")
Back to Journals » Journal of Pain Research » Volume 15
Management of Metastatic Disease in Campania (MAMETIC): An Observational Multicenter Retrospective and Prospective Trial on Palliative Radiotherapy in an Italian Region. Study Protocol
Authors Di Franco R, Cascella M , Fusco M, Borzillo V, Scipilliti E, Ferraioli P, Iannacone E , De Palma G, Silvestro G , Gherardi F, Buonopane S , Alberti D, Totaro G, Manzo R, Guida G, Cuomo A, Pignata S, Di Napoli M, Rossetti S, Celentano E , Crispo A, Grimaldi M, Ravo V , Muto P
Received 27 August 2021
Accepted for publication 30 December 2021
Published 8 April 2022 Volume 2022:15 Pages 1003—1010
DOI https://doi.org/10.2147/JPR.S336357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Rossella Di Franco,1 Marco Cascella,2 Mario Fusco,3 Valentina Borzillo,1 Esmeralda Scipilliti,1 Piera Ferraioli,1 Eva Iannacone,1 Giampaolo De Palma,1 Giustino Silvestro,1 Federica Gherardi,1 Sergio Buonopane,1 Domingo Alberti,1 Giuseppe Totaro,1 Roberto Manzo,1 Giovanna Guida,1 Arturo Cuomo,2 Sandro Pignata,4 Marilena Di Napoli,4 Sabrina Rossetti,4 Egidio Celentano,5 Anna Crispo,5 Maria Grimaldi,5 Vincenzo Ravo,1 Paolo Muto1
1Department of Radiation Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italia; 2Division of Anesthesia and Pain Medicine, Istituto Nazionale Tumori, IRCCS Fondazione G. Pascale, Napoli, Italia; 3Cancer Registry Unit, ASL Napoli 3 SUD, Napoli, Italia; 4Department of Uro-Gynecological, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italia; 5Epidemiology and Biostatistics Unit, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italia
Correspondence: Rossella Di Franco, Department of Radiation Oncology, Istituto Nazionale Tumori - IRCCS - Fondazione G. Pascale, Napoli, Italia, Email [email protected]
Background: In the Italian Campania Region, 30.517 new cases of solid cancer have been diagnosed, in 2019. Of those, patients with metastatic disease are up to 20%. This class of patients is extremely diversified and copious, and the offer of radiotherapy may vary in different geographical areas within the same region. The aim of this observational multicenter retrospective and prospective trial is to evaluate the occurrence of metastatic metastatic cancer patients candidates for palliative radiotherapy in several areas of a great Italian region, the management of the disease through RT approaches, and its impact on cancer-related pain and overall HRQoL.
Methods: This is a multicenter, retrospective and prospective observational investigation. The retrospective part of the study concerns all patients enrolled with a diagnosis of metastatic disease and treated in RT centers within the Campania Region between January 2019 and July 2020. The prospective phase is going to involve all the metastatic patients with an indication of palliative RT. Considering regional epidemiological data, we expect an enrollment of 12.500– 21.000 patients in 5 years.
Conclusion: The MAMETIC Trial in an observational study designed for investigating on the use of radiotherapy in patients with advanced disease within a regional area, and for evaluating the local response to the patient’s request. It can be a unique opportunity, not only to highlight possible geographic differences but also to regularly collect and share data to standardize the therapeutic offer within the regional area. ClinicalTrials.gov ID NCT04595032, retrospectively registered.
Keywords: palliative care, metastatic disease, radiotherapy, cancer pain, breakthrough cancer pain, quality of life
Background
The overall survival is the main outcome for evaluating healthcare system efficiency in cancer treatment. It is highly influenced by the diagnosis phase and cancer treatment efficacy. Secondary prevention, availability, and rapid access to treatments have a crucial influence.
