Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Mediating Effect of Self-Efficacy on the Relationship Between Perceived Social Support and Resilience in Patients with Recurrent Schizophrenia in China
Authors Wang LY ![]() , Li MZ, Jiang XJ, Han Y
, Li MZ, Jiang XJ, Han Y ![]() , Liu J, Xiang TT
, Liu J, Xiang TT ![]() , Zhu ZM
, Zhu ZM ![]()
Received 30 March 2022
Accepted for publication 28 June 2022
Published 1 July 2022 Volume 2022:18 Pages 1299—1308
DOI https://doi.org/10.2147/NDT.S368695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jun Chen
Video abstract presented by Liyi Wang.
Views: 164
Li-Yi Wang,1 Mei-Zhi Li,2 Xiao-Jian Jiang,1 Yang Han,3 Juan Liu,4 Ting-Ting Xiang,1 Zheng-Min Zhu1
1College of Nursing, Hunan University of Chinese Medicine, Changsha, Hunan, People’s Republic of China; 2Department of Nursing, Hunan Provincial Brain Hospital, Changsha, Hunan, People’s Republic of China; 3College of Civil Engineering, Central South University, Changsha, Hunan, People’s Republic of China; 4College of Basic Medicine, Ningxia Medical University, Yinchuang, Ningxia, People’s Republic of China
Correspondence: Xiao-Jian Jiang, College of Nursing, Hunan University of Chinese Medicine, Changsha, Hunan, 410208, People’s Republic of China, Tel +86 14781276032, Email [email protected] Yang Han, College of Civil Engineering, Central South University, Changsha, Hunan, 410075, People’s Republic of China, Tel +86 15111314076, Email [email protected]
Purpose: To explore the mediating effect of self-efficacy on the relationship between perceived social support and resilience in patients with recurrent schizophrenia in China.
Patients and Methods: In this cross-sectional study, a total of 176 patients with recurrent schizophrenia who were hospitalized in a tertiary hospital in Hunan Province, China, completed a general data questionnaire, the Connor Davidson Resilience Scale (CD-RISC), the Perceived Social Support Scale (PSSS) and the General Self-Efficacy Energy Scale (GSES).
Results: Among the 176 patients, the mean GSES score was 2.02± 0.61, the mean PSSS score was 56.77± 14.61, and the mean CD-RISC score was 58.06± 17.26. Self-efficacy played a partial mediating role between social support and resilience, and the mediating effect accounted for 42.56% of the total effect.
Conclusion: The resilience level of patients with recurrent schizophrenia in China is moderate and needs to be improved. This research revealed that self-efficacy played a part in mediating perceived social support and resilience in patients with recurrent schizophrenia in China. Perceived social support can indirectly affect resilience in patients with recurrent schizophrenia through self-efficacy. Comprehensive interventions in perceived social support and self-efficacy would help to improve the resilience of patients with recurrent schizophrenia.
Keywords: recurrent schizophrenia, perceived social support, self-efficacy, resilience, mediating effect
Introduction
The recurrence of schizophrenia in China is a serious concern. A study found that the recurrence rate of schizophrenia among patients in China was 41.3% one year after discharge, and the average recurrence time was 6.02 months.1 The recurrence rate within six months after discharge was as high as 1/3.2 Abroad, Nadeem3 found that the vast majority of schizophrenic patients will relapse within two years, and only 16.6% will not relapse within 10–15 years. The recurrence rate in schizophrenia patients with a first attack in China was found to be more than 80% in five years, which is much higher than that in other countries.4 Studies have shown that the economic burden of patients with recurrent schizophrenia is four times higher than that of patients without recurrent schizophrenia.5 The high recurrence rate leads to irreversible brain damage in patients and causes an enormous economic burden to families and society. At present, research on factors related to schizophrenia recurrence in China is in the initial stage, and there are few studies performing in-depth analyses of the relationships between various factors. Factors related to recurrence have not been clarified thus far and recurrence may be affected by many factors, such as heredity, environment, society, psychology and physiology.6 Many studies have shown that coping styles,7 resilience,8 self-efficacy,9 social support and negative life events affect schizophrenia relapse, and domestic research10,11 has shown lower efficacy, poor social support and lower resilience in persons with schizophrenia in China.
