Back to Journals » International Journal of Women's Health » Volume 15
Maternal Health Care Utilization Behavior, Local Wisdom, and Associated Factors Among Women in Urban and Rural Areas, Indonesia
Authors Damayanti NA ![]() , Wulandari RD
, Wulandari RD ![]() , Ridlo IA
, Ridlo IA ![]()
Received 24 August 2022
Accepted for publication 24 March 2023
Published 3 May 2023 Volume 2023:15 Pages 665—677
DOI https://doi.org/10.2147/IJWH.S379749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Nyoman Anita Damayanti, Ratna Dwi Wulandari, Ilham Akhsanu Ridlo
Department of Health Policy and Administration, Faculty of Public Health, Unversitas Airlangga, Surabaya, Indonesia
Correspondence: Nyoman Anita Damayanti, Department of Health Policy and Administration, Faculty of Public Health, Unversitas Airlangga, St. Ir. Soekarno, Kampus C, Surabaya, East Java, 60115, Indonesia, Tel +62818518232, Fax +62315920948, Email [email protected]
Purpose: Maternal mortality is one problem that still affects countries like Indonesia and others globally. The World Health Organization (WHO) notes that Southeast Asian countries have a high MMR. Indonesia’s maternal mortality ranks third highest in Southeast Asia, with a 177 maternal mortality rate per 100,000 live births in 2017. In 2018, the maternal mortality rate reached 91.45 per 100,000 live births. Pregnant women’s deaths can be caused inadequate medical care due to how frequently they seek treatment. This study intends to identify and analyze how knowledge, education, and myths affect pregnant women’s attitudes toward seeking health services.
Materials and Methods: The study involved 175 pregnant and postpartum women who visited 10 health public centers in two cities in East Java by accidental sampling. Data regarding intrapersonal, interpersonal, and local wisdom were collected through surveys with structured instruments and in-depth interviews. Data statistics used pathway analysis with a p-value of > 0.05.
Results: Intrapersonal, interpersonal, and local wisdom variables have a significant direct or indirect effect on utilizing health services. Knowledge was the variable with the greatest influence (t-value, 27.96).
Conclusion: Myth and culture as local wisdom and intrapersonal factors significantly affect the pattern of utilizing health services.
Keywords: healthcare utilization, maternal mortality, human and health, pregnancy, sociocultural
Introduction
Indonesia and other nations struggle with maternal mortality, among other issues. The World Health Organization (WHO) estimates a global maternal mortality ratio (MMR) of 211 in 2021, reaching as high as 1150 in South Sudan. Surprisingly, MMR have greatly increased in developing countries over the last few years, whereas only a slight increase have been reported in developed countries. For example, the MMR is 462 per 100,000 live births in very low-income countries compared to 11 per 100,000 live births in high-income countries. In Southeast Asia, Indonesia ranks third highest after Myanmar and Laos in 2017. The maternal mortality rate in Indonesia is 177 per 100,000 per live births.1–5 The regional health profile revealed that maternal mortality in East Java Province was 91.45 per 100,000 live births in 2018.6,7
Reducing maternal mortality has become a burden both nationally and globally. Some of the national efforts that have been done include providing health worker delivery services at health facilities, creating an alert village, increasing community involvement in family planning, and distributing health professionals fairly throughout the village.6,8 Pregnant women can readily obtain maternal health treatments and lower their risks of maternal death.9 In addition, maternal health during pregnancy, childbirth, and postpartum period are influenced by various factors. Four determinant factors, namely health status, reproductive status, access to healthcare services, and service utilization, have been found to impact maternal health.10–12 McCarthy and Maine claimed that factors influencing maternal mortality include the health of expectant mothers, their access to healthcare, and their actions as mothers to maintain their optimal health. Internal and external factors influence the three ideas expressed by McCarthy and Maine.13 Internal factors include age, gender, behavior (knowledge, attitudes, and actions), education, and economic status. External factors consist of culture, environment, and availability of facilities.13–15
A previous study reported that maternal mortality is affected by age, age of marriage, media, education, knowledge, family support, distance, employment, household size, urban population, income, and religion. Therefore, the relationship between maternal mortality and local wisdom, especially its association with myths and culture, should be explored and understood.
Maternal deaths can occur early in pregnancy for various reasons, such as pregnant mothers continuing to believe false myths and using inappropriate medical services. Following the study results in several Indonesian regions, legends are included in sociocultural factors that cause complications among pregnant women, childbirth, and postpartum.16,17 Myths can have an impact on low birth weight in addition to causing maternal complications, as demonstrated by the case study in Bharatpur, Nepal. Due to community constraints, pregnant women receive an inadequate and less diversified diet, resulting in a lesser optimal use of maternal health services.18 Some myths and cultural practices are held as beliefs—particularly those performed during pregnancy—have no scientific basis and may even be harmful.
Myths are considered old values and rituals that go hand in hand with new deals and traditions in the form of accurate health information during pregnancy, childbirth, and postpartum, which can influence the behaviors of using maternal health services.19 Moreover, the lack of health service utilization by pregnant mothers can result in unawareness of the risk of death either during pregnancy or childbirth.20,21 Rizqi and Rubai reported that health service utilization should be considered because it is one of the determinants of receiving inappropriate care and diagnostic delays.14
Health service utilization behavior is defined as actions taken by a person when sick or has a health problem that requires treatment to eliminate a health problem. The increasing number of healthcare facilities influences variations in seeking community treatment, and the types, methods, and equipment of available health services at healthcare facilities are also increasingly diverse.22–25 Based on these problems, this study focuses on the local wisdom and intrapersonal factors in pregnant women and identifies and analyzes the influence of education, knowledge, and myths on the attitudes of pregnant women in seeking health services.
Materials and Methods
Study Design, Setting, and Period
This study used a mixed-method approach by collecting data through surveys (quantitative) and in-depth interviews (qualitative). The maternal mortality rate in Bojonegoro is 8th, and the maternal mortality rate in Surabaya is 24th in East Java. The study population in this article was pregnant and postpartum women who visited 10 public health centers in Bojonegoro Regency, representing the rural area, and those in Surabaya City, representing the urban area by accidental sampling. The total sample was 175 participants. Data collection was conducted from June to August 2019. The Health Research Ethics Committee Commission provided authorization to conduct this study, and the ethical clearance at the Faculty of Nursing, Universitas Airlangga (1494-KEPK), was issued on June 19, 2019. The 1964 Helsinki Declaration and the institutional and research committee’s ethical guidelines were followed in all procedures. All participants provided informed consent. Participants were informed of their freedom to withdraw from the study without incurring any costs. Fairness, privacy, secrecy, anonymity, and participants’ rights to willingly engage in the study were upheld.
