Back to Journals » Risk Management and Healthcare Policy » Volume 13
Magnitude of Needlestick and Sharp Injury and Its Associated Factors Among Nurses Working at Health Institutions in Western Ethiopia, 2020
Authors Abadiga M ![]() , Mosisa G, Abate Y
, Mosisa G, Abate Y
Received 19 March 2020
Accepted for publication 1 September 2020
Published 15 September 2020 Volume 2020:13 Pages 1589—1602
DOI https://doi.org/10.2147/RMHP.S254641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Muktar Abadiga,1 Getu Mosisa,1 Yonas Abate2
1School of Nursing and Midwifery, Institute of Health Sciences, Wollega University, Nekemte, Ethiopia; 2Oromia Regional Health Bureau, Nekemte Health Center, Nekemte Town, Ethiopia
Correspondence: Muktar Abadiga Abawaji, Po. Box: 395, Nekemte Email [email protected]
Background: Needlestick and sharp injury represent a major occupational hazard in the healthcare environment with nurses experiencing a large proportion of the burden. It is a potential for transmission of bloodborne pathogens including the human immunodeficiency virus, hepatitis B and C virus. Needlestick and sharp injuries are neglected and are often not reported. Few studies have been conducted in Ethiopia, and no study was conducted particularly in the Western part of a country. Therefore, this study aimed to assess needlestick and sharp injuries and associated factors among nurses working at health institutions in western Ethiopia, 2020.
Methods: An institutional based cross-sectional study was conducted on 297 nurses, from January 15 to 30, 2020. The study participants were selected by a simple random sampling method and data were collected using a self-administered questionnaire. Multivariable logistic regression was used to identify associated factors of needlestick and sharp injury. The association between needle stick and sharp injury and associated factors were measured using the odds ratio at a 95% confidence interval. The statistical significance was made at a p-value of less than 0.05.
Results: Out of 297 nurses who participated in the study, 100 (33.7%) had encountered needlestick and sharp injury in the past 12 months. Recapping the needle (AOR=3.99 95% CI: 2.20, 7.21), non-utilization of infection prevention guideline (AOR= 2.69, 95% CI: 1.29, 5.60), not taking injection safety training (AOR = 2.25, 95% CI: 1.22, 4.13) and having job-related stress (AOR= 1.93, 95% CI: 1.10, 3.41) were significantly associated with the needlestick and sharp injury.
Conclusion: In this study, the magnitude of needlestick and the sharp injury was high. The nurse should not recap the needles, should utilize infection prevention guidelines, should minimize stress, and routine injection safety training should be given to minimize needlestick and sharp injuries.
Keywords: needlestick and sharp injury, associated factors, nurses, western Ethiopia
Background
Needlestick and sharp injuries are common occupational hazards to healthcare workers, and it occurs when sharp instruments such as needle and other sharp materials penetrate the skin.1 Needlestick injury is defined as injuries that are caused by objects such as hypodermic needles, blood collection needles, cannula, and needles used to connect parts of intravenous delivery systems.2 It can also be defined as a piercing body trauma caused by sharp medical equipment that is potentially contaminated with the body fluid of another person.3
Nurses are important parts of clinical service providers and have a greater proportion of patient care compared to other health care workers in most health care settings.4 Due to the nature of their working environment, nurses are at high risk of occupational hazards and injuries.5 Literature also revealed that nurses are the commonest group of health care workers (HCW) experiencing needlestick and sharp injuries.6
Needlestick and sharp injuries usually happen during medication administration, operative procedures, blood sample collection, needle recapping, and poor handling and disposal of sharp materials.7,8 Universal precautions are important for the prevention of occupational exposures and for the handling of potentially infectious materials of blood and body fluids.9 Needlestick and sharp injuries can be prevented by improving the knowledge and practice of HCWs through a comprehensive program that addresses institutional, behavioral, and device-related factors that contribute to the occurrence of needlestick injuries.10
In the world, more than 35 million HCWs are suffering from occupational needle stick and sharp injury every year. From this, about 3 million HCWs are exposed to bloodborne viruses each year.11 According to the Royal College of Nursing survey, almost half of all nurses had been encountered needle and sharp injuries.12 The magnitude of needlestick and sharp injuries were 37.0% in the United Kingdom13 and 70.3% in Nepal.14 In the United States, the CDC reported that the annual number of sharp injuries among the HCWs is 385,000.15
About 90% of needlestick and sharp injuries occur in developing countries while in developed countries the attributed fraction was < 10%.16 According to the WHO report, the number of needlestick and sharp injuries per person among HCWs is 4 per year in Africa, Asia, and Western Mediterranean.17 In Sub-Saharan Africa, an average of two to four HCWs suffers needlestick injuries per year.18 In Ethiopia, the prevalence of needlesticks and sharp injury is 19.1% in Bale zone,19 34.5% in Dessie town,20 43% in Dessie referral hospital,21 and 25.9% in central zone of Tigray.22
The exposure to needlestick and sharp injuries causes infections, illness, disability, and death of HCWs including nurses.23 It is a potential for transmission of bloodborne pathogens including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV).24 Literature showed that needlestick and sharp injury is responsible for 39% of HCWs contracting HCV, 37.6% HBV, and 4.4% HIV infection.25 In addition to the risk of acquiring a serious infection, needlestick and sharp injuries can cause bleeding, minor surface scratches, and visible skin injuries.26
The risk of occupational transmission of bloodborne pathogens in the resource-limited setting is high due to unsafe practices, unavailability, and low coverage of vaccination against the bloodborne pathogens.27 In Ethiopia, available literature showed that the vaccination coverage of health workers against HBV is 12.9%.28 Factors such as irregular utilization of protective gear, recapping of needles, long working hours, working in an emergency department, and not taking infection prevention training were contributed to the occurrence of needlestick and sharp injuries.20–23,29,30 Hospital overcrowding, a lower ratio of HCWs to patients, and inadequate safety equipment were also associated with needlestick and sharp injuries.31–33
Despite the risk of transmission of infectious particles, needlestick, and sharp injuries are neglected and are often not reported.34 The Centers for disease control and prevention estimates that though HCWs sustain approximately 385,000 needlestick and sharp injuries annually, half of these injuries are unreported.35 Few studies have been conducted in Ethiopia and no study was conducted particularly in the Western part of a country. Therefore, this study was aimed to assess needlestick and sharp injuries and associated factors among nurses working at health institutions in western Ethiopia.
Methods
Study Design and Setting
This study was conducted on nurses working at health institutions in western Ethiopia. The study was conducted from January 15 to January 30, 2020, in selected health care facilities. Institutional-based cross-sectional study design was conducted on nurses working at health institutions in western Ethiopia. There were 17 hospitals (1 specialized hospital, 12 general hospitals, 4 primary hospitals), and 172 health centers in the study area during the time of the study. The total number of nurses working at health institutions in the study area was 1452 nurses. The source population was all nurses who are working at health institutions in western Ethiopia. The study population was the selected nurses who are working at least one year in the selected health institutions. All nurses working at public health institutions in western parts of Ethiopia were included in the study. Nurses who were on annual leave were not included in the study.
Sample Size Determination and Sampling Techniques
The sample size was calculated using the formula for the estimation of a single population proportion. An assumption of 95% Confidence Level (CL), marginal error (d) of 0.05, and 25.9% (0.259) proportion of past 12 months prevalence of needlesticks and sharp injury in the central zone of Tigray22 was used for sample size calculation. Finally, after adding a non-response rate of 5%, a total of 310 nurses were invited to take part in the study. Using a random sampling technique of lottery methods, representative health facilities were selected. First, the name of each hospital and health centers found in the study area were listed and coded with random numbers. Then, from 17 hospitals and 172 health centers found in the study area, 6 hospitals and 23 health centers were randomly selected and included in the study. The proportional allocation to each health care facility was done based on their population size of nurses. Finally, a simple random sampling method using the list of nurses from each working department of health institutions was used to select the study participants. Nurses who fulfilled the inclusion criteria were selected by simple random sampling technique using their list from each working department.