Although it was demonstrated that the number of cancer deaths in 2005 and 2016 is roughly the same, the number of cancer deaths recorded with metastasis as a contributing cause of death tripled from 1953 (18.5%) to 2016 (55.5%).1 Furthermore, metastases are responsible for about 90% of cancer deaths worldwide.2
The proportion of all cancer deaths recorded with metastases ranged from 100% (testicular, sinus cancer) to 9.3% for central nervous system cancers. For prostate cancer, the cancer death rate recorded with metastasis as a contributing cause was only 50.5%. Breast cancer incidence has increased over the past decade, while breast cancer deaths are declining. The death rate from metastatic disease, however, is remarkably stable.2 In the Italian context, data from the Italian Association of Medical Oncology (AIOM) showed that for all solid tumors, 66.7% of cancer deaths were recorded with metastasis as a concomitant cause, although the proportions varied substantially between tumor groups.3
In metastatic disease, palliative care has the essential purpose to improve the health-related quality of life (HRQoL).4 The earliest diagnosis is provided, the greater will be the aims achieved and the efficacy of the treatments. The local presence of diagnostic and therapeutic possibilities can be decisive in the patient’s perspective on life. Nevertheless, in some geographical contexts, there may be deficiencies in the provision of particular palliative care interventions, such as radiation therapy (RT) approaches. These deficiencies can be expressed in terms of reduced supply of procedures, delays in delivery, and poor quality of the offer. Moreover, within a geographical region, inequality in access to diagnostic-therapeutic pathways can be detected.
Territorial cancer registers give a fundamental contribution for evaluating the incidence of cancer, the stage at diagnosis, and the correlation with particular environmental situations. In the Italian Campania Region, the recording cancer network has provided a General Cancer Registry of the population within each Local Health and a Regional Children’s Cancer Registry. Despite this, there is a lack of important data such as the prevalence of metastatic cancer, referring to the different territorial areas within the region.
Study Rationale
From the data mainly obtained from the SEER (Surveillance, Epidemiology, and End Results) archive, it is estimated that patients with metastatic disease represent up to 20% of the total number of solid tumors diagnosed.3 Furthermore, according to the latest AIOM report in 2019, and excluding non-melanoma skin cancers, the Campania Region diagnosed 30.517 new cases of solid cancer. Consequently, applying the United States (US) prevalence figure (20%), the number of metastatic patients for solid tumors in Campania should be around 6.100 patients, per year.5
On these premises, the MAnagement of METastatic disease In Campania (MAMETIC) study aims to evaluate metastatic cancer patients living in the Italian Campania region who refer to RT centers for palliative radiation treatments. Moreover, the management of the disease through RT approaches and its impact on cancer-related pain and overall patients’ HRQoL will be investigated.
All the data will be transmitted to the coordinating center and the initiative will be integrated with the regional oncology network (the General Cancer Registry). We estimate that this study will be useful not only to the RT community but it will also provide a regional assessment on the management of malignant disease, enhancing in turn the functioning of the network.
Methods
Overall Design
The MAMETIC Trial is a multicenter, retrospective and prospective observational investigation (Figure 1).
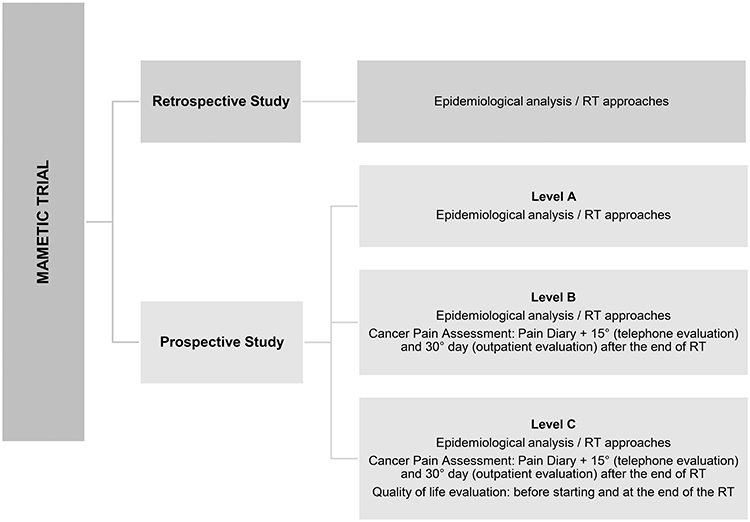 |
Figure 1 Flowchart of study design: Retrospective study consists of epidemiological analysis; prospective study consists of both epidemiological (level A, B and C), cancer pain assessment (level B and C) and patient’s quality of life (level C) analysis. |
Because in 2019, about 12.500 patients have been treated in the centers and it is estimated that 20–30% of the above-mentioned patients had metastasis, approximately 2.560 patients are expected to be enrolled.
