Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Mapping the Role of Digital Health Interventions to Enhance Effective Coverage of Antenatal Care: A Scoping Review
Authors Endehabtu BF ![]() , Gelaye KA
, Gelaye KA ![]() , Mengiste SA, Tilahun B
, Mengiste SA, Tilahun B
Received 29 September 2023
Accepted for publication 22 December 2023
Published 5 January 2024 Volume 2024:17 Pages 71—82
DOI https://doi.org/10.2147/JMDH.S438097
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Berhanu Fikadie Endehabtu,1,2 Kassahun Alemu Gelaye,3 Shegaw Angaw Mengiste,4 Binyam Tilahun1,2
1Department of Health Informatics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Center for Digital Health and Implementation Science, University of Gondar, Gondar, Ethiopia; 3Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4School of Business, University of South-Eastern Norway, Drammen, Norway
Correspondence: Berhanu Fikadie Endehabtu, Department of Health Informatics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, 196, Ethiopia, Tel +251921013129, Email [email protected]
Background: Antenatal care (ANC) is a core component of maternal health services. However, only half of the pregnant women in LMICs obtain WHO recommended minimum of four antenatal contacts. In addition, ANC 4+ is a commonly used indicator in monitoring ANC utilization. However, contact coverage alone provides no indications of service quality. In recent years, digital health interventions bring opportunities to provide quality maternal health care. Yet, there are few reviews on how digital health interventions contribute to improving effective coverage of antenatal care. A rigorous review that examines the role of digital health interventions in improving effective coverage of antenatal care is needed to examine how digital health solutions were rapidly deployed to support quality antenatal care service delivery.
Objective: This review aimed to map evidence on the role of digital health solutions on quality of antenatal care service to enhance effective ANC coverage.
Methods: A scoping review approach was used and four Databases (PubMed, Cochrane Library, Scopus and Embase) as well as search engines like Advanced Google Search and Google Scholar were searched from September 1 to 8, 2022. Thematic content analysis was used to present the findings.
Results: A total of 1701 articles were searched. A total of 27 full-text studies were included in the final analysis. The most reported use of digital health was for client education and behavior change communication. Most studies showed that digital health interventions have proven effective in improving antenatal care. However, most of the studies did not address to assess the quality of ANC services.
Conclusion: In this review, we found out that digital health solutions targeted at pregnant women can improve antenatal care services. There is body of evidence showing the effectiveness of digital health interventions on a range of maternal health outcomes. Few pieces of literature exist on the use of digital health interventions on the quality of antenatal care services. There is a need for more trial and program evaluation studies that examine the role of digital health interventions on the quality of ANC.
Keywords: digital health, digital interventions, antenatal care services, scoping review
Introduction
From the period 1990 to 2015, the number of maternal mortality globally dropped by 43%.1 Too many women, in general, still die from preventable health issues during pregnancy and childbirth.2 At the beginning of the Sustainable Development Goals (SDGs), maternal morbidity and mortality remained unacceptably high in most low- and middle-income countries.1,3 Most developing countries remain far from universal coverage of maternal health services.3–5 The high maternal mortality rate is striking, given that the knowledge and technology needed to reduce it have been available for many decades, and the costs of intervention are relatively low and affordable for most.4
Antenatal care (ANC) is a central component of maternity care provided by skilled healthcare providers to ensure positive pregnancy outcomes for both the mother and her baby.6–8 It is a scheduled, client-centered obstetric care focused on the mother’s well-being and fetal health through regular pregnancy monitoring.6 It provides an opportunity to screen, diagnose, and treat pre-existing health problems and identify, prevent, promote, and manage health issues during pregnancy.9,10 It is a vital link in the continuum of care across reproductive, maternal, newborn, and child health services. The World Health Organization (WHO) recommends a core package of essential interventions for routine ANC to ensure better perinatal and maternal outcomes. The essential interventions package is adaptable to different settings for countries to contextualize them according to their needs and resource capacities.6 However, the intervention package’s effectiveness can be assured when delivered with a specific frequency, timing, and right content.6,11–13
Globally, four or more contacts with healthcare professionals (ANC 4+) are commonly used indicators in monitoring ANC utilization.14,15 The limitation of “crude” or “contact” coverage as a measure is that it only provides the frequency of visits and fails to capture the quality of services offered in those visits. The contact coverage alone provides no indications of service quality and potentially overestimates the health benefits of the services.11–13
Effective coverage, in contrast, combines service utilization with the quality of care received.16 Assessing the effective coverage of essential ANC interventions is more comprehensive than ANC4+ for assessing ANC service provision.17 However, globally, more than 40% of pregnant women were not receiving early antenatal care in 2013.18
Digital health interventions are currently at the forefront of improving healthcare delivery and healthcare systems. It is also being applied to support the provision of safe, accessible, coordinated, and effective maternal health care.19 Numerous digital health interventions are being used to improve antenatal care service uptake.
Yet, there are few reviews on how digital health interventions improve the quality of antenatal care services. A rigorous review that examines the role of digital health interventions in improving effective coverage of antenatal care is needed to examine how digital health solutions were rapidly deployed to support quality antenatal care service delivery.
The review research questions are: What are the available pieces of evidence on the role of a digital health intervention in effective coverage of antenatal care? What evidence is available on the role of digital health intervention in improving effective coverage of ANC? What types of digital health interventions tested and improved effective coverage of ANC have been reported globally?” What core packages of antenatal care interventions are included in the digital intervention?
