")
Back to Journals » International Journal of General Medicine » Volume 16
Management and Anticoagulation Treatment of Non-Valvular Atrial Fibrillation in Elderly Patients: The Dali Study
Authors Huang H, Hu NQ, Yang JY, Xiang YL, Zhu YZ, Du QR, Yin XY, Lv JL, Li LH
Received 25 April 2023
Accepted for publication 4 August 2023
Published 14 August 2023 Volume 2023:16 Pages 3491—3501
DOI https://doi.org/10.2147/IJGM.S418674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hong Huang, Nai-Qing Hu, Jun-Yun Yang, Yu-Luan Xiang, Yuan-Zhao Zhu, Qian-Ru Du, Xue-Yan Yin, Jin-lin Lv, Li-Hua Li
Department of Gerontology, The First Affiliated Hospital of Dali University, Dali, Yunnan Province, 671000, People’s Republic of China
Correspondence: Li-Hua Li, Department of Gerontology, The First Affiliated Hospital of Dali University, Jiashibo Road 32, Dali, 671000, People’s Republic of China, Tel +86-872-2205663, Fax +86-872-2201096, Email [email protected]
Background: Non-valvular atrial fibrillation (NVAF) is associated with increased stroke in elderly populations, yet anticoagulant therapy is underutilized. We analyzed clinical characteristics and anticoagulation treatment rates of elderly NVAF patients hospitalized in Dali, China, to identify potential contributing factors.
Methods: We collected data for 155 elderly patients with NVAF aged ≥ 60 years, from July 01, 2020, to December 31, 2021. We analyzed the awareness rate, clinical characteristics, and anticoagulant treatment rate of atrial fibrillation (AF), and identified factors influencing treatment. Patients were followed up one year after discharge to assess vital status, cardiovascular events, and anticoagulation therapy status.
Results: Among 155 patients, 52.26% were female, and the average age was 75.77 years. The awareness rate of AF was 47.74% at admission, and only 21.94% received anticoagulant therapy. After discharge, the rate of anticoagulant therapy significantly increased to 70.97%, and 89.09% used new oral anticoagulants. Thromboembolic history and persistent AF predicted anticoagulant therapy at discharge, while male gender, previous bleeding history, and antiplatelet therapy predicted non-anticoagulant therapy. Out of 133 patients who completed a one-year follow-up, 23.31% died, 3.01% had strokes, and 3.01% experienced bleeding. Anticoagulant therapy decreased to 51.96% during the follow-up year.
Conclusion: Our findings highlight the low awareness rate and anticoagulant treatment rate, and high mortality among elderly NVAF patients in Dali. The development of comprehensive intervention strategies is critical to standardize AF management and improve prognosis.
Keywords: non-valvular atrial fibrillation, awareness rate of atrial fibrillation, anticoagulant therapy, stroke, all-cause death
Introduction
Atrial fibrillation (AF) is a prevalent age-related disease that affects the elderly predominately. As countries enter into an aging society, the incidence of AF is on the rise and shows no signs of abating.1 According to a 2010 Global Burden of Disease Study, there are an estimated 33 million patients diagnosed with AF worldwide. Trends suggest that this figure will surpass 8 million in the United States, and 9 million in China by 2050.1,2 Despite this, AF remains a widely overlooked arrhythmia in clinical practice, presenting a substantial burden on health care systems in high-income and low- to middle-income countries worldwide.3,4 Inadequate management of AF may lead to severe complications such as heart failure, stroke and dementia, posing further harm to patients’ health. Moreover, AF can also reduce patients’ quality of life significantly.5 Patients diagnosed with paroxysmal AF or persistent AF have been found to have a lower quality of life, including dimensions such as disease burden, overall life satisfaction, mental health, and physical function. The decline in quality of life has been comparable to that of heart failure and patients who have undergone coronary intervention.6
While some patients with AF may restore sinus rhythm with the aid of drug cardioversion, electrical cardioversion, or radiofrequency ablation, most require long-term heart rate control and anticoagulant therapy to prevent cardiovascular and cerebrovascular complications.7,8 AF significantly increases the risk of embolic stroke in patients, nearly five times more than patients without AF.9 Additionally, AF complicates the risk of heart failure and increases mortality in patients with myocardial infarction, identifying it as an independent risk factor for death.10 Furthermore, AF is an independent risk factor for dementia, independent of age, previous stroke, and other factors, and is more pronounced in younger and healthier individuals.11–13
AF shares common risk factors with cardiovascular disease, including hypertension, diabetes, structural heart disease, smoking and alcohol consumption, obesity or overweight, hyperlipidemia, and physical inactivity.14–22 The incidence of AF combined with coronary artery disease (CAD) has been rising rapidly in recent years, and the two diseases have a strong correlation with many common risk factors. CAD can promote the development of AF, and AF is an independent risk factor for CAD. Patients with AF combined with CAD often have a poor prognosis.23–26 Optimal control of both diseases is key to improving outcomes. For example, statins used in CAD have been shown to reduce the incidence and burden of AF. Therapies aimed at reducing the burden of CAD, such as percutaneous coronary intervention or bypass graft surgery, have also been shown to significantly reduce the burden of concomitant AF and improve morbidity and mortality.27 Similarly, therapies such as rate control in AF patients using β blockers or calcium channel blockers can significantly reduce coronary ischemia and myocardial oxygen uptake.28
The Dali Bai Autonomous Prefecture of China is located in the frontier minority areas. The economy is underdeveloped, and radiofrequency ablation has not been widely adopted, leaving significant disparities between the management of AF in the region and that in more developed areas. Therefore, the objective of this study is to investigate the clinical characteristics of elderly patients diagnosed with non-valvular atrial fibrillation (NVAF) in Dali, to appraise the awareness rate of AF, antithrombotic and anticoagulant treatment modalities, and to analyze its influencing factors to provide a scientific basis for the management of local AF and formulation of health policy.
