Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Magnitude of Depression and Associated Factors Among Patients on Tuberculosis Treatment at Public Health Facilities in Harari Regional State, Eastern Ethiopia: Multi-Center Cross-Sectional Study
Authors Abdurahman S, Yadeta TA, Ayana DA ![]() , Kure MA
, Kure MA ![]() , Ahmed J
, Ahmed J ![]() , Mehadi A
, Mehadi A ![]()
Received 14 April 2022
Accepted for publication 16 June 2022
Published 11 July 2022 Volume 2022:18 Pages 1405—1419
DOI https://doi.org/10.2147/NDT.S370795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Shame Abdurahman,1 Tesfaye Assebe Yadeta,2 Dasalegn Admassu Ayana,3 Mohammed Abdurke Kure,2 Jemal Ahmed,4 Ame Mehadi2
1Department of Public Health, Gorogutu Woreda Health Office, Kara-Mille, Oromia, Ethiopia; 2School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3School of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 4School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Ame Mehadi, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia, Tel +251919118839, Fax +251256668081, Email [email protected]
Background: Depression among tuberculosis patients remains a significant public health concern. Its burden and severity is increasing in low-income countries, especially in sub-Saharan Africa. Although it has negative impacts on quality of life, depression among tuberculosis patients is rarely studied in Ethiopia, particularly in the study area. Therefore, this study aimed to determine the magnitude of depression and associated factors among tuberculosis patients in Eastern Ethiopia.
Methods: A facility-based cross-sectional study was conducted from April 15 to May 15, 2021, among 213 tuberculosis patients in public health facilities of the Harari Regional State, Eastern Ethiopia. Study participants were selected using a systematic sampling technique. Data were collected using interviewer-administered questionnaire. Depression was assessed using Patients Health Questionnaire-9 (PHQ-9). Epi-data and SPSS were used for data processing and analysis. Bi-variable and multivariable logistic regressions were employed to determine the effects of predictors on depression. Statistical significance was considered at a p-value < 0.05.
Results: The magnitude of depression among tuberculosis patients was 52.1% [95% CI (45.4, 58.8%)]. Patient’s age of 25– 34 years [AOR = 0.31, 95% CI (0.128, 0.75)], female sex [AOR = 5.04; 95% CI (2.18, 11.62)], intensive phase of tuberculosis treatment [AOR = 2.56; 95% CI (1.118, 5.876)], HIV-positive status [AOR = 7.143; 95% CI (1.55, 32.93)], smoking history [AOR = 9.08; 95% CI (3.35, 24.61)] and having poor social support [AOR = 4.13; 95% CI (1.29, 13.22)] were factors statistically associated with depression.
Conclusion: In this study, the magnitude of depression was relatively high as more than half of the participants had depression. Advanced age, female sex, intensive phase of tuberculosis treatment, HIV-positive status, smoking history, and poor social support were identified as associated factors with depression. Therefore, this result calls all stakeholders to give duly emphasis on incorporating and integrating mental health support programs as routine practice in tuberculosis follow-up clinics, as screening, early detection and treatment, and training for all health care providers are very crucial in tackling depression among tuberculosis patients.
Keywords: magnitude, depression, tuberculosis, associated factors, Eastern Ethiopia
Introduction
The comorbidity of depression and tuberculosis (TB) is a growing public health problem globally and its severity increases in low- and middle-income countries.1,2 Depression is a common mental disorder characterized by sadness, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, feelings of tiredness, and poor concentration.2 It is the leading cause of disability worldwide, a major contributor to the global burden of disease, and can be long-lasting or recurrent, substantially impairing an individual’s ability to cope with daily life and can lead to suicide in its worst scenario.1,2
People with TB are often suffering from depression.1–6 The prevalence of depression among TB patients was reported variably in different countries. In Brazil (60.2%),7,8 Pakistan (56%),9 Cameron (61.1%),10 Angola (49.4%)11 and Nigeria (41.1%).12 In Ethiopia, 51.9% was reported from Eastern and 52.9% from Southcentral and Northern parts.13,14
Co-morbid depression, in people with TB, negatively affects timely diagnosis, service utilization, and adherence to treatment regimens, hinders good treatment outcomes, causes disability and poor quality of life, reduces social contact and social responsibilities, especially at the stage of coughing that leads to low self-esteem and hopelessness, delayed health care seeking, negative TB treatment outcomes like death and loss to follow-up, and poor treatment compliance that results in drug resistance, morbidity, and mortality.4,5,15–20
Several factors have been explained to be associated with depression among TB patients. The high prevalence of major depressive episode (MDE) in people with TB may be attributed to a combination of biological, social, and behavioral factors.15 Human Immune Deficient Virus (HIV) infection, poor social support, and perceived stigma have a higher risk of developing depression among TB patients.21,22 Being female, older ages, drug side effects, financial constraints, duration of illness, level of education, living in urban areas, having other comorbidities, and having had past anti-tuberculosis treatment were all significantly associated with depression.14,23,24
Despite the growing evolution of studies, the burden of depression among TB patients has not been well studied in Harari Regional State. Without addressing the burden of depressive illness among TB patients, adherence and prevention of disease transmission are bound to remain an enormous challenge. Therefore, this study aimed to determine the prevalence of depressive illness and associated factors among patients in TB treatment follow-up at Public Health Institutions of Harari regional state, eastern Ethiopia.