To answer these questions, we applied a scoping literature review to map the evidence of the role of digital health solutions in a range of effective coverage of antenatal care by thermalizing the interventions according to the types of digital health solutions.
Method
This review was conducted following the Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist,20 and it was guided by Joanna Briggs Institute (JBI) scoping review guidance.21
Eligibility Criteria
All studies carried out worldwide involving digital health interventions to improve antenatal care were considered for inclusion, while all studies other than those in the English language were excluded. Studies for which we were unable to retrieve the full text were excluded. A population, concept, and context (PCC) framework was used to determine the eligibility of our primary research question. The study used the PCC framework (Table 1) to align the study selection with the research question.
 |
Table 1 Eligibility of Studies According to the Participant, Concept, and Context (PCC) Framework |
Data Source and Search Strategy
Four databases (PubMed, Cochrane Library, Scopus, and Embase) and search engines like Advanced Google Search and Google Scholar were searched. The reference lists of the retrieved and pertinent articles were also hand-searched. We used different combinations of keywords and text to build the search strategy and identify relevant articles. Medical Subject Headings (MeSH) were used wherever applicable, and Boolean operators (AND, OR) were used to specify combinations of search terms. The search terms were grouped into three major categories of interest: Participant, concept, and context.
Initial searches and screening of titles were performed by an author (BF). Screening of abstracts and full texts was done independently by two authors (BF and AN). Any differences of judgment were discussed, and a consensus was reached; otherwise, a third reviewer (DA) was involved in mediating unresolved issues.
Data Charting Process/ Extraction
Using a customized data extraction template, two reviewers (BF and AN) independently screened the abstracts and full text of selected studies against the inclusion and exclusion criteria. The data extraction sheet using existing literature was designed on an MS Excel spreadsheet. Disagreements between the two reviewers in this process were discussed with the third reviewer (DA) until a consensus was reached. The information extracted included the author’s name, year of publication, study title, the purpose of study, type of study design, health issue studied, sample size or interventional group, control group, primary or secondary intervention, and Outcomes and Key findings.
Data Analysis and Synthesis
Built on the methodological framework for scoping reviews,22 we presented our findings in two ways. First, introductory numerical analysis and the distribution of the studies are included in the review. We determined the type of studies and their distributions by geographical location. Secondly, the study findings from the existing literature were presented using thematic content analysis. Our result was then structured into three categories: 1) types of digital health interventions commonly used for antenatal care service uptake, 2) the core package of ANC interventions addressed, and 3) the effect of the interventions. Labrique et al framework was adapted to simplify the interpretation for categorizing the digital health interventions according to their purpose.
Results
A total of 1701 articles were retrieved from the initial search. After duplications were removed, a total of 1329 studies remained. Of the 1329 articles screened, the titles were screened for relevance, which drastically reduced the number to 141. Then, we read the abstracts of 141 articles, of which 42 were shortlisted. Among the 42 abstracts, 7 of them could not be retrieved. The full text of 35 articles was reviewed using a data extraction sheet. Eight out of the 35 full-text articles were unrelated to antenatal care service utilization. A total of 27 full-text articles were included in the final analysis (see Figure 1).
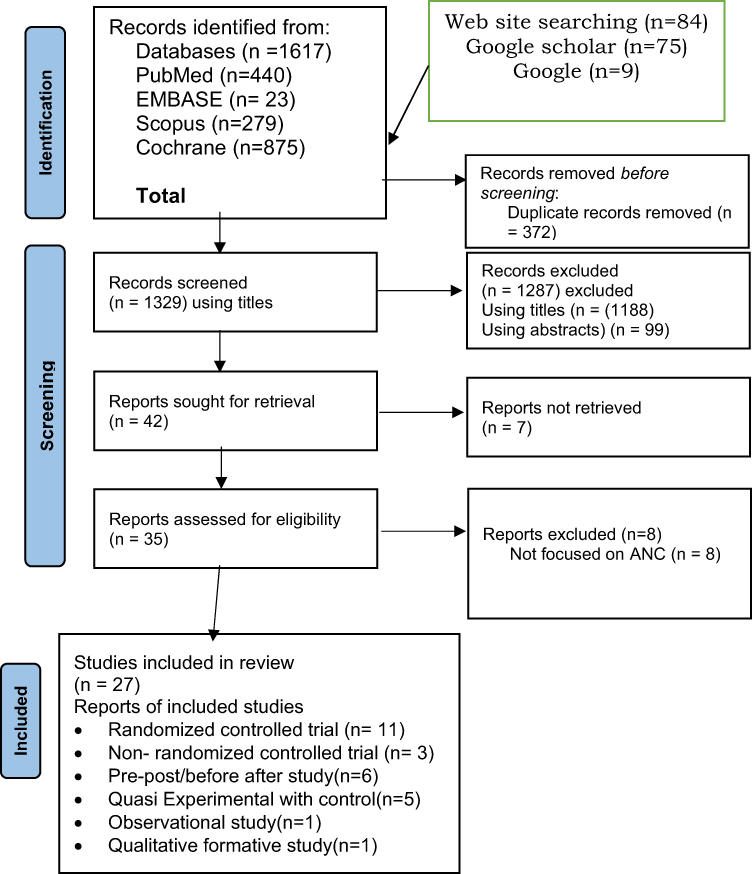 |
Figure 1 PRISMA (updated 2020) flow diagram for data bases and registry search of studies. Notes: PRISMA figure from Annals of Internal Medicine, Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473.20 Copyright © 2018 American College of Physicians. All Rights Reserved. Reprinted with the permission of American College of Physicians, Inc. |
Characteristics of Included Studies
Out of 27 studies that were included, 15 (56%) of them were conducted in Africa,23–37 nine were from Asia,33,38–45 two were from South America,46,47 and one Australia/Oceania.48 The other six studies were from six countries, Zanzibar, Nigeria, Samoa, Guinea, Bangladesh, and Myanmar, each contributing one.