Sample Size and Sampling Procedure
Two considerations should be addressed to determine the sample size. First, for correlation analysis, based on the preliminary study, the correlation coefficient between knowledge and health service utilization was 0.218; thus, a minimum sample of 163 participants was obtained. Second, based on the rule of thumb, a sample of 10–20 times the analyzed variable is required. This study used ten variables; therefore, a sample size of 100–200 was required.
With these two considerations, a sample of 175 participants was used. Probability proportionate to size sampling was taken with a ratio of participants visiting health centers in rural to urban areas of 2:1; hence, the sample sizes in rural and urban areas were 117 and 58 participants, respectively. Health service utilization is used as dependent variable, whereas intrapersonal (education, knowledge, attitude), interpersonal (institution support, distance, family support, community support), and intrapersonal factors (education and knowledge) were used as independent variables. Mothers’ knowledge about pregnancy, labor, and postpartum was calculated by summing up the total score of knowledge questions. A score of “1” denotes a correct answer, and “0” denotes a wrong answer. The knowledge category is divided into four. Respondents who score in the 75th percentile and above are labeled with “excellent knowledge”; 50th to 75th percentile, “good knowledge”; 25th to 50th percentiles, “moderate knowledge”; and <25th percentile, “poor knowledge”. Attitudes toward pregnancy, childbirth, and postpartum are the total scores derived from the Likert scale. Participants’ responses to each question in the attitude variable could range from “strongly agree”, “agree”, “somewhat agree”, “disagree”, or “strongly disagree”. For favorable questions, a score of 5 will be given if “strongly agree”; 4, “agree”; 3, “quite agree”; 2, “poorly agree”; or 1, “strongly disagree”, whereas unfavorable questions are assigned the opposite scores: 1 if “strongly agree”; 2, “agree”; 3, “quite agree”; 4, “poorly agree”; or 5, “strongly disagree”. The highest score of the attitude question is 25, whereas and the lowest score is 5. The attitude category is divided into four. Respondents who score in the ≥75th percentile are labeled with “very good attitude”; 50th to 75th percentile, “good attitude”; 25th to 50th percentile, “moderate attitude”; and <25th percentile, “poor attitude”.
Data Collection, Management, and Analysis
First, data were collected by a quantitative method using questionnaires. The questionnaires were analyzed by logistic and ordinal regression, and results showed that knowledge, existence of health facilities, culture, and mythical truths were factors that influenced mothers’ attitudes toward accessing health services. Education, knowledge, family support, the existence of health facilities, workplace support, and the presence of community associations, culture, and myths are elements that influence the health service utilization. Next, the path of influence is assessed between variables to develop a model. Then, a path analysis test was performed using the Linear Structural Relation (Lisrel) 8.8 version software.
After the data analysis, a qualitative study was conducted through in-depth interviews in focus-group discussion (FGD) and follow-up discussions to sharpen the model’s operability in each region. FGD was conducted by the facilitators and involved cadres and community leaders because they have an essential role in implementing maternal and child health programs. Parents or in-laws usually have an essential role in deciding, advising, and urging their children or in-laws to follow the family’s hereditary culture. In addition to the family, the community where pregnant women live can encourage mothers to carry out the tradition.
Results
Table 1 shows data collected in the Bojonegoro Regency and Surabaya City Health Centers. Table 1 describes that most pregnant women still believe myths in the community, as measured by the presence of food taboos, food recommendations, action prohibitions, and action recommendations in 160 (91.4%) participants. Moreover, most pregnant women finished high school (67, 38.3%). Meanwhile, the level of knowledge of the majority of participants was good and excellent in 59 (33.7%) participants. A total of 108 (61.7%) pregnant women also had an excellent attitude toward their pregnancy care, and 160 (91.4%) in the City of Surabaya and Bojonegoro Regency utilized health services by seeking treatment and visiting healthcare centers.
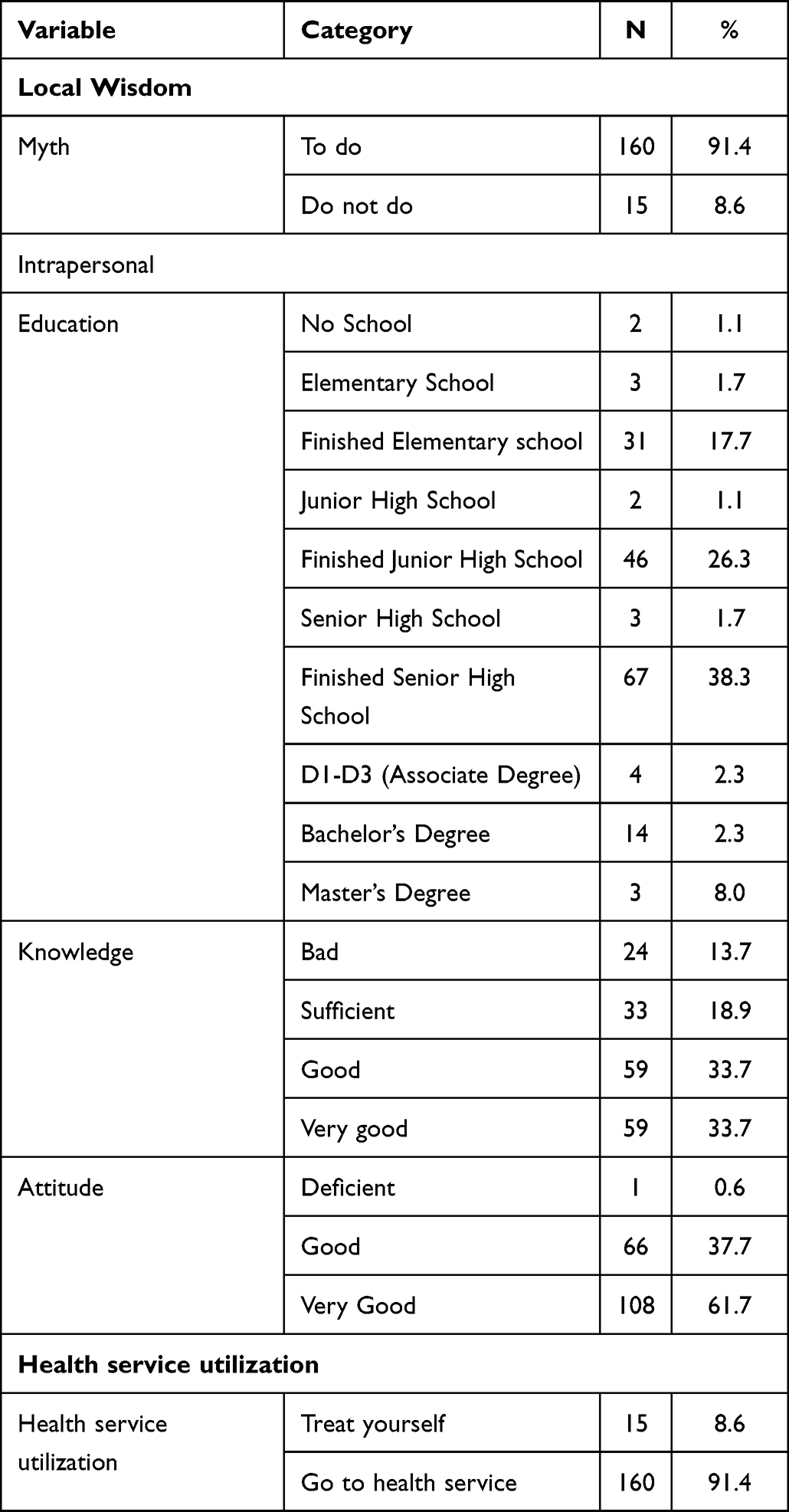 |
Table 1 Frequency of Local Wisdom, Intrapersonal, and Health Service Utilization on Pregnant Women in the City of Surabaya and Bojonegoro Regency |
Through in-depth interviews, we found that pregnant women had dietary restrictions on pineapple, durian, catfish, and banana flower. They also abstain from the following behaviors: after giving birth, they should not leave the house at Maghreb, not hurt animals, and not hate other people. From the results of the interviews, pregnant women turned to self-medication by seeking herbal and traditional therapies (from shamans and Islamic religious leaders) and taking medicines given without any medical advice. Meanwhile, those who utilized healthcare services are pregnant women who underwent consultations and utilized treatment at health facilities.