Measurement and Data Collection Procedure
A pretested structured self-administered questionnaire was used to collect data from the selected nurses. The questionnaires used in this study include various variables under dependent and independent variables. The dependent variable of the study was needlestick and sharp injury in the past 12 months and the independent variables were socio-demographic, work environment-related factors, and behavioral factors. Sociodemographic variables include sex, age, ethnicity, marital status, religion, educational status, monthly income, and work experience. Work environment-related factors include work institution, working department, shift work, supervision by other bodies, utilization of safety box and infection prevention guideline, recapping of a needle, injection safety training, and use of personal protective equipment. Behavioral factors include sleep disturbance, substance use, doing with assistance, perceived skill acquisition, job-related stress, satisfaction with the working environment, and perception of avoidability of NSSI. Nurses were considered encountered needle stick and sharp injury if they experienced at least one any piercing body trauma caused by sharp medical equipment in relation to his/her job in the health institution within the past 12months period. The outcome variable was asked as follows: “Have you ever experienced at least one needlestick or sharp injuries in relation to your job at your workplace within the past 12 months?” The response was coded as “yes” and “no”, indicating the presence or absence of needlestick and sharp injuries. A structured self-administered questionnaire was used to collect the data. The questionnaires were administered to the study participants by six trained BSc nurses and two MSc nurses as supervisors. The questionnaire was adapted from similar studies conducted on needlestick and sharp injury,19,20,22,36 and pretested before being used for this study. The data collection facilitators and supervisors were recruited from other health institutions and the data was collected for a duration of 15 days from January 15 to January 30, 2020.
Data Quality Control
The questionnaire was translated to the Afan Oromo language and then translated back to English by expertise to check for consistency. A pretest was done on 5% of the nurses who were working in other health institutions and some modifications were made. The one-day training was given for data collection facilitators and supervisors on the study instrument and data collection procedures. The supervisors also monitored data collection and checked the completeness of the questionnaire immediately after collection.
Data Processing and Analysis
The data were checked for completeness and consistency before data entry for analysis. Then, data were entered into Epi data version 3.1 and then exported to SPSS window version 20.0 for analysis. Descriptive statistics were done as univariate analysis and presented in the form of texts, tables, and figures. Bivariable logistic regression was conducted to find an association between each independent variable and needlestick and sharp injury. Multivariable logistic regression with backward elimination was used to identify associated factors of needlestick and sharp injury. The association was measured using odds ratio at a 95% confidence interval and the statistical significance was made at a p-value of less than 0.05. The result was presented using narration, tables, and figures.
Ethics Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Review Boards of Wollega University Ethical review board, institute of health sciences. Permission was also obtained from each respective health institution after clearly explaining the purpose of the study. After getting permission, all nurses were provided written consent, clearly stating the objectives of the study and their right to refuse. Then, written informed consent was obtained from each nurse. The filled questionnaires were carefully handled ensuring confidentiality and were kept under the secured custody of the corresponding author. The confidentiality of client-related data was maintained by avoiding potential identifiers and therefore, this study was conducted in accordance with the Declaration of Helsinki.
Results
Sociodemographic Characteristics of the Study Participants
Out of the total of 310 nurses invited to take part in the study, 297 were volunteered and participated in the study making a response rate of 95.8%. From these 297 nurses who participated in the study, 185 (62.3%) were males. Regarding the age of the study participants, 214 (72.1%) lie in the age group between 22–29 years. The majority of the study participants, 237 (79.8%) were Oromo in ethnicity. Concerning the religion, more than half, 202 (68%) were protestant. The majority of the study participants, 194 (65.3%) were married, 92 (31%) were single, 6 (2%) were divorced, and 5 (1.7%) were widowed. Concerning educational status, the majority of them, 237 (79.8%) were BSc degree holders, 50 (16.8%) were diploma and the rest 10 (3.4%) were master’s degrees and above. Regarding average monthly income, 32 (10.8%) of the respondents were earning less than or equal to 3000 EB, 127 (42.8%) were earning between 3001–4999 EB, 138 (46.5%) were earning a monthly income of 5000 and above EB. Concerning work experience, 121 (40.7%) had work experience of less than or equal to five years, 113 (38%) had work experience of 6–10 years and 63 (21.2%) had work experience of greater than 10 years (Table 1).
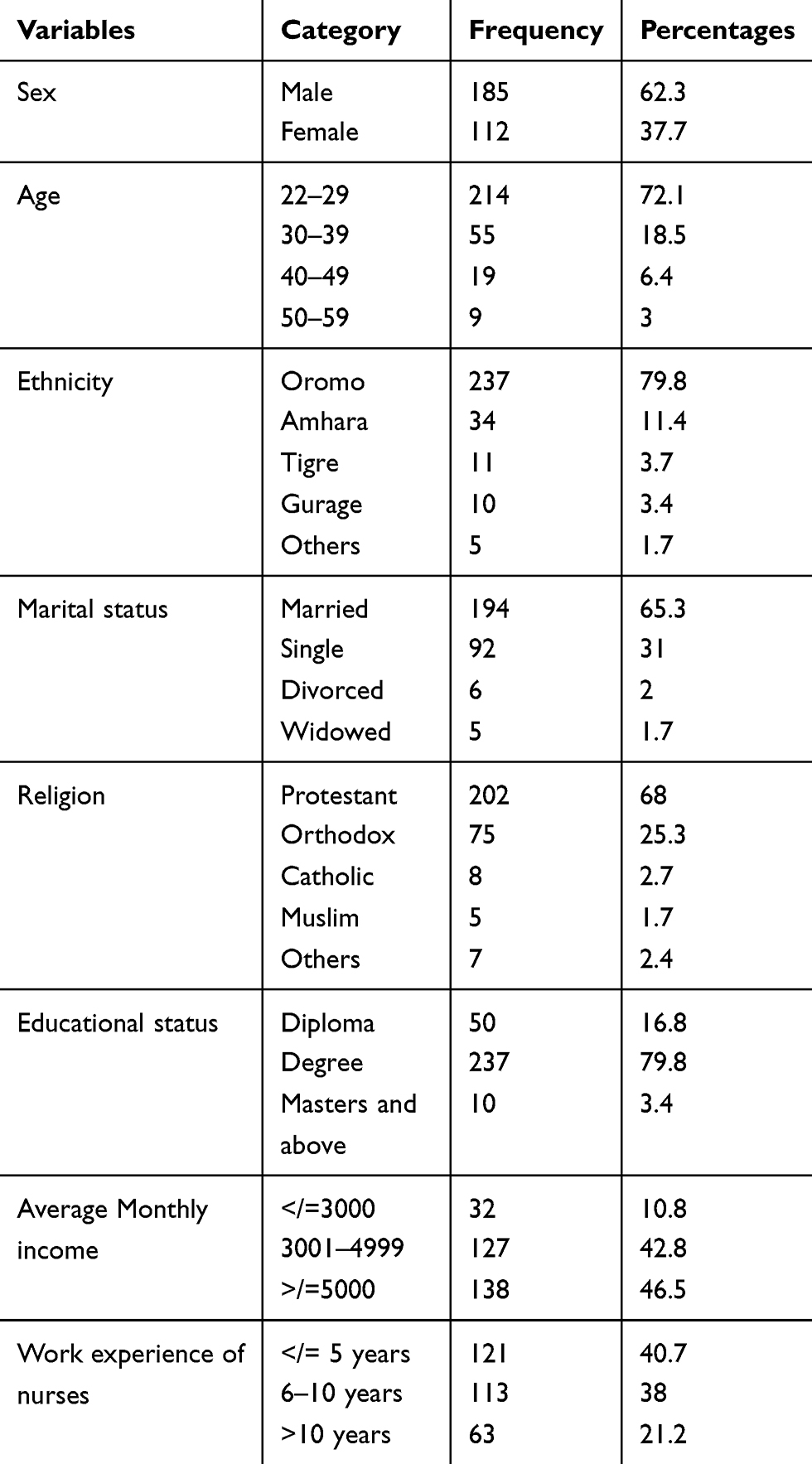 |
Table 1 Sociodemographic Characteristics of Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Health Care Providers’ Working Environment Related Characteristics
From a total of 297 nurses participated, 253 (85.2%) were working in hospitals and the remaining 44 (14.8%) were working in health centers. Fifty-seven (19.2%) of the nurses were working in the emergency department,75 (25.3%) were working in the outpatient department, 56 (18.9%) were working in the medical ward, 60 (20.2%) were working in the surgical ward, 36 (12.1%) were working in the pediatric ward and the remaining 13 (4.4%) were working in other departments. Regarding shift work, 173 (58.2%) had shift work. Two hundred forty-nine (83.8%) responded as there was supervision by other bodies. Two hundred eighty-four (95.6%) nurses utilize safety box and 241 (81.1%) reported utilization of infection prevention guidelines. Concerning the recapping of needles, 106 (35.7%) of the study participants reported recapping of the needle after injection or withdrawing blood. One hundred thirty-seven (46%) of the study participants had taken injection safety training. One hundred nighty-six (66%) of the respondents reported using personal protective equipment when they perform procedures. More than two-thirds of the study participants, 211 (71%) reported >/=40 working hours per week (Table 2).