The studies have different theoretical bases and designs. Eleven of these studies were randomized controlled trials; three were non-randomized controlled trials. Six were pre-post design studies; five were quasi-experimental designs with controls; the remaining two were observational and qualitative formative studies. The Studies included in the review were published from 2010 to 2022.
Types of Digital Health Interventions
The data from 27 final studies fall into six components of the mHealth and ICT applications framework developed by Labrique et al.49 The type of interventions in the above-mentioned studies lay in client education and behavior change communication, registries/vital event tracking, electronic decision support (information, protocols, algorithms, and checklists), data collection and reporting, provider-to-provider communication, and provider work planning and scheduling.
Of the 27 studies, 22 (81%) addressed client education and behavior change communication.23,26–29,31–38,41–48,50 Most of the studies were assigned to more than one category: Registries/vital event tracking (n=11),24–27,30,35,39–41,43,51 data collection and reporting (n=6),24,27,28,32,38,40 Provider to provider communication (n=2),34,35 electronic decision support (information, protocols, algorithms, checklists) (n=5),24,27,39–41 provider work planning and scheduling (n = 2).26,40 The results of the classification are illustrated below.
Client Education and Behavior Change Communication
Short message service (n=16),23,27–29,31,32,35,37,38,41–44,47,51 mobile midwife technology (n=1),33 mHealth intervention (voice message (n=1))50 and Mobile phone voucher component,34 RapidSMS system32 were among the digital interventions used for client education and behavior change communication. Some studies used multifaceted interventions. There are also studies with unspecified digital solutions for client education and behavior change communication.
Registries/Vital Event Tracking
CommCare mobile platform,24 RapidSMS system,25,26,51 mHealth application (unspecified),27 APAS software30 SMS based application (unspecified),35 eRegistry,39 a mobile application called Mobile for Mothers (MfM)41,43 were the interventions used for registration or vital event tracking.
Data Collection and Reporting
CommCare mobile platform,24 mHealth (unspecified)27 Mobile phone application,28 SGS collect,32 Smartphone application,38 and TeCHO+40 were among the digital interventions used for data collection and reporting.
Electronic Decision Support (Information, Protocols, Algorithms, Checklists)
CommCare mobile platform,24 mHealth application (unspecified),27 eRegistry,39 TeCHO+,40 and a mobile application—Mobile for Mothers (MfM)41 were used for electronic decision support.
Provider-to-Provider Communication
Only two studies and two digital applications: A frontline SMS-based application34 and SMS based application,35 were used for Provider-to-provider communication.
Provider Work Planning and Scheduling
Three studies used three interventions, such as the RapidSMS system,26 an SMS-based application (unspecified),35 and TeCHO+40 for provider work planning and scheduling.
The Content of the Antenatal Care Service Addressed
A total of 23 studies assessed the effectiveness of digital health interventions on the number of antenatal care visits. Fifteen studies23,27–29,31,32,34,37,38,41–45,47,51 treated the topic of antenatal follow-up reminders in improving ANC attendance. Based on the World Health Organization guideline,6 the reviewed studies are summarized in the following core packages of ANC interventions.
Maternal and Fetal Assessment
As mentioned above, 23 studies assessed the role of digital health solutions on antenatal care follow-up. However, only one study34 reports the effect of the intervention on early initiation and adherence to the ANC schedule. Four studies24,39,45,47 assessed the role of digital solutions on blood tests during ANC. Two of the studies24,47 included a blood test for Hgb, syphilis, blood type, and HIV, and the other two studies39 and 45 for anemia (Hgb) and blood group, respectively. Hypertension and gestational diabetes were assessed by three studies,24,28,39 fundal height and fetal growth monitoring,24,39 and Urine analysis24,47 were assessed.
Health Promotion, Prevention, and Treatment During Pregnancy
Health promotion, prevention, and treatment during pregnancy are core packages of antenatal care interventions. Most of the studies included in this review assessed at least one of the components. Tetanus vaccination,24,28,31,34,41,43–45,47,50 preventive treatment for malaria,24,31,34,36 delivery plan,23,24,26,27,29,35,41,43–45 child Vaccination,24,26,29,35,40,41 breastfeeding,23,24,28,40 Iron folic acid,23,24,31,40,41,43–45,47,50 PNC,23,26,27,45 danger sign of pregnancy,23,24,41 and deworming31 were the assessed core packages of the antenatal care interventions.
Strengthening the Healthcare System for ANC
Instituting continuous quality improvement and improving the documentation and reporting of ANC is one of the core packages of antenatal care interventions. Few studies reported the role of digital interventions in the documentation and reporting of ANC.24,27,28,40 Also, two studies reported that digital health interventions with decision-support algorithms produce recommendations for treatment, referral, and client follow-up.24,39
Effect on the Intended Outcome
Effect on Client Education and Behavior Change Communication
Most studies27–29,31–35,37,38,41–45,47,51 reported that digital interventions had a role in improved client education and behavior change communication.