Pregnant women are recommended to consume green beans so that the child’s hair becomes thicker at birth. There are also taboos for pregnant women to eat pineapple. (Pregnant Mother 1)
There is a belief of continence in the community; therefore, village midwives must exert more effort. (Bojonegoro Regency’s family welfare program member)
There are taboos given to pregnant women by the community people that can harm pregnant women. (Community leaders in Surabaya)
Shamans still exist; however, we still humanize humans. We continue to work together because of the terms, which we shall discuss later. Usually, there is still a division of roles. Then, regarding birth attendants, there is no traditional birth attendant; hence, in principle, we communicate with the shaman. (Health officials of Bojonegoro’s Division Head of Public Health and Nutrition)
Based on the analysis results in Figures 1 and 2, intrapersonal factors such as knowledge and education directly influence the benefits of health services but indirectly affect attitudes. Intrapersonal factors, including community support and institutional support, also influence the health service utilization and indirectly influence attitudes. Meanwhile, family support, an interpersonal variable, indirectly influences health services through attitudes. Meanwhile, social environmental factors that have direct and indirect influences include culture and myths.
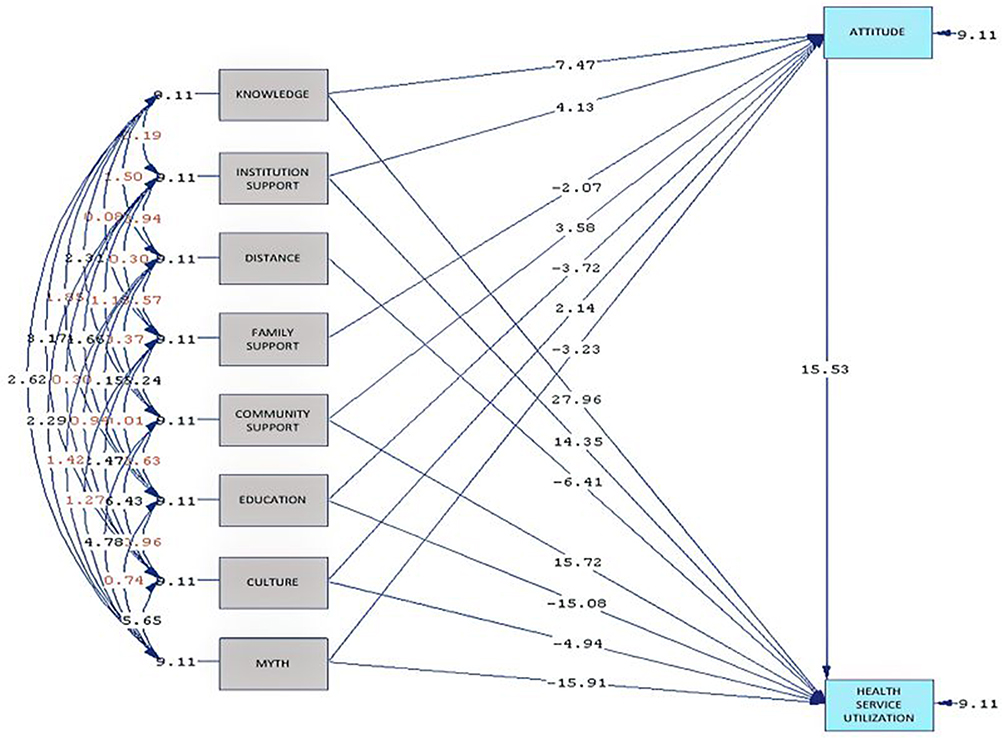 |
Figure 1 Pathway analysis of variables affecting health service seeking patterns (t-value) with chi-square 4.96 and p-value >0.05. |
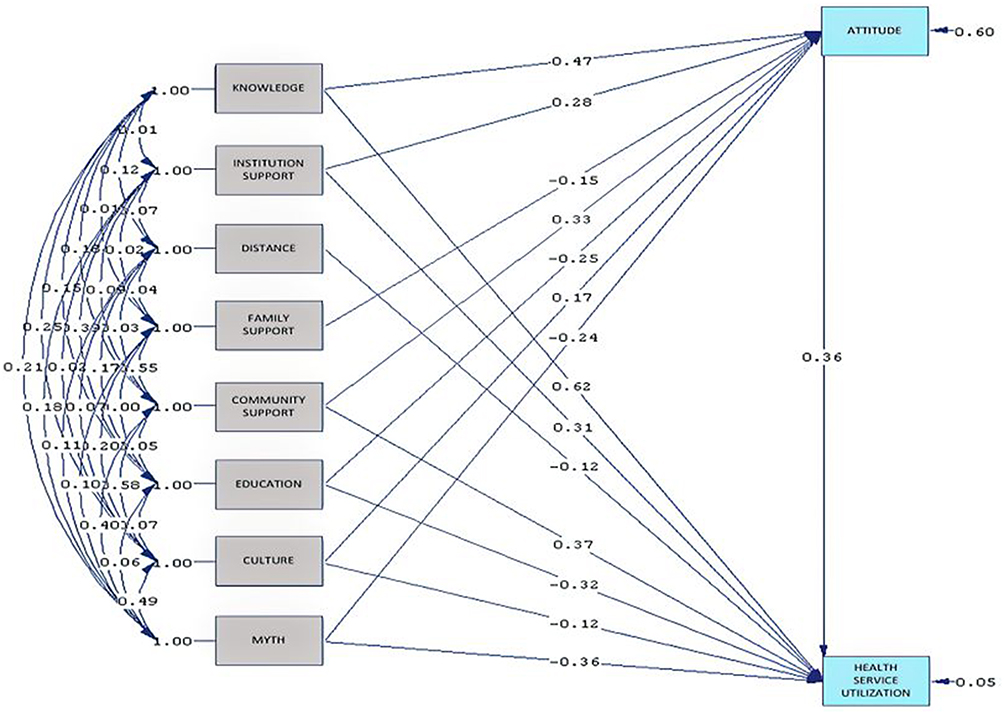 |
Figure 2 Path analysis of variables that affect health service seeking patterns (standardized coefficient) with chi-square 4.96 and p-value>0.05. |
Figure 1 describes that family support, culture, myths, community support, education, institutional support, and knowledge have a significant effect on attitudes with a t-value of −2.07; 2.14; −3.23; 3.58; −3.72; 4.13; and 7.47, respectively. Meanwhile, culture, distance to health facilities, institutional support, education, community support, myths, and knowledge significantly affect the health service utilization with a t-value of −4.94; −6.41; 14.35; −15.08; 15.72; −15.91 and 27.96, respectively. In addition, attitudes directly affect the utilization pattern of health services with a t-value of 15.53. Figure 1 provides a statistical test value of >1.96 and shows significant influencing paths. The magnitude of the influence of each independent variable on the intermediate and dependent variables is shown in Figure 2. The dependent variable was seeking health facilities.
