Back to Journals » ClinicoEconomics and Outcomes Research » Volume 11
Management Of Glaucoma In Developing Countries: Challenges And Opportunities For Improvement
Authors Delgado MF ![]() , Abdelrahman AM
, Abdelrahman AM ![]() , Terahi M, Miro Quesada Woll JJ, Gil-Carrasco F, Cook C, Benharbit M, Boisseau S, Chung E
, Terahi M, Miro Quesada Woll JJ, Gil-Carrasco F, Cook C, Benharbit M, Boisseau S, Chung E ![]() , Hadjiat Y
, Hadjiat Y ![]() , Gomes JAP
, Gomes JAP
Received 17 June 2019
Accepted for publication 3 September 2019
Published 27 September 2019 Volume 2019:11 Pages 591—604
DOI https://doi.org/10.2147/CEOR.S218277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Maria Fernanda Delgado,1 Ahmed Mostafa Abdelrahman,2 Malika Terahi,3 Juan Jose Miro Quesada Woll,4 Felix Gil-Carrasco,5 Colin Cook,6 Mohamed Benharbit,7 Sebastien Boisseau,8 Ernestine Chung,8 Yacine Hadjiat,8 José AP Gomes9
1Private Practice and Sociedad de Cirugía Ocular, Bogotá, Colombia; 2Department of Ophthalmology, Cairo University, Cairo, Egypt; 3Ophthalmology Department, CHU Nafissa Hammoud, Algiers, Algeria; 4Department of Ophthalmology, Hospital Central De Policia, Bogota, Colombia; 5Glaucoma Department, Hospital Luis Sánchez Bulnes, Asociación para Evitar la Ceguera en México I.A.P, Mexico City, Mexico; 6Division of Ophthalmology, University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa; 7Centre d’Ophtalmologie et d’Explorations Visuelles, Rabat, Morocco; 8Mundipharma Singapore Holding Pte Limited, Singapore, Singapore; 9Department of Ophthalmology and Visual Science, Federal University of São Paulo, São Paulo, Brazil
Correspondence: Yacine Hadjiat
Mundipharma Singapore Holding Pte Limited, 12 Marina View, #22-01, Asia Square Tower 2, Singapore 018961, Singapore
Tel +65 6511 1855
Fax +65 6511 1167
Email [email protected]
Abstract: Glaucoma is the leading cause of blindness in the developed and developing world. Not only is the clinical impact of this disease considerable, but associated economic and humanistic burdens – affecting patients, caregivers, and society – are substantial. Since glaucoma is an age-related disorder and populations in many developing countries are aging at a faster pace than in the developed world, increasing attention is being focused on ways to ameliorate the burdens of illness. In this paper, we examine the burdens of glaucoma with particular focus on developing countries, discuss some of the challenges that exist in delivering optimal glaucoma management within budget constraints, and bring into perspective how we could improve current healthcare systems, leverage technology, and strike an appropriate balance between cost and quality of care, thereby offering considerations to payors and policymakers in these countries that may result in longer-term cost savings, while concurrently striving to achieve the WHO Vision on the prevention of blindness and visual impairment.
Keywords: cost, quality, preservative-free, ocular surface disease, access, healthcare system, developing
Introduction
Glaucoma is the leading cause worldwide of irreversible blindness. In 2010, the projected global prevalence of primary open-angle glaucoma (POAG) and primary angle-closure glaucoma (PACG) was 60.5 million among persons aged 40+ years1 and 64.3 million among similar-aged persons in 2013.2 The former represents 2.65% of the global population over the age of 40 years in 2010.3 As the prevalence of glaucoma is known to be age-related, it is increasing in most parts of the world due to population aging.3 Remarkably, a large proportion of glaucoma cases worldwide remain undiagnosed or sub-optimally managed.4–10 This is particularly the case in many developing countries; the reasons for this are multi-factorial.
The prevalence and incidence of glaucoma in developing countries has been particularly difficult to estimate because of the scarcity of data. Broad 2010 data report the highest prevalence of POAG and ACG combined in Africa at 4.32% followed by Latin America (LATAM) at 3.35%.1 China, India and Southeast Asia had prevalence percentages between 2.38% and 2.66%.1 The LALES study4 in the United States evaluated Latin American subjects, specifically from Central America, but extrapolating results to the actual reality of LATAM countries should be done carefully. LALES reported a prevalence of open-angle glaucoma in subjects of Latino descent of 4.74%, increasing with age to 22% in subjects over age 80 years versus those between 40 and 49 years.4 That study also found that of those subjects diagnosed as having glaucoma, approximately three-quarters were unaware they had the disease.4 A 2013 publication reported an overall prevalence of 3.4% in a sample of subjects aged over 40 years in a population-based study conducted in south Brazil, although this is unlikely to be an accurate representation of the whole country.5 A recent national survey conducted in Algeria reported the prevalence of glaucoma in that country at 4.6%, approximately 380,000 to 450,000 cases at country level (Algerian Ministry of Health, 2008). Despite the limited data, a trend of higher prevalence of glaucoma can be observed particularly in Africa and LATAM,1,5 which is aligned with the well-studied African and Hispanic ancestry risk factor for glaucoma.3,4,6 This, combined with the high under-diagnosis rate of glaucoma,4 underscores a need to conduct further studies to even begin to understand the scale of this disease and its associated burden in developing countries to ensure adequate funding and strategies to improve glaucoma care.
Glaucoma prevention and treatment has been a major focus of international directives including the WHO Vision 2020 campaign.11 While this initiative has seen a decrease in worldwide blindness, most of the improvement has been due to increased use of cataract surgery, particularly in the developing world.11 It has not been from medical and pharmacologic interventions intended to treat elevated intraocular pressure (IOP) or prevent onset (or slow progression) of glaucoma symptoms or for that matter access to glaucoma care services.11
International bodies such as WHO and the World Bank have noted that in many emerging markets, populations are growing faster than those in the developed world.11,12 Moreover – and this is particularly relevant for medical conditions with an age-related component such as glaucoma – populations in many emerging markets are aging in a similar fashion as developed markets as a consequence of improvements in life expectancy.14 This poses a variety of challenges as well as opportunities for developing countries. The challenge, of course, is to find effective ways of balancing cost and affordability against access to care. The opportunity also is clear: to the extent that innovative treatments – many of which are expensive on a per-unit basis – have faced access barriers to date in many developing nations, evidence of the value of innovative treatment may afford avenues for improved patient outcomes in these markets.
With worldwide prevalence of glaucoma steadily rising along with the attendant burdens imposed by the disease, most countries – especially developing nations – remain distant from achieving the WHO Vision mission “to eliminate avoidable blindness by the year 2020”,11 a part of the Millennium Development Goals initiated by the commitment of world leaders to “build a more equitable, prosperous and safer world.”15 It therefore appears timely to consider how the management of glaucoma and one of its major complicating conditions – ocular surface disorder (OSD) – can be enhanced through increased use of innovative treatments and disease management initiatives. At the same time, understanding better the potential value proposition for increased uptake of innovative glaucoma treatments in developing countries will provide useful information to policymakers in these markets who must constantly balance cost–benefit considerations to address the healthcare needs of their constituent populations. There may also be other opportunities that remain underexplored, including reforming healthcare systems and leveraging technology to provide patients with access to glaucoma care.
Objectives And Methods
The objectives of this article are to (1) highlight what is known about the clinical, economic, and humanistic burden of glaucoma in general and as it pertains to developing world markets; (2) delineate some key considerations in the management of glaucoma in these markets; and (3) offer suggestions on how we can improve current healthcare systems and leverage technology for glaucoma management and strike an appropriate balance between cost and quality of care in developing world where access to quality care often is heavily influenced by financial considerations. In doing so, the intention is not only to bring into perspective the glaucoma care situation in developing countries but also to offer considerations to payors and policymakers in these countries that may result in longer-term cost savings, while concurrently closing the gap to achieving the WHO Vision on the prevention of blindness and visual impairment.11
A targeted (non-systematic) review of MEDLINE-indexed literature was conducted to identify pertinent literature using PubMed and the following search terms: <glaucoma>, <management>, <developing>, <emerging>, <cost>, <burden>, <ocular surface disease>, <generics>, and <cost-effectiveness>. This targeted search was supplemented by a search using the Google search engine and employing the same keywords. Relevant publications identified through these searches were evaluated by two reviewers prior to inclusion.
