")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Magnetic Resonance Imaging Characteristics of Autoimmune Glial Fibrillary Acidic Protein (GFAP) Astrocytopathy: A Pediatric Series in Southwest China
Authors Cheng W, He L, Luo H, Jiang Y, Tan C , Fan X
Received 16 April 2023
Accepted for publication 24 July 2023
Published 29 July 2023 Volume 2023:19 Pages 1685—1693
DOI https://doi.org/10.2147/NDT.S417492
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Weiqin Cheng,1 Ling He,1 Hechuan Luo,1 Yan Jiang,2 Chengbing Tan,2 Xiao Fan1
1Department of Radiology, Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, China International Science and Technology Cooperation Base of Child Development and Critical Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing, People’s Republic of China; 2Department of Neurology, Children’s Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, China International Science and Technology Cooperation Base of Child Development and Critical Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing, People’s Republic of China
Correspondence: Xiao Fan, Department of Radiology, Children’s Hospital of Chongqing Medical University, No. 136 Zhongshan Er Road, Yuzhong District, Chongqing, 400014, People’s Republic of China, Tel +86 13637907710, Email [email protected]
Objective: To investigate and summarize the magnetic resonance imaging (MRI) manifestations of autoimmune glial fibrillary acidic protein (GFAP) astrocytopathy in children.
Methods: We retrospectively analyzed data from 17 pediatric patients with autoimmune GFAP astrocytopathy confirmed by the detection of GFAP autoantibodies in cerebrospinal fluid in our single-center. Furthermore, we reviewed current literature and summarized previous findings on the MRI characteristics of this disease in children.
Results: In these 17 patients, the clinical manifestations and results of CSF analysis were suggestive of autoimmune disorder, with a good improvement. The lesions on MRI were most commonly located in the bilateral basal ganglia (70.6%), thalamus (64.7%), cerebral white matter (29.4%). 93.3% of the cerebral lesions were relatively scattered and small, 80% of the spinal lesions presented as longitudinally extensive ones. Both periventricular radial linear (PVRL) (53.8%) and punctate or linear enhancement in basal ganglia and thalamus (53.8%) were commonly observed, followed by the leptomeningeal enhancement (46.2% in the brain and 62.5% in the spinal cord). We then included 55 pediatric patients with MRI data from current literature in our analysis (n = 72, 44 males). Our results revealed similar MRI findings but the enhancement pattern between our series and previously published cases, that is, leptomeningeal enhancement in the brain 46.2% vs 31.4%, in spinal cord 62.5% vs 18.4%, and PVRL enhancement 53.8% vs 11.2%. There were no detailed reports on punctate or linear enhancement.
Conclusion: The MRI characteristics of autoimmune GFAP astrocytopathy in children could be suggestive. Scattered and small lesions (especially punctate or linear) in the bilateral thalamus, basal ganglia, and white matter, as well as longitudinally extensive spinal cord lesions (if present), with punctate, PVRL and leptomeningeal enhancement might be a distinct indication for the early diagnosis of this disorder.
Keywords: glial fibrillary acidic protein, GFAP, astrocytopathy, autoimmune, magnetic resonance imaging, children
Introduction
Autoimmune glial fibrillary acidic protein (GFAP) astrocytopathy was recently recognized as a type of autoimmune meningoencephalitis characterized by GFAP antibodies.1 This disease is characterized by acute or subacute onset, and most patients present nonspecific clinical manifestations, including encephalopathy, seizures, psychiatric symptoms, tremor, and meningeal symptoms.2–4 These nonspecific symptoms will likely be misdiagnosed as infectious meningitis, especially viral meningitis and tuberculous meningitis.5 In addition, autoimmune GFAP astrocytopathy principally occurs in adults (median age: 44–50 years), and only approximately 10% in children.2 Studies investigating are scarce, and it has been indicated that differences in clinical and MRI features between children and adults warrant further investigation, especially when it comes to magnetic resonance imaging (MRI) findings.6–8 Typical MRI features involve linear perivascular enhancement oriented radially to the ventricles; however, this pattern could only be detected in nearly half of the patients assessed.1,3,9
Herein, we report the clinical and imaging characteristics of 17 pediatric patients with autoimmune GFAP astrocytopathy, the largest pediatric series in Southwest China to our knowledge. We focused on neuroimaging features, in order to raise awareness and provide a greater insight to the diagnosis of this entity in children.
