Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Malnutrition, Airflow Limitation and Severe Emphysema are Risks for Exacerbation of Chronic Obstructive Pulmonary Disease in Japanese Subjects: A Retrospective Single-Center Study
Authors Yamaya M, Usami O, Nakayama S, Tode N, Yamada A, Ito S, Omata F ![]() , Momma H
, Momma H ![]() , Funakubo M, Ichinose M
, Funakubo M, Ichinose M
Received 13 November 2019
Accepted for publication 30 March 2020
Published 22 April 2020 Volume 2020:15 Pages 857—868
DOI https://doi.org/10.2147/COPD.S238457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Mutsuo Yamaya,1 Osamu Usami,2 Shoichi Nakayama,3 Naoki Tode,4 Aya Yamada,5 Shunsuke Ito,2 Fumiya Omata,2 Haruki Momma,5 Masakatsu Funakubo,6 Masakazu Ichinose4
1Department of Advanced Preventive Medicine for Infectious Disease, Tohoku University Graduate School of Medicine, Sendai 980-8575, Japan; 2Department of Respiratory Medicine, Kurihara Central Hospital, Kurihara 987-2205, Japan; 3Department of Medicine, Kurihara Central Hospital, Kurihara 987-2205, Japan; 4Department of Respiratory Medicine, Tohoku University Graduate School of Medicine, Sendai 980-8575, Japan; 5Department of Medicine and Science in Sports and Exercise, Tohoku University Graduate School of Medicine, Sendai 980-8575, Japan; 6Department of Radiology, Kurihara Central Hospital, Kurihara 987-2205, Japan
Correspondence: Mutsuo Yamaya
Department of Advanced Preventive Medicine for Infectious Disease, Tohoku University Graduate School of Medicine, Sendai 980-8575, Japan
Tel +81-22-717-7184
Fax +81-22-717-7576
Email [email protected]
Background: Different characteristics of patients with chronic obstructive pulmonary disease (COPD) between Western and Japanese populations have been reported. Risk factors for COPD exacerbation have been reported in Western countries but have not been studied in Japan.
Patients and Methods: We retrospectively examined risk factors for COPD exacerbation. A total of 156 Japanese patients were enrolled, and the records of 136 patients were analyzed.
Results: In the exacerbation group (n=60), body mass index, forced vital capacity (FVC), forced expiratory volume in one second (FEV1), the FEV1/FVC ratio (FEV1/FVC), the percent predicted values of FEV1 (%FEV1), and serum total protein (TP) and albumin concentrations were lower, and age, mortality rate, frequency of common cold and pneumonia, COPD severity rankings, modified Medical Research Council (mMRC) dyspnea score, and proportions of patients with severe emphysema (> 50% of low attenuation area) and receiving long-term oxygen therapy were higher than those in the nonexacerbation group (n=76). However, the proportion of patients with a greater number of eosinophils (≥ 200/μL and/or ≥ 2%) and the exhaled nitric oxide concentration did not differ between the two groups. In the univariate analysis, the risk factors for exacerbation were age; long-term oxygen therapy; low FVC, FEV1, FEV1/FVC and %FEV1; high COPD severity ranking and mMRC score; severe emphysema; hypoproteinemia (< 6.5 g/dL); hypoalbuminemia (< 3.5 g/dL); leukocytosis; lymphocytopenia; and anemia. In the multivariate analysis, the risk factors were hypoalbuminemia, hypoproteinemia and low FEV1. Additionally, in patients in the exacerbation-induced mortality subgroup, age, exacerbation frequency, mMRC score and the proportion of patients with lymphocytopenia were higher, and FVC, %FVC, FEV1, serum TP concentration and the lymphocyte number were lower than those in the exacerbation survival subgroup.
Conclusion: Malnutrition, airflow limitation and severe emphysema were risks for exacerbation and mortality associated with infection in Japanese patients with COPD.
Keywords: malnutrition, chronic obstructive pulmonary disease, exacerbation, severe emphysema, airflow limitation
Introduction
Exacerbations of chronic obstructive pulmonary disease (COPD) are associated with the aggravation of symptoms, such as dyspnea, cough and sputum, and respiratory failure-induced mortality.1,2 Several risk factors for COPD exacerbation have been reported in Western countries, including severe airflow limitation, the presence of comorbidities such as bronchiectasis and heart failure, biomarkers including C-reactive protein (CRP), past history of exacerbation, poor health status, the presence of emphysema, long-term oxygen therapy and leukocytosis.2,3 A recent report demonstrated the relationship between elevated levels of blood eosinophils and severe COPD exacerbations.4
Furthermore, several markers indicating malnutrition, such as low body mass index (BMI), weight loss, nutritional depletion and low serum vitamin D, are associated with increases in mortality or the recurrence of new exacerbations.5–10 Additionally, the development of pulmonary infection, which causes COPD exacerbation,11 is associated with hypoalbuminemia.12 We demonstrated that low BMI values and hypoalbuminemia were risk factors for pneumonia in a Japanese population.13 However, the roles of hypoalbuminemia, an important biomarker of malnutrition,14 in the development of exacerbation have not been well studied.
