Back to Journals » Clinical Epidemiology » Volume 13
Maternal Smoking During Pregnancy and Offspring Head Growth in Comparison to Height and Weight Growth Up to 6 Years of Age: A Longitudinal Study
Authors Karvonen M ![]() , Saari A, Sund R
, Saari A, Sund R ![]() , Sankilampi U
, Sankilampi U
Received 8 July 2021
Accepted for publication 14 September 2021
Published 12 October 2021 Volume 2021:13 Pages 959—970
DOI https://doi.org/10.2147/CLEP.S327766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor H Sorensen
Marjo Karvonen,1,2 Antti Saari,1,2 Reijo Sund,1 Ulla Sankilampi1,2
1School of Medicine, Institute of Clinical Medicine, University of Eastern Finland, Kuopio, Finland; 2Department of Pediatrics, Kuopio University Hospital, Kuopio, Finland
Correspondence: Marjo Karvonen Email [email protected]
Background: Maternal smoking during pregnancy causes fetal growth retardation. Thereafter, it has been associated with excessive childhood weight gain and decreased linear growth in the offspring. However, it is not known whether head circumference (HC), the surrogate of brain size in childhood, is altered after intrauterine tobacco exposure. We assessed the association of maternal smoking during pregnancy with offspring HC growth up to age 6 years in comparison with length/height growth and weight gain.
Methods: We combined data from Medical Birth Register and longitudinal growth data from primary care of 43,632 children (born 2004– 2017). Linear mixed effects models were used for modeling, adjusting for potential perinatal and socioeconomic confounders.
Results: At birth, maternal smoking during pregnancy was associated with a mean deficit of 0.19 standard deviation score (SDS) (95% CI: − 0.25, − 0.12) in HC, − 0.38 SDS (95% CI: − 0.43, − 0.32) in length, and − 0.08 SDS (95% CI:− 0.14, − 0.02) in weight-for-length. HC in smokers’ children failed to catch up to that of non-smokers’ children. Height of smokers’ infants reached that of non-smokers’ infants by 12 months but declined thereafter. Weight-for-height of smokers’ infants exceeded the level of non-smokers’ infants at 3 months and remained significantly elevated thereafter. HC in the offspring of mothers who quit smoking in the first trimester was not deficient, but their weight-for-height was elevated.
Conclusion: HC of smokers’ children is still deficient at age 6 years. Since most of the head growth occurs during the first 2 years of life, the defect may be permanent. In smokers’ children, weight gain was excessive up to 6 years and height was deficient at 6 years consistent with previous literature. Efforts should be made to encourage pregnant women to quit smoking in the beginning of the pregnancy.
Keywords: maternal smoking, tobacco exposure, child growth, head circumference, weight, height
Plain Language Summary
- Maternal smoking during pregnancy is associated with reduced weight, length and head circumference of the newborn. Postnatally, these children tend to gain excessive weight, whereas their height growth is not increased in a similar way. The impact of maternal smoking during pregnancy on head growth in childhood is less well characterized. Head circumference is an indicator of brain size in childhood.
- The aim of this study was to clarify how maternal smoking in pregnancy is associated with child head growth, in comparison with growth in weight and height from birth to age 6 years in a population of 43,632 children.
- We showed that maternal smoking after the first trimester of pregnancy was associated with a slightly smaller head size in offspring at least until the age of 6 years.
- Most of the head and brain growth occur during the first two years of life, and the persisting deficit in head size at 6 years may be permanent.
- No deficit was observed in the head size of those children whose mothers had quit smoking in the first trimester of pregnancy.
- Efforts should be taken to encourage pregnant women to quit smoking in the beginning of the pregnancy.
Introduction
Maternal smoking during pregnancy is among the most common risk behaviors that harm unborn fetuses. In Europe, the prevalence of smoking in pregnancy varies from less than 5% in Lithuania to 19% in Scotland; in the US, the numbers range from 2% in California up to 27% in West Virginia.1–3 Intrauterine exposure to tobacco smoke has been associated with neurodevelopmental issues including cognitive deficits and behavioral problems.4,5 These associations have been linked to biological factors such as impaired brain growth due to fetal hypoxia,6,7 alterations in brain structure and function,8 and epigenetic changes.9 On the other hand, familial and genetic factors have largely explained the associations between maternal smoking in pregnancy and offspring neurobehavioral problems such as attention deficit hyperactivity disorder (ADHD).4 However, there is consistent evidence of a causal environmental effect of maternal smoking in pregnancy on fetal growth resulting in reduced weight, length, and HC at birth.4,10–12
Maternal smoking during pregnancy has been associated with excessive childhood weight gain and obesity in the offspring13,14 as well as with a deficit in postnatal height growth up to adolescence.15–18 Head circumference (HC) is a surrogate measurement of brain size at birth and during childhood,19,20 and it is not known whether maternal smoking during pregnancy alters the growth of the developing brain permanently. A complete catch-up in HC during the first year of life has been observed in some studies,11,21–23 whereas others have reported suboptimal head growth during the first year of life.13,18 These studies with conflicting results have limitations, such as relatively small study samples from less than 200 to around 2000 infants with short follow-up times mostly limited to infancy, or lack of controlling for confounding factors that could affect head growth.
The aim of this study was to assess the association of maternal smoking during pregnancy with postnatal head growth in comparison with postnatal length/height growth and weight gain in a large population-based cohort of mothers and children, using up-to-date growth references and auxological methodology and controlling for perinatal and socio-demographic confounding factors.
Materials and Methods
Study Design and Population
The original study population comprised all 51,489 children (51.5% boys) born in Finland between January 1, 2004, and August 31, 2017, and living in the city of Espoo, Finland, on September 14, 2017 (Figure 1). This study links perinatal and birth outcome data of the Finnish Medical Birth Register maintained by the Finnish Institute for Health and Welfare (THL) with data on the socioeconomic status of the mothers from Statistics Finland and the longitudinal growth data from birth to 6 years of age obtained from primary care electronic health records. The exclusion criteria included a preterm or post-term birth (before 37 or after 42 gestation weeks, n = 4705), a major congenital anomaly or syndrome (diagnostic codes Q00-07, Q75, Q85-87, and Q90-99 according to the International Classification of Diseases, 10th version, ICD-10, n = 603), or in vitro fertilization (n = 1821). We also excluded mother–child pairs for whom data were not available on socioeconomic status (n = 72) or maternal smoking during pregnancy (n = 656). The final population comprised 43,632 children (51.2% boys) (Figure 1).
