Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Maximal Respiratory Pressures and Maximum Voluntary Ventilation in Young Arabs: Association with Anthropometrics and Physical Activity
Authors Bairapareddy KC ![]() , Augustine A, Alaparthi GK
, Augustine A, Alaparthi GK ![]() , Hegazy F, Shousha TM
, Hegazy F, Shousha TM ![]() , Ali SA, Nagaraja R, Chandrasekaran B
, Ali SA, Nagaraja R, Chandrasekaran B
Received 11 August 2021
Accepted for publication 24 September 2021
Published 14 October 2021 Volume 2021:14 Pages 2923—2930
DOI https://doi.org/10.2147/JMDH.S333710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kalyana Chakravarthy Bairapareddy,1 Anulucia Augustine,2 Gopala Krishna Alaparthi,1 Fatma Hegazy,1 Tamer Mohamed Shousha,1,3 Sara Atef Ali,1 Ravishankar Nagaraja,4 Baskaran Chandrasekaran5
1Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates; 2Department of Cardiovascular and Respiratory Physiotherapy, MGM College of Physiotherapy, Navi Mumbai, Maharashtra, India; 3Faculty of Physical Therapy, Cairo University, Cairo, Egypt; 4Department of Biostatistics, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, 110007, India; 5Department of Exercise Sciences and Sports, Manipal College of Health Professions, Manipal Academy of Higher Education, Manipal, Karnataka, India
Correspondence: Kalyana Chakravarthy Bairapareddy
Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates
Email [email protected]
Background: Maximum inspiratory pressure (MIP), maximum expiratory pressure (MEP) and maximum voluntary ventilation (MVV) measurements assist in determining the respiratory muscle strength and endurance. These determinants of respiratory muscles vary significantly by age, gender, height, and ethnic origin. Normative values for maximum respiratory pressures (MRPs) and MVV would aid in evaluating respiratory muscle function in athletes, estimating performance, and assisting in rehabilitation. In addition, the reference values may aid in determining the efficacy of therapeutic interventions in young people with chronic respiratory diseases. The purpose of this study was to see how respiratory muscle strength indices correlated with anthropometric and physical activity characteristics in young Arabs.
Methodology: The study included 80 male volunteers and 85 female volunteers ranging in age from 18 to 30 years. MicroRPM was used to measure MIP and MEP, and pulmonary function test data, including MVV values, were recorded. All subjects completed the Global Physical Activity Questionnaire (GPAQ) and anthropometric measurements. Unpaired t-tests or Mann–Whitney U-tests were used to determine male-female differences. Using the Pearson correlation coefficient and Spearman Rho correlation coefficient tests, MIP and MEP values were correlated with body composition and physical activity. Using stepwise multiple linear regression analysis, the relationships between respiratory function (MVV, MIP, and MEP) and PFT values (FVC, FEV1, and FEV1/FVC), physical activity, and sedentary behavior were investigated.
Results: MIP, MEP, and MVV values were significantly lower in females than in males. MIP, MEP, and MVV values had a moderate correlation with forced vital capacity, forced expiratory volume in 1 second, and height, but not with weight, BMI, or GPAQ. Age, gender, and body mass index were found to be significant predictors of maximal respiratory pressures in a young Arab population.
Conclusion: Maximum respiratory pressures and maximal voluntary ventilation were significantly lower in young Arabs than in other ethnic groups; these values were influenced by gender and height but not by levels of physical activity.