It has been reported that Japanese and Korean patients with COPD have lower BMI values than Western patients with COPD.15–17 In addition, Japanese patients with COPD tend to suffer from dominant emphysema in which the occurrence of malnutrition is more frequent.18 These findings suggest the more important roles of the presence of malnutrition and severe emphysema in the development of exacerbations induced by pulmonary infection in Japanese and Asian patients with COPD. In fact, Lin et al reported the role of hypoproteinemia in early readmission following COPD exacerbation in Chinese subjects.19 However, in Japanese patients with COPD, risk factors for COPD exacerbations associated with malnutrition, airflow limitation and severe emphysema have not been well studied.
The main purpose of this study was to identify exacerbation-related factors associated with infection in Japanese patients with COPD by focusing on the roles of hypoalbuminemia, airflow limitation and severe emphysema.
Patients and Methods
Design, Setting and Participants
We enrolled patients according to the order of the first visit date or discharge date and analyzed patient records. Patients meeting one of the following inclusion criteria were enrolled: patients who visited the Kurihara Central Hospital to receive treatment and/or examination for COPD or who were admitted to receive treatment for COPD between April 2008 and June 2019.
Ethics Statement
The Kurihara Central Hospital Ethics Committee approved this retrospective study. Informed consent was obtained from all patients, or an informed consent waiver was obtained from the Kurihara Central Hospital Ethics Committee in cases where patients were referred to other hospitals or clinics or were deceased at the review of the records. Patient data were reviewed with confidentiality and compliance with the Declaration of Helsinki.
Measurements
The following information regarding the characteristics and examination data was obtained at the first visit or upon admission to the hospital: age; sex; observation period from first visit or admission; frequency of exacerbation, common cold and pneumonia; smoking history; death during observation period and cause of death; comorbidities; drugs for treatment of COPD; treatment with long-term oxygen therapy; BMI; data of pulmonary function tests, including forced vital capacity (FVC), percent predicted values of FVC (%FVC), forced expiratory volume in one second (FEV1), FEV1/FVC ratio (FEV1%), percent predicted values of FEV1 (%FEV1) and severity rankings of COPD; severity of dyspnea [modified Medical Research Council (mMRC) score]; the concentration of nitric oxide in the exhaled air (FeNO); radiologic evidence; and the severity of emphysema. The severity rankings of COPD classification, such as GOLD I–IV, were defined based on %FEV1 according to the GOLD guidelines.20
We also checked the following hospital data: the numbers of white blood cells (WBCs) and lymphocytes and the hemoglobin (Hb) level in the peripheral venous blood and serum levels of total protein (TP), albumin, total cholesterol, uric acid, blood urea nitrogen (BUN), creatinine and C-reactive protein (CRP).
We checked the examination data described above at the exacerbation time during the observation period, and the data at the first exacerbation time were used for analysis.
Qualitative Analysis of Emphysema
The patients underwent a chest computed tomography (CT) scan (Toshiba Medical Systems, Otawara, Japan) at full inspiration. The extent of emphysema was estimated using the low attenuation area (LAA) % (the percent of voxels with an apparent X-ray attenuation value below −950 HU). Emphysema was reported as absent, mild, moderate, or severe if the LAA% was <5%, 5–25%, 25–50%, or >50% of the lung, respectively.2,21
Definition of COPD Exacerbation, Common Cold and Pneumonia
An exacerbation event was defined as an emergency visit and/or admission to the hospital because of COPD.9 Ten symptoms of upper respiratory tract infections were recorded, and common cold was defined as a total symptom score of greater than 5, as described previously.22 Pneumonia was diagnosed based on the following standard criteria: fever (body temperature ≥37.8°C), high CRP level and infiltrate shadows on chest X-rays and/or CT scan.23
Statistical Analysis
The results are expressed as the means ± SDs. For the comparison of continuous variables between the two groups, Student’s t-test, Pearson’s chi-squared test or Fisher’s exact test was used. The chi-squared test or Fisher’s test was performed to assess differences in rates. Univariate and multivariate Cox proportional hazard regression analyses were also performed with the stepwise method to identify risk factors for COPD exacerbation. All analyses were performed using SPSS version 21 (IBM Japan, Tokyo, Japan).
Results
Characteristics of Subjects
In the present study, 156 patients were initially enrolled; 20 patients were excluded because the values of FVC/FEV1 were 70% or greater in 5 patients and because the pulmonary function test was not performed in 15 patients due to severe condition (n=12), dementia (n=2) or pneumothorax (n=1) (Figure 1).
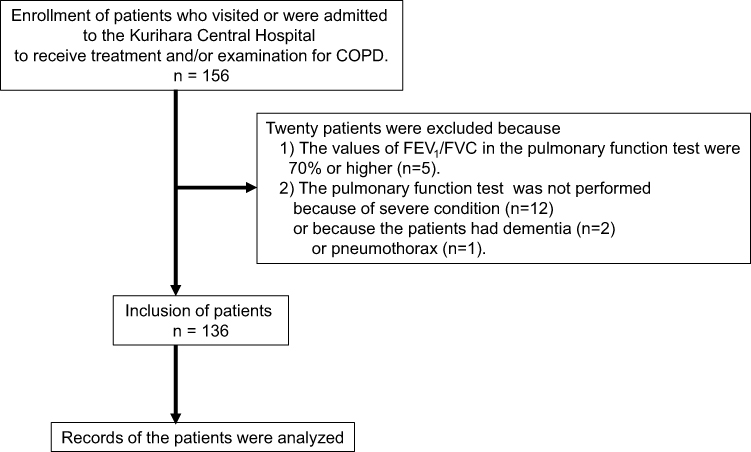 |
Figure 1 Schematic diagram outlining the patient selection process. Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in one second; FVC, forced vital capacity. |
In the 136 analyzed patients, 60 patients presented exacerbation (exacerbation group), and 76 patients did not present exacerbation (nonexacerbation group). The characteristics of the analyzed patients are shown in Table 1.
 |
Table 1 Characteristics of Patients |
The patients in the exacerbation group were older than those in the nonexacerbation group (Table 1). The sex distribution and observation period were matched in both groups.