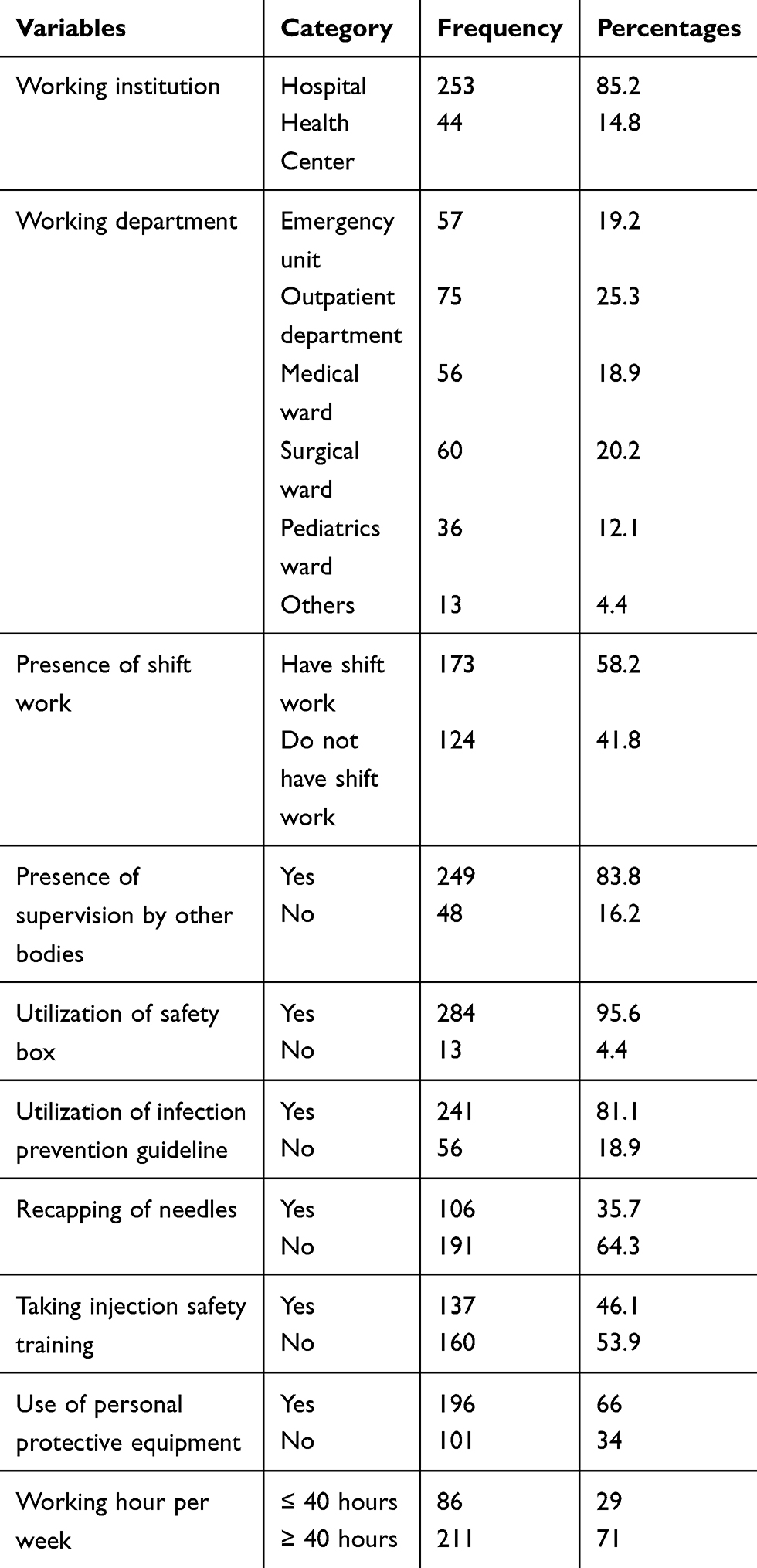 |
Table 2 Health Care Provider Working Environment Related Characteristics of Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Behavioral Related Characteristics of the Study Participants
About one third, 95 (32%) of the respondents reported as they had sleep disturbance. Seventy-two (24.2%) of nurses had reported current substance use and 178 (59.9%) had reported performing their work with assistance from senior nurses. Two hundred four (68.7%) had a perception that they have skill acquisition and about one third, 100 (33.7%) of the nurses had job-related stress. One hundred fifty-seven (52.9%) of the nurses had satisfaction with their working environment. The majority of the study participants, 240 (80.8%) had the perception that needlestick and sharp injuries are avoidable. Two hundred fifty-six (86.2%) of the study participants had perceived disease transmission by needlestick and sharp injuries are possible (Table 3).
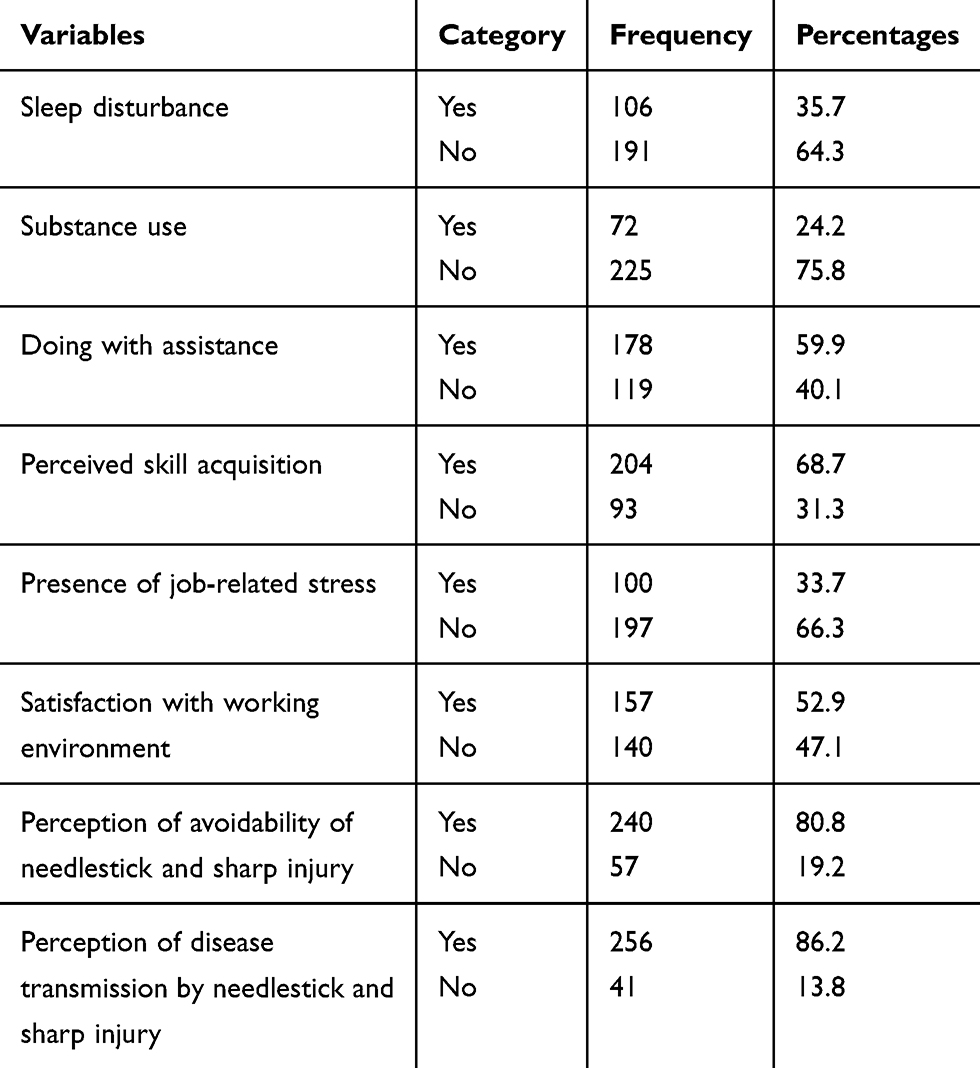 |
Table 3 Behavioral Related Characteristics of Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Needlestick and Sharp Injury-Related Characteristics
The magnitude of needlestick and the sharp injury was determined by asking the nurses if they had encountered at least one injury in the past 12 months. The nurses were considered encountering the injury if they experienced at least one injury in the past 12 months. Accordingly, from the total of the study participants, 100 (33.7%) had encountered needlestick and sharp injury in the past 12 months (Figure 1).