Keywords: maximal respiratory pressures, maximum voluntary ventilation, anthropometrics, physical activity, young Arabs
Introduction
Maximal Respiratory Pressures (MRPs) namely Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressures (MEP) are important components of pulmonary function test. These are mouth pressures produced by static effort and are the indicators of respiratory muscle strength.1,2 Clinically, the respiratory pressures are denoted as Maximal Inspiratory Pressure (PI max) and Maximal Expiratory Pressure (PE max), where PI max is a measure of inspiratory muscle strength and PE max denotes abdominal and intercostal muscle strength.3 Respiratory muscle strength reflects the function of respiratory pump which play a crucial role in ventilation and gas-exchange process.4,5 In addition to the afore mentioned components, Maximal Voluntary Ventilation (MVV) indicates the respiratory muscle endurance and signifies the lung function in healthy young adults and chronic respiratory diseases population.6 It is also observed that reduced ventilatory muscle strength influences cardiopulmonary endurance and athletic performance of healthy young adult population.7,8
MRPs are affected by factors such as age, gender, BMI, and ethnicity; one study found differences in respiratory muscle strength based on age and gender.9 Furthermore, ethnic variations have shown to influence the pulmonary function variables.10 According to one study, Libyan children had forced vital capacity and forced expiratory volume in one second that were 20% lower than the values predicted for Jordanian children11,12 Evidence suggests that not taking ethnic differences into account when performing lung function tests can lead to diagnostic errors.13
Various strength training strategies are available to improve cardiopulmonary endurance and athletic performance. The evaluation of respiratory muscle strength, on the other hand, becomes critical during routine clinical examinations because it establishes a baseline and allows the training program to be tailored accordingly.14 MIP and MEP can be reliably measured using the Respiratory Pressure Meter (RPM) device. Micro RPM is a non-invasive tool that provides clinicians and researchers with information on the efficiency of respiratory muscle strength and has a wide range of clinical applications.15 A recent study demonstrated the method of measuring the maximum respiratory pressures by end expiratory occlusion technique in patients on mechanical ventilation.16 Variables in pulmonary function tests should be interpreted using reliable population-based reference values. Furthermore, the literature on MRP reference values is based on a western population, resulting in variability due to a lack of selection criteria and a small sample size.1–3 A similar study on the Indian population, however, found lower MIP and MEP values than those found in western studies.17
Because MRPs are influenced by a variety of demographic factors, ethnic-specific reference values for respiratory muscle strength are required, which are currently unavailable for the Arab population. Additionally, there is a paucity of research on the relationship between anthropometric measurements and respiratory muscle strength. Thus, the objective of this research is to establish normative reference ranges for respiratory muscle strength in a young and healthy Middle Eastern Asian population.
Methodology
The cross-sectional study was conducted on healthy young adults of both genders. The cross-sectional study was conducted on healthy young adults of both genders. The University of Sharjah’s Research Ethics Committee (REC-19-06-11-01) gave their approval. A verbal advertisement was used to recruit participants, and 167 of them were chosen using convenient sampling. At a 5% level of significance and 90% power, sample size was calculated using an expected correlation coefficient between FVC and BMI of −0.4 and a partial correlation coefficient between FVC and BMI controlling for age and gender of −0.6. A 20% non-response rate was also taken into account. Sample size computation resulted in the sample size of 124. The study did, however, include 165 participants. The participants were informed about the study’s purpose, and it was carried out in accordance with the Helsinki Declaration. Each test procedure was explained in the language that the participants understood best. The study included asymptomatic adult population of 18–30 years of age group and with no history of chronic cardio-respiratory conditions. Smokers, participants with skeletal deformities of the chest wall, neuromuscular conditions and those who will not be able to follow the test procedures were excluded from the study.
Each participant underwent an evaluation program consisting of Pulmonary Function Tests, before the commencement of the study. Baseline parameters such as height, weight, Body Mass Index (BMI) and physical activity were recorded.