Materials and Methods
Patients
We retrospectively enrolled all patients with autoimmune GFAP astrocytopathy at the Children’s Hospital of Chongqing Medical University (the largest tertiary children’s medical center in Southwest China and one of the National Centers for Children’s Health in China) between September 2019 and January 2022, aged 0–18years. Autoimmune GFAP astrocytopathy was diagnosed by the presence of noninfectious meningoencephalomyelitis and GFAP-IgG in cerebrospinal fluid (CSF). The inclusion criteria were as follows: (1) patients who was at the initial attack when admitted; (2) GFAP-IgG was detected in their CSF samples; (3) MRI scanning was carried out before therapy. Patients were excluded according to the following criteria: (1) poor imaging quality due to obvious motion artifacts; (2) patients with sequela manifestations due to previous injuries, such as encephalomalacia.
Clinical data were evaluated through medical record reviews. Children were subjected to clinical examinations, CSF examination, and brain and/or spinal cord MRI scanning. The Ethics Committee of our hospital approved the study, and the need for informed consent was waived because of the retrospective nature of this research. Clinical and MRI data were blindly and respectively reviewed by two experienced neurologists (CB Tan and Y Jiang) and two neuroradiologists (WQ Cheng and X Fan). A consensus was reached through discussion in the event of disagreement.
Clinical Data
All clinical manifestations and laboratorial data in the early stages of disease activity and before immunotherapy were collected, as well as treatment and clinical outcomes. CSF studies included cell count, biochemical analysis, and oligoclonal bands (OCBs). Serum and CSF samples were examined for GFAP-IgG using a cell-based assay relying on HEK293 cells cotransfected with human GFAP and pEGFP-N1 as reported previously.1,6,8 Considering that overlapping symptoms are commonly observed, other autoimmune and demyelinating antibodies, including anti-N-methyl-D-aspartate receptor (NMDAR), myelin oligodendrocyte glycoprotein (MOG), gamma-aminobutyric acid receptor A (GABAAR) and Yo, leucine-rich glioma-inactivated protein 1 (LGI1), aquaporin-4 (AQP-4) and antimyelin basic protein (MBP) antibodies, were also tested at onset both in serum and CSF samples. Tumor screening was also performed.
MRI Scanning Method
All MRI examinations were assessed, including the following sequences: T1 fluid-attenuated inversion recovery (FLAIR)-axial [TR/TI = 2000/20 msec, TE = 800 msec], T2 weighted (T2w)-axial [TR/TE = 2200/80 msec], T2 FLAIR-axial [TR/TE = 8000/81 msec, TI = 2382 msec], T2w sagittal [TR/TE = 2200/80 msec], and T1w with a contrast medium (0.2 mL/kg, Omniscan, GE, USA) on axial, sagittal, and coronal views [TR/ TE = 250/2.3 msec]. Thirteen patients continued to undergo spinal MRI one week after the onset, with sagittal and axial images on T1w and T2w [sagittal: TR/TE = 410/6.8 msec; TR/TE = 2000/90 msec, axial: TR/TE = 659/20 msec; TR/TE = 3684/100 msec]. Among the 17 children included in this study, nine underwent MRI examinations using scanners with a field strength of 1.5 T (Signa Horizon Lx; General Electric Medical System, Milwaukee, WI, USA) and eight using a 3.0 T scanner (Philips, Achieva 3T, Netherlands). MR images of patients at the onset of the disease were reviewed, and the lesion distribution and enhancement patterns were recorded.
A follow-up brain MRI was available for all included patients except two for discharge at their own requests. Only five patients underwent spinal re-scanning due to previous lesions or suspected additional lesions.
Results
Clinical and Laboratorial Characteristics
A total of 17 children diagnosed with autoimmune GFAP astrocytopathy (8 males and 9 females) were included in this study, with a median age at onset of 9.5 years (range: 3–15 years) and a median MRI follow-up length of five months (ranging from 20 days to 36 months). The GFAP-IgG titers in CSF ranged from 1:32 to 1:320, with a cutoff value of 1:32 (n = 10, 1:32; n = 5, 1:100; n = 2, 1:320). GFAP-IgG was detected in the serum samples of 10 patients (titers range: 1:16–1:100), whereas four were negative, and three patients refused to undertake the test. Fifteen children presented with acute or subacute neurological symptoms, and only two patients had a chronic course. Flu-like prodromes were prevalent in six children. The main neurological symptoms included consciousness disturbance (n = 14, 82.4%), fever (n = 13, 76.5%), motor dysfunction (n = 11, 64.7%), headache (n = 10, 58.8%), dizziness (n = 10, 58.8%), dysautonomia (n = 7, 41.2%), abnormal vision (n = 6, 35.3%), seizure (n = 5, 29.4%), psychosis (n = 3, 17.6%), hyponatremia and hypokalemia (n = 2, 11.8%), and diabetes insipidus (n = 1, 5.9%).