Conceptual Framework
This conceptual framework was developed after reviewing different related literature. The figure shows the factors associated with depression among TB patients. These independent variables have a direct and indirect contribution to depression among patients with TB (Supplementary File 1).
Methods and Materials
Study Setting, Period, and Design
A facility-based cross-sectional study was conducted from April 15 to May 15, 2021, in Harari Regional State public health institutions, Eastern Ethiopia. Harari Regional State, whose capital, Harar, is located 526 km away from Addis Ababa in the Eastern direction. According to the 2021 Ethiopian Central Statistical Agency population projection (based on the 2007 Census, CSA), the total population of the region was 270,000 of which 136,000(50.37%) were males and the majority 151,200(56%) of people were urban dwellers, unlike most other regions in Ethiopia. and the majority 151,200 (56%) of people were urban dwellers, unlike most other regions in Ethiopia. According to the Regional Health Bureau, the health worker per 1000 population ratio is 2.8. The region has two public hospitals, one Federal Police Hospital, one private General hospital, eight government health centers, 34 health posts, and one Family Guidance Association.
Population, Eligibility Criteria, and Sampling Procedure
Two hundred and thirteen TB patients who were under anti TB treatments for more than one month (after starting medication for a month) and who attended selected health institutions during the study period and ≥18 years of age have participated in this study. All TB patients, who were seriously ill (unable to provide required information), had hearing and communication problems, those on treatment for less than a month, and those who had completed treatment were excluded from the study.
Two public hospitals and five health centers were selected randomly (by lottery method) from 10 public health facilities in the region, then proportional allocation was used to select study participants. Accordingly, 52 patients were selected from Jugol General Hospital, 65 from Hiwot Fana Comprehensive Specialized Hospital (HFCSH), and 18, 20, 14, 24, and 20 participants were selected from, Amir Nur, Aboker, Jinella, Hakim, and Hassengay health centers, respectively. The first participant was selected randomly using the patient’s serial number of the registration book during follow-up and the consecutive participants were selected by systematic random sampling (K=N/n=2 intervals) until the final sample size was obtained. The detailed sampling procedure is shown in Figure 1.
 |
Figure 1 Flow diagram of sampling procedure to select patients with tuberculosis attending Harari Region Public Health Institutions, Eastern Ethiopia, 2021 (n= 213). |
The required sample size was determined using the single population proportion formula by considering a 95% of confidence level, 5% margin of error, 10% non-response rate, and 51.9% prevalence of depression among TB patients: from a previous study.13 The calculated sample size was 422 and the total number of TB patients on follow-up at public health facilities in the study area was 432. Since the number (432) of TB patients on follow-up was less than 10,000, the final sample size was adjusted by the population correction formula yielding a final sample size of 213. The sample size for the second objective was calculated using Epi–info version 7 software. Finally, the sample size for the first objective was larger than that for the second objective. Therefore, the sample size for the first objective, 213, was used to capture an appropriate sample for both study objectives.
Data Collection Procedure
The data were collected in the local language of the patients by seven nurses using face-to-face interviews after informed voluntary and signed consent were obtained in regular TB clinics. Review of documents, patients’ TB cards, registration books, and medical files were also used to obtain some of the baseline information.
Structured pretested interviewer-administered questionnaire was used to collect data, and it has four components: The first part contains: participants’ socio-demographic characteristics and clinical conditions; the second part contains: patient health questionnaire-9 (PHQ-9) depression scale, the third part contains: Oslo social support scale and the fourth part contains: perceived TB stigma scale.25 The outcome variable (Depression) was measured using the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is a self-report Questionnaire developed based on the 9 depressive symptoms and designed to screen for depression in primary care and other medical care settings.38 It has 9 items, and each item has a 4-point Likert scale (0 = not at all, 1 = several days, 2 = more than half the days, and 3 = nearly every day). Summary scores ranged from 0 to 27. Depression was defined using a score of 10 or higher, a well-validated cut point used in health care settings.25,26 The PHQ-9 has been previously used and formally validated in Ethiopia in many different studies in different settings. PHQ-9 is also culturally validated in the Ethiopian context with specificity and sensitivity of 67% and 86%, respectively.13,14,25 It was found reliable (Cronbach’s α=0.91) in the current study. Social support was assessed by a 3-item Oslo social support scale, which ranges from 3 to 14. Oslo-3 has three categories: a score of 3–8 is poor support, 9–11 moderate support, and 12–14 strong support. It was reliable in the study (Cronbach’s α = 0.91).14,25,27 It had Cronbach’s α = 0.85 in the current study. The Stigma felt by TB patients was assessed by using a 12-item perceived TB stigma scale; consisting of a 4-point Likert scale (strongly disagree, disagree, agree, strongly agree) questions concerning perceived isolation, shame, guilt, and disclosure of the TB status.25,27 The item scores of the stigma questions were summed up to construct a single stigma variable. Respondents were classified as having or not having perceived TB stigma using the mean score of the stigma scale as a cutoff point which was highly reliable in the study (Cronbach’s α = 0.89).17,27 It was found reliable (Cronbach’s α=0.91) in the current study. All the above instruments were adopted and translated to the local language (Amharic and Afan Oromo) language and then translated back to English by a language expert to check for consistency.