Procedure
Participants were enrolled in the study based on inclusion criteria, and prior to the study, each participant signed a written consent form. The height was measured with a metric stadiometer, which consists of a centimeter-calibrated ruler and a wall-mounted sliding headpiece. The measurements were taken in centimeters. The body weight was measured in Kilograms using a digital weighing scale. Body mass index (BMI) was calculated using the formula: body weight in kilograms divided by height in square meters. Global Physical Activity Questionnaire (GPAQ) full version evaluates PA under the following domains of “Activity at work”, “Activities performed on travel to and fro” and “Recreational activities”. Short-term (10 days) test–retest reliability of GPAQ was observed to be 0.93 to 0.96 whereas; long-term (three months) ranged from 0.53 to 0.83 and has low-to-moderate validity.18
The Pulmonary Function Test was performed using Spiro lab portable device (MIR-Spiro Lab Spirometer, Medical International Research, Italy, 2020). The device consisted of a mouthpiece, turbine and digital monitor that displays the test results. FVC, FEV1, FVC/FEV1, and MVV were measured according to the standards outlined in the American Thoracic Society guideline. The participants were asked to perform a series of forced inhalation and exhalation as fast as they could for 12–15 seconds for MVV, and the maximum volume achieved over 15 seconds was measured in percentage.19,20
MIP and MEP were measured using a MicroRPM, device (CareFusion UK 232 Ltd, Basingstoke, UK) a portable device which consists of a mouth-pressure manometer with a rubber flanged mouthpiece and a small digital monitor that displays the test results in cm H2O. The Participants remained seated with trunk erect, hip and knee flexed to 90 degrees and foot placed on the ground. A nose clip was used in all the maneuvers; in order to ensure no air leak around the mouthpiece. Before the measurement of the MIP and MEP, each participant performed five maximum inspiratory and maximum expiratory maneuvers to familiarize with the procedure. For measurement of MIP, the participants were asked to make a maximal inspiratory effort starting from the Residual Volume (RV) and the values were recorded. For MEP, a maximal expiratory effort starting from Total Lung Capacity was performed. Three trials were conducted each maintained for one second and the highest value was recorded. A rest pause of one minute was followed between each trial maneuver, and five minutes between MIP and MEP maneuver.15
Statistical Analysis
The data recorded from all the participants was analyzed using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics was used to present the demographic data, mean values of MIP and MEP for 18–30 years of age. The Shapiro–Wilk test was used to ensure that continuous variable distributions were normal. Unpaired t-tests or Mann–Whitney U-tests were used to assess differences between male and female participants. Pearson correlation coefficient of Spearman Rho correlation coefficient test were used to study the correlation of MIP and MEP values with body composition and physical activity. Stepwise multiple linear regression analysis was used to assess the associations of respiratory function (MVV, MIP, and MEP) with PFT values (FVC, FEV1, FEV1/FVC), physical activity, and sedentary behavior (percent sedentary time), adjusted for gender, age, height, weight and BMI. The level of significance for multiple regression analysis and correlation was set at P<0.05.
Results
A total of 165 participants data (80 males, 85 females) was recorded and analyzed. The mean age of the participants was 23.90 ± 3.14 years. The details of anthropometric measures, pulmonary function tests and physical activity components of the male and female participants are mentioned, respectively, in Table 1.