The mean exacerbation frequency was 1.6 times during the observation period, with a mean of 50 months, in the exacerbation group. The frequency of the common cold and pneumonia and the proportion of patients who developed the common cold and pneumonia in the exacerbation group were higher than those in the nonexacerbation group (Table 1).
Among patients in the exacerbation group, 22 patients died, and the causes of death were respiratory failure (n=17), cancer (n=4) and uncertain (sudden death) (n=1) (Table 1). In patients in the nonexacerbation group, 4 patients died of causes other than respiratory failure.
In addition to treatment for COPD, the patients were treated with drugs for comorbid conditions (Table 1). The proportions of patients with comorbidities, including bronchial asthma, did not differ between the two groups. A total of 119 patients received treatment with either long-acting muscarinic antagonists (LAMAs), long-acting β2-agonists (LABAs), inhaled corticosteroids (ICSs), mucolytics, theophylline, oral corticosteroids, leukotriene receptor antagonists or macrolides alone or in combination (Table 1).
The proportion of patients who were treated with a combination of LAMAs and LABAs, a combination of LAMAs, LABAs and ICSs or a combination of ICSs and LABAs did not differ between the two groups (Table 1).
In addition, the proportions of patients who received treatment with mucolytics, theophylline or oral steroids in the exacerbation group were higher than the proportions of patients who received these treatments in the nonexacerbation group (Table 1).
The proportion of patients who received treatment with long-term oxygen therapy in the exacerbation group was more than four times higher than the proportion in the nonexacerbation group (Table 1).
BMI, Pulmonary Function Test, Dyspnea Score, FeNO and Chest CT
The mean BMI was 22.1 kg/m2, and the total number of patients who were underweight (<20 kg/m2)5,9 was 37 (27.2%). The BMI values of patients in the exacerbation group were lower than those of patients in the nonexacerbation group (Table 2). The proportion of patients who were underweight did not differ between the two groups (Table 2).
 |
Table 2 Data on BMI, Pulmonary Function Test, Dyspnea Score, FeNO, Chest CT and Laboratory Examination |
The values of the pulmonary function test results, including FVC, %FVC, FEV1, FEV1/FVC and %FEV1, of patients in the exacerbation group were lower than the values of the patients in the nonexacerbation group (Table 2), and the severity rankings of COPD (GOLD classification) were higher in the exacerbation group than those in the nonexacerbation group (Table 2). The mMRC score, which indicates the severity of dyspnea, was higher in the exacerbation group than that in the nonexacerbation group (Table 2).
The mean value of FeNO and the proportion of patients with high FeNO values (>35 ppb)24 did not differ between the two groups (Table 2).
The proportion of patients who exhibited emphysema on chest CT was 98% in the exacerbation group and 88% in the nonexacerbation group; however, the proportion of patients with emphysema did not differ between the two groups (Table 2). In contrast, the proportion of patients with severe degrees of emphysema (>50% of LAA)21 in the exacerbation group was more than three times higher than that in the nonexacerbation group (Table 2).
Peripheral Blood Biochemical Examination
The serum levels of TP and albumin in patients in the exacerbation group were lower than those in patients in the nonexacerbation group (Table 2). In particular, the serum albumin levels in the exacerbation group were more than 20% lower than those in the nonexacerbation group. Furthermore, serum CRP levels in the exacerbation group were higher than those in the nonexacerbation group (Table 2).
The proportions of patients with low values of serum TP (<6.5 g/dL) and albumin (<3.5 g/dL) and with high CRP values in the exacerbation group were higher than those in the nonexacerbation group (Table 2).
Peripheral Blood Examination
The number of WBCs and neutrophils in patients in the exacerbation group was higher than that in patients in the nonexacerbation group (Table 2). In contrast, the number of lymphocytes and the Hb value in the exacerbation group were lower than those in the nonexacerbation group (Table 2). The number of eosinophils did not differ between the two groups.
The proportions of patients with leukocytosis (>9000/μL WBC) and lymphocytopenia (<1000/μL lymphocytes) in the exacerbation group were higher than those in the nonexacerbation group (Table 2). In contrast, the proportion of patients with a greater number of eosinophils in the peripheral blood (≥200/μL or ≥2%) did not differ between the two groups.