Study Variables and Measurements
Dependent variable: In this study, the outcome variable was Depression among TB patients. Independent variables: in this study, the explanatory variables were categorized as: Demographic factors (age, sex, ethnicity, religion, marital status, occupational status, educational status, residence, family size, family income), Health-related factors (Health-related issues chronic medical illnesses/Comorbidity (Diabetes, Hypertension, HIV/AIDS, cardiac disease), drug of chronic illness (isoniazid, cycloserine)), Clinical factors (phase of TB treatment, Family history of depression, Type of tuberculosis, Category of TB treatment, TB treatment duration, TB illness severity) and Psycho-Social factors (Perceived TB Stigma/Stigmatizing, Substance use, Prior psycho-social experiences, Social Support).
Operational Definitions
Depression is based on the PHQ-9 depression scale classified as 0–4 no depression, 5–9 Mild depression, 10–14 Moderate depression, 15–19 Moderately severe depression, and 20–27 Severe depression.25,26 Social support is based on Oslo social support scale, with scores of 3–8 as poor support, 9–11 as moderate support, and 12–14 as strong support.14,25,27 Current Alcohol user: refers to an individual who had used alcohol drinks in the past three months.25,26 Current khat chewer is an individual who had used khat continuously or daily in the past three months.14,25,27 Current Cigarette Smoker refers to an individual who had used cigarettes daily in the past three months.28 Perceived TB stigma Scale is based on a 12-items scale and the scores of the stigma questions were summed to construct a single stigma variable that is classified as having or not having perceived TB stigma using the mean of the stigma scale as a cutoff point.17,27
Data Quality Control
The data collection instruments/questionnaire has been developed after reviewing the relevant literature on the subject to include all the possible variables that address the objective of the study. The questionnaire was first prepared in English and translated into local languages (Amharic and Afan Oromo) then translated back to English by a language expert to check for consistency. The data were collected by trained data collectors and supervisors. Two-day training was given to data collectors and supervisors on the objectives of the study, the contents of the questionnaire, and particularly on issues related to the confidentiality of the responses and the rights of respondents. A pre-test was conducted on 5% of study participants one week before the actual data collection, was done at Federal Police General Hospital and Erer Health Center on TB patients. Both health facilities and TB patients selected for pre-test were not part of the study. Continuous supervision of the data collection process was carried out by trained supervisors. The collected data were rechecked daily to ensure completeness and consistency. All questionnaires were reviewed, checked for errors and incompleteness at the end of each day.
Data Processing and Analysis
The socio-demographic, biological/clinical factors, health-related, and illness variables were double entered into Epi-data version 3.1 and exported to SPSS version 22 for further analysis. The data were sorted, summarized, cleaned, and checked for missing values using frequencies and cross-tabulations. Description of means, frequencies, and proportion of the given data for each variable was calculated. Descriptive statistics (cross tab) was also done to identify tuberculosis patients with depression and without depression and its magnitude. Bivariate analysis was done to see the association of each independent variable with the outcome variable. Those variables having a p-value less than 0.25 were entered into a multivariable logistic regression model to identify the effect of each independent variable with the dependent variables upon controlling confounding factors. A p-value of less than 0.05 was considered to be statistically significant, and an adjusted odds ratio with 95% CI was calculated to measure the strength of the association and identify associated factors of depression among TB patients.
Ethical Consideration
This study was conducted according to the Declaration of Ethical Approval secured by Haramaya University College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (IHRERC). After submission of a formal support letter obtained from IHRERC to Harari Regional Health Bureau and selected health institutions; Informed, voluntary written and signed consent was obtained from the head of selected health institutions and all participants prior to data collection.