A cluster randomized controlled trial in Zanzibar was conducted in primary health facilities. Twenty-four healthcare facilities were randomized to either the intervention or control groups. The intervention consisted of two components mobile phone voucher and short message service. The mobile phone voucher helped pregnant women to communicate with primary healthcare providers, and the SMS component was used to send appointment reminders and educational messages about ANC and PNC. The central outcome measure of the study was 4+ ANC visits. In the intervention category, 44% of women attained four or more ANC visits compared to 31% in the comparator group (OR, 2.39; 95% CI 1.03–5.55). Also, in the intervention group, 72% of women received two doses of tetanus vaccination versus 56% in the control group, and 65% received two doses of prophylaxis for malaria, 52% in the control group (OR, 1.97; 95% CI, 0.98–3.94). Most women in the intervention group mentioned that receiving text messages influenced the number of times they attended antenatal care, and the educational messages helped them know about pregnancy danger signs.34
Coleman et al29 reported that 72% of those exposed to SMS text messages had higher odds of attending the recommended four antenatal visits than 46% of participants in the control group (OR: 3.21, 95% CI 1.73–5.98).
A single-blind randomized controlled trial conducted in Kenya among 241 interventions and 119 groups reported that short message service improved the uptake of focused antenatal care. Short message reminders improved the probability of using focused antenatal care by 19.6 times (OR: 19.6, P<0.001, CI=10.06–38.37).37
A randomized controlled trial in Kenya evaluated the impact of mobile telephone support on Maternal Health Service Care. A significant association was observed between the intervention category and the number of ANC visits (96.4% in the intervention group and 92.3% in the comparator group, P value: 0.002).31 Also, this study reported a significantly higher proportion of women on follow-up who received counseling on diet, place of delivery, malarial prophylaxis, iron and vitamin supplements, deworming, and drugs.31
In Ghana, a qualitative study was conducted to explore the role of mobile technology in the lives of pregnant mothers. The Mobile Midwife technology regularly sends reminders to pregnant women for ANC visits. A total of three FGDs were conducted, and 19 individuals were interviewed. It was found that women increasingly gained trust in the Mobile Midwife technology. Women expressed that the frequency of ANC visits increased after the introduction of mobile technology.33
In Ethiopia, a community-based randomized control trial (RCT) was conducted in three woredas of the Guraghe zone. Mobile phones equipped with frontline SMS-based, a locally developed application was distributed to all health extension workers to both intervention woredas who filled maternal, child, and stock-related forms. The system also sent a reminder for HEWs. The study confirmed the positive impact of SMS-based mobile phone intervention in most of the selected MCH service indicators, such as improvement in the percentage of the recommended number of ANC visits.35
In India, a quasi-experimental study with controls was conducted to assess the impact of the mHealth intervention on maternal health knowledge, antenatal care (ANC) attendance, and delivery in a health facility. Mobile for Mother (MFM) mobile application sends pregnancy-related information to pregnant women through text, pictures, and voice prompts. The results indicated that women in the intervention group had higher maternal health knowledge and were more likely to have 4+ ANC visits.
However, few studies23,48 reported that digital health interventions had no positive effect on client education and behavioral change communication.
A controlled clinical trial study was conducted in South Africa to increase antenatal health knowledge and awareness by sending text messages about clinic procedures at antenatal visits. A total of 102 women (intervention: text message) and 104 (control: standard of care) were recruited. Text messages with antenatal health information were sent to pregnant women. The results showed no statistically significant difference between the two groups (P > 0.05). However, evidence from self-reported behavior and the focus group discussion suggests that text messages have the potential to motivate change in health-seeking behavior.23
In Samoa, a Quasi-Experimental study was conducted to assess facilitators and barriers to implementing an SMS text messaging intervention for pregnant women in Samoa and to assess its impact on ANC attendance. A weekly base educational text message was sent to the intervention group. The study reported that text message has a negative effect on ANC attendance. In the intervention group attended 15% fewer ANC visits than the comparison group (P=0.004).48
Effect on Registries/Vital Event Tracking
Eleven studies reported digital applications’ role in registration or vital event tracking.24,25,30,39 In Nigeria, a pre-post study was conducted to assess whether CommCare mobile phone application had an effect on the quality of ANC services. The application helps community health workers to register clients and following-up clients on scheduled visits. The introduction of CommCare improved the quality score from 13.3 at baseline to 17.2 at the end line (P < 0.0001).24
In Kenya, an evaluation study was conducted to assess the impact of the mobile health system on antenatal and postnatal attendance. A total of 20 community health workers and 67 pregnant women or new mothers were interviewed to assess the adherence following the registration of 800 women into mobile health system ANC/PMTCT Adherence System (APAS). All CHWs stated that APAS help them track vital events efficiently, as compared to paper-based tracking systems.30
A cluster randomized controlled trial was conducted in Palestine at primary healthcare units. The intervention was an eRegistry with clinical decision support for antenatal care. A total of 133 clinics with 120 clusters were included and randomly assigned either to the control (paper-based documentation) or intervention (eRegistry with clinical decision support) groups. The study reported that the intervention improved guideline adherence for screening and management of anemia 2297 [44.3%] of 5182 vs (1535 [28.9%] of 5320 [AOR: 1.88 [95% CI 1.52–2.32]]), hypertension 7314 [96.6%] of 7569 vs (7555 [94.7%] of 7982 [AOR 1.62 [95% CI: 1.29–2.05]]), and gestational diabetes 2189 (50.7%) of 4321 vs 1726 (39.7%) of 4348 [AOR: 1.45 [95% CI 1.14–1.83]]) at eligible antenatal contacts.39
Effect on Data Collection and Reporting
Four studies24,28,32,40 demonstrated that digital interventions positively affect antenatal care service utilization and quality of care by facilitating data collection and reporting.
