Back to Journals » Infection and Drug Resistance » Volume 16
Maternal Infection with Listeria monocytogenes in Twin Pregnancy
Authors Huang P ![]() , Guo X
, Guo X ![]() , Duan M
, Duan M ![]() , Li H, Han C
, Li H, Han C ![]() , Xue F
, Xue F
Received 5 February 2023
Accepted for publication 21 April 2023
Published 27 April 2023 Volume 2023:16 Pages 2511—2518
DOI https://doi.org/10.2147/IDR.S407244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Pengzhu Huang,1,2,* Xin Guo,1,2,* Mengke Duan,1,2 Huanrong Li,1,2 Cha Han,1,2 Fengxia Xue1,2
1Department of Gynecology and Obstetrics, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China; 2Tianjin Key Laboratory of Female Reproductive Health and Eugenics, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fengxia Xue; Cha Han, Department of Gynecology and Obstetrics, Tianjin Medical University General Hospital, Tianjin, China; Tianjin Key Laboratory of Female Reproductive Health and Eugenics, Tianjin Medical University General Hospital, Tianjin, People’s Republic of China, Tel +86-22-60363769, Fax +86-22-27813550, Email [email protected]; [email protected]
Abstract: Listeria monocytogenes is the conditional pathogenic bacteria, and pregnant women are at higher risk of infection due to depressed immunity. Infection with Listeria monocytogenes in twin pregnancy is rare but devastating, which puts forwards a great challenge for clinical management. Here, a 24-year-old woman was diagnosed with twin pregnancy, intrauterine death of one fetus and fever at 29+4 week of gestation. Two days later, she developed into pericardial effusion, pneumonedema and potential septic shock. The emergent cesarean delivery was performed after anti-shock treatment. One alive and another dead fetus were delivered. Then, she developed postpartum hemorrhage after the surgery. Urgent exploratory laparotomy was conducted at the sites of cesarean section and B-Lynch suture to stop bleeding. The culture of blood and maternal side of both placentas indicated Listeria monocytogenes. Following anti-infection therapy with ampicillin-sulbactam, she recovered well and discharged with negative result of blood bacterial culture and normal inflammatory indicators. The patient was hospitalized for a total of 18 days including 2 days in the intensive care unit (ICU), and the anti-infection treatment was conducted throughout the course. Symptoms of the Listeria monocytogenes infection in pregnancy are non-specific, which should be paid more attention in case of unexplained fever and fetal distress. The blood culture is effective for accurate diagnosis. Listeria monocytogenes infection is associated with poor pregnancy outcomes. Close monitoring of fetal condition, early intervention with antibiotics, timely termination of pregnancy and comprehensive management of complications are essential for better prognosis.
Keywords: Listeria monocytogenes, twin pregnancy, outcomes
Introduction
Listeriosis is a foodborne infection caused by the pathogenic agent Listeria monocytogenes. Listeria monocytogenes inhibits widely in the environment and could be isolated from soil, water and vegetation; in addition, it is psychrophilic and capable of surviving at low temperature like in the refrigerator.1 Listeriosis is usually transmitted through contaminated processed and ready-to-eat food. Sporadic cases and outbreak of foodborne listeriosis have been reported to be caused by dairy products, fruits and vegetables, meat or fish products like deli meats.1 One prospective study reported that healthy people had 5 to 9 exposures to Listeria monocytogenes per person per year.2 Once ingested food contaminating with large amounts of Listeria monocytogenes, the innate host-defense system in the digestive system would be impaired that could further lead to invasive disease.1 Epidemiological studies have indicated that infection of Listeria monocytogenes is rare but relatively lethal. In the United States, the overall annual incidence of listeriosis ranged from 0.25 to 0.32 cases per 100,000 population from 2004 to 2009, but the fatality rate was high as 18%.3 Furthermore, the annual incidence varied from 0.26 to 0.31 cases per 100,000 population in the period from 2008 to 2016 in the United States.4 In Europe, the incidence of listeriosis was 0.42 per 100,000 population in 2020 and the overall fatality rate was 13.0%.5