Methods
Study Population
We consecutively enrolled 208 patients aged ≥60 years with a diagnosis of AF who were hospitalized in the Department of Geriatrics at the First Affiliated Hospital of Dali University between July 1, 2020, and December 31, 2021, irrespective of the reason for their hospitalization. Patients who did not originate from Dali (n = 40), those with valvular AF (n = 11), and those with incomplete data (n = 2) were excluded. The remaining 155 patients were included in the final statistical analysis. After discharge, a one-year phone-call follow-up was conducted to explore patients’ vital status, anticoagulant therapy, incident stroke, bleeding events, surgery, and readmission to the hospital. This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Dali University (NO. DFY202006001), and patients provided written informed consent. The study protocol conforms to the ethical guidelines of the 2013 Declaration of Helsinki.29
Data Collection
Patient information was collected, including gender, age, nationality, height, weight, occupation, and history of smoking and drinking. Previous medical history, including pre-admission diagnosis, was obtained, and other medical history such as antithrombotic and anticoagulant therapy usage, bleeding history, stroke history, surgical treatment, medications, hypertension, diabetes mellitus, CAD, chronic obstructive pulmonary disease, thromboembolic disease, heart failure, hyperthyroidism, and liver and kidney diseases were gathered from medical records and telephone questionnaires. Fasting venous blood was collected to measure various indicators, including liver function, kidney function, blood sugar, blood lipids, electrolyte levels, blood routine, and coagulation function. Both CHA2DS2-VASC and HAS-BLED scores were calculated.30
Relevant Definitions
Paroxysmal AF is defined as AF lasting up to seven days. Persistent AF is defined as AF lasting more than seven days but no more than 12 months. Permanent AF is defined as AF lasting for more than one year that cannot be terminated, or recurrence after termination of AF.31 In this study, persistent AF encompasses both persistent and permanent AF. Newly diagnosed AF refers to AF diagnosed during hospitalization without any prior history of AF. Stroke in this study refers to ischemic stroke. The bleeding history refers to previous instances of intracranial hemorrhage, gastrointestinal bleeding, nasal bleeding, oral bleeding, skin and mucosal ecchymosis, ecchymosis, and hemorrhoids bleeding that required hospitalization. Incident stroke refers to a stroke that occurred during the post-hospitalization to follow-up period. Incident bleeding refers to bleeding that occurs during the post-hospitalization to follow-up period. The New York Heart Association Cardiac Function Classification (NYHA) was used to classify heart function in this study.32 Thromboembolism includes pulmonary embolism, deep vein thromboembolism, and thromboembolism in other parts of the body. Smoking was defined as continuous or cumulative smoking for 6 months or more during a patient’s lifetime. The smoking index was calculated as the product of the number of cigarettes smoked per day and the number of years smoked. Drinking was defined as self-reported alcohol consumption by the patients.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics Version 25.0 software. Normally distributed measurement data were expressed as mean ± standard deviation, and an independent sample t-test was used for comparison between two groups. Non-normally distributed measurement data were presented as M (Q1, Q3), and a rank-sum test was used for comparisons between two groups. Count data were reported as frequency (n) or percentage (%), and either chi-square or Fisher’s exact test was used for comparisons between two groups. The Cox proportional hazards model was used to analyze the predictive factors for anticoagulant treatment adherence and all-cause mortality one year after discharge in patients with AF. The statistical power of our study was determined to be 87%. The significance level was set at P <0.05.
Results
Characteristics of the Study Population
The study analyzed 155 patients with NVAF, with an average age of 75.77 ± 7.51 years. Of the patients included in the study, 45 (29.03%) had a history of smoking, all of whom were male. The average smoking index was 722. Additionally, 22 patients (14.19%) reported a history of drinking, all of whom were male.