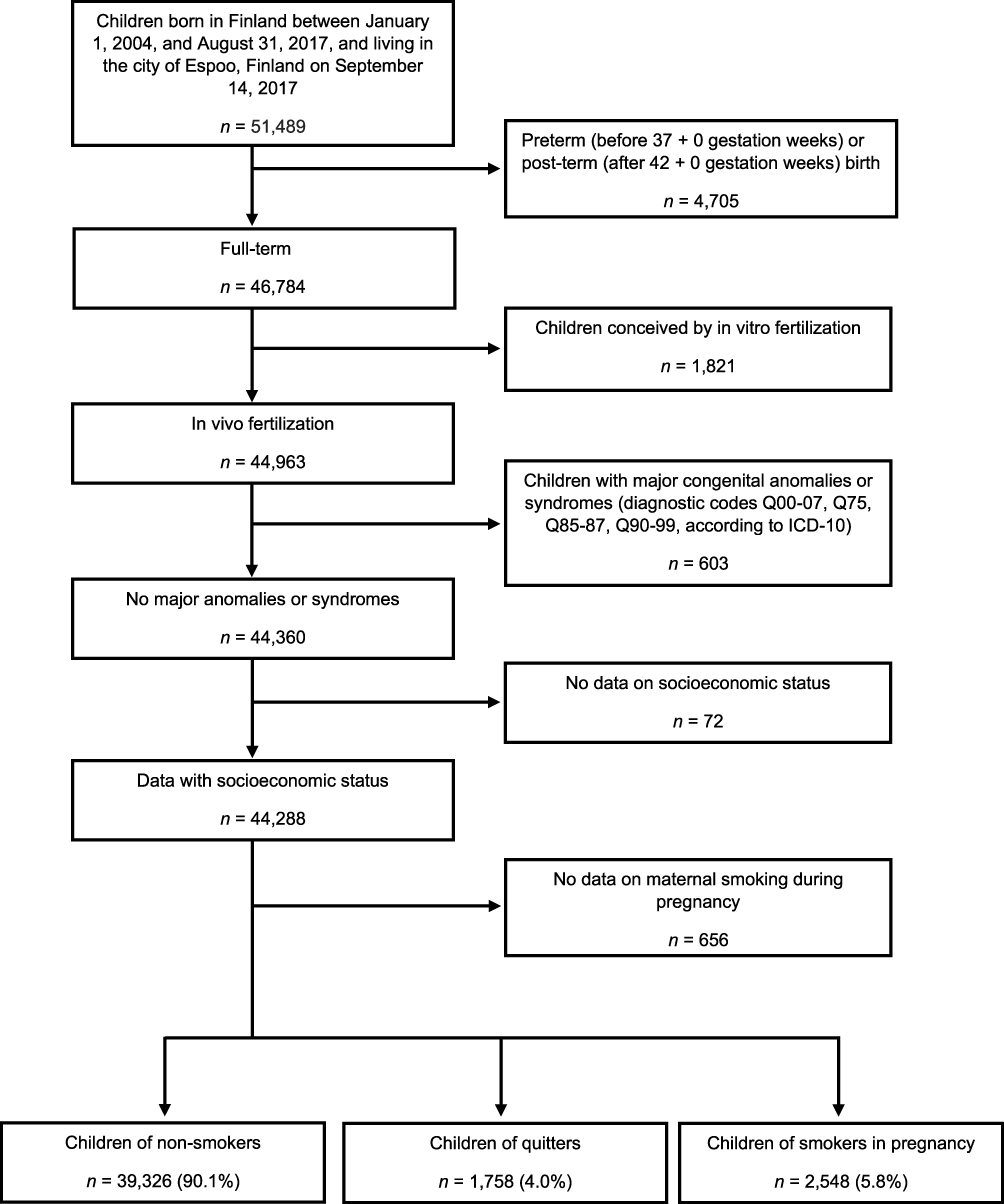 |
Figure 1 Flow diagram of the study population. Perinatal data were obtained from the Finnish Medical Birth Register. Non-smokers did not smoke at all during pregnancy, quitters stopped smoking during the first trimester, and smokers continued smoking after the first trimester. Abbreviation: ICD-10, International Classification of Diseases, 10th version. |
Auxological Measurements
Birth weight, length, and head circumference of all newborns were measured at the birth hospital and registered in Medical Birth Register and primary care files. After birth, all infants and children in Finland are provided regular free-of-charge primary care visits, which include auxological evaluations by trained nurses. HC, weight, and length/height are measured using standardized techniques. There is a minimum of 11 visits during the first 24 months of life, and thereafter annual visits up to 6 years of age. Longitudinal growth data of the study population were gathered from the electronic health records of Espoo primary care. In the 43,632 children, there were 575,421 HC measurements, 572,938 length/height measurements, and 572,699 weight measurements between 0 and 6 years of age (median 14 HC, length/height and weight measurements per subject, range 1–37; range 1–36 in weight measurements). HC, weight, and length/height measurements were converted into SDS units using population-based growth references.24–26
Covariates
The information regarding maternal smoking habits during pregnancy was self-reported by the mothers and gathered in Medical Birth Register by primary care nurses who meet the mothers regularly during the pregnancy. Smoking status was classified as 1) non-smokers who did not smoke at all during pregnancy, 2) quitters who stopped smoking during the first trimester, and 3) smokers who continued smoking after the first trimester. Previous studies have shown a good agreement of Medical Birth Register smoking data with the medical records.27,28 Data on the quantity of smoking were not gathered in the register.
Medical Birth Register data on potential risk factors that may affect fetal or postnatal growth were used as exclusion criteria (Figure 1) or covariates in the statistical analyses. Maternal age, height, and pre-pregnancy body-mass index (BMI), which was calculated according to maternal pre-pregnancy height and weight (weight (kg)/[height (m)]2), were used as continuous variables. The rest were categorical variables: parity (primi- or multiparous), living status (cohabiting or single), dichotomous indicators for any hypertensive or diabetic condition of the mother or for assisted fertility treatments (after excluding those conceived by in vitro fertilization), birth asphyxia (defined as umbilical pH <7.05 or ICD-10 codes O68, P20, or P21), or plurality (twinning or single birth). Child’s age and sex were included in the HC, weight, and length/height SD conversion algorithms.24–26 Diagnoses of maternal hypertensive or diabetic conditions were set by doctors in primary care and maternal outpatient clinics during pregnancy.
Data on socioeconomic status (SES) based on the occupation of the mother were obtained from Statistics Finland. SES was classified into 4 categories: SES I) upper white-collar worker, SES II) lower white-collar worker, SES III) blue-collar worker, and SES IV) others, including entrepreneurs, students, pensioners, homemakers, and those not included in SES I–III.
