Back to Journals » Cancer Management and Research » Volume 13
Matching-Adjusted Indirect Comparison of Ribociclib Plus Fulvestrant versus Palbociclib Plus Letrozole as First-Line Treatment of HR+/HER2− Advanced Breast Cancer
Authors Fasching PA, Delea TE, Lu YS, De Boer R, Hurvitz SA, Moynahan A, Chandiwana D, Lanoue B, Hu H, Thuerigen A, O'Shaughnessy J
Received 15 July 2021
Accepted for publication 12 October 2021
Published 1 November 2021 Volume 2021:13 Pages 8179—8189
DOI https://doi.org/10.2147/CMAR.S325043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kenan Onel
Peter A Fasching,1 Thomas E Delea,2 Yen-Shen Lu,3 Richard De Boer,4 Sara A Hurvitz,5 Aaron Moynahan,2 David Chandiwana,6 Brad Lanoue,6 Huilin Hu,6 Astrid Thuerigen,7 Joyce O’Shaughnessy8
1University Hospital Erlangen, Comprehensive Cancer Center Erlangen—EMN, Department of Gynecology and Obstetrics, Friedrich-Alexander University Erlangen—Nuremberg, Erlangen, Germany; 2Policy Analysis Inc. (PAI), Brookline, MA, USA; 3National Taiwan University Hospital, Taipei, Taiwan; 4Peter MacCallum Cancer Centre, Victoria, Australia; 5University of California, Los Angeles, Jonsson Comprehensive Cancer Center, Los Angeles, CA, USA; 6Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA; 7Novartis Pharma AG, Basel, Switzerland; 8Department of Medical Oncology, Baylor University Medical Center, Texas Oncology and US Oncology Network, Dallas, TX, USA
Correspondence: Peter A Fasching
University Hospital Erlangen, Comprehensive Cancer Center Erlangen—EMN, Department of Gynecology and Obstetrics, Friedrich-Alexander University Erlangen, Maximiliansplatz 2, Erlangen, 91054, Germany
Email [email protected]
Purpose: Cyclin-dependent kinase 4/6 inhibitors (CDK4/6i) plus endocrine therapy are recommended for first-line treatment of hormone receptor–positive/human epidermal growth factor receptor 2–negative (HR+/HER2−) advanced breast cancer (ABC). However, not all CDK4/6i trials have reported significant overall survival (OS) benefit, and there have been no head-to-head trials. Two trials have reported OS outcomes in first-line patients: MONALEESA-3 reported significant OS benefit with first- or second-line ribociclib plus fulvestrant (RIB+FUL) versus placebo plus fulvestrant (PBO+FUL), while PALOMA-1 reported no significant OS benefit for palbociclib plus letrozole (PAL+LET) versus LET in first-line postmenopausal patients. Matched-adjusted indirect comparisons (MAICs) are an established method for comparing efficacy of treatments from different trials. We used an MAIC to compare first-line patients from MONALEESA-3 and PALOMA-1.
Patients and Methods: An unanchored MAIC of progression-free survival (PFS) and OS in first-line patients with HR+/HER2− ABC treated with RIB+FUL versus PAL+LET was conducted using individual patient data from MONALEESA-3 and aggregated data from PALOMA-1. To match patients in PALOMA-1, patients in MONALEESA-3 were limited to those with no prior endocrine therapy for ABC and no (neo) adjuvant LET ≤ 12 months before enrollment. PFS and OS were compared using Kaplan–Meier estimators and Cox regression.
Results: A total of 329 and 178 patients from RIB+FUL and PBO+FUL arms, respectively, of MONALEESA-3 were matched to 84 and 81 patients from PAL+LET and LET arms of PALOMA-1. After weighting, OS was significantly longer for RIB+FUL versus PAL+LET (hazard ratio [HR], 0.50; 95% CI, 0.32– 0.77; p = 0.0020). PFS favored RIB+FUL versus PAL+LET, although the difference was not statistically significant (HR, 0.77; 95% CI, 0.54– 1.10; p = 0.1553).
Conclusion: Using MAIC to adjust for trial differences, OS comparisons favored RIB+FUL over PAL+LET as first-line treatment in postmenopausal patients with HR+/HER2− ABC. These exploratory results suggest a significant increase in OS benefit with RIB treatment compared with PAL.
Keywords: MONALEESA-3, PALOMA-1, overall survival, CDK4/6 inhibitor
Introduction
Cyclin-dependent kinase (CDK) 4/6 inhibitors, including ribociclib, palbociclib, and abemaciclib, in combination with an aromatase inhibitor (AI) or fulvestrant are the standard of care for treatment of patients with hormone receptor–positive and human epidermal growth factor receptor 2–negative (HR+/HER2−) advanced breast cancer (ABC) who have not received prior treatment for advanced disease. The use of CDK4/6 inhibitors in the first-line setting is based on the results of several phase 3, randomized, placebo-controlled trials in exclusively first-line patients or combined populations of patients receiving first and subsequent lines of therapy.1–7 However, no head-to-head trials have been conducted that compare CDK4/6 inhibitors in this setting.