The American Psychological Association defines resilience as a process of adaptation to adversity, trauma, threats or major sources of stress.12 Richardson13 proposed the resilience process model theory, which states that after individuals experience the influence of risk factors, the physical system will carry out functional reorganization so that the biological psychological nervous system will reach a higher level and reshape the self-protection mechanism. Therefore, resilience is an important protective factor. Relevant studies have shown that paying attention to the development of resilience in patients with schizophrenia is conducive to exploring support resources in the process of rehabilitation and supporting the transformation from defect orientation to resource orientation from the perspective of mental illness.14 Abroad, Gooding PA15 proposed improving resilience, which could allow patients to resist negative ideas and impulses, such as self-injury or suicide, and highlighted external factors that supported resilience, including social support, reciprocity and religious coping. He16 suggested that cognitive performance and a high level of resilience are positively correlated and that improving resilience can improve cognitive function. Cognitive impairment is a core feature of schizophrenia. Yeo17 proposed that a higher level of resilience was associated with a lower severity of specific symptomatology, including positive symptoms, negative symptoms, depressive symptoms, suicidal ideation, cognitive deficits, and better insight. Therefore, positive psychological tolerance and coping ability can be obtained by improving the resilience of patients with recurrent schizophrenia. The determinants of resilience include biological, psychological, social and cultural factors that interact in complex ways.18,19 Abroad, Sedić20 found that low resilience levels in individuals at clinical high risk for psychosis and schizophrenia and a higher level of resilience were associated with better social functioning and less severe negative, anxiety and depressive symptoms. Evidence also suggests that the presence of resilience in individuals with schizophrenia-spectrum disorders is associated with improved psychosocial functioning.21 Guo22 and Izydorczyk23 showed that schizophrenia patients with higher resilience and optimism show higher levels of happiness and self-efficacy, which in turn are associated with lower perceived stress and higher personal control. Therefore, improving the level of resilience has a positive effect on patients with recurrent schizophrenia.
Perceived social support is an individual’s subjective perception and evaluation of external support.24 Relevant evidence shows that the perceived social support of patients with recurrent schizophrenia in China has a positive protective effect on resilience, is significantly positively correlated with resilience and has a positive effect on the perception and prediction of an individual’s mental health.25 Perceived social support can effectively regulate an individual’s psychological pressure and promote the development of their physical and mental health.
Self-efficacy is an individual’s perception of and belief about his or her ability to take action and to cope with various environmental challenges; it refers to a relatively stable ability or self-confidence in general.26 Self-efficacy was significantly positively correlated with optimism and resilience. Optimism was significantly positively correlated with resilience and its dimensions. The two dimensions of “social support” and “positive cognition” in resilience could significantly predict the self-efficacy of schizophrenic patients.27 Therefore, resilience and self-efficacy influence each other in patients with schizophrenia. Domestic evidence shows that the level of self-efficacy in patients with recurrent schizophrenia is low, which needs to be improved.28 Conner29 found that the higher the perception and understanding of social support was, the higher an individual’s self-efficacy. High level of social support helps to ensure good and positive psychological situation and physical and mental experience of patients with schizophrenia, and brings individual satisfaction, pleasure, self-confidence and comfortable living conditions.30 Therefore, improving the level of perceived social support can effectively improve the level of self-efficacy.
Given the associations among self-efficacy, perceived social support and resilience found in separate studies among patients with recurrent schizophrenia, we hypothesized that self-efficacy might mediate the relationship between perceived social support and resilience. To the best of our knowledge, this hypothesis has not been empirically examined. At the same time, the resilience level of patients with recurrent schizophrenia in China have not been fully explored in existing studies. Therefore, this study aimed to explore (1) the level of resilience in patients with recurrent schizophrenia in China; (2) the correlation between perceived social support and resilience in patients with recurrent schizophrenia; and (3) the mediating effect of self-efficacy on the relationship between perceived social support and resilience in patients with recurrent schizophrenia. This study provides a theoretical basis for improving the resilience level of patients with recurrent schizophrenia.
Materials and Methods
Study Design and Participants
From July to December 2021, We conducted a cross-sectional survey of patients with recurrent schizophrenia from a tertiary hospital in Hunan Province, China, through cluster sampling. In this survey, the inclusion criteria included the following: (1) native Chinese speakers; (2) patients with schizophrenia diagnosed by the CCMD-3 or ICD-10;28 (3) patients who met the clinical remission criteria according to the Positive and Negative Mental Symptom Scale (PANSS),31 including scores of mild or below (≤3 points) for at least six months for delusions, conceptual disorganization, hallucinations, emotional withdrawal, passive/apathetic social withdrawal, a lack of spontaneity and flow of conversation, mannerisms and posturing, and stereotyped thinking; (4) Having patients with past history of recurrence of acute psychosis: the recurrence criteria were a PANSS total score that increased by >25%, a Clinical Global Impression (CGI)32 score ≥6 (significantly deteriorated) and experiencing serious self-injury or destruction and obvious suicidal cognition for >1 week; (5) patients who were hospitalized ≥2 times; (6) patients with a stable state of mind; and (7) patients who were able to understand the survey’s content. The exclusion criteria included (1) patients with severe physical diseases or organic brain lesions and (2) patients with intellectual disabilities who could not communicate normally. Complete and logical questionnaires were considered valid. Ultimately, 10 questionnaires were incomplete, 7 were not logical, 4 were vague and 3 were lost. A total of 176 patients who met the criteria completed valid questionnaires, resulting in an effective response rate of 88%.
Procedure
Each participant completed a questionnaire within 20 minutes; the questionnaire included a table collecting general information and evaluations of perceived social support, self-efficacy and resilience. The researchers developed unified questionnaire guidance and training for designated nursing staff in each department before issuing the questionnaire language. The integrity of each questionnaire was examined, and the questionnaires were immediately recovered after evaluation. Clinical disease information was obtained through accessing the medical records system. Participants voluntarily participated in the study and signed informed consent forms. This study was approved by the Hospital Ethics Committee (K2019011).