The study found that among the 155 patients with NVAF, the mean CHA2DS2-VASc score was 5.26 ± 1.55, and the mean HAS-BLED score was 2.28 ± 1.10. Among them, 94 patients (60.65%) had a CHA2DS2-VASc score ≥2 and HAS-BLED score <3, and 80.85% (76/94) received anticoagulant treatment. Additionally, 61 patients (39.35%) had a CHA2DS2-VASc score ≥2 and HAS-BLED score ≥3, and 63.93% (39/61) received anticoagulant treatment. Table 1 provides further details on this information.
 |
Table 1 Distribution of CHA2DS2-VASc Score and HAS-BLED Score in the NVAF Patients |
The Awareness Rate of AF, Antiplatelet and Anticoagulant Treatment Rate of NVAF Patients on Admission
Among the 155 patients with NVAF, 81 (52.26%) were unaware of their AF upon admission, and 74 (47.74%) were aware. Only 34 patients (21.94%) received regular anticoagulant therapy upon admission, with 10 patients (29.41%) being treated with warfarin and 24 patients (70.59%) receiving NOACs. Antiplatelet therapy was administered to 18 patients (11.61%), while 5 patients (3.23%) received a combination of anticoagulation treatment and antiplatelet therapy. One patient underwent radiofrequency ablation. Relevant details can be found in Table 2.
 |
Table 2 Awareness and Treatment Rates of AF, Antiplatelet and Anticoagulant Use for NVAF Patients Upon Admission |
The Rate of Anticoagulant Therapy and the Use of NOACs in NVAF Patients at Discharge
Upon discharge, 70.97% (110/155) of NVAF patients received anticoagulant therapy. 10.91% (12/110) of them received warfarin, while 89.09% (98/110) received NOACs. Among those receiving NOACs, 74.49% (73/98) were treated with rivaroxaban, and 25.51% (25/98) were treated with edoxaban. Additionally, 22.58% (35/155) received antiplatelet therapy, with 68.57% (24/35) being treated with aspirin and 31.43% (11/35) with clopidogrel. Moreover, anticoagulant therapy combined with antiplatelet therapy was observed in 7.10% (11/155) of the patients. More information can be found in Table 3.
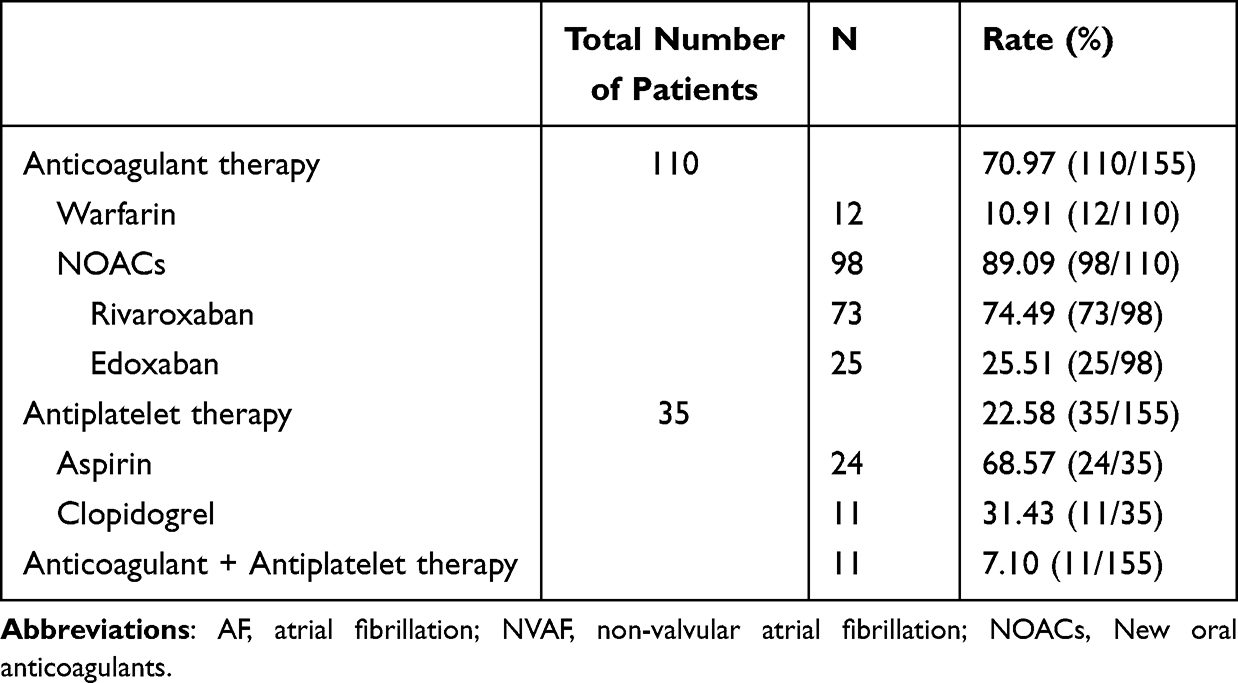 |
Table 3 Rates of Antiplatelet and Anticoagulant Treatment at Discharge in NVAF Patients and Usage of NOACs |
Comparison of Patients Receiving Anticoagulant and Non-Anticoagulant Therapy
Patients who received anticoagulant therapy at discharge had a higher prevalence of thromboembolic disease (17.27% vs 2.22%, P = 0.023), heart failure (76.36% vs 57.78%, P = 0.021), and persistent AF (41.82% vs 22.22%, P = 0.021) compared to those who did not receive anticoagulant therapy. However, patients receiving anticoagulant therapy had a lower proportion of coronary heart disease (20.00% vs 44.44%, P = 0.002), bleeding history (6.36% vs 33.33%, P < 0.001), and antiplatelet therapy (10.00% vs 53.33%, P < 0.001) (Table 4).