Compared with the general population, pregnant women are at nearly 10 to 20 times risk to the infection of Listeria monocytogenes due to compromised immunity.6 In the United States, the annual incidence of listeriosis in the period from 2008 to 2016 was 0.23 to 0.27 non-pregnant cases per 100,000 population, but it increased to 2.59 to 4.92 per 100,000 population for pregnant-associated cases.4 In Germany, 5576 listeriosis cases have been reported from 2010 to 2019 and pregnancy-associated cases accounted for nearly 9% of them (n = 486) with 241 maternal and 245 neonatal cases.7 Similarly, 5696 patients hospitalized for listeriosis in Spain from 1997 to 2015 and 7% and 4% of whom were pregnant women and newborns, respectively.8 The infected pregnant women are often asymptomatic or manifest with non-specific flu-like or gastrointestinal symptoms.9 However, the diagnosis of listeriosis may be easily ignored due to non-specific clinical manifestations and infection with Listeria monocytogenes is usually associated with poor outcomes. One study enrolled 134 pregnant women hospitalized for Listeria infection from 2007 to 2018 in the United States and found that the risk of severe maternal morbidity was 21.2-time higher in women with Listeria during pregnancy than in those without, specifically the risk of sepsis (28.1% vs 0.1%, P < 0.001), shock (1.4% vs 0.0%, P < 0.001) and acute respiratory distress syndrome (2.8% vs 0.1%, P < 0.001).10 In addition, maternal infection could be transmitted vertically to the fetus, leading to fetal or neonatal infection with severe complications like fetal distress, preterm birth, miscarriage or stillbirth, neonatal sepsis, neonatal asphyxia and meningitis.9 Therefore, it remains huge challenge for accurate diagnosis and timely treatment of Listeria monocytogenes infection.
Here, we report a case of infection with Listeria monocytogenes in twin pregnancy that developed into septic shock and delivered one alive but another dead fetus. Maternal infection of Listeria monocytogenes in twin pregnancy is rarely reported but associated with poor fetal outcomes. Besides, this case presented with severe maternal complications, which are different from commonly reported non-specific symptoms. Therefore, analysis of clinical features of this disease and our management experience may help clinical management in similar conditions.
Case Presentation
The 24-year-old woman, gravida 2, para 1, was admitted to another hospital at 29+1 week of gestation for fever of 39.2°C and right low abdominal pains. She was diagnosed with ovarian cyst at early pregnancy. Doppler ultrasound showed dichorionic-diamniotic twin pregnancy; both fetuses showed increased fetal heart rate of 164bpm and 180bpm, respectively, indicating the potential intrauterine hypoxia; the latter fetus had a little ascites. White blood cell (WBC) count was 19.85×109/L, neutrophils 84.9% and C-reactive protein (CRP) 20.22mg/L. Although oral cephalosporin was taken in the following days, the temperature still fluctuated at 37.5 to 38.6°C. TORCH tests were performed in the first trimester, and the results were negative, including toxoplasmosis, rubella, cytomegalovirus, and herpes simplex virus. The results of serological status for other pathogens such as syphilis, gonococcus, trichomonad, mycotoxin, human immunodeficiency virus, hepatitis B virus and hepatitis C virus were also negative.
At 29+4 week of gestation, she was transferred to our hospital due to intrauterine death of one fetus for half-day. Her temperature was 36.6°C, and WBC count was 22.14×109/L, neutrophils 81.6%, CRP 195.76mg/L. Intravenous injection of cefuroxime sodium and intramuscular injection of dexamethasone sodium phosphate were administered for anti-infection and promoting fetal lung maturation. On the 2nd day evening, she had chest distress and could not lie flat. The blood gas analysis revealed PH 7.456, PCO2 28.4 mmHg, PO2 75.7 mmHg, Ca2+ 0.94mmol/L, K+ 3.01mmol/L. Nasal cannula oxygen therapy and supplement with calcium and potassium were prescribed. On the 3rd day morning, chest distress recurred. Her temperature increased to 39.5°C and blood pressure decreased to 105/59 mmHg. The routine blood examination showed WBC count 12.6×109/L, red blood cell (RBC) count 3.71×1012/L, hemoglobin 80g/L, neutrophils 86.5%, lymphocyte 6.8%. The blood biochemical examination showed Ca2+ 2.00mmol/L, K+ 3.4mmol/L, Na+ 134mmol/L, albumin 29g/L, brain natriuretic peptide (BNP) 175.0pg/mL. Since there is potential bacterial infection, blood culture was administered to identify the pathogen. The chest Computed Tomography (CT) indicated cardiac insufficiency and pulmonary edema (Figure 1). After the consultation of Multi-Disciplinary Treatment (MDT) group, heart failure, pulmonary edema with infection, respiratory alkalosis with metabolic acidosis and intrauterine infection of Listeria monocytogenes were considered and anti-infection with ampicillin-sulbactam was started.
