")
Back to Journals » Journal of Pain Research » Volume 15
Meaning in Life and Pain: The Differential Effects of Coherence, Purpose, and Mattering on Pain Severity, Frequency, and the Development of Chronic Pain
Authors Boring BL , Maffly-Kipp J, Mathur VA , Hicks JA
Received 10 September 2021
Accepted for publication 5 January 2022
Published 3 February 2022 Volume 2022:15 Pages 299—314
DOI https://doi.org/10.2147/JPR.S338691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Brandon L Boring,1 Joseph Maffly-Kipp,1 Vani A Mathur,1,2 Joshua A Hicks1
1Department of Psychological and Brain Sciences, Texas A&M University, College Station, TX, 77843, USA; 2Institute for Neuroscience, Texas A&M University, College Station, TX, 77843, USA
Correspondence: Brandon L Boring
Department of Psychological and Brain Sciences, Texas A&M University, 4235 TAMU, College Station, TX, 77843, USA
, Email [email protected]
Objective: Meaning in life is consistently associated with better health outcomes across a range of mental and physical domains. However, meaning in life is a complex construct involving three distinct facets: coherence, purpose, and mattering. While these facets have been studied individually in relation to pain, they have not been assessed concurrently to parse out their potential distinct contributions to pain outcomes. We sought to identify the unique relationships of these individual facets of meaning with pain experiences and specify the components associated with pain-related resilience.
Methods: The associations of coherence, purpose, and mattering with pain outcomes were examined across three studies. Study 1 used data from the Midlife in the United States National Survey to determine associations between facets and the frequency of various recently experienced pains, and the development of chronic pain nine years later. Study 2 cross-sectionally observed the association between facets and recent pain severity in young adults. Using a diary-type approach, Study 3 captured fluctuations of pain severity in relation to the facets across the span of four weeks.
Results: Coherence was uniquely associated with less headache, backache, joint, and extremities pain frequency in Study 1, over and above purpose and mattering, controlling for other health variables. Coherence was also associated with lower odds of developing chronic pain. In Study 2, coherence was associated with less pain severity and fully mediated the relationship between global meaning in life and pain. Study 3 found that coherence predicted the most unique variance in weekly pain fluctuations.
Conclusion: Across three studies and timescales, coherence was uniquely associated with fewer and less severe pain experiences over and above purpose and mattering. These findings provide support for the value of coherence as a resilience factor in the context of pain and suggest a potential benefit for coherence-specific interventions in clinical settings.
Keywords: pain, coherence, purpose, mattering, meaning in life
Introduction
Meaning in life (MIL) fosters resilience and acceptance, and promotes improved health outcomes, particularly within the context of pain.1–3 Global reports of MIL are associated with better adjustment and well-being among people with chronic pain and less pain among those with breast cancer.4–6 However, multiple theoretical perspectives assert that MIL is multidimensional, comprising three interrelated facets – coherence (or comprehension), purpose, and mattering (or significance) – potentially complicating interpretation of this literature.7–13 Current consensus suggests that MIL is experienced when people are able to make sense of their lives (coherence), believe they are pursuing important goals (purpose), and feel that their lives matter to both themselves and the outside world (mattering). These three facets are distinguishable within MIL, yet the unique influence of each of these facets on pain has not been examined.7,11,13,14
Drawing on his experiences in concentration camps, Frankl (1959) asserted that the construction of meaning is a necessary step to transcending physical suffering.2 Current theoretical models build off Frankl’s ideas; for example, Park’s (2010) influential meaning-making model focuses on the importance of both situational and global meaning in one’s life, and how successful meaning making efforts (eg, finding a silver lining in a previously incomprehensible traumatic event) can influence global perceptions of MIL.1,3,11 Martela and Steger (2016) further suggest that researchers need to consider different facets or “meanings of meaning,” including purpose, coherence, and mattering, if they want to better understand how MIL influences psychological and physical health.7,15 However, in the existing literature, only two of these facets have been considered in relation to pain experiences, and they have been examined in isolation. Purpose, for example, predicts better recovery following knee surgery in people with knee osteoarthritis, as well as habituation to heat and cold pain in the laboratory.16,17 Studies suggest that coherence is associated with less bodily pain in older adults, less painful somatic complaints in adolescents, and lower pain catastrophizing in people with chronic pain; however, these have used a measure (the Sense of Coherence scale) that assesses perceived comprehension, manageability, and meaningfulness, and not specifically coherence per se as operationalized by MIL researchers, adding further confusion to understanding the impact of MIL on pain outcomes.13,14,18–22 Mattering itself has not been examined in the context of pain.
Disambiguation of these unique facets is essential for informing future work, especially in relation to clinical interventions for those suffering from pain. For example, acceptance-based interventions for chronic pain often aim to help people find meaning in their pain, but MIL is often used nonspecifically in these contexts.23,24 A more thorough understanding of the relationship between MIL and pain could inform therapeutic approaches that leverage the psychological benefits of one facet specifically, rather than a more general conceptualization of meaning. Empirical and theoretical exploration in this area may therefore allow for more targeted clinical efforts for the treatment of pain.
Within the present research, we concurrently assessed coherence, mattering, and purpose across a breadth of pain experiences over three separate studies. In Study 1, we cross-sectionally observed the association of the facets with the frequency of various types of recent acute pain, and longitudinally assessed whether the facets predicted the odds of developing chronic pain using an opensource dataset to establish an initial basis for subsequent studies. In Study 2, we cross-sectionally examined these constructs’ association with recent pain severity, and then built upon this in Study 3 by assessing their relationship longitudinally. As the independence of each facet of MIL has been demonstrated in other contexts and guided by George and Park’s (2016) framework, we hypothesized that coherence, purpose, and mattering would differentially relate to the frequency of acute pain (Study 1), the development of chronic pain (Study 1), and pain severity cross-sectionally (Study 2) and longitudinally (Study 3). Due to the exploratory nature of these analyses, there were no specific predictions regarding which facet would relate most strongly to pain outcomes.
Study 1 Method
Participants
Data were taken from Waves 2 (2004–2005) and 3 (2013–2014) of the Midlife in the United States (MIDUS), an opensource dataset.25,26 The MIDUS is an ongoing longitudinal study assessing sociodemographic, behavioral, and health data gathered through telephone surveys using random digit dialing and mailed questionnaires. Wave 2 of the MIDUS contained 4963 total participants. For cross-sectional analysis, after selecting only those who reported not having chronic pain at Wave 2, 2484 participants remained (53.7% female). Participants’ ages ranged from 30 to 83 years old (M = 55.10 ± 12.28). For cross-sectional analysis within Wave 3, after selecting only those who reported not having chronic pain, 1663 participants remained (53.3% female). Participants’ ages ranged from 42 to 92 years old (M = 64.03 ± 11.08).
For longitudinal analyses, we selected only those who reported not having chronic pain at Wave 2 and who had data for all variables of interest at both Waves 2 and 3, resulting in a total of 1511 participants (53.2% female). Participants’ ages at Wave 2 ranged from 30 to 83 years old (M = 54.79 ± 11.27). Demographic information on race, education, and marital status are reported in Table 1. This study protocol was submitted to the Texas A&M University Institutional Review Board, who determined that this secondary analysis of existing data was not human subjects research.