Statistical Analyses
The association of maternal smoking during pregnancy with postnatal longitudinal head growth as well as with length/height and weight-for-length/height growth were evaluated using linear mixed effects models for repeated measures with heterogeneous autoregression correlation structure. Growth data were grouped by age categories, between which the within-subject correlation was taken into account in the models. During the first 6 months of life infants and their families visit child health clinic every month or even more frequently. To simplify the analyses, we used less frequent intervals to form the age groups: birth (until third day after birth), 3 months (fourth day after birth – 0.38 years), 6 months (0.39–0.75 years), 12 months (0.76–1.25 years), 18 months (1.26–1.75 years), 2 years (1.76–2.50 years), 3 years (2.51–3.50 years), 4 years (3.51–4.50 years), 5 years (4.51–5.50 years), and 6 years (5.51–7.00 years; the median age of the last age group was 6.0 years). If several measurements were available for a child within the age category, only one measurement nearest to the intended age was used in the analyses. For example, all measurements between 2.51 (circa 30 months) and 3.50 years (42 months) were considered possible for representing the 3-year measurement, but the measurement closest to the age of 3 years was chosen for analyses.
The number of HC, length/height, and weight measurements by age group is provided in the Supplemental Materials Tables S1–S3. Also, scatter plots of 5% random samples of the HC, length/height and weight measurements by age are provided in the Supplemental Materials Figure S1. Multivariate models were adjusted for potential confounding factors: maternal height, age and pre-pregnancy BMI, parity, living status, SES, maternal hypertensive or diabetic condition, birth asphyxia, assisted fertility treatments (after excluding those conceived by in vitro fertilization), and plurality (twinning or single birth).
Linear mixed models were also used for unadjusted analyses for HC, length/height, and weight-for-length/height as a baseline comparison.
All analyses were performed using SPSS statistical software version 27 (IBM Corp., Armonk, NY).
Results
Tobacco Exposure During Pregnancy
Altogether, 43,632 children were included in the final study population. Mothers of 39,326 children (90.1%) were non-smokers during pregnancy, mothers of 1758 children (4.0%) stopped smoking during the first trimester (“quitters”), and mothers of 2548 (5.8%) children smoked after the first trimester (Figure 1). Mothers who smoked during pregnancy were the youngest, and those who did not smoke during pregnancy were the oldest mothers (Table 1). Smokers belonged less often to the highest SES group than did non-smokers [4.6% (95% CI: 3.8, 5.5) vs 34.8% (95% CI: 34.3, 35.2)] and were less often multiparous [51.3% (95% CI: 49.4, 53.3) vs 56.3% (95% CI: 55.8, 56.8), respectively]. Smokers had a slightly higher pre-pregnancy BMI compared with that of quitters or non-smokers [median 23.1 kg/m2 (interquartile range (IQR) 20.5, 26.7) vs 22.8 kg/m2 (IQR 20.8, 25.9) and 22.4 kg/m2 (IQR 20.5, 25.0), respectively]. Smokers and quitters were also slightly shorter than non-smokers. A greater proportion of smokers than non-smokers were single [19.3% (95% CI: 17.6, 20.9) vs 3.5% (95% CI: 3.3, 3.6)].
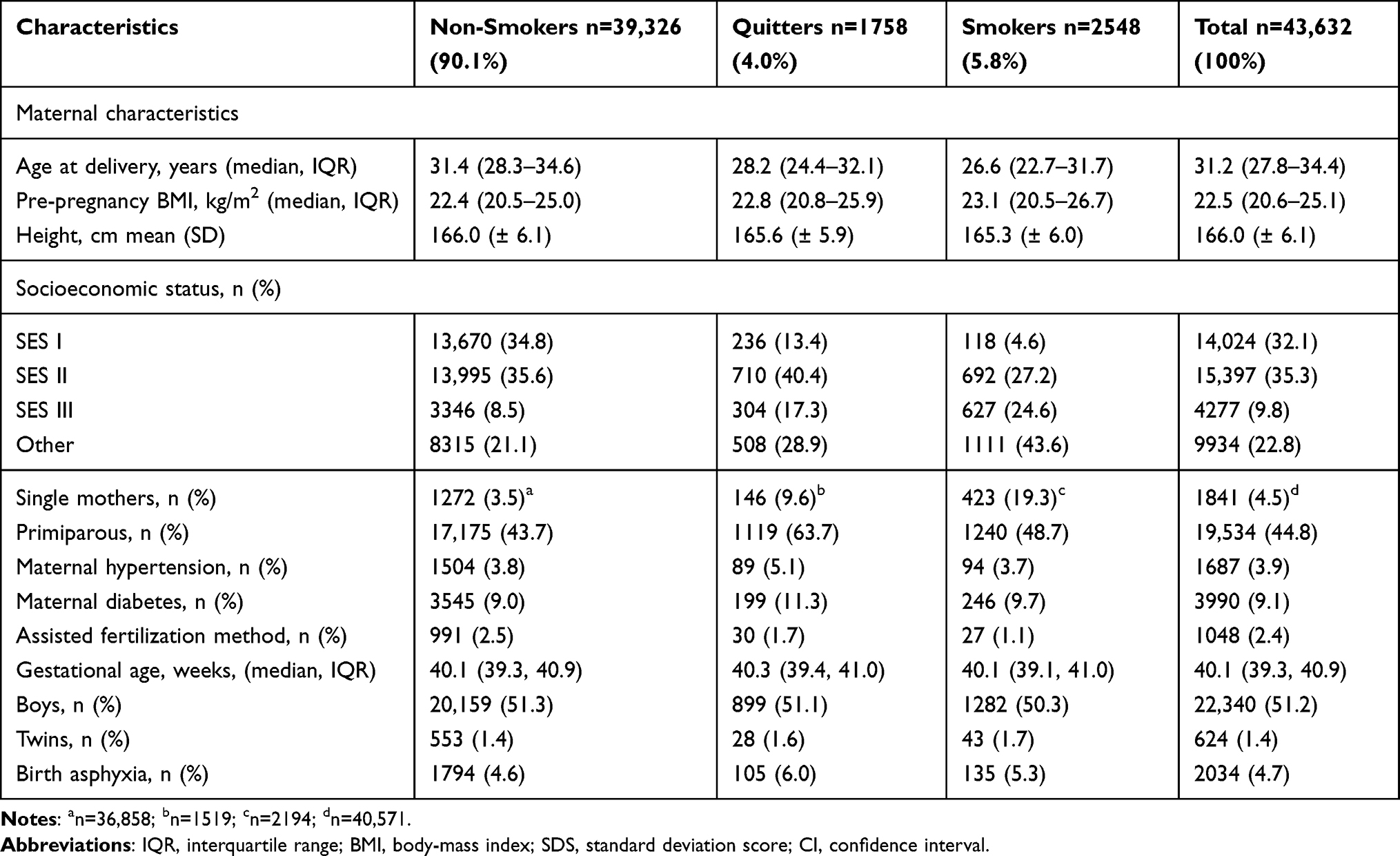 |
Table 1 Characteristics of the Study Population (N = 43,632) by Maternal Smoking Status |
Head Circumference
At birth, the mean unadjusted HC SDS was significantly smaller in smokers’ newborns (mean −0.31 SDS, 95% CI: −0.37, −0.25) than in non-smokers’ newborns (mean −0.06 SDS, 95% CI: −0.07, −0.04) (Table 2). The unadjusted HC SDS in the smokers’ children continued to be smaller than in the non-smokers’ children throughout childhood. At 6 years, the mean unadjusted HC SDS of the smokers’ children was −0.29 SDS (95% CI: −0.33, −0.25), whereas that of the non-smokers’ children was −0.07 SDS (95% CI: −0.09, −0.06) (Table 2).