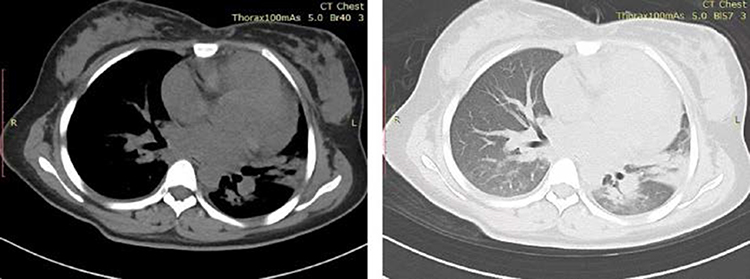 |
Figure 1 Chest CT images of the patient on the 3rd day of admission showed enlarged heart shadow, pericardial effusion, ground-glass opacity and patchy consolidation as well as thickened bronchovascular bundle in bilateral lung. |
On the 3rd day afternoon, there is still hypotension of 102/58 mmHg and hypoxemia of PO2 67.9 mmHg. The caesarean section was considered to reduce maternal cardiopulmonary burden. On the way to operating room, the patient could not lie flat. Her blood pressure decreased dramatically to 60–70/40–50 mmHg with increased heart rate of 120–140 bpm, indicating there was potential septic shock. After anti-shock treatment, general anesthesia and immediate cesarean section were conducted. One alive fetus of 1505g was delivered, and the Apgar score at 1, 5 and 10 minutes was 8, 10 and 10, respectively. The other fetus was dead, and the amniotic fluid was aeruginous. Maternal side of both placentas and fetal membrane was swabbed for the bacterial culture. The uterus was limp and feeble without any contraction. Bilateral uterine artery ligation was performed, which effectively reduced intrauterine haemorrhage. Additional B-Lynch suture enhanced the uterine contraction. After the surgery, the patient was transferred to intensive care unit (ICU) with blood pressure of 90/60 mmHg, heart rate of 115 bpm and SPO2 93%. According to the instructions of obstetrician, ampicillin-sulbactam and oxytocin were prescribed for anti-infection and promotion of postpartum uterine involution, respectively.
However, 1350 mL blood-like liquid was drained from pelvic cavity 4.5 hours after the surgery. Despite hemostasis therapy like cryoprecipitate and erythrocyte suspension infusion, the potential hemorrhage was not corrected with blood pressure 98/66 mmHg and hemoglobin 50g/L. Thus, an urgent exploratory laparotomy was performed. The uterus contracted poorly and blood oozed at the sites of cesarean section and B-Lynch suture, which were corrected by hemostatic suture and oxytocin injection into the myometrium. A total of 900mL plasma, 1600mL erythrocyte suspension and 10U cryoprecipitate were infused during surgery, after which the patient’s condition had been improved with blood pressure 105/75mmHg, heart rate 88bpm, SPO2 99% and hemoglobin 80g/L. Following mechanical ventilation, hemostasis and anti-infection therapy in the ICU, the patient recovered well with blood pressure 110/78mmHg, heart rate 84bpm, SPO2 100%. Two days after surgery, condition of the patient has improved with the body temperature 36.5°C, blood pressure 122/81mmHg and heart rate 73bpm. Therefore, she was transferred to the department of obstetrics and ampicillin-sulbactam was continued for anti-infection.
The result of blood and placenta tissue culture verified Listeria monocytogenes infection. Pathological examination of the alive fetus showed multifocal fibrinous exudate and focal infarction in the placenta. Meanwhile, the dead fetus manifested with regional infarction, extensive inflammatory cell infiltration and multifocal abscess in the placenta as well as acute inflammation and infarction in the fetal membrane. Following treatment with ampicillin-sulbactam for 16 days, the patient recovered well with no signs of fever. The blood culture revealed negative of bacteria and inflammatory indicators were normal with WBC count 7.07×109/L and neutrophils 44%. The patient was discharged on the 18th day of admission. Results of the laboratory test of the patient during the hospitalization are shown in Table 1.