Study Setting
RT centers joining the study can enter patient data in appropriate eCRFs. An eCRF will be provided for the retrospective part of the study. About the prospective part, RT centers can choose 3 levels of membership:
- Level A: epidemiological data entry on clinical features (metastatic cancers) and RT offered.
- Level B: level A plus pain features and analgesic therapy data.
- Level C: adds to the two previous levels data on HRQoL.
We have chosen to offer a different membership option to collect the greatest number of epidemiological information (primary objective). From the centers that will be able to enter the most complete data (Level B and level C), it will be possible to obtain data to achieve the secondary objectives.
Outcome Measures
The primary objective of the study is focused on the data collection concerning metastatic cancers candidates for palliative Radiotherapy in the Campania region. This objective regards both the retrospective and prospective phases of the study.
For this purpose, will be recorded:
- Epidemiological data (patient/disease):
- Patient data
- Cancer type
- Metastasis
- Incidence of metastatic disease at diagnosis
- Time between first diagnosis and the onset of metastases
Secondary objectives of the study are:
- Characterization of palliative RT offered
- Cancer pain features
- Patients’ HRQoL
Study Population
Eligible candidates for MAMETIC are metastatic patients candidates for palliative RT.
- Patients with bone metastases. They are about 70% of cancer patients in advanced stage of disease.6 They often have complicated lesions, with tumor tissue invading the muscle or nerve structures close to the bone. These lesions usually cause constant or intermittent pain, with a neuropathic component. In addition to baseline pain, the patient may have episodes of BTcP (Breakthrough cancer Pain) that compromise the HRQoL. As a result, they may have severe movement restrictions and an increased risk of pathological bone fracture.7,8
- Patients with metastases affecting the thoracic district with primary or secondary locally advanced disease. Symptoms such as dyspnea, chest pain, cough, hemoptysis, and dysphagia can be controlled with radiation treatments in 2/3 of these patients. Palliative mediastinal RT can improve obstructive dysphagia in locally advanced esophageal cancer.9 At the same time, it can improve esophageal function after insertion of a stent.10 Again, in patients with mediastinal syndrome, radiant treatment of the whole or part of mediastinum can ameliorate the HRQoL.
- Patients with bleeding, who may have neoplastic bleeding in the gastrointestinal, genitourinary, upper respiratory tract, or pelvic tract. For these patients, RT can have an important hemostatic effect and consequently can improve symptoms and hematological values. Radiant treatment can be used for hemostatic purposes in patients with bladder, rectal or gynecological malignancies with an improvement of the symptoms in 50–75% of cases.
- Patients with brain or spinal cord metastases. This category includes patients with symptomatic or asymptomatic brain metastases, patients with symptomatic or asymptomatic bone marrow compression, and those with cauda equina syndrome. In patients with paraplegia caused by spinal cord compression, 10% of motility can be recover if treatment is early. The presence of brain metastases can cause severe symptoms such as epilepsy, focal neurological symptoms, or intracranial hypertension symptoms such as nausea, vomiting, or headache.11
- Patients with symptomatic lymph node lesions who may have neck lymph node packages or pelvic district.
Eligibility criteria are summarized in Table 1.
