Back to Journals » Cancer Management and Research » Volume 15
Management Strategies for Adults with Locally Advanced, Unresectable or Metastatic Malignant Perivascular Epithelioid Cell Tumor (PEComa): Challenges and Solutions
Authors Czarnecka AM, Skoczylas J, Bartnik E, Świtaj T, Rutkowski P ![]()
Received 30 October 2022
Accepted for publication 28 June 2023
Published 7 July 2023 Volume 2023:15 Pages 615—623
DOI https://doi.org/10.2147/CMAR.S351284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Antonella D'Anneo
Anna M Czarnecka,1 Jacek Skoczylas,1 Ewa Bartnik,2,3 Tomasz Świtaj,1 Piotr Rutkowski1
1Department of Soft Tissue/Bone Sarcoma and Melanoma, Maria Sklodowska-Curie National Research Institute of Oncology, Warsaw, Poland; 2Institute of Genetics and Biotechnology, Faculty of Biology, University of Warsaw, Warsaw, Poland; 3Institute of Biochemistry and Biophysics, Polish Academy of Sciences, Warsaw, Poland
Correspondence: Anna M Czarnecka, Department of Soft Tissue/Bone Sarcoma and Melanoma, Maria Sklodowska-Curie National Research Institute of Oncology, W.K. Roentgena 5 street, Warsaw, 02-781, Poland, Tel + 48 22 546 2194, Email [email protected]
Abstract: PEComa (PEC tumor; perivascular epithelioid cell tumors) is a rare group of tumors of mesenchymal origin composed of perivascular epithelioid cells (PEC) with features of melanotic and smooth muscle differentiation. In this article, we would like to present the current treatment options for this group of tumors. PEComas are classified as tumors of uncertain malignant potential because recurrences occur after radical treatment. The primary treatment is surgical resection with negative margins. Due to the different locations of the tumors, often the cooperation of multispecialty surgeons is required during the operations. In locally advanced cases, cytoreduction and HIPEC may be effective but still are an experimental treatment. For nonresectable PEComa chemotherapy, mTOR inhibitors and VEGFR inhibitors are used.
Keywords: PEComa, sarcoma, surgery, chemotherapy, oncology
Introduction
Perivascular epithelioid cell tumors (PEComa; PEC tumors) are a group of rare mesenchymal origin tumors derived from perivascular epithelioid cells (PEC) expressing features of melanotic and smooth muscle differentiation.1 PEComas are classified as tumors of uncertain malignant potential, because recurrences after radical treatment may develop after many years (>10). The PEComa family of tumors in addition to the “malignant” PEComa NOS (not otherwise specified) also covers less aggressive angiomyolipomas (AML), clear cell sugar tumor (CCST), pulmonary and primary extrapulmonary sugar tumor (PEST), as well as lymphangioleiomyomatosis (LAM), clear cell myomelanocytic tumor (CCMM), primary cutaneous PEComa and cutaneous clear cell myomelanocytic tumor (CCCMT).2 Malignant PEComas are estimated to be diagnosed in 0.12 to 0.24 per million people around the world. More common angiomyolipomas – with an incidence of 30 per 100,000 individuals worldwide – are most commonly diagnosed as small asymptomatic renal tumors with a high fat tissue content. In a patient without any predisposing factors, it is referred to as sporadic AML.3 At the same time, AML development may also result from a genetic syndrome caused by germline-inactivating mutations in the TSC1 and TSC2 genes, the tuberous sclerosis complex (TSC, Bourneville-Pringle disease). This syndrome is characterized by the development of PECOmas, but also other solid tumors such as hamartomas, as well as diseases of the central nervous system including epilepsy, autism, and intellectual disability of various degrees.4 TSC2-mutated tumors have an overactivated PIK3-Akt-mTOR pathway.5 The second characterized molecular abnormality in the pathogenesis of PEComa is TFE3 translocations that by transcriptional up-regulation activate MET signaling.6,7 In AML related to TSC, numerous usually large tumors are diagnosed with a tendency to bleeding and progressive kidney insufficiency as a result.8 In approximately 8% of cases of AML, more commonly those associated with tuberous sclerosis, the dominance of epithelial cells is observed in the tumor and they can show characteristics of nuclear atypia resulting in the development of epithelioid angiomyolipoma (EAML).9 A small percentage of EAML cases have a tendency to malignant transformation.10
Diagnosis
About 1/5 of PEComas are diagnosed during diagnostic imaging for a different reason.11 In the remaining cases, the most common symptoms in advanced tumors are the result of the tumor pressing on adjacent organs. Since malignant behavior of PEComas is uncertain, Folpe et al12 proposed the division of PEComas into three categories of risk: benign tumors, tumors with uncertain malignancy potential, and malignant tumors (Table 1). A biopsy is always required to make a definitive diagnosis and define the potential of malignancy. The most commonly used is core needle biopsy with ultrasound or computed tomography guidance. As a last resort, an open biopsy may be performed. A core-needle biopsy allows for a diagnosis with the same effectiveness as an open biopsy with a lower risk of complications.13 In general, a size of more than 5 cm and a mitotic rate of 1/HPF are significantly associated with malignant behavior and risk of recurrence (Table 1).12 Bleeker risk category is a risk factor significantly associated with OS, as well as presence of synchronous metastases at the time of diagnosis.12,14