The phase 3 MONALEESA-3 trial, which compared ribociclib plus fulvestrant versus placebo plus fulvestrant in postmenopausal women who had received no more than one prior endocrine therapy (ET) for advanced disease, and the phase 3 MONALEESA-7 trial, which compared ribociclib plus an AI or tamoxifen versus placebo plus an AI or tamoxifen in pre-/perimenopausal women who had received no prior ET for advanced disease, have reported significant overall survival (OS) benefit with ribociclib treatment.6–10 OS data for phase 3 studies of other CDK4/6 inhibitors in combination ET in the first-line setting, including the phase 3 PALOMA-2 trial of palbociclib plus letrozole and the phase 3 MONARCH-3 trial of abemaciclib plus letrozole, have not yet been published.1,3 However, the well-designed phase 2 PALOMA-1 trial of palbociclib plus letrozole versus letrozole in first-line postmenopausal patients has reported data on both progression-free survival (PFS) and OS.11,12 A comparison of ribociclib plus fulvestrant versus palbociclib plus letrozole based on data from MONALEESA-3 and PALOMA-1 may aid in understanding potential differences in survival outcomes for patients receiving different CDK4/6 inhibitor/endocrine combinations in the first-line setting. The ET partners used in MONALEESA-3 (fulvestrant) and PALOMA-1 (letrozole) differ. However, the PARSIFAL study demonstrated a median PFS of 27.9 vs 32.8 months (HR, 1.13 [95% CI, 0.89–1.45]; P = 0.321) for palbociclib plus fulvestrant vs palbociclib plus letrozole. The 3-year OS rate was 79.4% vs 77.1% (HR, 1 [95% CI, 0.68–1.48]; P = 0.986). The relatively consistent PFS and OS outcomes observed in PARSIFAL when first-line palbociclib was combined with letrozole or with fulvestrant suggested that these two ET partners could potentially be used in a comparison.13
Matching-adjusted indirect comparison (MAIC) is a methodology that has been used to compare two treatments in the absence of randomized controlled trials comparing these treatments directly and is accepted by some health technology assessment agencies.14 With MAIC, individual patient data (IPD) from one trial are weighted such that the aggregate statistics for baseline characteristics match those for patients in the other trial of interest as reported in the associated study publication. Weighting ensures that comparisons of efficacy across studies are not biased by differences in patient characteristics (though they may be biased by unobserved factors that are not matched by weighting).14 MAIC is similar to propensity score weighting, as with both approaches, patients in one study are weighted such that the aggregate baseline characteristics of that trial match those of the other. However, whereas propensity score weighting requires individual patient data from both trials (in order to conduct logistic regression analysis to calculate propensity scores and associated weights), MAIC requires individual patient data from only one of the two trials and uses the method of moments to calculate the weights.
The objective of this study was to conduct an MAIC of PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole as first-line treatment of HR+/HER2− ABC based on the results of the MONALEESA-3 (NCT02422615) and PALOMA-1 (NCT00721409) trials.
Materials and Methods
Overview
This study entailed an MAIC of PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole as first-line treatment of HR+/HER2− ABC using IPD from the MONALEESA-3 trial, for which IPD was available, and summary data reported in the study publication of the PALOMA-1 trial.11 To match patients in PALOMA-1, patients in MONALEESA-3 were limited to those with no prior ET for advanced disease and no (neo) adjuvant letrozole in the 12 months prior to enrollment. Patients in each arm (active treatment and control) of MONALEESA-3 were then weighted so that summary statistics on baseline characteristics for the selected patients matched those reported for patients in the corresponding arms of PALOMA-1. While the primary focus was on the comparison of active arms of the two trials, the control arms (placebo plus fulvestrant in MONALEESA-3 and letrozole in PALOMA-1) were also compared to permit assessment of the adequacy of matching, given prior published information regarding the relative efficacy of fulvestrant and letrozole in a first-line population. Data from MONALEESA-3 were from the same database closure, which was used for the final per protocol OS analysis (June 3, 2019, data cutoff). Data for PALOMA-1 were from the final analysis reported by Finn et al in Lancet Oncology in 2015 (November 29, 2013, data cutoff).11
The MONALEESA-3 trial was conducted in accordance with the Good Clinical Practice guidelines and Declaration of Helsinki. Written informed consent was provided by all the patients. The study protocol and any modifications were approved by an independent ethics committee or institutional review board at each site (Supplemental Table 1). A steering committee comprising participating international investigators and Novartis representatives oversaw the study conduct. An independent data monitoring committee assessed the safety data.
MAIC Weighting
Patient baseline demographic and disease characteristics used in the matching procedure included all those characteristics reported in the published reports of the PALOMA-1 trial that could be calculated for patients in MONALEESA-3 and included the following: age (<65 years, ≥65 years); Eastern Cooperative Oncology Group performance status (ECOG PS; 0, 1); stage (II/III, IV); site of metastasis (visceral, bone only); prior chemotherapy (yes, no); prior ET (tamoxifen, anastrozole, letrozole, exemestane); and time to disease recurrence (>12 months, ≤12 months, de novo).
Calculation of MAIC weights was conducted using the method of moments with active treatment and control arms weighted separately.14 Distributions of inverse probability of treatment weights for patients in MONALEESA-3 were plotted as histograms. Effective sample sizes were calculated.
Analyses
PFS and OS were compared for ribociclib plus fulvestrant (from MONALEESA-3) versus palbociclib plus letrozole (from PALOMA-1) and for placebo plus fulvestrant (from MONALEESA-3) versus letrozole (from PALOMA-1) using Kaplan–Meier methods. Time-to-event data for PFS and OS for patients in PALOMA-1 were obtained by digitizing the reported Kaplan–Meier curves for PFS and OS in the trial publication. Reconstructed individual patient event-time data for PFS and OS for palbociclib plus letrozole and letrozole monotherapy were generated using an adaptation of a published algorithm.15
Kaplan–Meier curves were generated for PFS and OS for active and control arms alternately using the unweighted and weighted data from MONALEESA-3. Results based on weighted data are less likely to be confounded than those based on unweighted data; the latter are provided for transparency. Kaplan–Meier estimates of median, 12-, and 24-month PFS and OS were calculated for ribociclib plus fulvestrant versus palbociclib plus letrozole and for placebo plus fulvestrant versus letrozole using the unweighted and weighted samples from MONALEESA-3. Inferential statistics (95% CIs and P values) for median, 12-, and 24-month PFS and OS were calculated using nonparametric bootstrapping. The bootstrapping procedure included the estimation of the MAIC weights.