CSF analysis revealed abnormalities in 16 patients (94.1%). Pleocytosis was observed in 15 patients (median: 154 × 106/L, range: 63–334 × 106/L), and elevated protein levels and low glucose in twelve (median: 1.20 g/L, range: 0.52–1.84 g/L) and six cases (median: 2.31 mmol/L, range: 2.18–2.39 mmol/L), respectively. One patient was diagnosed with overlapping syndrome, due to detection of both GFAP and NMDAR antibodies. The remaining 16 children had no other autoimmune and demyelinating antibodies in the serum or CSF. None of these 17 patients had OCBs in their CSF sample, a history of traumatic brain injury or tumor. Additionally, alpha fetal protein (AFP) and other tumor markers were not significantly increased; abdominal ultrasound examination did not find any solid tumors.
MRI Characteristics
Brain MRI was performed in all patients, of whom 13 were intravenously injected contrast agents. Spinal cord MRI was performed in 13 patients, of whom eight were intravenously injected contrast agents in the early stage of disease. MRI findings are summarized in Table 1.
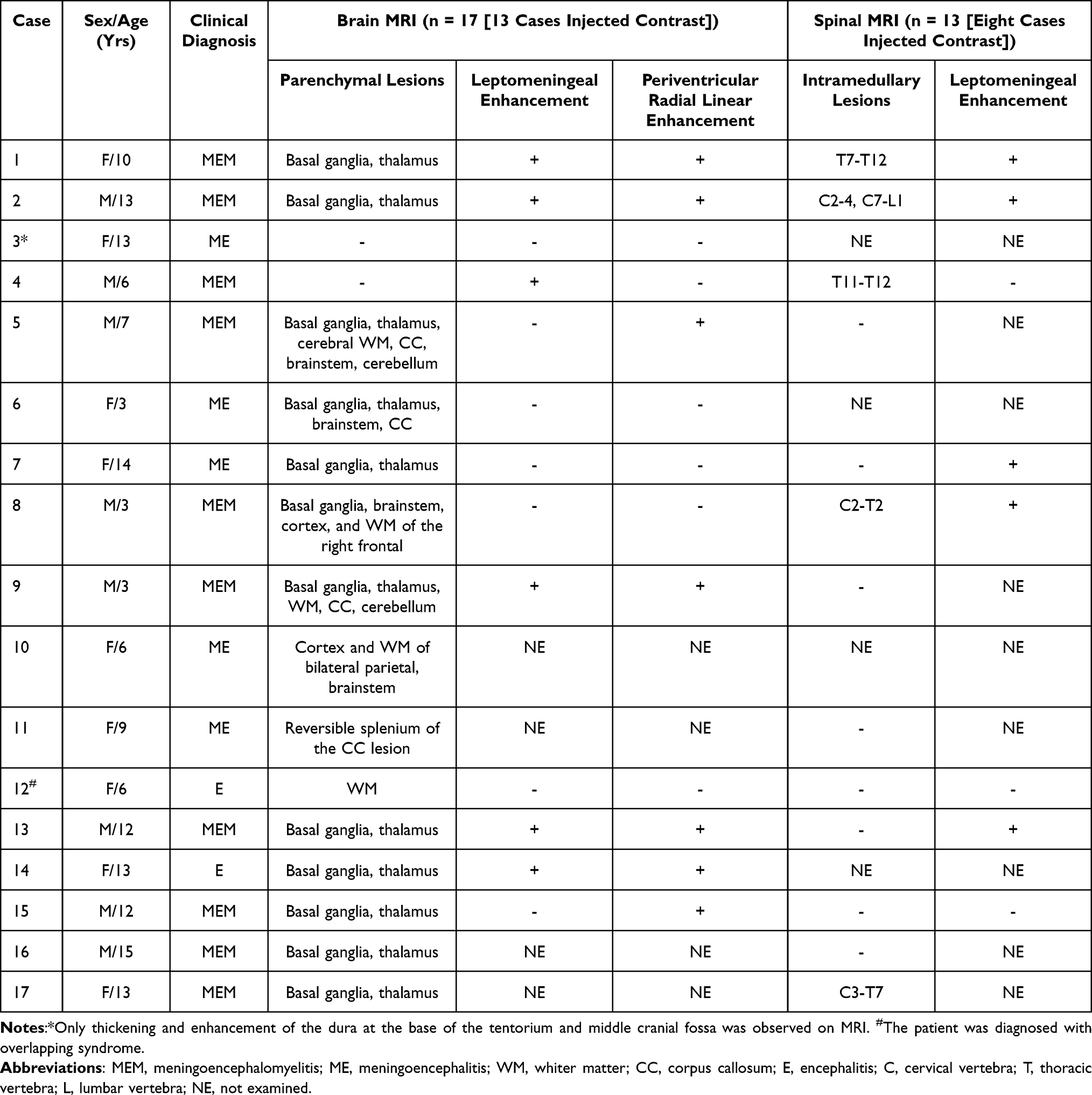 |
Table 1 The MRI Characteristics in Our Series of 17 Pediatric Patients with Autoimmune GFAP Astrocytopathy |
On brain MRI in 17 patients, 16 cases (94.1%) revealed abnormalities. Fifteen cases (88.2%) demonstrated abnormal hyperintensity on T2w and T2 FLAIR images. Hyperintensity lesions were located in the bilateral basal ganglia (n = 12), thalamus (n = 11), cerebral white matter (n = 5), corpus callosum (n = 4), brainstem (n = 4), cortex (n = 2), and cerebellum (n = 2). Except for one case (No.9), in which symmetrical and diffuse parenchymal lesions were observed, parenchymal lesions relatively small and scattered were found in all remaining patients (14/15, 