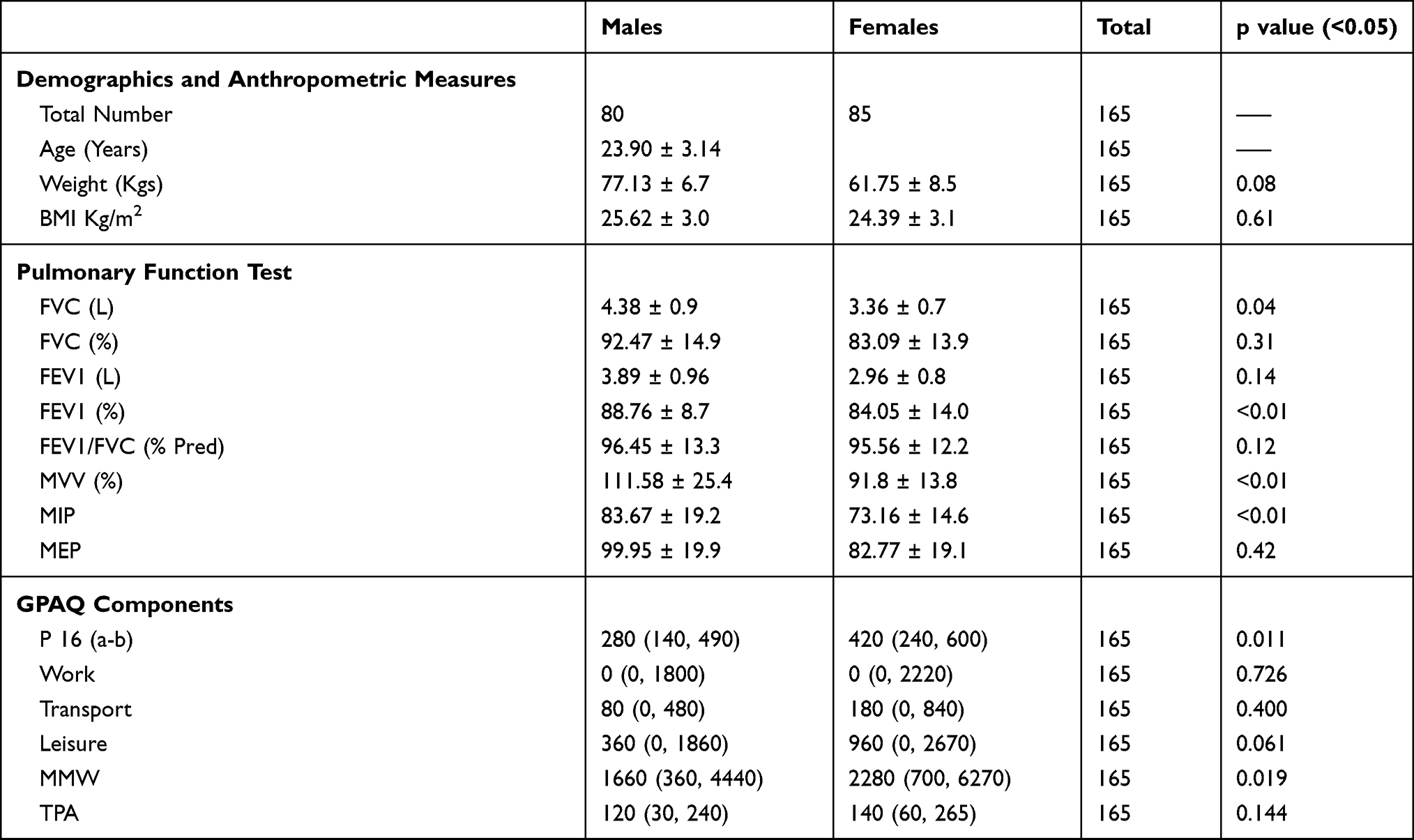 |
Table 1 Demographics, Anthropometric, Pulmonary Function Test, Maximal Respiratory Pressures and Physical Activity Components of GPAQ |
Correlation of MIP, MEP and MVV with Demographics, Anthropometric, Measures, Pulmonary Function Test and Physical Activity Components
The association of maximal respiratory pressures and MVV with demographics, anthropometrics, pulmonary function test and physical activity levels are mentioned in Table 2. In demographics, MIP and MVV showed negative little to no relationship with age respectively. Similarly, BMI showed negative little to no association with MIP, MEP and MVV, respectively. MVV showed a fair relationship with MIP and MEP. The physical activity components showed little to no relationship with maximal respiratory pressures and MVV.
 |
Table 2 Correlation Coefficient (r) of MIP, MEP and MVV with Demographics, Anthropometric Measures, Pulmonary Function Test Measures and Global Physical Activity Questionnaire (GPAQ) Components |
Association of MIP, MEP and PFT Values (FVC, FEV1 and MVV) with Age, Gender and BMI Using Regression Analysis
The description of multiple linear regression model of MIP, MEP and PFT values (FVC, FEV1 and MVV) are shown in Table 3. As age, gender and BMI showed a best predictive power to MRPs and PFT values, it was considered as the independent variable in regression analysis. Scatter plot of MIP, MEP and PFT values with age, gender and BMI are shown in Figures 1–5, respectively.