Hazard ratios (HRs) for PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole and for placebo plus fulvestrant versus letrozole were calculated using Cox proportional hazards regression analysis using the unweighted and weighted samples from MONALEESA-3. Inferential statistics for HRs from Cox regression were based on robust sandwich estimators.14 The validity of the proportional hazards assumptions for the comparison of PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole and for the comparison of placebo plus fulvestrant versus letrozole was assessed based on the test of the linearity of the Schoenfeld residuals.
Calculation of MAIC weights was conducted in R (R Core Team, Vienna, Austria: http://www.R-project.org/) using an adaptation of sample code from the NICE DSU Technical Support Document 18: Methods for Population-Adjusted Indirect Comparisons in Submission to NICE.16 Kaplan–Meier curve estimation and Cox regression were conducted using SAS (SAS Institute, Cary, North Carolina, USA).
Results
Study Subjects
The identification of patients in MONALEESA-3 who met criteria for inclusion in PALOMA-1 is shown in (Figure 1). Of the 484 and 242 patients enrolled in MONALEESA-3 randomized to ribociclib plus fulvestrant and placebo plus fulvestrant, respectively, 110 (23%) and 44 (18%) were excluded due to receipt of ET in the advanced setting. An additional 45 of 484 (9%) and 20 of 242 (8%) were excluded for receipt of letrozole within 12 months of enrollment. A total of 329 of 484 (68%) patients receiving ribociclib plus fulvestrant and 178 of 242 (74%) patients receiving placebo plus fulvestrant were included in the analysis.
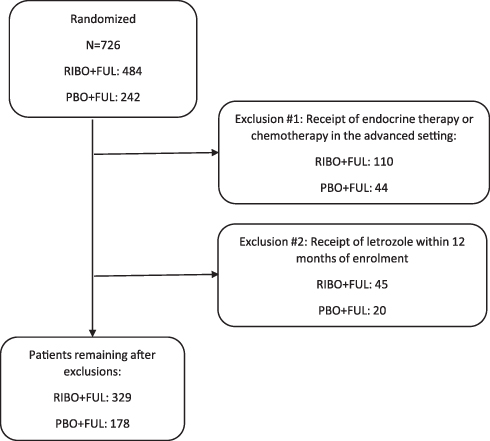 |
Figure 1 MONALEESA-3 patient selection. |
Patient Characteristics
Baseline characteristics for selected patients from MONALEESA-3 and all patients from PALOMA-1 before MAIC weighting are reported in Table 1. Patients from MONALEESA-3 were similar to patients from PALOMA-1 (standardized mean difference <10%) in terms of age and disease stage. However, patients in MONALEESA-3 were less likely to have ECOG PS = 1, more likely to have visceral or bone-only metastases (versus other nonvisceral), and more likely to have received prior antihormonal therapy. MAIC weighting was able to match all characteristics included in the matching algorithm.