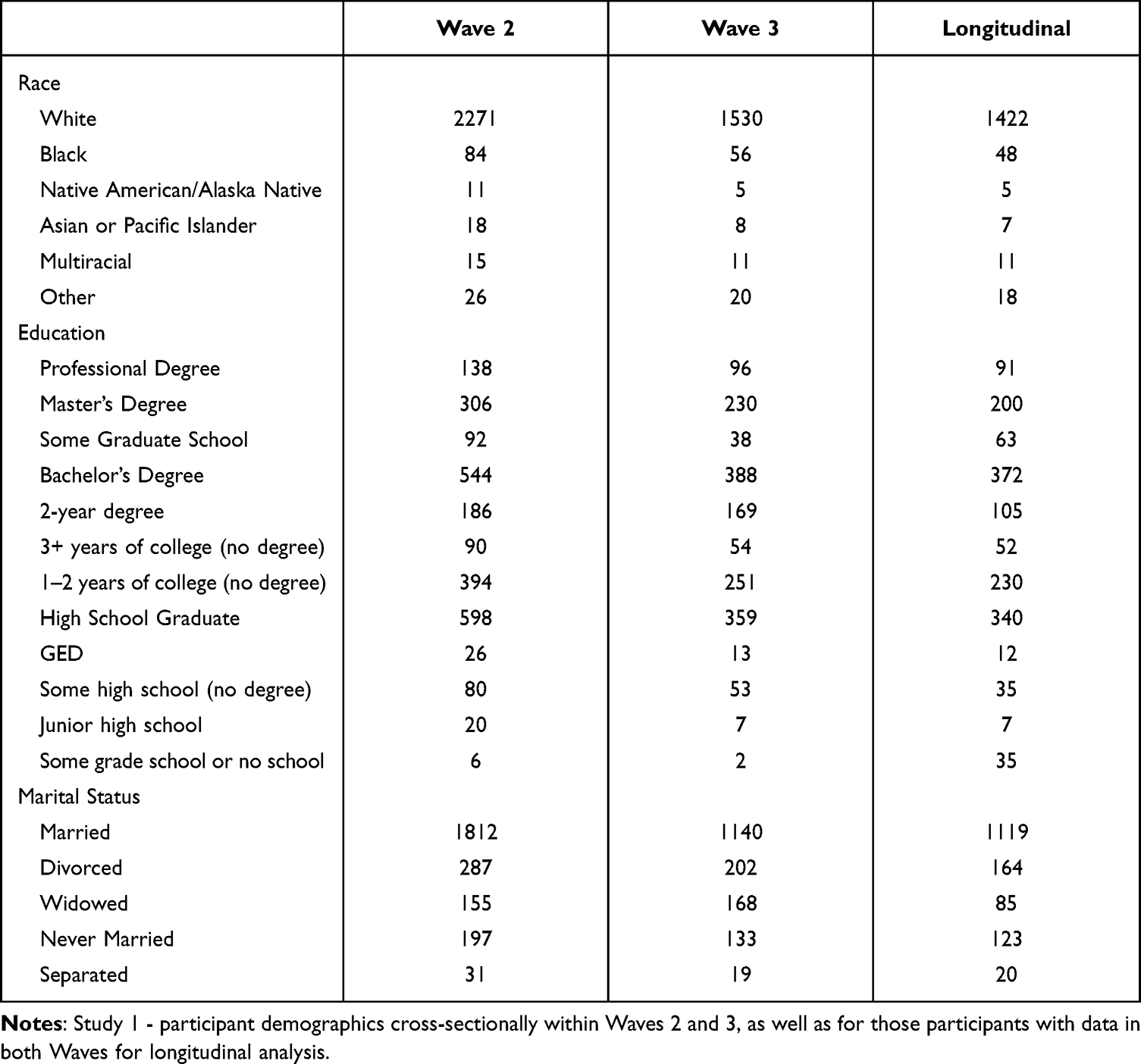 |
Table 1 Participant Demographics |
Measures
Chronic Pain
The presence of chronic pain was assessed using the question
Do you have chronic pain, that is do you have pain that persists beyond the time of normal healing and has lasted from anywhere from a few months to many years?
Participants answered “Yes” or “No”. Values were re-coded from the original MIDUS dataset so that odds ratios >1 would reflect increased odds of developing chronic pain (ie, “yes” = 2, and “no” = 1).
Pain Frequency
Participants were asked about the frequency with which they had experienced four types of pain (ie headaches, backaches, aches/joint stiffness, and extremities aches/pain) over the previous 30 days on a scale of 1 (almost every day) to 6 (not at all). These values were re-coded for analysis so that higher scores indicated more frequent instances of pain.
Coherence, Mattering, and Purpose
Coherence and mattering were measured using the Social Coherence and Social Contribution subscales of a social well-being measure.27 Participants were asked to describe the extent to which they agreed with two items for coherence (eg “I cannot make sense of what’s going on in the world”; α = 0.639) and three items for mattering (eg “I have nothing important to contribute to society”; α = 0.704) on a scale of 1 (strongly agree) to 7 (strongly disagree). Scores for each facet were calculated as the sum of their respective items, with higher scores indicating greater endorsement of each unique facet.
Purpose was measured using the purpose subscale of a psychological well-being measure.28,29 Participants indicated how much they agreed with seven items (eg “I don’t have a good sense of what it is I’m trying to accomplish in life”; α = 0.694) on a scale of 1 (strongly agree) to 7 (strongly disagree). Scores were calculated as the sum of the items, with higher scores indicating greater purpose.
Self-Evaluated Physical and Mental Health
Self-rated physical and mental health – “In general, would you say your [physical health/mental or emotional health] is excellent, very good, good, fair, or poor?” – were reported on a scale of 1 (excellent) to 5 (poor).
BMI
BMI was calculated within the MIDUS by dividing the participants’ self-reported weight (recorded in lbs. and converted to kilograms) from their self-reported height (recorded in inches and converted to meters squared).
Depression
Depression was calculated as the accumulated “Yes” responses to seven questions assessing both depressed affect (eg “During two weeks in the past 12 months, when you felt sad, blue or depressed, did you lose interest in most things?”) and anhedonia (eg “During two weeks in the past 12 months, when you lost interest in most things, did you have a lot more trouble concentrating than usual?”). Totals ranged from 0 to 7, with higher scores indicating greater depression.
Anxiety
Participants were asked how frequently they experienced 10 items (eg “How often over the past 12 months you were restless because of your worry”) using a scale of 1 (most days) to 4 (never). Anxiety scores were calculated as the total number of “most days” responses, where higher scores indicated greater anxiety.
Number of Chronic Conditions
Participants responded “Yes” or “No” to whether they had experienced 30 different chronic conditions (eg asthma, ulcers) in the past 12 months.
Analysis Plan
Analyses were conducted using SPSS (version 25; IBM Corp, Armonk, NY). Separate hierarchical linear regression analyses were conducted for the frequency of each acute pain within two separate Waves of the MIDUS. Demographics (ie chronological age, gender, race, education level, and marital status) were included in the first step of the regression, and covariates associated with physical and mental health (ie self-rated physical and mental/emotional health, BMI, depression, anxiety, and the number of other chronic conditions) were included in the second step, modeled after prior research on psychosocial predictors of pain using the MIDUS.30 Coherence, purpose, and mattering scores were added concurrently in the final step of the regression. After selecting only those participants without chronic pain at Wave 2, a logistic regression was then conducted to determine the independent predictive value of the facets of MIL on the development of chronic pain between Waves 2 and 3, over and above covariates.
Study 1 Results
Predictor and outcome variable descriptive statistics for cross-sectional analyses and for longitudinal analysis can be found in Table 2. Results of cross-sectional analyses within each Wave for headache, backache, joint pain, and extremities pain can be found in Table 3. Controlling for demographics and health variables, coherence was associated with less pain frequency for all domains within each Wave, excluding Wave 3 headaches (while not significant, trended in the same direction), whereas purpose was only associated with less frequent headaches and less frequent back pain in Wave 2 and with more frequent joint pain in Wave 3. Mattering was only associated with more frequent back pain in Wave 2.