 |
Table 3 Association of MIP, MEP and PFT Values (FVC, FEV1 and MVV) with Age, Gender and BMI Using Regression Analysis |
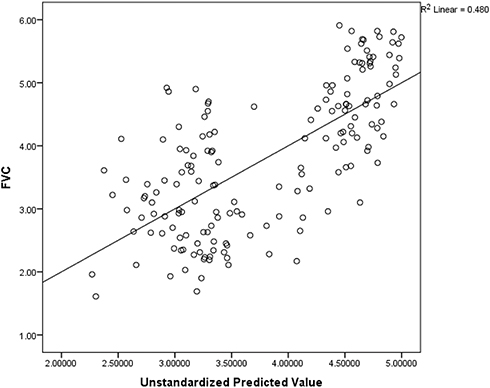 |
Figure 1 Scatter diagram of FVC with age, gender and BMI (R2- coefficient of determination). |
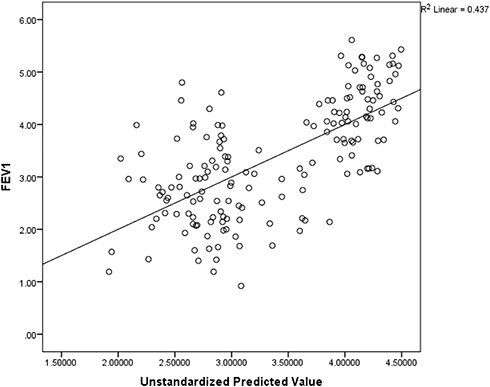 |
Figure 2 Scatter diagram of FEV1 with age, gender and BMI (R2- coefficient of determination). |
 |
Figure 3 Scatter diagram of MVV with age, gender and BMI (R2- coefficient of determination). |
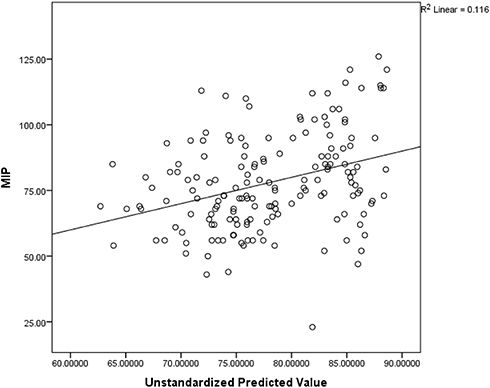 |
Figure 4 Scatter diagram of MIP with age, gender and BMI (R2- coefficient of determination). |
 |
Figure 5 Scatter diagram of MEP with age, gender and BMI (R2- coefficient of determination). |
Prediction equations of FVC, FEV1, MVV, MIP and MEP are mentioned below:
- FVC = 4.09 −0.012 Age + 1.56 Gender −0.09 BMI
- FEV1 = 3.77 −0.013 Age + 1.45 Gender −0.09 BMI
- MVV = 125.11 −1.56 Age + 22.45 Gender −0.79 BMI
- MIP = 91.29 −0.04 Age + 11.50 Gender −1.17 BMI
- MEP = 84.86 −0.02 Age + 18.85 Gender −0.87 BMI (Where, female= 1 and male= 2)
Discussion
The goal of this research was to determine the normative maximum respiratory pressures of a healthy young Middle Eastern Asian population. In our study, we used the age group of 18–30 years to predict MIP, MEP, MVV, and PFT values. The reported mean values of MIP in male is 83.67± 19.2 and MEP is 99.95 ± 19.9 whereas in female the MIP is 73.16 ± 14.6 and MEP is 82.77 ± 19. The MIP and MEP values obtained were similar to those found in a study by Gil Obando et al (MIP: 75cmH2O, MEP: 96.4 cmH2O).21 This could be attributed to the higher MVV values exhibited by the participants (Males: 111.58% ± 25.4, Females: 91.8% ± 13.8) as MVV is considered as an indirect measure of respiratory muscle strength. However, the MRP values obtained in our study differ from those reported in other studies by Black et al and Rodriguez, who reported higher average MIP and MEP values of 94.5 cm H2O and 175 cm H2O, respectively.22,23 Poor motivation, device calibration, geographical, ethnical differences, and the number of test trials are all possible causes of variation across populations. The number of trials used to measure MIP and MEP may have an impact on the test results, as observed by Black, Hyatt,22 and Leech,24 who found that Ringqvist’s results were lower because the latter used the best of many trials to measure these parameters.25 Furthermore, according to a study by Nambiar et al and Vyas et al, MRPs in COPD patients are much lower than in healthy people, which has a negative impact on physical functioning.26
Our findings revealed a significant gender effect, which is consistent with previous findings in the literature, in which males had higher MIP and MEP values than females.17,27 Men had MRP values that were 10–15% higher than female participants in our study. MIP and MEP values of 115.3 and 125.23 cm H2O in males and 86.2 and 88.6 cm H2O in females were found in studies across different populations by Smyth, Chapman, and Neder et al27,28 Anatomical, structural, and hormonal factors could all be contributing to the observed differences.