Measures
General Information
The table collecting general information included two dimensions: (1) demographic information of patients with recurrent schizophrenia, including age, sex (male, female), education level, monthly income, marital status, and occupation, and (2) disease information, including the disease course, onset age, number of hospitalizations, and medications.
General Self-Efficacy Scale (GSES)
Developed by Schwarzer, German scholar and revised by Wang Caikang.33 It is used to measure the overall self-confidence of individuals when dealing with different environmental challenges or new things. It contains 10 items rated on a 4-point Likert scale, ranging from 1 (not at all true) to 4 (very true). The scores of all items are summed and divided by 10 to calculate the standardized score, with a higher standardized score indicating stronger self-efficacy. The Cronbach’s alpha was 0.927 in the current sample, which indicates good reliability.
Perceived Social Support Scale (PSSS)
The Perceived Social Support Scale was compiled by Zimet34 and translated by Xiao Shuiyuan.34 It is used to emphasize an individual’s self-understanding and self-feeling. It contains 12 items that address the three dimensions of family support, friend support and other support and uses 7 levels, ranging from 1 (strongly disagree)~7 (strongly agree). Total scores range from 12~84, with scores of 12~36 indicating low-level perceived social support, 37~60 indicating medium-level perceived social support, and 61~84 indicating high-level perceived social support. The Cronbach’s α coefficient was 0.898.
Connor Davidson Resilience Scale (CD–RISC)
This scale was compiled by Connor and Davidson; it is used to evaluate an individual’s resilience.35 The Chinese version of the scale was translated and revised by Xiao Nan and Zhang Jianxin in 2007.36 This study adopts the Chinese version of the scale. It contains 25 items that address the three dimensions of strength, tenacity and optimism that are rated on a five-point Likert scale, ranging from 0 (never) ~4 (always). A score of 0~35 points represents a low level of resilience, 36~64 points represents a medium level, and 65~100 points represents a high level. The Cronbach’s α coefficient was 0.89.
Data Analysis
All statistical analyses were performed using SPSS 22.0. Count data are expressed as relative numbers. Measurement data are expressed as ( ). Pearson’s correlation was conducted to analyze the relationship among perceived social support, self-efficacy and resilience in patients with recurrent schizophrenia. The bootstrap program plug-in of the Process operation macro compiled by Preacher and Hayes37 was used to test the mediating effect of self-efficacy in the relationship between social perceived support and resilience. The test level was α = 0.05.
). Pearson’s correlation was conducted to analyze the relationship among perceived social support, self-efficacy and resilience in patients with recurrent schizophrenia. The bootstrap program plug-in of the Process operation macro compiled by Preacher and Hayes37 was used to test the mediating effect of self-efficacy in the relationship between social perceived support and resilience. The test level was α = 0.05.
Results
Demographic and Disease Information of Patients with Recurrent Schizophrenia
Among the 176 patients with recurrent schizophrenia, the age range was 14 to 62 years (mean=29.92 years, SD=11.22); ninety-five were male (54.1%), and eighty-one were female (45.9%). The majority of patients (75.6%) were without spouses; nearly two-thirds had an education level (61.3%) of high school and below. Eighty-four patients were unemployed (47.9%); nearly two-thirds of the patients (63.3%) were living in urban areas, and one-third (36.7%) were living in rural areas. The per capita monthly income was as follows: < 1000 yuan (12%), 1000 yuan~2999 yuan (43.8%), 3000 yuan~4999 yuan (30%), ≥5000 yuan (14.2%).
The median number of hospitalizations was 2.0, and the median disease duration was 5.0 years. Sixty-one patients had other diseases (34.7%), and nearly two-thirds (65.3%) had no complications; three-fourths of the patients received combined medications (88%).
Correlation Analysis of Self-Efficacy, Perceived Social Support and Resilience of Patients with Recurrent Schizophrenia
The correlations among the continuous variables are shown in Table 1. There were significant correlations between perceived social support, self-efficacy and resilience among patients with recurrent schizophrenia. Specifically, there was a strong and significant positive relationship between perceived social support and self-efficacy (r=0.273, p=0.01). There was a strong and significant positive relationship between self-efficacy and resilience (r=0.634, p=0.01). There was a positive relationship between perceived social support and resilience (r=0.470, p=0.05).