93.3%), most of which were spotted or linear. All basal ganglia and thalamus lesions presented as punctate and linear hyperintensities on T2w and T2 FLAIR images (Figure 1A and B). After enhancement, seven of 13 cases (53.8%) showed periventricular radial linear (PVRL) enhancement (Figure 1C), seven (53.8%) demonstrated punctate or linear enhancement in both basal ganglia and thalamus (Figure 1D), and six cases (46.2%) showed leptomeningeal enhancement. Surprisingly, a female child with corpus callosum involvement presented as reversible splenium of corpus callosum lesion, which was her only MRI finding. Besides, one patient depicted a novel enhancement pattern of hypertrophic dura mater in the anterior-middle fossa, cerebellum, and slope (Figure 1E).
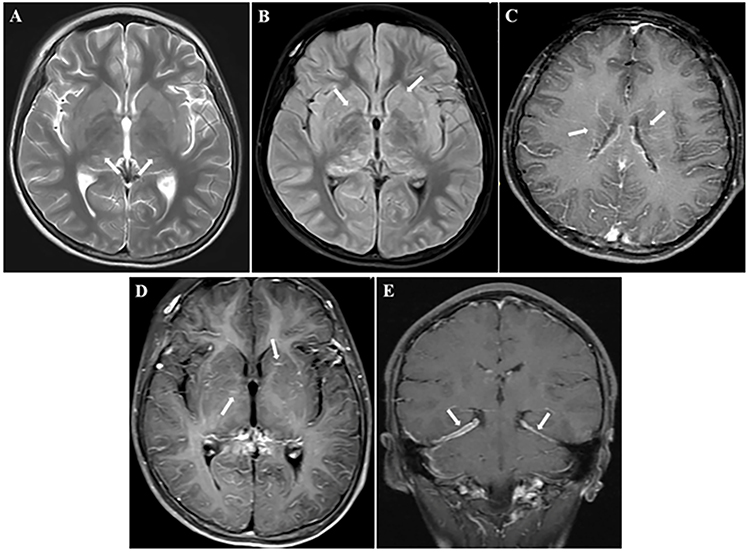 |
Figure 1 MRI findings of autoimmune GFAP astrocytopathy in this pediatric cohort. T2-weighted (A) and fluid-attenuated inversion recovery (FLAIR) (B) images showed punctate and linear hyperintensities located in the bilateral basal ganglia (white arrows in (B) and thalamus (white arrows in (A). Gadolinium-enhanced brain MRI showed periventricular radial linear enhancement (white arrows in (C), punctate or linear enhancement in both basal ganglia and thalamus (white arrows in (D), and hypertrophic dura mater (white arrows in (E) around the cerebellum. |
On spinal MRI in 13 patients, five (38.5%) exhibited abnormal spinal cord signals on T2w, which were mainly involved in the central gray matter, and four cases (80%) demonstrated longitudinally extensive spinal cord lesions (LESCLs) (involving ≥3 spinal cord segments) that were mostly distributed in the cervical and thoracic segments. Gadolinium-enhanced MRI revealed leptomeningeal enhancement in five of eight children (62.5%).