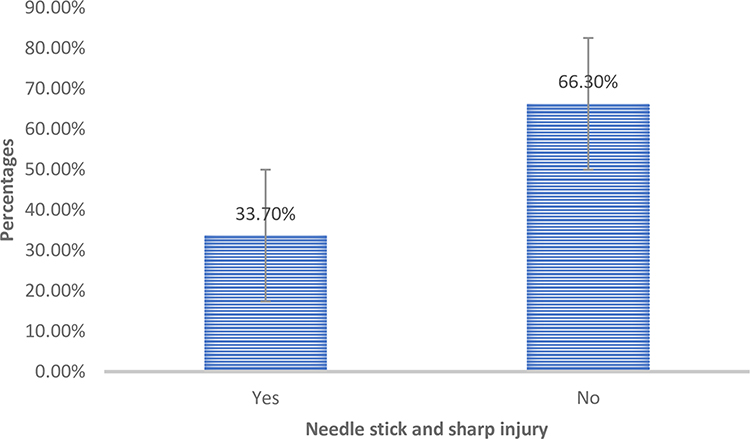 |
Figure 1 Magnitude of needlestick and sharp injury among nurses who participated in the study at health institutions in western Ethiopia, 2020. |
Regarding the frequency of the injury, 47 (15.8%) of the nurses encountered one time within the past 12 months, 38 (12.8%) encountered 2–4 times within the past 12 months, 10 (3.4%) encountered > 4 times within the past 12 months and 5 (1.7%) do not recall how often they encountered the injury. Regarding the type of injury encountered, 48 (16.2%) of the respondents had superficial needlestick or sharp injury, 36 (12.1%) had moderate needlestick or sharp injury and 16 (5.4%) had deep needlestick or sharp injury. Concerning the equipment that caused the injury, 55 (18.5%) of the respondents were injured by the needle, 14 (4.7%) were injured by surgical equipment, 20 (6.7%) were injured by medication vial or ampoule and 11 (3.7%) were injured by other objects. Thirty-four (11.4%) of the nurses had encountered NSSI while suturing wounds, 33 (11.1%) were injured while giving the injection, 10 (3.4%) were injured while recapping needle, 6 (2%) encountered NSSI while withdrawing blood sample and 17 (5.7%) were encountered the injury while performing other tasks. Seventy-three (24.6%) of the nurses who encountered NSSI had received care after the injury and 27 (9.1%) had not received care after the injury. Thirty-seven (12.5%) of the nurses have encountered the injury at the emergency unit, 11 (3.7%) at the outpatient department, 9 (3%) at the medical ward, 9 (3%) at the pediatric ward, 10 (3.4%) at the surgical ward, and 24 (8.1%) were encountered the injury at other departments (Table 4).
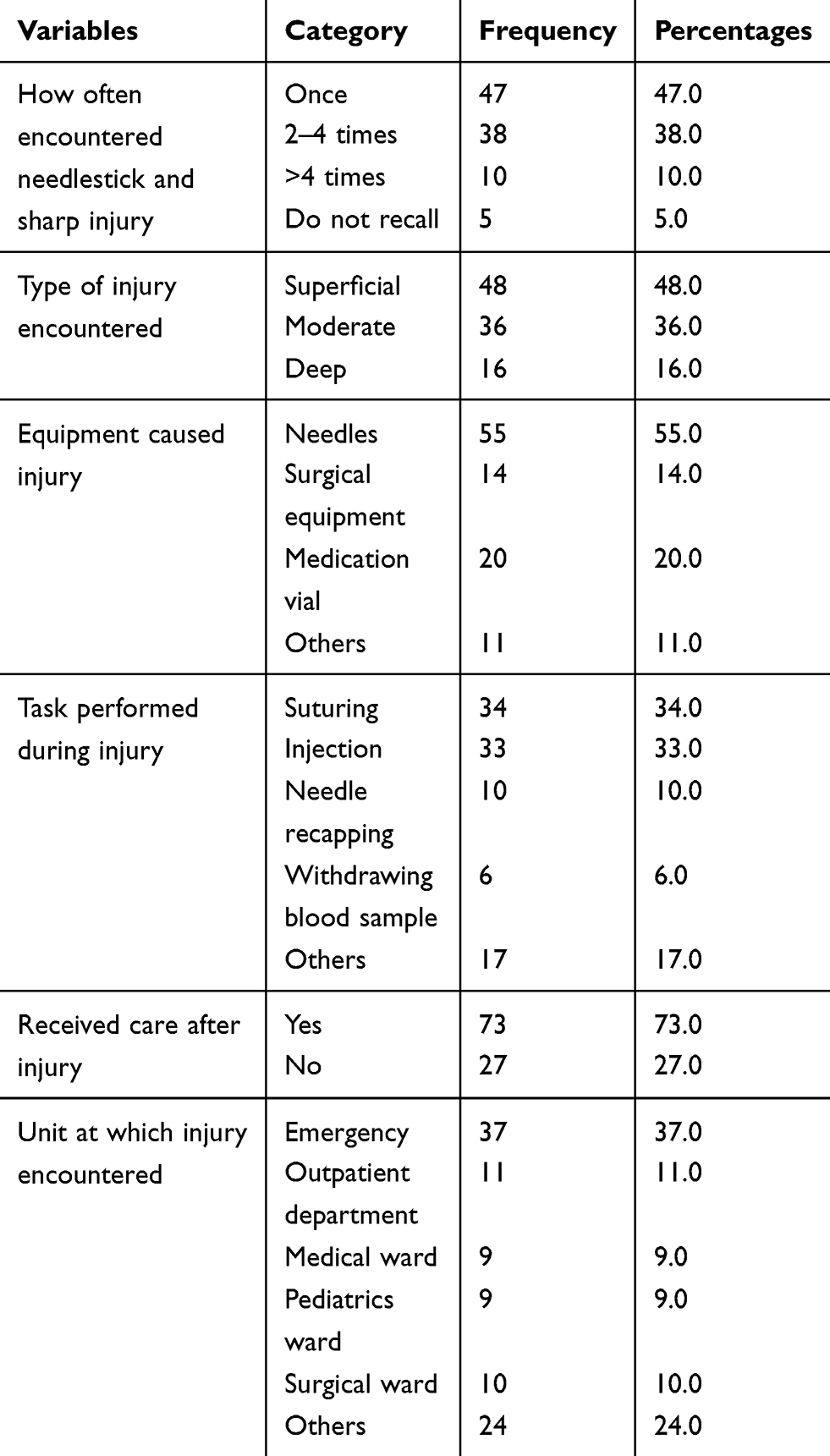 |
Table 4 Needlestick and Sharp Injury Related Characteristics of Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Bivariable Logistic Regression Analysis
Bivariable logistic regression was conducted to identify the association between needlestick and sharp injury and each independent variable. In bivariable logistic regression analysis, health care providers’ working environment related characteristics such as recapping of needles after utilization, not the utilization of infection prevention guidelines, not taking injection safety training, and not the utilization of personal protective equipment were associated with needlestick and sharp injury at P-value less than 0.25. In addition, behavioral related characteristics such as having sleep disturbance and the presence of job-related stress were associated with needlestick and sharp injury at P-value less than 0.25 (Table 5).