Univariate and Multivariate Analyses of Risk Factors for Exacerbation
Univariate analysis showed that age and long-term oxygen therapy were associated with exacerbation (Table 3). In addition, FVC, %FVC, FEV1, FEV1/FVC, and %FEV1 were negatively associated with exacerbation (Table 3). Furthermore, the severity rankings of COPD; mMRC score; presence of severe emphysema (>50%); low values of TP, albumin and Hb; high CRP values; leukocytosis; and lymphocytopenia were positively associated with the development of exacerbation (Table 3).
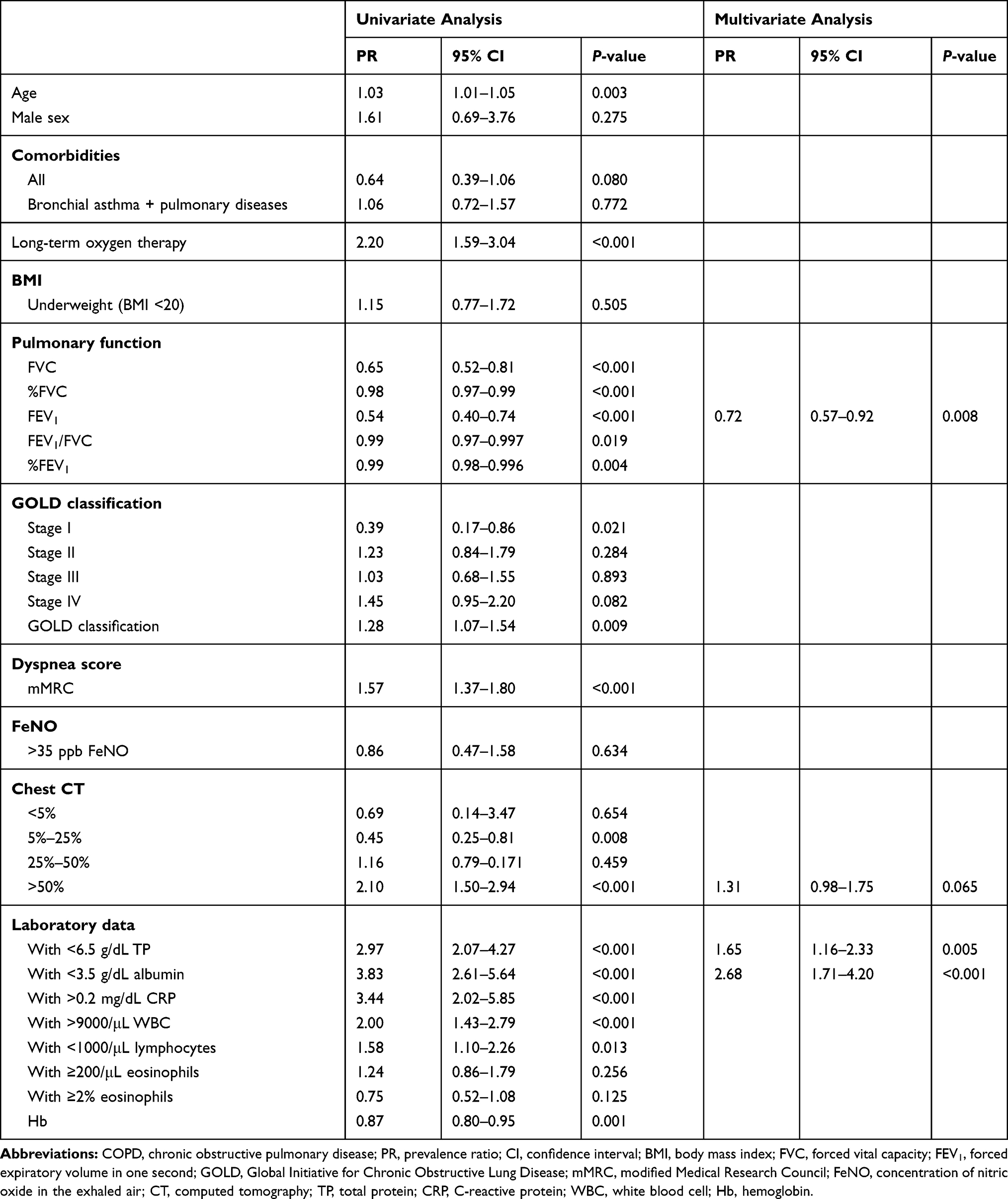 |
Table 3 Univariate and Multivariate Analyses of Risk Factors for the Exacerbation of COPD (Stepwise Method) |
In the multivariate analysis, the following risk factors for exacerbation were identified: low FEV1, hypoproteinemia and hypoalbuminemia (Table 3). Hypoalbuminemia was the strongest indicator.
Characteristics of Patients in the Exacerbation-Induced Mortality Subgroup
We also examined the risks for mortality caused by exacerbation-induced respiratory failure. In patients in the subgroup of exacerbation-induced mortality caused by respiratory failure (n=17), age, frequency of exacerbation, proportion of patients receiving long-term oxygen therapy and mMRC score were higher than those in the exacerbation survival subgroup (n=38) (Table 4). In addition, the values of FVC, % FVC, FEV1, serum concentrations of TP, the number of WBCs and lymphocytes in the exacerbation-induced mortality subgroup were lower than those in the exacerbation survival subgroup (Table 4).
