. The problem with having two watches: assessment of fit when RMSEA and CFI disagree. Multivar Behav Res. 2016;51:220–239.
66. Harper S, Lynch J, Hsu WL, et al. Life course socioeconomic conditions and adult psychosocial functioning. Int J Epidemiol. 2002;31:395–403.
67. Stuck AE, Walthert JM, Nikolaus T, et al. Risk factors for functional status decline in community-living elderly people: a systematic literature review. Soc Sci Med. 1999;48:445–469.
68. van der Vorst A, Zijlstra GAR, Witte ND, et al. Limitations in activities of daily living in community-dwelling people aged 75 and over: a systematic literature review of risk and protective factors. PLoS One. 2016;11:e0165127.
69. Stormacq C, Van den Broucke S, Wosinski J. Does health literacy medicate the relationships between socioeconomic status and health disparities? Integrative review. Health Promot Int. 2019;34:e1–e17.
70. van Groenou MIB, van Tilburg TG. Network size and support in old age: differentials by socio-economic status in childhood and adulthood. Ageing Soc. 2003;23:625–645.
71. Tengku Mohd TAM, Yunus RM, Hairi F, et al. Social support and depression among community dwelling older adults in Asia: a systematic review. BMJ Open. 2019;9:e026667.
72. Kelly ME, Duff H, Kelly S, et al. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: a systematic review. Syst Rev. 2017;6:259.
73. White AM, Philogene GP, Fine L, et al. Social support and self-reported health of older adults in the United States. Am J Public Health. 2009;99:1872–1878.
74. Bisconti TL, Bergeman CS. Perceived social control as a mediator of the relationships among social support, psychological well-being, and perceived health. Gerontologist. 1999;39:94–103.
75. Kong F, Zhao J, You X. Self-esteem as mediator and moderator of the relationship between social support and subjective well-being among Chinese University students. Soc Indic Res. 2013;112:151–161.
76. Hatch SL, Dohrenwend BP. Distribution of traumatic and other stressful life events by race/ethnicity, gender, SES and age: a review of the research. Am J Comm Psychol. 2007;40:313–332.
77. Norris FH. Epidemiology of trauma: frequency and impact of different potentially traumatic events on different demographic groups. J Consult Clin Psychol. 1992;2:60409–60418.
78. Hanibuchi T, Muranaka A, Hanaoka K, et al. Regional differences in response rate in a social survey: analysis of survey completion data of the JGSS cumulative data 2000–2006. JGSS Research Series. 2022;1(11):181–192.
79. Matthews KA, Gallo LC. Psychological perspectives on pathways linking socioeconomic status and physical health. Ann Rev Psychol. 2011;62:501–530.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.