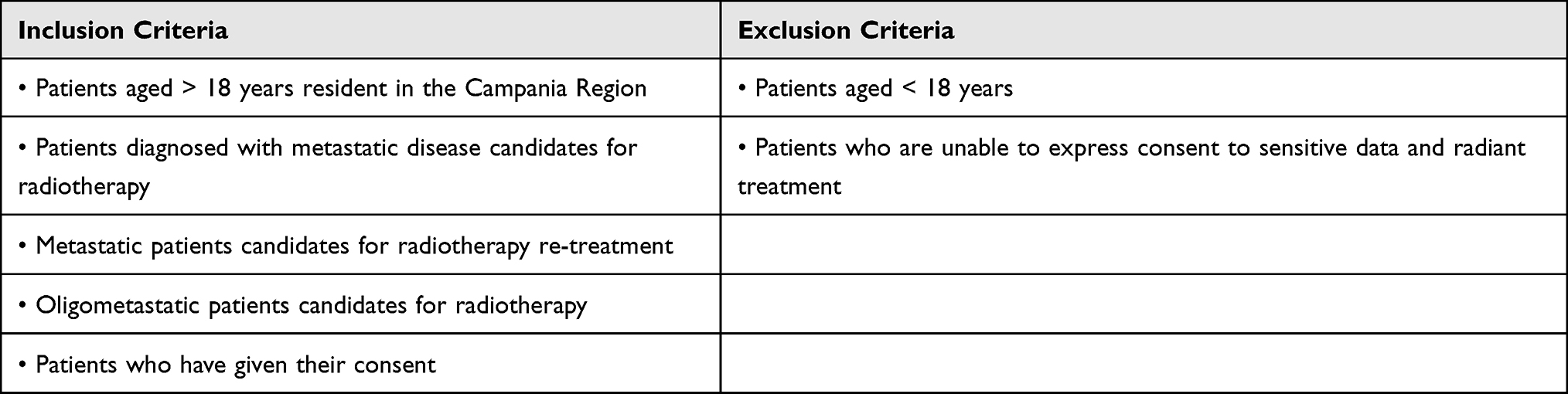 |
Table 1 MAMETIC-Trial: Eligibility Criteria |
Clinical Variables
Clinical characteristics of patients will be collected from hospital clinical documentation and RT treatment plans, according to data needed for the study. Data will be identified in the medical record and collected in specific eCRF:
- Address
- Weight
- Height
- Primary tumor
- Date of the first diagnosis
- Stage c/pTNM at diagnosis
- Therapies carried out for the primary tumor (surgery, chemotherapy, hormone therapy, immunotherapy, target therapies, RT)
- Metastatic disease diagnosis date
- Pre-treatment radiotherapy visit date
- Start and end date of palliative RT
- Possible request for rapid access to RT
- Indications for palliative RT (bone marrow compression, mediastinal syndrome, hemostasis, bone metastasis painful, painless bone metastasis, compression or infiltration pain, bone - lung - liver - lymph node - adrenal oligometastasis, brain metastases, primitive encephalic with expired PS)
- Type of treatment: RT flash, SBRT
- Prescribed dose and fractions
- Re-treatment.
- Type of pain (neuropathic, nociceptive, mixed) and intensity measured through the Numeric Rating Scale (NRS) score. This latter is an 11-point scale (from 0 to 10), with higher scores indicating greater pain intensity.
- Breakthrough cancer pain (BTcP) [defined as “a transitory flare of pain that occurs on a background of relatively well-controlled baseline pain”12] in terms of number of episodes/day; pain intensity.13
- Pain flare (a transient worsening of the bone pain after RT) in terms of intensity (NRS).
- Data about pain therapy: drugs (adjuvant drugs, opioids, non-opioid analgesics) and doses.14
- Adverse events of the pain therapy.