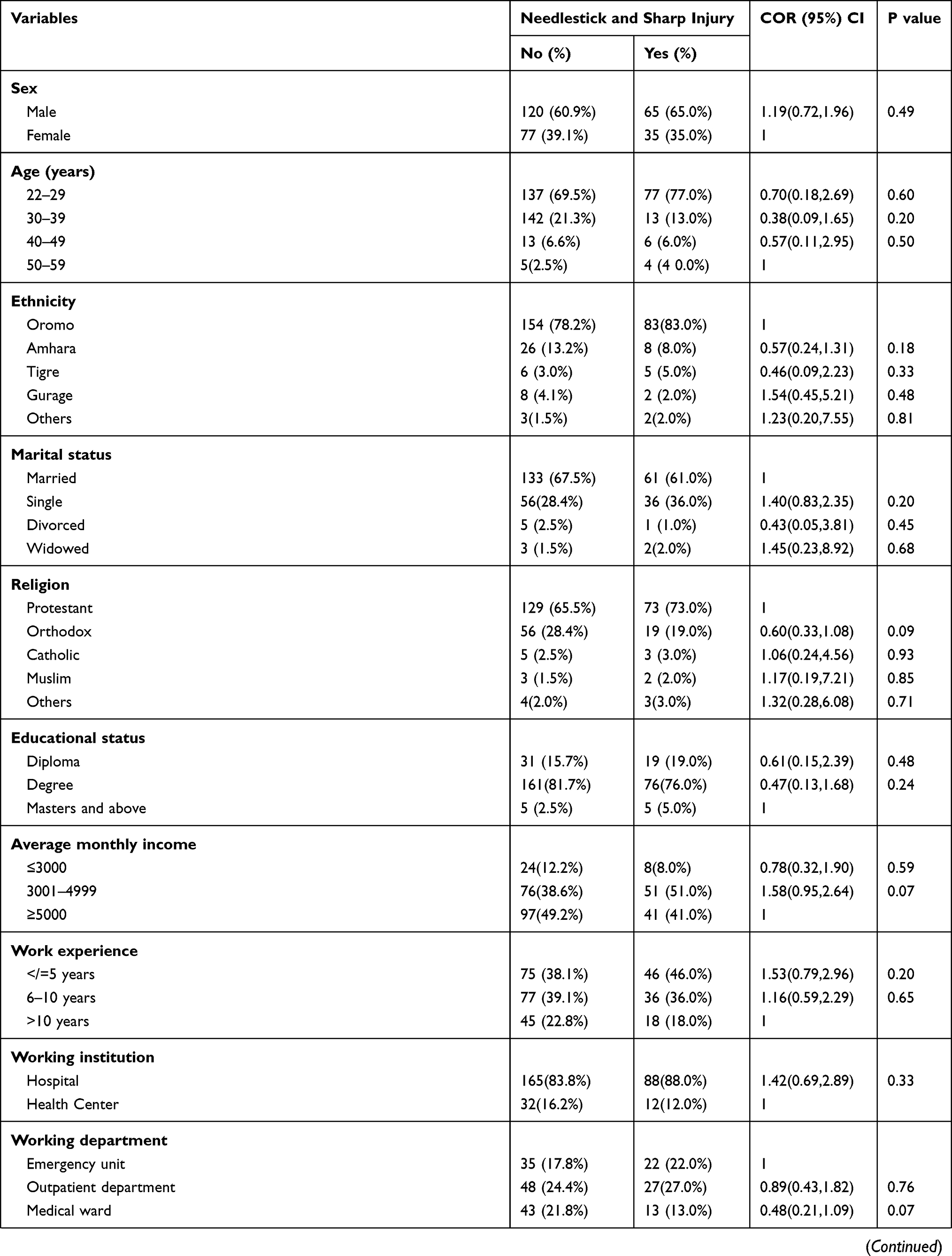 | 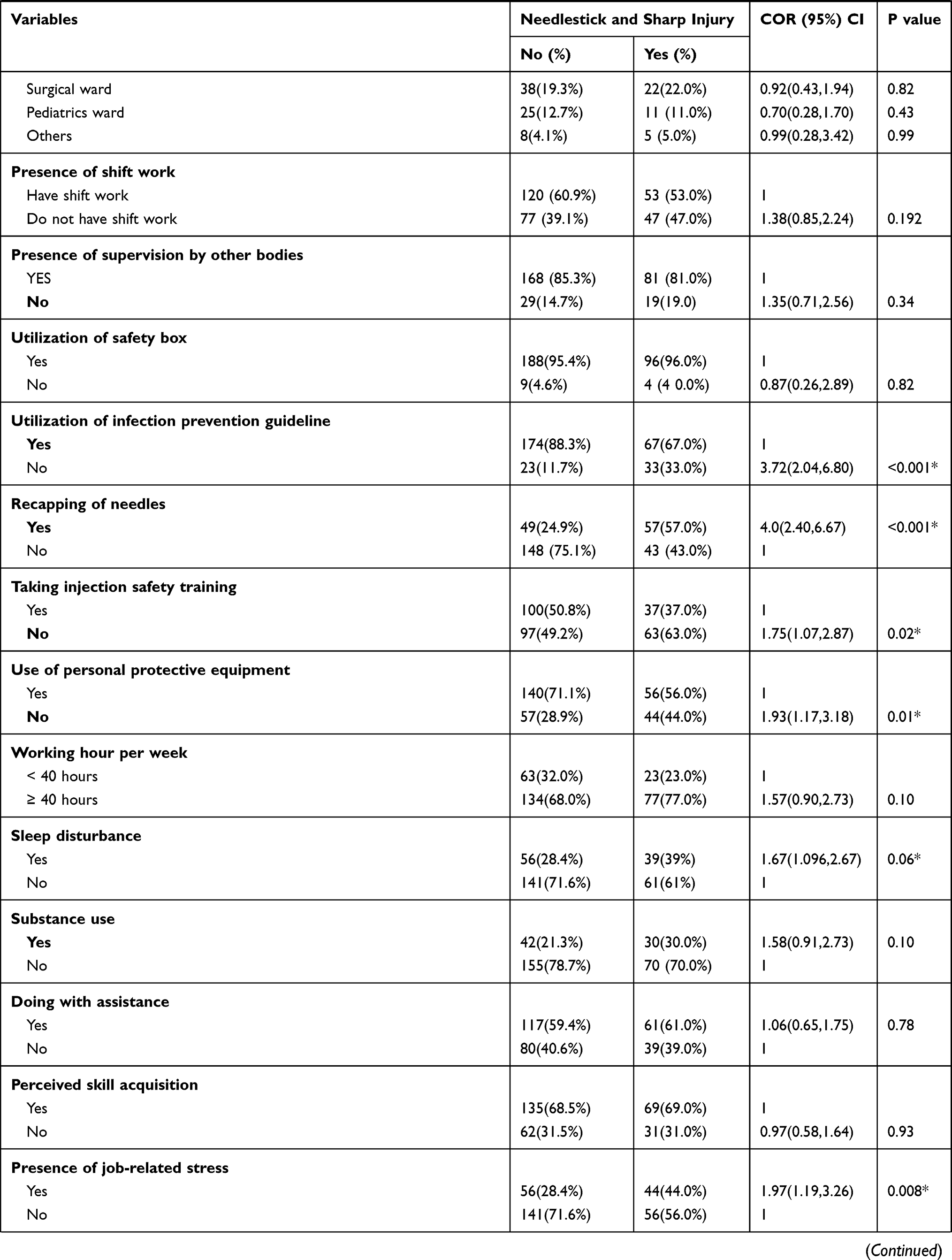 | 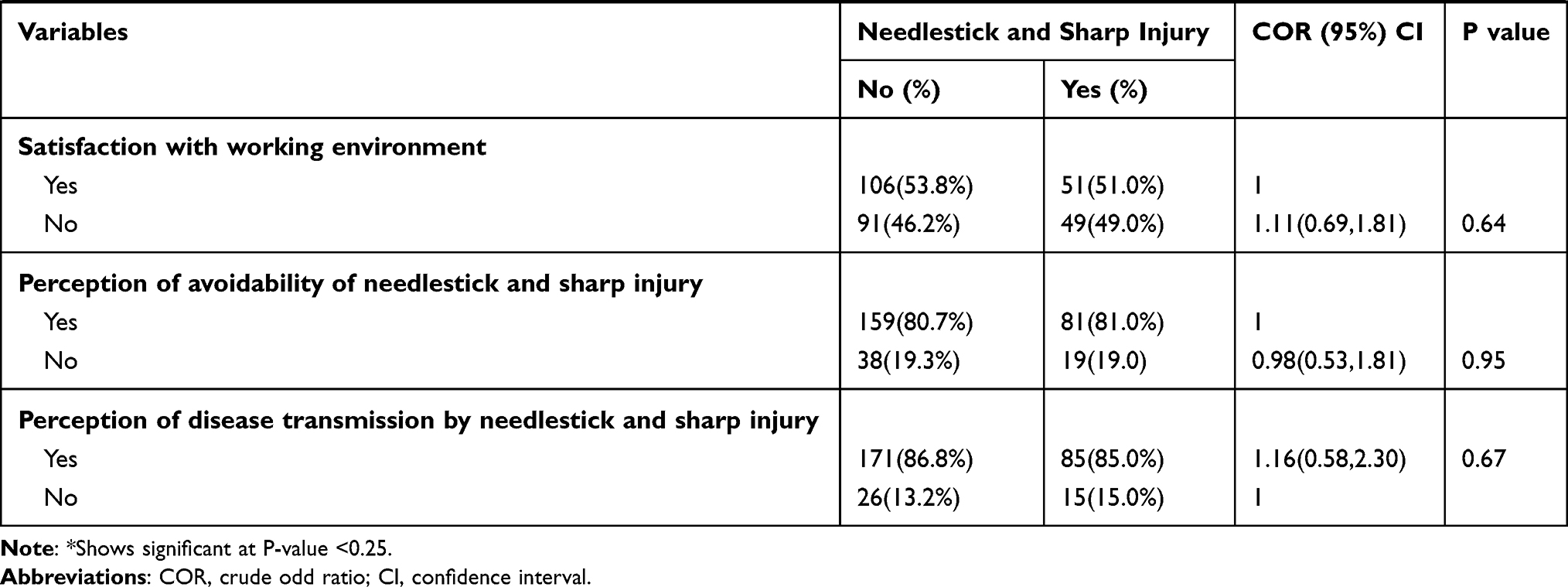 |
Table 5 Bivariable Logistic Regression Analysis of Factors Associated with Needlestick and Sharp Injury Among Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Multivariable Logistic Regression Analysis
The final model of logistic regression, variables such as non-utilization of infection prevention guidelines, recapping of needles, not taking injection safety training, and presence of job-related stress were associated with needlestick and sharp injury at P value less than 0.05. Nurses who do not utilize infection prevention guidelines were 2.69 times as likely to encounter needlestick and sharp injury than those who utilize infection prevention guidelines (Adjusted odd ratio= 2.69, 95% Confidence interval: 1.29, 5.60). Nurses who recap the needle after utilization were 3.99 times as likely to encounter needlestick and sharp injury than those who do not recap the needle (Adjusted odd ratio=3.99 95% Confidence interval: 2.20, 7.21). Nurses who have not taken injection safety training were 2.25 times as likely to encounter needlestick and sharp injury than those who have taken injection safety training (Adjusted odd ratio = 2.25, 95% Confidence interval: 1.22, 4.13). Nurses who have job-related stress were 1.93 times as likely to develop needlestick and sharp injury than those who do not experience job-related stress (Adjusted odd ratio = 1.93, 95% Confidence interval: 1.10, 3.41) (Table 6).