Treatments and Outcomes
During hospitalization, fifteen patients (88.2%) were treated with first-line immunotherapy as an acute attack therapy, including intravenous methylprednisolone (n = 14) and intravenous immunoglobulin (n = 11), while 10 patients received a combination of both therapies. The remaining two cases did not accept either treatment. On discharge, all patients achieved a good prognosis with clinically significant or complete improvement. In the subsequent outpatient follow-up, two patients were lost and another two relapsed with previous similar symptoms. Of the two patients who relapsed, one was readmitted for overlapping syndrome (No.3), and the other refused to receive immunotherapy during hospitalization (No.10). Reexamination brain MRIs were also carried out in these 15 patients (follow-up time: 20 days to 36 months), showing that lesions were maximally reduced in size or disappeared after immunotherapy. Lesions were completely resolved in five cases.
Literature Review on Neuroimaging
We then performed a review of current literature, using “GFAP autoimmunity” or “GFAP astrocytopathy” as the search terms, to identify research studies performed on children (<18 years) with GFAP astrocytopathy with CSF and/or serum GFAP-IgG. Studies lacking MRI original data were excluded. Data of 55 pediatric patients were collected from nine publications,4,6,7,10–15 and Table 2 summarizes the MRI characteristics of 72 children with autoimmune GFAP astrocytopathy (17 cases in the present study and 55 cases in previously published studies), including 28 girls and 44 boys.
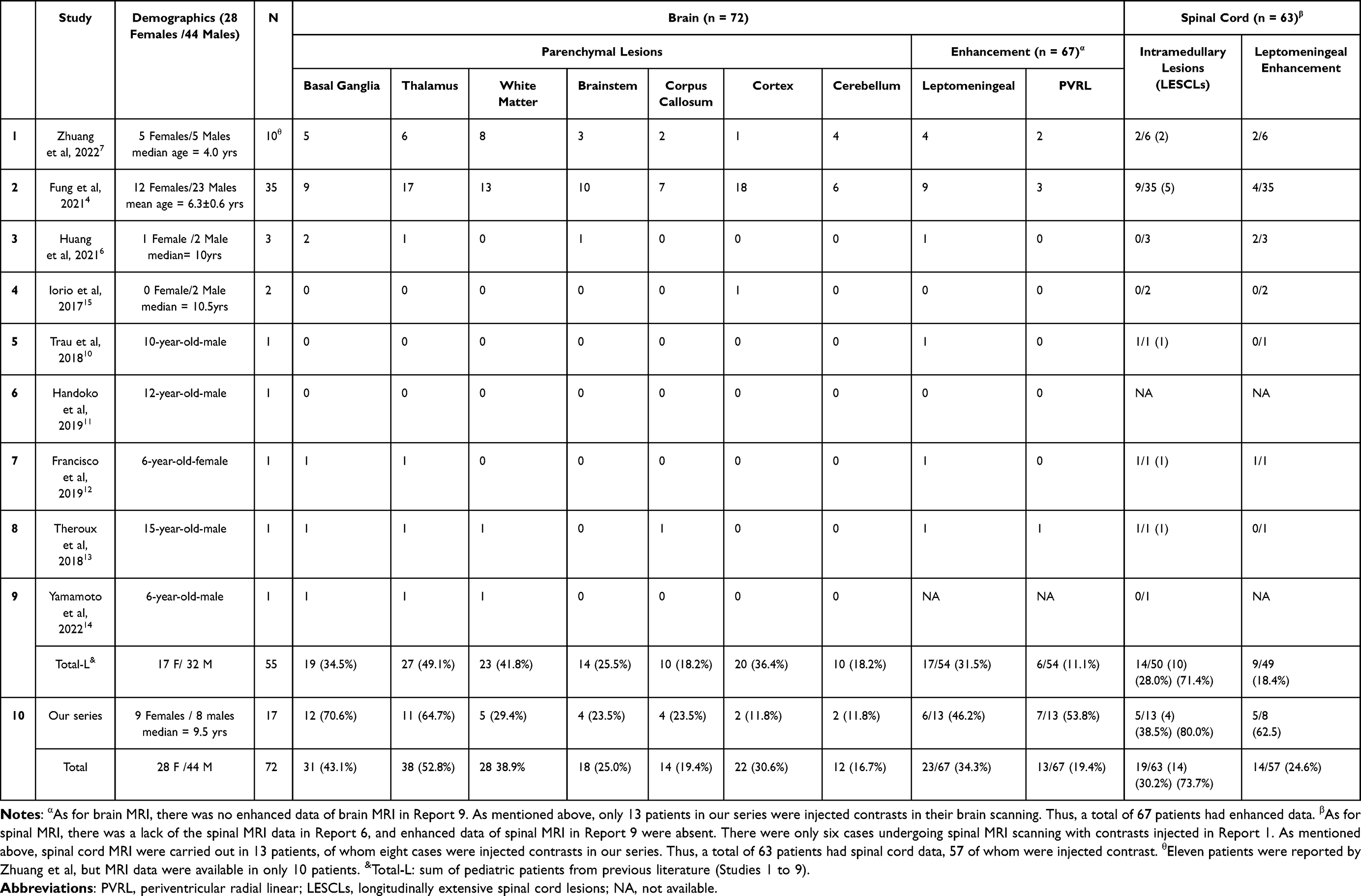 |
Table 2 A Review of the MRI Characteristics of All Pediatric Patients with Autoimmune GFAP Astrocytopathy Published in the Last 6 Years |
In this pediatric literature series of autoimmune GFAP astrocytopathy, MRI findings were heterogeneous and multifocal, and brain MRI was rarely normal. Basal ganglia, thalamus, cerebral white matter (periventricular, subcortical), callosum, brainstem, cerebellum, cortex, spinal cord, and meninges could be involved in this disease. T2w and/or T2 FLAIR hyperintensities in the brain parenchyma were mostly located in the thalamus (52.8%), followed by basal ganglia (43.1%) and cerebral white matter (38.9%). 