Figure 2 shows that knowledge has a direct and indirect influence on the health service utilization among pregnant women. Knowledge had a 0.62 direct impact on the use of health services, whereas attitude had a 0.47×0.36 = 0.169 indirect impact. Community support and myths significantly impact health service utilization, whereas myths have a negative impact since the more people believe myths, the lesser they utilize health services. Figure 2 present that the direct impact on the use of health services of community support was 0.37, and that of myth was −0.36. Community support had a positive influence. More people use health services when there is an excellent community support and vice versa.
Family support (−0.15), myths (−0.24), and educational level (−0.25) have a negative impact on attitudes. Family support in the form of decision-making for pregnant women can have a negative effect on attitudes. Implementing societal myths such as dietary restrictions contrary to health science could negatively influence the mother’s perspective. Meanwhile, culture (0.17), community support (0.33), institutional support (0.28), and knowledge (0.47) positively influence the attitudes. Cultural practices at 4 or 7 months could also help improve maternal attitudes. The presence of community and institutional support such as classes for pregnant women, check permits, and leave policies can improve maternal attitudes. The higher the mother’s knowledge, the higher the mother’s perspective.
Culture (−0.12), distance to health facilities (−0.12), educational level (−0.32), and myths (−0.36) negatively affect the utilization pattern of health services. Culture could negatively influence the design and utilization of health services. When mothers experience health issues, they tended to choose conventional remedies such as massage rather than visiting a hospital. Mothers would have less access to medical care at the health facility further from their residence. However, institutional support (0.31), community support (0.37), and knowledge (0.62) all have a favorable impact on how often people use health services. The utilization of maternal health services increases as the community and institutional support increases. The pattern of health service utilization was directly correlated with the mother’s educational level. It was consistent with the mother’s mindset, which positively impacts the planning of health service utilization.
Discussion
Influence of Myth and Culture as Local Wisdom on Health Service Utilization Behaviors
A pregnant woman’s health should be crucially monitored because of high risks for both the mother and fetus. Pregnant women’s access to high-quality healthcare services is a social issue that extends beyond medicine. The issue of local knowledge should be considered in manage maternal mortality. In particular, pregnant women’s adherence to regional mythology and culture may be detrimental to their ability to preserve their health. Even if the post-industrial period of societal development has begun, not all people are entirely sensible in their actions. Both rural and urban pregnant women are still influenced by various taboos and irrational myths.
Local knowledge can be interpreted as habits, rules, and values due to the cognitive efforts adopted by specific or local communities considered reasonable and wise, which are implemented and obeyed by the community.26 Myth is information considered to have occurred even though it does not always happen. In rural areas with still thick customs, myths are used as a way of life and are firmly held in life.27,28
Culture becomes the local identity of a community that is unique and different from other communities.29 Indonesian women come from different cultures and try to maintain the health of their pregnancy in various ways based on their environmental culture. However, maintaining a healthy pregnancy based on past cultural traditions may differ from the current approach due to scientific intervention.27 Thus, culture and myths related to pregnancy that is believed and practiced by the community should be understood as a step in identifying knowledge and behavior gaps that can harm the health of pregnant women and fetuses. Many Indonesian women who become new mothers do not know how to take care of their children; hence, they listen to their parents and grandparents, who also make decisions during pregnancy and implement traditional practices based on their culture and myths.30 The results showed that 91.4% of pregnant women still practice pregnancy-related myths and cultures, even though these cultures and myths have not been proven true and have an impact on the health of pregnant women and fetuses.
The results showed that myths affect the pattern and attitudes of seeking health services. In total, the influence of myths on the design of health service utilization is negative, either directly or indirectly (through perspectives). In other words, the more people prefer to utilize self-medication, the more falsehoods are perpetuated. Myth is a variable that has a direct negative effect on the utilization pattern of health services, indicating that the stronger the pregnant women run myths, the more likely they will self-medicate if they have complaints. Myths are passed from era to age and contains terrible consequences that will be accepted if not carried out by pregnant women, making them scared to violate them and thereby choose to do it voluntarily or forced.24,31
The findings of this study are consistent with those of Vora’s, who found a connection between myths and health service utilization.32 Myths that permeate a society typically involve eating habits and behaviors. Even though the surrounding community continues to impose restrictions on eating certain foods or acting in specific ways among pregnant women, restricting a pregnant woman’s eating is unacceptable, and thus, they should be allowed to eat anything as long as they are eating healthy foods with good nutrition for both the mother and baby. Moreover, the culture that is believed and lived by the mother has an influence on the choice of treatment method among pregnant women. Generally, parents or in-laws play a critical role in determining, advising, and suggesting their child or daughter-in-law in carrying out the culture that is believed to be passed down from generation to generation in the family. Apart from the family, the community where pregnant women live can encourage mothers to carry out traditions.33,34
Food taboos during pregnancy are a set of systematic rules about which foods or combinations should not be consumed because they harm the pregnant woman and fetus.29 Pregnant women abstain from consuming foods that are the richest sources of iron, carbohydrates, animal protein, and micronutrients not only in Indonesia but also in Ethiopia,35 Gambia,36 Nigeria,22 South Africa,37 and the Democratic Republic of the Congo38 because the baby may have bad habits after birth or may have a disease at birth. In addition, in several low- and middle-income countries in Asia, dietary restrictions also include restrictions on the quantity and quality of food consumed by pregnant women.1,18,39 For example, protein-rich foods are rarely given to pregnant women. All of the above dietary restrictions are only based on traditional beliefs without scientific basis. Balanced nutrition is essential for pregnant women and fetuses. In fact, the conceptual framework of The United Nations Children’s Fund Food-Care Health indicated that cultural beliefs and practices related to food during pregnancy are one of the fundamental causes of maternal malnutrition that will have an impact on the health and fitness of pregnant women and quality of fetal growth and development even after birth. Malnutrition is defined as a deficiency of macronutrients and micronutrients, especially vitamin A, folic acid, iodine, iron, calcium, and zinc, which are very important to meet their needs during pregnancy.40 The myth is also associated with the discovery of recommended and forbidden foods that apply to pregnant and lactating women to promote safety and health for mothers and babies.