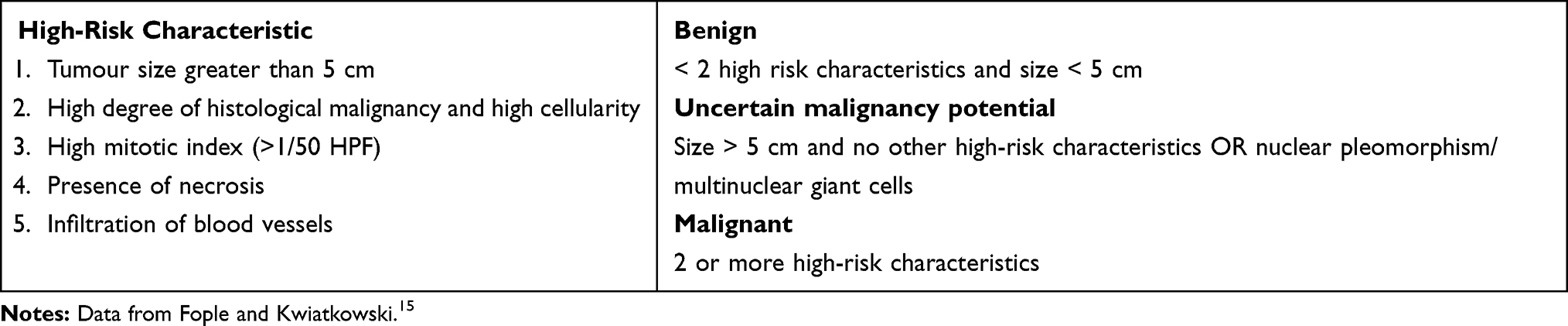 |
Table 1 Classification of PEComa |
Molecular Characteristics
In the most recent PEComa analysis, the most common mutations were found in the TP53 gene (47% of cases), ATRX (32%), and MSH3 (17%). Mutations in the TSC1 and TSC2 genes were found in 11% and 29% of patients, respectively. Presence of TSC1 vs TSC2 mutation was reported not to impact PFS or OS in differently while on mTOR on chemotherapy treatment.16 Although TSC1/2 and TFE3 were considered to be mutually exclusive,17 it has recently been reported that TSC1/2-mTOR pathway and TFE3 overexpression may be detected concordantly.18 In France, a retrospectively study (NCT05617105) is ongoing to define the percentage of tumors with FISH (Fluorescence In Situ Hybridization) identified TFE3 rearrangements in 100 PEComa patients in University Hospital in Strasbourg. Tuberous sclerosis complex (TSC) related PEComa is also studied in NCT05676099 biosample repository and natural history database study.
Interestingly, TP53 mutations occurred less frequently (25 vs 60%, p = 0.055) in tumors mutated with TSC1/2 compared to tumors with wild type TSC1. At the same time, mutations in MSH3 (in 25% of cases, n = 1/4) and ERCC2 (14%, n = 2/14) were only reported in TSC1/2-mutated tumors.5 In general, PEComas are also characterized by a specific transcriptomic signature with the overexpressed DAPL1, MLANA, SULT1C2, GPR143, and CHI3L1 genes and with epigenetic signatures of lysosomal and melanocytic proteins as biomarkers.19 Furthermore, the PEComa tumour microenvironment is characterized by a significant influx of NK and fibroblasts, and a decreased number of CD8+ T cells and B cells.5 PEComa tumors are also being characterized in NCT03967834 MIRAS Project From SARRA (SARcome RAre) Project of the French Sarcoma Group (MIRAS) that is designed for multimodal immune characterization of rare soft tissue sarcomas.
Selection Criteria for Surgery
Due to the rarity of the disease, there are no clear established and described criteria for the operability of PEComa. However, the process of qualifying for surgery takes into account that the most common locations for the development of PEComa are the uterus, skin, liver, and colon.12 Moreover, large malignant PEComas are diagnosed especially in the extraperitoneal space.20 The surgery qualification should be multidisciplinary with surgeons experienced in liver surgery, vascular surgery, and retroperitoneal tumors, also due to the risk of metastases to the lungs of 90%.21 In particular, each patient should undergo staging before qualifying for surgery.
Radical Treatment of Primary Tumor
Radical resection is the basis for the treatment of PEComa as these tumors are characterized by resistance to standard chemotherapy and radiotherapy.12 As we have shown previously, surgery in the reference sarcoma center is associated with longer disease control (Figure 1).22
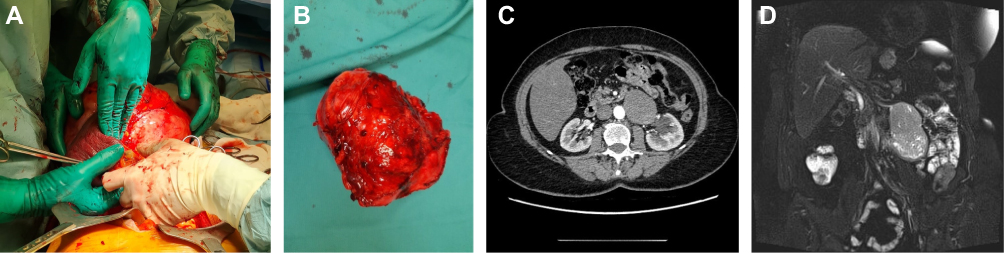 |
Figure 1 PEComa tumor radiological imaging and resection. (a) Intraoperative picture of PEComa resection, (b) PEComa after resection, (c) CT scan of PEComa, (d) MRI scan of PECma. |
Due to the rarity of PEComa, there are few studies in the available literature on the surgical technique for resection of these tumors. Most of the available sources describe a single case or a series of cases. It appears that optimal management does not differ from surgery of other sarcomas and the most important factor is en bloc radical resection (Figure 1).23 As reported in the literature, multiple organ resections11 or lymphadenectomy are rarely necessary due to the rareness of metastases to the lymph nodes in these sarcomas.24 However, in our analysis, we have shown that it is very important to refer patients to specialized sarcoma surgery centers,22 as it may lead to better local control and final results of therapy. Furthermore, the multidisciplinary approach allows for the improvement of treatment outcomes. Unfortunately, there are no clear criteria for “operability” and therefore each patient should be individually evaluated by the surgical team. The most important is the possibility of macroscopically radical (R0) resection and, in the presence of metastases, their resectability.25 There are no data on the results of cytoreduction surgery; however, by analogy with other sarcomas, it can be anticipated that such surgeries do not improve survival and expose patients to extensive and high-risk surgery. Cytoreduction procedure in conjunction with intraperitoneal chemotherapy is still experimental and feasible in clinical trials.26
Laparoscopic and Robotic Surgery
As in any surgical procedure, attempts are made to treat PEComa with a laparoscopic and robotic approach. Due to the rarity of this disease, mostly case reports are published.27 In the analysis of these articles, it is worth noting that patients may benefit from minimally invasive access, resulting in less postoperative pain and shorter hospitalization. However, there are no data on oncological results. Nevertheless, it seems that as long as the principles of oncological resection R0 are met, such operations should be proposed, especially in the case of smaller tumors.