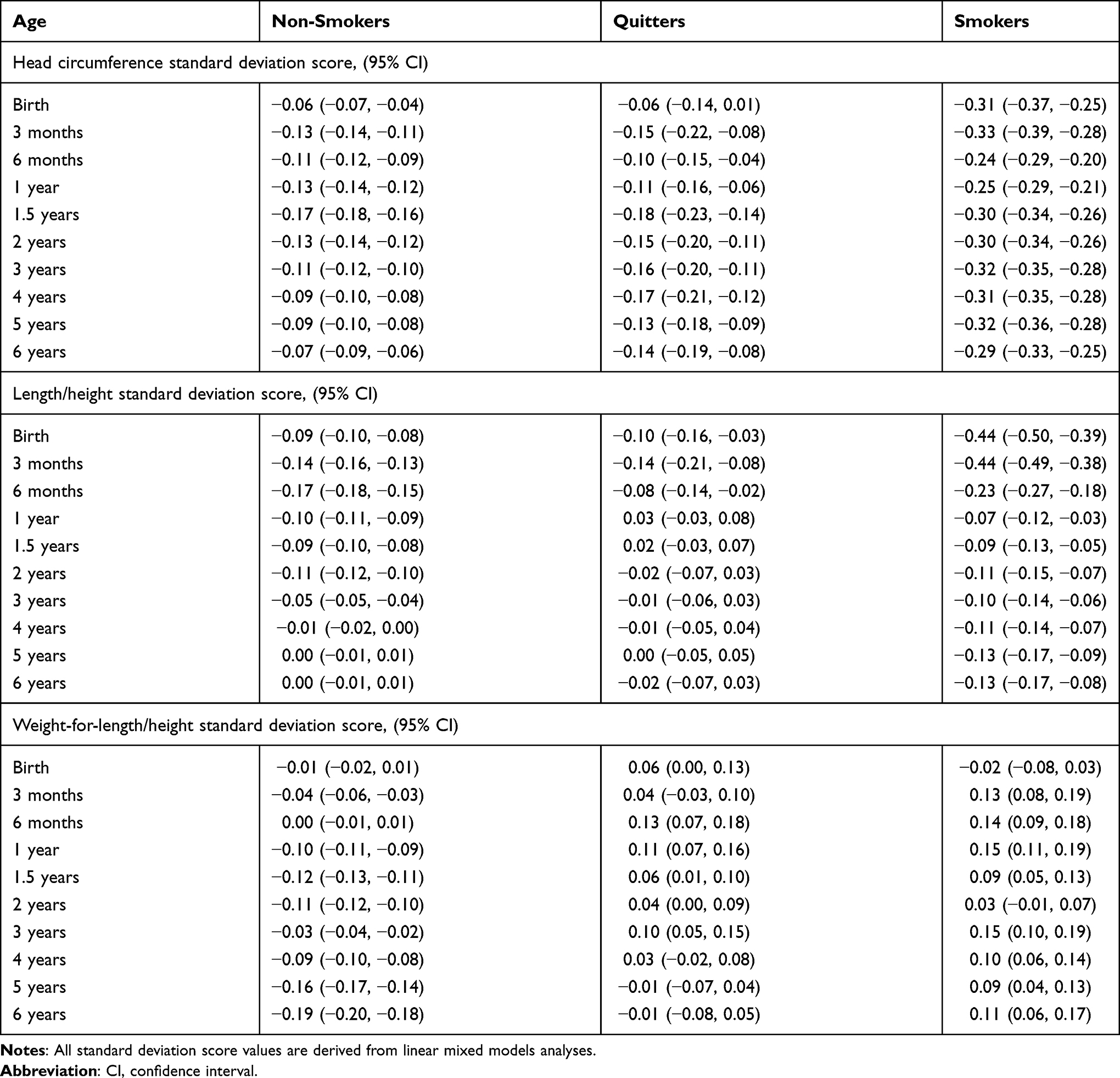 |
Table 2 Mean Unadjusted Standard Deviation Scores (Head Circumference, Length/Height, and Weight-for-Length/Height) by Maternal Smoking Status from Birth to 6 Years of Age |
After adjusting for confounding factors, the differences in HC SDS between smokers’ and non-smokers’ offspring remained significant from birth to 6 years of age (Figure 2A, Table 3). The adjusted HC of smokers’ infants at birth was on average 0.19 SDS smaller (95% CI: 0.12, 0.25) than in non-smokers’ (Figure 2A). The mean difference between the HC of smokers’ and non-smokers’ offspring at 6 years of age was −0.15 SDS (95% CI: −0.19, −0.10) (Figure 2A) corresponding to 2 mm.