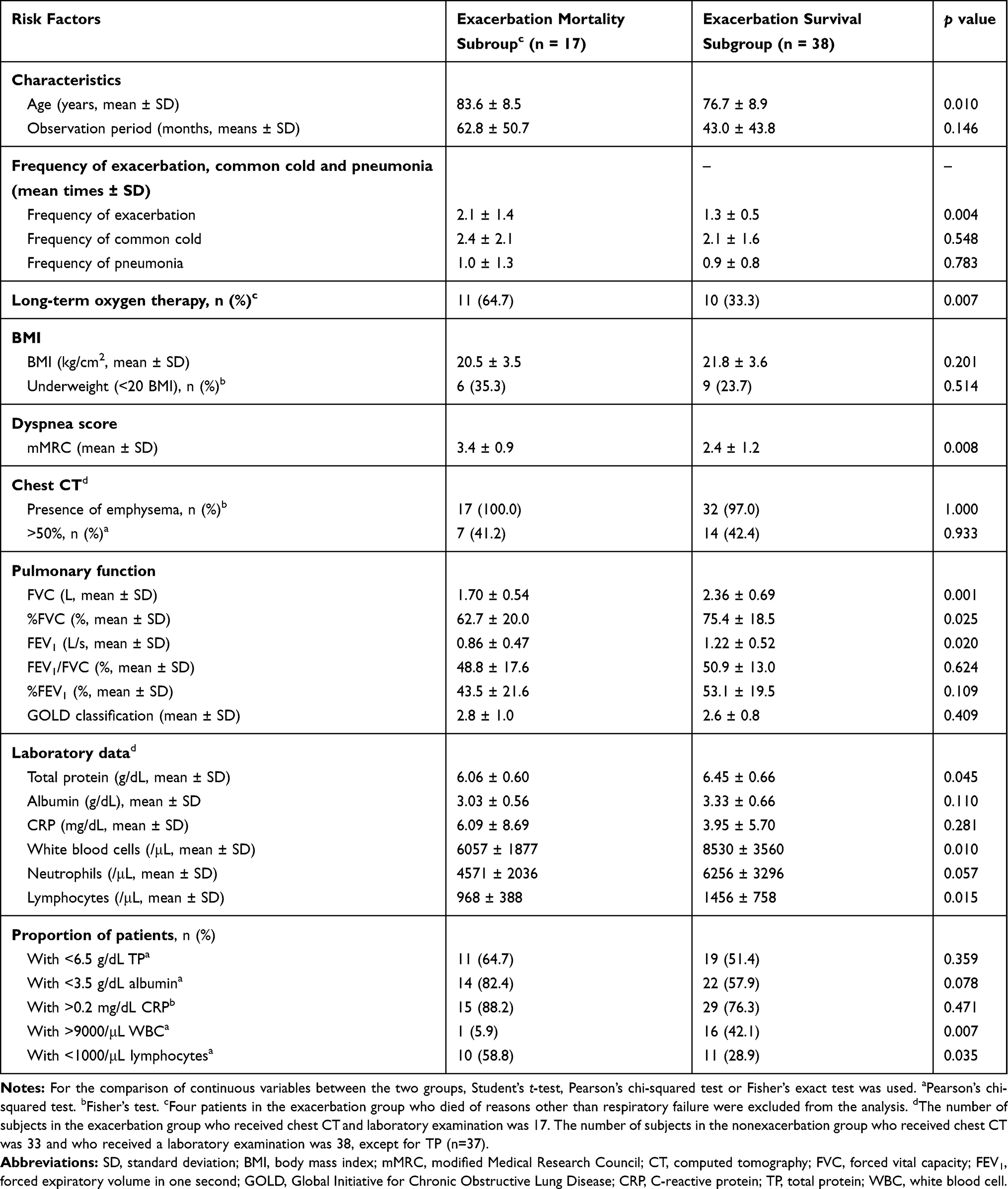 |
Table 4 Characteristics and Laboratory Examination Data in the Respiratory Failure-Induced Mortality Exacerbation Subgroup or Exacerbation Survival Subgroup |
In the exacerbation-induced mortality subgroup, the proportions of patients with lymphocytopenia were higher than those in the exacerbation survival subgroup (Table 4).
Discussion
We demonstrated that the values of FVC, %FVC, FEV1, FEV1/FVC, and % FEV1 in the exacerbation group were lower than those in the nonexacerbation group and that the severity rankings of COPD, mMRC score and proportions of patients receiving long-term oxygen therapy in the exacerbation group were higher than those in the nonexacerbation group. In the univariate analysis, long-term oxygen therapy; low values of FVC, %FVC, FEV1, FEV1/FVC and %FEV1; and high COPD severity ranking and mMRC scores were associated with COPD exacerbation. Furthermore, in the multivariate analysis, low values of FEV1 were associated with exacerbation. Thus, the factors that indicate airflow limitation were associated with COPD exacerbation in Japanese patients, as demonstrated in studies in Western patients with COPD.2,3
Furthermore, the patients in the exacerbation group were older than those in the nonexacerbation group, and age was associated with COPD exacerbation in the univariate analysis. Additionally, the proportion of patients with severe degrees of emphysema in the exacerbation group was higher than that in the nonexacerbation group. These findings were consistent with those of previous reports conducted in Western countries,2,3,7 and these two factors, namely, older age and severe degree of emphysema, may be associated with increased mortality in older Japanese patients with COPD with severe emphysema.25
In addition, BMI and serum concentrations of TP and albumin were lower and the proportions of patients with hypoproteinemia and hypoalbuminemia were higher in the exacerbation group than in the nonexacerbation group. Univariate and multivariate analyses showed that hypoproteinemia and hypoalbuminemia were risks for exacerbation, and hypoalbuminemia was the strongest indicator. These findings suggest that hypoalbuminemia and hypoproteinemia are also risks for exacerbation in Japanese patients with COPD.