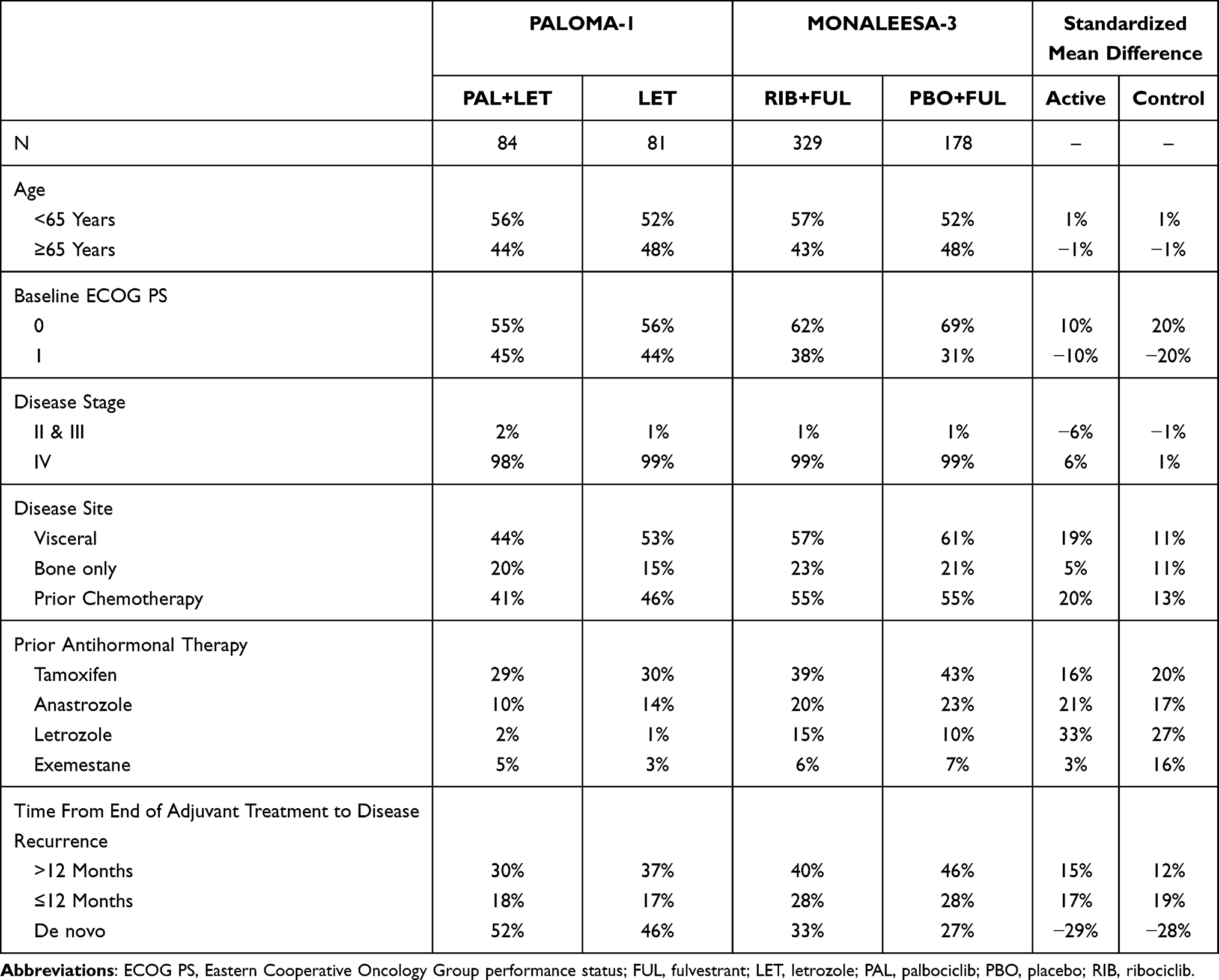 |
Table 1 Characteristics of Patients in PALOMA-1 and MONALEESA-3 Meeting Inclusion Criteria for PALOMA-1 Before Weighting |
MAIC Weights
Histograms of the distribution of MAIC weights for patients receiving ribociclib plus fulvestrant and placebo plus fulvestrant in MONALEESA-3 who met criteria for inclusion in PALOMA-1 are shown in Figure 2. The weights ranged from 0.00003 to 3.272 for ribociclib plus fulvestrant and from 0.044 to 3.788 for placebo plus fulvestrant. The 2.5th to 97.5th percentile range was 0.087 to 2.970 for ribociclib plus fulvestrant and 0.080 to 2.558 for placebo plus fulvestrant. After weighting, the effective sample size was estimated to be 221 for ribociclib plus fulvestrant and 117 for placebo plus fulvestrant; compared with the original sample for the selected patients, this represents a 33% reduction in sample size for the former and a 34% reduction in sample size for the latter.
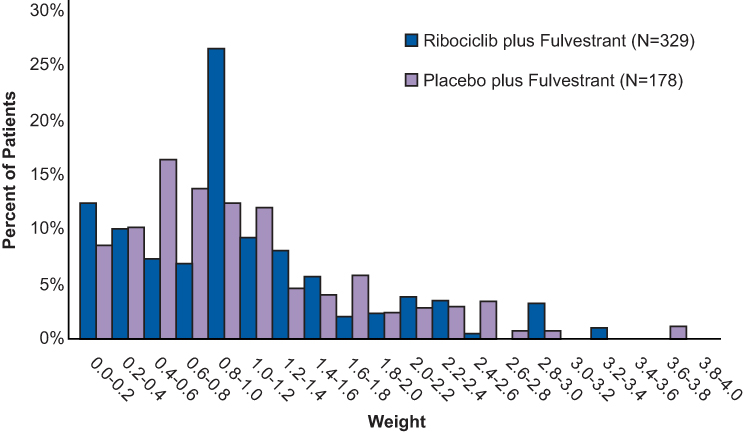 |
Figure 2 Distribution of match-adjusted indirect comparison weights for patients in MONALEESA-3 meeting inclusion criteria for PALOMA-1. |
PFS
Kaplan–Meier estimates of PFS for patients in PALOMA-1 and selected patients in MONALEESA-3 are shown in Figure 3. The median PFS for ribociclib plus fulvestrant (weighted) was 27.8 months (95% CI, 23.8–35.8), while the median PFS for palbociclib plus letrozole (based on reconstructed data) was 20.5 months (95% CI, 14.1–27.5). The estimated difference in median PFS was 7.4 months (95% CI, −0.7 to 17.3) and the estimated HR was 0.77 (95% CI, 0.54–1.10; p = 0.1553) (Table 2). The median PFS for placebo plus fulvestrant (weighted) was 16.5 months (95% CI, 12.9–21.9) compared with a median PFS for letrozole alone (based on reconstructed data) of 10.0 months (95% CI, 5.8–13.0). The estimated difference in median PFS was 6.5 months (95% CI, 1.7–14.4) and estimated HR was 0.58 (95% CI, 0.42–0.82; p = 0.0019) (Table 3). Overall, analyses using unweighted data were generally consistent with that of the weighted data.