In Nigeria, a pre-post study was conducted to determine the effect of CommCare mobile phone application on the quality of ANC services. The CommCare application guides CHWs in collecting client data (medical information) in real-time helps CHWs to collect information during the examination (maternal and fetal danger signs, and fetal heart rate) and lab results (protein or glucose in the urine, malaria test, UTI test, Hbg levels). Through the initiation of CommCare, the quality score improved from 13.3 at baseline to 17.2 at the end line (P < 0.0001).24
In the Thai-Myanmar, a randomized control trial was conducted to evaluate an electronic mobile phone application to improve the quality of antenatal care. A web-based and mobile technology system module was developed to generate ANC visit schedule dates. The study showed that the mobile phone application had more complete records for Hepatitis B screening, physical examination, education and counseling, and birth preparedness plans. Overall, the intervention improved the quality of ANC coverage by increasing the completeness of records and the number of ANC visits, and highly acceptable for healthcare providers.28
A quasi-experimental study was conducted in Ghana to assess the impact of Technology for maternal and child health (T4MCH) on MCH services utilization and continuum of care. The implementation of T4MCH increased antenatal care attendance by 18 percentage points [95% CI: −17.0; 52.0] compared to the control.32
In India, a mixed-method design with a realist evaluation approach was conducted to assess changes in the coverage, quality of data reporting maternal and child health services, and time spent in the documentation before and after the introduction of the TeCHO+ app. The survey was conducted in 32 sub-centers across two districts of Gujarat State in India. A total of 29 nurses, 12 data entry operators, and 10 primary health center medical officers were purposefully selected from 32 PHCs and interviewed to understand the pathways leading to the program outcome. The coverage of full antenatal care (ANC; 75.6% vs 67.9%, p-value <0.0001), consumption of at least 180 iron-folic acid tablets (93% vs 77%, p-value <0.001), and early initiation of breastfeeding (42.7% vs 24.2%, p-value <0.001), improved. The overall concordance rate for routine maternal health indicators (a measure of data quality) improved from 69.1% to 80.5%.40
Effect on Provider-to-Provider Communication
Lund et al34 reported that mobile phone improved timely referrals between different health system levels and enabled health workers to consult patients with higher levels of care.34 A community-based randomized control trial study in Ethiopia demonstrated that the Frontline SMS-based applications facilitated emergency referrals from health posts to health centers and prepared HCs to receive patients.35
Effect on Electronic Decision Support (Information, Protocols, Algorithms, Checklists)
In Nigeria, a Pre/Post-Intervention study introduced a mobile case management and decision support application to assess the effect of the interventions on the quality of antenatal care services provided by the lower-level cadre. Client records included demographic data, medical history, screening information, and laboratory test results were assessed. The app contained decision support algorithms covering the core areas of ANC services, including screening for pre-eclampsia and management of obstetric danger signs and test results that were out of normal range; the app generates a recommendation for treatment, referral, and client follow-up. The intervention improved the overall quality score from 13.3 at baseline to 17.2 at the end line (p<0.0001).24
Venkateswara et al39 reported that eRegistry with a decision support system improved screening and management for anemia, gestational diabetes, and hypertension. The clinical decision for antenatal care in the eRegistry was greater for most process outcomes but failed to demonstrate its effect on adverse health outcomes.39
Effect on Provider Work Planning and Scheduling
Saha et al40 reported that TeCHO+ helped to automatically generate daily work plans that capacitate the Auxiliary Nurse Midwives (ANMs) to track beneficiaries, and alerts for high-risk cases help ANMs follow-up and encourage beneficiaries to take referral services. The study reported that TeCHO+ intervention had improved access to care and impacted coverage and data reporting quality of various maternal outcomes.
Discussion
With the exponential growth of digital health implementation, there is a growing need to examine interventions according to their specific approaches and targeted health outcomes addressed. This review shows that most of the studies took place in Africa and Asia, while some were conducted in South America and other parts of the globe.
Digital solutions are increasingly being utilized to increase the quality of prenatal care and collect pregnancy data. Except for three, all the studies included in this review showed some evidence that digital health interventions could play a role in improving antenatal care service utilization.
However, the design and outcomes of the studies varied, making it difficult to compare them directly. The studies demonstrated the role in various ways, such as increased service utilization, improved antenatal care attendance, reduced missed appointments, and increased knowledge and awareness of antenatal health services.
In the majority of the studies, the authors did not state the intervention pathways through which it would be delivered to target groups. In addition, several studies combined multiple digital health interventions,27,28,34,35,41,51 making it difficult to describe to what extent the specific intervention brought the desired outcome.
Based on our analysis, the most reported use of digital health interventions was for client education and behavior change communication,27–29,31–38,41–48,50,51 followed by Registries and vital event tracking.24–27,30,34,35,39,41,43,51 Other categories were digital health solutions as a data collection and reporting system aimed to ensure data recording and completeness.24,27,28,32,38,40 The other category was the electronic decision support system,24,27,39–41 which aimed to demonstrate how the decision support system could help screen and diagnose any health issues and ensure the quality of services. Also, a few studies were categorized into the provider-to-provider communication category34,35 to improve access to care providers’ consultation and facilitate communication during the referral of pregnant women in the case of an emergency.