MIP, MEP, and MVV all had a negative relationship with age (r = −0.00, 0.02, and −0.15) when they were correlated with demographics. This is in line with a study by Costa, who found a negative correlation between MIP and MEP and age in both men and women. The data revealed contradicts the findings of several studies. According to the previous studies,15,17 respiratory muscle strength declines by 8–10% per decade, with a peak in the second and third decades. The participants’ narrow age range of 18–30 years could be one reason for the negative correlation with age. This is in line with a study by Misri et al, in which the MRP values of participants aged 18 to 25 years showed no statistically significant relationship with age.29 Furthermore, the lack of a link between MRPs and age may be due to the fact that age-related pulmonary function declines in the middle of the third decade.30
MIP, MEP, and MVV had no relationship with weight or BMI, which is consistent with a study by Vyas et al, who found no change in MRPs as a function of weight and BMI.27 Various studies, on the other hand, projected weight and BMI as strong predictors,24,31 stating that the diaphragm muscle varies almost threefold in underweight people to increased muscle mass in normal healthy built people.31 Physical activity components measured with the GPAQ had no correlation with MRPs or MVV in our study. There are a few studies that support our findings that MIP, MEP, and MVV have no relationship with moderate to severe physical activity,26,32 whereas other studies found a positive correlation.33
MIP, MEP, and PFT values (FVC, FEV1) showed a moderately significant relationship, which is consistent with previous research that found a strong correlation between MRPs and FVC and FEV1.25,33 MIP, MEP, and FEV1, FVC in COPD patients showed a highly significant correlation with a positive linear trend.26 MIP and MEP had a moderate relationship (r= 0.27, p=0.01) with MVV, which is consistent with a study by Pradeep Kumar et al, who found the highest correlation between MVV and MRPs.26 Because these two factors are linked, respiratory muscle endurance measured by MVV may have a direct impact on respiratory muscle strength measured by MIP and MEP. MVV would serve as a baseline parameter of respiratory muscle strength, helping to assess and rehabilitate the respiratory muscle in the young adult population by identifying the normative values and influencing factors of MRPs.
To obtain a prediction equation for MIP, MEP, and PFT values, regression analysis was used (FVC, FEV1 and MVV). Age, gender, and BMI were used as independent variables in the equations. Gender and maximal respiratory pressures were found to have a significant relationship in our study. There was no evidence of a link between age, BMI, and maximum respiratory pressures. Gender and BMI had a significant impact on FVC, FEV1, and MVV. As a result, age, gender, and BMI are all important predictors of maximum respiratory pressures.