Based on interviews, the myth about dietary restrictions was also determined in this study, namely, the existence of taboos on eating pineapple for pregnant women. Malnutrition in pregnant women and fetuses can occur if the nutritional needs of pregnant women are not met because pregnant women require increased quantity and quality of nutrients. Pregnant women’s behavior regarding consuming certain foods recommended or prohibited by culture can harm the health of pregnant women and fetuses. Every recommendation or prohibition on a pregnant woman’s has consequences on the nutritional status.41
In this study, culture indirectly positively affected (through attitudes) the health service utilization. Cultural factors that have a significant influence on pregnant women’s attitudes and pattern of health service utilization in this study were also observed by Zambia,36 who stated that the culture that existed in a community greatly influenced the patterns of thinking and attitudes that ultimately influenced the maternal health service utilization. The community sees physical, psychological, and social problems during pregnancy, childbirth, and after birth as a sign of neglected relationships with their ancestors.36
One of the roles and functions of local knowledge in society related to pregnancy and birth is as a moral and spiritual guide for the community because the measure of truth in specific life systems refers to the community’s perspective on the pregnancy and birthing process. This measure of truth creates values that the community believes to be good.26 Sociocultural beliefs and cultural practices adversely affect pregnancy and birth, even among educated women.42 The beliefs attached to a woman are influenced by family experiences, local cultural norms, and values, including during pregnancy, childbirth, and postpartum.43
However, traditional culture also has a positive impact. Although the effect of each pregnancy-related culture and myth held by the community regarding pregnancy can be considered, if it has a negative impact, it must be changed so as not to endanger the safety of the lives of pregnant women and fetuses.33 Pregnancy-related cultural beliefs and practices in developing countries can prevent pregnant women from accessing and receiving appropriate antenatal delivery and post-natal care, including increasing the possibility of giving birth at home without a competent health worker to assist with delivery. One of the causes is the difficulty of accessing information that can help pregnant women make decisions, including seeking health services during pregnancy and increasing pregnant women and families’ awareness of the impact of adverse pregnancy cultural practices.44 The WHO supported culturally appropriate maternity care services to improve maternal and newborn health with careful consideration of individual preferences and aspirations; thus, the community culture is assessed as an essential component of quality care.28
One of the solutions to pregnancy and childbirth complications is to understand that the sociocultural aspect is the cause of the problem. The results of this study indicate that although most pregnant women have sought health services if they experience problems during pregnancy, most of them still treat themselves at home. It can be influenced by the belief of ancestors who forbid modern health services and even prevented them from going to health facilities for pregnancy check-ups.45 Self-medication carried out by pregnant women and their families without being accompanied by competent health workers will increase maternal complications.
Self-medication is a common practice in society, not only in Indonesia but also worldwide, including Mexico. However, the impact caused by ignorance in handling pregnant women should be considered to promote optimal health of pregnant women and fetuses. For example, paracetamol is considered safe to relieve fever, dizziness, and pain symptoms. A study revealed that excessive doses of paracetamol could cause respiratory and nervous disorders in newborns.46 The WHO defines self-medication as the selection and use of medicines by individuals to treat diseases experienced and recognized by themselves. Self-medication is not only limited to medications commonly prescribed by doctors but also traditional herbal products and use of leftover medicines from previous prescriptions. Pregnant women tended to self-medicate due to the following reasons: drugs easily accessible, save time, sociodemographic factors, maternal disease history, and lack of knowledge about the effects and risks of using drugs without a doctor’s advice.47,48 The SDG targets can be achieved by identifying determinants of self-medication in pregnant women and how often it is practiced. It is related to improving the drug sales service from pharmacies or drug stores without a doctor’s prescription. Inadequate enforcement of regulations that every drug consumed by pregnant women must use a doctor’s prescription to reduce risks and to provide education to families and community, as a sociocultural environment to be wiser in using and suggesting herbal medicines35,49 regarding the consequences of self-medication and the use of herbal medications in pregnant women.50
Every pregnant woman who adheres to her traditional beliefs, culture, norms, and practices can directly or indirectly protect or even endanger her own health and the fetus.29 The health and well-being of women in most societies will depend on the cultural context in which they live. Cultural knowledge was gained comes from life stories, and social experiences were passed down from generation to generation, which greatly affected their health decisions during pregnancy and thereby affected the growth and development of the unborn child.51 Decision-making during pregnancy, including choosing to self-medicate and giving birth at home, is also influenced by social vulnerability and powerlessness, and fear of the unknown; therefore, families who have experienced pregnancy are generally the ones who make decisions.24
In Indonesia, behavior related to public health becomes more complex because it is a multicultural country with diverse ethnicities and various health service providers. A study revealed that people’s behavior in seeking care can be determined by multiple internal factors, such as individual characteristics and perceptions and beliefs about the disease and its treatment, including pregnancy.52 The ability of women to seek health services during pregnancy will ensure a decrease in MMR during childbirth. It is considered one of the critical strategies to reduce maternal mortality by providing access to and utilization of maternal and child health services.31
Effects of Knowledge on Health Service Utilization Behavior
The level of focus and perception of the object significantly impact the knowledge generated by the sensing process. Without knowledge, one lacks the foundation for forming judgments and choosing how to respond to current issues.53 The results showed that knowledge positively affected the attitudes and behaviors of pregnant women in seeking health services. The effect of familiarity is positive, ie, the better the understanding, the more participants will choose health services over self-medication. A previous study reported that knowledge influences mothers to access health services. Knowledge can increase awareness of pregnant women about the importance of maintaining health during pregnancy and the risks that can be experienced during pregnancy, childbirth, and postpartum. Pregnant women should seek professional help if health problems arise to broaden their knowledge on the pregnancy, childbirth, and puerperium.23
Knowledge is one of the predisposing factors that impact the utilization of maternal health services. The higher the knowledge possessed by pregnant women, the higher the optimal utilization of maternal health services.54 Pregnant women who are exposed to various pregnancy information through television, the Internet, and associations of pregnant women have better understanding of the health problems that they may face and thereby choose proper health service facilities to solve these problems.32
A study in Tarus Health Center showed that highly knowledgeable mothers can understand the purpose, benefits, and timing of antenatal care (ANC) and take advantage of complete and optimal ANC. This behavior can last long if it is based on sound knowledge and awareness of pregnancy health services.55 Good learning is needed in supporting the health of pregnant women because insufficient knowledge about pregnancy is one of the causes of health problems in the community. Good new behavior will help reduce health cases/problems or will improve health service indicators in the community.