 |
Table 2 Cox Regression Analysis of PFS and OS: RIB+FUL versus PAL+LET |
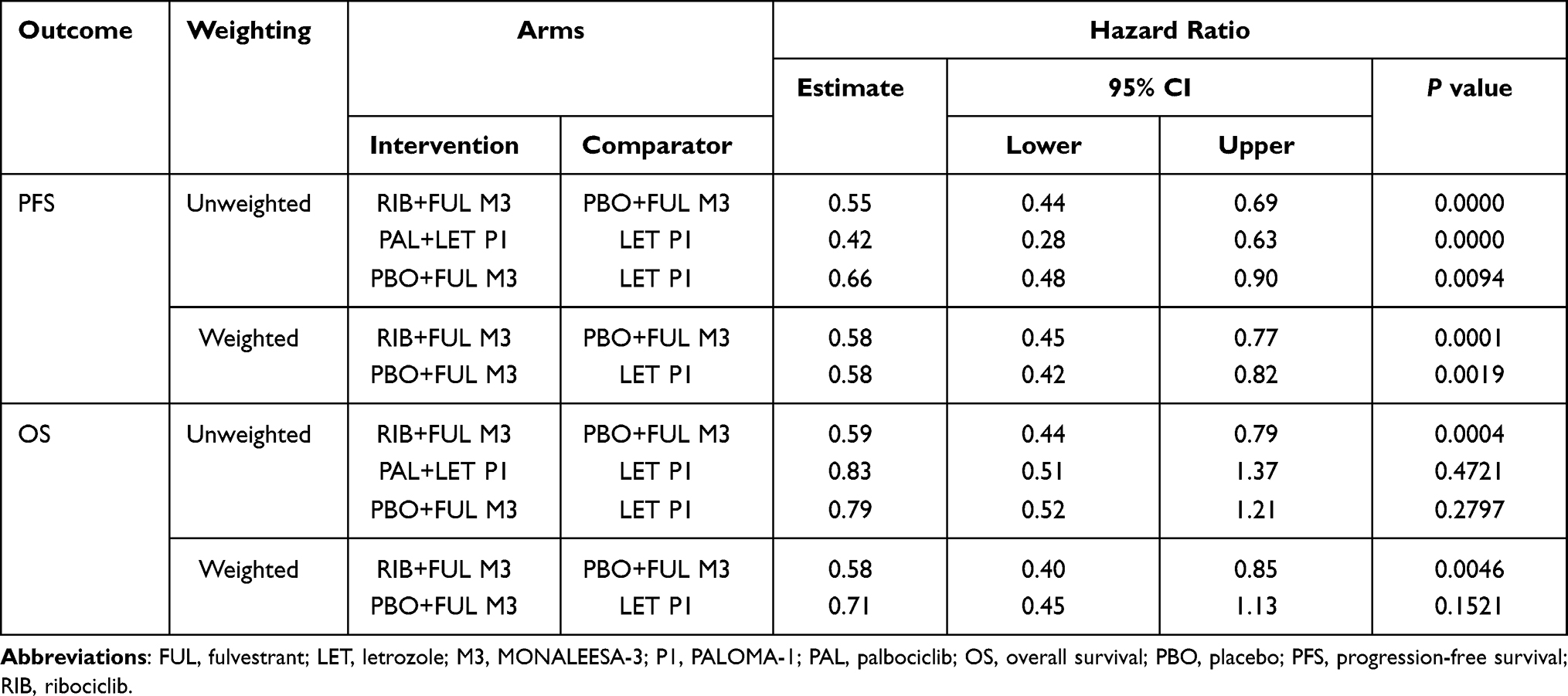 |
Table 3 Cox Regression Analysis of PFS and OS: RIB+FUL versus PBO+FUL, PAL+LET versus LET or PBO+FUL versus LET |
 |
Figure 3 Kaplan–Meier (A) PFS for RIB+FUL versus PAL+LET, (B) PFS for PBO+FUL versus LET, (C) OS for RIB+FUL versus PAL+LET, (D) OS for PBO+FUL versus LET. |
For patients in MONALEESA-3 meeting inclusion criteria for PALOMA-1, the HR for PFS for ribociclib plus fulvestrant (weighted) versus placebo plus fulvestrant (weighted) was 0.58 (95% CI, 0.45–0.77; p = 0.0001). The HR for PFS for palbociclib plus letrozole versus letrozole based on the reconstructed event-time data was 0.42 (95% CI, 0.28–0.63; p < 0.0001).
OS
Kaplan–Meier estimates of OS for patients in PALOMA-1 and selected patients in MONALEESA-3 are shown in Figure 3. The median OS was not estimable for ribociclib plus fulvestrant (weighted) and the median OS was also not estimable for palbociclib plus letrozole (based on reconstructed data). The HR for ribociclib plus fulvestrant (weighted) versus palbociclib plus letrozole was 0.50 (95% CI, 0.32–0.77; p = 0.0020). Median OS was 40.4 months (95% CI, 39.6-not estimable [NE]) for placebo plus fulvestrant (weighted) compared with 33.2 months (95% CI, 27.2-NE) for letrozole (based on reconstructed data). The estimated difference in median OS for the control arms of the two trials was 7.2 months (95% CI, NE-NE). The HR for OS for placebo plus fulvestrant versus letrozole was 0.71 (95% CI, 0.45–1.13; p = 0.1521). Overall, analyses using unweighted data were generally consistent with that of the weighted data.
For patients in MONALEESA-3 meeting criteria for inclusion of PALOMA-1, the HR for OS for ribociclib plus fulvestrant (weighted) versus placebo plus fulvestrant (weighted) was 0.58 (95% CI, 0.40–0.85; p = 0.0046). The HR for OS for palbociclib plus letrozole versus letrozole in PALOMA-1 based on the reconstructed event time data was 0.83 (95% CI, 0.51–1.37; p = 0.4721).