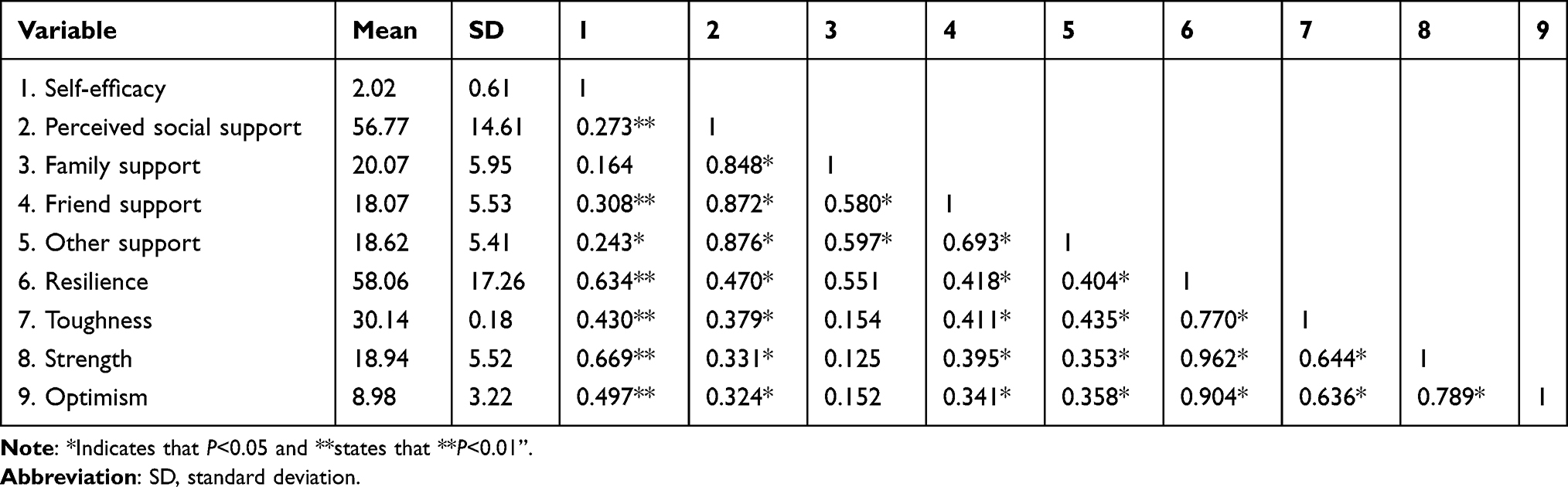 |
Table 1 Correlation Analysis of Self-Efficacy, Perceived Social Support and Resilience of Patients with Recurrent Schizophrenia (r) |
Mediating Effect of Self-Efficacy on the Relationship Between Perceived Social Support and Resilience in Patients with Recurrent Schizophrenia
The study examined the correlations among self-efficacy, perceived social support and resilience of patients with recurrent schizophrenia. The Process plug-in was selected to analyze the mediating effect of self-efficacy on the relationship between perceived social support and resilience in patients with recurrent schizophrenia. The perceived social support of patients with recurrent schizophrenia was taken as the independent variable, self-efficacy as the mediating variable, and resilience as the dependent variable; 5000 bootstrap samples and 95% confidence intervals (95% CIs) were selected.
The results showed that perceived social support had a positive predictive effect on resilience in patients with recurrent schizophrenia (β=0.438, P<0.001). Perceived social support positively predicted self-efficacy (β=0.115, P<0.001). Self-efficacy played a partial mediating role between perceived social support and resilience, suggesting that the partial effect of perceived social support on the resilience of schizophrenic patients was derived from the influence of self-efficacy. The value of the mediating effect was 0.186, accounting for 42.56% of the total effect, as shown in Table 2. The mediation model is shown in Figure 1.
 |
Table 2 Mediating Effect of Self-Efficacy on the Relationship Between Perceived Social Support and Resilience in Patients with Recurrent Schizophrenia |
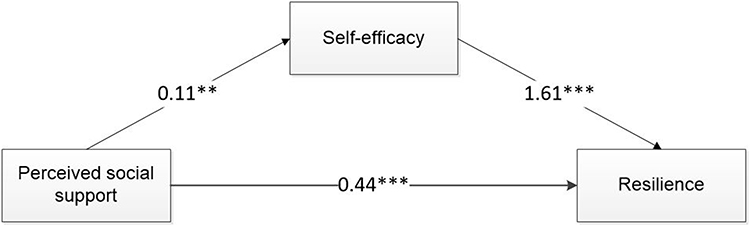 |
Figure 1 A mediation model of the role of self-efficacy in the relationship between perceived social support and resilience in patients with recurrent schizophrenia. Note: **Indicates that P<0.01 and ***states that P<0.001”. |
Discussion
Analysis of Perceived Social Support, Self-Efficacy and Resilience in Patients with Recurrent Schizophrenia
The perceived social support score in this study (mean=56.77, SD=14.61) was moderate, similar to the results of Xia Pinzhen.38 And the perceived social support score of rural patients with schizophrenia is lower than that of urban patients, which is consistent with the results of Yu.39 The analysis is due to low income in rural areas, poverty, family members of patients pay more attention to family livelihoods, ignoring the care of patients. Among the three dimensions of perceived social support, family support scored the highest, followed by friend support and, finally, by other support. This shows that the majority of patients receive material and emotional support from their own families and that they received less psychological support from their friends, leaders, colleagues and medical staff. The reason for this is that the majority of patients experience multiple recurrences during the course of the disease, and recurrence is a serious event that changes the trajectory of the disease. The quality of life of patients is significantly impaired, and social and work participation is reduced. At this time, patients are particularly dependent on material, spiritual and psychological support from their families. In addition, Fan40 suggests the social support could reduce the severity of psychotic symptoms. Cheng41 also proposed the peer co-delivered vocational rehabilitation services may enhance the social support received by persons with schizophrenia and improve their occupational outcomes. The peer co-delivered belongs to friend support in perceived social support. Therefore, it is suggested that family and friend participation in nursing care be increased and the utilization of social support for patients be improved so that close family and friend relationships can help patients recover, enable them to perceive effective emotional and social support, and improve their level of perceived social support.