Metastasectomy
In the described cases, metastasectomy of metastatic foci (lung, kidney, liver) also allowed long-term control of the disease.14,23,28 Due to the importance of surgical treatment for long-term survival, patients with initially advanced diseases have unfavorable prognoses. However, due to resistance to chemotherapy and radiation therapy, surgery should always be considered in the case of countable and resectable metastases as in other sarcomas. Patients with synchronous metastases should be evaluated for the possibility of resection and control of the primary tumor followed by resection of distant metastases. Data are not available on the sequence strategy for primary tumor excision and metastasis.29 Bourgmayer et al14 in their article mention that patients may benefit from neoadjuvant therapy prior to metastatic resection; however, these data are only available for a small number of patients. Therefore, the decision should be individualized for each patient during a multidisciplinary meeting.
Neoadjuvant and Adjuvant Treatment
Until now, the efficacy of adjuvant or neoadjuvant chemotherapy has not been demonstrated in PEComa. The use of neoadjuvant or adjuvant therapy is currently not recommended outside of clinical trials or a case-specific MDT-based treatment plan in reference centers.30 Perioperative radiotherapy is not routinely recommended in PEComa treatment.14 Response to neoadjuvant stereotactic radiation therapy (SBRT; 8 fractions of 7.5Gy) has been reported in a case of unresectable liver PEComa. A decrease in tumor volume allowed radical resection, and the patient remained disease-free for at least 21 months in this case.31 In another case, chemotherapy with ifosfamide, vincristine and dactinomycin has been described to considerably decrease PEComa vascularization – but not tumor size – and has been suggested to promote less blood loss during subsequent resection.32 In another report, neoadjuvant chemotherapy with epirubicin, cisplatin, and ifosfamide resulted in a decrease in tumor volume and enabled pelvic PEComa resection.33 Finally, a case of advanced large intestine PEComa with liver metastases treated with adjuvant sirolimus after radical resection was reported, but local recurrence and new liver metastases to the liver were described.34
Treatment of Advanced and Metastatic Diseases
Chemotherapy
Chemotherapy induces a low number of objective responses in PEComa. The most recent meta-analysis confirms the low efficacy of two chemo-regimens that are most commonly used. The first chemo-regimen - anthracycline-based therapy typically used for soft tissue sarcomas (STS) and the second - gemcitabine-based therapy do not induce long-term responses. For both regimens, the median PFS is 3 months with a numerically higher ORR of 20% for gemcitabine-based (95% CI: 4.3; 48.1) and ORR of 13% for anthracycline-based (95% CI: 2.8; 33.6).14 In PEComas adriamycin in monotherapy, high-dose ifosfamide, Gemcitabine with docetaxel and dacarbazine have been used in the past.30 In a retrospective study of 53 patients, Gemcitabine and anthracycline-based therapy induced median PFS of 3.4 and 3.2 months, respectively.35 In another series of 49 patients treated at Istituto Nazionale Tumori in Milan and the Italian Rare Cancer Network, gemcitabine-based combinations were the most effective and resulted in 25% objective responses, with almost 3 months of duration.36 No other large PEComa studies are available at this point in time. In our center, 27 patients were treated radically for PEComa between 1999 and 2019 and 15 were treated with sirolimus as described below. In reports from other groups, treatment with doxorubicin and ifosfamide resulted in a 9-month stabilization of the disease obtained in a patient with PEComa of the large intestine with metastases to the liver and a response in the form of a decrease in the mass of an upper extremity PEComa by 80% after 6 cycles (partial response PR). Objective responses were also reported for dacarbazine treatment and complete responses for vincristine monotherapy (Table 2).