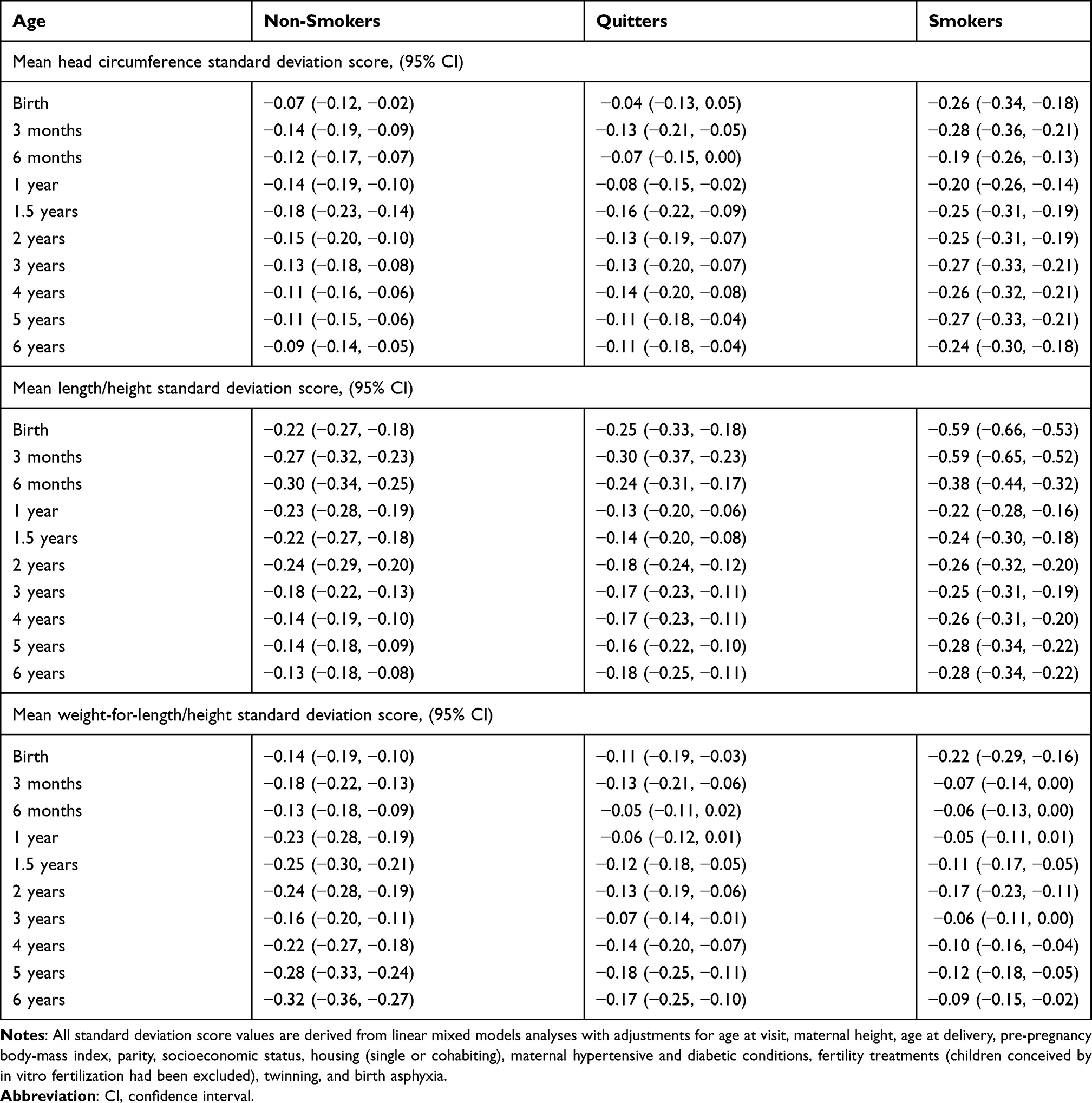 |
Table 3 Mean Adjusted Standard Deviation Scores for Head Circumference, Length/Height, and Weight-for-Length/Height by Maternal Smoking Status from Birth to 6 Years of Age |
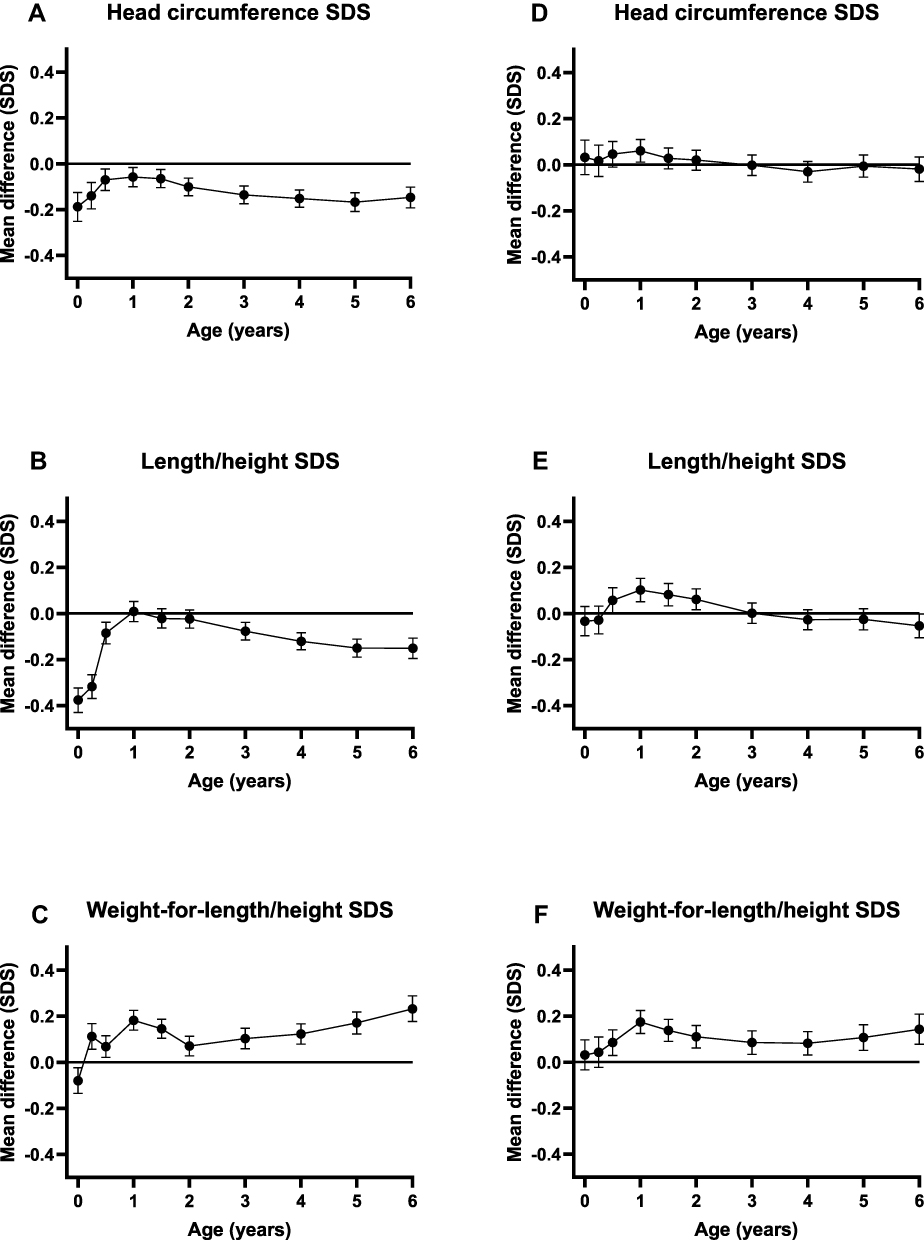 |
Figure 2 The mean difference in HC, length/height, and weight-for-length/height SDS from birth to 6 years of age between children of mothers who smoked during pregnancy and those of non-smoking mothers (marked as a line at zero), panels (A–C), and between children of mothers who quit smoking during first trimester and those of non-smoking mothers (marked as a line at zero), panels (D–F). Solid lines indicate the mean difference in (A and D) head circumference (HC), (B and E) length/height, and (C and F) weight-for-length/height. Error bars indicate 95% confidence intervals. Mean differences are derived from linear mixed models with adjustments for age at visit, maternal height, age at delivery, pre-pregnancy BMI, parity, socioeconomic status, housing (single or cohabiting), maternal hypertensive and diabetic conditions, fertility treatments (children conceived by in vitro fertilization had been excluded), twinning, and birth asphyxia. |
In the children of quitters, the mean unadjusted or adjusted HC SDS did not differ from HC SDS of non-smokers’ children from birth to 6 years of age (Figure 2D, Tables 2 and 3).