 |
Table 4 Factors Affecting Anticoagulant Therapy at Discharge in NVAF Patients |
Binary logistic regression analysis showed that gender, thromboembolic disease, bleeding history, antiplatelet therapy, and persistent atrial fibrillation were influential factors in anticoagulant therapy. Thromboembolic disease (OR = 70.014, 95% CI 3.220–1522.320, P = 0.007) and persistent AF (OR = 4.052, 95% CI 1.172–14.007, P = 0.027) were significant predictors of anticoagulant therapy, with male patients (OR = 0.232, 95% CI 0.061–0.880, P = 0.032), bleeding history (OR = 0.014, 95% CI 0.002–0.098, P < 0.001), and antiplatelet therapy (OR = 0.048, 95% CI 0.013–0.168, P < 0.001) being predictors of non-anticoagulant therapy (Table 5).
 |
Table 5 Multivariate Analysis of Predictors of Anticoagulant Therapy in NVAF Patients |
Reasons for Non-Anticoagulant Therapy in NVAF Patients at Discharge
Among the non-anticoagulated patients with NVAF, 6 (13.33%) had a prior history of bleeding, 6 (13.33%) expressed concerns regarding the possibility of bleeding, 22 (48.89%) had a high risk of bleeding as indicated by the HAS-BLED score of 3 or more, 2 (4.44%) reported a lack of information provided by their physicians, 1 (2.22%) had recently undergone surgical treatment, 1 (2.22%) experienced severe thrombocytopenia, and 7 (15.56%) had an unknown etiology (Figure 1).
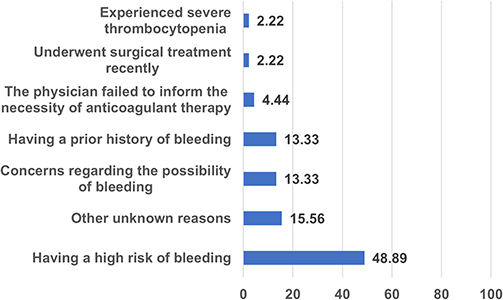 |
Figure 1 Reasons and Frequency for Non-Anticoagulant Therapy in NVAF Patients. The values presented in the figure are expressed as percentages (%). Abbreviation: NVAF, non-valvular atrial fibrillation. |
One-Year Follow-Up Study of Patients with NVAF After Discharge
A total of 133 patients (85.81%) were included in the one-year follow-up study of NVAF patients discharged from the hospital. Among these patients, the mortality rate was 23.31% (31/133), 53 (51.96%) received anticoagulant treatment, and out of those, 39 (73.58%) used NOACs. The heart failure readmission rate was 15.69% (16/102), and the incident stroke rate was 3.92% (4/102). Among the latter, three cases were not treated with anticoagulant therapy, one case was treated with anticoagulant therapy, and two cases were treated with antiplatelet therapy. The surgical treatment rate was 1.96% (2/102), out of which one case was treated with radiofrequency ablation, and the other with left atrial appendage occlusion.
Reasons for Non-Anticoagulant Therapy in NVAF Patients After Discharge
Out of the total discharged patients, only 53 received anticoagulant therapy one year after their discharge. Twelve patients with NVAF did not receive anticoagulation therapy at the time of discharge. Among the patients who discontinued anticoagulant therapy, 27.03% (10/37) were not aware of the need for long-term medication, while 24.32% (9/37) reported feeling ill and were unable to tolerate the medication. 10.81% (4/37) patients stopped taking the medicine after their symptoms improved, while 10.81% (4/37) had bleeding events and 5.41% (2/37) were worried about bleeding. Additionally, 5.41% (2/37) patients underwent surgical treatment, and 5.41% (2/37) experienced stomach discomfort after taking the medication. 5.41% (2/37) patients considered the medication to be expensive. Only 2.70% (1/37) patient faced difficulty in purchasing the medicine, and in one instance, the physician recommended discontinuing the medication.