30.2% (19/63) of these pediatric patients undergoing spinal MRI scanning manifested intramedullary lesions, 73.7% (14/19) of whom showed LESCLs. After enhancement, only 19.4% (13/67) children undergoing cerebral enhanced MRI depicted a PVRL pattern. Leptomeningeal enhancement in the brain and spinal cord accounted for 34.3% and 24.5%, respectively.
Discussion
GFAP astrocytopathy is a severe inflammatory central nervous system (CNS) disorder of autoimmune etiology, which predominantly affects the meninges, brain, and spinal cord.3,16,17 In 2016, Fang et al1 from Mayo Clinic in the United States first proposed and named the disease. A specific GFAP antibody as a biomarker of the disease has been confirmed in suffered canine models and patients.1,18,19 Few neuropathological studies have demonstrated extensive inflammation and microglial activation, but there are still differences in pathological characteristics, such as whether the vessel wall is affected.1,9,15 Owing to the fact that this is a newly described entity, standard diagnostic criteria for this disorder are still unavailable. However, it is widely accepted that MRI plays a very important role in detecting and localizing lesions in CNS, as well as in the diagnosis of this challenging disease and differentiation. The majority of existing reports on this topic has been published in the neuroimmunology field and almost exclusively involve adult patients.3,8,20 This study presented the clinical and radiological features of 17 children with autoimmune GFAP astrocytopathy and then reviewed a total of 55 pediatric cases with previously reported MRI data. Therefore, we believe that this pediatric series of autoimmune GFAP astrocytopathy is sufficiently large and can thus provide some neuroradiological clues to promote the earlier and quicker diagnosis of this disorder and enable clinicians to adjust the respective treatment.