- For the pain evaluation, patients will report pain data (NRS, episodes of BTcP) and therapy in a Pain Diary. Follow-ups will be performed on the 15th (telephone revaluation) and 30th day (outpatient revaluation) after the end of RT treatment.
- c. Level C. In addition to what is specified for levels A and B, the following tools for assessing the patients’ HRQoL will be adopted before starting and at the end of the RT treatment:
- The European Organization for Research and Treatment of Cancer (EORTC) QLQC15-PAL questionnaire,15 and Palliative Performance Score (PPS)16 for all patients.
- The EORTC QLQ-BM2217 questionnaire; van der Linden Score;18 Mizumoto Prognostic Score19 for assessing the HRQoL in patients with bone metastases.
- The Spinal Instability Neoplastic Score (SINS)20 used for investigating the incidence of spinal instability in patients with spinal metastases.
- The American Spinal Injury Association (ASIA) Score21 for evaluation of the functional impairment because of the spinal cord injury/compression.
- The Mini-Mental State Examination (MMSE)22 for assessing cognitive function in patients with brain metastases.
Data Collecting and Statistical Considerations
The data collection and registration procedures will be carried out through specific CRFs organized on an electronic platform managed by the coordinating center which will be responsible for the privacy of sensitive data. The platform was created with a management software developed with Microsoft Net technology, Web App made with Internet Information Services (IIS 10) pattern, MVC, Razor syntax, Jquery 3.4.1 scripting language. Net framework version 4.8. SQL Server 2019 database version 15. Crystal Reporting for Visual Studio 2019.
The data will be transmitted to the coordinating center when each form is completed by the operator of the individual center. Every 3 months a report of the total amount of patients entered in the platform will be sent by the coordinating center to every center participating in the study.
A descriptive analysis will summarize the total number and stratification of patients with metastatic disease by place of residence and tumor location. Metastatic tumors at diagnosis will be differentiated from metastatic disease developed later. Every center is going to fill a form for each patient with mandatory socio-demographic and anamnestic information (Level A) and information on pain and HRQoL (Levels B and C). This process lets the study produce a compliance survey by a single center and carry on a comparative analysis for subsequent levels on qualitative variables (presence of pain; typology and characterization of pain) through the Chi-Square Test and quantitative variables (pain scale, scores on quality of life) with T-test and ANOVA. Nonparametric tests will be provided where the population distribution does not have a known form (normal Gaussian). The significance of the tests is fixed with p <0.05.
Discussion
Palliative RT is an efficient component of supportive and palliative care in the oncology field and palliation of advanced and metastatic cancers symptoms are one of the most common indications for RT.
Although it was estimated that patients with metastatic disease represent up to 20% of the total number of solid tumors diagnosed, the use of palliative RT treatments potentially involves only up to 40% of patients in a radiation oncology center.23
The oncological incidence data, detected by population risk and collected from the Cancer registries, show different standardized rates in various regional territorial areas. Moreover, at the regional level, data on territorial distribution and evolution of tumors towards the advanced stages are absent. In addition to oncological mortality data, this knowledge could occur significantly to understand the causes of the several territorial possibilities in the organization of diagnostic-therapeutic-care pathways in terms of socio-economic structure of reference population, degree of diagnostic anticipation and different stage at diagnosis, availability of territorial diagnosis and treatment structures, level of care standards. Furthermore, there is a lack of precise knowledge on coverage and methods of RT services regional delivery in the advanced stages of neoplastic pathology in Campania.
Conclusion
A regional observational study that provides information on the use of radiotherapy in patients with advanced disease, their territorial management, and their impact on the HRQoL of patients, can represent an important opportunity to observe territorial alternatives and can help in the management of metastatic patients and improve the therapeutic offer. At the same time, since this is a multicenter study involving several almost all RT centers in the region, it can represent a useful moment will help standardize and share the RT protocols adopted in the treatments of advanced tumors and their complications in a great Italian region.