Length/Height and Weight-for-Length/Height
Smokers’ infants were shorter at birth compared with non-smokers’ infants (unadjusted and adjusted values, see Tables 2 and 3). At birth, the mean adjusted difference in weight-for-length was −0.08 SDS (95% CI: −0.14, −0.02) and in length −0.38 SDS (95% CI: −0.43, −0.32) (Figure 2B and C). The smokers’ offspring showed a distinct linear growth pattern during infancy. They caught up completely in weight and length by 1 year of age. Thereafter, they continued to gain weight, while the linear growth in height was stunted in comparison to non-smoking mothers’ offspring. Eventually, at 6 years of age, smokers’ children were heavier [weight-for-height difference 0.23 SDS (95% CI: 0.18, 0.29)] and shorter [height-for-age difference −0.15 SDS (95% CI: −0.20, −0.11), corresponding to 7 mm] than children whose mothers did not smoke during pregnancy (Figure 2B and C).
Offspring of those who quit smoking during the first trimester did not differ significantly in height growth from non-smokers’ offspring from birth to 6 years of age (Table 3, Figure 2E). However, offspring of quitters had an increased weight gain that was comparable to that of smokers’ children (Table 3, Figure 2F).
Discussion
We demonstrated that maternal smoking during pregnancy has a longstanding association with the offspring head circumference. After exposure to tobacco via maternal smoking during pregnancy, the HC catch-up growth during infancy and childhood was incomplete, resulting in a smaller HC in the smoker’s children than in the unexposed children at 6 years of age. This deficit was, however, small, corresponding to 0.2 cm at the age of 6 years. Reassuringly, HC growth of children whose mothers quit smoking during the first trimester did not differ from that of the offspring of non-smokers. Birth length and weight were reduced in newborns who had been exposed to maternal smoking, but they seemed to catch up to their unaffected counterparts during the first years of life.
The major strength of this study was the large study population with a long follow-up. The study cohort was assessed by a well-organized primary care system that performed repeated auxological checks. Compared to previous studies assessing association of maternal smoking during pregnancy with postnatal head growth, this study was larger, and the follow-up time was longer.15,18,23,29 The analyses were adjusted for potential confounders including socioeconomic status according to mother’s occupation.
A possible limitation of this study was that we did not have information on postnatal tobacco exposure by passive smoking or through breast milk. However, in a study of maternal smoking during lactation and growth, in a cohort of 1494 children,22 feeding type (bottle or breast) or postnatal exposure to tobacco smoke in the household did not play a significant role in growth from birth to 1 year of age. Moreover, mothers who quit smoking during pregnancy tend to start smoking again during the first months postpartum.30 Thus, our finding of the deficit in HC limited only to the offspring of smokers, not of quitters, suggests a stronger association between prenatal rather than postnatal tobacco exposure and offspring HC. Furthermore, we did not have information on the number of cigarettes smoked by the mother, which is why dose–response relationship could not be assessed. Another limitation of the study was that we did not have information on several other potential confounders, including other substance use, maternal psychiatric or neuropsychiatric conditions, or paternal characteristics. Socioeconomic status of the mother’s partner was not available, either. Even though we aimed to control for potential confounders, the association between maternal smoking in pregnancy and postnatal head growth of the offspring may involve residual confounding related to SES or to other familial confounding. As we were not able to use a family-based study design, it attenuates inferring of causality of the association. Furthermore, in the study population, non-smokers’ offspring was mildly under the mean SDS values of the growth references, which did not, however, affect the comparisons between the smoking groups. This observation might be due to ethnic differences between the Finnish growth reference of children born between 1983 and 2008, and the present cohort of children born between 2004 and 2017, the latter being probably more multi-ethnic. Average HC in children of Finnish origin has been shown to be larger than average HC depicted by the multiethnic WHO growth charts or reported from some other, especially non-Caucasian people.24,31 We could not include ethnicity in the analyses, because in Finland ethnicity is not recorded in perinatal or child health data. We know that since 2000 the part of Finland in which the study was conducted has had growing yearly net migration from abroad and in 2017 more than a quarter of childbirths were of foreign language speaking mothers.32 Smoking in pregnancy seems, though, to be rarer in migrants compared to the general population in Finland.33
In most previous studies, which assessed cohorts of 326 to 2151 infants, the catch-up in HC growth after maternal smoking during pregnancy was seen within 12 months.11,15,22,23 In children of heavy smokers, an HC deficit until 2 years of age18 or up to 5 years of age16 has been reported. In the latter study, statistical testing or adjustments for confounding factors were not done. Consistent with our study, a persisting deficit in HC was reported by a small prospective cohort study of 363 children,29 but, unlike our study, they did not observe any catch-up growth in smokers’ children. This previous study suffered from methodological issues concerning the longitudinal HC growth analysis; growth curves were made using the study’s own data for standardization, and no adjustments for confounding factors were made. In the cross-sectional analysis, they failed to show significant differences in HC between the offspring of smokers and non-smokers from 6 months to 5 years of age. Methodologically, the study most similar to ours was performed by Durmuş et al.13 Consistent with our findings, they reported an HC deficit at 1 year of age [−0.10 SDS (95% CI: −0.18, −0.01)] in the infants of smokers when compared with those of non-smokers. However, HC was not followed any further. Height growth in children of smokers was similarly deficient at 4 years of age in the study of Durmus et al13 (−0.10 SDS, 95% CI: −0.19, −0.01) and in ours (−0.12 SDS, 95% CI: −0.16, −0.08), and continued to be stunted in our study (mean difference at age 6 years −0.15 SDS, 95% CI: −0.20, −0.11). Our finding of higher weight-for-length/height in the children of smokers after 3 months of age compared with children of non-smokers was also consistent with Durmuş et al and other studies.14 On the contrary to the finding of Durmus et al, in our study, also the children of mothers who had quit smoking during the first trimester had an increased weight gain comparable to that of smokers’ children. An elevated risk for childhood overweight after maternal smoking during early pregnancy has been previously reported.34
HC is a surrogate measurement of brain size in childhood,19,20 and pre- and postnatal head growth is positively associated with neurocognitive outcome.35 Catch-up growth in HC after exposure to maternal smoking during pregnancy occurs during the first 6–12 months of life,11,22,36 when HC reaches already around 80% of its final size. In animal studies, prenatally administered nicotine resulted in reduced amounts of brain cells, and later neurons seemed to be replaced by glia.37,38 Thus, what was lost during fetal life, could not be fully repaired later. Studies investigating structural changes in offspring brain after maternal smoking during pregnancy have demonstrated reduced regional volumes in several cortical areas of the brain, in cerebellum, and corpus callosum.8,39–41 Deficits in total brain volume and in HC were observed still at ages 10–14 (N = 35) in children who had been prenatally exposed to tobacco, but the study failed to show significance when the results were adjusted for other substance use.41 Insulin-like growth factor-1 (IGF-1) is a major regulator of brain growth and development pre- and postnatally,42 and reduced plasma concentrations of IGF-1 have been measured in newborns after prenatal tobacco exposure.43 The risk of childhood overweight and obesity after prenatal tobacco exposure seems to be related with metabolic programming, through changes in epigenome44 and in IGF-growth factor axis.45 Metabolic programming may be involved with the stunted linear growth45 of these children as well.