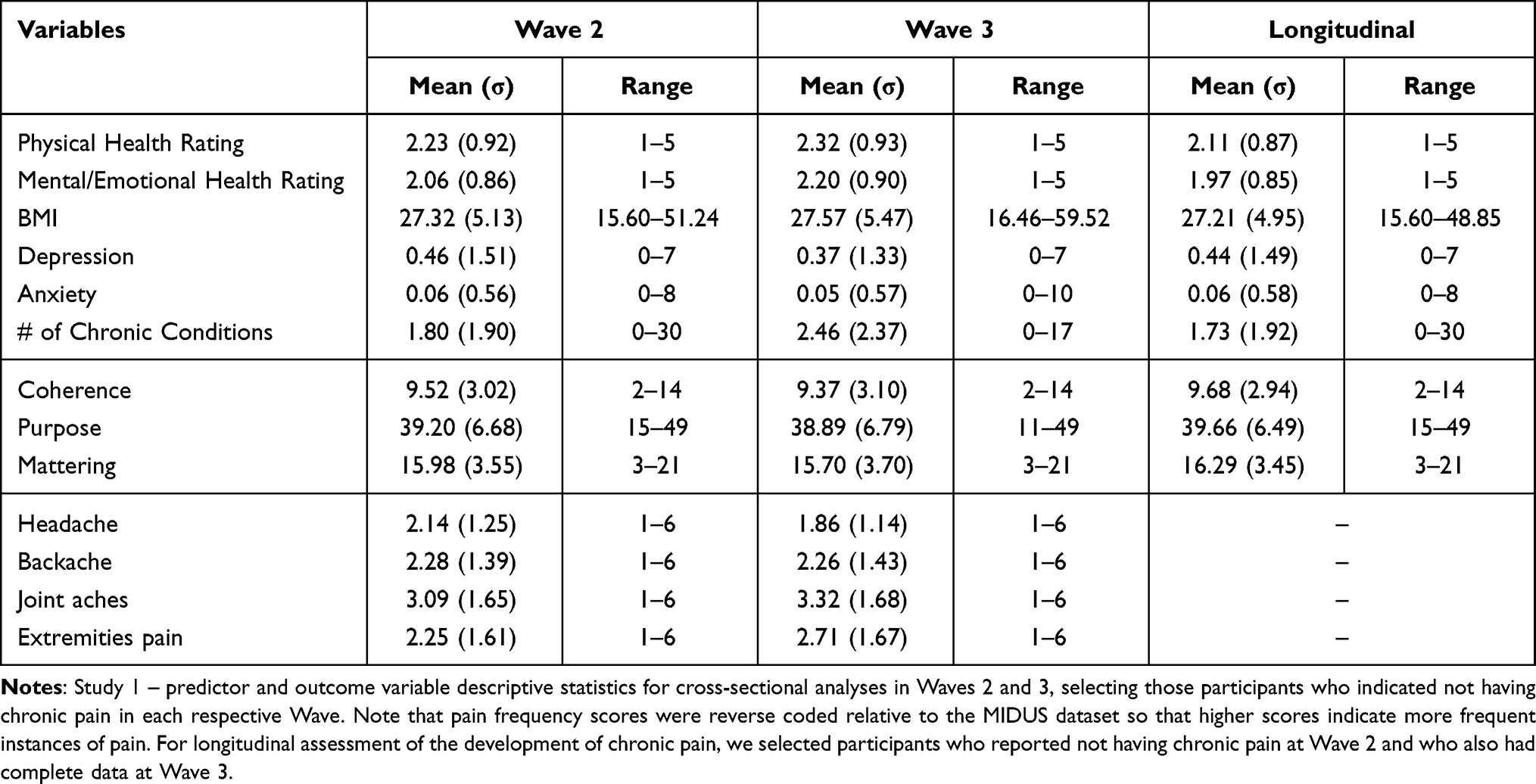 |
Table 2 Study 1 Variable Descriptive Statistics |
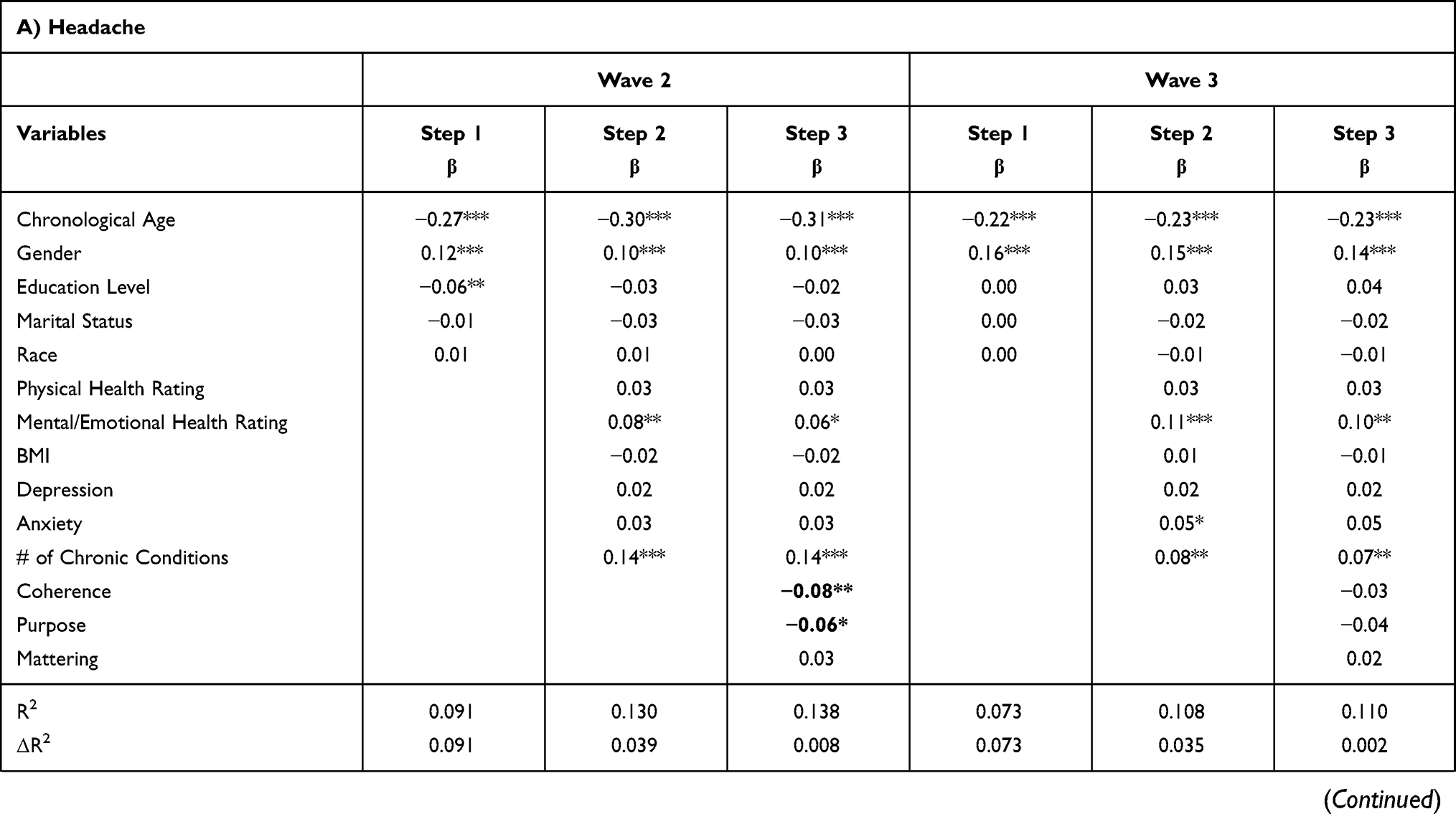 | 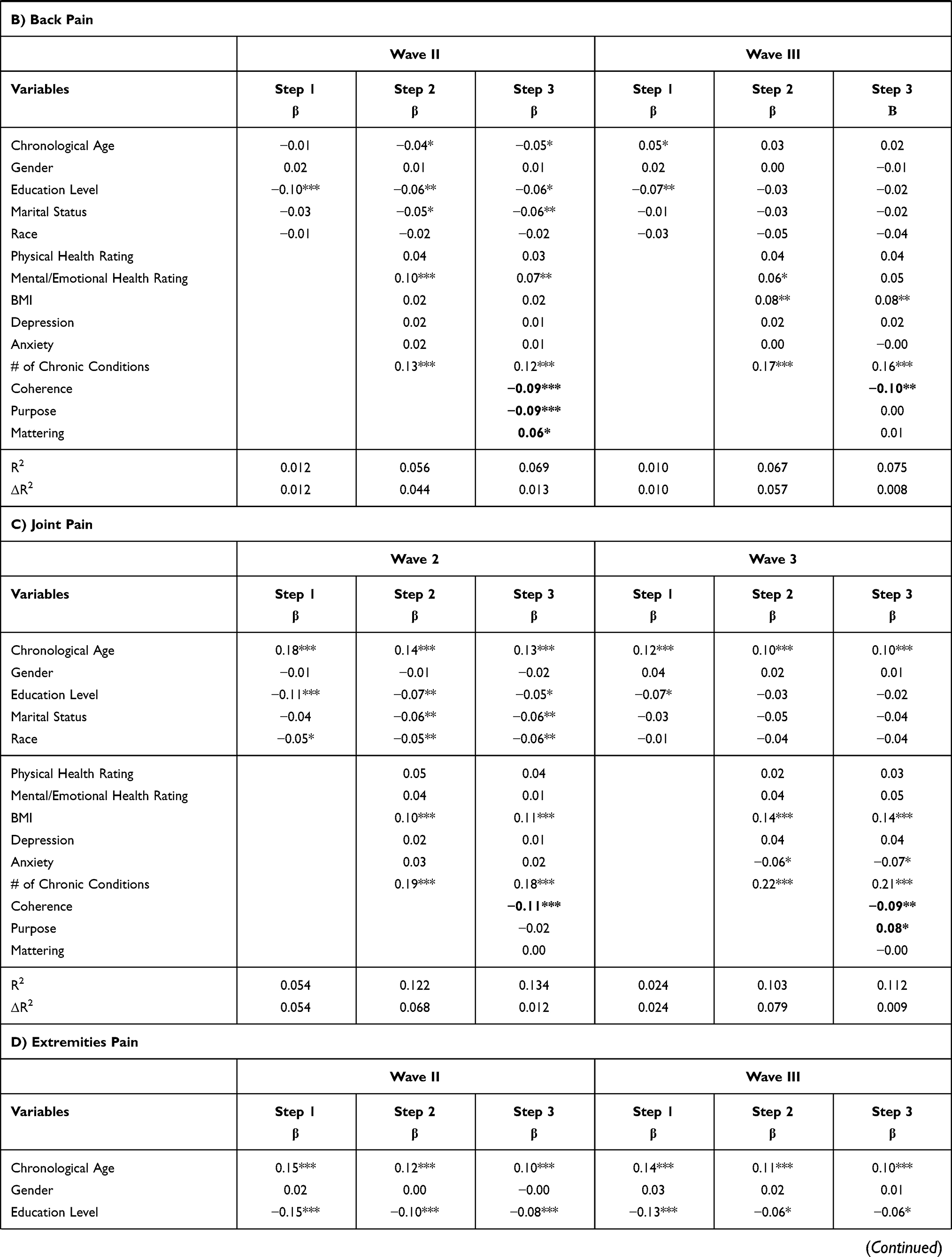 |  |
Table 3 Facets of Meaning Predicting Pain Frequencies |
Results of longitudinal analysis showed that coherence (OR = 0.948, 95% CI [0.906, 0.992], p = 0.021), but not purpose (OR = 0.995, 95% CI [0.974, 1.018], p = 0.687), or mattering (OR = 1.013, 95% CI [0.972, 1.056], p = 0.546) was associated with decreased odds of developing chronic pain controlling for all other variables (Table 4). The number of chronic conditions was the only other significant predictor for the development of chronic pain (OR = 1.129, 95% CI [1.055, 1.208], p < 0.001).