Abbreviations
AIOM, Association of Medical Oncology; ASIA, American Spinal Injury Association; BTcP, breakthrough cancer pain; EORTC, European Organization for Research and Treatment of Cancer; HRQoL, Health-related quality of life; IMRT, intensity-modulated radiation therapy; MAMETIC, MAnagement of METastatic disease In Campania; NRS, numeric rating scale; RT, radiotherapy; SEER, Surveillance, Epidemiology and End Results; SBRT, stereotactic body radiation therapy; SINS, spinal instability neoplastic score; 3DCRT, three-dimensional conformal radiation therapy; VMAT, volumetric modulated arc therapy.
Data Sharing Statement
The authors declare the availability of data and material.
Ethics Approval and Consent to Partecipate
The MAMETIC Trial is promoted by the Division of Radiotherapy of National Cancer Institute - IRCCS Fondazione Pascale, Naples (Italy), in collaboration with the Divisions of Anesthesia and Pain Medicine, Uro-Gynecological Medical Oncology, Epidemiology and Biostatistics of the Fondazione Pascale, and with the Cancer Registry Unit ASL-Napoli 3 South. The local Ethics Committee approved the protocol on July 8, 2020 (n. 868/2020).
Each interested center will submit the protocol to its ethics committee to be approved before accrual. After approval, the center will receive a dedicated electronic case report form (CRF). Eligible patients who provided written consent and meet the inclusion criteria are anonymously registered on the CRF by assigning a numerical code.
The Trial is to be conducted in strict compliance with the Protocol, in the version in force as accepted by the Principal Investigator and approved by the Ethics Committee and the Competent Authority in accordance with the Helsinki Declaration, the Guidelines for Good Clinical Practice E6 (R2), 14 June 2017, EMA/CHMP/ICH/135/, and in accordance with the applicable laws on transparency, data protection regulations.
Consent for Publication
The authors consent to data’s publication.
Acknowledgments
The authors gratefully acknowledge Mrs. Diana d’Alterio for the contribute in the manuscript editing and Mr. Rocco Saviano for the technical support in creating the electronic platform.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The trial will be conducted without external funding.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Dillekås H, Rogers MS. Straume O - Are 90% of deaths from cancer caused by metastases? Cancer Med. 2019;8(12):5574–5576.
2. Dillekas H, Demicheli R, Ardoino I, Jensen SA, Biganzoli E, Straume O. The recurrence pattern following delayed breast reconstruction after mastectomy for breast cancer suggests a systemic effect of surgery on occult dormant micrometastases. Breast Cancer Res Treat. 2016;158(1):169–178.
3. Italian Association of Medical Oncology. AIOM-AIRTUM. [Data on cancer in Italy, 2019]. In Italian. Brescia: Intermedia Editore; 2020. Available from: https://www.aiom.it/wp-content/uploads/2019/09/2019_Numeri_Cancro-operatori-web.pdf.
4. Cascella M, Crispo A, Esposito G, et al. Multidimensional Statistical Technique for Interpreting the Spontaneous Breakthrough Cancer Pain Phenomenon. A Secondary Analysis from the IOPS-MS Study. Cancers. 2021;13(16):4018. doi:10.3390/cancers13164018
5. Huang JF, Shen J, Li X, et al. Incidence of Patients With Bone Metastases at Diagnosis of Solid Tumors in Adults: a Large Population-Based Study. Ann Transl Med. 2020;8(7):482. doi:10.21037/atm.2020.03.55
6. Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res. 2006;12:6243s–9s. doi:10.1158/1078-0432.CCR-06-0931
7. Falivene S, Pezzulla D, Di Franco R, et al. Painful bone metastasis in elderly treated with radiation therapy: single- or multiple-fraction regimen? A multicentre retrospective observational analysis. Aging Clin Exp Res. 2017;29(Suppl 1):143–147.