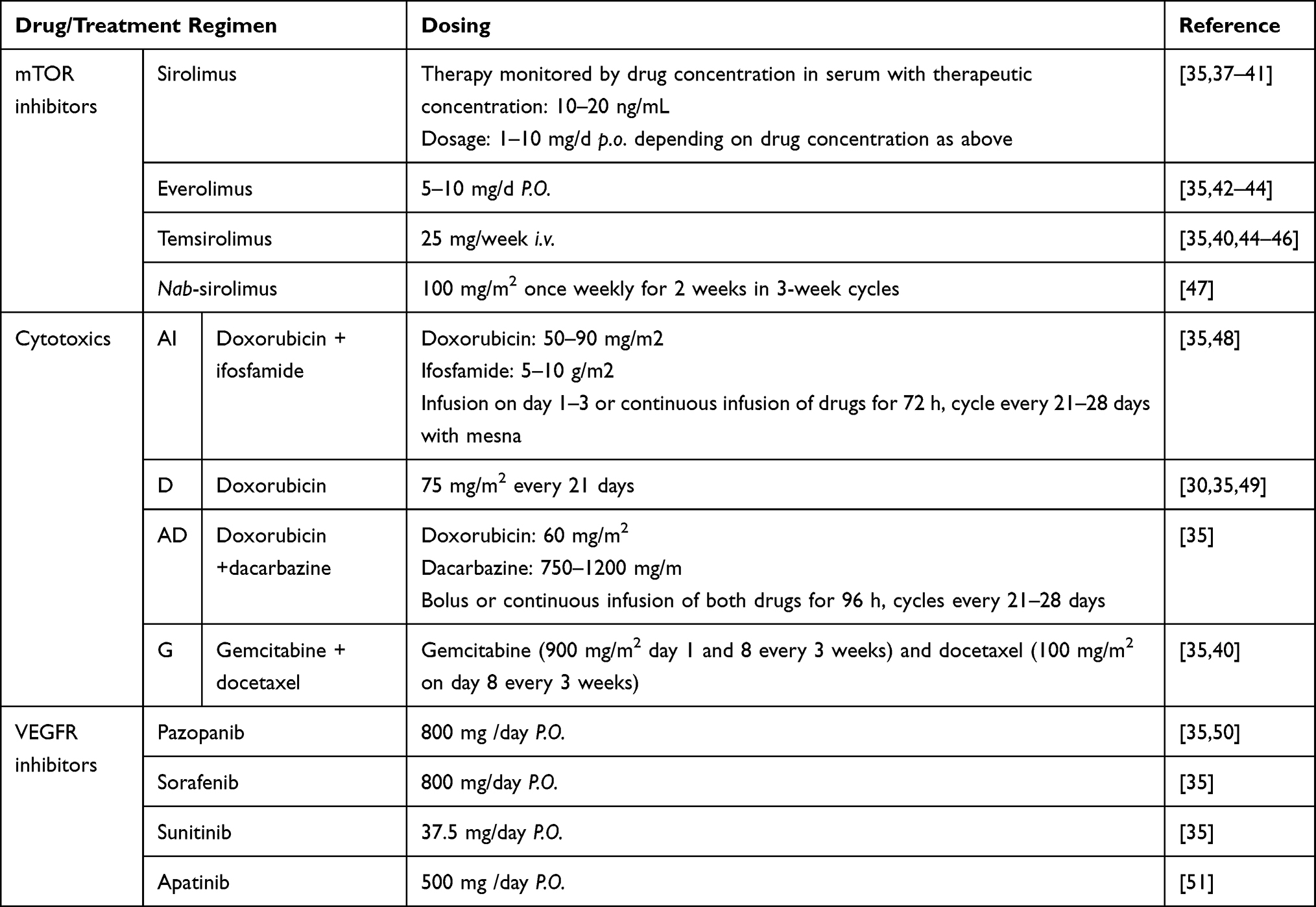 |
Table 2 Drugs and Therapy Regimens Used in PEComa |
mTOR Inhibitors
Due to genetic background and an increase in the activity of the mTOR signaling pathway in PEComa, long-term responses to treatment with mTOR inhibitors are observed in these patients (Table 2).52 In a retrospective study, the benefit of using mTOR inhibitors in patients with locally advanced or disseminated PEComa with ORR: 41% and PFS: 9 months; compared to classical chemotherapy based on gemcitabine or anthracyclines with ORR: 20% and 13% along with PFS: 3.4 and 3.2 months, respectively.35 This was confirmed by us in a 10-year observational study. In our center, fifteen PEComa patients were treated systematically. The median PFS was 4.9 months for first-line chemotherapy, while at the time of analysis it was not reached (95% CI 42.0-NA) for sirolimus. Only one OR was achieved with chemotherapy, but it was 73% (11/15 cases) for sirolimus treatment.22 The majority of other data on the use of mTOR inhibitors in patients with PECOma are case reports and case series. The first interesting report came from Italiano et al who described a case of a response to temsirolimus after resection of uterine PEComa with a single metastasis to the lung. A 35% decrease in tumor size was observed with subsequent lobectomy. The patient remained disease-free for 9 months after surgery, continuing treatment with temsirolimus.45 A 20-month stabilization of the disease (SD) was observed in a patient with a disseminated form of renal PEComa treated with sirolimus.37 Therapy was complicated by strong adverse effects in the first month of treatment, associated with a drug level in the blood of 156.8 ng/mL, which disappeared during 5 weeks after dose adjustment. A case of pancreatic PEComa has also been described, in which no resection was performed and sirolimus therapy was introduced that produced a partial response that was maintained for 42 months.38 Sirolimus is also effective in the treatment of other PEComa subtypes, including lymphangioleiomyomatosis (LAM) and lymphangioleiomyoma or extrapulmonary LAM (E-LAM).22
The retrospective study of Royal Marsden hospital of mTOR inhibitors in the treatment of ten cases of advanced metastatic PEComa (8 women, 2 men, median age 47.5 years) confirmed the efficacy of sirolimus therapy in PEComa. Nine patients received sirolimus at a median dose of 4 mg/d p, and one patient received temsirolimus at a dose of 25mg/week intravenously. In this case series, PR was observed in 50%, SD in 10%, and PD in 10%. In the 3 remaining patients, rapid progression occurred in the first days of treatment. Toxicity analysis revealed that among 9 patients who received sirolimus, the drug dose was reduced in 5 cases and treatment was intermittently interrupted due to adverse effects. At the time of analysis in 7 patients, the treatment was stopped, in 6 among them due to disease progression. The overall survival rate of 1 year was 78.8%, while the median OS was 2.4 years, with a median observation time of 1.9 years.41 We have also confirmed this efficacy of the mTOR inhibitor – sirolimus in a long-term study. After a median follow-up of 55.7 (range: 3.2–220) months, the 5 year OS was 65% in our patients.22
Everolimus has also been reported to be effective in patients with PEComa. In a series of five patients with PEComa metastases in the digestive tract, receiving sirolimus or everolimus, a clinical response was obtained in four cases (follow-up between 1 and 47 months), with progression and death 23 months after diagnosis in one of the patients.53 A 36-month stabilization of the disease has also been described in a patient with kidney PEComa with metastases to the lungs in response to everolimus treatment.54 It should be remembered that the efficacy of everolimus treatment was confirmed in PEComa subtype, TSC-related AML, in a randomized, double-blind, placebo-controlled trial with more than 50% of patients experiencing at least a 50% reduction in tumor volume in the first 6 months of treatment.55 In clinical practice, everolimus should also be considered as an active treatment option in patients with tuberous sclerosis, who do not qualify for surgical treatment. In these cases, initial dose 10 mg per day would be a recommended approach. Everolimus treatment may result in complete response, even as early as 3 months after therapy initiation.56 The EAML subtype, which has a high potential for a malignant course, can also be effectively treated with everolimus.57 It was recently reported to be effective in malignant renal epithelioid angiomyolipoma in routine clinical practice when prescribed at the dose of 10mg once daily.58 Everolimus was also effective in other treatments of the PEComa subtype – in E-LAM22 and advanced LAM in general.59 The presence of mutations in the TSC1/TSC2 genes and the overexpression of the ribosomal protein pS6-S235/236 are indicated as markers of the expected response to sirolimus, temsirolimus or everolimus.30