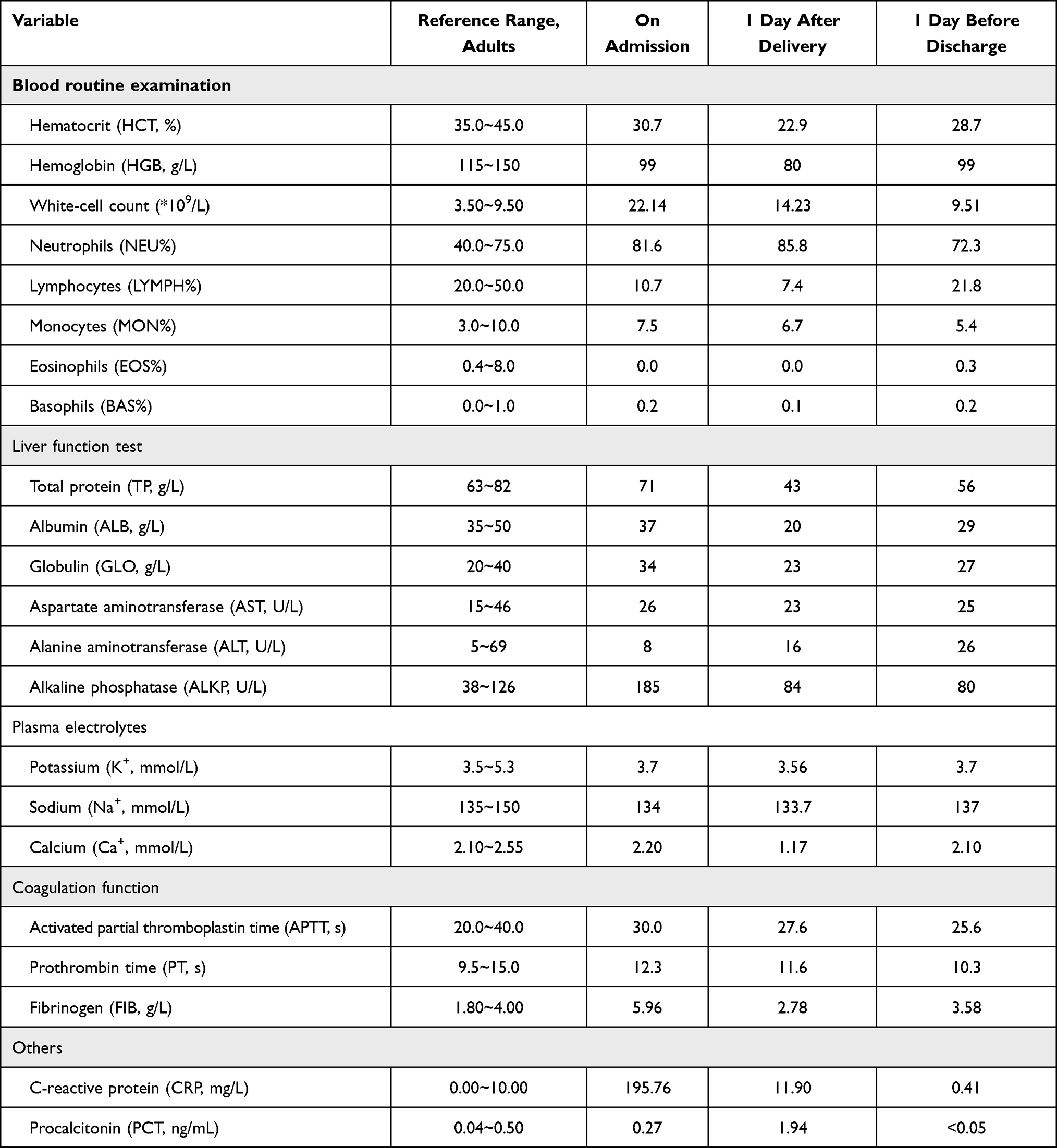 |
Table 1 Results of the Laboratory Test |
The survived newborn was admitted to the neonatal ICU (NICU) of our hospital one day after delivery (correspondence to the 30th gestational week) due to difficult feeding and repeated vomiting. He was diagnosed with neonatal dehydration, premature and low birth weight infant and suspected of neonatal sepsis and intracranial infection. The lumbar puncture was conducted to obtain cerebrospinal fluid (CSF) for further examination. And CSF was transparent and yellow but “1+” for Pandy test. Besides, aerobic cultures of whole blood and CSF showed no colony formation. The brain MRI did not show any abnormalities. The coagulation function was disordered with prolonged PT (22.0 seconds) and APTT (75.2 seconds) as well as elevated level of D-dimer (553ng/mL). The newborn was treated with anti-infection and nutrition support. His condition was closely monitored, and several episodes of apnea were presented during the hospitalization. However, condition of the newborn suddenly deteriorated on the 29th days of admission (at the 34th gestational week) with blood pressure 74/47 mmHg and SPO2 68%, hs-CRP >5 mg/L, CRP 75.42 mg/L, PCT 13.356 ng/mL. Therefore, the newborn was diagnosed with neonatal sepsis and treated with meropenem and immune globulin in addition to other supportive interventions. Furthermore, the newborn presented with feeding refusal and abdominal distension. The abdominal plain radiography showed multiple sites with gas accumulation in the intestine. The potential neonatal necrotizing enterocolitis was considered according to the clinical presentations and examinations. Finally, family members of the newborn decided to transfer to the Department of Pediatric Surgery in another hospital for further therapy.