 |
Table 4 Longitudinal Predictors of the Development of Chronic Pain |
Study 1 Discussion
Study 1 provided initial evidence for the unique association of the three facets of MIL to pain experiences. Coherence was consistently and most strongly associated with less pain in all body regions relative to purpose and mattering. Purpose and mattering were both occasionally (and unexpectedly) associated with more frequent pain experiences. Importantly, the relationship between coherence and pain frequency was found even when controlling for other variables associated with both pain and meaning, such as depression and anxiety.31–33 Furthermore, coherence at Wave 2, but not purpose or mattering, predicted reduced odds for developing chronic pain in Wave 3, suggesting that the ability to make sense of the world may help individuals interpret and overcome pain experiences that may lead to chronification. However, while the items used to assess coherence and mattering appear to capture the essence of each respective construct, the measures were developed to assess different aspects of social well-being, not MIL per se.27–29 Recently, researchers have developed new measures to specifically measure the three facets of MIL.14 As such, we conducted a second study using this newer validated measure of MIL to conceptually replicate the findings of Study 1. Additionally, to further distinguish between associations of the three facets within MIL, we assessed global MIL and conducted mediation analysis to determine if coherence drives the relationship between meaning constructs and pain outcomes.
Study 2 Method
Participants
Participants were recruited from an undergraduate student research pool and were compensated with class credit. Participants (n = 519) were predominantly female (n = 366), ranging from 18 to 24 years old (M = 18.68, SD = 0.99), with sample size based off of suggested power analyses.34,35 Participants identified as White (n = 410), Asian (n = 46), more than one race or multiracial (n = 19), Black or African American (n = 17), (South Asian) Indian (n = 9), American Indian/Alaska Native (n = 8), Other (n = 3; specifically: 1 Hispanic, 1 Latino, and 1 declined to respond), and 7 participants chose not to provide this information. In response to a separate question assessing ethnicity, 112 participants also identified as Hispanic/Latino. This study was approved by the Texas A&M University IRB.
Procedure
Participants were administered a survey online on a device of their own choosing. After providing informed consent, participants completed the questionnaires described below, and were then debriefed. The study took approximately 20 minutes to complete.
Measures
Meaning in Life
Global MIL and its three facets were assessed using Costin & Vignoles’ recently validated scale.14 Participants rated their agreement with each item on a scale of 1 (strongly disagree) to 7 (strongly agree). Global MIL was assessed with four items (α = 0.892) such as “My life as a whole has meaning”. Coherence was assessed with four items (α = 0.677) such as “I can make sense of the things that happen in my life”, purpose (α = 0.803) with four items such as “I have a good sense of what I am trying to accomplish in life”, and mattering (α = 0.823) with four items such as “Even considering how big the universe is, I can say that my life matters”. Two items within each measurement were reverse coded; scores were calculated as the average of the four items within each domain.
Pain
Pain severity was assessed using the four-item severity subsection of the Brief Pain Inventory (BPI).36 Participants reported their current pain as well as their average, lowest, and worst pain during the past week on a scale of 0 (no pain) to 10 (pain as bad as you can imagine). A total severity score was calculated as the average of the four items (α = 0.833).
Anxiety
Anxiety was assessed using the Generalized Anxiety Disorder-7 scale (GAD-7).37 Participants were asked to rate how frequently they had been bothered by seven items (eg “feeling nervous, anxious, or on edge”) over the previous 2 weeks on a scale of 0 (not at all) to 3 (nearly every day). Anxiety scores were calculated as the sum of the items (α = 0.894).
Depression
Depression was assessed using the depression subscale of the Depression Anxiety Stress Scales (DASS).38 Participants indicated the extent to which 14 items (eg “I felt downhearted and blue”) applied to them over the past week using a scale of 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Depression scores were calculated as the sum of the items (α = 0.954).
Analysis Plan
Analyses were conducted using SPSS (version 25; IBM Corp, Armonk, NY). A hierarchical multiple regression was conducted to determine the independent predictive value of facets of meaning on pain severity over and above covariates. Demographics (age, gender, and race) and covariates known to be associated with pain and MIL (depression and anxiety) were included in the first two steps of the regression, respectively.39–41 Coherence, purpose, and mattering were added concurrently in the final step of the model. To further differentiate between the facets and their association with pain, we conducted a mediation analyses with the three facets of MIL entered together as mediators between global meaning in life and pain severity using Hayes’ PROCESS macro for SPSS.
Study 2 Results
Predictor and outcome variable descriptive statistics can be found in Table 5. Bivariate correlations indicate that pain severity was negatively correlated with global MIL, coherence, and purpose, but was not correlated with mattering (Table 6). Regression analysis found that the negative relationship between coherence and pain severity remained even after controlling for covariates (β = −0.182, 95% CI [−0.488, −0.118], p = 0.001), while the relationship with purpose was no longer significant (β = 0.011, 95% CI [−0.144, 0.176], p = 0.846); furthermore, a positive association between mattering and pain severity emerged (β = 0.124, 95% CI [0.034, 0.277], p = 0.012; Table 7).