The categorization of the studies into various digital health interventions demonstrates that empirical evidence exists on the role of digital health interventions on client education and behavior change communication, registries and vital events tracking data collection, and reporting of antenatal care service. However, little is known about provider-to-provider communication, provider work scheduling and planning, supply chain management, and electronic health records.
Many studies23,27–29,31,32,34,37,38,41–45,47,51 treated the topic of antenatal follow-up reminders in improving ANC attendance. The way the interventions were delivered was not uniform. Some sent SMS to the pregnant women unidirectional,23,29,31,32,34,36–38,48 and some sent SMS from the pregnant women to the health facilities bidirectional,47 and/or voice messaging.45 Also, some studies26,27,30,35 sent SMS directly to the healthcare providers to facilitate and coordinate ANC-related services.
In all studies,25,37,48 the rest addressed more than one antenatal care service content.
According to the World Health Organization’s recommendations, all pregnant women should be screened for a health condition, tested for a basic blood test, follow the recommended number of ANC visits, and start their first ANC before 16 weeks of gestation.6 Many studies assessed the role of digital health solutions on antenatal care follow-up. However, only one study34 reports the effect of the intervention on early initiation and adherence to the ANC schedule. Some studies tried to demonstrate the role of digital solutions on blood tests during ANC. Studies24,47 included a blood test for Hgb, syphilis, blood type, and HIV, and the other two studies39 and 45 for anemia (Hgb) and Blood group, respectively.
Health promotion, prevention, and treatment during pregnancy are core packages of antenatal care interventions. The majority of studies evaluated the role of digital solutions on one of the components. Tetanus vaccination,24,28,31,34,41,43–45,47,50 Iron folic acid,23,24,31,40,41,43–45,47,50 and delivery plan23,24,26,27,29,35,41,43–45 were the core components of ANC assessed followed by preventive treatment for malaria,24,31,34,36 child vaccination,24,26,29,35,40,41 breastfeeding,23,24,28,40 and PNC.23,26,27,45 However, only three studies demonstrated the role of digital interventions on danger signs of pregnancy.23,24,41
With a comprehensive search strategy, this review analyzed the role of digital health interventions in the effective coverage of ANC. Most studies demonstrated that digital health interventions used for client educational and behavioral change communication were positively associated with antenatal care service utilization. However, the interventions must be contextualized so that the delivery channel and the content are appropriate for the target audience. We identified three delivery channels through which digital health interventions are used for client education and behavioral change communication: direct messaging (unidirectional or bidirectional), voice counseling, and job aid/photograph applications. These three ways of delivery are prominently different from one another in several core implementation elements, which affect the intensity of client education and BCC delivery and are, therefore, likely to affect its effect on ANC service uptake. These include the frequency of communication, length, and complexity of content delivered. The messages should be tailored to the recipient’s trimester of pregnancy. Trials of direct messaging interventions with a primary focus on antenatal care have shown effectiveness in improving the uptake of ANC services.27–29,31–35,37,38,41–45,47,51
Though, much of the literature reported the role of digital solutions on several antenatal attendances, and few studies evaluated the effect of interventions on the quality of ANC. The number of antenatal care attendances alone could not be a guarantee for improved maternal health outcomes. We consider the review findings are promising; more rigorous studies are needed to determine the role of digital health interventions to enhance the effective coverage of antenatal care services. Also, most studies used digital health interventions for client education and behavior change communication for improved ANC; only one study assessed the effect of the intervention on pregnant women’s worries,42 and the study reported that digital targeted client communication has no effect on pregnant women’s worries.
Limitations
We conducted an extensive search. However, some eligible studies may have been missed due to the title screening being done by a single individual, as this might entail a risk of rejecting relevant reports. Also, some digital health programs may be unevaluated and unreported. In addition, not retrieved articles and studies published in languages other than English were not included.
Conclusion
This review identified that digital health solutions targeted at pregnant women can improve antenatal care services. There are emergent pieces of evidence indicating the effectiveness of digital health interventions on a range of maternal health outcomes, but the majority of the available literature focuses on the crude coverage of antenatal care. Few pieces of literature exist concerning the use of digital health interventions on the quality of antenatal care services. There is a need for more trial and evaluation studies that examine the role of digital health interventions to enhance the effective coverage of ANC.
Abbreviations
ANC, Antenatal care; ANMS, Auxiliary Nurse Midwives; CHW, Community Health Worker; EMR, Electronic Health Records; EHR, Electronic Health Records; LMICS, Low- and Middle-Income Countries; JBI, Joanna Briggs Institute; MCH, Maternal and Child Health; MeSH, Medical Subject Headings; MFM, mobile for Mother; PCC, Population; Concept; and Context; PNC, Postnatal care; RCT, Randomized Controlled trial; SMS, Short Message Service; SDGS, Sustainable Development Goals; T4MCH, Technology for maternal and child health; WHO, World Health Organization.
Data Sharing Statement
Data are available upon reasonable request from corresponding author.
Acknowledgments
We would like to thank Adane Nigussie and Dessie Abebaw for their willingness to select study and extract data.
Author Contributions
All authors made a significant contribution, in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Trends in Maternal Mortality: 1990–2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2015.
2. World Health Organization. Tracking Universal Health Coverage: 2021 Global Monitoring Report. World Health Organization; 2021.