During the follow-up, the patient had been readmitted with fever at the 4th week after first discharge from our hospital. Blood tests were performed, which showed an increased WBC count (10.09×109/L) but a normal neutrophil ratio (62.8%) as well as normal CRP (15.69 mg/L). The blood culture was performed to verify the potential Listeria monocytogenes reinfection, but there was no colony formation. The CT scan of the chest indicated relieving of conditions of the heart and lung (Figure 2). The brain MRI indicated that there were no abnormalities of the brain except for the inflammation in bilateral ethmoid sinus and maxillary sinus (Figure 3). The timeline of the patient’s disease course since the admission to our hospital is shown in Figure 4.
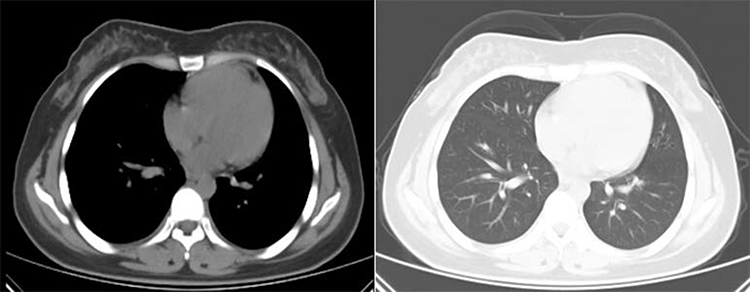 |
Figure 2 Chest CT images of the patient 4 weeks after discharge. Compared with the findings on the 3rd day of admission, there was decreased ground-glass opacity and patchy consolidation as well as thinner bronchovascular bundle in the both lungs. The heart shadow and pericardial effusion as well as pleural effusion were also reduced. |
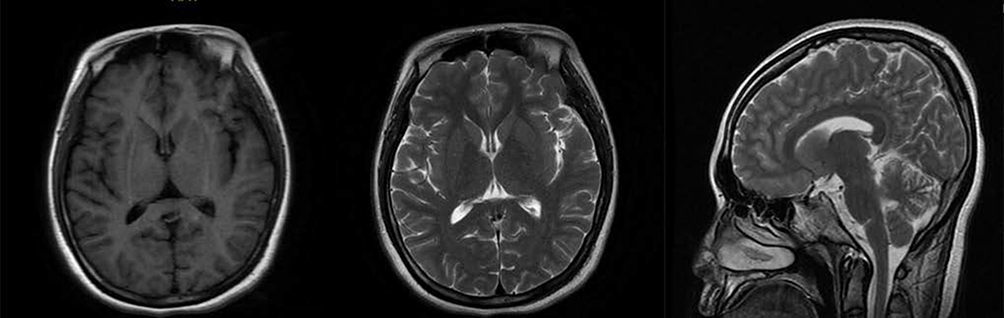 |
Figure 3 Brain MRI images of the patient 4 weeks after discharge. There were no abnormalities in the morphology of bilateral cerebral hemispheres, cerebellum and brain stem. The cerebral ventricle did not dilate and cerebral sulci or fissure did not widen. However, shadow of the mucosa of bilateral ethmoid sinus and maxillary sinus was thickened. |
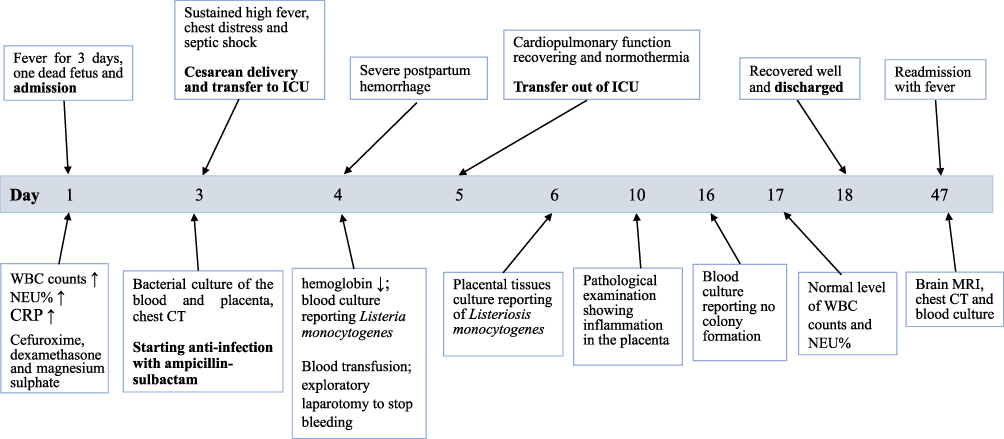 |
Figure 4 Timeline of clinical presentations, examination and treatment of the patient since the admission to our hospital. Key results were: (1) The twin-pregnant women was admitted with fever for 3 days and one dead fetus; (2) On the 3th day of admission, the patient still had fever and presented with chest distress, breathlessness and potential septic shock; the cesarean section was performed after anti-shock therapy and one alive newborn was delivered; ampicillin-sulbactam was used since then for the potential Listeria monocytogenes infection; (3) On the 4th day, severe postpartum hemorrhage occurred and blood transfusion as well as exploratory laparotomy were conducted to