Influencing Factors of Anticoagulant Therapy One Year After Discharge
Compared to the non-anticoagulant treatment patients, those received anticoagulant treatment were more likely to have a thromboembolic history (24.53% vs 2.04%, P = 0.003), a history of stroke (18.87% vs 4.08%, P = 0.045), and persistent AF (49.06% vs 18.37%, P = 0.001). The proportion of patients with CAD was lower in the anticoagulant treatment group (18.87% vs 42.86%, P = 0.008), as was the proportion with bleeding history (5.66% vs 22.45%, P = 0.030) (Table 6).
 |
Table 6 Factors Affecting Anticoagulant Therapy in NVAF Patients One Year After Discharge |
Our study conducted a Cox regression analysis to investigate the predictors of anticoagulation therapy in NVAF patients one year after discharge. The results presented in Table 7 show that age (HR = 1.063, 95% CI 1.013–1.115, P = 0.012), male gender (HR = 2.547, 95% CI 1.106–5.862, P = 0.028), and thromboembolism history (HR = 3.220, 95% CI 1.326–7.820, P = 0.010) were identified as statistically significant independent predictors of anticoagulation therapy. On the other hand, bleeding history (HR = 0.235, 95% CI 0.056–0.981, P = 0.047), anticoagulant therapy when discharged (HR = 0.289, 95% CI 0.099–0.844, P = 0.023) and antiplatelet therapy when discharge (HR = 0.319, 95% CI 0.105–0.972, P = 0.044) were identified as statistically significant independent predictors of non-anticoagulation therapy.
 |
Table 7 Cox Regression Analysis of Anticoagulant Therapy in NVAF Patients One Year After Discharge |
Determinants of One-Year All-Cause Mortality Among Patients with NVAF
A multivariate model was used to analyze various independent variables including age, gender, hypertension, diabetes, CAD, chronic obstructive pulmonary disease, stroke history, bleeding history, anticoagulant therapy, persistent AF, and NYHA cardiac function grade IV to determine the determinants of one-year all-cause mortality among patients with NVAF. The findings revealed that age (HR = 1.057, 95% CI 1.005–1.111, P = 0.031) and NYHA IV (HR = 2.503, 95% CI 1.148–5.458, P = 0.021) were statistically significant independent risk factors associated with all-cause mortality in NVAF patients (Table 8).
 |
Table 8 Cox Regression Analysis of All-Cause Mortality in NVAF Patients One Year After Discharge |
Discussion
The major findings of this study indicate a concerning lack of awareness of AF among elderly patients upon hospital admission. This results in a low rate of anticoagulation therapy for such patients, despite their increased risk of thromboembolic disease. Additionally, the high utilization of NOACs among patients receiving anticoagulation therapy suggests a preference for these drugs over traditional anticoagulant medications. Furthermore, the study identified thromboembolic disease and persistent AF as the most significant predictors of anticoagulation therapy at the time of discharge. However, the rate of anticoagulant therapy for NVAF significantly declined after one year of discharge, indicating the need for improved long-term treatment adherence and education for both patients and healthcare providers. Overall, these findings highlight the importance of increased NVAF diagnosis awareness and improved management strategies for elderly patients with NVAF to reduce their risk of thromboembolic events and improve long-term outcomes.
Our study found that the awareness rate of NVAF among hospitalized elderly patients in Dali, China, was low at only 47.74%, and the rate of anticoagulation therapy was also low at 21.94%. This is consistent with several other studies that have reported low rates of anticoagulation therapy in AF patients in China, including a study by Siu et al which reported an overall rate of anticoagulation therapy of only 22.8% in NVAF patients aged 80 years or older,33 and a study by Guo et al which reported a rate of 26.4% in AF patients aged 85 years or older.8 The low rates of anticoagulation therapy in these studies8,33–35 and ours may be due to a lack of awareness among patients and healthcare providers about the importance of anticoagulation therapy for preventing stroke in AF patients, as well as concerns about the risk of bleeding associated with anticoagulants in elderly patients. However, the most exciting finding was that the majority of NVAF patients were discharged with standardized anticoagulation therapy. This indicates that even geriatric physicians in tertiary hospitals located in remote areas of western China can adhere to guidelines and provide standardized anticoagulation therapy.
In contrast, our study found a high rate of NOACs use among patients receiving anticoagulation therapy, at 70.59%, while the rate of antiplatelet therapy was only 11.61%. This is similar to the findings of several other studies which have reported a trend towards increased use of NOACs and decreased use of antiplatelet therapy in NVAF patients,36 including a study by Yu et al which reported a shift from antiplatelet therapy to NOACs in NVAF patients in China between 2012 and 2017. The study found that the use of NOACs was rapidly increasing, with rivaroxaban and dabigatran being the most frequently used. The average growth rates of overall visit and expenditure of OAC were 15.8% and 57.5%, respectively.36 The higher rate of NOACs use in our study may be due to the fact that NOACs have been shown to be effective and safe in preventing stroke in NVAF patients,37,38 and therefore healthcare providers may be more likely to prescribe them.