Nab-sirolimus, which is sirolimus albumin-bound nanoparticle, has recently been approved for PEComa treatment. It was registered by the FDAFDA on the basis of the results of the AMPECT trial. In this trial, patients with malignant PEComa received nab-sirolimus (100 mg/m2 IV days 1 and 8 of every 21-day cycle) as first-line treatment until progression, unacceptable toxicity, or withdrawal of consent. The primary endpoint of the nab-sirolimus study was the objective response rate (ORR). Secondary endpoints included the duration of response (DOR) and disease control rate (DCR), = complete response (CR) + partial response (PR) + stable disease (SD) at 12 weeks. As recently shown, ORR was 39% (12/31 patients), while DCR was 71% and was higher in patients with TSC1 or TSC2 inactivating alterations (ORR = 64%). In detail, 1 patient achieved complete response (CR) and 11 partial responses (PR) were reported. Furthermore, 52% (16/31) of the patients had stable disease (SD), with 10 cases of SD lasting more than 12 weeks. At the same time, the median DOR was not reached after 3 years of follow-up.60 In the majority of patients, the objective response was reached at 6 weeks, with a median response time of 1.4 months. At six months, the PFS was 71% and 8/12 (67%) of the respondents were treated for more than 1 year and 5/12 (42%) for more than 2 years. The median PFS was 10.6 months and the median OS was 40.8 months. Progressive disease as the best response was observed only in 10% (3/31) of patients.61 The FDA approved nab-sirolimus for intravenous use in the treatment of patients with locally advanced unresectable or metastatic malignant PEComas in July 2021. An open label phase Ib/II multi-center study (NCT05625919) of safety and efficacy of sirolimus for injection (albumin-bound) in patients with advanced malignant PEComa is ongoing in Beijing Jishuitan Hospital.
Few interesting cases of effective targeted therapy in PECOma have been published. A case of 1-year SD in response to pazopanib combined with nivolumab for advanced lower extremity PEComa with metastases to the bones and lungs has been recently published.50 The potential efficacy of angiogenesis inhibitors – pazopanib, sorafenib, sunitinib – in advanced PEComa patients has also been suggested in patients with advanced PEComa. Unfortunately, a low number of objective responses (8.3%) was seen (8.3%) with PFS of 5.4 months.35 Few cases of successful apatinib 500 mg of daily treatment PEComa treatment have been published.51 Apatinib treatment in a patient with TFE3 mutation resulted with 7-month PFS.51 Also, case of combined therapy with apatinib (250 mg/d) and a camrelizumab - anti-programmed cell death protein 1 (PD-1) antibody (200 mg/2 weeks) was also described.62 Imatinib treatment was reported to be ineffective in a PECOma case32 On the contrary, pembrolizumab was reported to cause CR in a patient with PEComa expressing programmed cell death ligand 1 (PD-L1).63 At the same time, nivolumab was also reported to be effective in an EAML case with high expression of PD-L1 and T cell infiltration in the tumor (Table 2).64 PEComa patients were also enrolled in NCT02834013 study with nivolumab and ipilimumab. This immunotherapy combination was also used in NCT04741438 (RAR-Immune) and Alliance A091401 trials that also enrolled PEComa patients, but no results are available.65 The role of radiotherapy in PEComa is not clear. It is not routinely recommended, except symptoms palliation in metastatic disease.
Summary
For diagnostic accuracy, PEComa immunohistochemical evaluation should be supplemented with molecular studies including fluorescence in situ hybridization (FISH) and next-generation sequencing (NGS) with a sarcoma panel. Primary treatment for PEComa is surgical resection with negative margins. Such a procedure is the optimal procedure due to the different location of tumors; often the cooperation of multispecialty surgeons is required during the qualification process. Surgery at the reference sarcoma center is associated with a longer disease control.22 In locally advanced cases, cytoreduction and HIPEC may be effective but still are experimental treatments.
For nonresectable PEComa chemotherapy, mTOR inhibitors and VEGFR inhibitors (ie, pazopanib, apatinib) may be used.51 Also, case of combined therapy with VEGFR inhibitor in combination with anti-PD-1 was also described.62 Most recently, nab-sirolimus was approved for PEComa treatment and seems to be the most active treatment option now. There are no specific PEComa treatment guidelines due to the rarity of this disease, so the second-line treatment choice should be based on MDT discussion. To predict the potential response to mTOR inhibitors, the pathologist should assess the level of expression of the phosphorylated S6 ribosomal protein, reflecting the activation of the mTOR pathway, during the diagnosis of PEComa. It predicts early response. Negative risk factors significantly associated with shorter OS are the presence of metastases at initial diagnosis and the grouped Bleeker risk category.
Disclosure
Prof. Dr. Piotr Rutkowski reports personal fees from BMS, MSD, Novartis, Merck, Pierre Fabre, Sanofi, Philogen, and Astra Zeneca, outside the submitted work. The authors report that they have no other conflicts of interest in this work.
References
1. Klimczak A, Pękul M, Wiater K, Rutkowski P. PEComa – grupa rzadkich nowotworów pochodzenia mezenchymalnego. Nowotwory J Oncol. 2011;61(1):52.