The Clinical, Economic, And Humanistic Burdens Of Glaucoma
Clinical Burden
The clinical burden of glaucoma in developed countries has been well described in the literature,3 but, until recently, scant attention was paid to the burden of disease in the developing world. Persons with glaucoma who live in these countries are at a particular disadvantage – studies have shown that they have a higher risk of progressing to blindness and present to the clinic with more advanced disease on average than same-aged persons with glaucoma in developed countries.6,13 It also has been noted that age-adjusted incidence of glaucoma (and glaucoma-related blindness) may be higher in developing countries for reasons not entirely clear.6,13
Exactly why persons with glaucoma in developing countries appear to be at increased risk of progressing to blindness remains a highly debated topic. The progression of vision loss with passage of time is personalized and a variety of factors may come into play. In the early stage of disease, increased IOP – if poorly controlled – leads to variable progression of vision loss with attendant decrements in health-related quality of life, greater accident risk, and reduced experience of activities of daily living, such as ability to walk, read, or drive an automobile.3,16–18
Economic Burden
The direct medical and non-medical costs of glaucoma are known to be meaningful3 from a global and developed-country standpoint. The magnitude of these costs in the developing world and emerging markets has been poorly documented to date. Calculations based on data from the 1990s and 2000s suggest that per-patient direct costs (adjusted to reflect 2017 prices) range from approximately AUD500 (approximately USD346) in Australia to more than USD1800 in the USA.3,19,20 One would not anticipate per-patient costs in developing world markets to be as high as in the USA after adjusting for cross-market differences in relative prices. A recent prospective study conducted in Mexico City suggests that direct medical costs of glaucoma treatment are in the range of USD450–550 annually following adjustments to reflect 2017 prices, irrespective of patient income and disease severity.21 This appears to be similar even in a country like Nigeria where the direct cost of antiglaucoma medication was estimated at USD480 annually.22 As glaucoma prevalence increases with population growth and aging, however, total direct costs of glaucoma will tend to increase more than proportionately in nominal terms due to the additive effects of price inflation.
The financial burden of glaucoma tends to increase as disease severity increases.3,20,21 Late-stage disease is associated with higher indirect costs (eg, work loss, family/home help and rehabilitation costs) that become the predominant driver of overall costs.23,24 In Europe, the average annual direct medical cost of glaucoma-related blindness has been estimated to be €429–€523 per patient while annual total costs, including the indirect cost components noted above, were estimated to be between €11,758 and €19,111.23 In 2005, the annual direct medical costs of individuals with late-stage glaucoma averaged €830 per patient across France, Denmark, Germany, and the United Kingdom.24 In contrast, the largest contributor to total annual maintenance costs was assistance in the home, a form of indirect cost, which was estimated to range from €633 in Germany to €4878 in France.
The indirect cost of late-stage glaucoma in developing countries remains unclear. A Nigerian study indicates that the indirect medical cost of glaucoma which includes medical tests, transportation and care by patient escorts averaged at USD1264.80 per annum – disease stage was not specified.22 Nevertheless, the cost of treatment/hospitalization cost because of accidents arising from vision loss and work loss (indirect cost impacts that are independent of socioeconomic status) should not be underestimated. In Nigeria, Rivers State – a region with fewer cases of glaucoma-related blindness in the country – the estimated additional direct and indirect cost to the economy was USD3,064,587 per annum from patients already blind.22
Humanistic Burden
As noted previously, glaucoma adversely affects patients’ health-related quality of life (HRQoL) in multiple ways.3 Psychological burden increases as vision decreases, along with a growing fear of blindness, anxiety, and depression.25–27 On a quality of life scale from 0 to 1, where 0 represents death and 1 represents perfect health, a mean utility value of 0.64 was reported in an Indian population with glaucoma, much lower than the scores reported in similar studies in Americans with glaucoma, and even lower than those reported in a study conducted in Brazil (0.82–0.93).28–30 This suggests that patients in developing countries may feel a stronger impact on their quality of life when they suffer from glaucoma.
Access To Eye Care Medical Facilities
A Brazilian publication flagged delays in glaucoma diagnosis as a challenge in developing countries,5 and this is more so in these resource-challenged nations (diagnosis rate of POAG: 8%) than in developed countries (diagnosis rate of POAG: 34%).1 The resultant impact is evident as highlighted by a Nigerian survey reporting that most of their patients have moderate or severe disease at presentation.31 This observation is not unique to Nigeria – visual impairment has been reported to be more prevalent and severe in developing countries,32 and this has a cascade impact on things such as productivity and care cost.22 Diagnosis and even monitoring can be a more complicated issue in developing nations due to limited access to eye care medical facilities; reasons include (but are not limited to) distance or travel cost to an adequate eye care facility or cost of treatment.5,21,22,31
It is therefore logical that early detection and optimal management of glaucoma is a means to prevent blindness and reduce clinical, economic and humanistic burdens related to this disease in developing countries. To do this, improving patient access to good quality eye care facilities is a critical step and this will require close partnership of key stakeholders including payors, policymakers, clinicians and allied healthcare professionals.
Integrating Primary Care And Technology In Eye Care
Primary care physicians are well positioned to play a role in the prevention and management of glaucoma including screening, patient education and treatment of non-complex diseases.33 Their relationship with their patients allows basic monitoring and quick referrals to the eye specialists as needed.33,34 They also have the potential to influence patient behavior such as treatment compliance.33
A primary healthcare approach to address access issues with eye care has been recommended by the WHO in 1984.34 Nevertheless, a review of the literature suggests that the integration of primary care into glaucoma management in developing countries appears relatively far from it. The key barriers observed include the lack of knowledge on the diagnosis and management of glaucoma, or of the disease itself; a fragile, fragmented and/or under-resourced healthcare system; and availability of eye care services.5,34–38
Education of primary care physicians and allied health workers appears to be an important step in their integration to glaucoma care. The effectiveness of cascade training by tertiary Centres of Excellence/specialists has been well supported in India and the sub-Saharan Africa in general ophthalmology and other fields, respectively – it is important to maintain this to ensure quality care.34,35 To ensure functional and sustainable integration, it is also critical to select tasks that can be most appropriately managed in a primary care setting and to have competent and reasonably well-equipped glaucoma specialists/eye care centres to receive referrals.34,35 Task sharing by enabling a general healthcare personnel with the appropriate skills and training also can help to ease the workload in an under-resourced environment, such as the “Vision Guardians” – trained local volunteers from villages in India who supported with activities like patient education and organization of community screening programmes.34,35
With the increasing use of mobile devices and advancements in technology, telemedicine has started to gain traction in recent years.38 Tele-glaucoma is an approach to disease management that could bring enhanced patient access to glaucoma screening, detection and follow-up care by utilizing technology.38–40 This may be pertinent to developing countries as technology can potentially reduce the cost of healthcare and perhaps support the achievement of the wider goal of reducing the burden arising from high numbers of patients with late-stage glaucoma.
There are two main tele-glaucoma modalities.39 The first is the “store and forward” telemedicine where relevant diagnostic data are collected from the patients by the screening team (eg, trained technicians) and sent via encrypted internet connection to a clinician or specialist located remotely from the testing site for analysis.39 The other model is via telepresence, where diagnostic data are collected in a similar manner, but a specialist provides live/real-time consultations via an online platform.39
There has been an increase in development in the field of tele-glaucoma with the recording of IOP via home devices or a temporary sensor on the eye that connects to smartphones, or the use of smartphones to photograph images of the retina which potentially removes the need to put in place more expensive machines for such diagnostic tests in satellite clinics in the primary care setting.38,40 A review of 45 studies on tele-glaucoma indicates that it offers early detection of glaucoma, reduction in waiting and travel times, increased referral rates and ultimately cost savings which benefit both patients and the healthcare system.41
Telemedicine has been identified as a critical piece to support the healthcare system in India.42 The mobile-Health services (m-Health) is a system owned by the Indian government.42 It provides 24-hr service at less than $1 per consultation.42 A paramedical staff equipped with laptops, high-speed wireless connection, and medical diagnostic equipment consult with physicians using video conferencing and provide guidance to mobile users.42 Important success factors for m-Health include the level of wireless data technology adoption in India, robust devices and service ecosystems and the partnership of telecom ecosystem contributors.42 While this system appears more appropriate for basic medical guidance, it underscores the possibilities of using technology in glaucoma management in a developing country.42
Do Current Healthcare Systems Need Reform?