stop bleeding; (4) On the 4th and 6th day of admission, Listeria monocytogenes infection was identified through culture of blood and placenta tissue, respectively; (5) On the 16th day, the placenta tissue culture found no colony formation; (6) On the 18th day, the patient was discharged; (7) On the 47th day (4 weeks after discharge), the patient was readmitted with fever. The blood culture result was negative. |
Discussion
Listeria monocytogenes is a gram-positive, aerobic and facultative anaerobe that could cause illness in human. As a food-borne pathogen, it is transmitted mostly through processed and ready-to-eat food such as refrigerated meat, milk and vegetables. In addition to dietary habits, immunity may be another important factor that influences the susceptibility of listeriosis. The annual incidence of listeriosis ranges from 1 to 10 per million people worldwide, and pregnant women are at 16- to 18-fold higher risk of infection than the general population.11 Since listeria monocytogenes could be transmitted vertically to the fetus, it is alarming that there may be poor maternal, fetal and neonatal outcomes such as miscarriage, preterm birth, fetal stillbirth, neonatal distress, septicemia, meningitis and central nervous system infection.12
Infection with Listeria monocytogenes could occur throughout the pregnancy.13 However, symptom of Listeria monocytogenes infection in pregnancy is non-specific, which is difficult to be diagnosed accurately. Wu et al13 reported that the initial clinical symptom of 93 pregnant women with listeria monocytogenes infection was fever (96.8%), intermittent lower abdominal pain (53.8%), abnormal fetal movement and/or abnormal fetal heartbeat (29.0%). Some symptoms are usually found in other diseases such as gastrointestinal or respiratory tract infections; thus, listeriosis is easily neglected. Median time from symptom onset to clinical visit is 3.4 (0.1–19) days.14 Therefore, delay of the diagnosis may affect subsequent treatment and even cause serious pregnancy outcomes. Symptoms like fever or fetal distress may indicate Listeria monocytogenes infection and should be paid attention. The etiological detection is essential for the accurate diagnosis if there was unexplained fever.