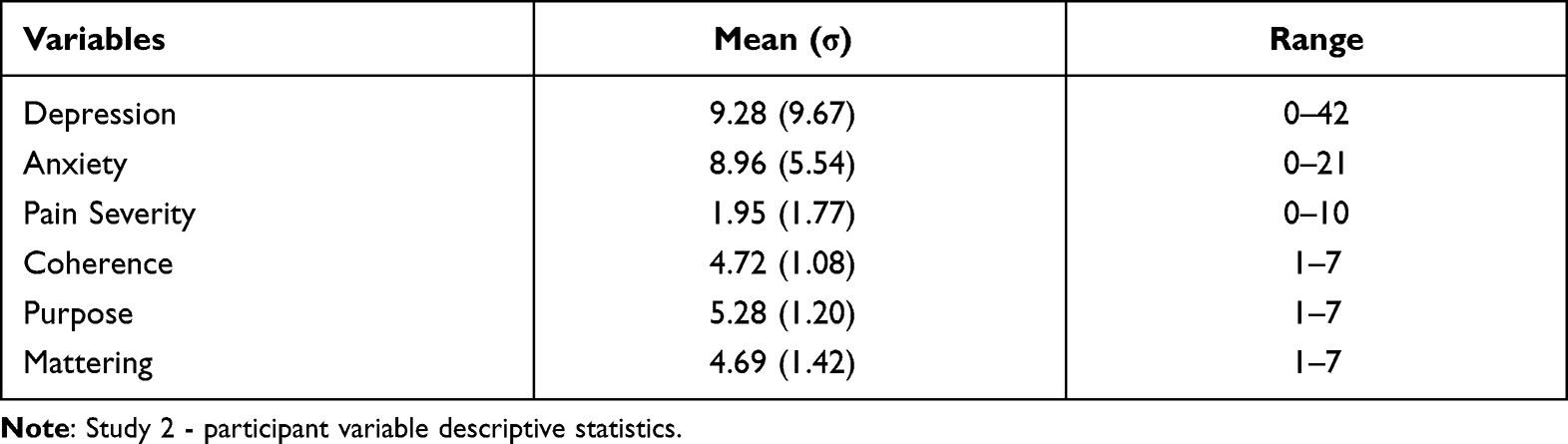 |
Table 5 Study 2 Variable Descriptive Statistics |
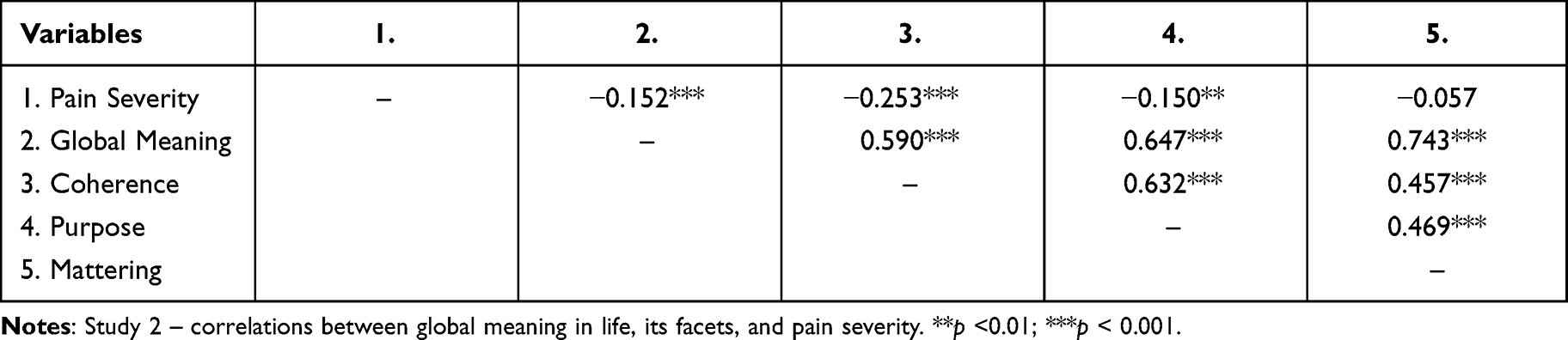 |
Table 6 Meaning in Life, Its Facets, and Pain Correlations |
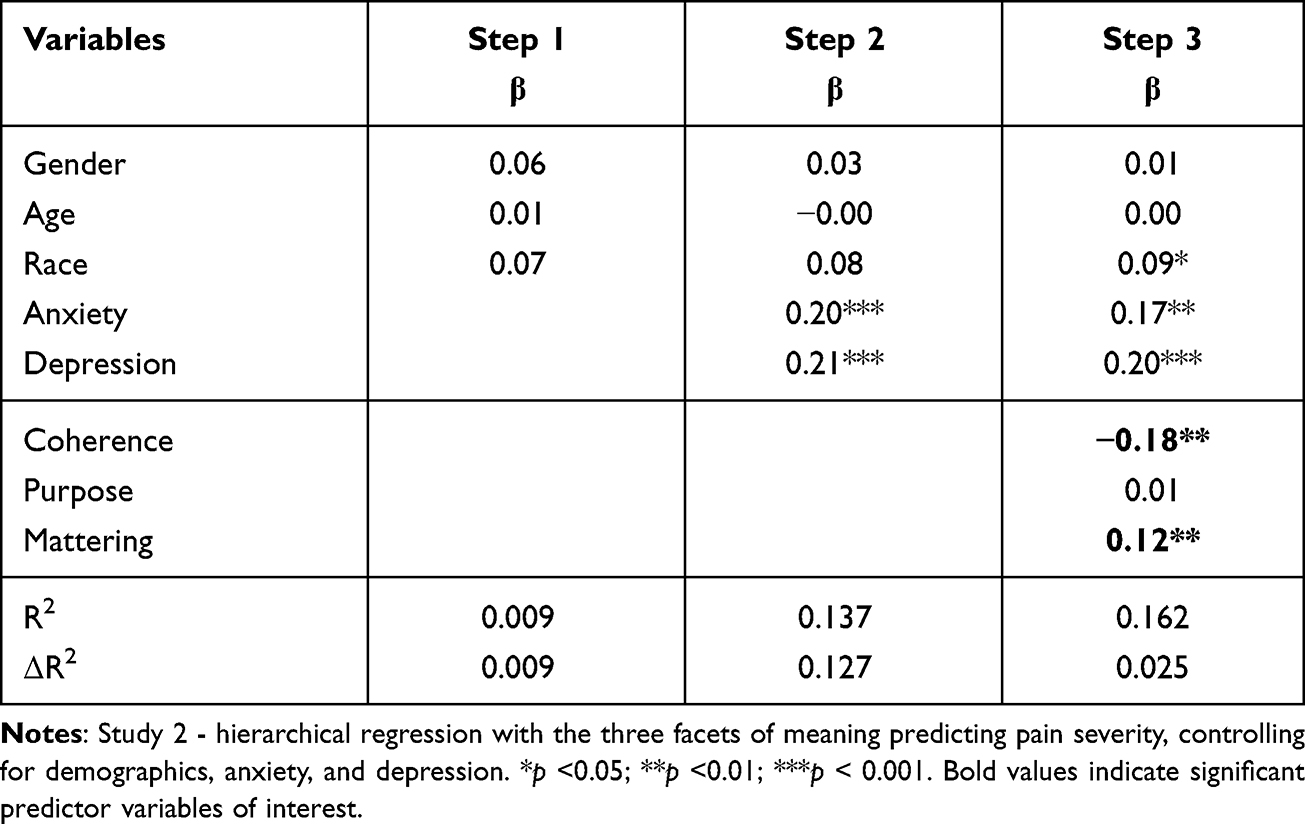 |
Table 7 Facets of Meaning Predicting Pain Severity |
Within mediation analysis, global MIL was used to predict pain severity, with the three facets added concurrently as mediators (Figure 1). The total effects of MIL on pain severity were significantly and negatively related. Global MIL was positively associated with each facet of MIL. In turn, coherence negatively predicted pain severity, mattering positively predicted pain severity, and purpose had no significant association. After taking coherence into account, global MIL had no direct effect on pain severity.
 |
Figure 1 Study 2 – Mediation analysis with Global Meaning in Life as the predictor, the facets of Meaning in Life (ie, coherence, purpose, and mattering) as the mediators, and pain severity as the outcome. Note: *p < .05; ***p < 0.001. |
Study 2 Discussion
Study 2 supported and built upon the findings of Study 1 such that coherence was uniquely associated with less severe pain. While purpose had no association with pain severity, mattering was associated with greater pain severity, further supporting the results of Study 1. These findings were strengthened through coherence’s complete mediation of the relationship between global MIL and pain severity, suggesting that assessing MIL by itself may fail to capture individual variations in pain outcomes, further supporting the need to measure all facets when predicting an individual’s pain experiences. However, this study was limited by its cross-sectional design; as such, we conducted a third study to further assess the impact of the individual facets of MIL on pain severity longitudinally. We also wanted to support the validity of our findings using the same current measure of the facets of MIL used in Study 2.
Study 3 Methods
Participants
Participants were undergraduates recruited through the university’s psychology student research pool as part of a larger study assessing existentialism. There were 155 participants, 17 of whom were excluded for failing an integrity check item or failing to complete at least 2 of the weekly surveys, leaving the study sufficiently powered for repeated measures.34,42,43 The final sample (N = 138) was 66.4% White 16.4% Asian, 12.1% Hispanic/Latino, 1.4% Black, and 3.6% did not report. Their ages ranged from 18 to 25 (M = 19.01, SD = 1.12). Within the final sample, 60.0% of participants completed all four weekly surveys, 30.7% completed 3, and 9.3% completed 2 weekly surveys. Participants were compensated with course credit. This study was approved by the Texas A&M University IRB.
Procedure
Participants initially had two weeks to complete a baseline survey. Three weeks after this window concluded, all participants were emailed the links to follow-up surveys each Monday for four consecutive Mondays. Participants had 24 hours to complete each follow-up survey before the link expired. Once they completed the fourth weekly survey, their participation was complete. All surveys were taken online using Qualtrics software.
Measures
Meaning in Life
MIL was assessed using the same scales used in Study 2.14 At the baseline measurement, items were framed at the trait level, using the same language as Study 2. The weekly measures were framed in reference to the past week (eg, “This week, I could make sense of the things that happened in my life.”).
Pain
Pain severity was again assessed using the four-item severity subsection of the BPI.36 Descriptive and scale statistics for all study materials can be found in Table 8.