Results
Socio-Demographic Characteristics of Study Participants
A total of 213 tuberculosis patients participated in the study. The mean age of the participants was 36.38 years (±13.82SD) ranging from 18 to 80 years old and nearly half 106 (49.8%) were below 35 years of age. More than half of the participants were male 114 (61.24%), 121 (56.8%) were Oromo, 127 (59.6%) were Muslim, 113 (53.1%) were married, 93 (43.7%) were farmers or daily laborers, 149 (70%) were urban residents and 73 (34.3%) were primary school educated (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Tuberculosis Patients Attending Harari Region Public Health Institution, Eastern Ethiopia, from April 15 to May 15, 2021 (n = 213) |
Clinical, Health, and Treatment-Related Characteristics of Study Participants
One hundred fifty-five (72.8%) patients were diagnosed with pulmonary TB. The majority of respondents, 149 (70.0%) were in the new TB treatment category, while 16 (7.5%) were MDR-TB and 126 (59.2%) were in the continuation phase of TB treatment. The majority of respondents (70.9%) rated their TB illness as mild-to-moderate type, 32 (15.0%) had comorbid HIV illness and 28 (13.1%) had a family history of mental illness. Regarding drug regimens, 32 (15.0%), 16 (7.5%), and 32 (15.0%) were on Isoniazid, Cycloserine, and ART drugs, respectively, while 39 (18.3%) of the participants missed their Anti-TB medication and all of them, 39 (18.3%), missed drugs more than one day (Table 2).
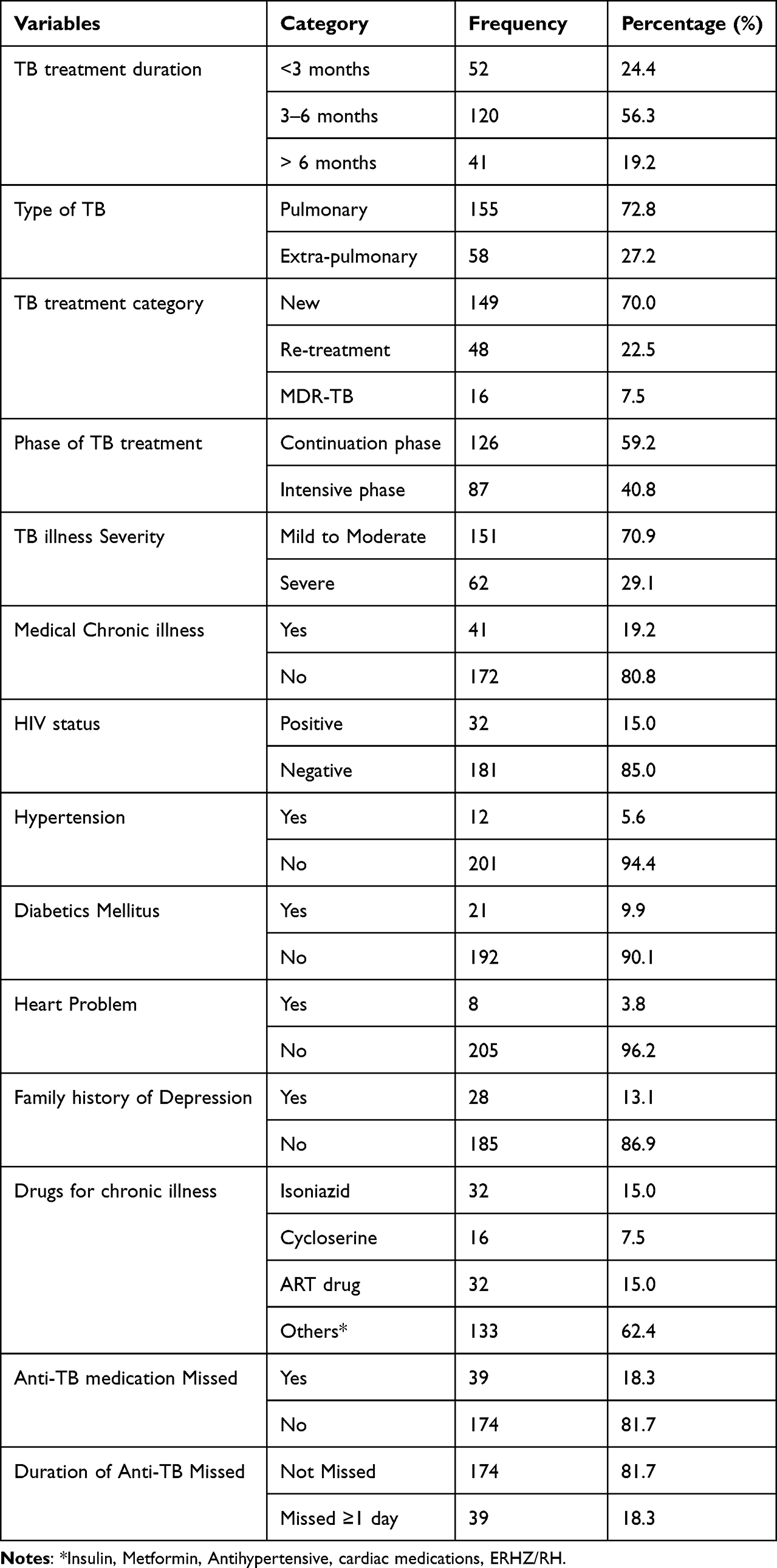 |
Table 2 Clinical, Health, and Treatment-Related Factors Among TB Patients in Public Health Institution of Harari Regional State, Eastern Ethiopia, 2021 |
Substance Use and Psycho-Social Characteristics of Study Participants
Substance use was reported by 125 (58.7%) of the respondents; of which 79 (37.1%), 93 (43.7%), and 114 (53.5%) had reported drinking alcohol, cigarettes smoking, and chewing khat, respectively, during the study period. Poor social support and perceived TB stigma were reported by 93 (43.7%) and 117 (54.9%) of the respondents, respectively (Table 3).