The importance of having a strong healthcare system as a foundation for thriving initiatives was highlighted by a quote from His Highness the Aga Khan in Mozambique in 2010 that “an enabling environment is a setting where additional development initiatives can take root and thrive.”43 Primary care integration and telemedicine can only take root and thrive with a strong and well-set-up healthcare system. Damji underscores several critical elements to create an enabling environment, such as good quality leadership and governance, and an optimal teaching and learning environment which was previously discussed.43 Of interest was the discussion on the role of healthcare systems where the critical need to structure the system for long-term success was highlighted amongst other things.43 This brings to question if current healthcare systems in developing countries are well set-up to prevent blindness or disease progression from glaucoma. The continuously increasing burdens of glaucoma suggest room for improvement. Perhaps, the customization of successful healthcare systems in eye care may be considered.
The LV Prasad Eye Institute (LVPEI) of India’s five-tier pyramidal model of eye care delivery is an excellent example of a high-quality, comprehensive system that is equitable and sustainable with an aim to fulfil the WHO Vision 2020.35 It encompasses all levels of care from primary to advanced tertiary and services are interlinked. Figure 1 illustrates the structure and accompanying services of the model. The system covers health promotion, prevention, treatment, and rehabilitation.35 The critical aspect of this model is the commitment that everyone received the care they require irrespective of complexity and cost.35 The big question thus lies in sustainability particularly in finance and human resource. Table 1 shows the points that make this system sustainable.
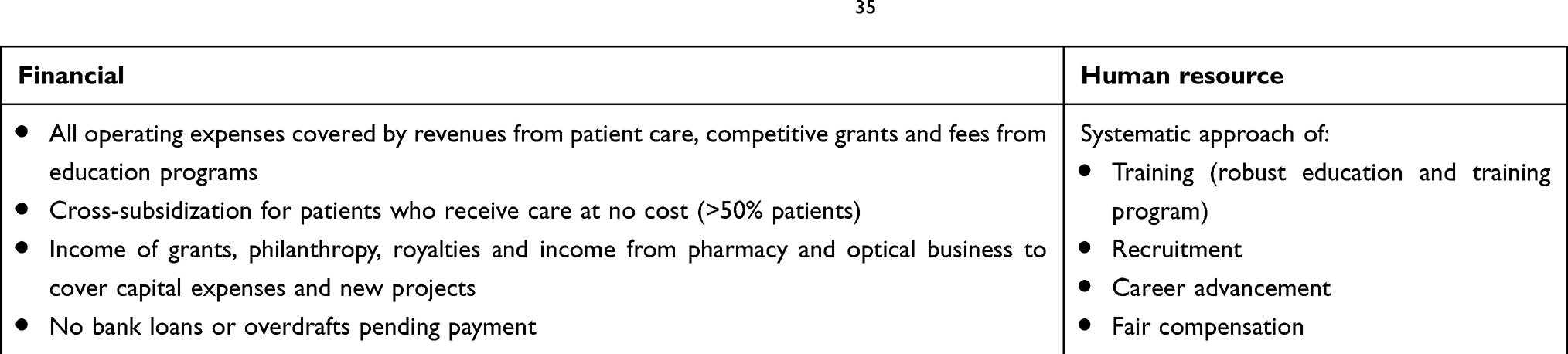 |
Table 1 Financial and human resource sustainability of the LVPEI model35 |
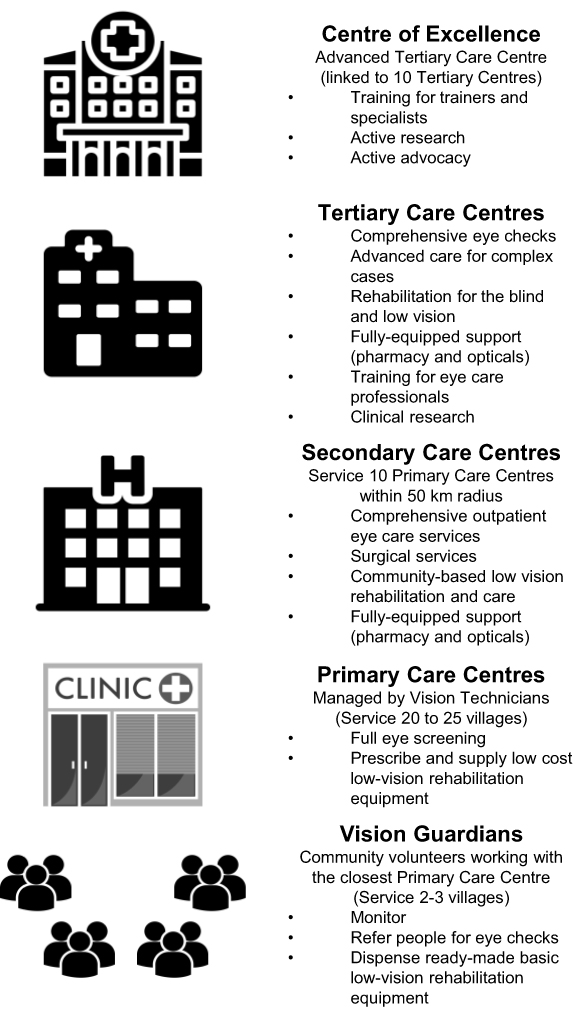 |
Figure 1 LV Prasad Eye Institute’s model of eye care delivery. |
It is clear that there is still a journey for many developing countries to optimize their glaucoma care, starting from the integration of primary care to reforming the healthcare system. Further, it is pertinent for stakeholders and decision-makers to understand that some level of financial investment will be needed to ensure appropriate infrastructure, equipment, equipment maintenance, supplies and/or technology to maintain quality of care for any new initiative.34 There are numerous considerations and variations in healthcare systems between countries. Nevertheless, the implementation of any or a combination of the discussed approaches customized to individual countries may ultimately result in a cost-effective solution with a positive impact on the economic burden in the long term.
Optimizing Glaucoma Management
Ensuring that patients receive the optimal management for their disease without increasing the indirect costs is also a critical consideration. In countries such as Africa, patients are sometimes offered surgery as a first line of treatment before eye drops due to the cost of glaucoma drugs and low compliance with medication.44 However, post-surgical follow-ups and post-surgical complications can result in more indirect costs.4 It is therefore important to look at how glaucoma management administered through eye drops can be optimized.
There is a paucity of publications focused on developing countries exploring the optimization of glaucoma management through eye drops such as glaucoma treatment–related OSD and addressing it or any adverse effects that arise due to poor quality control of medications. Nevertheless, such issues faced by patients are generic regardless of socioeconomic status when they use antiglaucoma medications. Therefore, it is still relevant to look at the following areas using published information from developed countries but putting it into context for developing nations.