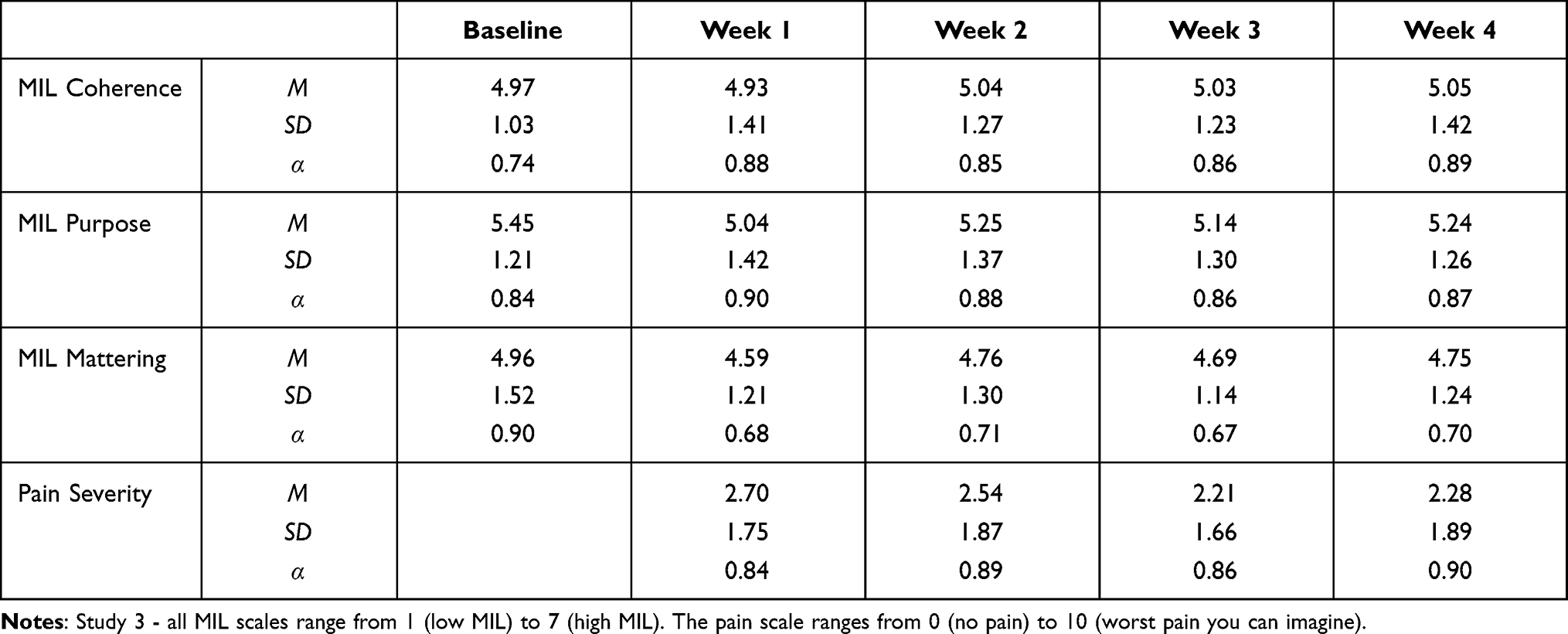 |
Table 8 Descriptive and Scale Statistics for Primary Study Variables |
Analysis Plan
Analyses were conducted using Jamovi version 1.6.23. We utilized linear mixed-modeling to determine whether each facet of weekly MIL would independently predict weekly pain severity. All weekly predictor variables were nested within-individuals, and were centered based on each individual’s unique mean (ie, cluster-based centered). For a model that included trait-level MIL, these variables were centered based on the sample mean. All models used a random intercept.
Study 3 Results
First, we tested whether weekly fluctuations in coherence, purpose, and mattering would predict weekly fluctuations in pain. Coherence emerged as a significant negative predictor of pain severity, b = −0.25 (SE = 0.08), t = −3.04, p = 0.003, 95% CI [−.42, −0.09]. Neither purpose, b = −0.09 (SE = 0.09), t = −1.01, p = 0.314, 95% CI [−.26, 0.08], nor mattering, b = −0.14 (SE = 0.09), t = −1.49, p = 0.136, 95% CI [−.31, 0.04] were significant predictors of pain severity.
Next, we entered baseline measurements of the facets into the model to determine whether trait levels of coherence, purpose, and mattering predicted weekly fluctuations in pain above and beyond weekly fluctuations in MIL. In this model, baseline coherence predicted the most unique variance in weekly pain (Table 9). Baseline purpose also emerged as a significant positive predictor. All weekly measures of the facets became nonsignificant.
 |
Table 9 Linear Mixed Model with MIL Facets Predicting Pain Severity |
Study 3 Discussion
The results of Study 3 supported the findings of Study 2, extending them to a longitudinal design. Weekly fluctuations in coherence uniquely negatively predicted weekly fluctuations in pain severity over and above the purpose and mattering. Furthermore, baseline coherence was the strongest predictor of pain severity when weekly and baseline measures of purpose and mattering were included in the model. The finding that baseline purpose positively predicted pain severity – while unexpected – replicates results from Study 1 showing that greater purpose was associated with more frequent joint pain in Wave 3. Overall, these results provide further support for the unique predictive power of coherence in pain outcomes.
General Discussion
Meaning in life, as a broad construct, has previously been identified as a pain-related resilience factor. However, MIL researchers generally recognize that the nuanced nature of the concept comprises multiple facets – including coherence, purpose, and mattering – that contribute to overall MIL. Identifying their unique relationships with pain can guide future research and improve current clinical practices that incorporate MIL. Across three separate studies, coherence was consistently associated with lower pain experiences to a greater degree than purpose or mattering, even when controlling for other pain- and MIL-related variables. This finding was robust and consistent across three large and unique samples, using both cross-sectional and longitudinal analyses. This included pain severity in young adults, the frequency of headache, back pain, joint pain, and extremities pain within two separate Waves of the MIDUS, as well as the development of chronic pain across Waves. Furthermore, coherence completely mediated the relationship between global MIL and pain severity, suggesting that it may be more indicative of pain outcomes than global MIL itself.
These results help clarify the unique role that individual facets of MIL play in regard to pain outcomes. Coherence involves incorporating the events of the past and present and projections of the future to envision one’s life and environment as a whole.11 Individuals with greater coherence may be better adapted to weave painful experiences into their overall life-view, reducing worry about pain experiences by integrating them into their understanding of the world. One way this may occur is via acceptance of painful experiences; acceptance of disease is associated with better health outcomes in general (eg lower disability and increased life satisfaction), as well as with a higher sense of coherence.44,45 Others have suggested that coherence may be associated with healthier lifestyle choices (eg physical activity), potentially further protecting against the development of pain-related outcomes.46 Future research should seek to elucidate precisely why judgments of coherence relate to pain outcomes in this way, and how this relationship might advance current understandings of both MIL and pain.
One unexpected finding was that mattering was associated with more frequent back pain in Study 1 and greater pain severity in Study 2. One possible explanation for this relationship is that a sense of mattering involves focusing on how one’s life has an impact on others or something greater than themselves.14 A concern about one’s obligations and contribution to others might increase distress when one is unable to fulfill that duty due to their pain, which may in turn further amplify pain.47,48 Indeed, recent research suggests that, for Americans, not disengaging from personal obligations increases the risk for inflammation and poor cardiovascular health.49 Additionally, having a greater sense of mattering may involve self-enhancement, or the tendency to overestimate the positive aspects of one’s self while downplaying the negative (eg, “My existence is significant in the grand scheme of things”) which may over-inflate the extent to which one feels that they matter to others or in general.11,50 However, those that self-enhance are often overly optimistic and tend to believe that they are less likely to develop disease, and are more likely to avoid or downplay self-relevant health information.51 In turn, these thought processes engender the belief that one is immune to the effects of participating in risky behavior. Together the optimistic views of one’s health along with the disregard of beneficial health information may contribute to greater pain experiences for those for whom mattering is important.
Purpose, meanwhile, is driven by the pursuit of multiple life goals.52 As such, pain may interfere with one’s ability to complete their goals, affecting one’s purpose, as well as increasing stress or depression that in turn may contribute to pain chronification.53,54 For instance, people with cancer whose goals were defined by career success, financial stability, and independence reported reduced purpose from before chemotherapy began to follow-ups months later.55 However, these individuals continued to emphasize the importance of those goals, suggesting that the difficulty or inability to achieve them due to chemotherapy was potentially impacting their purpose. Having purpose may help motivate people to push through pain but may not act to prevent its development, frequency, or severity. Ultimately, these interpretations are speculative, and future research should aim to further clarify these relationships.