8. Giugliano FM, Franco RD, Iadanza L, et al. (2014) Elderly Patients with Painful Bone Metastases. The Impact of Comorbidity on the Choice of Radiation Therapy Regimen. J Palliat Care Med. 2014;4:199. doi:10.4172/2165-7386.1000199
9. Kassam Z, Wong RKS, Ringash J, et al. A phase I/II study to evaluate the toxicity and efficacy of accelerated fractionation radiotherapy for the palliation of dysphagia from carcinoma of the oesophagus. Clin Oncol (R Coll Radiol). 2008;20:53–60.
10. Javed A, Pal S, Dash NR, et al. Palliative stenting with or without radiotherapy for inoperable esophageal carcinoma: a randomized trial. J Gastrointest Cancer. 2012;43:63–69.
11. Borzillo V, Giugliano FM, Di Franco R, et al. Radiosurgery and Stereotactic Radiotherapy for Brain Metastases According the New Prognostic Indexes: our Preliminary. Exp Neurol Neurophysiol. 2015;6:6.
12. Portenoy RK, Hagen NA. Breakthrough pain: definition, prevalence, and characteristics. Pain. 1990;41:273–281.
13. Cuomo A, Cascella M, Forte CA, et al. Careful Breakthrough Cancer Pain Treatment through Rapid-Onset Transmucosal Fentanyl Improves the Quality of Life in Cancer Patients: results from the BEST Multicenter Study. J Clin Med. 2020;9(4):1003. doi:10.3390/jcm9041003
14. Cascella M, Forte CA, Bimonte S, et al. Multiple effectiveness aspects of tapentadol for moderate-severe cancer-pain treatment: an observational prospective study. J Pain Res. 2018;12:117–125. doi:10.2147/JPR.S181079
15. Lam K, Zeng L, Zhang L, et al. Predictive factors of overall well-being using the EORTC QLQ-C15-PAL extracted from the EORTC QLQ-C30. J Palliat Med. 2013;16(4):402–408.
16. Yoon SJ, Choi SE, LeBlanc TW, Suh SY. Palliative Performance Scale Score at 1 Week After Palliative Care Unit Admission is More Useful for Survival Prediction in Patients With Advanced Cancer in South Korea. Am J Hosp Palliat Care. 2018;35(9):1168–1173.
17. Mendez LC, Raman S, Wan BA, et al. Quality of life in responders after palliative radiation therapy for painful bone metastases using EORTC QLQ-C30 and EORTC QLQ-BM22: results of a Brazilian cohort. Ann Palliat Med. 2017;6(Suppl 1):S65–S70.
18. van der Linden YM, Dijkstra SPDS, Vonk EJA, Marijnen CAM, Leer JWH. Dutch Bone Metastasis Study Group. Prediction of survival in patients with metastases in the spinal column: results based on a randomized trial of radiotherapy. Cancer. 2005;103(2):320–328.
19. Mizumoto M, Harada H, Asakura H, et al. Prognostic factors and a scoring system for survival after radiotherapy for metastases to the spinal column: a review of 544 patients at Shizuoka Cancer Center Hospital. Cancer. 2008;113(10):2816–2822.
20. Shi DD, Hertan LM, Lam TC, et al. Assessing the utility of the spinal instability neoplastic score (SINS) to predict fracture after conventional radiation therapy (RT) for spinal metastases. Pract Radiat Oncol. 2018;8(5):e285–e294.
21. van Middendorp JJ, Goss B, Urquhart S, Atresh S, Williams RP, Schuetz M. Diagnosis and Prognosis of Traumatic Spinal Cord Injury. Global Spine J. 2011;1(1):1–8.
22. Murray KJ, Scott C, Zachariah B, et al. Importance of the mini-mental status examination in the treatment of patients with brain metastases: a report from the radiation therapy oncology group protocol. Int J Radiation Oncol Biol Phys. 2000;48(1):59–64.
23. Cellini F, Manfrida S, Deodato F, et al. Pain REduction with bone metastases STereotactic radiotherapy (PREST): a Phase III randomized multicentric trial. Trials. 2019;20(1):609.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.