OSD And Its Management In Glaucoma Patients
The prevalence of OSD varies depending on the test used for evaluation and has been reported to range between 22% and 78% of patients with medically treated glaucoma as compared with approximately 15% of the general population aged 65 years and older in western populations.46,47 The incidence and prevalence of OSD, much like that of glaucoma, is poorly delineated from a population standpoint in the developing world. Nevertheless, studies from Brazil47 and Thailand48 on patients with glaucoma show a prevalence of approximately 38% to 73% using various measures of OSD – a pattern similar to that in western populations (developed countries). Studies have shown that the prevalence increases with increasing number of eye drops per day or antiglaucoma medications, the latter reported in Thailand48 and Germany,49 respectively, further highlighting that the issues of OSD faced once patients receive antiglaucoma medications are not subjected to economic development. However, it may be suggested that the prevalence of OSD in developing countries could be higher due to the lack of access to glaucoma medications and eye care facilities in general.5,21,22,31 As such, the observation in the United States that most glaucoma patients with moderate-to-severe OSD were not diagnosed and did not receive treatment for their disease despite being in a developed country50 is notable and suggests that OSD in glaucoma patients tends to be under-recognized and under-diagnosed potentially due to clinical focus on IOP management and evidence of glaucoma progression. Short-term use of topical glaucoma medications – even in healthy persons – has been shown to be associated with changes in ocular surface such as reduced corneal sensitivity, tear film stability, and basal secretion.51 Evidence further suggests that prolonged use of many topical glaucoma medications leads to further incremental deterioration of the ocular surface in patients with established OSD.52
Compounding the issue of OSD in many glaucoma patients is the occurrence of dry eye disease (DED). Many commonly used medications, including several that are known to be secreted into the tear film, contribute to DED.53 The co-incidence of DED with OSD is known to exacerbate OSD symptoms and complicate its management.53 It is important, therefore, to recognize that the severity of OSD symptoms can have a potentially important iatrogenic component and that appropriate glaucoma management involves consideration of factors such as DED that may further complicate the clinical picture.
Studies conducted over the last 25 years have noted an increased incidence of OSD and ocular surface changes among persons living or working in metropolitan areas with elevated levels of airborne environmental pollutants (including traffic-dense areas) or in poorly ventilated buildings.54–57 Whether this, taken together with the well-documented elevated levels of airborne pollutants in many metropolitan areas within developing nations,56 contributes to increased incidence and greater severity of OSD in these areas is not entirely clear and certainly worthy of further investigation.
The development of OSD in glaucoma patients has been shown to have an additive negative impact on HRQoL apart from that of the underlying glaucoma or its progression.58,59 Risk of developing OSD is known to increase from exposure to benzalkonium chloride (BAK) and other preservatives used in the formulation of many topical glaucoma treatments.58 Using OSD Index for measuring symptoms of dry eye, 59% of patients using drugs containing preservatives reported symptoms in at least 1 eye, with severe symptoms reported by 27%; Schirmer testing showed 61% of patients with decrease in tear production in at least one eye and severe tear deficiency in 35% of patients.45 In a study, after adjustment for age and sex, each additional BAK-containing eye drop was associated with an approximately two-times increased odds of showing abnormal results, and the prevalence of signs and symptoms was dose-dependent, increasing with the number of preserved eye drops.45 BAK-containing eye drops were also shown to be associated with increased levels of proinflammatory and proapoptotic effects on conjunctival cells versus non-preserved medications.60
As in all pharmacologic management of chronic disease, the need to weigh risks of drug exposure against the benefits of treatment is necessary. In the minds of some clinicians, the benefits of IOP reduction and the potential slowing of glaucoma progression justify the use of drugs that are known to increase the risk of ocular surface complications or to worsen established OSD pathology. Others may be more concerned with managing the risks and, as such, may be willing to trade off some measure of efficacy in favor of fewer treatment-related adverse events. In this regard, it is important to note that pharmacologic treatment of OSD can further complicate glaucoma management. For example, while the use of calcineurin phosphate inhibitors to treat symptoms of OSD and reverse tear film breakup is common in the developed world, it is far less so in developing countries due to cost factors. In several regions of the world, preservative-containing steroid drops continue to be employed frequently. While ocular steroids are invaluable in the treatment of conditions such as anterior uveitis as a means of suppressing inflammation and immunoresponse, the role of steroid drops in deregulating IOP – which may worsen the underlying glaucoma and defeat the intended effects of treatment – has been noted on multiple occasions.61 A variety of visual disturbances ranging from blurred vision to haloing and tunnel vision have been noted with steroid-induced glaucoma.61
The need to manage OSD adds further to the already meaningful economic burden of glaucoma. There may be considerable savings from avoidance or prevention of OSD and related symptoms in the developing world and emerging markets, particularly when one also considers the possible exacerbating effect of exposure to environmental toxins and pollutants which already may place patients at increased risk of OSD. There is also some evidence that better control of IOP can be achieved in patients with poorly controlled glaucoma and severe OSD when appropriate and efficient treatment of the OSD is undertaken.60 Of note, treatment options are available that can significantly reduce OSD-related symptoms and even prevent the onset of ocular surface impairment without compromising IOP reduction.
Generics In The Treatment Of Glaucoma
There is no question that the spike in the availability of generic formulations of many drugs used in the management of glaucoma has improved access to care worldwide due to greater affordability. What often is under-appreciated, however, is that expanded use of drugs in general – and of generics in particular – carries risks as well as benefits. Drugs are not benign, and even in the best of circumstances, side effects and treatment-related adverse events are possible. If the deleterious effects are severe enough to require treatment, that treatment comes with incremental cost and its own risks. Those who consider only the cost of medication in assessing affordability and its implication for access to care run the risk of ignoring the burdens created by side effects, inappropriate use, and other factors.
This is particularly relevant in any discussion of pharmacologic management of glaucoma, as the prevalence of use of generic medications has skyrocketed in recent years due to many patent expirations. Many factors affect the efficacy of a topical glaucoma medication apart from the ingredients inside the container.63 Among these are:
- Bottle material, shape, and size
- Drop size (which can affect dosing and patient adherence)
- Exposure to heat
- Changes in containers due to multi-sourcing of generic medications
The ingredients of many branded medications are matched to the bottle material being used as a means of ensuring stability, reducing the risk of agglomeration or adhesion of active ingredient to the container, and the like.63–65 Bottle shape and size can present issues as well, particularly to the extent that this is unregulated in most markets worldwide.63–65 When a generic is prescribed, a patient may receive his/her medication in a different-shaped bottle with each refill prescription and thus may face ease-of-use issues in administering the drug.63–65 Concerns over ease of use may be even greater in elderly than in non-elderly patients because of potential limitations in dexterity.63,64
Drop size coming out of the container is an obvious potential hazard because of the attendant risk of under- or over-dosing. In the USA, for example, branded formulations of many glaucoma medications deliver a drop size ranging from 30 to 50 μL.63 But in markets where containers are poorly regulated, the drop size can vary based on differences in the container’s tip.63–65 It was reported that a new generic formulation of timolol required patients to pierce the tip to create a hole.63 Some patients did not understand the need to do this and thought they were administering drugs but were not.63 Moreover, the need for patients to pierce the tip themselves raised the possibility of contamination of contents as well as variability in the size of opening created.63–65 Aside from the concerns noted above and how they may adversely affect drug effectiveness and safety, variations in drop size obviously also affect the rate at which medication is consumed and thus may have unintended cost consequences.
Quality control among manufacturers of generic medications also has been a major concern and has been widely reported in the world press. Problems ranging from variations in active ingredient content versus label to impurities found in the drugs, imperfect ingredient matching, and fraudulent formulations have been reported.63–65 The excipients used in formulating generic drugs differ from those employed in the manufacture of the branded counterparts and this can affect bioavailability and potentially safety.61–63
These issues and others with generic formulations may lead to unintended adverse consequences.65 Unlike for generic formulations of drugs in most therapeutic areas, regulatory bodies do not require clinical studies demonstrating bioequivalence or comparable pharmacokinetic profile to branded products to support approval or marketing authorization of generic ophthalmologics.65 Even in markets such as the USA, where Good Manufacturing Practice (GMP) standards apply to marketed generic drugs, issues can occur. A case report from the USA described a glaucoma patient who experienced a 10-point increase in IOP following a switch from a branded formulation to the generic equivalent.66 Once the patient was switched back to the branded formulation, the IOP reverted to the baseline level.66
Uncertainty regarding the consistency of quality, efficacy, and safety of generic ophthalmologics should compel policymakers – particularly in extremely cost-conscious developing countries – to consider more carefully the risk versus benefits of generics use. In a study in India conducted by Banga and colleagues,67 of 245 bottles evaluated, only 86 (35.1%) had the correct amount of the drug; seven bottles (2.86%) were overfilled and the remaining 152 bottles (62.04%) were underfilled. The drop size of all bottles varied from 29.4 to 67.47 μL.67 What are the implications of such variation to the patients prescribed these medications? A drug that is cheaper than another may not be cheaper in the long run if its use leads to comparatively more complications, loss of efficacy, or safety issues requiring medical intervention and treatment. In the ideal, a better understanding of these issues will spur more cogent thinking about the full cost implications of using generics in place of branded products, even while keeping in mind the need to balance affordability with access.