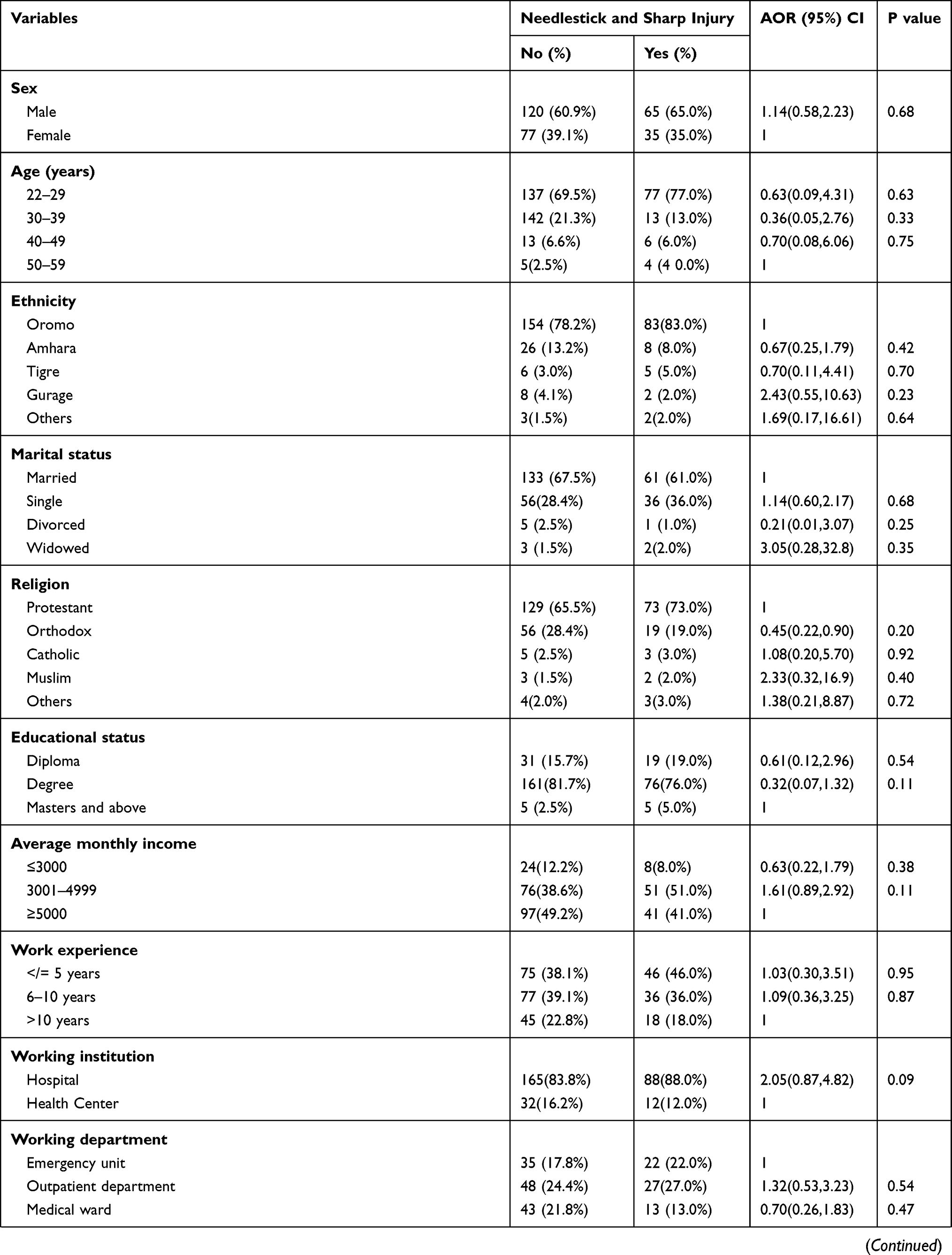 | 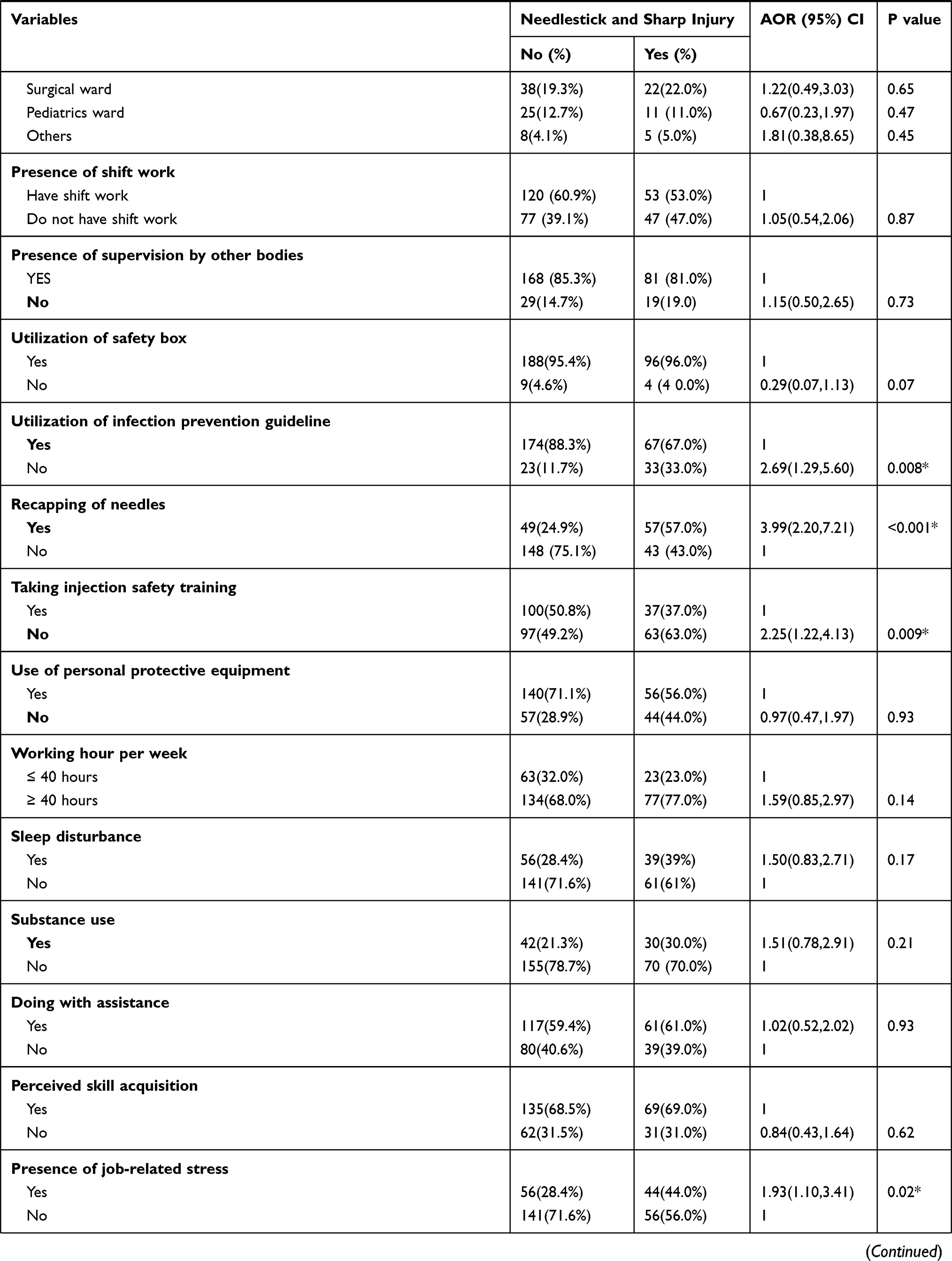 | 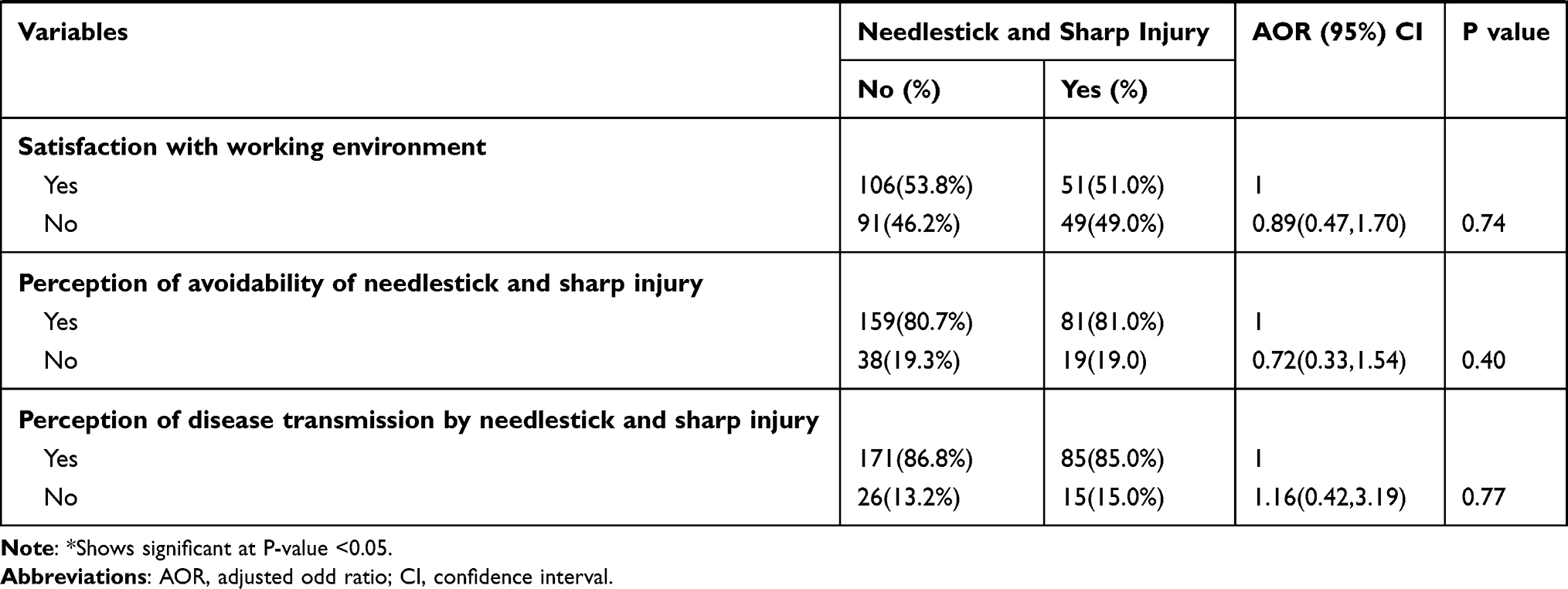 |
Table 6 Multivariable Logistic Regression Analysis of Factors Associated with Needlestick and Sharp Injury Among Nurses Who Participated in the Study at Health Institutions in Western Ethiopia, 2020 (n=297) |
Discussion
In the health care environment, needlestick and sharp injury represent the most common workplace health hazards.1 Nurses are the largest workforce in the health care setting and the most vulnerable group to occupational health hazards, particularly to needlestick and sharp injury.4,6 This study aimed to assess the magnitude and associated factors of needlestick and sharp injury among nurses working at health institutions in western Ethiopia.
The study result showed that about 100 (33.7%) nurses had encountered at least one needlestick and sharp injury in the past 12 months. This finding is comparable with the finding from Dessie town 34.5%,20 and greater than findings from East Gojjam 22.2%,37 North West Ethiopia 18.7%,38 Bale 19.1%,19 Dire Dawa 26.6%36 and Tigray 25.9%.22 On the other hand, the magnitude of needle stick and sharp injury in this study is lower than the finding from Turkey 44.3%39 and Dessie referral hospital 43%.21 The difference between the findings may be related to the variation of health care settings. So, with variation in the health care setting, availability of personal protective equipment, adequate sharp materials, and nurses to patient ratio varies. In addition, study participant’s skill, availability of up to date training on infection prevention, and culture of reporting encountered needlestick and sharp injury differs which might lead to variation in the magnitude of needlestick and sharp injury.
In this study, Nurses who do not utilize infection prevention guidelines were 2.69 times as likely to encounter needlestick and sharp injury than those who utilize infection prevention guidelines. This finding is consistent with the findings of the study conducted in North West Ethiopia,38 and Dessie town.20 This finding implies that there is a need to give more emphasis on infection prevention guidelines in health care settings. This finding shows that having infection prevention guidelines in every department and utilizing it can minimize the risk of needlestick and sharp injuries among the nurses and other health care workers.
Recapping of the needle after utilization is one of the contributing factors for the occurrence of needlestick injury. In this study, Nurses who recap the needle after utilization were 3.99 times as likely to encounter needlestick and sharp injury than those who do not recap the needle (Adjusted odd ratio=3.99 95% Confidence interval: 2.20, 7.21). Recapping needles is dangerous because it can result in accidental punctures, which can lead to exposure to infectious agents. This result is similar to the studies conducted in North West Ethiopia,38 Bale zone,19 DireDawa,36 Tigray,22 and Jimma Zone.40 The first step in preventing needlestick and sharp injuries should focus on efforts to eliminate the practice of recapping of the needles.