Our study also found that thromboembolic disease and persistent AF were significant predictors of anticoagulation therapy at discharge, while male patients, previous bleeding history, and antiplatelet therapy were predictors of non-anticoagulant therapy at discharge. This is consistent with the findings of several other studies which have identified similar predictors of anticoagulation therapy in NVAF patients, including a study by Reynolds et al which identified a history of stroke or transient ischemic attack, heart failure as predictors of anticoagulation therapy,39 and a study by DeWilde et al which identified male sex, previous bleeding history, and use of antiplatelet therapy as predictors of non-anticoagulant therapy.40
Despite an increase in the use of NOACs in recent years, the anticoagulant treatment rate for NVAF remains low,37,41,42 highlighting the need to educate patients about the importance of anticoagulation therapy. Moreover, patient compliance with anticoagulant therapy after discharge was only 51.96%, which is significantly lower than the rate at discharge. Non-anticoagulant therapy is a common issue among elderly patients with AF, with various factors influencing treatment discontinuation.37,39,41 According to the present study, these factors may include lack of patient education on the importance of anticoagulation, inadequate physician-patient communication, financial constraints, fear of adverse events, and lack of follow-up and monitoring after discharge.
CAD is a well-known risk factor for thromboembolic complications in AF, and recent studies have supported this association.14,43 In fact, one study has suggested that CAD should be included in the “V” of the CHA2DS2-VASc score.14 The choice of antithrombotic agents for patients with CAD combined with AF depends on the clinical status of CAD. Recent studies have shown that in patients with chronic coronary syndrome combined with AF, NOACs alone are comparable in efficacy to combined NOACs and aspirin, but with the advantage of significantly lower bleeding risk. However, in patients with acute coronary syndrome, guidelines recommend combining P2Y12 antiplatelet agents with oral anticoagulants (preferably NOACs) for at least 6–12 months, followed by continued use of oral anticoagulants only. For patients undergoing percutaneous coronary intervention (PCI), guidelines recommend triple antithrombotic therapy consisting of aspirin, a P2Y12 drug, and NOACs for 1 month after PCI, followed by the combination of a P2Y12 drug and NOACs for 6–12 months. After 1 year, most patients need to continue with oral NOACs only.44–46 In this study, 27% of patients had AF combined with CAD at discharge, but only 20% received anticoagulation and 7% received combined anticoagulation and antiplatelet therapy, which is lower than the recommended guidelines. The low rate of combined therapy may be due to concerns about bleeding risk. Future research is needed to investigate the effectiveness and safety of combined therapy in elderly patients with chronic CAD.
Our study has several strengths, including a comprehensive evaluation of clinical characteristics and anticoagulation therapy status. However, there are some limitations that need to be considered. A major limitation of this study is its single-center design and small sample size, which may limit the generalizability of our findings to other populations. In addition, the follow-up period of one year may not provide an accurate representation of the long-term outcomes of anticoagulation therapy in NVAF patients. Future studies should consider larger sample sizes with multi-center, and collect data on socioeconomic status, education level, and medical insurance types to provide a more comprehensive understanding of the factors that influence anticoagulant therapy.
Conclusions
Our study highlights the low awareness and low rate of anticoagulation therapy for NVAF among hospitalized elderly patients in Dali, China. Thromboembolic disease and persistent AF were significant predictors of anticoagulation therapy at discharge, while non-compliance was identified as a common issue. Future studies should include larger samples and multi-center designs to provide a more comprehensive understanding of influencing factors.
Acknowledgments
This study was supported financially by grants from the National Natural Science Foundation of China (82260076, 81860084). The authors gratefully acknowledge the voluntary participation of all study participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Du X, Guo L, Xia S, et al. Atrial fibrillation prevalence, awareness and management in a nationwide survey of adults in China. Heart. 2021;107(7):535–541. doi:10.1136/heartjnl-2020-317915
2. Chang SS, Dong JZ, Ma CS, et al. Current status and time trends of oral anticoagulation use among Chinese patients with nonvalvular atrial fibrillation: the Chinese Atrial Fibrillation Registry Study. Stroke. 2016;47(7):1803–1810. doi:10.1161/STROKEAHA.116.012988
3. Shi S, Tang Y, Zhao Q, et al. Prevalence and risk of atrial fibrillation in China: a national cross-sectional epidemiological study. Lancet Reg Health West Pac. 2022;23:100439. doi:10.1016/j.lanwpc.2022.100439
4. Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16(2):217–221. doi:10.1177/1747493019897870
5. Guo Y, Kotalczyk A, Imberti JF, et al. Quality indicators in the management of elderly Chinese patients with atrial fibrillation: a report from the Optimal Thromboprophylaxis in Elderly Chinese Patients with Atrial Fibrillation (ChiOTEAF) registry. Eur Heart J Qual Care Clin Outcomes. 2022;8(6):651–658. doi:10.1093/ehjqcco/qcab057
6. Westerman S, Wenger N. Gender differences in atrial fibrillation: a review of epidemiology, management, and outcomes. Curr Cardiol Rev. 2019;15(2):136–144. doi:10.2174/1573403X15666181205110624
7. Li LH, Sheng CS, Hu BC, et al. The prevalence, incidence, management and risks of atrial fibrillation in an elderly Chinese population: a prospective study. BMC Cardiovasc Disord. 2015;15(1):31. doi:10.1186/s12872-015-0023-3
8. Guo Y, Kotalczyk A, Imberti JF, et al. Oral anticoagulation improves survival in very elderly Chinese patient s with atrial fibrillation: a report from the Optimal Thromboprophylax is in Elderly Chinese Patients with Atrial Fibrillation (ChiOTEAF) reg istry. Int J Stroke. 2022;17(6):661–668. doi:10.1177/17474930211046743