3. Mehboob R, Gilani SA, Khalid S, Hassan A, Alwazzan A. Maternal Mortality Ratio in Low Income Developing Countries. Women’s Health: IntechOpen; 2021.
4. World Health Organization. International Bank for Reconstruction and Development. Tracking Universal Health Coverage: 2017 Global Monitoring Report. World Bank Group. World Health Organization and International Bank for Reconstruction and Development The World Bank; 2017.
5. World Health Organization. Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. World Health Organization; 2019.
6. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization; 2016.
7. Rooney C. Antenatal Care and Maternal Health: How Effective is It? A Review of the Evidence. World Health Organization; 1992.
8. Munjanja S. Antenatal Care. Opportunities for Africa’s Newborns: Practical Data, Policy and Programmatic Support for Newborn Care in Africa. Geneva, Switzerland: World Health Organization; 2006:55–62.
9. Bhutta ZA, Das JK, Bahl R, et al. Can available interventions end preventable deaths in mothers, newborn babies, and stillbirths, and at what cost? Lancet. 2014;384(9940):347–370. doi:10.1016/S0140-6736(14)60792-3
10. Villar J, Bergsjø P. Scientific basis for the content of routine antenatal care I. Philosophy, recent studies, and power to eliminate or alleviate adverse maternal outcomes. Acta Obstet Gynecol Scand. 1997;76(1):1–14. doi:10.3109/00016349709047778
11. Marchant T, Tilley-Gyado RD, Tessema T, et al. Adding content to contacts: measurement of high quality contacts for maternal and newborn health in Ethiopia, north east Nigeria, and Uttar Pradesh, India. PLoS One. 2015;10(5):e0126840. doi:10.1371/journal.pone.0126840
12. Carvajal–Aguirre L, Amouzou A, Mehra V, Ziqi M, Zaka N, Newby H. Gap between contact and content in maternal and newborn care: an analysis of data from 20 countries in sub–Saharan Africa. J Glob Health. 2017;7(2). doi:10.7189/jogh.07.020501
13. Hodgins S, D’Agostino A. The quality–coverage gap in antenatal care: toward better measurement of effective coverage. Global Health. 2014;2(2):173–181. doi:10.9745/GHSP-D-13-00176
14. World Health Organization. Global Reference List of 100 Core Health Indicators. World Health Organization; 2015.
15. Watkins K. The State of the World’s Children 2016: A Fair Chance for Every Child. ERIC; 2016.
16. Kyei NN, Chansa C, Gabrysch S. Quality of antenatal care in Zambia: a national assessment. BMC Pregnancy Childbirth. 2012;12(1):1–11. doi:10.1186/1471-2393-12-151
17. Nguhiu PK, Barasa EW, Chuma J. Determining the effective coverage of maternal and child health services in Kenya, using demographic and health survey data sets: tracking progress towards universal health coverage. Trop Med Inter Health. 2017;22(4):442–453. doi:10.1111/tmi.12841
18. Victora CG, Fenn B, Bryce J, Kirkwood BR. Co-coverage of preventive interventions and implications for child-survival strategies: evidence from national surveys. Lancet. 2005;366(9495):1460–1466. doi:10.1016/S0140-6736(05)67599-X
19. World Health Organization. WHO Guideline: Recommendations on Digital Interventions for Health System Strengthening. World Health Organization; 2019.
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
21. Peters MD, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
22. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
23. Pactr. Antenatal health promotion via short message service at a Midwife Obstetrics Unit in South Africa: a mixed methods study; 2014. Available from: https://trialsearchwhoint/Trial2aspx?TrialID=PACTR201406000841188.
24. McNabb M, Chukwu E, Ojo O, et al. Assessment of the quality of antenatal care services provided by health workers using a mobile phone decision support application in northern Nigeria: a pre/post-intervention study. PLoS One. 2015;10(5):e0123940. doi:10.1371/journal.pone.0123940
25. Ngabo F, Nguimfack J, Nwaigwe F, et al. Designing and implementing an innovative SMS-based alert system (RapidSMS-MCH) to monitor pregnancy and reduce maternal and child deaths in Rwanda. Pan Afr Med J. 2012;13:1.
26. Hategeka C, Ruton H, Law MR. Effect of a community health worker mHealth monitoring system on uptake of maternal and newborn health services in Rwanda. Glob Health Res Policy. 2019;4:8. doi:10.1186/s41256-019-0098-y
27. Shiferaw S, Spigt M, Tekie M, Abdullah M, Fantahun M, Dinant G-J. The effects of a locally developed mHealth intervention on delivery and postnatal care utilization; a prospective controlled evaluation among health centres in Ethiopia. PLoS One. 2016;11(7):e0158600. doi:10.1371/journal.pone.0158600
28. Pactr. Efficacy of electronic mobile phone application compared with mother and child health booklet in improving quality of antenatal care from first visit through third trimester at Kenyatta National Hospital, a randomized controlled trial; 2019. Available from: https://trialsearchwhoint/Trial2aspx?TrialID=PACTR202001700173081.
29. Coleman J, Black V, Thorson AE, Eriksen J. Evaluating the effect of maternal mHealth text messages on uptake of maternal and child health care services in South Africa: a multicentre cohort intervention study. Reprod Health. 2020;17(1):160. doi:10.1186/s12978-020-01017-3
30. Mushamiri I, Luo C, Iiams-Hauser C, Ben Amor Y. Evaluation of the impact of a mobile health system on adherence to antenatal and postnatal care and prevention of mother-to-child transmission of HIV programs in Kenya. BMC Public Health. 2015;15(1):1–16. doi:10.1186/s12889-015-1358-5
31. Fedha T. Impact of mobile telephone on maternal health service care: a case of Njoro division. Open J Prev Med. 2014;2014:1.