Training, particularly safety-related training plays a significant role to minimize hospital-related needle stick and sharp injuries. In this study, Nurses who have not taken injection safety training were 2.25 times as likely to encounter needlestick and sharp injury than those who have taken injection safety training (Adjusted odd ratio = 2.25, 95% Confidence interval: 1.22, 4.13). This finding suggests that effective training on the safety of injection may enhance awareness and improves the skills of nurses to reduce unsafe practices and the risk of needlestick and sharp injuries. Studies conducted in Dessie town,20 Tigray,22 and North West Ethiopia38 also showed similar findings with our current study.
Job-related stress also plays a major role in increasing the risk of needlestick and sharp injury. Nurses who have job-related stress were 1.93 times as likely to develop needlestick and sharp injury than those who do not experience job-related stress (Adjusted odd ratio = 1.93, 95% Confidence interval: 1.10, 3.41). This may be due to the fact that work-related stress can be damaging to a persons’ physical and mental health, while its high levels have been related to work-related injuries and low levels of productivity. Job-related stress results in loss of compassion for patients and an increased incidence of practice errors. This finding is in line with the studies conducted in East Gojjam37 and Dessie town.20
Limitation of the Study
Due to the cross-sectional nature of the data, the study cannot show the cause and effect relationship. Therefore, the relationship between needlestick and sharp injury and various independent variables cannot be considered as having direct cause and effect relationships. Lack of control groups and residual confounding may alter the associations between dependent and independent variables. Recall bias might be introduced because needlestick and the sharp injury was asked for the past 12 months. This means that the nurses might forget the experience of needlestick and sharp injury especially the type of injuries encountered. The nurses might not report the injury and therefore underreporting of the needlestick and sharp injury might be occurred in this study.
Conclusions
The result of this study indicated a high magnitude of needlestick and sharp injuries among nurses. Not utilizing infection prevention guidelines, recapping of needles, not taking injection safety training and the presence of job-related stress was associated with the needlestick and sharp injury. The nurse should adhere to infection prevention guidelines, should not recap the needles, should minimize job-related stress, and safety-related training should also be given to minimize and prevent the occurrence of needlestick and sharp injuries.
Abbreviations
AOR, adjusted odd ratio; CDC, communicable disease control; CI, confidence interval; HBV, hepatitis B virus; HCW, health care worker; HCV, hepatitis C Virus; HIV, human immunodeficiency virus; NSSI, needlestick and sharp injury; SPSS, statistical package for social science; WHO, World Health Organization.
Acknowledgment
We are grateful to the study participants who voluntarily agreed to be interviewed and participated in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that no competing interests in this work.