Despite the absence or non-specificity of symptoms, maternal infection with Listeria monocytogenes is usually associated with poor pregnancy outcomes, which is destructive for the fetus and neonates. One prospective study conducted in France reported that only 5% of pregnant women with listeriosis had an uneventful outcome; more than 80% of pregnant women with infection had severe complications such as fetal loss (26%, 24/107) and premature delivery before 32 gestational weeks (19%, 20/107).15 The gestational age at the time of maternal listeriosis has a significant impaction on the fetal outcomes. One cohort study enrolling 166 patients with pregnancy-related listeriosis in Israel found that abortion was common in the second trimester than in the third trimester (55.3% vs 1.5%), whereas preterm labor (27.7% vs 52.3%) and abnormal fetal heart rate monitoring (0 vs 22.2%) were less common in the second trimester.16 In addition, incidence of fetal viability was higher in the third trimester (95.3%) than in the second trimester (29.2%) and one week of pregnancy increased 33% chance of live birth.16 Maternal listeriosis combined with other complicated conditions put both the mother and the fetus at higher risk. One study reported that one pregnant woman with listeriosis, sepsis and preterm premature rupture of membranes delivered a live neonate, but the neonate was dead shortly after birth.17 In addition, several studies have reported that maternal listeriosis with twin pregnancy is associated with poor outcomes such as septicemia, postpartum hemorrhage, premature delivery, fetal or neonatal death and infant listeriosis.12,18,19
Once pregnant women are presumptively exposed to Listeria monocytogenes and have fever higher than 38.1°C with or without other symptoms, blood and placenta culture, fetal surveillance as well as timely antibiotics are recommended to minimize potential poor pregnancy outcomes.20 Antenatal maternal antimicrobial therapy has been reported to be correlated with lowering the severity of neonatal listeriosis, indicating the necessity of antimicrobial treatment when there are signs of listeriosis.21 Penicillins are sensitive to Listeria monocytogenes infection, and ampicillin is an effective drug of choice, whereas cephalosporin antibiotics are not active against it.22 However, cephalosporins are often used initially for unidentified infection, which may be caused by non-specific symptoms and time-consuming blood culture. Therefore, it is important for obstetricians to comprehensively consider the patients’ condition and examination results.
There are certain limitations in the current study as follows. Firstly, this study reported the clinical features of one case with Listeria monocytogenes infection in twin pregnancy, focusing on the dynamic clinical changes and outcomes of the patient. However, the number of enrolled subjects is too small so that we could not come to the uniform conclusion of this condition, which should be verified in more patients. Secondly, this study mainly described the clinical presentation and prognosis of the patient which was rarely reported in clinic but without the evidence proving the direct causality between twin pregnancy and infection with Listeria monocytogenes. Since Listeria monocytogenes infection in pregnancy may be caused by impaired immunity, whether twin pregnancy aggravates this impairment and leads to the infection is currently unknown.
Conclusion
Twin pregnancy with the Listeria monocytogenes infection is rarely reported but devastating with poor maternal and fetal prognosis. Infection of Listeria monocytogenes should be considered if pregnant women had fever and fetal distress. Timely diagnosis, close monitoring and anti-infection with ampicillin may help to obtain optimal outcomes.
Informed Consent and Ethical Approval
This study complies with ethical standards and informed consent for publication of the personal information and clinical data have been obtained from the patient.
Funding
This study was supported by National Nature Science Foundation of China (Grant 82071674 and Grant 81972448), Beijing‐Tianjin‐Hebei Basic Research Cooperation Project (22JCZXJC00160) and Tianjin Key Medical Discipline (Specialty) Construction Project.
Disclosure
Pengzhu Huang and Xin Guo contributed equally to this work as co-first authors. The authors declare that they have no conflict of interests.