The self-efficacy score in this study (mean=2.02, SD=0.61) was slightly lower than that of the relevant survey results.42 The reason is that patients with recurrent hospitalization are influenced by various factors, such as a lack of entertainment, changes to their environment, greatly limited living space, and fear of communication with people; due to repeated recurrences, these factors not only seriously impact a patient’s self-confidence in rehabilitation but also may cause them to stop treatment. In addition, fifty-one patients in this study were hospitalized ≥5 times (28%), indicating a high frequency of recurrence; four-fifths of the patients had a disease duration ≥2 years (80%), and the longer the duration was, the lower the patient’s confidence in active rehabilitation and the poorer his or her treatment compliance. Previous studies have pointed out that the disease duration and number of hospitalizations are negatively correlated with self-efficacy; therefore, in this survey, the overall self-efficacy of the patients with recurrent schizophrenia was low. It is suggested that medical staff should frequently evaluate patients’ general self-efficacy levels and its influencing factors and formulate individualized nursing interventions according to the specific situation of patients to improve their levels of self-efficacy.
The total score of resilience in this study (mean=50.06, SD=17.26), which was at a moderate level, was lower than that of the relevant research results28 (mean=60.71, SD=16.52). It has been reported42 that being married and being a parent/guardian are the influencing factors of the resilience scale, while sex, work and medication use are the influencing factors of the optimism score on the resilience scale. An analysis of the reasons for this revealed that nearly four-fifths of the hospitalized patients with recurrent schizophrenia did not have a spouse (75.6%), suggesting impaired resilience; in addition, nearly fifty percent (47.9%) of the patients were unemployed. One-fifth of the patients (12%) were treated with a single medication, while four-fifths (88%) were treated with combined medications, suggesting that their resilience and optimism were impaired. Resilience is the ability to physically rebound in the face of difficult experiences. Patients cannot participate in work normally and have substantial psychological responsibilities. In addition, confounding factors such as lack of family support, psychiatric history, living place and long-term effects of psychotropic medication lead to a decrease in the psychological endurance of patients with recurrence and failure to rebound from mental trauma. Therefore, it is suggested that not only should family support be strengthened and that there should be interventions for adverse medication reactions but also that the resilience level of patients with recurrence be frequently evaluated and that targeted intervention measures be taken.
Correlation Analysis of Perceived Social Support, Self-Efficacy and Psychological Resilience in Patients with Recurrent Schizophrenia
Correlation analysis showed that the total score of perceived social support was positively correlated with the total score of resilience in patients with recurrent schizophrenia (r= 0.470, P<0.01). Wang43 also proposed some preliminary evidence of associations between perceived social support and outcomes in schizophrenia, bipolar disorder and anxiety disorders. Family support and friend support were highly correlated (r=0.551, r=0.418, P<0.01), indicating that the higher the family and friend support of patients with recurrent schizophrenia was, the higher the level of resilience. There was a significant positive correlation between the self-efficacy score and resilience score (r=0.634, P<0.01), which was consistent with the results of Liu Dongwei.44 Kong45 suggests that resilience played a partial mediating role in the relationship between perceived social support and health self-efficacy among migrant older adults, Compared with my research results, it is found that self-efficacy and resilience are significantly correlated, and they are mutually causal, that is, the higher the level of self-efficacy is, the higher the level of resilience is, and high resilience will also improve the level of self-efficacy. Reasons analysed that schizophrenia patients with higher self-efficacy levels were more aware of their individual value in the face of negative events, and they were able to obtain a sense of control and autonomy of the external environment in a timely manner, which promoted their ability to transform difficulties from diseases into experience resources and enhanced their stress resistance and resilience. Therefore, the correlation among these factors suggests that mental hospitals and other medical and health institutions should improve resilience for patients with recurrent schizophrenia by actively intervening their perceived social support and self-efficacy.
Self-Efficacy Plays a Partial Mediating Role Between Perceived Social Support and Resilience
Self-efficacy16 is an overall relatively stable sense of competence or self-confidence that individuals show in coping with challenges in various environments. Zhou46 indicated that self-efficacy and motivation may act as mediators in the relationship between neurocognition and self-management in schizophrenia. It is consistent with our research results that self-efficacy plays a mediating role in schizophrenia. This study showed that after adding self-efficacy, the effect of perceived social support on the resilience of patients with recurrent schizophrenia was still significant, indicating that perceived social support can indirectly affect the resilience of patients with recurrent schizophrenia through self-efficacy. Self-efficacy was an intermediary variable between perceived social support and resilience, and the mediating effect was 42.56%. The reason for this is that, on the one hand, the social support of patients with recurrent schizophrenia is a favorable factor for improving their self-efficacy levels; that is, the more social support a patient receives, the higher their self-efficacy level. The lack of family warmth in patients with recurrent schizophrenia makes them vulnerable to helplessness, loneliness and loss of confidence in life. Perceived social support from peers, relatives and friends can buffer the adverse effects of negative factors.42 The better a patient’s self-efficacy is, the more active his or her social life and the wider his or her social support.