Discussion
The objective of this study was to compare PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole when used as first-line therapy for postmenopausal women with HR+/HER2− ABC based on the results of an MAIC of the MONALEESA-3 and PALOMA-1 trials. IPD for patients in the MONALEESA-3 trial were obtained from Novartis. Aggregate data from PALOMA-1 were obtained from the PALOMA-1 study publication. As patients in PALOMA-1 generally represented a subset of those enrolled in MONALEESA-3, it was possible to select a subgroup of patients from MONALEESA-3 who would meet the criteria for inclusion in PALOMA-1. While these selected patients differed in many reported baseline characteristics from those in PALOMA-1, MAIC weighting eliminated all differences between trials in observed baseline characteristics. After adjusting for differences in patient populations in the MONALEESA-3 and PALOMA-1 trials, a significant benefit for OS was observed as well as numerically longer PFS for ribociclib plus fulvestrant versus palbociclib plus letrozole. Comparison of the endocrine monotherapy arms of these two trials favored fulvestrant over letrozole, which is similar to what has been reported in prior clinical studies such as FIRST, which showed improved time to progression and OS for fulvestrant versus anastrozole and FALCON, which showed improved PFS.17,18 It should be noted that these two studies had inclusion criteria that may have resulted in differences in patient populations compared with MONALEESA-3 and PALOMA-1. FIRST included patients with tumors that were HER2+, and FALCON included only patients with no prior ET (ET naïve). Additionally, the PFS benefit in FALCON was observed mainly in patients with bone-only disease and to a lesser extent in patients with visceral disease.19 The PARSIFAL trial, which was conducted in a first-line population, showed that the potential advantage of fulvestrant over letrozole was lost when a CDK4/6 inhibitor was added. In PARSIFAL, the median PFS for first-line palbociclib plus fulvestrant was 27.9 months versus 32.8 months for palbociclib plus letrozole (HR, 1.13 [95% CI, 0.89 −1.45]; P = 0.321). The primary endpoint analysis did not show statistical superiority or non-inferiority in PFS for palbociclib plus fulvestrant versus palbociclib plus letrozole. The 3-year OS rate was 79.4% versus 77.1% (HR, 1 [0.68–1.48]; P = 0.986), the objective response rate was 46.5% versus 50.2% (P = 0.414), and the clinical benefit rate was 70.8% versus 69.1% (P = 0.692). These data suggest that the efficacy of fulvestrant versus letrozole when combined with a CDK4/6 inhibitor may be similar, and that the significantly favorable OS observed in the current MAIC analysis may not be due to the difference in ET partner and thus possibly a difference in the CDK4/6 inhibitor agent per se.13
While MAIC is a relatively novel methodology, it has been used with increasing frequency in recent years. A search of MEDLINE for articles including the words “matching-adjusted indirect treatment comparison” and “cancer” in the title identified 32 articles published from 2017 to 2021, including one study of patients with breast cancer.20 This study used MAIC to compare PFS and OS and frequency of adverse events for ribociclib plus letrozole versus palbociclib plus letrozole using individual patient data from MONALEESA-2 and published results of PALOMA-2 (for PFS) and PALOMA-1 (for OS). The indirect treatment comparison of ribociclib plus letrozole versus palbociclib plus letrozole used MAIC-unadjusted and MAIC-adjusted data from MONALEESA-2, and was conducted using anchored indirect comparisons through the common comparator arm of letrozole using the Bucher method.21 The HR for PFS for ribociclib plus letrozole versus palbociclib plus letrozole based on the Bucher indirect treatment comparison was 0.959 (95% CI, 0.681–1.350) before MAIC adjustment and 0.904 (95% CI, 0.644–1.268) after MAIC adjustment. The HR for OS for ribociclib plus letrozole versus palbociclib plus letrozole was 0.918 (95% CI, 0.492–1.710) before MAIC adjustment and 0.839 (95% CI, 0.440–1.598) after MAIC adjustment.20
Limitations of this analysis should be noted. Our results are based on unanchored indirect comparison. While such comparisons are generally considered less robust than anchored comparisons, an anchored comparison of ribociclib plus fulvestrant versus palbociclib plus letrozole was not feasible, as it is not possible to construct a linked evidence network of trials in comparable populations connecting fulvestrant (the control arm of MONALEESA-3) with letrozole (the control arm of PALOMA-1) without some relatively strong assumptions regarding the impact of differences in patient characteristics across trials on treatment effects. Although trials comparing fulvestrant with the AI, anastrozole, (FIRST and FALCON) have been reported,18,22 the populations of these studies differ from that evaluated in PALOMA-1. In particular, FIRST allowed the inclusion of patients that were HER2+, and FALCON included only patients that had no prior ET. In contrast, MONALEESA-3 and PALOMA-1 included only patients that were HR+/HER2−, and both allowed prior (neo) adjuvant ET. While it might be feasible to construct an evidence network linking fulvestrant and letrozole using trials of other treatments such as tamoxifen and exemestane, construct of such a network would require the relaxation of one or more of the inclusion criteria of PALOMA-1 to include these trials and also require additional links in the network, each associated with additional uncertainty and possibility of bias. Additional limitations include differences in study design between the two trials. MONALEESA-3 was a double-blind phase 3 trial and PALOMA-1 was an open-label phase 2 trial; both were randomized, multicenter, international trials.
The limitations in anchored comparisons of ribociclib plus fulvestrant versus palbociclib plus letrozole above notwithstanding, Giuliano and colleagues conducted a network meta-analysis (NMA) of ET versus chemotherapy in postmenopausal women with HR+/HER2− MBC and reported numerically more favorable but statistically similar PFS for palbociclib plus letrozole versus anastrozole (HR = 0.42; 95% CI, 0.25–0.70) and ribociclib plus fulvestrant versus anastrozole (HR = 0.48; 95% CI, 0.31–0.74).23 OS was not examined. In an anchored ITC of CDK4/6 inhibitors in combination with letrozole in HR+/HER2− ABC, Petrelli and colleagues reported similar PFS for palbociclib plus letrozole versus ribociclib plus letrozole (HR = 1.04; 95% CI, 0.73–1.48).24 This study did not evaluate efficacy of CDK4/6 inhibitors in combination with fulvestrant and also did not examine OS. The results of these studies with respect to PFS are therefore qualitatively consistent with those reported herein and provide no information with respect to the comparison of OS.
While there is no widely accepted “reasonable range” for MAIC weights, large outlier weights may indicate that a small proportion of patients in the weighted group are similar to those in the unweighted group and therefore the effective sample size may be small. The maximum weights in our study were 3.272 for ribociclib plus fulvestrant and 3.788 for placebo plus fulvestrant. Thus, it is not likely that patients with large weights had an undue influence on results. While some patients had relatively small weights (the minimum weights were 0.00003 and 0.044 for ribociclib plus fulvestrant and placebo plus fulvestrant, respectively), this is not a problem per se but rather suggests that some patients in MONALEESA-3 were relatively dissimilar to those in PALOMA-1 and were therefore effectively excluded, which is appropriate.