2. Sobiborowicz A, Czarnecka AM, Szumera-Ciećkiewicz A, Rutkowski P, Świtaj T. Diagnosis and treatment of angiomyolipoma (AML) tumours. Oncol Clin Pract. 2020;16(3):116–132. doi:10.5603/OCP.2020.0008
3. Fittschen A, Wendlik I, Oeztuerk S, et al. Prevalence of sporadic renal angiomyolipoma: a retrospective analysis of 61,389 in- and out-patients. Abdom Imaging. 2014;39(5):1009–1013. doi:10.1007/s00261-014-0129-6
4. Słowińska M, Jóźwiak S, Peron A, et al. Early diagnosis of tuberous sclerosis complex: a race against time. How to make the diagnosis before seizures. Orphanet J Rare Dis. 2018;13(1):25. doi:10.1186/s13023-018-0764-z
5. Seeber A, Holzer L, Elliott A, et al. Deciphering the molecular landscape and the tumor microenvironment of perivascular epithelioid cell neoplasma (PEComa). J Clin Oncol. 2021;39(15_suppl):11539. doi:10.1200/JCO.2021.39.15_suppl.11539
6. Tsuda M, Davis IJ, Argani P, et al. TFE3 fusions activate MET signaling by transcriptional up-regulation, defining another class of tumors as candidates for therapeutic MET inhibition. Cancer Res. 2007;67(3):919–929. doi:10.1158/0008-5472.CAN-06-2855
7. Szumera-Cieækiewicz A, Kuczkiewicz-Siemion O, Seliga K, et al. Pigmented/melanocytic malignant perivascular epithelioid cell tumor with TFE3-SFPQ(PSF) rearrangement – a challenging diagnosis of PEComa family of tumors. Pol J Pathol. 2019;70(4):317–322. doi:10.5114/pjp.2019.93136
8. Bissler JJ, Christopher Kingswood J. Renal manifestation of tuberous sclerosis complex. Am J Med Genet C Semin Med Genet. 2018;178(3):338–347. doi:10.1002/ajmg.c.31654
9. Aydin H, Magi-Galluzzi C, Lane BR, et al. Renal angiomyolipoma: clinicopathologic study of 194 cases with emphasis on the epithelioid histology and tuberous sclerosis association. Am J Surg Pathol. 2009;33(2):289–297. doi:10.1097/PAS.0b013e31817ed7a6
10. Lee W, Choi SY, Lee C, et al. Does epithelioid angiomyolipoma have poorer prognosis, compared with classic angiomyolipoma? Investig Clin Urol. 2018;59(6):357–362. doi:10.4111/icu.2018.59.6.357
11. Zizzo M, Ugoletti L, Tumiati D, et al. Primary pancreatic perivascular epithelioid cell tumor (PEComa): a surgical enigma. A systematic review of the literature. Pancreatology. 2018;18(3):238–245. doi:10.1016/j.pan.2018.02.007
12. Bleeker JS, Quevedo JF, Folpe AL. ”Malignant” perivascular epithelioid cell neoplasm: risk stratification and treatment strategies. Sarcoma. 2012;2012:541626. doi:10.1155/2012/541626
13. Kiefer J, Mutschler M, Kurz P, et al. Accuracy of core needle biopsy for histologic diagnosis of soft tissue sarcoma. Sci Rep. 2022;12(1):1886. doi:10.1038/s41598-022-05752-4
14. Bourgmayer A, Nannini S, Bonjean P, Kurtz JE, Malouf GG, Gantzer J. Natural history and treatment strategies of advanced PEComas: a systematic review. Cancers. 2021;13(20):5227. doi:10.3390/cancers13205227
15. Folpe AL, Kwiatkowski DJ. Perivascular epithelioid cell neoplasms: pathology and pathogenesis. Hum Pathol. 2010; 41(1):1–15. doi:10.1016/j.humpath.2009.05.011
16. Liu L, Dehner C, Grandhi N, et al. The Impact of TSC-1 and −2 mutations on response to therapy in malignant PEComa: a multicenter retrospective analysis. Genes. 2022;13(11):1932. doi:10.3390/genes13111932
17. Malinowska I, Kwiatkowski DJ, Weiss S, Martignoni G, Netto G, Argani P. Perivascular epithelioid cell tumors (PEComas) harboring TFE3 gene rearrangements lack the TSC2 alterations characteristic of conventional PEComas: further evidence for a biological distinction. Am J Surg Pathol. 2012;36(5):783–784. doi:10.1097/PAS.0b013e31824a8a37
18. Schmiester M, Dolnik A, Kornak U, et al. TFE3 activation in a TSC1-altered malignant PEComa: challenging the dichotomy of the underlying pathogenic mechanisms. J Pathol. 2021;7(1):3–9. doi:10.1002/cjp2.187
19. Giannikou K, Azim -A-A, Adib E, et al. Distinct oncogenic signatures in malignant PEComa and leiomyosarcoma identified by integrative RNA-seq and H3K27ac ChIP-seq analysis. J Clin Oncol. 2022;40(16_suppl):11552. doi:10.1200/JCO.2022.40.16_suppl.11552
20. D’Andrea D, Hanspeter E, D’Elia C, Martini T, Pycha A. Malignant perivascular epithelioid cell neoplasm (PEComa) of the pelvis: a case report. Urol Case Rep. 2016;6:36–38. doi:10.1016/j.eucr.2016.02.004
21. Casali PG, Abecassis N, Aro HT, et al. Soft tissue and visceral sarcomas: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv51–iv67. doi:10.1093/annonc/mdy096
22. Sobiborowicz A, Świtaj T, Teterycz P, et al. Feasibility and long-term efficacy of PEComa Treatment—20 years of experience. J Clin Med. 2021;10(10):2200. doi:10.3390/jcm10102200