Strategies For Improving Quality Of Glaucoma Care At An Affordable Cost
There is a plethora of agents, both branded and generic, available for the clinician’s use in managing glaucoma and associated complications such as OSD. And, as discussed previously in this paper, innovative strategies such as teleglaucoma management are becoming more widely available. These agents and modalities vary considerably in their ingredient cost, safety profiles, efficacy, accessibility, and ease of use. In any individual case, there will be considerations regarding indication or contraindication for one drug versus another. Nonetheless, the reality for many patients with glaucoma – particularly those on the more severe end of the spectrum where the risk of progression to major visual impairment or blindness is significant – is that multiple pharmacologic agents are required to achieve acceptable disease management. Anytime polypharmacy is required to manage a disease, this should raise concerns over potential drug–drug interaction, cumulative safety considerations, and the like. Indeed, in the treatment of glaucoma, the use of multiple agents containing BAK or similar preservatives has been shown to contribute to cumulative ocular surface changes, cumulative risk of OSD, and increased OSD severity.58
Cost-effective treatment of any medical condition requires a careful balance between efficacy, safety, patient tolerability/acceptability and adherence, quality of life considerations, and net system cost.68 Many newer therapies offer one or more of these clinical and humanistic benefits – but can these benefits be achieved at a reasonable cost? In the case of glaucoma, the current opinion suggests that the treatment goal should be to improve efficacy and tolerability with (1) fewer systemic side effects; (2) less dosing complexity; and (3) fewer daily drops to drive patient compliance – all at a reasonable cost.68
Taking these various factors into consideration individually, there is little doubt as to what would constitute an appropriate goal for treatment efficacy: the goal should be significant, sustained IOP reduction.68 In terms of safety and tolerability, the goal is also fairly clear: avoidance of ocular surface complications and adverse visual changes, which have been shown to have a significant negative impact on quality of life, tolerability, and patient compliance.68,69 The issue of dosing complexity is a very real concern that is often given scant attention even in the developed world. As noted earlier, polypharmacy can lead to clinical complications, but it also creates a disease management conundrum – especially in glaucoma patients due to the age-related prevalence of the disease. Finding ways to reduce the drug administration burden for glaucoma patients is key to driving improvements in compliance and adherence to prescribed therapy.68–70 Associated with this is a reduction in the total number of drops a patient may require in managing his/her condition – also critical to driving compliance and adherence.68 But this is not always a straightforward exercise. For example, in some developing markets, it has been noted that pharmacies often produce combinations of individually marketed generic medications through compounding, as a means of reducing the administration burden on the patient. While this sounds interesting in theory, it should be noted that any compounded combination created is only as efficacious and safe as the individual ingredients employed. The same caution and concerns should be applied, therefore, to compounded generics as to the individual ingredients themselves.
In recent years, several manufacturers have introduced new agents that not only offer additive clinical efficacy but are formulated without preservatives, thus mitigating risks associated with ocular surface changes. Some of these, such as prostaglandin analogues, represented entirely new classes of drugs with a different mechanism of action from existing treatment options. Some prostaglandin analogues, such as tafluprost, were introduced de novo with preservative-free formulation. More recently, some manufacturers have introduced preservative-free formulations of drugs that have been available for many years, such as latanoprost. Removal of preservatives from glaucoma drugs offers clear benefit associated with reduction of risk (and therefore cost associated with treatment) of ocular surface changes and OSD, both of which also are implicated as contributors to decrements in quality of life in a substantial portion of the population of patients with glaucoma.
As one example, the fixed-dose combination of dorzolamide and timolol, historically marketed in a BAK-containing formulation, has been reformulated without preservatives71 by two manufacturers and is in the process of being introduced in selected markets worldwide. Evidence gleaned from both clinical trials and real-world studies long has suggested that this fixed-dose combination offers important clinical benefits which compare favorably to other treatment options in terms of sustained IOP reduction, long-term IOP control, and patient tolerability.71–87 Future availability of preservative-free formulations in developing world may offer important advantages that weigh favorably in the cost/benefit and cost/effectiveness calculus.
Even within existing drug classes, there are clear options for optimizing the balance between efficacy, safety, tolerability, potential quality concerns, impact on patient quality of life, and cost. Among prostaglandin analogues, for example, tafluprost provides efficacy in IOP lowering in various settings, with improvements in OSD symptoms and patient satisfaction when compared with latanoprost.88–98 Travoprost and tafluprost monotherapies were suggested to be cost-effective relative to latanoprost alone.99,100 However, such drug–drug cost-effectiveness or budget impact studies are limited in developing countries. Moreover, indirect costs should also be considered to understand the true impact of a management strategy. The disparity between healthcare reimbursement systems between countries underscores the urgent need to conduct such analyses tailored to each country to better inform payors and policymakers.
Conclusion
Striking the appropriate balance among often conflicting goals and objectives is never easy or straightforward. The challenge exists in all markets, but of course with more resources available to devote to healthcare spending, the developed world has a somewhat easier task in addressing these needs as compared with the developing countries. In recent years, the WHO has promoted the use of community health workers as part of interdisciplinary health teams in an attempt to enhance access to affordable healthcare in resource-challenged countries.101 Such programmes offer real potential to expand access to glaucoma screening and treatment, but shortages of qualified workers, amongst others, have posed issues in the implementation of such programmes in many regions that could benefit from them. The potential use of telemedicine, though underexplored in developing countries, could potentially help to address some of the issues that were highlighted in this article.
Adding to the complexity in many developing markets is population growth, which can introduce another dimension to the problem in developing markets – for example, how much do governments and society spend on diseases of the elderly, such as glaucoma, versus, say, broad immunization schemes to prevent common diseases of childhood, or universal screening for common disorders. In Brazil, the government has screening programmes for the detection of systemic hypertension and diabetes (as two examples) and may offer free medication to those who screen positive.5 Such government programmes should be considered for glaucoma screening despite cost, access, and disease-related challenges in the screening of this disease. This will allow for early diagnosis and management before the progression to late-stage disease, the latter of which comes with the significant overall cost to the country’s economy.22
The above challenges reinforce the imperative of seeking efficiency in treatment – gaining the maximum clinical benefit possible when treating a given disease for the expenditures required – what appears to be more achievable in the near future. As this article has endeavored to illustrate, the naïve perspective focused solely on drug or intervention cost is insufficient to achieve the appropriate balance between clinical, economic, and humanistic objectives. Net system cost always should be considered if the true goal is to enhance cost-efficiency in glaucoma care – or any healthcare – delivery. Fortunately, there appear to be options in the management of glaucoma that offer a real potential for achieving a better balance of these important objectives.
Acknowledgment
The authors acknowledge the invaluable contribution made by Mason W. Russell of IBM Watson Health, Cambridge, MA, USA for his assistance in medical writing and project management. Funding for medical writing was provided by Mundipharma Singapore Holding Pte Ltd., Singapore.