 |
Table 3 Psycho-Social and Substance Use Factors Among TB Patients in Public Health Institution of Harari Regional State, Eastern Ethiopia, 2021 |
The Magnitude of Depression Among Tuberculosis Patients
The prevalence of probable depression among TB patients was found to be 52.1% (95% CI = 45.4, 58.8%) in this study (Figure 2). Among study participants who revealed depression, the majority 76 (35.7%) were with Mild Depression (Table 4).
 |
Table 4 Depression Score Among Tuberculosis Patients Attending Harari Region Public Health Institution, Eastern Ethiopia, 2021 (n = 213) |
 |
Figure 2 Magnitude of depression among tuberculosis patients attending Harari Region Public Health Institutions, Eastern Ethiopia, from April 15 to May 15, 2021 (n=213). |
Factors Associated with Depression Among Tuberculosis Patients
In bivariate analysis, variables being age, sex, TB treatment duration, TB treatment category, phase of TB treatment, HIV comorbid, smoking, number of packets smoked per day, drinking alcohol, frequency of drinking alcohol per week, number of bottles/cups of drinking alcohol, frequency of chewing khat per week, Oslo social support scale and perceived TB stigma scale were significantly associated with depression. All variables having a p-value of less than 0.25 were entered into a multivariable analysis (Table 5).
 |
Table 5 Bivariate and Multivariate Analysis of Factors Associated with Depression Among Tuberculosis Patients Attending Harari Region Public Health Institution, Eastern Ethiopia, 2021 (N = 213) |
In multivariate analysis, depression was 68.9% less frequent among the age groups of 25–34 years old than those in the age groups of 35 and above years [AOR = 0.31, 95% CI (0.13, 0.75)]. Regarding genders, females were 5.04 times more likely develop depression than males [AOR = 5.04; 95% CI (2.18, 11.62)]. Moreover, patients in the intensive phase of TB treatment were 2.56 times more frequent to have depression as compared with those in the continuation phase of TB treatment [AOR = 2.56; 95% CI (1.12, 5.88)]. Similarly, depression was 7.14 times higher among HIV-positive patients than in their counterparts (HIV-negative patients) [AOR = 7.14; 95% CI(1.55, 32.93)]. Likewise, cigarette smokers were 9.08 times more frequently depressed than non-smokers [AOR = 9.08; 95% CI (3.35, 24.61)]. Finally, poor social support was 4.13 times more frequently associated with depression as compared to those who had strong social support [AOR = 4.13; 95% CI(1.29, 13.22)] (Table 5).
Discussion
The magnitude of depression among tuberculosis patients was found to be 52.1% in this study. This finding was consistent with other studies conducted in Eastern Ethiopia (51.9%),13 South Central Ethiopia (the Silte and Gurage zones) and northern Ethiopia (Bahir Dar zone) (52.9%)14 and Southern Ethiopia (54%),7 Brazil (60.2%),8 Pakistan (56%),9 and Cameron (61.1%).10
A higher magnitude of depression than that of the current study was reported in two studies carried out in Pakistan (72.2%)29 (80%).30 Unlike the current study, a lower magnitude of depression was reported in studies done in Wolayta Sodo (43.4%)27 and Addis Ababa (31.1%),25 Ethiopia, and Nigeria (41.1%).12 This might be due to variation in the study area, study design, sample size, the population studied, and the screening tools used.