23. Chen Z, Han S, Wu J, et al. A systematic review: perivascular epithelioid cell tumor of gastrointestinal tract. Medicine. 2016;95(28):e3890. doi:10.1097/MD.0000000000003890
24. Mazeron JJ, Suit HD. Lymph nodes as sites of metastases from sarcomas of soft tissue. Cancer. 1987;60(8):1800–1808. doi:10.1002/1097-0142(19871015)60:8<1800::AID-CNCR2820600822>3.0.CO;2-N
25. Dudek W, Schreiner W, Mykoliuk I, Higaze M, Sirbu H. Pulmonary metastasectomy for sarcoma—survival and prognostic analysis. J Thorac Dis. 2019;11(8):3369–3376. doi:10.21037/jtd.2019.08.10
26. Sugarbaker PH. Long-term survival is possible using cytoreductive surgery plus HIPEC for sarcomatosis—Case report of 2 patients. Int J Surg Case Rep. 2019;64:10–14. doi:10.1016/j.ijscr.2019.09.009
27. Bhanushali AH, Dalvi AN, Bhanushali HS. Laparoscopic excision of infra-renal PEComa. J Minim Access Surg. 2015;11(4):282–284. doi:10.4103/0972-9941.166439
28. Lin K-H, Chang N-J, Liou L-R, M-S S, Tsao M-J, Huang M-L. Successful management of perivascular epithelioid cell tumor of the rectum with recurrent liver metastases. Medicine. 2018;97(31):e11679. doi:10.1097/MD.0000000000011679
29. Stamenovic D, Hohenberger P, Roessner E. Pulmonary metastasectomy in soft tissue sarcomas: a systematic review. J Thorac Dis. 2021;13(4):2649–2660. doi:10.21037/jtd-2019-pm-13
30. Machado I, Cruz J, Lavernia J, Rayon JM, Poveda A, Llombart-Bosch A. Malignant PEComa with metastatic disease at diagnosis and resistance to several chemotherapy regimens and targeted therapy (m-TOR Inhibitor). Int J Surg Pathol. 2017;25(6):543–549. doi:10.1177/1066896917701245
31. Kirste S, Kayser G, Zipfel A, Grosu A-L, Brunner T. Unresectable hepatic PEComa: a rare malignancy treated with stereotactic body radiation therapy (SBRT) followed by complete resection. Radiat Oncol. 2018;13:28. doi:10.1186/s13014-018-0974-5
32. Armah HB, Parwani AV. Perivascular epithelioid cell tumor. Arch Pathol Lab Med. 2009;133(4):648–654. doi:10.5858/133.4.648
33. Liu J-L, Lin Y-M, Lin M-C, Yeh K-T, Hsu J-C, Chen C-J. Perivascular epithelioid cell tumor (PEComa) of the uterus with aggressive behavior at presentation. Hematol Oncol Stem Cell Ther. 2009;2(3):426–430. doi:10.1016/S1658-3876(09)50013-1
34. Scheppach W, Reissmann N, Sprinz T, Schippers E, Schoettker B, Mueller JG. PEComa of the colon resistant to sirolimus but responsive to doxorubicin/ifosfamide. World J Gastroenterol. 2013;19(10):1657–1660. doi:10.3748/wjg.v19.i10.1657
35. Sanfilippo R, Jones RL, Blay J-Y, et al. Role of Chemotherapy, VEGFR Inhibitors, and mTOR Inhibitors in advanced perivascular epithelioid cell tumors (PEComas). Clin Cancer Res. 2019;25(17):5295–5300. doi:10.1158/1078-0432.CCR-19-0288
36. Hindi N, Sanfilippo R, Stacchiotti S, et al. 1450P - systemic therapy in perivascular epithelioid cell tumors (Pecoma). Ann Oncol. 2014;25:iv506. doi:10.1093/annonc/mdu354.39
37. Raimondi A, Colombo F, Pintarelli G, et al. Prolonged activity and toxicity of sirolimus in a patient with metastatic renal perivascular epithelioid cell tumor: a case report and literature review. Anticancer Drugs. 2018;29(6):589–595. doi:10.1097/CAD.0000000000000634
38. Gondran H, Thebaud E, Moreau A, et al. First pancreatic perivascular epithelioid cell tumor (PEComa) treated by mTOR inhibitor. Pancreatology. 2019;19(4):566–568. doi:10.1016/j.pan.2019.05.459
39. Tang S-H, Liu Y-C, Hsiao -H-H, et al. Huge soft tissue PEComa with aggressive lung and bone metastases. J Cancer Res Pract. 2017;4(3):115–118. doi:10.1016/j.jcrpr.2017.04.001
40. Starbuck KD, Drake RD, Budd GT, Rose PG. Treatment of advanced malignant uterine perivascular epithelioid cell tumor with mTOR inhibitors: single-institution experience and review of the literature. Anticancer Res. 2016;36(11):6161–6164. doi:10.21873/anticanres.11208
41. Benson C, Vitfell-Rasmussen J, Maruzzo M, et al. A retrospective study of patients with malignant PEComa receiving treatment with sirolimus or temsirolimus: the Royal Marsden Hospital experience. Anticancer Res. 2014;34(7):3663–3668.
42. Weeber F, Koudijs MJ, Hoogstraat M, et al. Effective therapeutic intervention and comprehensive genetic analysis of mTOR signaling in PEComa: a case report. Anticancer Res. 2015;35(6):3399–3403.
43. Gennatas C, Michalaki V, Kairi PV, Kondi-Paphiti A, Voros D. Successful treatment with the mTOR inhibitor everolimus in a patient with perivascular epithelioid cell tumor. World J Surg Oncol. 2012;10:181. doi:10.1186/1477-7819-10-181
44. Chen S-C, Yang C-W, Yen -C-C, Tseng C-H, Chao T-C. Perivascular Epithelioid Cell Tumors (PEComas) Refractory to mTOR Inhibitors. J Cancer Res Pract. 2014;1(2):128–133.