Efforts are needed from midwives and other healthcare workers as educators for pregnant women and their families to ensure that they receive proper health services during pregnancy to prevent complications, one of which is by providing counseling that can increase knowledge during visits to authorized healthcare workers to dispel myths. Although knowledge and information are increasingly developing and advancing, not all people abandon traditional knowledge (myths). After all, they are considered ancestral heritage that needs to be preserved; thus, it will definitely affect the actions of pregnant women in choosing maternal health services.16 The minimal knowledge of pregnant women and their families about pregnancy and maternal health services will increase the risk of complications for the mother and fetus.56
Effects of Education on Health Service Utilization Behavior
Education harms health service-seeking attitudes and behaviors. The low understanding of mothers cannot be separated from the low educational level and can impact the decision-making of pregnant women in seeking health services.57 A Bangladesh study demonstrated a positive relationship between maternal education and safe pregnancy, indicating that women who are more educated are more aware of pregnancy health. Thus, knowing how education, employment, and healthcare facilities can significantly impact women’s status and perceptions of health service utilization behavior, especially in rural areas, is essential.58
Educated women tend to have a greater awareness of the existence of ANC services and advantages of using those services. They are more aware of health problems, know more about the availability of healthcare services, and use more information effectively than uneducated women. In addition, higher educational levels tend to positively influence the health service utilization behavior, and education can increase a woman’s control over her pregnancy. In addition, it can help expose women to more health messages, enabling them to recognize danger signs and complications and take appropriate action. These women may have a more significant opportunity to receive health information and pay more attention to maternal health.59 A previous study reported that the higher the education level of a pregnant woman, the higher the possibility of using sustainable health services, including the management of complications during pregnancy; thus, the goal of realizing the health of pregnant women will be achieved optimally.60
Influence of Attitude on Health Service Utilization Behaviors
Attitude allows people to evaluate an object in the form of positive and negative assessments. Attitudes toward seeking health services are measured by the responses raised by participants to statements about seeking treatment.39 The results showed that attitudes positively affected health service utilization. The WHO has recognized that midwives can handle most pregnancy problems and have the skills to refer more complicated complications to doctors, such as handling uncomplicated deliveries.61 ANC is a unique pattern of care organized for pregnant women to achieve excellent health status and increase the chances of safe delivery and postpartum period. Ideally, the implementation of ANC is carried out in a health facility and handled by professional health workers who have the ability and authority in ANC, including family planning, preconception, pregnancy, and post-natal care to reduce morbidity and mortality.62
Seeking and utilizing health services from professional health workers during pregnancy is a preventive method and an effort to reduce pregnancy- and childbirth-related complications. Pregnant women’s symptoms and their reaction must be evaluated to determine when and where to check their health conditions, both in medical facilities and at traditional assistance centers, which play a role in seeking healthcare during pregnancy (shamans). Attitudes in determining a pregnant woman’s decision to suspend her health condition are based on various considerations, such as personal needs, family support, sociocultural, and easy access to health services.23
Conclusion
Culture, myth, education, and knowledge significantly affect pregnant women’s attitudes. In addition, culture, teaching, myths, and learning substantially affect the pattern of health service utilization among pregnant women. Hence, they should be used as basis for providing health education among pregnant women to instill cultural messages. Attitudes directly affect the pattern of health service utilization; thus, factors influencing the attitudes of pregnant women should be carefully considered to maximize the health service utilization, maintain and improve the optimal health status of pregnant women and fetuses, and reduce the MMR and IMR in Indonesia.
Data Sharing Management
All data and materials used in this study will be available from the corresponding author upon reasonable request.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Health Research Ethics Committee Commission at the Faculty of Nursing, Universitas Airlangga, with registry number 1494-KEPK on June 19, 2019. The authors certify that the patient(s) has/have signed the inform consent forms. All procedures involving the participants were conducted in accordance with the ethical standards established by the institutional and research committees and the 1964 Helsinki Declaration.
In the form, the participant(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. They understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Acknowledgments
Authors are grateful to Simlitabmas (Sistem Informasi Penelitian dan Pengabdian kepada Masyarakat) and Kemendikbud ristekdikti (Kementerian Pendidikan, Kebudayaan, Riset, dan Teknologi Pendidikan Tinggi).
Author Contributions
All authors equally contributed to the idea, study design, implementation, data gathering, analysis, and interpretation. The article was written, revised, and subjected to critical review by all authors, who also agreed on the journal to which it would be submitted. The authors also agreed to be responsible for all aspects of the work and reviewed and approved each version before during submission, revision, and final acceptance for publication.
Disclosure
The authors report no conflicts of interest associated with this work.
References
1. Javaheri M, Mohammadi Y. Trends and causes of maternal mortality in West of Iran from 2002 to 2016: implications for sustainable development goals. J South Asian Fed Obstet Gynaecol. 2020;12:159–162. doi:10.5005/jp-journals-10006-1785
2. Kusuma D, Cohen J, McConnell M, Berman P. Can cash transfers improve determinants of maternal mortality? Evidence from the household and community programs in Indonesia. Soc Sci Med. 2016;163:10–20. doi:10.1016/j.socscimed.2016.06.020
3. Mohamed AA, Bocher T, Magan MA, et al. Experiences from the field: a qualitative study exploring barriers to maternal and child health service utilization in IDP settings Somalia. Int J Womens Health. 2021;13:1147–1160. doi:10.2147/IJWH.S330069
4. World Health Organization. Maternal mortality across countries; 2017.
5. Lawrence ER, Klein TJ, Beyuo TK. Maternal mortality in low and middle-income Countries. Gynecol Obstetrics. 2022;2022:713–733. doi:10.1016/j.ogc.2022.07.001