9. Gutierrez C, Blanchard DG. Diagnosis and treatment of atrial fibrillation. Am Fam Physician. 2016;94(6):442–452.
10. Bjorck S, Palaszewski B, Friberg L, et al. Atrial fibrillation, stroke risk, and warfarin therapy revisited: a population-based study. Stroke. 2013;44(11):3103–3108. doi:10.1161/STROKEAHA.113.002329
11. Bansal N, Zelnick LR, An J, et al. Incident atrial fibrillation and risk of dementia in a diverse, community-based population. J Am Heart Assoc. 2023;12(6):e028290. doi:10.1161/JAHA.122.028290
12. Rouch L, Xia F, Bahorik A, et al. Atrial fibrillation is associated with greater risk of dementia in older veterans. Am J Geriatr Psychiatry. 2021;29(11):1092–1098. doi:10.1016/j.jagp.2021.02.038
13. Kim D, Yang PS, Yu HT, et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a population-based cohort. Eur Heart J. 2019;40(28):2313–2323. doi:10.1093/eurheartj/ehz386
14. Steensig K, Olesen KKW, Thim T, et al. Should the presence or extent of coronary artery disease be quantified in the CHA2DS2-VASc score in atrial fibrillation? A report from the Western Denmark Heart Registry. Thromb Haemost. 2018;118(12):2162–2170. doi:10.1055/s-0038-1675401
15. Middeldorp ME, Ariyaratnam JP, Kamsani SH, et al. Hypertension and atrial fibrillation. J Hypertens. 2022;40(12):2337–2352. doi:10.1097/HJH.0000000000003278
16. Aune D, Feng T, Schlesinger S, et al. Diabetes mellitus, blood glucose and the risk of atrial fibrillation: a systematic review and meta-analysis of cohort studies. J Diabetes Complications. 2018;32(5):501–511. doi:10.1016/j.jdiacomp.2018.02.004
17. Pathak RK, Abhilash SP, Hendriks JM. A team-based approach toward risk factors of atrial fibrillation. Card Electrophysiol Clin. 2021;13(1):257–262. doi:10.1016/j.ccep.2020.11.008
18. Huxley RR, Lopez FL, Folsom AR, et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123(14):1501–1508. doi:10.1161/CIRCULATIONAHA.110.009035
19. Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation: a prospective study and dose-response meta-analysis. J Am Coll Cardiol. 2014;64(3):281–289. doi:10.1016/j.jacc.2014.03.048
20. Aune D, Sen A, Schlesinger S, et al. Body mass index, abdominal fatness, fat mass and the risk of atrial fibrillation: a systematic review and dose-response meta-analysis of prospective studies. Eur J Epidemiol. 2017;32(3):181–192. doi:10.1007/s10654-017-0232-4
21. Ragbaoui Y, Chehbouni C, Hammiri AE, et al. Epidémiologie de l’association fibrillation atriale et insuffisance cardiaque [Epidemiology of the relationship between atrial fibrillation and heart failure]. Pan Afr Med J. 2017;26:116. French. doi:10.11604/pamj.2017.26.116.11470
22. Mozaffarian D, Furberg CD, Psaty BM, et al. Physical activity and incidence of atrial fibrillation in older adults: the cardiovascular health study. Circulation. 2008;118(8):800–807. doi:10.1161/CIRCULATIONAHA.108.785626
23. Kannel WB, Abbott RD, Savage DD, et al. Coronary heart disease and atrial fibrillation: the Framingham Study. Am Heart J. 1983;106(2):389–396. doi:10.1016/0002-8703(83)90208-9
24. Aronow WS, Ahn C, Mercando AD, et al. Correlation of atrial fibrillation, paroxysmal supraventricular tachycardia, and sinus rhythm with incidences of new coronary events in 1359 patients, mean age 81 years, with heart disease. Am J Cardiol. 1995;75(2):182–184. doi:10.1016/S0002-9149(00)80074-0
25. Soliman EZ, Safford MM, Muntner P, et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern Med. 2014;174(1):107–114. doi:10.1001/jamainternmed.2013.11912
26. Liang F, Wang Y. Coronary heart disease and atrial fibrillation: a vicious cycle. Am J Physiol Heart Circ Physiol. 2021;320(1):H1–H12. doi:10.1152/ajpheart.00702.2020
27. Wibawa K, Dewangga R, Nastiti KS, et al. Prior statin use and the incidence of in-hospital arrhythmia in acute coronary syndrome: a systematic review and meta-analysis. Indian Heart J. 2023;75(1):9–16. doi:10.1016/j.ihj.2023.01.004
28. Manolis AJ, Poulimenos LE, Ambrosio G, et al. Medical treatment of stable angina: a tailored therapeutic approach. Int J Cardiol. 2016;220:445–453. doi:10.1016/j.ijcard.2016.06.150
29. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
30. Lip GY. Implications of the CHA2DS2-VASc and HAS-BLED scores for thromboprophylaxis in atrial fibrillation. Am J Cardiol. 2011;124:111–114.