There were a few limitations to this research. First, the measurement of pain varied across studies. Whereas Study 1 assessed the frequency of recent pains and the development of chronic pain over time, Studies 2 and 3 measured recent pain severity. However, the consistent finding that coherence, but not purpose or mattering, was associated with multiple types of pain experiences strengthens the reliability of these findings. Second, the samples included only participants in the United States; as the concept of MIL has been shown to vary between cultures, it would be reasonable to predict that the relationships between pain and different facets of meaning may differ in other populations.66 Furthermore, the lack of racial and ethnic diversity within the MIDUS (Study 1) limits the generalizability of this (widely used) sample. While the representation of most racial groups in Studies 2 and 3 more closely resembles 2019 population estimates in the United States, Black Americans were underrepresented in these samples, and this approach is known to underrepresent the experiences of minoritized populations.67 Finally, we used different measures to assess the facets of MIL in Study 1 relative to Studies 2 and 3, as we used opensource data for Study 1 and utilized the measures available to us within that data. However, the questionnaires in the MIDUS have been validated and tap into each facet, and the measures used in Studies 2 and 3 are current adaptations of the constructs, with some of the items being repurposed from those early measures.14,27–29 Nonetheless, future studies should continue to use the most current measures of MIL within health-related research.
This investigation potentially contributes to the understanding of how the association between MIL and pain relates to other important life outcomes. For example, previous research suggests that chronic pain can negatively impact one’s phenomenological experience of self.56 Multi-method approaches to understanding these abstract relationships are needed in order to better contextualize the diverse psychological consequences of pain and their practical implications.57 Chronic pain can frequently lead to outcomes like depression, anxiety, and suicidality, which are themselves closely tied to disruptions in MIL and demoralization.58–60 Elucidation of the mechanistic forces behind these relationships (eg, the unique contribution of coherence) can further contextualize previous research and ultimately inform future investigations aimed at reducing the individual and societal costs of pain.
The current findings have important clinical implications as well. Clinical interventions focusing on addressing MIL have been implemented to increase well-being and optimism, and to decrease anxiety.24 Furthermore, patients suffering from pain have expressed interest in incorporating meaning in life interventions; targeting coherence specifically may bolster the success of these interventions.61 While empirical support for meaning-based interventions is scant, Acceptance and Commitment Therapy (ACT) for chronic pain relies in part on value formation, identity building and mindfulness meditation to foster psychological flexibility.62,63 Given that self-knowledge and mindfulness both positively predict MIL, it is reasonable to speculate that ACT improves pain experiences in part through sense-making processes.64,65 Further, the identity-specific aspects of ACT may provide context and theoretical support for the unique importance of coherence that was observed here.
In conclusion, the current findings highlight the unique contribution of coherence in buffering against pain experiences. Further, these findings are the first to demonstrate the importance of studying individual facets of MIL together in the context of pain. Rather than focusing on MIL broadly, future studies and clinical interventions could benefit from incorporating measures of coherence, purpose, and mattering in their assessment of pain outcomes to observe their distinct impacts on pain experiences.
Disclosure
The authors report no conflicts of interest in this work.
This research did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Portions of these data were to be presented at the International Association for the Study of Pain’s 2020 World Congress on Pain in Amsterdam, The Netherlands (postponed due to COVID-19).
References
1. Park CL. Making sense of the meaning literature: an integrative review of meaning making and its effects on adjustment to stressful life events. Psychol Bull. 2010;136(2):257–301. doi:10.1037/a0018301
2. Frankl VE. Man’s Search for Meaning: From Death Camp to Existentialism.
3. Park CL. Meaning, spirituality, and growth: protective and resilience factors in health and illness. In: Baum A, Revenson TA, Singer J, editors. Handbook of Health Psychology. Psychology Press; 2012:405–429.
4. Dezutter J, Luyckx K, Wachholtz A. Meaning in life in chronic pain patients over time: associations with pain experience and psychological well-being. J Behav Med. 2015;38(2):384–396. doi:10.1007/s10865-014-9614-1
5. Anand S. Meaning in life and pain among breast cancer patients. Indian J Health Wellbeing. 2014;5(3):320–324.
6. Dezutter J, Casalin S, Wachholtz A, Luyckx K, Hekking J, Vandewiele W. Meaning in life: an important factor for the psychological well-being of chronically ill patients? Rehabil Psychol. 2013;58(4):334–341. doi:10.1037/a0034393
7. Martela F, Steger MF. The three meanings of meaning in life: distinguishing coherence, purpose, and significance. J Posit Psychol. 2016;11(5):531–545. doi:10.1080/17439760.2015.1137623
8. Steger MF, Frazier P, Kaler M, Oishi S. The meaning in life questionnaire: assessing the presence of and search for meaning in life. J Couns Psychol. 2006;53(1):80–93. doi:10.1037/0022-0167.53.1.80
9. Reker GT, Peacock EJ. The Life Attitude Profile (LAP): a multidimensional instrument for assessing attitudes toward life. Can J Behav Sci. 1981;13(3):264–273. doi:10.1037/h0081178
10. Czekierda K, Banik A, Park CL, Luszczynska A. Meaning in life and physical health: systematic review and meta-analysis. Health Psychol Rev. 2017;11(4):387–418. doi:10.1080/17437199.2017.1327325
11. George LS, Park CL. Meaning in life as comprehension, purpose, and mattering: toward integration and new research questions. Rev Gen Psychol. 2016;20(3):205–220. doi:10.1037/gpr0000077
12. Hicks JA, Routledge C. The Experience of Meaning in Life: Classical Perspectives, Emerging Themes, and Controversies. Hicks JA, Routledge C eds. Springer Science + Business Media; 2013.
13. King LA, Hicks JA. The science of meaning in life. Annu Rev Psychol. 2021;72(1):1–24. doi:10.1146/annurev-psych-072420-122921
14. Costin V, Vignoles VL. Meaning is about mattering: evaluating coherence, purpose, and existential mattering as precursors of meaning in life judgments. J Pers Soc Psychol. 2020;118(4):864–884. doi:10.1037/pspp0000225
15. Steger MF. Meaning and well-being. In: Diener E, Oishi S, Tay L, editors. Handbook of Well-Being. DEF Publishers; 2018:544–553.
16. Smith BW, Zautra AJ. The role of purpose in life in recovery from knee surgery. Int J Behav Med. 2004;11(4):197–202. doi:10.1207/s15327558ijbm1104_2
17. Smith BW, Tooley EM, Montague EQ, Robinson AE, Cosper CJ, Mullins PG. The role of resilience and purpose in life in habituation to heat and cold pain. J Pain. 2009;10(5):493–500. doi:10.1016/j.jpain.2008.11.007
18. Antonovsky A. The structure and properties of the coherence scale. Soc Sci Med. 1993;36(6):725–733. doi:10.1016/0277-9536(93)90033-Z
19. Chumbler NR, Kroenke K, Outcalt S, et al. Association between sense of coherence and health-related quality of life among primary care patients with chronic musculoskeletal pain. Health Qual Life Outcomes. 2013;11(1):1–8. doi:10.1186/1477-7525-11-216
20. García-Moya I, Moreno C, Rivera F. Sense of coherence and biopsychosocial health in Spanish adolescents. Span J Psychol. 2013;16(2013):1–10. doi:10.1017/sjp.2013.90
21. Wiesmann U, Dezutter J, Hannich HJ. Sense of coherence and pain experience in older age. Int Psychogeriatr. 2014;26(1):123–133. doi:10.1017/S1041610213001695
22. Giglio RE, Rodriguez-Blazquez C, De Pedro-cuesta J, Forjaz MJ. Sense of coherence and health of community-dwelling older adults in Spain. Int Psychogeriatr. 2015;27(4):621–628. doi:10.1017/S1041610214002440
23. Veehof MM, Oskam MJ, Schreurs KMG, Bohlmeijer ET. Acceptance-based interventions for the treatment of chronic pain: a systematic review and meta-analysis. Pain. 2011;152(3):533–542. doi:10.1016/j.pain.2010.11.002
24. Guerrero-Torrelles M, Monforte-Royo C, Rodríguez-Prat A, Porta-Sales J, Balaguer A. Understanding meaning in life interventions in patients with advanced disease: a systematic review and realist synthesis. Palliat Med. 2017;31(9):798–813. doi:10.1177/0269216316685235
25. Ryff C, Almeida DM, Ayanian J, et al. Midlife in the United States (MIDUS 2), 2004–2006. Ann Arbor, MI Inter-university Consort Polit Soc Res [distributor]; 2017.