6. Indonesia Ministry of National Development Planning UNCF. SDG baseline report on children in Indonesia; 2017.
7. Rizkianti A, Afifah T, Saptarini I, Rakhmadi MF. Women’s decision-making autonomy in the household and the use of maternal health services: an Indonesian case study. Midwifery. 2020;90:102816. doi:10.1016/j.midw.2020.102816
8. Indriani D, Damayanti NA, Teguh D, et al. The maternal referral mobile application system for minimizing the risk of childbirth. J Public Health Res. 2020;9:105–109. doi:10.4081/jphr.2020.1813
9. Omer S, Zakar R, Zakar MZ, Fischer F. The influence of social and cultural practices on maternal mortality: a qualitative study from South Punjab, Pakistan. Reprod Health. 2021;18:97. doi:10.1186/s12978-021-01151-6
10. Rachmawati PD, Kurnia ID, Asih MN, et al. Determinants of under-five mortality in Indonesia: a nationwide study. J Pediatr Nurs. 2022;65:e43–e48. doi:10.1016/j.pedn.2022.02.005
11. Zhang M, Zhang W, Yang H, et al. Design and evaluation of maternal early warning system to reduce preventable maternal mortality in pregnancy and puerperium for high-risk women in China. Midwifery. 2022;112:103392. doi:10.1016/j.midw.2022.103392
12. Renbarger KM, McIntire E, Twibell R, et al. Descriptions of maternal mortality from nurses who practice in perinatal settings. Nurs Womens Health. 2022;26(4):288–298. doi:10.1016/j.nwh.2022.05.003
13. McCarthy J, Maine D. A framework for analyzing the determinants of maternal mortality. Stud Fam Plann. 1992;23:23–33. doi:10.2307/1966825
14. Rizqi YNK, Rubai WL. Integration of the maternal death prevention program based on the health belief model framework. KEMAS J Kesehat Masy. 2020;15:432–440. doi:10.15294/kemas.v15i3.20373
15. Yadav AK, Jena PK, Sahni B, Mukhopadhyay D. Comparative study on maternal healthcare services utilisation in selected Empowered Action Group states of India. Health Soc Care Community. 2021;29:1948–1959. doi:10.1111/hsc.13309
16. Novitasari F, Fitriyah N. Socio-cultural aspects and knowledge of pregnant women about pregnancy-related myths in the Village of Mojosarirejo, District of Driyorejo, Gresik Regency. J Biom Dan Kependud. 2019;8:83. doi:10.20473/jbk.v8i1.2019.77-86
17. Yadav AK, Jena PK. Explaining changing patterns and inequalities in maternal healthcare services utilization in India. J Public Aff. 2022;22:e2570. doi:10.1002/pa.2570
18. Bansal P, Garg S, Upadhyay HP. Prevalence of low birth weight babies and its association with socio-cultural and maternal risk factors among the institutional deliveries in Bharatpur, Nepal. Asian J Med Sci. 2019;10:77–85. doi:10.3126/ajms.v10i1.21665
19. Juariah J. Kepercayaan dan praktik budaya pada masa kehamilan masyarakat Desa Karangsari, Kabupaten Garut [Cultural beliefs and practices in pregnancy community in Karangsari Village, Garut District]. Sosiohumaniora. 2018;20:162–167. Indonesian. doi:10.24198/sosiohumaniora.v20i2.10668
20. Damayanti NA, Wulandari RD, Hargono A. Pengembangan model sistem informasi surveillance faktor risiko dan kohort ibu dan anak integrasi berbasis continum of care di Surabaya [Development of risk factor surveillance information system model and integrated mother and child cohort based on continum of care in Surabaya]; 2016. Indonesian.
21. Damayanti NA, Setijanto D, Hargono A, et al. Integrated information system for early detection of maternal risk factors based on continuum of care approach of mother and toddler cohorts. Healthc Inform Res. 2019;25:153–160. doi:10.4258/hir.2019.25.3.153
22. Chika O. Health seeking behaviour of pregnant women in South East of Nigeria: implication for improved natal and postnatal care. Int J Sci. 2017;6:37–41.
23. Liu G, Xue Y, Qian Z, et al. Healthcare-seeking behavior among pregnant women in the Chinese hierarchical medical system: a cross-sectional study. Int J Equity Health. 2019;18:129. doi:10.1186/s12939-019-1037-8
24. Ahmad R, Zhu NJ, Lebcir RM, Atun R. How the health-seeking behaviour of pregnant women affects neonatal outcomes: findings of system dynamics modelling in Pakistan. BMJ Glob Health. 2019;4:e001242. doi:10.1136/bmjgh-2018-001242
25. Yadav AK, Nag S, Jena PK, Paltasingh KR. Determinants of antenatal care utilisation in India: a count data modelling approach. J Dev Policy Pract. 2021;6:210–230. doi:10.1177/24551333211030349
26. Pesurnay AJ. Local wisdom in a new paradigm: applying system theory to the study of Local Culture in Indonesia. IOP Conf Ser Earth Environ Sci. 2018;175:012037. doi:10.1088/1755-1315/175/1/012037
27. Susie Perbawasari I. Internalization of life cycle values based on local wisdom: measuring the indungbeurang exemplary in maintaining pregnancy health in the Indigenous Community of Naga Village. Ann Romanian Soc Cell Biol. 2021;25:8941–8948.
28. Jones E, Lattof SR, Coast E. Interventions to provide culturally-appropriate maternity care services: factors affecting implementation. BMC Pregnancy Childbirth. 2017;17:267. doi:10.1186/s12884-017-1449-7
29. Nayak D, Dey S. Cultural beliefs on antenatal care among women in selected areas of bhubaneswar- a descriptive study. Clin Med. 2020;7:11.