In our series of 17 patients, the peak age of onset was 9.5 years, which is consistent with previous reports.6,8 Previous pediatric studies have reported a relatively wide range of onset age (range: 11 months–17 years).7,11,13,14,21 Nevertheless, a few studies reported a younger age of onset mostly in preschool children4,7 and some argued that this condition was more common in adolescence.21 This difference may be due to the small sample size employed in all pediatric studies. There was no sex predominance in our cases. In addition, the clinical manifestations and results of CSF analysis were suggestive of an autoimmune disorder, with a good improvement. All of these above findings are similar with the previous studies in children and adults.4,10,12,20,22 There were still four patients with GFAP-IgG positive in their CSF samples but negative in the serum. Data about the specificity of GFAP-IgG in the serum is limited, due to development of different detection methods.22 For now, positivity in CSF has more diagnostic value, with a high specificity and sensitivity.1,9,17
Regarding the MRI characteristics, our study identified that the lesions in brain parenchyma were most commonly located in the bilateral basal ganglia (70.6%), thalamus (64.7%), and cerebral white matter (29.4%). Moreover, we found that punctate or linear enhancement in both basal ganglia and thalamus was the most common pattern of enhancement (53.8%). Although rarely reported, this finding is consistent with previous neuropathological findings demonstrating extensive inflammation around small vessels and perivascular region originating from GFAP-enriched areas (the basal ganglia, thalamus, white matter, etc.).2,7,9,23 Other common patterns of enhancement were PVRL (53.8%) and leptomeningeal (46.2% in the brain and 62.5% in the spinal cord), which could be explained by gadolinium leakage from the damaged blood–brain barrier (BBB). Although less abnormal signals (38.5%) were found on spinal MRI, these lesions predominantly showed LESCLs, which might be possibly misdiagnosed by neuroradiologists as other demyelinating diseases like acute disseminated encephalomyelitis, more common in children. Thus, we need to be alert to this MRI manifestation.
Furthermore, we identified 55 pediatric patients with detailed MRI data in previously published studies, and we found that the common locations of cerebral lesions in our series were roughly similar to those reported in these pediatric cohorts. However, lesions in the spinal cord, even LESCLs, were found to be more common compared to the results of previous pediatric reports (38.5% vs 28.0%, 80% vs 71.4%, respectively). Enhancement was also more frequently observed in our series compared to current literature, ie, leptomeningeal enhancement in the brain (46.2% vs 31.5%) and in the spinal cord (62.5% vs 18.4%), and PVRL enhancement (53.8% vs 11.1%). These inconsistencies may be due to sampling bias. Our institution is highly specialized and serves as a national referral center. Therefore, there is a higher probability of severe cases in our institution.
For this total of 72 pediatric cases with MRI data, cerebral lesions were commonly scattered and small, located in the bilateral thalamus, basal ganglia, and white matter; lesions in the basal ganglia and thalamus were usually punctate or linear. These MRI features are in agreement with previous findings in adults.3,20,24 Xiao et al24 declared that distinct small (<2 cm), symmetrical T2 FLAIR lesions in ganglia and thalamus might be prominent features of autoimmune GFAP astrocytopathy, and could thus be helpful in distinguishing this disorder from other autoimmune inflammatory diseases of the CNS. However, diffuse abnormalities in periventricular white matter, which is a common feature in adult patients, were not so frequently found in pediatric patients (only one in our series).1,8,9 Therefore, it is uncertain whether the pathogenesis and lesion sites are consistent between adults and children, and further investigation is necessary. In terms of enhancement, the PVRL pattern was significantly more common in our study (53.8%) compared to previously reported pediatric patients (8.5–20.0%),4,7 although this was broadly in accordance with cohorts performed in adults,1,3,21,25 with an incidence of approximately 32–100% (mostly around 50%). In particular, we also found that punctate or linear enhancement in both basal ganglia and thalamus was a common pattern in children (53.8%), which is not usually reported in adult cohorts.17,20,21 It could be suggested that more severe acute inflammatory reactions in basal ganglia and thalamus are observed in children, causing BBB damage. Whether this can infer that these vulnerable parts of children are associated with a more obvious inflammatory response needs further study.
Nonetheless, two patients in our series exhibited unusual MRI manifestations. One patient demonstrated only reversible splenial lesion syndrome, which was consistent with the clinical diagnosis of mild encephalitis/encephalopathy with reversible splenic lesions (MERS). Previously, only one pediatric case had been associated with MERS and GFAP astrocytopathy.26 The relationship between autoimmune GFAP astrocytopathy and MERS has been observed scarcely and remains to be explored. Another girl presented with thickening and enhancement of dura mater, which was diagnosed as hypertrophic pachymeningitis (HP) with autoimmune GFAP astrocytopathy. This case has been firstly reported by our co-authors (CB Tan and Y Jiang), and it has been suggested that GFAP-related HP might be related to meningeal immunity.27 Finally, one patient was diagnosed with overlapping syndrome due to detection of both GFAP and NMDAR antibodies, which is the most common type according to literature.1,4
This study has several limitations. First, our study may have selection bias due to a retrospective design. Second, GFAP-IgG testing processes in our center have only been performed for a relatively short time and pediatric cases were rarely reported in literature; thus, sample size was limited. Besides, although radiological follow-up was obtained in most of patients, this was not systematically done, particularly assessments of the spinal cord. Therefore, multicenter, larger cohorts with more advanced MRI protocols will be needed to further validate this observation.