The role of hypoalbuminemia as a risk factor for COPD exacerbation has not been well studied, although hypoproteinemia has been reported as a risk factor for early readmission due to COPD exacerbation and for the worst prognosis in Chinese subjects.12,19 Malnutrition causes decreased cell-mediated and humoral immunity, such as decreased lymphocyte proliferation, low function of polymorphonuclear leukocytes and monocytes, deficient release of cytokines including interleukin (IL)-6, and lower antibody response to vaccines.26
Cytokines, such as interferon and IL-6, have been suggested to act as host defense systems against viral infection in the lungs as well as to induce inflammation.27 In the present study, the proportion of patients with the common cold and pneumonia and the frequency of the common cold and pneumonia in the exacerbation group were higher than those in the nonexacerbation group, although we could not collect sufficient information regarding the species of bacteria and viruses that caused pneumonia and the common cold. Therefore, the malnutrition observed in the present study might have caused immune-deficient conditions in combination with lymphocytopenia, which is associated with respiratory bacterial and viral infection and the subsequent development of COPD exacerbation.11,28,29
The mean BMI that we reported in the present study (22 kg/m2) was lower than that reported in Western patients with COPD (27 kg/m2)15,16 and consistent with the values reported in Japan (22–23 kg/m2).17,18 Furthermore, the proportion of patients with low BMI (<20 kg/m2) in the present study (27.2%) was higher than that among Western patients with COPD (9.5%).5 In contrast, several reports also demonstrated the association of low BMI with mortality and/or exacerbation in Western patients with COPD.5,9 We demonstrated that the BMI in the exacerbation group was lower than that in the nonexacerbation group. Similar to a study conducted in Chinese patients,30 these findings suggest a more important role of low BMI as a risk for exacerbation in Japanese patients with COPD than in Western patients.
Differences in the characteristics of patients with COPD between Japanese and Western patients have been reported, including emphysema-dominant COPD evidenced by chest CT in Japanese patients in addition to lower BMI and more frequent malnutrition.18 In fact, in the present study, emphysema was observed on CT in 98% of patients in the exacerbation group and 88% of patients in the nonexacerbation group, and this proportion in the exacerbation group was higher than that in the report conducted in Western countries (75%).2 Furthermore, the proportion of patients with severe emphysema in the exacerbation group was higher than that in the nonexacerbation group. These findings suggest that severe emphysema might also be a more important risk for exacerbation in Japanese patients with COPD than in Western patients with COPD.
The proportions of patients who received treatment with mucolytics, theophylline, oral steroids or long-term oxygen therapy in the exacerbation group were higher than the proportions of patients who received these treatments in the nonexacerbation group. Because the mMRC score and the severity rankings of COPD were higher in the exacerbation group than in the nonexacerbation group, the patients in the exacerbation group might be treated with these drugs and long-term oxygen therapy more frequently to improve severe dyspnea or to prevent exacerbation.3,31,32
In patients in the exacerbation-induced mortality subgroup, age, mMRC score, and the proportion of patients with lymphocytopenia was higher, and the values of FVC, %FVC, FEV1, serum TP concentration and lymphocyte number were lower than those in the exacerbation survival subgroup. These findings may show the presence of more severe dyspnea due to air flow limitation and air flow limitation-induced severe air trapping in older patients in the exacerbation-induced mortality subgroup. Impaired mucociliary clearance due to severe airway obstruction may be associated with infection.33 The combination of these risks might have caused more severe COPD exacerbation through impaired defense mechanisms in the exacerbation-induced mortality subgroup.
Couillard et al demonstrated the relationship between severe COPD exacerbations and higher eosinophil levels.4 However, in the present study, the number of eosinophils and the proportions of patients with a greater number of eosinophils did not differ between the exacerbation group and the nonexacerbation group. The values were observed at the time of exacerbation, and it was uncertain whether the eosinophil values were persistent, as Singh et al suggested in Western patients with COPD,34 because patients were treated with systemic steroids at the time of exacerbation and in the context of a stable condition in some patients. The reasons for the differences in eosinophil levels between the study by Couillard et al4 and the present study are uncertain; however, increased neutrophils were reported in Western patients with COPD with exacerbation,34,35 suggesting the role of neutrophilic inflammation rather than eosinophilic inflammation in COPD exacerbation in Japanese patients.
The patients were enrolled according to the order of the first visit date or the discharge date from the hospital after treating the exacerbation, and patient records were analyzed to prevent any selection bias.