32. Nuhu AGK, Dwomoh D, Amuasi SA, et al. Impact of technology for maternal and child health intervention on health services utilization and continuum of care in Northern Ghana: a quasi-experimental study; 2022.
33. Entsieh AA, Emmelin M, Pettersson KO. Learning the ABCs of pregnancy and newborn care through mobile technology. Global Health Action. 2015;8(1):29340. doi:10.3402/gha.v8.29340
34. Lund S, Nielsen BB, Hemed M, et al. Mobile phones improve antenatal care attendance in Zanzibar: a cluster randomized controlled trial. BMC Pregnancy Childbirth. 2014;14(1):1–10. doi:10.1186/1471-2393-14-29
35. Atnafu A, Otto K, Herbst CH. The role of mHealth intervention on maternal and child health service delivery: findings from a randomized controlled field trial in rural Ethiopia. mHealth. 2017;3:39. doi:10.21037/mhealth.2017.08.04
36. Flueckiger RM, Thierno DM, Colaço R, et al. Using short message service alerts to increase antenatal care and malaria prevention: findings from implementation research pilot in Guinea. Am J Trop Med Hyg. 2019;101(4):806–808. doi:10.4269/ajtmh.19-0202
37. Makunyi EG. Utilization of Mobile Phone Short Message Service to Enhance Uptake of Focused Antenatal Care in Tharaka Nithi County, Kenya; 2018.
38. Kaewkungwal J, Singhasivanon P, Khamsiriwatchara A, Sawang S, Meankaew P, Wechsart A. Application of smart phone in” Better Border Healthcare Program”: a module for mother and child care. BMC Med Inf Decis Making. 2010;10(1):1–12. doi:10.1186/1472-6947-10-69
39. Venkateswaran M, Ghanem B, Abbas E, et al. A digital health registry with clinical decision support for improving quality of antenatal care in Palestine (eRegQual): a pragmatic, cluster-randomised, controlled, superiority trial. Lancet Digital Health. 2022;4(2):e126–e36. doi:10.1016/S2589-7500(21)00269-7
40. Saha S, Quazi ZS. Does digitally enabling frontline health workers improve coverage and quality of maternal and child health services? Findings from a mixed methods evaluation of TECHO+ in Gujarat. Front Public Health. 2022;10:856561. doi:10.3389/fpubh.2022.856561
41. Ilozumba O, Van Belle S, Dieleman M, Liem L, Choudhury M, Broerse JEW. The effect of a community health worker utilized mobile health application on maternal health knowledge and behavior: a quasi-experimental study. Front Public Health. 2018;6:133. doi:10.3389/fpubh.2018.00133
42. Bogale B, Mørkrid K, Abbas E, et al. The effect of a digital targeted client communication intervention on pregnant women’s worries and satisfaction with antenatal care in Palestine-a cluster randomized controlled trial. PLoS One. 2021;16(4):e0249713. doi:10.1371/journal.pone.0249713
43. Choudhury A, Asan O, Choudhury MM. Mobile health technology to improve maternal health awareness in tribal populations: mobile for mothers. J Am Med Inf Assoc. 2021;28(11):2467–2474. doi:10.1093/jamia/ocab172
44. Indira E, Thomas PE, Sri Hari M. Mobile text messages-a silent revolution for a sound antenatal care. Indian J Public Health Res Dev. 2017;8(4):563–569. doi:10.5958/0976-5506.2017.00399.0
45. Chowdhury ME, Shiblee SI, Jones HE. Does mHealth voice messaging work for improving knowledge and practice of maternal and newborn healthcare? BMC Med Inform Decis Mak. 2019;19(1):179. doi:10.1186/s12911-019-0903-z
46. Souza F, Santos W, Santos R, et al. Effectiveness of mobile applications in pregnant women’s adherence to prenatal consultations: randomized clinical trial. Rev Brasil De Enferm. 2021;74(74Suppl 5):e20190599. doi:10.1590/0034-7167-2019-0599
47. Oliveira-Ciabati L, Vieira CS, Franzon ACA, et al. PRENACEL - A mHealth messaging system to complement antenatal care: a cluster randomized trial. Reproductive Health. 2017;14. doi:10.1186/s12978-017-0407-1
48. Watterson JL, Castaneda D, Catalani C. Promoting antenatal care attendance through a text messaging intervention in Samoa: quasi-experimental study. JMIR mHealth and uHealth. 2020;8(6):e15890. doi:10.2196/15890
49. Labrique AB, Vasudevan L, Kochi E, Fabricant R, Mehl G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Global Health. 2013;1(2):160–171. doi:10.9745/GHSP-D-13-00031
50. Prinja S, Nimesh R, Gupta A, Bahuguna P, Gupta M, Thakur JS. Impact of m‐health application used by community health volunteers on improving utilisation of maternal, newborn and child health care services in a rural area of Uttar Pradesh, India. Trop Med Inter Health. 2017;22(7):895–907. doi:10.1111/tmi.12895
51. Pactr. Utilization of short message service to enhance uptake of focused antenatal care among women in Tharaka Nithi County, Kenya; 2017. Available from: https://trialsearchwhoint/Trial2aspx?TrialID=PACTR201801002231314.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.