31. Levy S. Classification system of atrial fibrillation. Curr Opin Cardiol. 2000;15(1):54–57. doi:10.1097/00001573-200001000-00007
32. Caraballo C, Desai NR, Mulder H, et al. Clinical implications of the New York Heart Association Classification. J Am Heart Assoc. 2019;8(23):e014240. doi:10.1161/JAHA.119.014240
33. Siu C-W, Tse H-F. Net clinical benefit of warfarin therapy in elderly Chinese patients w ith atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7(2):300–306. doi:10.1161/CIRCEP.113.000858
34. Guo Y, Kotalczyk A, Imberti JF, et al. Poor adherence to guideline-directed anticoagulation in elderly Chinese patients with atrial fibrillation: a report from the Optimal Thromboprophylaxis in Elderly Chinese Patients with Atrial Fibrillation (ChiOTEAF) registry. Eur Heart J Qual Care Clin Outcomes. 2023;9(2):169–176. doi:10.1093/ehjqcco/qcab054
35. Guo Y, Wang H, Kotalczyk A, et al. One-year follow-up results of the optimal thromboprophylaxis in Elderly Chinese Patients with Atrial Fibrillation (ChiOTEAF) registry. J Arrhythm. 2021;37(5):1227–1239. doi:10.1002/joa3.12608
36. Yu Z, Yu L, Shan C. Trends of ambulatory oral anticoagulant prescription in five major cities of China, 2012–2017. BMC Health Serv Res. 2020;20(1):209. doi:10.1186/s12913-020-5072-3
37. Wu J, Zhang Y, Liao X, et al. Anticoagulation therapy for non-valvular atrial fibrillation: a mini-review. Front Med. 2020;7:350. doi:10.3389/fmed.2020.00350
38. Aktan A, Güzel T, Aslan B, et al. Comparison of the real-life clinical outcomes of warfarin with effective time in therapeutic range and non-vitamin K antagonist oral anticoagulants: insight from the AFTER-2 trial. Kardiol Pol. 2023;81(2):132–140. doi:10.33963/KP.a2022.0287
39. Reynolds MR, Shah J, Essebag V, et al. Patterns and predictors of warfarin use in patients with new-onset atrial fibrillation from the FRACTAL Registry. Am J Cardiol. 2006;97(4):538–543. doi:10.1016/j.amjcard.2005.09.086
40. DeWilde S, Carey IM, Emmas C, et al. Trends in the prevalence of diagnosed atrial fibrillation, its treatment with anticoagulation and predictors of such treatment in UK primary care. Heart. 2006;92(8):1064–1070. doi:10.1136/hrt.2005.069492
41. Shang L, Zhang Y, Zhao Y, et al. Contemporary oral anticoagulant therapy of patients with atrial fibrillation in China: status, obstacles, and strategies for improvement. Biosci Trends. 2022;16(5):317–329. doi:10.5582/bst.2022.01278
42. Güzel T, Aktan A, Kılıç R, et al. Oral anticoagulant use and long-term follow-up results in patients with non-valvular atrial fibrillation in Turkey AFTER-2 study. Anatol J Cardiol. 2022;26(7):567–576. doi:10.5152/AnatolJCardiol.2022.1597
43. Batta A, Hatwal J, Batta A, et al. Atrial fibrillation and coronary artery disease: an integrative review focusing on therapeutic implications of this relationship. World J Cardiol. 2023;15(5):229–243. doi:10.4330/wjc.v15.i5.229
44. Fanaroff AC, Li S, Marquis-Gravel G, et al. Atrial fibrillation and coronary artery disease: a long-term perspective on the need for combined antithrombotic therapy. Circ Cardiovasc Interv. 2021;14(12):e011232. doi:10.1161/CIRCINTERVENTIONS.121.011232
45. Matsuzawa Y, Kimura K, Yasuda S, et al. Antithrombotic therapy for atrial fibrillation and coronary artery disease in patients with prior atherothrombotic disease: a post hoc analysis of the AFIRE trial. J Am Heart Assoc. 2021;10(21):e020907. doi:10.1161/JAHA.121.020907
46. Angiolillo DJ, Bhatt DL, Cannon CP, et al. Antithrombotic therapy in patients with atrial fibrillation treated with oral anticoagulation undergoing percutaneous coronary intervention: a North American Perspective: 2021 update. Circulation. 2021;143(6):583–596. doi:10.1161/CIRCULATIONAHA.120.050438
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.