Disclosure
Dr Maria Fernanda Delgado reports personal fees from Mundipharma, personal fees from Allergan, personal fees from Iridex, personal fees from Sophia, outside the submitted work; Dr Mohamed Benharbit reports personal fees from Jamjoom Pharma (AAO Chicago 2016), Mundipharma (WGC Helsinki 2017), ESCRS Lisbon 2017 THEA, SFO 2018 THEA, CGS Montreal 2018 THEA, nothing from ALLERGAN, outside the submitted work. Dr Sebastien Boisseau, Dr Ernestine Chung and Dr Yacine Hadjiat are employees of Mundipharma. Prof. Dr. José AP Gomes reports grants, personal fees, non-financial support from Allergan, grants, personal fees, non-financial support from Alcon, personal fees, non-financial support from Genon, grants, personal fees, non-financial support from Mundipharma, grants, personal fees, non-financial support from Shire, grants, personal fees, non-financial support from Thea, grants, personal fees, non-financial support from Ofta, grants from Fapesp, grants from Cnpq, grants from Capes, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90:262–267. doi:10.1136/bjo.2005.081224
2. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
3. Varma R, Lee PP, Goldberg I, Kotak S. An assessment of the health and economic burdens of glaucoma. Am J Ophthalmol. 2011;152(4):515–522. doi:10.1016/j.ajo.2011.06.004
4. Varma R, Ying-Lai M, Francis BA, et al. Prevalence of open-angle glaucoma and ocular hypertension in Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004;111(8):1439–1448. doi:10.1016/j.ophtha.2004.01.025
5. Leite MT, Sakata LM, Medeiros FA. Managing glaucoma in developing countries. Arq Bras Oftalmal. 2011;74(2):83–84. doi:10.1590/S0004-27492011000200001
6. Chen PP. Risk and risk factors for blindness from glaucoma. Curr Opin Ophthalmol. 2004;15(2):107–111. doi:10.1097/00055735-200404000-00009
7. de Voogd S, Ikram MK, Wolfs RC, et al. Incidence of open-angle glaucoma in a general elderly population: the Rotterdam Study. Ophthalmology. 2005;112(9):1487–1493. doi:10.1016/j.ophtha.2005.04.018
8. Tielsch JM, Sommer A, Katz J, et al. Racial variations in the prevalence of primary open-angle glaucoma. The Baltimore Eye Survey. JAMA. 1991;266(3):369–374. doi:10.1001/jama.1991.03470030069026
9. Quigley HA, West SK, Rodriguez J, et al. The prevalence of glaucoma in a population-based study of Hispanic subjects: proyecto VER. Arch Ophthalmol. 2001;119(12):1819–1826. doi:10.1001/archopht.119.12.1819
10. Mitchell P, Smith W, Attebo K, Healey PR. Prevalence of open-angle glaucoma in Australia. The Blue Mountains Eye Study. Ophthalmology. 1996;103(1):1661–1669. doi:10.1016/S0161-6420(96)30449-1
11. World Health Organization. Vision 2020: The Right to Sight. Action Plan 2006–2011. Geneva: World Health Organization; 2006.
12. International Finance Corporation, World Bank Group. Private Healthcare in Emerging Markets: An Investor’s Perspective. Washington, DC: World Bank Group;2015.
13. Omoti AE, Osahon AI, Waziri-Erameh MJ. Pattern of presentation of primary open-angle glaucoma in Benin City, Nigeria. Trop Doct. 2006;36(2):97–100. doi:10.1258/004947506776593323
14. Shetty P. Grey matter: aging in developing countries. Lancet. 2012;379:1285–1287. doi:10.1016/S0140-6736(12)60541-8
15. Faal H. Millennium development goals and eye health. Indian J Ophthalmol. 2012;60:411–415. doi:10.4103/0301-4738.100538
16. McKean-Cowdin R, Varma R, Wu J, Hays RD, Azen SP. Severity of visual field loss and health-related quality of life. Am J Ophthalmol. 2007;143(6):1013–1023. doi:10.1016/j.ajo.2007.02.022
17. McKean-Cowdin R, Wang Y, Wu J, Azen SP, Varma R. Impact of visual field loss on health-related quality of life in glaucoma: the Los Angeles Latino Eye Study. Ophthalmology. 2008;115(6):941–948. doi:10.1016/j.ophtha.2007.08.037
18. Haymes SA, Leblanc RP, Nicolela MT, Chiasson LA, Chauhan BC. Risk of falls and motor vehicle collisions in glaucoma. Invest Ophthalmol Vis Sci. 2007;48(3):1149–1155. doi:10.1167/iovs.06-0886
19. Rein DB, Zhang P, Wirth KE, et al. The economic burden of major adult visual disorders in the United States. Arch Ophthalmol. 2006;124(12):1754–1760. doi:10.1001/archopht.124.12.1754
20. Taylor HR, Pezzullo ML, Keeffe JE. The economic impact and cost of visual impairment in Australia. Br J Ophthalmol. 2006;90(3):272–275. doi:10.1136/bjo.2005.080986
21. Lazcano-Gomez G, Ramos-Cadena M, Torres-Tamayo M, et al. Cost of glaucoma treatment in a developing country over a 5-year period. Medicine. 2016;95(47):1–5. doi:10.1097/MD.0000000000005341
22. Adio AO, Onua AA. Economic burden of glaucoma in Rivers State, Nigeria. Clin Ophthalmol. 2012;6:2023–2031. doi:10.2147/OPTH.S37145
23. Poulsen PB, Buchholz P, Walt JG, Christensen TL, Thygesen J. Cost-analysis of glaucoma-related blindness in Europe. Int Congress Ser. 2005;1282:262–266. doi:10.1016/j.ics.2005.05.091
24. Thygesen J, Aagren M, Arnavielle S, et al. Late-stage, primary open-angle glaucoma in Europe: social and health care maintenance costs and quality of life of patients from 4 countries. Curr Med Res Opin. 2008;24(6):1763–1770. doi:10.1185/03007990802111068
25. Mabuchi F, Yoshimura K, Kashiwagi K, et al. High prevalence of anxiety and depression in patients with primary open-angle glaucoma. J Glaucoma. 2008;17(7):552–557. doi:10.1097/IJG.0b013e31816299d4
26. Zhang X, Olson DJ, Le P, Lin F-C, Fleischman D, Davis RM. The association between glaucoma, anxiety, and depression in a large population. Am J Ophthalmol. 2017;183:37–41. doi:10.1016/j.ajo.2017.07.021
27. Caceres V. Managing fear and depression in glaucoma patients. American Society of Cataract and Refractive Surgery EyeWorld. 2012. Available from: https://www.eyeworld.org/article-managing-fear-and-depression.
28. Moore D, West J. Glaucoma in the developing world. American Academy of Ophthalmology EyeWiki; 2019. Available from: http://eyewiki.aao.org/Glaucoma_in_the_Developing_World.
29. Gupta V, Srinivasan G, Mei SS, et al. Utility values among glaucoma patients: an impact on the quality of life. Br J Ophthalmol. 2005;89:1241–1244. doi:10.1136/bjo.2005.068858
30. Palleta Guedes RA, Palleta Guedes VM, Freitas SM, et al. Utility values for glaucoma in Brazil and their correlation with visual function. Clin Ophthalmol. 2014;8:529–535. doi:10.2147/OPTH.S60105
31. Adekoya BJ, Adepoju FG, Moshood KF, et al. Challenges in the management of glaucoma in a developing country; a qualitative study of providers’ perspectives. Niger J Med. 2015;24:315–322.
32. Thomas R. Glaucoma in developing countries. Indian J Ophthalmol. 2012;60:446–450. doi:10.4103/0301-4738.100546
33. Rotshtein A, Karkabi K, Geyer O, et al. Primary care physicians’ role perception and self-reported performance in glaucoma care: a survey study. BMC Res Notes. 2015;8:776. doi:10.1186/s13104-015-1770-z
34. Du Toit R, Faal HB, Etya’ale D, et al. Evidence for integrating eye health into primary health care in Africa: a health systems strengthening approach. BMC Health Serv Res. 2013;13:102. doi:10.1186/1472-6963-13-102
35. Rao GN. The Barrie Jones Lecture—eye care for the neglected population: challenges and solutions. Eye (Lond). 2015;29:30–45. doi:10.1038/eye.2014.239
36. Yan X, Liu T, Gruber L, et al. Attitudes of physicians, patients, and village health workers toward glaucoma and diabetic retinopathy in rural China: a focus group study. Arch Ophthalmol. 2012;130:761–770. doi:10.1001/archophthalmol.2012.145
37. Onabolu OO, Bodunde OT. Awareness and knowledge of glaucoma among primary care givers in a developing country. Ann Trop Med Public Health. 2014;7:5–8. doi:10.4103/1755-6783.144997
38. Mohammadpour M, Heidari Z, Mirghorbani M, et al. Smartphones, tele-ophthalmology, and VISION 2020. Int J Ophthalmol. 2017;10:1909–1918.
39. Ooms A, Khoury AS, Szirth B. Teleglaucoma. Am Acad Ophthalmol. 2018. Available from: http://eyewiki.aao.org/Tele-Glaucoma. Accessed August 4, 2019.