26. Ryff C, Almeida D, Ayanian J, et al. Midlife in the United States (MIDUS 3), 2013–2014. Ann Arbor, MI Inter-university Consort Polit Soc Res [distributor]; 2017.
27. Keyes CLM. Social well-being. Soc Psychol Q. 1998;61(2):121–140. doi:10.2307/2787065
28. Ryff C, Keyes CLM. The structure of psychological well-being revisited. J Pers Soc Psychol. 1995;69(4):719. doi:10.1037/0022-3514.69.4.719
29. Ryff C. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J Pers Soc Psychol. 1989;57(6):1069–1081. doi:10.1037/0022-3514.57.6.1069
30. Edwards RR. The association of perceived discrimination with low back pain. J Behav Med. 2008;31(5):379–389. doi:10.1007/s10865-008-9160-9
31. Disabato DJ, Kashdan TB, Short JL, Jarden A. What predicts positive life events that influence the course of depression? A longitudinal examination of gratitude and meaning in life. Cognit Ther Res. 2017;41(3):444–458. doi:10.1007/s10608-016-9785-x
32. Walter SA, Jones MP, Talley NJ, et al. Abdominal pain is associated with anxiety and depression scores in a sample of the general adult population with no signs of organic gastrointestinal disease. Neurogastroenterol Motil. 2013;25(9):741–749. doi:10.1111/nmo.12155
33. Yek MH, Olendzki N, Kekecs Z, Patterson V, Elkins G. Presence of meaning in life and search for meaning in life and relationship to health anxiety. Psychol Rep. 2017;120(3):383–390. doi:10.1177/0033294117697084
34. Brysbaert M. How many participants do we have to include in properly powered experiments? A tutorial of power analysis with reference tables. J Cogn. 2019;2(1):1–38. doi:10.5334/joc.72
35. Schönbrodt FD, Perugini M. At what sample size do correlations stabilize? J Res Pers. 2013;47(5):609–612. doi:10.1016/j.jrp.2013.05.009
36. Cleeland CS, Ryan K. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singapore. 1994;23(2):129–138.
37. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
38. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales.
39. Ishida R, Okada M. Effects of a firm purpose in life on anxiety and sympathetic nervous activity caused by emotional stress: assessment by psycho-physiological method. Stress Health. 2006;22(4):275–281. doi:10.1002/smi.1095
40. Von Korff M, Simon G. The relationship between pain and depression. Br J Psychiatry. 1996;168(30):101–108. doi:10.1192/s0007125000298474
41. Volkert J, Härter M, Dehoust MC, et al. The role of meaning in life in community-dwelling older adults with depression and relationship to other risk factors. Aging Ment Health. 2019;23(1):100–106. doi:10.1080/13607863.2017.1396576
42. Aust F, Diedenhofen B, Ullrich S, Musch J. Seriousness checks are useful to improve data validity in online research. Behav Res Methods. 2013;45(2):527–535. doi:10.3758/s13428-012-0265-2
43. Guo Y, Logan HL, Glueck DH, Muller KE. Selecting a sample size for studies with repeated measures. BMC Med Res Methodol. 2013;13(1). doi:10.1186/1471-2288-13-100
44. Berglund B, Mattiasson AC, Nordström G. Acceptance of disability and sense of coherence in individuals with Ehlers-Danlos syndrome. J Clin Nurs. 2003;12(5):770–777. doi:10.1046/j.1365-2702.2003.00776.x
45. Wicksell RK, Ahlqvist J, Bring A, Melin L, Olsson GL. Can exposure and acceptance strategies improve functioning and life satisfaction in people with chronic pain and whiplash-associated disorders (WAD)? A randomized controlled trial. Cogn Behav Ther. 2008;37(3):169–182. doi:10.1080/16506070802078970
46. Wainwright NWJ, Surtees PG, Welch AA, Luben RN, Khaw KT, Bingham SA. Healthy lifestyle choices: could sense of coherence aid health promotion? J Epidemiol Community Health. 2007;61(10):871–876. doi:10.1136/jech.2006.056275
47. Tang NKY, Goodchild CE, Hester J, Salkovskis PM. Mental defeat is linked to interference, distress and disability in chronic pain. Pain. 2010;149(3):547–554. doi:10.1016/j.pain.2010.03.028
48. Schieman S, Taylor J. Statuses, roles, and the sense of mattering. Sociol Perspect. 2001;44(4):469–484. doi:10.1525/sop.2001.44.4.469
49. Hartanto A, Yee-Man Lau I, Yong JC. Culture moderates the link between perceived obligation and biological health risk: evidence of culturally distinct pathways for positive health outcomes. Soc Sci Med. 2020;244:112644. doi:10.1016/j.socscimed.2019.112644
50. Alicke MD, Sedikides C. Self-enhancement and self-protection: what they are and what they do. Eur Rev Soc Psychol. 2009;20(1):1–48. doi:10.1080/10463280802613866
51. Klein WMP, Cooper KL. On the physical health costs of self-enhancement. In: Chang EC editor. Self-Criticism and Self-Enhancement: Theory, Research, and Clinical Implications. American Psychological Association; 2009:141–158. doi:10.1037/11624-009.
52. McKnight PE, Kashdan TB. Purpose in life as a system that creates and sustains health and well-being: an integrative, testable theory. Rev Gen Psychol. 2009;13(3):242–251. doi:10.1037/a0017152
53. Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2017;95(6):1257–1270. doi:10.1002/jnr.23802
54. Currie SR, Wang J. More data on major depression as an antecedent risk factor for first onset of chronic back pain. Psychol Med. 2005;35(9):1275–1282. doi:10.1017/S0033291705004952
55. Pinquart M, Silbereisen RK, Fröhlich C. Life goals and purpose in life in cancer patients. Support Care Cancer. 2009;17(3):253–259. doi:10.1007/s00520-008-0450-0
56. Smith JA, Osborn M. Pain as an assault on the self: an interpretative phenomenological analysis of the psychological impact of chronic benign low back pain. Psychol Health. 2007;22(5):517–534. doi:10.1080/14768320600941756
57. Costanza A, Chytas V, Piguet V, et al. Meaning in life among patients with chronic pain and suicidal ideation: mixed methods study. JMIR Form Res. 2021;5(6):e29365. doi:10.2196/29365
58. Racine M. Chronic pain and suicide risk: a comprehensive review. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87:269–280. doi:10.1016/j.pnpbp.2017.08.020
59. Costanza A, Baertschi M, Richard-Lepouriel H, Weber K, Pompili M, Canuto A. The presence and the search constructs of meaning in life in suicidal patients attending a psychiatric emergency department. Front Psychiatry. 2020;11:1–7. doi:10.3389/fpsyt.2020.00327
60. Costanza A, Baertschi M, Richard-Lepouriel H, et al. Demoralization and its relationship with depression and hopelessness in suicidal patients attending an emergency department. Int J Environ Res Public Health. 2020;17(7):2232. doi:10.3390/ijerph17072232
61. Winger JG, Ramos K, Steinhauser KE, et al. Enhancing meaning in the face of advanced cancer and pain: qualitative evaluation of a meaning-centered psychosocial pain management intervention. Palliat Support Care. 2020;18(3):263–270. doi:10.1017/S1478951520000115
62. Wetherell JL, Afari N, Rutledge T, et al. A randomized, controlled trial of acceptance and commitment therapy and cognitive-behavioral therapy for chronic pain. Pain. 2011;152(9):2098–2107. doi:10.1016/j.pain.2011.05.016
63. Hayes SC, Strosahl KD, Bunting K, Twohig M, Wilson KG. What is acceptance and commitment therapy? In: Hayes SC, Strosahl KD, editors. A Practical Guide to Acceptance and Commitment Therapy. Springer US; 2004:3–29.
64. Schlegel RJ, Hicks JA, King LA, Arndt J. Feeling like you know who you are: perceived true self-knowledge and meaning in life. Personal Soc Psychol Bull. 2011;37(6):745–756. doi:10.1177/0146167211400424
65. Allan BA, Bott EM, Suh H. Connecting mindfulness and meaning in life: exploring the role of authenticity. Mindfulness. 2015;6(5):996–1003. doi:10.1007/s12671-014-0341-z
66. Kudla D, Kujur J, Tigga S, Tirkey P, Rai P, Fegg MJ. Meaning in life experience at the end of life: validation of the hindi version of the schedule for meaning in life evaluation and a cross-cultural comparison between Indian and German palliative care patients. J Pain Symptom Manage. 2015;49(1):79–88. doi:10.1016/j.jpainsymman.2014.05.013
67. United States Census Bureau. Race and Hispanic origin; 2019. Available from: https://www.census.gov/quickfacts/fact/table/US/PST045219.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.