This study had some limitations. The nature of the present study was exploratory, and the main purpose of this study was to identify factors that are associated with the development of exacerbation in patients with COPD. Therefore, we could not precisely estimate the necessary sample size at the beginning of this study. However, we presumed that we needed approximately 50 patients in each group based on the conventional estimation that a value of the number of events per variable = 10 is most prudent when a proportional hazard regression model is used.36 Therefore, the sample sizes for the two groups (60 and 76) were thought to be sufficient to demonstrate the risks for exacerbation. As a result, we found that malnutrition, airflow limitation and severe emphysema were risks for exacerbation associated with infection in Japanese patients with COPD. These findings indicated that the effect sizes of these variables might be sufficient to detect statistical significance even in the small sample size in the present study.
Second, in the present study, patients visited the hospital by themselves or were referred from 8 clinics and 5 hospitals. The characteristics of patients with COPD that we demonstrated in the study, such as low BMI and high proportion of patients with emphysema, were similar to those of studies that were conducted in different areas of Japan.17,37,38 However, this study was performed as a retrospective and single-center study by analyzing records of patients who were treated in one hospital. Therefore, prospective and multicenter studies are needed to confirm that the evidence observed in the present study represents risk factors for COPD exacerbation in Japanese subjects.
In conclusion, malnutrition, airflow limitation and severe emphysema were risks for exacerbation and mortality associated with infection in Japanese patients with COPD.
Acknowledgments
This work was supported by grants of research support from Astellas Pharma Inc. (RS2017A000223, RS2018A000301 and RS2019A000174) and Teijin Pharma Co., Ltd. (TJNS20170731009, TJNS20180506002 and TJNS20190417024).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soler-Cataluña JJ, Martinez-Garcia MA, Román Sánchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925–931. doi:10.1136/thx.2005.040527
2. Müllerova H, Maselli DJ, Locantore N, et al. Hospitalized exacerbations of COPD: risk factors and outcomes in the ECLIPSE cohort. Chest. 2015;147:999–1007. doi:10.1378/chest.14-0655
3. Mantero M, Rogliani P, Di Pasquale M, et al. Acute exacerbations of COPD: risk factors for failure and relapse. Int J Chron Obstruct Pulmon Dis. 2017;12:2687–2693. doi:10.2147/COPD.S145253
4. Couillard S, Larivée P, Courteau J, et al. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest. 2017;151:366–373. doi:10.1016/j.chest.2016.10.003
5. Landbo C, Prescott E, Lange P, et al. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160:1856–1861. doi:10.1164/ajrccm.160.6.9902115
6. Chailleux E, Laaban JP, Veale D. Prognostic value of nutritional depletion in patients with COPD treated by long-term oxygen therapy: data from the ANTADIR observatory. Chest. 2003;123:1460–1466. doi:10.1378/chest.123.5.1460
7. Zapatero A, Barba R, Ruiz J, et al. Malnutrition and obesity: influence in mortality and readmissions in chronic obstructive pulmonary disease patients. J Hum Nutr Diet. 2013;1:16–22. doi:10.1111/jhn.12088
8. Genao L, Durheim MT, Mi X, et al. Early and long-term outcomes of older adults after acute care encounters for chronic obstructive pulmonary disease exacerbation. Ann Am Thorac Soc. 2015;12:1805–1812. doi:10.1513/AnnalsATS.201504-250OC
9. Hallin R, Koivisto-Hursti UK, Lindberg E, et al. Nutritional status, dietary energy intake and the risk of exacerbations in patients with chronic obstructive pulmonary disease (COPD). Respir Med. 2006;100:561–567. doi:10.1016/j.rmed.2005.05.020
10. Zhu M, Wang T, Wang C, et al. The association between vitamin D and COPD risk, severity, and exacerbation: an updated systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2016;11:2597–2607. doi:10.2147/COPD.S101382
11. Sethi S. New Developments in the pathogenesis of acute exacerbations of chronic obstructive pulmonary disease. Curr Opin Infect Dis. 2004;17:113. doi:10.1097/00001432-200404000-00008
12. Li F, Yuan MZ, Wang L, et al. Characteristics and prognosis of pulmonary infection in patients with neurologic disease and hypoalbuminemia. Expert Rev Anti Infect Ther. 2015;13:521–526. doi:10.1586/14787210.2015.1019471
13. Matsusaka K, Kawakami G, Kamekawa H, et al. Pneumonia risks in bedridden patients receiving oral care and their screening tool: malnutrition and urinary tract infection-induced inflammation. Geriatr Gerontol Int. 2018;18:714–722. doi:10.1111/ggi.13236
14. Ignacio de Ulíbarri J, González-Madroño A, de Villar NG, et al. CONUT: a tool for controlling nutritional status. First validation in a hospital population. Nutr Hosp. 2005;20:38–45.