40. Rani PK, Nangia V, Murthy KR, Khanna RC, Das T. Community care for diabetic retinopathy and glaucoma in India: a panel discussion. Indian J Ophthalmol. 2018;66(7):916–920. doi:10.4103/ijo.IJO_910_17
41. Thomas SM, Jeyaraman MM, Hodge WG, et al. The effectiveness of teleglaucoma versus in-patient examination for glaucoma screening: a systematic review and meta-analysis. PLoS One. 2014;9:e113779. doi:10.1371/journal.pone.0113779
42. Kappal R, Mehndiratta A, Anandaraj P, et al. Current impact, future prospects and implications of mobile healthcare in India. Cent Asian J Glob Health. 2014;3:116.
43. Damji KF. Strengthening institutional capacity for glaucoma care in sub-Saharan Africa. Middle East Afr J Ophthalmol. 2013;20:107–110. doi:10.4103/0974-9233.110601
44. Ramchandani M. Glaucoma in the developing world. Comment on: effect of beta radiation on success of glaucoma drainage surgery in South Africa: randomised controlled trial. [BMJ. 2006]. BMJ. 2006;333:932. doi:10.1136/bmj.39016.626771.80
45. Leung EW, Medeiros FA, Weinreb RN. Prevalence of ocular surface disease in glaucoma patients. J Glaucoma. 2008;17:350–355. doi:10.1097/IJG.0b013e31815c5f4f
46. Schein OD, Munuz B, Tielsch JM, et al. Prevalence of dry eye among the elderly. Am J Ophthalmol. 1997;124(6):723–728. doi:10.1016/S0002-9394(14)71688-5
47. Costa VP, Marcon IM, Galvão Filho RP, Malta RFS. The prevalence of ocular surface complaints in Brazilian paients with glaucoma or ocular hypertension. Arq Bras Oftalmol. 2013;76(4):221–225. doi:10.1590/S0004-27492013000400006
48. Ruangvaravate N, Prabhasawat P, Vachirasakchai V, Tantimala R. High prevalence of ocular surface disease among glaucoma patients in Thailand. J Ocul Pharmacol Ther. 2018;34(5):387–394. doi:10.1089/jop.2017.0104
49. Erb C, Gast U, Schremmer D. German register for glaucoma patients with dry eye. I. Basic outcome with respect to dry eye. Graefes Arch Clin Exp Ophthalmol. 2008;246:1593–1601. doi:10.1007/s00417-008-0881-9
50. Fechtner RD, Godfrey DG, Budenz D, Stewart JA, Stewart WC, Jasek MC. Prevalence of ocular surface complaints in patients with glaucoma using topical intraocular pressure-lowering medications. Cornea. 2010;29(6):618–621. doi:10.1097/ICO.0b013e3181c325b2
51. Terai N, Muller-Holz M, Spoerl E, et al. Short term effect of topical antiglaucoma medication on tear-film stability, tear secretion, and corneal sensitivity in healthy subjects. Clin Ophthalmol. 2011;5(1):517–525. doi:10.2147/OPTH.S18849
52. Stewart WC, Stewart JA, Nelson LA. Ocular surface disease in patients with ocular hypertension and glaucoma. Curr Eye Res. 2011;36(5):391–398. doi:10.3109/02713683.2011.562340
53. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. Ocul Surf. 2017;15:511–538. doi:10.1016/j.jtos.2017.05.004
54. Torricelli AA, Matsuda M, Novaes P, et al. Effects of ambient levels of traffic-derived air pollution on the ocular surface: analysis of symptoms, conjunctival goblet cell count and mucin 5AC gene expression. Environ Res. 2014;131:59–63. doi:10.1016/j.envres.2014.02.014
55. Torricelli AA, Novaes P, Matsuda M, et al. Correlation between signs and symptoms of ocular surface dysfunction and tear osmolarity with ambient levels of air pollution in a large metropolitan area. Cornea. 2013;32(4):e11–5. doi:10.1097/ICO.0b013e31825e845d
56. Torricelli AA, Novaes P, Matsuda M, et al. Ocular surface adverse effects of ambient levels of air pollution. Arq Bras Oftalmol. 2011;74(5):377–381. Review. doi:10.1590/S0004-27492011000500016
57. Saxena R, Srivastava S, Trivedi D, et al. Impact of environmental pollution on the eye. Acta Ophthalmol Scand. 2003;81:491–494. doi:10.1034/j.1600-0420.2003.00119.x
58. Kastelan S, Tomic M, Soldo KM, et al. How ocular surface disease impacts the glaucoma treatment outcome. Biomed Res Intl. 2013;2013:1–7. doi:10.1155/2013/696328
59. Uchino M, Shaumberg DA. Dry eye disease: impact on quality of life and vision. Curr Ophthalmol Rep. 2014;1(2):51–57. doi:10.1007/s40135-013-0009-1
60. Pisella PJ, Pouliquen P, Baudouin C. Prevalence of ocular symptoms and signs with preserved and preservative free glaucoma medication. Br J Ophthalmol. 2002;86:418–423. doi:10.1136/bjo.86.4.418
61. Feroze KB, Khazaeni L. Steroid Induced Glaucoma. StatPearls Publishing LLC; 2019.
62. Batra R, Tailor R, Mohamed S. Ocular surface disease exacerbated glaucoma: optimizing the ocular surface improves intraocular pressure control. J Glaucoma. 2014;23:56–60. doi:10.1097/IJG.0b013e318264cd68
63. Kahook MY. Branded vs. generic: proceed with caution. Rev Ophthalmol. 2014. Available from: https://www.reviewofophthalmology.com/article/branded-vs-generic-proceed-with-caution. Accessed January 16, 2018.
64. Terrie YC. Ophthalmic medications: the safety and efficacy of brand-name versus generic formulations. US Pharm. 2015;40(suppl):56–66.
65. Zore M, Harris A, Tobe LA, et al. Generic medications in ophthalmology. Br J Ophthalmol. 2013;97:253–257. doi:10.1136/bjophthalmol-2012-302245
66. Karmel M. Generic vs. branded drugs: just how equal is equal? Am Acad Ophthalmol EyeNet. 2011. Available from: https://www.aao.org/eyenet/article/generic-vs-branded-drugs-just-how-equal-is-equal. Accessed January 16, 2018.
67. Banga HK, Gupta AK, Singh G. Volumetric and cost evaluation study of glaucoma medical therapy. Int J Appl Basic Med Res. 2015;5:96–99. doi:10.4103/2229-516X.157153