45. Italiano A, Delcambre C, Hostein I, et al. Treatment with the mTOR inhibitor temsirolimus in patients with malignant PEComa. Ann Oncol. 2010;21(5):1135–1137. doi:10.1093/annonc/mdq044
46. Bunch K, Sunde J. Fertility sparing treatment of a malignant uterine perivascular epithelioid cell tumor: a case report. Gynecol Oncol Case Rep. 2014;8:14–16. doi:10.1016/j.gynor.2014.01.001
47. Wagner AJ, Ravi V, Riedel RF, et al. nab-sirolimus for patients with malignant perivascular epithelioid cell tumors. J Clin Oncol. 2021;39(33):3660–3670. doi:10.1200/JCO.21.01728
48. Osei DA, Alvandi F, Brooks JS, Ogilvie CM. PEComa of the upper extremity: a unique case and description of an initial response to neoadjuvant chemotherapy. Sarcoma. 2007;2007:53056. doi:10.1155/2007/53056
49. Flechter E, Zohar Y, Guralnik L, Passhak M, Sela GB. Long-lasting stable disease with mTOR inhibitor treatment in a patient with a perivascular epithelioid cell tumor: a case report and literature review. Oncol Lett. 2016;12(6):4739–4743. doi:10.3892/ol.2016.5231
50. Alnajar H, Brickman A, Buckingham L, Arvanitis LD. Metastatic malignant PEComa of the leg with identification of ATRX mutation by next-generation sequencing. Virchows Arch. 2018;472(3):499–503. doi:10.1007/s00428-017-2208-x
51. Xu J, Gong X-L, Wu H, Zhao L. Case Report: gastrointestinal PEComa With TFE3 Rearrangement Treated With Anti-VEGFR TKI Apatinib. Front Oncol. 2020;10:10. doi:10.3389/fonc.2020.00010
52. Rutkowski P, Przybył J, Świtaj T. Genetics of rare mesenchymal tumors: implications for targeted treatment in DFSP, ASPS, CCS, GCTB and PEComa. Int J Biochem Cell Biol. 2014;53:466–474. doi:10.1016/j.biocel.2014.03.024
53. Doyle LA, Hornick JL, Fletcher CDM. PEComa of the gastrointestinal tract: clinicopathologic study of 35 cases with evaluation of prognostic parameters. Am J Surg Pathol. 2013;37(12):1769–1782. doi:10.1097/PAS.0b013e31829caab3
54. Huľová S, Sycova-Mila Z, Macák D, et al. Dia-gnostic challenges and extraordinary treatment response in rare malignant PEComa tumor of the kidney. Klin Onkol. 2018;31(6):448–452. doi:10.14735/amko2018448
55. Robles NR, Peces R, Gómez-Ferrer Á, et al. Everolimus safety and efficacy for renal angiomyolipomas associated with tuberous sclerosis complex: a Spanish expanded access trial. Orphanet J Rare Dis. 2016;11:128. doi:10.1186/s13023-016-0517-9
56. Purwar R, Soni K, Shukla M, Verma A, Kumar T, Pandey M. TFE3-associated perivascular epithelioid cell tumor with complete response to mTOR inhibitor therapy: report of first case and literature review. World J Surg Oncol. 2022;20(1):62. doi:10.1186/s12957-021-02462-5
57. Sobiborowicz A, Czarnecka AM, Szumera-Ciećkiewicz A, Rutkowski P, Świtaj T. Diagnosis and treatment of malignant PEComa tumours. Oncol Clin Pract. 2020;16(1):22–33. doi:10.5603/OCP.2020.0003
58. Gu L, Peng C, Zhang F, Fang C, Guo G. Sequential everolimus for angiomyolipoma associated with tuberous sclerosis complex: a prospective cohort study. Orphanet J Rare Dis. 2021;16(1):277. doi:10.1186/s13023-021-01913-2
59. Goldberg HJ, Harari S, Cottin V, et al. Everolimus for the treatment of lymphangioleiomyomatosis: a Phase II study. Eur Respir J. 2015;46(3):783–794. doi:10.1183/09031936.00210714
60. Dickson MA, Ravi V, Riedel RF, et al. nab-Sirolimus for patients with advanced malignant PEComa with or without prior mTOR inhibitors: biomarker results from AMPECT and an expanded access program. J Clin Oncol. 2022;40(16_suppl):11574. doi:10.1200/JCO.2022.40.16_suppl.11574
61. Wagner AJ, Ravi V, Riedel RF, et al. Long-term follow-up for duration of response (DoR) after weekly nab -sirolimus in patients with advanced malignant perivascular epithelioid cell tumors (PEComa): results from a registrational open-label phase II trial, AMPECT. J Clin Oncol. 2020;38:11516. doi:10.1200/JCO.2020.38.15_suppl.11516
62. Zhong J, Hu Y, Si L, et al. Primary perivascular epithelioid cell tumor (PEComa) in bone: a review of the literature and a case arising in the humerus with multiple metastases. J Bone Oncol. 2021;26:100336. doi:10.1016/j.jbo.2020.100336
63. McBride A, Garcia AJ, Sanders LJ, et al. Sustained response to pembrolizumab in recurrent perivascular epithelioid cell tumor with elevated expression of programmed death ligand: a case report. J Med Case Rep. 2021;15(1):400. doi:10.1186/s13256-021-02997-x
64. Lattanzi M, Deng FM, Chiriboga LA, et al. Durable response to anti-PD-1 immunotherapy in epithelioid angiomyolipoma: a report on the successful treatment of a rare malignancy. J Immunother Cancer. 2018;6(1):97. doi:10.1186/s40425-018-0415-x
65. D’Angelo SP, Mahoney MR, Van Tine BA, et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): two open-label, non-comparative, randomised, Phase 2 trials. Lancet Oncol. 2018;19(3):416–426. doi:10.1016/S1470-2045(18)30006-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.