References
1. Deisenhammer S, Radon K, Nowak D, Reichert J. Needlestick injuries during medical training. J Hosp Infect. 2006;63:263–267. doi:10.1016/j.jhin.2006.01.019
2. Norsayani MY, Noor HI. Study on incidence of needlestick injury and factors associated with this problem among medical students. J Occup Health. 2003;45(3):172–178. doi:10.1539/joh.45.172
3. Zhang M, Wang H, Miao J, Du X, Li T, Wu Z. Occupational exposure to blood and body fluids among health care workers in a general hospital, China. Am J Ind Med. 2009;52(2):89–98. doi:10.1002/ajim.20645
4. Ramsay JA. The development and use of JHAs in the emergency department. J Saf Health Environ Res. 2005;2(2):2–18.
5. Senthil A, Anandh B, Jayachandran P, et al. Perception and prevalence of work-related health hazards among health care workers in public health facilities in southern India. Int J Occup Med Environ Health. 2015;21(1):74–81. doi:10.1179/2049396714Y.0000000096
6. Ng YW, Noor H. Needlestick injury among medical personnel in accident and emergency department of two teaching hospitals. Med J Malaysia. 2007;62:9
7. Foley M, Leyden A. American nurses association independent study module, needlestick safety and prevention, 2003. Sóttþann. 2012;2:3–6.
8. Rodrigues C. Needlestick injuries and the health care worker. Indian J Med Res. 2010;131:384–386.
9. Rapiti E, Prüss ÜA, Hutin Y. Sharps Injuries: Assessing the Burden of Disease from Sharps Injuries to Health-Care Workers at National and Local Levels. Geneva: WHO Environmental Burden of Disease Series; 2005.
10. Wang H, Fennie K, He G, Burgess J, Williams AB. “A training programme for prevention of occupational exposure to bloodborne pathogens: impact on knowledge, behaviour and incidence of needlestick injuries among student nurses in Changsha, People’sRepublic of China,”. J Adv Nurs. 2003;41(2):187–194.
11. Shiao J, Guo L, Laws ML. Estimation of the risk of blood borne pathogens to health-care workers after a needlestick injury in Taiwan. Am J Infect Control. 2005;30(1):15–20. doi:10.1067/mic.2002.119928
12. Royal College of Nursing. Needlestick injuries: the point of prevention. London, England: Author; 2009. Available from: http://www.rcn.org.uk/__data/assets/pdf_file/0007/230884/003313.pdf.
13. Saia M, Hofmann F, Sharman J, et al. Needlestick injuries: incidence and cost in the United States, United Kingdom, Germany, France, Italy, and Spain. Biomed Int. 2010;1:41–49.
14. Singh B, Paudel B, Kc S. Knowledge and practice of health care workers regarding needlestick injuries in a tertiary care center of Nepal. Kathmandu Univ Med J. 2015;51(3):230–233.
15. Centers for Disease Control and Prevention. Workbook for designing, implementing and evaluating a sharp injury prevention program. Atlanta: The Centers; 2008. Available from: www.cdc.gov/sharpssafety/pdf/sharpsworkbook_2008.pdf.
16. Sagoe MC, Pearson RD, Perry J, Jagger J. Risks to healthcare workers in developing countries. N Engl J Med. 2001;345(7):538–541. doi:10.1056/NEJM200108163450711
17. World Health Organization. The World Health Report. Geneva, Switzerland: WHO; 2012.
18. Nsubuga FM, Jaakkola MS. Needle stick injuries among nurses in sub-Saharan Africa. Trop Med Int Health. 2005;10(8):773–781. doi:10.1111/j.1365-3156.2005.01453.x
19. Bekele T, Gebremariam A, Kaso M, Ahmed K, Tang JW. Factors associated with occupational needlestick and sharps injuries among hospital healthcare workers in Bale Zone, Southeast Ethiopia. PLoS One. 2015;10(10):e0140382. doi:10.1371/journal.pone.0140382
20. Kebede A, Gerensea H. Prevalence of needlestick injury and its associated factors among nurses working in public hospitals of Dessie town, Northeast Ethiopia. BMC Res Notes. 2018;11:413. doi:10.1186/s13104-018-3529-9
21. Abebe AM, Kassaw MW, Shewangashaw NE. Prevalence of needle-stick and sharp object injuries and its associated factors among staff nurses in Dessie referral hospital Amhara region, Ethiopia. BMC Res Notes. 2018;11:840. doi:10.1186/s13104-018-3930-4
22. Weldesamuel E, Gebreyesus H, Beyene B, Teweldemedhin M, Welegebriel Z, Tetemke D. Assessment of needlestick and sharp injuries among health care workers in central zone of Tigray, northern Ethiopia. BMC Res Notes. 2019;12:654. doi:10.1186/s13104-019-4683-4
23. Bekele A, Kotisso B, Shiferaw S. Work-related operating theatre accidents among surgical residents in Addis Ababa, Ethiopia. East Cent Afr J Surg. 2008;13(1):27–33.
24. De Laune S. Risk reduction through testing, screening and infection control precautions with special emphasis on needlestick injuries. Infect Control Hosp Epidemiol. 1990;11(10):563–565. doi:10.2307/30145186
25. Nagandla K, Kumar K, Bhardwaj A, et al. Prevelence of needlestick Injuries and their under-reporting among health care workers in the departments of obstetrics and gynaecology. Inter Arc Med. 2015;18:8.
26. Kermode M, Jolley D, Langkham B, Tomas MS, Crofts N. Occupational exposure to blood and risk of blood borne virus infection among health care workers in rural north Indian health care settings. Am J Infect Control. 2005;33(4):34–41. doi:10.1016/j.ajic.2004.07.015
27. Sofola OO, Uti OG. Hepatitis B virus infection and prevention in the dental clinic: knowledge and factors determining vaccine uptake in a Nigerian dental hospital. Nig Q J Hosp Med. 2008;18(3):145–148.
28. Abebaw TA, Aderaw Z, Gebremichael B. Hepatitis B virus vaccination status and associated factors among health care workers in Shashemene Zonal Town, Shashemene, Ethiopia: a cross sectional study. BMC Res Notes. 2017;10:260. doi:10.1186/s13104-017-2582-0
29. Hanafi M, Mohamed AM, Kassem MS, Shawki M. Needlestick injuries among healthcare workers of University of Alexandria hospitals. East Mediterr Health J. 2011;17(1):26–35. doi:10.26719/2011.17.1.26
30. Kakizaki M, Ikeda N, Ali M, et al. Needlestick and sharps injuries among healthcare workers at public tertiary hospitals in an urban community in Mongolia. BMC Res Notes. 2011;4:184. doi:10.1186/1756-0500-4-184
31. Nelson R. Needlestick injuries: going but not gone: some hospitals still don’t get the point. Am J Nurs. 2004;104:25–26.
32. Vranes A, Jankovic S, Vranes B. Safety practice professional exposure to blood and blood-containing materials in Serbian health care workers. J Occup Health. 2006;48:377–382. doi:10.1539/joh.48.377
33. Chan M, Ho A, Christine M. Investigating the knowledge, attitudes and practice patterns of operating room staff towards standard and transmission-based precautions results of cluster analysis. J Clin Nurs. 2008;17:1051–1062.
34. Sharma GK, Gilson MM, Nathan H, Makary MA. Needlestick injuries among medical students: incidence and implications. Acad Med. 2009;84(12):1815–1821. doi:10.1097/ACM.0b013e3181bf9e5f
35. CDC. Sharps Injuries Stop Sticks Campaign. Centers for Disease Control and Prevention; National Institute for Occupational Safety and Health; 2010.
36. Mekonnen R, Yosef H, Teklegiorgis K, Tesfaye F, Dagne I. Magnitude and impact of occupational related needlestick and sharp injuries and associated factors among health care workers in Dire Dawa, Eastern Ethiopia. Med Saf Glob Health. 2018;7:1. doi:10.4172/2574-0407.1000141
37. Aderaw Z. Assessment on magnitude of needlestick and sharp injuries and associated factors among health care workers in East Gojjam Zone Health Institutions, Amahara Regional State, Ethiopia. Glob J Med Res Dis. 2013;13(3):41–49.
38. Dilie A, Amare D, Gualu T. Occupational exposure to needlestick and sharp injuries and associated factors among health care workers in Awi Zone, Amhara Regional State, Northwest Ethiopia. J Environ Public Health. 2017;2016. doi:10.1155/2017/2438713.
39. Akyol AD, Kargin C. Needlestick and sharp injuries among nurses. Glob J Nurs Forensic Stud. 2016;1:109. doi:10.4172/2572-0899.1000109
40. Bidira K, Woldie M, Nemera G. Prevalence and predictors of needlestick injury among nurses in public hospitals of Jimma Zone, South West Ethiopia. Int J Nurs Miwifery. 2014;6(7):90–96.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.