In this study, the severity of depression was classified into five categories based on the patient health questionnaire-9 (PHQ-9) and ranges from mild to the most severe form that may need critical treatment. Accordingly, 45.6% of the TB patients were identified with mild-to-moderate depression, while a few (6.6%) had a severe form of depression that requires appropriate treatments. This finding was comparable with other studies, such as the Ethiopian study carried out in eastern Ethiopia revealing 49.1% mild to moderate and 2.7% severe form.13 Identifying the severity of depression among TB patients may be essential to tackle negative TB-treatment outcomes, poor anti-TB drug adherence, which may in turn increase the risk of drug resistance, poor quality of life and disability associated with severe forms of depression.13,14
In this study, the ages of TB patients were found to be significantly associated with depression, revealing that older ages were highly affected by depression. Being above 35 years was more associated with depression compared to being aged between 25 and 34 years, which was 68.9% protective for depression. This is in agreement with other studies.13,14,23,31 The possible reason for this may be a young people may engage in different activities to earn money, which may increase social interaction and most probably get support from colleagues or relatives. At an older age, living in poor countries may be challenging as the habit of saving was low, and engagement in economical activities may be stressful besides the challenges of TB like stigma, discrimination, and anti-TB side effects.23 These stressful life events and chronicity of TB were associated with depression in studies conducted in Southern Ethiopia. Research has shown that for every 14 years increase in age, the risk of having depression increases by 19.0%; however, the reasons are not clear.13,14
Consistent with other studies,2,8,10,25,27,32–35 being female was five times more likely to be associated with depression. This could be due to the higher global prevalence of depression among women in the general population, biological factors like hormonal fluctuation with pregnancy and menstruation, and social factors like the burden of household responsibilities and the social roles of women in society.2,36
Being in the intensive phase of TB treatment was found to be significantly associated with depression in this study, this finding is in line with other studies.26,37 This might be related to the severity of illness as symptoms of TB tend to be more prominent during the intensive phase and likely to improve over time during the continuation phase.37 This could be because the symptoms of tuberculosis tend to be worse in the intensive phase compared to the continuation phase of TB treatment. Probably, coughing, chest pain, night sweats, and fevers affect an individual’s quality of life in terms of sleep, appetite, and self-esteem hence more chances of one being depressed. However, depression can also increase the severity of the physical symptoms of TB.26
In agreement with other studies,10,26,27 HIV-positive status was found to be strongly associated with depression. HIV-positive patients were seven times more likely to be depressed than their counterparts. This might be because HIV infection itself is associated with depression. Being diagnosed with HIV, which is a terminal life-long disease associated with high levels of stigma, may also lead to high rates of mental disorders. Hence, TB and HIV co-infected patients can be at higher risk of common mental disorders as a result of stigma and discrimination by society.26
In current study, depression was nine times more frequent among cigarette smokers compared to non-smokers, and this finding is in line with other studies.28,31 This might be because depression is higher among substance users as compared to non-users.31
Furthermore, the study indicated that depression was four times more likely among TB patients who had poor social support than in those who had strong social support, this is supported by other studies.25,27 The possible explanation is that poor social support gives patients a feeling of being neglected, isolated, and worthless, and in contrast strong social support is vital for the prevention of such feelings. Thus, increased psychological distress may result from poor social support and TB illness.27
Limitation of the Study
Due to the nature of the cross-sectional study design, it was difficult to establish the cause–effect relationship between the predictors and the outcome variable, and the study was not triangulated with a qualitative study. Recall bias was one of the limitations of the study since some of the questions were asked about an event that occurs 24 hours back. This could be minimized by probing the respondents about the events. The similarity between symptoms of Tuberculosis and depression may overlap, especially at the early stage of TB, and is minimized by excluding one month after diagnosis of TB patients. This study assessed only the probable prevalence of depression as a screening rather than utilizing a diagnostic tool.
Conclusions
This study revealed a high magnitude of depression in patients with TB. Being older ages, females, intensive phase, HIV-positive, smoking, and poor social support were significantly associated with depression. Institution-based mental health routine screening programs, targeting chronic diseases like TB and HIV, should be established to tackle the problem of co-morbid depression at the facility level. Integrating tuberculosis and mental health support by regional health offices and supporting organizations are strongly recommended to decrease depression among TB patients. Regional health offices should be collaborated with the supporting organization to improve access to health facilities having special attention to Comorbid depression in TB patients. Health System Management should emphasize on routine screening, early detection and management, and proper training for all health care providers. Early screening with appropriate psychiatric assessments and treatment with pharmacotherapy or psychotherapy should be incorporated as a routine practice in TB clinics. Further qualitative studies should be conducted to triangulate the findings and a comparative study should be done to assess depression from other segments of the population in the study setting.
Abbreviations
EPTB, Extra Pulmonary Tuberculosis; HFCSH, Hiwot Fana Comprehensive Specialized Hospital; HIV, Human Immune Deficiency Virus; IHRERC, Institutional Health Research Ethics Review Committee; MDE, Major Depressive Episode; MDR/TB, Multidrug-Resistant Tuberculosis; PHQ, Patients Health Questionnaire; PTB, Pulmonary Tuberculosis.
Data Sharing Statement
Datasets used for the analysis are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Health Research and Ethics Review Committee (IHRERC) of College of Health and Medical Sciences, Haramaya University. An official support letter obtained from IHRERC was submitted to Harari Regional Health Bureau and selected health institutions. The Head of health institutions was informed about the purpose, benefits, risks, and the participant’s rights. All participants were informed about the purpose, benefits, risks, and the right to participate, refuse/withdraw from the study at any time. Informed voluntary written and signed consent was obtained from all participants after the information sheet was read to and/or they read it on their own. The confidentiality of the data was strictly followed.
Acknowledgments
The authors acknowledge Gorogutu Woreda Health Office for funding the study. The authors are grateful for Haramaya University, College of Health and Medical Sciences Institutional Health Research Ethical Review Committee for giving the ethical clearance. The authors are also appreciate the study participants, Harari Regional Health Bureau, and Public Health Institutions staffs and all individuals who have directly or indirectly contributed to the completion of this study.