Conclusion
Maximum respiratory pressures and maximal voluntary ventilation were significantly lower in young Arabs than in other ethnic groups; these values were influenced by gender and height, but not by physical activity levels. The normative values of maximal respiratory pressures (MIP, MEP) and MVV found in our study could be useful in identifying respiratory muscle dysfunction in young patients with chronic respiratory diseases.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Mcelvaney G, Blackie S, Morrison NJ, Wilcox PG, Fairbarn MS, Pardy RL. Maximal static respiratory pressures in the normal elderly. Am Rev Respir Dis. 1989;139:277–281. doi:10.1164/ajrccm/139.1.277
2. Evan JA, White WA. The assessment of maximal respiratory mouth pressure in adults. Resp Care. 2009;54:1348–1359.
3. Costa D, Gonçalves HA, Lima LP, Ike D, Cancelliero KM, Montebelo MI. New reference values for maximal respiratory pressures in the Brazilian population. J Bras Pneumol. 2010;36:306–312. doi:10.1590/S1806-37132010000300007
4. Pryor AJ, Prasad AS. Physiotherapy for Respiratory and Cardiac Problems: Adults and Pediatrics.
5. Frownfelter D, Elizabeth D. Cardiovascular and Pulmonary Physical Therapy.
6. Suh MR, Kim DH, Jung J, et al. Clinical implication of maximal voluntary ventilation in myotonic muscular dystrophy. Medicine. 2019;98(18):e15321. doi:10.1097/MD.0000000000015321
7. Amann M. Pulmonary system limitations to endurance exercise performance in humans. Exp Physiol. 2012;97(3):311–318. doi:10.1113/expphysiol.2011.058800
8. HajGhanbari B, Yamabayashi C, Buna TR, et al. Effects of respiratory muscle training on performance in athletes: a systematic review with meta-analyses. J Strength Cond Res. 2013;27(6):1643–1663. doi:10.1519/JSC.0b013e318269f73f
9. Chen HI, Kuo CS. Relationship between respiratory muscle function and age, sex, and other factors. J Appl Physiol. 1989;66(2):943–948. doi:10.1152/jappl.1989.66.2.943
10. Ip MS, Karlberg EM, Karlberg JP, Luk KD, Leong JC. Lung function reference values in Chinese children and adolescents in Hong Kong. I. Spirometric values and comparisons with other populations. Am J Respir Crit Care Med. 2000;162:424–429. doi:10.1164/ajrccm.162.2.9905057
11. Mukhtar MS, Rao GM, Morghom LO, Patrick JM. Spirometric standards of Libyan boys and girls. Respiration. 1989;56:227–234. doi:10.1159/000195805
12. Sliman NA, Dajani BM, Shubair KS. Pulmonary function in normal Jordanian children. Thorax. 1982;37:
13. Greenough A, Hird MF, Everett L, Price JF. Importance of using lung function regression equations appropriate for ethnic origin. Pediatr Pulmonol. 1991;11:207–211. doi:10.1002/ppul.1950110305
14. American Thoracic Society. ATS statement pulmonary rehabilitation. Thorax. 1999;159:1666–1682.
15. Dimitriadis Z, Kapreli E, Konstantinidou I, Oldham J, Strimpakos N. Test/retest reliability of maximum mouth pressure measurements with the MicroRPM ihealthy volunteers. Respir Care. 2011;56(6):776–782. doi:10.4187/respcare.00783
16. Spadaro S, Marangoni E, Ragazzi R, et al. A methodological approach for determination of maximal inspiratory pressure in patients undergoing invasive mechanical ventilation. Minerva Anestesiol. 2015;81(1):33–38. Epub 2014 May 27. PMID: 24861720.