68. European Glaucoma Society. Terminology and Guidelines for Glaucoma.
69. Holló G, Katsanos A, Boboridis KG, et al. Preservative-free prostaglandin analogs and prostaglandin/timolol fixed combinations in the treatment of glaucoma: efficacy, safety and potential advantages. Drugs. 2018;78:39–64. doi:10.1007/s40265-017-0843-9
70. Fiscella R, Green A, Patuszynski DH, et al. Medical therapy cost considerations for glaucoma. Am J Ophthalmol. 2003;136:18–25. doi:10.1016/S0002-9394(03)00102-8
71. Shedden A, Adamsons IA, Getson AJ, et al. Comparison of the efficacy and tolerability of preservative-free and preservative-containing formulations of the dorzolamide/timolol fixed combination (COSOPT™) in patients with elevated intraocular pressure in a randomized clinical trial. Graefes Arch Clin Exp Ophthalmol. 2010;248:1757–1764. doi:10.1007/s00417-010-1397-7
72. Boyle JE, Ghosh K, Gieser DK, et al. A randomized trial comparing the dorzolamide-timolol combination given twice daily to monotherapy with timolol and dorzolamide. Dorzolamide-Timolol Study Group. Ophthalmology. 1998;105(10):1945–1951. doi:10.1016/S0161-6420(98)91046-6
73. Strohmaier K, Snyder E, DuBiner H, et al. The efficacy and safety of the dorzolamide-timolol combination versus the combination administration of its components. Ophthalmology. 1998;105:1936–1944. doi:10.1016/S0161-6420(98)91045-4
74. Clineschmidt CM, Williams RD, Snyder E, et al. A randomized trial in patients inadequately controlled with timolol alone comparing the dorzolamide-timolol combination to monotherapy with timolol or dorzolamide. Dorzolamide-Timolol Combination Study Group. Ophthalmology. 1998;105:1952–1959. doi:10.1016/S0161-6420(98)91047-8
75. Parmaksiz S, Yüksel N, Karabas VL, et al. A comparison of travoprost, latanoprost, and the fixed combination of dorzolamide and timolol in patients with pseudoexfoliation glaucoma. Eur J Ophthalmol. 2006;16(1):73–80. doi:10.1177/112067210601600113
76. He M, Wang W, Huang W. Efficacy and tolerability of the fixed combinations latanoprost/timolol versus dorzolamide/timolol in patients with elevated intraocular pressure: a meta-analysis of randomized controlled trials. PLoS One. 2013;8(12):e83606. doi:10.1371/journal.pone.0083606
77. Babić N, Veljko A, Miljković A, et al. Comparison of the efficacy and safety of fixed combination travoprost/timolol and dorzolamide/timolol in patients with primary open-angle glaucoma and ocular hypertension. Srp Arh Celok Lek. 2013;141(7–8):441–446. doi:10.2298/SARH1308441B
78. Sezgin Akçay BI, Güney E, Bozkurt KT, Ünlü C, Akçali G. The safety and efficacy of brinzolamide 1%/timolol 0.5% fixed combination versus dorzolamide 2%/timolol 0.5% in patients with open-angle glaucoma or ocular hypertension. J Ocul Pharmacol Ther. 2013;29:882–886. doi:10.1089/jop.2013.0102
79. Konstas AG, Quaranta L, Yan DB, et al. Twenty-four hour efficacy with the dorzolamide/timolol-fixed combination compared with the brimonidine/timolol fixed combination in primary open-angle glaucoma. Eye (Lond). 2012;26(1):80–87. doi:10.1038/eye.2011.239
80. Lesk MR, Koulis T, Sampalis F, et al. Effectiveness and safety of dorzolamide–timolol alone or combined with latanoprost in open-angle glaucoma or ocular hypertension. Ann Pharmacother. 2008;42:498–504. doi:10.1345/aph.1K565
81. Quaranta L, Miglior S, Floriani I, et al. Effects of the timolol-dorzolamide fixed combination and latanoprost on circadian diastolic ocular perfusion pressure in glaucoma. Invest Ophthalmol Vis Sci. 2008;49:4226–4231. doi:10.1167/iovs.08-1744
82. Takeda S, Mimura T, Matsubara M. Effect of 3 years of treatment with a dorzolamide/timolol (1%/0.5%) combination on intraocular pressure. Clin Ophthalmol. 2014;8:1773–1782.
83. Hutzelmann J, Owens S, Shedden A, et al. Comparison of the safety and efficacy of the fixed combination of dorzolamide/timolol and the concomitant administration of dorzolamide and timolol: a clinical equivalence study. International Clinical Equivalence Study Group. Br J Ophthalmol. 1998;82(11):1249–1253. doi:10.1136/bjo.82.11.1249
84. Galose MS, Elsaied HM, Macky TA, et al. Brinzolamide/timolol versus dorzolamide/timolol fixed combinations: a hospital-based, prospective, randomized study. Indian J Ophthalmol. 2016;64(2):127–131. doi:10.4103/0301-4738.179718
85. Lee NY, Park HY, Park CK. Comparison of the effects of dorzolamide/timolol fixed combination versus latanoprost on intraocular pressure and ocular perfusion pressure in patients with normal-tension glaucoma: a randomized, crossover clinical trial. PLoS One. 2016;12(11):1–16.
86. Inoue K, Shiokawa M, Sugahara M, et al. Three-month evaluation of dorzolamide hydrochloride/timolol maleate fixed-combination eye drops versus the separate use of both drugs. Jpn J Ophthalmol. 2012;56(6):559–563. doi:10.1007/s10384-012-0186-8
87. Crichton AC, Harasymowycz P, Hutnik CM, et al. Effectiveness of dorzolamide–timolol (COSOPT) in patients who were treatment naive for open-angle glaucoma or ocular hypertension: the COSOPT first-line study. J Ocul Pharmacol Ther. 2010;26(5):503–511. doi:10.1089/jop.2010.0032
88. Uusitalo H, Pillunat LE, Ropo A, et al. Efficacy and safety of tafluprost 0.0015% versus latanoprost 0.005% eye drops in open-angle glaucoma and ocular hypertension: 24-month results of a randomized, double-masked phase III study. Acta Ophthalmol. 2010;88(1):12–19. doi:10.1111/j.1755-3768.2010.01862.x
89. Hamacher T, Airaksinen J, Saarela V, Liinamaa MJ, Richter U, Ropo A. Efficacy and safety levels of preserved and preservative-free tafluprost are equivalent in patients with glaucoma or ocular hypertension: results from a pharmacodynamics analysis. Acta Ophthalmol. 2008;Suppl (Oxf) 242:14–19. doi:10.1111/j.1755-3768.2008.01381.x
90. Uusitalo H, Chen E, Pfeiffer N, et al. Switching from a preserved to a preservative-free prostaglandin preparation in topical glaucoma medication. Acta Ophthalmol. 2010;88:329–336. doi:10.1111/j.1755-3768.2010.01907.x
91. Lanzl I, Hamacher T, Rosbach K, et al. Preservative-free tafluprost in the treatment of naive patients with glaucoma and ocular hypertension. Clin Ophthalmol. 2013;7:901–910.
92. Egorov E, Ropo A. Adjunctive use of tafluprost with timolol provides additive effects for reduction of intraocular pressure in patients with glaucoma. Eur J Ophthalmol. 2009;19(2):214–222. doi:10.1177/112067210901900207
93. Hommer A, Kimmich F. Switching patients from preserved prostaglandin analog monotherapy to preservative-free tafluprost. Clin Ophthalmol. 2011;5:623–631.
94. Konstas AGP, Quaranta L, Katsanos A, et al. Twenty-four hour efficacy with preservative free tafluprost compared with latanoprost in patients with primary open angle glaucoma or ocular hypertension. Br J Ophthalmol. 2013;97:1–6.
95. Mochizuki H, Itakura H, Yokoyama T, Takamatsu M, Kiuchi Y. Twenty-four-hour ocular hypotensive effects of 0.0015% tafluprost and 0.005% latanoprost in healthy subjects. Jpn J Ophthalmol. 2010;54:286–290. doi:10.1007/s10384-010-0828-7
96. Uusitalo H, Egorov E, Kaarniranta K, Astakhov Y, Ropo A. on behalf of the Switch Study Tafluprost Study Groups. Benefits of switching from latanoprost to preservative-free tafluprost eye drops: a meta-analysis of two Phase IIIb clinical trials. Clin Ophthalmol. 2016;10:445–454. doi:10.2147/OPTH
97. Hommer A, Mohammed Ramez O, Burchert M, Kimmich F. IOP-lowering efficacy and tolerability of preservative-free tafluprost 0.0015% among patients with ocular hypertension or glaucoma. Curr Med Res Opin. 2010;26(8):1905–1913. doi:10.1185/03007995.2010.492030
98. Erb C, Lanzl I, Seidova SF, Kimmich F. Preservative-free tafluprost 0.0015% in the treatment of patients with glaucoma and ocular hypertension. Adv Ther. 2011;28(7):575–585. doi:10.1007/s12325-011-0038-9
99. Makino K, Charles H, Tilden D, et al. Health economic evaluation of preservative-free tafluprost versus preserved latanoprost in the treatment of open-angle glaucoma or ocular hypertension (OH). Value Health. 2010;15:A643. doi:10.1016/j.jval.2012.08.242
100. Payet S, Denis P, Berdeaux G, Launois R. Assessment of the cost effectiveness of travoprost versus latanoprost as single agents for treatment of glaucoma in France. Clin Drug Investig. 2008;28(3):183–198. doi:10.2165/00044011-200828030-00005
101. World Health Organization. WHO Guideline on Health Policy and System Support to Optimize Community Health Worker Programmes. World Health Organization; 2018. Available from: https://apps.who.int/iris/bitstream/handle/10665/275474/9789241550369-eng.pdf. Accessed August 4, 2019.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.