Authors’ Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Gorogutu Woreda Health Office. The funding agency had no role in designing, analyzing, and writing of the work reported.
Disclosure
The authors report that there are no conflicts of interest in this work.
References
1. World Health Organization. Depression; 2018.
2. World Health Organisation. Depression and Other Common Mental Disorders: Global Health Estimates. Geneva, Switzerland: World Health Organization; 2017.
3. Katon W, Lin EH, Kroenke K. The association of depression and anxiety with 35 medical symptom burden in patients with chronic medical illness. Gen Hosp Psychiatry. 2007;29(2):147–155. doi:10.1016/j.genhosppsych.2006.11.005
4. Sweetland A, Oquendo M, Wickramaratne P, Weissman M, Wainberg M. Depression: a silent driver of the global tuberculosis epidemic. World Psychiatry. 2014;13:325–326. doi:10.1002/wps.20134
5. Sweetland AC, Kritski A, Oquendo MA, et al. Addressing the tuberculosis-depression syndemic to end the tuberculosis epidemic. Int J Tuberc Lung Dis. 2017;21:852–861. doi:10.5588/ijtld.16.0584
6. Ugarte-Gil C, Ruiz P, Zamudio C, Canaza L, Otero L, Kruger H. Association of major depressive episode with negative outcomes of tuberculosis treatment. PLoS One. 2013;8:e69514. doi:10.1371/journal.pone.0069514
7. Ambaw F, Mayston R, Hanlon C, Alem A. Burden and presentation of depression among newly diagnosed individuals with TB in primary care settings in Ethiopia. BMC Psychiatry. 2017;17(1):57. doi:10.1186/s12888-017-1231-4
8. de Castro-Silva KM, Carvalho AC, Cavalcanti MT, Martins PS, Franc¸a JR, Oquendo M. Prevalence of depression among patients with presumptive pulmonary tuberculosis in Rio de Janeiro, Brazil. Braz J Psychiatry. 2019;41:316–323. doi:10.1590/1516-4446-2018-0076
9. Rizvi N, Rizvi N. Frequency of depression and anxiety among tuberculosis patients. J Tuberc Res. 2016;4:183–190. doi:10.4236/jtr.2016.44021
10. Kehbila J, Ekabe CJ, Aminde LN, Noubiap JJN, Fon PN, Monekosso GL. Prevalence and correlates of depressive symptoms in adult patients with pulmonary tuberculosis in the southwest region of Cameroon. Infect Dis Poverty. 2016;5(51). doi:10.1186/s40249-016-0145-6
11. Paulo BX, Peixoto B. Emotional distress patients with several types of tuberculosis. A pilot study with patients from the sanatorium Hospital of Huambo. Int J Mycobacteriol. 2016;5:S58. doi:10.1016/j.ijmyco.2016.11.002
12. Ige OM, Lasebikan VO. Prevalence of depression in tuberculosis patients in comparison with non-tuberculosis family contacts visiting the DOTS clinic in a Nigerian tertiary care hospital and its correlation with disease pattern. Ment Health Fam Med. 2011;8(4):235–241.
13. Dasa T, Roba A, Weldegebreal F. Prevalence and associated factors of depression among tuberculosis patients in Eastern Ethiopia. BMC Psychiatry. 2019;19:82. doi:10.1186/s12888-019-2042-6
14. Ambaw F, Mayston R, Hanlon C, Alem A. Is depression associated with pathways to care and diagnosis delay in people with tuberculosis in Ethiopia? Global Mental Health. 2019;6(e20):1–11. doi:10.1017/gmh.2019.17
15. Sweetland AC, Jaramillo E, Wainberg ML, et al. Tuberculosis: an opportunity to integrate mental health services in primary care in low-resource settings. Lancet Psychiatry. 2018;5:952–954. doi:10.1016/S2215-0366(18)30347-X
16. Kardas P, Lewek P, Matyjaszczyk M. Determinants of patient adherence: a review of systematic reviews. Front Pharmacol. 2013;4:91. doi:10.3389/fphar.2013.00091
17. Ambaw F, Mayston R, Hanlon C, Medhin G, Alem A. Untreated depression and tuberculosis treatment outcomes, quality of life and disability, Ethiopia. Bull World Health Organ. 2018;96(4):243. doi:10.2471/BLT.17.192658
18. Morris DM, Quezada L, Bhat P, Moser K, Smith J. Social, Economic and psychological impacts of MDR-TBTreatment in Tijuana, Mexico: a Patient’sPerspective. Int J Tuberc Lung Dis. 2013;17(7):954–960. doi:10.5588/ijtld.12.0480
19. Pachi A, Bratis D, Moussas G, Tselebis A. Psychiatric morbidity and other factors affecting treatment adherence in pulmonary tuberculosis patients. Tuberc Res Treat. 2013;2013:489865. doi:10.1155/2013/489865