On the other hand, self-efficacy can affect resilience through positive coping, indicating that patients with recurrent schizophrenia with high self-efficacy tend to adopt positive coping and thus improve their resilience. A higher level of self-efficacy can make individuals more effectively perceive the positive components of self-personality and adopt a positive perspective in the face of disease to enhance their internalized stress resistance and resilience.47 This is consistent with Lee48 research results, indicating that emotional discomfort will reduce self-efficacy, and low self-efficacy will also lead to negative emotions, thereby reducing resilience. Therefore, it is suggested that strong continuous psychological support mechanisms be formed among hospitals, communities and families and that the self-efficacy levels of patients be continuously improved. Intervention measures such as the focus solution model, traditional Chinese material methods and stress management based on commitment therapy (ACT)49–52 can effectively improve patients’ perceived social support and self-efficacy, thereby improving the level of resilience and the quality of life of patients with recurrent schizophrenia.
In addition, this study found that self-efficacy was not a complete mediator between perceived social support and resilience in patients with recurrent schizophrenia and indicated that other influencing factors need to be further explored. Future research should include more mediating variables, explore the path of action between mediating variables, and more clearly reveal the multiple mediating mechanisms of perceived social support affecting resilience, so as to provide a theoretical basis for clinical intervention path.
However, there are several limitations in the current research. First, we only selected patients with recurrent schizophrenia who were hospitalized in a tertiary hospital in Hunan Province, China. Therefore, the extent to other groups need further research to confirm. Finally, the sample source was limited; in the future, researchers can increase the sample size and conduct research analysis in multiple centers and from multiple angles.
Conclusion
The resilience level of patients with recurrent schizophrenia in China is moderate and needs to be improved. This research revealed that self-efficacy played a part in mediating perceived social support and resilience in patients with recurrent schizophrenia in China. Perceived social support can indirectly affect resilience in patients with recurrent schizophrenia through self-efficacy. Comprehensive interventions in perceived social support and self-efficacy would help to improve the resilience of patients with recurrent schizophrenia.
Data Sharing Statement
We cannot disclose the data because of the particularity of the survey population. To obtain the data, please contact the corresponding author.
Ethics Statement
This study complies with the Declaration of Helsinki. All participants and their families fully understood the protocol of all questionnaires before registration, according to the principle of voluntary participation and anonymity, and signed written informed consent forms for this study. The research was reviewed by the Medical Ethics Committee of Hunan Provincial Brain Hospital, and the ethical number is K2019011.
Funding
This study was supported by the Key Research and Development Program of Ningxia Hui Autonomous Region (Special Project for Foreign Scientific and Technological Cooperation) (Grant no. 2019BFG02023); the project funded by the 2021 Scientific Research of Hunan Health Commission (Grant no. 202114052222); and the projects funded by Hunan Innovative Province Construction Special Funding (Grant no. 2021 SK2009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hongwei L, Liang M, Zhang C, et al. Validity and reliability test of schizophrenia recurrence risk scale. Chin J Mental Health. 2020;34(03):181–185.
2. Zhengyu S, Weiyun X, Zuo W, et al. Prediction validity evaluation of schizophrenia recurrence precursor scale. Neurol Dis Mental Health. 2021;21(12):850–854.
3. Nadeem Z, Mc Intosh A, Lawrie S. Schizophrenia. Evid Based Ment Health. 2004;7(1):2–3. doi:10.1136/ebmh.7.1.2
4. Weiyun X, Zuo W, Rongjie M, et al. The introduction and cultural debugging of the schizophrenia recurrence precursor scale. Clin J Psychiatry. 2018;28(4):237–240.
5. Pennington M, McCrone P. The cost of relapse in schizophrenia. Pharmacoeconomics. 2017;35(9):921–936. doi:10.1007/s40273-017-0515-3
6. Xiaolian W, Wanwen W, Zhuwan W. The study of individual resilience training on the prevention of relapse in patients with schizophrenia in community. Chin Med Innovation. 2021;18(32):99–103.
7. Jingqun W, Zixuan C, Qinghua W, et al. The relationship between psychological competence and mental health: a Chain mediator of perceived social support and resilience. Psychol Explor. 2021;41(02):176–185.
8. Xin C, Hua H. Research progress of resilience in patients with schizophrenia. Lab Med Clin. 2019;16(02):264–266.
9. Hongmei Z, Zhansheng Z, Zhigang S, et al. The risk factor of relapse on patients with schizophrenia. J Int Psychiatry. 2017;44(03):
10. Shengxia Z, Liang L, Zhenjuan L. The characteristics of recovery and its influencing factors in long-term treatment of children with schizophrenia. J Nurs PLA. 2018;35(21):6–10.
11. Hui Y, Yufei Y, Guiping P, et al. Effect of intrinsic cognitive therapy with musical memory on coping styles of female patients with chronic schizophrenia. J Rehabil Theory Pract. 2022;28(3):350–355.
12. Steven MS, Dennis SC. The science of resilience: implications for the prevention and treatment of depression. Science. 2012;338(6103):79–82. doi:10.1126/science.1222942
13. Richardson AK, Katsuki A, Katsuki A, Yoshimura R. Effects of the number of hospitalizations on cognitive function in Japanese patients with stable schizophrenia [published online ahead of print, 2020 Sep 4]. CNS Spectr. 2020;26:1–6.