The MAIC methodology can only control for the characteristics reported in the study publication of the PALOMA-1 trial; results therefore may be confounded by other unreported factors. However, as noted previously, the finding of significantly improved PFS and numerically improved OS for the placebo plus fulvestrant arm of MONALEESA-3 versus the letrozole arm of PALOMA-1 is consistent with published, randomized controlled trials of fulvestrant versus AIs, suggesting that unobserved confounding may be limited.17,18
PFS and OS for PALOMA-1 were based on reconstructed IPD. Although the reconstructed Kaplan–Meier curves were similar to the reported curves, it was not feasible to exactly match the reported curves from PALOMA-1. The HR for PFS for palbociclib plus letrozole versus letrozole based on the reconstructed event-time data was 0.42 (95% CI, 0.28–0.63; p < 0.0001), which is more favorable than that reported in the trial publication for PALOMA-1 (HR, 0.488; 95% CI, 0.319–0.748; p = 0.0004).11 On the other hand, the HR for OS for palbociclib plus letrozole versus letrozole based on the reconstructed event-time data was 0.83 (95% CI, 0.51–1.37; p = 0.4721), which is less favorable than that reported in the trial publication for PALOMA-1 (HR, 0.813; 95% CI, 0.492–1.345; p = 0.42).11 Given that the differences in the results based on the actual and reconstructed IPD are relatively small, they are not likely to substantially bias the findings reported here.
According to the study publication,11 PALOMA-1 excluded patients who “had brain metastases” whereas MONALEESA-3 excluded “patients with central nervous system (CNS) involvement unless they met ALL of the following criteria: a. At least 4 weeks from prior therapy completion (including radiation and/or surgery) to starting the study treatment. b. Clinically stable CNS tumor at the time of screening and not receiving steroids and/or enzyme inducing anti-epileptic medications for brain metastases.”
While patients with brain metastases were not excluded from the analysis, the number of patients with CNS metastases within the subgroup of patients in MONALEESA-3 who met inclusion criteria for PALOMA-1 was small. Given this small proportion of patients and that those with stable brain metastases are more likely to have a better prognosis than those with brain metastases overall, the inclusion of these patients in MONALEESA-3 is not likely to have materially impacted the comparison. Furthermore, because patients with brain metastases generally have a poorer prognosis than those without, any bias (likely small) would favor palbociclib plus letrozole.
Conclusion
CDK4/6 inhibitors in combination with an AI or fulvestrant are the standard of care for patients with HR+/HER2− ABC who have not received prior treatment for advanced disease. Although randomized controlled trials comparing the approved CDK4/6 inhibitor combinations are not available, it is important to understand if there are any differences in efficacy between the approved agents. Unadjusted cross-trial comparisons are difficult to interpret since patient characteristics may differ between the trials of interest. However, matched indirect comparisons can be more informative because they account and control for differences in patient characteristics. Our analysis, using an MAIC methodology to compare PFS and OS for ribociclib plus fulvestrant versus palbociclib plus letrozole based on the MONALEESA-3 and PALOMA-1 trials, demonstrated a significantly longer OS and numerically longer PFS with ribociclib plus fulvestrant. These exploratory results suggest a significant increase in OS benefit with ribociclib treatment compared with palbociclib in this group of patients, which may be useful for patients, clinicians, and policy makers when considering the use of CDK4/6 inhibitors in this setting.
Acknowledgments
This study was sponsored by Novartis, which also provided financial support for medical editorial assistance. We thank William Ho, PhD, of MediTech Media, for medical editorial assistance with this manuscript. Ribociclib was discovered by Novartis Institutes for BioMedical Research in collaboration with Astex Pharmaceuticals. Data from this paper were presented at the European Society for Medical Oncology Virtual Congress 2020 as a poster presentation with interim findings. The poster’s abstract was published in Ann Oncol. 2020;31(Supplement 4):S377-S378; https://doi.org/10.1016/j.annonc.2020.08.432.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to take responsibility and be accountable for the contents of the article.
Funding
The financial support for this study was provided by Novartis.
Disclosure
PAF reports personal fees for advisory boards from Novartis, Roche, Pfizer, Celgene, Merck Sharp & Dohme, Macrogenics, Eisai, Puma, Lilly, AstraZeneca; lectures from Daiichi-Sankyo, Merck Sharp & Dohme, Lilly; research support from BionTech, Cepheid, and Novartis. TED reports personal fees and research funding from Novartis and Pfizer. YSL reports clinical trial study fees from Novartis; grants from Astra Zenica, Eli Lilly, Novartis, Roche, Merck Sharp & Dohme, and Pfizer; personal fees from Pfizer, Boehringer Ingelheim, and Eisai. RDB reports personal fees from Novartis, Pfizer, Eli Lilly, Roche, Genomic Health, AstraZeneca. SAH reports grants from Ambryx, Amgen, AstraZeneca, Arvinas, Bayer, Cytomx, Daiichi Sankyo, Dignitana, Genentech/Roche, Gilead, Glaxo-Smith Kline, Immunomedics, Lilly, Macrogenics, Novartis, Obi Pharma, Pfizer, Pieris, Puma Biotechnology, Radius, Sanofi, Samumend, Seattle Genetics, Zymeworks, Phoenix Molecular Designs Ltd.; travel from Lilly. AM reports grants from Novartis. DC reports employment and stock ownership from Novartis. BL reports employment and stock ownership from Novartis. HH reports employment and stock ownership from Novartis. AT reports employment and stock ownership from Novartis. JO reports personal fees for consulting/advisory boards from AbbVie, Agendia, Amgen, Aptitude Health, AstraZeneca, Bayer, Bristol-Myers Squibb, Celgene, Clovis Oncology, Daiichi Sankyo, Eisai, G1 Therapeutics, Genentech, Gilead Sciences, GRAIL, Halozyme, Heron, Immunomedics, Ipsen, Lilly, Merck, Myriad, Nektar, Novartis, Pfizer, Pharmacyclics, Pierre Fabre, Puma, Prime Oncology, Roche, Samsung Bioepis, Sanofi, Seagen, Syndax Pharmaceuticals, Taiho Oncology, Takeda, Synthon, and Seattle Genetics. The authors report no other conflicts of interest in this work.