References
1. Schlech WF, Fischetti VA, Novick RP. Epidemiology and clinical manifestations of Listeria monocytogenes infection. Microbiol Spectr. 2019;7(3). doi:10.1128/microbiolspec.GPP3-0014-2018
2. Grif K, Patscheider G, Dierich MP, Allerberger F. Incidence of fecal carriage of Listeria monocytogenes in three healthy volunteers: a one-year prospective stool survey. Eur J Clin Microbiol Infect Dis. 2003;22(1):16–20. doi:10.1007/s10096-002-0835-9
3. Silk BJ, Date KA, Jackson KA, et al. Invasive listeriosis in the Foodborne Diseases Active Surveillance Network (FoodNet), 2004–2009: further targeted prevention needed for higher-risk groups. Clin Infect Dis. 2012;54(Suppl 5):S396–404. doi:10.1093/cid/cis268
4. Pohl AM, Pouillot R, Bazaco MC, et al. Differences among incidence rates of invasive listeriosis in the US FoodNet population by age, sex, race/ethnicity, and pregnancy status, 2008–2016. Foodborne Pathog Dis. 2019;16(4):290–297. doi:10.1089/fpd.2018.2548
5. The European Union One Health. 2020 zoonoses report. EFSA J. 2021;19(12):e06971. doi:10.2903/j.efsa.2021.6971
6. Khsim IEF, Mohanaraj-Anton A, Horte IB, et al. Listeriosis in pregnancy: an umbrella review of maternal exposure, treatment and neonatal complications. BJOG. 2022;129(9):1427–1433. doi:10.1111/1471-0528.17073
7. Wilking H, Lachmann R, Holzer A, Halbedel S, Flieger A, Stark K. Ongoing high incidence and case-fatality rates for invasive listeriosis, Germany, 2010–2019. Emerg Infect Dis. 2021;27(9):2485–2488. doi:10.3201/eid2709.210068
8. Herrador Z, Gherasim A, López-Vélez R, Benito A. Listeriosis in Spain based on hospitalisation records, 1997 to 2015: need for greater awareness. Euro Surveill. 2019;24(21). doi:10.2807/1560-7917.ES.2019.24.21.1800271
9. Madjunkov M, Chaudhry S, Ito S. Listeriosis during pregnancy. Arch Gynecol Obstet. 2017;296(2):143–152. doi:10.1007/s00404-017-4401-1
10. Craig A, Federspiel J, Wein L, Thompson J, Dotters-Katz S. Maternal and obstetric outcomes of listeria pregnancy: insights from a national cohort. J Matern Fetal Neonatal Med. 2022;35(25):10010–10016. doi:10.1080/14767058.2022.2083494
11. Craig AM, Dotters-Katz S, Kuller JA, Thompson JL. Listeriosis in pregnancy: a review. Obstet Gynecol Surv. 2019;74(6):362–368. doi:10.1097/OGX.0000000000000683
12. Li C, Zeng H, Ding X, et al. Perinatal listeriosis patients treated at a maternity hospital in Beijing, China, from 2013–2018. BMC Infect Dis. 2020;20(1):601. doi:10.1186/s12879-020-05327-6
13. Xu L, Du Y, Wu Y. Neglected listeria infection in pregnancy in China: 93 cases. J Matern Fetal Neonatal Med. 2022;35(25):9549–9557. doi:10.1080/14767058.2022.2047925
14. Kuang L, Lai Y, Gong Y. Analysis of listeriosis infection cases during pregnancy among 70 131 deliveries. J Obstet Gynaecol Res. 2022;48(1):66–72. doi:10.1111/jog.15063
15. Charlier C, Perrodeau É, Leclercq A, et al. Clinical features and prognostic factors of listeriosis: the MONALISA national prospective cohort study. Lancet Infect Dis. 2017;17(5):510–519. doi:10.1016/S1473-3099(16)30521-7
16. Elinav H, Hershko-Klement A, Valinsky L, et al. Pregnancy-associated listeriosis: clinical characteristics and geospatial analysis of a 10-year period in Israel. Clin Infect Dis. 2014;59(7):953–961. doi:10.1093/cid/ciu504
17. Dunphy L, Polkampali M, Simmons W, Fowler G. Maternal sepsis caused by Listeria monocytogenes with a fatal fetal outcome. BMJ Case Rep. 2022;15(10):e249989. doi:10.1136/bcr-2022-249989
18. Lu B, Wu J, Yang J, Cui Y. Listeriosis in two twin pregnancies after in vitro fertilization with differential outcome and literature review. J Matern Fetal Neonatal Med. 2019;32(10):1741–1746. doi:10.1080/14767058.2017.1410790
19. Joshi MS, Matthews M. Intrauterine infection of non-presenting twin: a rare occurrence. J Obstet Gynaecol. 2006;26(6):569–570. doi:10.1080/01443610600821663
20. Pucci L, Massacesi M, Liuzzi G. Clinical management of women with listeriosis risk during pregnancy: a review of national guidelines. Expert Rev Anti Infect Ther. 2018;16(1):13–21. doi:10.1080/14787210.2018.1417837
21. Charlier C, Kermorvant-Duchemin E, Perrodeau E, et al. Neonatal listeriosis presentation and outcome: a prospective study of 189 cases. Clin Infect Dis. 2022;74(1):8–16. doi:10.1093/cid/ciab337
22. Temple ME, Nahata MC. Treatment of listeriosis. Ann Pharmacother. 2000;34(5):656–661. doi:10.1345/aph.19315
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.