14. Weiwei Y, Shuai G, Rufang Z, et al. Investigation and analysis of psychological resilience and influencing factors in patients with stable schizophrenia. Qilu Nurs J. 2018;24(23):45–48.
15. Gooding PA, Littlewood D, Owen R, Johnson J, Tarrier N. Psychological resilience in people experiencing schizophrenia and suicidal thoughts and behaviours. J Ment Health. 2019;28(6):597–603. doi:10.1080/09638237.2017.1294742
16. He Q, Jantac Mam-Lam-Fook C, Chaignaud J, et al. Influence of polygenic risk scores for schizophrenia and resilience on the cognition of individuals at-risk for psychosis. Transl Psychiatry. 2021;11(1):518. doi:10.1038/s41398-021-01624-z
17. Yeo JJ, Chew QH, Sim K. Resilience and its inter-relationship with symptomatology, illness course, psychosocial functioning, and mediational roles in schizophrenia: a systematic review. Asia Pac Psychiatry. 2022;14(2):e12486. doi:10.1111/appy.12486
18. Dongwei L, Xinghua R, Yuqiu Z, et al. Reliability and validity of Chinese version of Resilience Scale in patients with schizophrenia. Chin J Pract Nurs. 2020;36(18):1366–1371.
19. Boxin C, Xiafang J, Huanqin Z, et al. The influencing factors of mental resilience in hospitalized patients with schizophrenia in stable period. Zhongguokang med. 2021;33(4):74–78.
20. Sedić B, Štrkalj Ivezić S, Petrak O, et al. Differences in resilience, self-stigma and mental health recovery between patients with schizophrenia and depression. Psychiatr Danub. 2021;33(Suppl 4):518–528.
21. Wambua GN, Kilian S, Ntlantsana V, et al. The association between resilience and psychosocial functioning in schizophrenia: a systematic review and meta-analysis. Psychiatry Res. 2020;293:113374. doi:10.1016/j.psychres.2020.113374
22. Guo S, He N, Liu Z, et al. Brain-wide functional dysconnectivity in schizophrenia: parsing diathesis, resilience, and the effects of clinical expression. Can J Psychiatry. 2020;65(1):21–29. doi:10.1177/0706743719890174
23. Izydorczyk B, Sitnik-Warchulska K, Kühn-Dymecka A, et al. Resilience, sense of coherence, and coping with stress as predictors of psychological well-being in the course of schizophrenia. The study design. Int J Environ Res Public Health. 2019;16(7):1266. doi:10.3390/ijerph16071266
24. Liting F, Ruixue M, Zhiguang F, et al. Understanding the impact of social support on sleep quality in the elderly: the mediating and moderating role of rumination. Chin J Gerontol. 2022;42(1):208–211.
25. Lök N, Bademli K. The relationship between the perceived social support and psychological resilience in caregivers of patients with schizophrenia. Community Ment Health J. 2021;57(2):387–391. doi:10.1007/s10597-020-00665-w
26. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
27. Yingying M, Dongwei L, Lina M, et al. Effect of stigma on loneliness in patients with schizophrenia: chain mediating effect of resilience and hope. China Health Administration. 2020;37(11):844–847.
28. Yunfei D, Zeping X. Comparison of Chinese classification and diagnostic criteria for mental disorders version 3 with international classification of diseases version 10. J Clin Psychiatry. 2013;23(6):426–427.
29. Vaskinn A, Ventura J, Andreassen OA, et al. A social path to functioning in schizophrenia: from social self-efficacy through negative symptoms to social functional capacity. Psychiatry Res. 2015;228(3):803–807. doi:10.1016/j.psychres.2015.05.019
30. Lilianna GJ, Lilian C. Effect of primipara self-efficacy and perceived social support on postpartum depression. Gen Nurs. 2021;19(03):302–305.
31. He YL, Zhang MY. Positive and Negative Syndrome Scale (PANSS) and its application. Clin J Psychiatry. 1997;7:35–37.
32. Correll CU, Davis RE, Weingart M, et al. Efficacy and safety of lumateperone for treatment of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2020;77(4):349–358. doi:10.1001/jamapsychiatry.2019.4379
33. Schwarzer R, Born A. Optimistic self-beliefs: assessment of general perceived self-efficacy in thirteen cultures. World Psychol. 1997;3(1/2):177–190.
34. Zimet GD, Dahlem NW, Zimet SG, et al. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
35. Conner M, Davidson RT. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anx. 2003;18(2):76–82. doi:10.1002/da.10113
36. Yu XN, Zhang JX. A comparison between the Chinese version of ego-resiliency scale and Connor-Davidson resilience scale. Psychol Sci. 2007;30(5):1169–1171.
37. Preacher KJ, Hayes AF. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav Res Methods Instrum Comput. 2004;36(4):717–731. doi:10.3758/BF03206553
38. Fanzhen X. Effect of holistic rehabilitation nursing on negative emotion and perceived social support in convalescent schizophrenic patients. China Higher Med Educ. 2017;03:145–146.