30. Turner C, Pol S, Suon K, et al. Beliefs and practices during pregnancy, post-partum and in the first days of an infant’s life in rural Cambodia. BMC Pregnancy Childbirth. 2017;17:116. doi:10.1186/s12884-017-1305-9
31. Dapaah JM, Nachinaab JO. Sociocultural determinants of the utilization of maternal health care services in the Tallensi District in the Upper East Region of Ghana. Adv Public Health. 2019;2019:e5487293. doi:10.1155/2019/5487293
32. Vora KS, Koblinsky SA, Koblinsky MA. Predictors of maternal health services utilization by poor, rural women: a comparative study in Indian States of Gujarat and Tamil Nadu. J Health Popul Nutr. 2015;33:9. doi:10.1186/s41043-015-0025-x
33. Sahin E, Sahin NH. Cultural practices before and during pregnancy: example of Turkey. New Trends Issues Proc Adv Pure Appl Sci. 2018;97–103. doi:10.18844/gjpaas.v0i10.3749
34. Yadav AK, Jena PK. Maternal health outcomes of socially marginalized groups in India. Int J Health Care Qual Assur. 2020;33(2):172–188. doi:10.1108/IJHCQA-08-2018-0212
35. Beyene KG, Beza SW. Self-medication practice and associated factors among pregnant women in Addis Ababa, Ethiopia. Trop Med Health. 2018;46:10. doi:10.1186/s41182-018-0091-z
36. Honkavuo L. Women’s experiences of cultural and traditional health beliefs about pregnancy and childbirth in Zambia: an ethnographic study. Health Care Women Int. 2021;42:374–389. doi:10.1080/07399332.2021.1898613
37. Marabele PM, Maputle MS, Ramathuba DU, Netshikweta L. Cultural factors contributing to maternal mortality rate in Rural Villages of Limpopo Province, South Africa. Int J Womens Health. 2020;12:691–699. doi:10.2147/IJWH.S231514
38. Ramazani IB-E, Ntela S-DM, Ahouah M, Ishoso DK, Monique R-T. Maternal mortality study in the Eastern Democratic Republic of the Congo. BMC Pregnancy Childbirth. 2022;22:452. doi:10.1186/s12884-022-04783-z
39. Tieu Y, Konnert C, Quigley L. Psychometric properties of the inventory of attitudes toward seeking mental health services (Chinese version). Can J Aging Rev Can Vieil. 2018;37:234–244. doi:10.1017/S0714980818000041
40. Chakona G, Shackleton C. Food taboos and cultural beliefs influence food choice and dietary preferences among pregnant women in the Eastern Cape, South Africa. Nutrients. 2019;11:2668. doi:10.3390/nu11112668
41. Jardí C, Aparicio E, Bedmar C, et al. Food consumption during pregnancy and post-partum ECLIPSES Study. Nutrients. 2019;11:2447. doi:10.3390/nu11102447
42. Al-Ateeq MA, Al-Rusaiess AA. Health education during antenatal care: the need for more. Int J Womens Health. 2015;7:239–242. doi:10.2147/IJWH.S75164
43. Downe S, Finlayson K, Oladapo O, Bonet M, Gülmezoglu AM. What matters to women during childbirth: a systematic qualitative review. PLoS One. 2018;13:e0194906. doi:10.1371/journal.pone.0194906
44. Abebe H, Beyene GA, Mulat BS. Harmful cultural practices during perinatal period and associated factors among women of childbearing age in Southern Ethiopia: community based cross-sectional study. PLoS One. 2021;16:e0254095. doi:10.1371/journal.pone.0254095
45. Takaeb AEL. Exploration of socio-cultural determinants of maternal mortality in Indonesia.
46. Alonso-Castro AJ, Ruiz-Padilla AJ, Ruiz-Noa Y, et al. Self-medication practice in pregnant women from central Mexico. Saudi Pharm J. 2018;26:886–890. doi:10.1016/j.jsps.2018.03.008
47. Pereira G, Surita FG, Ferracini AC, Madeira C de S, Oliveira LS, Mazzola PG. Self-medication among pregnant women: prevalence and associated factors. Front Pharmacol. 2021;12:659503.
48. Niriayo YL, Mohammed K, Asgedom SW, Demoz GT, Wahdey S, Gidey K. Self-medication practice and contributing factors among pregnant women. PLoS One. 2021;16:e0251725. doi:10.1371/journal.pone.0251725
49. Zewdie T, Azale T, Shimeka A, Lakew AM. Self-medication during pregnancy and associated factors among pregnant women in Goba town, southeast Ethiopia: a community based cross sectional study. BMC Res Notes. 2018;11:713. doi:10.1186/s13104-018-3821-8
50. Tuha A, Faris AG, Mohammed SA, Gobezie MY. Self-medication and associated factors among pregnant women attending antenatal care at Kemisie General Hospital, North East Ethiopia. Patient Prefer Adherence. 2020;14:1969–1978. doi:10.2147/PPA.S277098
51. Andina-Díaz E. Beliefs and dietary practices in pregnancy and the puerperium: application of the Health Traditions Model. Enferm Glob. 2021;12:110–121.
52. Widayanti AW, Green JA, Heydon S, Norris P. Health-seeking behavior of people in Indonesia: a narrative review. J Epidemiol Glob Health. 2020;10:6–15. doi:10.2991/jegh.k.200102.001
53. Abdulrida H, Hassan R, Sabri M. Knowledge and health-seeking practices of mothers attending primary health-care centers in Baghdad al-karkh sector about danger signs in newborns. Mustansiriya Med J. 2018;17:29. doi:10.4103/MJ.MJ_7_18
54. Wau H, Razella N. Utilization of Antenatal Care (ANC) services by pregnant women in Binjai City and factors affecting. KEMAS J Kesehat Masy. 2020;15:390–398. doi:10.15294/kemas.v15i3.20613
55. Tassi WD, Sinaga M, Riwu RR. Analisis faktor-faktor yang berhubungan dengan perilaku ibu hamil dalam pemanfaatan pelayanan antenatal care (K4) di wilayah kerja puskesmas tarus [Analysis factors associated with the behavior of pregnant women in the utilization of antenatal care services (K4) in the Tarus Health Centre's working area]. Media Kesehat Masy. 2021;3:175–185. Indonesian
56. Khan S, Haider SI, Bakhsh R. Socio-economic and cultural determinants of maternal and neonatal mortality in Pakistan. Glob Reg Rev. 2020;1–7. doi:10.31703/grr.2020(V-I).01
57. Inayah N, Fitriahadi E. Hubungan pendidikan, pekerjaan dan dukungan suami terhadap keteraturan kunjungan ANC pada ibu hamil trimester III [Relationship between education, work and husband’s support on the regularity of ANC visits in third trimester pregnant women]. JHeS J Health Stud. 2019;3:64–70. Indonesian. doi:10.31101/jhes.842
58. Nasrin M, Sarker MNI, Huda N. Determinants of health care seeking behavior of pregnant slums dwellers in Bangladesh; 2018. Available from: https://www.semanticscholar.org/paper/Determinants-of-health-care-seeking-behavior-of-in-Nasrin-Sarker/1a28e07a04ecbc19ae316e34ed0b186f0e0fe982.
59. Ali S, Ali S, Suhail N. Importance of storing medicines on required temperature in pharmacies and role of community pharmacies in rural areas: literature review. Manag J Nurs. 2016;6:32–42.
60. Dharmayanti I, Azhar K, Tjandrarini DH, Hidayangsih PS. Pelayanan pemeriksaan kehamilan berkualitas yang dimanfaatkan ibu hamil untuk persiapan persalinan di Indonesia [Quality pregnancy check services used by pregnant women for delivery preparation in Indonesia]. J Ekol Kesehat. 2019;18:60–69. Indonesian. doi:10.22435/jek.18.1.1777.60-69
61. Peprah P, Mawuli Abalo E, Nyonyo J, Okwei R, Agyemang-Duah W, Amankwaa G. Pregnant women’s perception and attitudes toward modern and traditional midwives and the perceptional impact on health seeking behaviour and status in rural Ghana. Int J Afr Nurs Sci. 2018;8:66–74. doi:10.1016/j.ijans.2018.03.003
62. Osuala E. Hypertension awareness and perception: Health Education Implication on prevention and control among rural dwellers, South East Nigeria. IOSR J Nurs Health Sci. 2017;6:63–68. doi:10.9790/1959-0601046368
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.