References
1. Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925–1936. doi:10.1056/NEJMoa1607303
2. Cristofanilli M, Turner NC, Bondarenko Iet al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): final analysis of the multicentre, double-blind, phase 3 randomised controlled trial. Lancet Oncol. 2016;17:425–439. doi:10.1016/S1470-2045(15)00613-0
3. Goetz MP, Toi M, Campone M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. 2017;35(32):3638–3646. doi:10.1200/JCO.2017.75.6155
4. Sledge GW
5. O’Shaughnessy J, Petrakova K, Sonke GS, et al. Ribociclib plus letrozole versus letrozole alone in patients with de novo HR+, HER2- advanced breast cancer in the randomized MONALEESA-2 trial. Breast Cancer Res Treat. 2018;168(1):127–134. doi:10.1007/s10549-017-4518-8
6. Slamon DJ, Neven P, Chia S, et al. Phase III randomized study of ribociclib and fulvestrant in hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer: MONALEESA-3. J Clin Oncol. 2018;36(24):2465–2472. doi:10.1200/JCO.2018.78.9909
7. Tripathy D, Im SA, Colleoni M, et al. Ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive, advanced breast cancer (MONALEESA-7): a randomised phase 3 trial. Lancet Oncol. 2018;19(7):904–915. doi:10.1016/S1470-2045(18)30292-4
8. Slamon D, Neven P, Chia S. Ribociclib + fulvestrant in postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: results from MONALEESA-3. ASCO 2018 Annual Meeting; 2018.
9. Slamon D. Overall survival results from the Phase III MONALEESA-3 study of fulvestrant ± ribociclib in postmenopausal patients with HR+/HER2− advanced breast cancer. ESMO 2019 Congress. Barcelona; 2019.
10. Tripathy D, Sohn J, Im S, et al. First-line ribociclib vs placebo with goserelin and tamoxifen or a non-steroidal aromatase inhibitor in premenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: results from the randomized phase III MONALEESA-7 trial. San Antonio Breast Cancer Symposium Publication Number: GS2-05; 2017.
11. Finn RS, Crown JP, Lang I, et al. The cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2-negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 study. Lancet Oncol. 2015;16(1):25–35. doi:10.1016/S1470-2045(14)71159-3
12. Finn RS, Boer K, Bondarenko I, et al. Overall survival results from the randomized phase 2 study of palbociclib in combination with letrozole versus letrozole alone for first-line treatment of ER+/HER2- advanced breast cancer (PALOMA-1, TRIO-18). Breast Cancer Res Treat. 2020;183(2):419–428.
13. Llombart-Cussac A, Pérez-García JM, Bellet M, et al. PARSIFAL: a randomized, multicenter, open-label, Phase II trial to evaluate palbociclib in combination with fulvestrant or letrozole in endocrine-sensitive patients with estrogen receptor (ER)[+]/HER2[-] metastatic breast cancer. J Clin Oncol. 2020;38(15_suppl):1007. doi:10.1200/JCO.2020.38.15_suppl.1007
14. Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton Nj. Methods for population-adjusted indirect comparisons in health technology appraisal. Med Decis Making. 2018;38(2):200–211. doi:10.1177/0272989X17725740
15. Guyot P, Ades AE, Ouwens MJ, Welton NJ. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12:9. doi:10.1186/1471-2288-12-9
16. Phillippo DM, Ades AE, Dias S, Palmer S, Abrams KR, Welton NJ. NICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submission to NICE; 2016. Available from: http://www.nicedsu.org.uk.
17. Ellis MJ, Llombart-Cussac A, Feltl D, et al. Fulvestrant 500 mg versus anastrozole 1 mg for the first-line treatment of advanced breast cancer: overall survival analysis from the phase II FIRST study. J Clin Oncol. 2015;33(32):3781. doi:10.1200/JCO.2015.61.5831
18. Robertson JF, Bondarenko IM, Trishkina E, et al. Fulvestrant 500 mg versus anastrozole 1 mg for hormone receptor-positive advanced breast cancer (FALCON): an international, randomised, double-blind, phase 3 trial. Lancet. 2016;388(10063):2997–3005.
19. Ellis MJ, Bondarenko I, Trishkina E, et al. FALCON: a phase III randomised trial of fulvestrant 500 mg vs. anastrozole for hormone receptor-positive advanced breast cancer. Ann Oncol. 2016;27(6):1–36. doi:10.1093/annonc/mdw435
20. Tremblay G, Chandiwana D, Dolph M, Hearnden J, Forsythe A, Monaco M. Matching-adjusted indirect treatment comparison of ribociclib and palbociclib in HR+, HER2- advanced breast cancer. Cancer Manag Res. 2018;10:1319–1327. doi:10.2147/CMAR.S163478
21. Bucher HC, Guyatt GH, Griffith LE, Walter SD. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683–691. doi:10.1016/S0895-4356(97)00049-8
22. Robertson JF, Llombart-Cussac A, Rolski J, et al. Activity of fulvestrant 500 mg versus anastrozole 1 mg as first-line treatment for advanced breast cancer: results from the FIRST study. J Clin Oncol. 2009;27(27):4530–4535. doi:10.1200/JCO.2008.21.1136
23. Giuliano M, Schettini F, Rognoni C, et al. Endocrine treatment versus chemotherapy in postmenopausal women with hormone receptor-positive, HER2-negative, metastatic breast cancer: a systematic review and network meta-analysis. Lancet Oncol. 2019;20(10):1360–1369. doi:10.1016/S1470-2045(19)30420-6
24. Petrelli F, Ghidini A, Pedersini R, et al. Comparative efficacy of palbociclib, ribociclib and abemaciclib for ER+ metastatic breast cancer: an adjusted indirect analysis of randomized controlled trials. Breast Cancer Res Treat. 2019;174(3):597–604. doi:10.1007/s10549-019-05133-y
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.