39. Yu YH, Peng MM, Bai X, et al. Schizophrenia, social support, caregiving burden and household poverty in rural China. Soc Psychiatry Psychiatr Epidemiol. 2020;55(12):1571–1580. doi:10.1007/s00127-020-01864-2
40. Fan CH, Hsu SC, Hsiao FH, et al. The association of social support and symptomatic remission among community-dwelling schizophrenia patients: a cross-sectional study. Int J Environ Res Public Health. 2021;18(8):3977. doi:10.3390/ijerph18083977
41. Cheng KY, Yen CF. The social support, mental health, psychiatric symptoms, and functioning of persons with schizophrenia participating in peer co-delivered vocational rehabilitation: a pilot study in Taiwan. BMC Psychiatry. 2021;21(1):268. doi:10.1186/s12888-021-03277-0
42. Aijun C, Changge P, Ruiling L, et al. The effect of focus-solving model on resilience and self-efficacy of hospitalized psychiatric patients during rehabilitation. Chin J Physician. 2021;23(01):110–113.
43. Wang J, Mann F, Lloyd-Evans B, et al. Associations between loneliness and perceived social support and outcomes of mental health problems: a systematic review. BMC Psychiatry. 2018;18(1):156. doi:10.1186/s12888-018-1736-5
44. Liu D, Zhou Y, Li G, et al. The factors associated with depression in schizophrenia patients: the role of self-efficacy, self-esteem, hope and resilience. Psychol Health Med. 2020;25(4):457–469. doi:10.1080/13548506.2019.1695862
45. Kong LN, Zhu WF, Hu P, et al. Perceived social support, resilience and health self-efficacy among migrant older adults: a moderated mediation analysis. Geriatr Nurs. 2021;42(6):1577–1582. doi:10.1016/j.gerinurse.2021.10.021
46. Zhou C, Li Z. Modelling of self-management in schizophrenia: the role of neurocognition, self-efficacy and motivation. J Clin Nurs. 2020;29(21–22):3966–3976. doi:10.1111/jocn.15407
47. Boxin C, Xiafang J, Huanqin Z, et al. The influencing factors of mental resilience in hospitalized patients with schizophrenia in stable period. Chin Ming Kang Med. 2021;33(4):74–78.
48. Lee SJ, Lawrence R, Bryce S, et al. Emotional discomfort mediates the relationship between self-efficacy and subjective quality of life in people with schizophrenia. J Ment Health. 2021;30(1):20–26. doi:10.1080/09638237.2019.1581355
49. Xiaomin Z, Hequn L, Yiren W, et al. The level of self-efficacy and its influencing factors in tuberculosis patients. China J Infect Control. 2017;16(06):
50. Junyan W, Xiaowei X, Tong L, et al. Correlation between resilience and cognitive function in patients with first-episode schizophrenia. Chin Med J. 2021;101(37):3006–3011. doi:10.3760/cma.j.cn112137-20210203-00341
51. Wanling C, Guizhen Z, Yalan L. Effect of family and social support on quality of life in patients with schizophrenia. Health Vocational Educ. 2021;39(8):128–130.
52. Abu Sabra MA, Hamaideh SH, Hamdan-Mansour AM. Testing efficacy of relapse prevention intervention among patients diagnosed with schizophrenia in Jordan. Issues Ment Health Nurs. 2022;1–13. doi:10.1080/01612840.2022.2025634
53. Wang CK, Hu ZF, Liu Y. Research on reliability and validity of general self-efficacy scale. Appl Psychol. 2001;7(1):37–40.
54. Zuoji Z. Manual of Behavioral Medicine Scale [MCD]. Beijing: China Medical Electronic Audio-visual Press; 2005:156–158.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Mediating Effects of Resilience on Perceived Social Support and Fear of Cancer Recurrence in Glioma Patients
Zhong M, She F, Wang W, Ding L, Wang A
Psychology Research and Behavior Management 2022, 15:2027-2033
Published Date: 6 August 2022
Drug Attitude and Medication Adherence of Patients with Early Psychosis in South Korea: Mediating Effect of Medication Adherence Self-Efficacy
Choi YA, Kweon YR
Patient Preference and Adherence 2023, 17:1247-1255
Published Date: 12 May 2023
Path Analysis of Self-Efficacy, Coping Style and Resilience on Depression in Patients with Recurrent Schizophrenia
Wang L, Li M, Guan B, Zeng L, Li X, Jiang X
Neuropsychiatric Disease and Treatment 2023, 19:1901-1910
Published Date: 1 September 2023
Mediating and Suppressing Effects of Coping Styles Between Resilience and Empathy for Pain in Clinical Nurses: A Cross-Sectional Study
Huang Y, Li B, Feng S, Jiang S, Zeng K
Journal of Multidisciplinary Healthcare 2024, 17:4653-4667
Published Date: 7 October 2024
Trait Mindfulness, Resilience, Self-Efficacy, and Postpartum Depression: A Dominance Analysis and Serial-Multiple Mediation Model
Mei X, Mei R, Li Y, Yang F, Liang M, Chen Q, Ye Z
Psychology Research and Behavior Management 2025, 18:743-757
Published Date: 31 March 2025