15. Lim JU, Lee JH, Kim JS, et al. Comparison of World Health Organization and Asia-Pacific body mass index classifications in COPD patients. Int J Chron Obstruct Pulmon Dis. 2017;12:2465–2475. doi:10.2147/COPD.S141295
16. Vestibo J, Edwards LD, Scanlon PD, et al. ECLIPSE investigators. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;465:1184–1192. doi:10.1056/NEJMoa1105482
17. Suzuki M, Makita H, Konnno S, et al. Hokkaido COPD Cohort Study Investigators. Asthma-like features and clinical course of chronic obstructive pulmonary disease. An analysis from the Hokkaido COPD cohort study. Am J Respir Crit Care Med. 2016;194:1358–1365. doi:10.1164/rccm.201602-0353OC
18. Takahashi S, Betsuyaku T. The chronic obstructive pulmonary disease comorbidity spectrum in Japan differs from that in western countries. Respir Investig. 2015;53:259–270. doi:10.1016/j.resinv.2015.05.005
19. Lin J, Xu Y, Wu X, et al. Risk factors associated with chronic obstructive pulmonary disease early readmission. Curr Med Res Opin. 2014;30:315–320. doi:10.1185/03007995.2013.858623
20. Global Initiative for Obstructive Lung Disease. GOLD 2019 report. Global strategy for the diagnosis, management and prevention of COPD; 2019 Report. Available from: https://goldcopd.org.
21. Zhao Z, Jiang C, Zhao D, et al. Two CHRN susceptibility variants for COPD are genetic determinants of emphysema and chest computed tomography manifestations in Chinese patients. Int J Chron Obstruct Pulmon Dis. 2017;12:1447–1455. doi:10.2147/COPD.S134010
22. Jackson SS, Dowling HF, Spiesman IG, et al. Transmission of the common cold to volunteers under controlled conditions. I. The common colds as a clinical entity. Arch Intern Med. 1958;101:267–278. doi:10.1001/archinte.1958.00260140099015
23. Jackson ML, Nelson JC, Jackson LA. Risk factors for community-acquired pneumonia in immunocompetent seniors. J Am Geriatr Soc. 2009;57:882–888. doi:10.1111/j.1532-5415.2009.02223.x
24. Tamada T, Sugiura H, Takahashi T, et al. Biomarker-based detection of asthma-COPD overlap syndrome in COPD populations. Int J Chron Obstruct Pulmon Dis. 2015;10:2169–2176. doi:10.2147/COPD.S88274
25. Haruna A, Muto S, Nakano Y, et al. CT scan findings of emphysema predict mortality in COPD. Chest. 2010;138:635–640. doi:10.1378/chest.09-2836
26. Lesourd BM. Nutrition and immunity in the elderly: modification of immune responses with nutritional treatments. Am J Clin Nutr. 1997;66:478S–484S. doi:10.1093/ajcn/66.2.478S
27. Ma JH, Song SH, Guo M, et al. Long-term exposure to PM2.5 lowers influenza virus resistance via down-regulating pulmonary macrophage Kdm6a and mediates histones modification in IL-6 and IFN-β promoter regions. Biochem Biophys Res Commun. 2017;493:1122–1128. doi:10.1016/j.bbrc.2017.09.013
28. Ozawa H, Asai S, Jin G, et al. Severe pneumonia caused by a novel influenza A (H1N1) virus in an asymptomatic emphysematous smoker. Intern Med. 2010;49:1667–1670. doi:10.2169/internalmedicine.49.3293
29. Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164:1618–1623. doi:10.1164/ajrccm.164.9.2105011
30. Wu Z, Yang D, Ge Z, et al. Body mass index of patients with chronic obstructive pulmonary disease is associated with pulmonary function and exacerbations: a retrospective real world research. J Thorac Dis. 2018;10:5086–5099. doi:10.21037/jtd.2018.08.67
31. Zhou Y, Wang X, Zeng X, et al. Positive benefits of theophylline in a randomized, double-blind, parallel-group, placebo-controlled study of low dose, slow-release theophylline in the treatment of COPD for 1 year. Respirology. 2006;11:603–610. doi:10.1111/j.1440-1843.2006.00897.x
32. Tatsumi K, Fukuchi Y, Study Group PEACE. Carbocisteine improves quality of life in patients with chronic obstructive pulmonary disease. J Am Geriatr Soc. 2007;55:1884–1886. doi:10.1111/j.1532-5415.2007.01373.x
33. Daviskas E, Anderson SD, Shaw J, et al. Mucociliary clearance in patients with chronic asthma: effects of β2 agonists. Respilorogy. 2005;10:426–435.
34. Singh D, Kolsum U, Brightling CE, et al. ECLIPSE investigators. Eosinophilic inflammation in COPD: prevalence and clinical characteristics. Eur Respir J. 2014;44:1697–1700. doi:10.1183/09031936.00162414
35. Tuncay EA, Karakurt Z, Aksoy E, et al. Eosinophilic and non-eosinophilic COPD patients with chronic respiratory failure: neutrophil-to-lymphocyte ratio as an exacerbation marker. Int J Chron Obstruct Pulmon Dis. 2017;12:3361–3370. doi:10.2147/COPD.S147261
36. Peduzzi P, Concato J, Feinstein AR, et al. Importance of events per independent variable in proportional hazards regression analysis. II. Accuracy and precision of regression estimates. J Clin Epidemiol. 1995;48:1503–1510. doi:10.1016/0895-4356(95)00048-8
37. Tatsumi K, Kasahara Y, Kurosu K, et al. Clinical phenotypes of COPD: results of a Japanese epidemiology survey. Respirology. 2004;9:331–336. doi:10.1111/j.1440-1843.2004.00611.x
38. Miyazaki M, Nakamura H, Chubachi S, et al. Analysis of comorbid factors that increase the COPD assessment test scores. Respir Res. 2014;15:13. doi:10.1186/1465-9921-15-13
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.