Conclusions
Despite partial catch-up growth during the first months of life, head size in children of smoking mothers fails to achieve that of unexposed children. Because most HC growth occurs during the first 2 years of life, it is likely that the persisting gap between the HC of children of smoking and non-smoking mothers from birth to 6 years of age may be permanent. A defect in HC growth might be a rough measure of underlying cascades. All efforts should be taken to encourage pregnant women to quit smoking in order to protect the offspring brain.
Abbreviations
BMI, body-mass index; HC, head circumference; ICD-10, International Classification of Diseases, 10th version; SES, socioeconomic status; SDS, standard deviation score.
Statement on Ethics
This register-based study has been approved by the ethics committee of the Northern Savo Hospital District (DNr 64/2010) and permissions have been obtained from the register holders, the National Institute for Health and Welfare (THL/582/5.05.00/2009;
THL/504/5.05.00/2010;THL/1010/5.05.00/2018), Statistics Finland (TK-53-839-18/u1183_a) and Espoo Municipality Institutional Review Board (4.9.2008/DNo 1224).
Acknowledgments
We thank statisticians Marja-Leena Lamidi M.Sc. and Tuomas Selander M.Sc. for their valuable advice on statistical analyses.
Funding
This work was supported by Arvo and Lea Ylppö Foundation, Päivikki and Sakari Sohlberg Foundation, Finnish Medical Foundation, Kuopio University Hospital, State Research Funding and National Graduate School of Clinical Research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Euro-Peristat project with SCPE and Eurocat. European Perinatal health report. The health of pregnant women and babies in Europe in 2010; 2013. Available from: http://www.europeristat.com.
2. de Wolff MG, Backhausen MG, Iversen ML, Bendix JM, Rom AL, Hegaard HK. Prevalence and predictors of maternal smoking prior to and during pregnancy in a regional Danish population: a cross-sectional study. Reprod Health. 2019;16(1):1–9. doi:10.1186/s12978-019-0740-7
3. Curtin SC, Matthews TJ. Smoking prevalence and cessation before and during pregnancy: data from the birth certificate, 2014. Natl Vital Stat Rep. 2016;65(1):1–14.
4. Rice F, Langley K, Woodford C, Davey Smith G, Thapar A. Identifying the contribution of prenatal risk factors to offspring development and psychopathology: what designs to use and a critique of literature on maternal smoking and stress in pregnancy. Dev Psychopathol. 2018;30(3):1107–1128. doi:10.1017/S0954579418000421
5. Braun JM, Daniels JL, Kalkbrenner A, Zimmerman J, Nicholas JS. The effect of maternal smoking during pregnancy on intellectual disabilities among 8-year-old children. Paediatr Perinat Epidemiol. 2009;23(5):482–491. doi:10.1111/j.1365-3016.2009.01056.x
6. Abel EL. Smoking during pregnancy: a review of effects on growth and development of offspring. Hum Biol. 1980;52(4):593–625.
7. Lehtovirta P, Forss M. The acute effect of smoking on intervillous blood flow of the placenta. Br J Obstet Gynaecol. 1978;85(10):729–731. doi:10.1111/j.1471-0528.1978.tb15592.x
8. Bublitz MH, Stroud LR. Maternal smoking during pregnancy and offspring brain structure and function: review and agenda for future research. Nicotine Tob Res. 2012;14(4):388–397. doi:10.1093/ntr/ntr191
9. Buck JM, Yu L, Knopik VS, Stitzel JA. DNA methylome perturbations: an epigenetic basis for the emergingly heritable neurodevelopmental abnormalities associated with maternal smoking and maternal nicotine exposure. Biol Reprod. 2021;105:644–666.
10. Cliver SP, Goldenberg RL, Cutter GR, Hoffman HJ, Davis RO, Nelson KG. The effect of cigarette smoking on neonatal anthropometric measurements. Obstet Gynecol. 1995;85(4):625–630. doi:10.1016/0029-7844(94)00437-I
11. Ong KK, Preece MA, Emmett PM, Ahmed ML, Dunger DB; ALSPAC Study Team. Size at birth and early childhood growth in relation to maternal smoking, parity and infant breast-feeding: longitudinal birth cohort study and analysis. Pediatr Res. 2002;52(6):863–867. doi:10.1203/00006450-200212000-00009
12. Brand JS, Gaillard R, West J, et al. Associations of maternal quitting, reducing, and continuing smoking during pregnancy with longitudinal fetal growth: findings from Mendelian randomization and parental negative control studies. PLoS Med. 2019;16(11):e1002972. doi:10.1371/journal.pmed.1002972
13. Durmus B, Kruithof CJ, Gillman MH, et al. Parental smoking during pregnancy, early growth, and risk of obesity in preschool children: the Generation R Study. Am J Clin Nutr. 2011;94(1):164–171. doi:10.3945/ajcn.110.009225
14. Oken E, Levitan EB, Gillman MW. Maternal smoking during pregnancy and child overweight: systematic review and meta-analysis. Int J Obes. 2008;32(2):201–210. doi:10.1038/sj.ijo.0803760
15. Dunn HG, McBurney AK, Ingram S, Hunter CM. Maternal cigarette smoking during pregnancy and the child’s subsequent development: I. Physical growth to the age of 6 1/2 years. Can J Public Health. 1976;67(6):499–505.
16. Elwood PC, Sweetnam PM, Gray OP, Davies DP, Wood PD. Growth of children from 0–5 years: with special reference to mother’s smoking in pregnancy. Ann Hum Biol. 1987;14(6):543–557. doi:10.1080/03014468700009381
17. Martinez-Mesa J, Menezes AM, Gonzalez DA, et al. Life course association of maternal smoking during pregnancy and offspring’s height: data from the 1993 Pelotas (Brazil) birth cohort. J Adolesc Health. 2012;51(6Suppl):S53–s57. doi:10.1016/j.jadohealth.2012.08.014
18. Kanellopoulos TA, Varvarigou AA, Karatza AA, Beratis NG. Course of growth during the first 6 years in children exposed in utero to tobacco smoke. Eur J Pediatr. 2007;166(7):685–692. doi:10.1007/s00431-006-0308-8
19. Bartholomeusz HH, Courchesne E, Karns CM. Relationship between head circumference and brain volume in healthy normal toddlers, children, and adults. Neuropediatrics. 2002;33(5):239–241. doi:10.1055/s-2002-36735
20. Lindley AA, Benson JE, Grimes C, Cole TM, Herman AA. The relationship in neonates between clinically measured head circumference and brain volume estimated from head CT-scans. Early Hum Dev. 1999;56(1):17–29. doi:10.1016/S0378-3782(99)00033-X
21. Barr HM, Streissguth AP, Martin DC, Herman CS. Infant size at 8 months of age: relationship to maternal use of alcohol, nicotine, and caffeine during pregnancy. Pediatrics. 1984;74(3):336–341.