20. Ruiz-Grosso P, Cachay R, de la Flor ASA, Schwalb A, Ugarte-Gil C. Association between tuberculosis and depression on negative outcomes of tuberculosis treatment: a systematic review and meta-analysis. PLoS One. 2020;15(1):e0227472. doi:10.1371/journal.pone.0227472
21. Naidoo P, Mwaba K. Helplessness depression, and social support among people being treated for tuberculosis in South Africa. Soc Behav Pers. 2010;38(10):1323–1334. doi:10.2224/sbp.2010.38.10.1323
22. Lee L-Y, Tung -H-H, Chen S-C, Fu C-H. Perceived stigma and depression in initially diagnosed pulmonary tuberculosis patients. J Clin Nurs. 2017;26(23–24):4813–4821. doi:10.1111/jocn.13837
23. Thomas BE, Shanmugam P, Malaisamy M, et al. Psycho-socio-economic issues challenging multidrug resistant tuberculosis patients: a systematic review. PLoS One. 2016;11:e0147397. doi:10.1371/journal.pone.0147397
24. Javaid A, Mehreen S, Khan MA, Ashiq N, Ihtesham M. Depression and its associated factors with multidrug-resistant tuberculosis at baseline. J Depress Anxiety. 2017;6:253. doi:10.4172/2167-1044.1000253
25. Molla A, Mekuriaw B, Kerebih H. Depression and associated factors among patients with tuberculosis in Ethiopia: a cross-sectional study. Neuropsychiatr Dis Treat. 2019;8(15):1887–1893. doi:10.2147/NDT.S208361
26. Alinaitwe R Prevalence and factors associated with depressive illness in patients with tuberculosis in mulago hospital; 2019.
27. Duko B, Gebeyehu A, Ayano G. Prevalence and correlates of depression and anxiety among patients with tuberculosis at WolaitaSodo University Hospital and Sodo health center, WolaitaSodo, South Ethiopia, cross sectional study. BMC Psychiatry. 2015;15. doi:10.1186/s12888-015-0598-3
28. Koyanagi A, Vancampfort D, Carvalho AF. Depression comorbid with tuberculosis and its impact on health status: cross-sectional analysis of community-based data from 48 low-and middle-income countries. BMC Med. 2017;15(1):209. doi:10.1186/s12916-017-0975-5
29. Zaman K. Tuberculosis: a global health problem. J Health Popul Nutr. 2010;28(2):111. doi:10.3329/jhpn.v28i2.4879
30. Sulehri MA, Dogar IA, Sohail H. Prevalence of depression among tuberculosis patients.
31. Dos Santos APC, Lazzari TK, Silva DR. Health-related quality of life, depression and anxiety in hospitalized patients with tuberculosis. Tuberc Respir Dis. 2017;80:69–76. doi:10.4046/trd.2017.80.1.69
32. Goncalves DA, Mari Jde J, Bower P, Gask L, Dowrick C, Tofoli LF. Brazilian multicentre study of common mental disorders in primary care: rates and related social and demographic factors. Cad Saude Publica. 2014;30:623–632. doi:10.1590/0102-311X00158412
33. Walker I, Khan AM, Khan AM, et al. Depression among multidrug-resistant tuberculosis patients in Punjab, Pakistan: a large cross-sectional study. Int J Tuberc Lung Dis. 2018;22(7):773–778. doi:10.5588/ijtld.17.0788
34. Duko B, Bedaso A, Ayano G. The prevalence of depression among patients with tuberculosis: a systematic review and meta-analysis. Ann Gen Psychiatry. 2020;19(1):1–11. doi:10.1186/s12991-020-00281-8
35. Tomita A, Ramlall S, Naidu T, et al. Major depression and household food insecurity among individuals with multidrug-resistant tuberculosis (MDR-TB) in South Africa. Soc Psychiatry Psychiatr Epidemiol. 2019;54:387–393. doi:10.1007/s00127-019-01669-y
36. Prince M, Patel V, Saxena S, Maj M, Maselko J, Phillips MR. No health without mental health. Lancet. 2007;370(9590):859–877. PMID: 17804063. doi:10.1016/S0140-6736(07)61238-0
37. Buberwa GB. Prevalence of depression among tuberculosis patients attending clinics in Temeke municipal, Dar es Salaam. Doctoral dissertation, Tanzania: Muhimbili University of Health and Allied Sciences. 2013.
38. Spitzer RL, Kroenke K, Williams JB, Group PHQPCS, Group PHQPCS. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Jama. 1999;282(18):1737–1744.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence and Associated Factors of Diabetes Mellitus Among Newly Enrolled Tuberculosis Patients in Lubumbashi (DRC)
Kakisingi C, Mwamba C, Muteba MK, Kasamba E, Kabamba M, Tanon A, Situakibanza H
Risk Management and Healthcare Policy 2024, 17:171-180
Published Date: 17 January 2024