17. Gopalakrishna A, Vaishali K, Prem V, Aaron P. Normative values for maximal respiratory pressures in an Indian Mangalore population: a cross-sectional pilot study. Lung India. 2011;28(4):247. doi:10.4103/0970-2113.85684
18. Herrmann SD, Heumann KJ, Der Ananian CA, Ainsworth BE. Validity and reliability of the global physical activity questionnaire (GPAQ). Meas Phys Educ Exerc Sci. 2013;17(3):221–235. doi:10.1080/1091367X.2013.805139
19. Spiro Lab. Medical international research, user manual rev; 2015.
20. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. Am J Respir Crit Care Med. 2019;200(8):e70–88. doi:10.1164/rccm.201908-1590ST
21. Gil Obando LM, López López A, Ávila CL. Normal values of the maximal respiratory pressures in healthy people older than 20 years old in the City of Manizales-Colombia. Colomb Médi (Cali). 2012;43(2):119–125.
22. Black L, Hyatt R. Maximal respiratory pressures: normal values and relationship to age and sex. Am Rev Respir Dis. 1969;99(5):696–702.
23. Rodriguez J, Mantilla AM, Mantilla D, et al. Maximum inspiratory and expiratory pressure: normal values in apparently healthy adult individuals Valencia 2001–2002. Rev Salus Online. 2004;8(3):4–10.
24. Neder J, Andreoni S, Lerario M, Nery L. Reference values for lung function tests. II. Maximal respiratory pressures and voluntary ventilation. Braz J Med Biol Res. 1999;32(6):719. doi:10.1590/S0100-879X1999000600007
25. Ringqvist T. The ventilatory capacity in healthy subjects: an analysis of causal factors with special reference to the respiratory forces. Scan J Clin Lab Invest. 1966;18(Suppl. 88):1–179.
26. Nambiar VK, Ravindra S, Kumar BN. Maximal inspiratory and expiratory pressures in men with chronic obstructive pulmonary disease: a cross-sectional study. Indian J Respir Care. 2018;7(2):88. doi:10.4103/ijrc.ijrc_5_18
27. Vyas PK, Bindroo PS, Gondha M, Mathur RS, Ghtawat G, Lakkappan V. Measurement of maximal respiratory static pressure in stable COPD patients and their co-relation with various physiological anthropometric and spirometry parameters and arterial blood gas tension. Arch Pulmonol Respir Care. 2020;6(1):033–042. doi:10.17352/aprc.000049
28. Smyth RJ, Chapman KR, Rebuck AS. Maximal inspiratory and expiratory pressures in adolescents: normal values. Chest. 1984;86(4):568–572. doi:10.1378/chest.86.4.568
29. Neder JA, Andreoni S, Castelo-Filho A, Nery LE. Reference values for lung function tests. Braz J Med Biol Res. 1999;32(6):703–707. doi:10.1590/S0100-879X1999000600006
30. Misri ZK, Saboo RC. Maximal mouth pressure estimation as a parameter of respiratory muscle function in healthy medical students. Kasturba Med Coll. 2000;18(2):42–46.
31. Chan CC, Cheong TH, Wang YT, Poh SC. Transdiaphragmatic pressure in young adult Singaporeans – normal values and a comparison between different respiratory manoeuvres. Aust NZ J Med. 1996;26(1):75–81. doi:10.1111/j.1445-5994.1996.tb02910.x
32. Chaves GSS, Texeira MA, Freitas DA, Mendes REF, Maciel ACC, Mendonça KMPP. Pressões respiratórias máximas de adolescentes brasileiros com diferentes níveis de atividade física [Maximal respiratory pressures of Brazilian adolescents with different levels of physical activity]. Conscientiae Saude. 2013;12(2):274–281. Portuguese. doi:10.5585/conssaude.v12n2.4227
33. Miranda APB, Gastaldi AC, Souza HCD, Santos JLF. The influence of physical fitness on respiratory muscle strength in the elderly. Am J Sports Sci. 2015;3(1):6–12. doi:10.11648/j.ajss.20150301.12
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.