22. Boshuizen HC, Verkerk PH, Reerink JD, Herngreen WP, Zaadstra BM, Verloove-Vanhorick SP. Maternal smoking during lactation: relation to growth during the first year of life in a Dutch birth cohort. Am J Epidemiol. 1998;147(2):117–126. doi:10.1093/oxfordjournals.aje.a009423
23. Day N, Cornelius M, Goldschmidt L, Richardson G, Robles N, Taylor P. The effects of prenatal tobacco and marijuana use on offspring growth from birth through 3 years of age. Neurotoxicol Teratol. 1992;14(6):407–414. doi:10.1016/0892-0362(92)90051-B
24. Karvonen M, Hannila ML, Saari A, Dunkel L. New Finnish reference for head circumference from birth to 7 years. Ann Med. 2012;44(4):369–374. doi:10.3109/07853890.2011.558519
25. Saari A, Sankilampi U, Hannila ML, Kiviniemi V, Kesseli K, Dunkel L. New Finnish growth references for children and adolescents aged 0 to 20 years: length/height-for-age, weight-for-length/height, and body mass index-for-age. Ann Med. 2011;43(3):235–248. doi:10.3109/07853890.2010.515603
26. Sankilampi U, Hannila ML, Saari A, Gissler M, Dunkel L. New population-based references for birth weight, length, and head circumference in singletons and twins from 23 to 43 gestation weeks. Ann Med. 2013;45(5–6):446–454. doi:10.3109/07853890.2013.803739
27. Teperi J. Multi method approach to the assessment of data quality in the Finnish Medical Birth Registry. J Epidemiol Community Health. 1993;47(3):242–247. doi:10.1136/jech.47.3.242
28. Gissler M, Teperi J, Hemminki E, Meriläinen J. Data quality after restructuring a national medical registry. Scand J Soc Med. 1995;23(1):75–80. doi:10.1177/140349489502300113
29. Vik T, Jacobsen G, Vatten L, Bakketeig LS. Pre- and post-natal growth in children of women who smoked in pregnancy. Early Hum Dev. 1996;45(3):245–255. doi:10.1016/0378-3782(96)01735-5
30. Jones M, Lewis S, Parrott S, Wormall S, Coleman T. Re-starting smoking in the postpartum period after receiving a smoking cessation intervention: a systematic review. Addiction. 2016;111(6):981–990. doi:10.1111/add.13309
31. Natale V, Rajagopalan A. Worldwide variation in human growth and the World Health Organization growth standards: a systematic review. BMJ Open. 2014;4(1):e003735. doi:10.1136/bmjopen-2013-003735
32. Sipilä S Väestötietoisku_ lopullinen-1.pdf: Espoon väestönmuutokset vuonna; 2017. Available from: https://www.sttinfo.fi/tiedote/tilastot-ja-tutkimukset–kuukausitiedote-helmikuu-2019?publisherId=3385&releaseId=69852911.
33. Bastola K, Koponen P, Härkänen T, Luoto R, Gissler M, Kinnunen TI. Delivery and its complications among women of Somali, Kurdish, and Russian origin, and women in the general population in Finland. Birth. 2019;46(1):35–41. doi:10.1111/birt.12357
34. Oken E, Huh SY, Taveras EM, Rich-Edwards JW, Gillman MW. Associations of maternal prenatal smoking with child adiposity and blood pressure. Obes Res. 2005;13(11):2021–2028. doi:10.1038/oby.2005.248
35. Emond AM, Lira PI, Lima MC, Grantham-McGregor SM, Ashworth A. Development and behaviour of low-birthweight term infants at 8 years in northeast Brazil: a longitudinal study. Acta Paediatr. 2006;95(10):1249–1257. doi:10.1080/08035250600615127
36. Fenercioglu AK, Tamer I, Karatekin G, Nuhoglu A. Impaired postnatal growth of infants prenatally exposed to cigarette smoking. Tohoku J Exp Med. 2009;218(3):221–228. doi:10.1620/tjem.218.221
37. Slotkin TA, Orband-Miller L, Queen KL, Whitmore WL, Seidler FJ. Effects of prenatal nicotine exposure on biochemical development of rat brain regions: maternal drug infusions via osmotic minipumps. J Pharmacol Exp Ther. 1987;240(2):602–611.
38. Slotkin TA. Fetal nicotine or cocaine exposure: which one is worse? J Pharmacol Exp Ther. 1998;285(3):931–945.
39. de Zeeuw P, Zwart F, Schrama R, van Engeland H, Durston S. Prenatal exposure to cigarette smoke or alcohol and cerebellum volume in attention-deficit/hyperactivity disorder and typical development. Transl Psychiatry. 2012;2:e84. doi:10.1038/tp.2012.12
40. Ekblad M, Korkeila J, Parkkola R, et al. Maternal smoking during pregnancy and regional brain volumes in preterm infants. J Pediatr. 2010;156(2):185–90.e1. doi:10.1016/j.jpeds.2009.07.061
41. Rivkin MJ, Davis PE, Lemaster JL, et al. Volumetric MRI study of brain in children with intrauterine exposure to cocaine, alcohol, tobacco, and marijuana. Pediatrics. 2008;121(4):741–750. doi:10.1542/peds.2007-1399
42. Dyer AH, Vahdatpour C, Sanfeliu A, Tropea D. The role of Insulin-Like Growth Factor 1 (IGF-1) in brain development, maturation and neuroplasticity. Neuroscience. 2016;325:89–99. doi:10.1016/j.neuroscience.2016.03.056
43. Pringle PJ, Geary MP, Rodeck CH, Kingdom JC, Kayamba-Kay’s S, Hindmarsh PC. The influence of cigarette smoking on antenatal growth, birth size, and the insulin-like growth factor axis. J Clin Endocrinol Metab. 2005;90(5):2556–2562. doi:10.1210/jc.2004-1674
44. Rogers JM. Smoking and pregnancy: epigenetics and developmental origins of the metabolic syndrome. Birth Defects Res. 2019;111(17):1259–1269. doi:10.1002/bdr2.1550
45. Puche JE, Castilla-Cortázar I. Human conditions of insulin-like growth factor-I (IGF-I) deficiency. J Transl Med. 2012;10:224. doi:10.1186/1479-5876-10-224
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.