Conclusion
The clinical manifestations and imaging findings of autoimmune GFAP astrocytopathy in children can vary. However, some MRI characteristics can provide an insight for the subsequent diagnosis and differentiation of this disorder. Autoimmune GFAP astrocytopathy should be highly suspected in children with a proposed autoimmune disease when the MRI features are shown as following: scattered and small lesions (especially punctate or linear) in bilateral thalamus, basal ganglia, and white matter, with punctate, PVRL and leptomeningeal enhancement.
Ethics Approval and Informed Consent
The Children’s Hospital of Chongqing Medical University’s institutional review board approved this study, and the need for informed consent was waived due to its retrospective nature. Direct contact with the patient is not required, so it will not adversely affect the rights and health of the patient. This retrospective study complies with the Declaration of Helsinki, abides by the principle of confidentiality, and will not release patient information.
Funding
This work was supported by the clinical new technology project in the Children’s Hospital of Chongqing Medical University [grant number 202026].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fang B, McKeon A, Hinson S, et al. Autoimmune glial fibrillary acidic protein astrocytopathy: a novel meningoencephalomyelitis. JAMA Neurol. 2016;73(11):1297–1307. doi:10.1001/jamaneurol.2016.2549
2. Kunchok A, Zekeridou A, McKeon A. Autoimmune glial fibrillary acidic protein astrocytopathy. Curr Opin Neurol. 2019;32(3):452–458. doi:10.1097/WCO.0000000000000676
3. Xiao J, Chen X, Shang K, et al. Clinical, neuroradiological, diagnostic and prognostic profile of autoimmune glial fibrillary acidic protein astrocytopathy: a pooled analysis of 324 cases from published data and a single-center retrospective study. J Neuroimmunol. 2021;360:577718. doi:10.1016/j.jneuroim.2021.577718
4. Fang H, Hu W, Jiang Z, et al. Autoimmune glial fibrillary acidic protein astrocytopathy in children: a retrospective analysis of 35 cases. Front Immunol. 2021;12:761354. doi:10.3389/fimmu.2021.761354
5. Yang X, Zhang C, Zhang J, et al. Autoimmune glial fibrillary acidic protein astrocytopathy mimics infectious meningitis: two case reports. Mult Scler Relat Disord. 2020;45:102350. doi:10.1016/j.msard.2020.102350
6. Huang H, Bai K, Fu Y, et al. Glial fibrillary acidic protein astrocytopathy in pediatric patients: a retrospective study. Front Pediatr. 2020;8:626564. doi:10.3389/fped.2020.626564
7. Zhuang X, Jin K, Li X, Li J. Autoimmune glial fibrillary acidic protein astrocytopathy in children: a retrospective study. Eur J Med Res. 2022;27(1):11. doi:10.1186/s40001-022-00641-y
8. Dubey D, Hinson SR, Jolliffe EA, et al. Autoimmune GFAP astrocytopathy: prospective evaluation of 90 patients in 1 year. J Neuroimmunol. 2018;321:157–163. doi:10.1016/j.jneuroim.2018.04.016
9. Long Y, Liang J, Xu H, et al. Autoimmune glial fibrillary acidic protein astrocytopathy in Chinese patients: a retrospective study. Eur J Neurol. 2018;25(3):477–483. doi:10.1111/ene.13531
10. Trau SP, Gallentine WB. Autoimmune GFAP-associated meningoencephalomyelitis: a report of a pediatric patient. Pediatr Neurol. 2018;82:50. doi:10.1016/j.pediatrneurol.2018.02.001
11. Handoko M, Hong W, Espineli E, Saxena K, Muscal E, Risen S. Autoimmune glial fibrillary acidic protein astrocytopathy following herpes simplex virus encephalitis in a pediatric patient. Pediatr Neurol. 2019;98:85–86. doi:10.1016/j.pediatrneurol.2019.05.010
12. Francisco C, Meddles K, Waubant E. Pediatric glial fibrillary acidic protein meningoencephalomyelitis: a case report and review of the literature. Mult Scler Relat Disord. 2019;29:148–152. doi:10.1016/j.msard.2018.12.008
13. Theroux LM, Goodkin HP, Heinan KC, Quigg M, Brenton JN. Extreme delta brush and distinctive imaging in a pediatric patient with autoimmune GFAP astrocytopathy. Mult Scler Relat Disord. 2018;26:121–123. doi:10.1016/j.msard.2018.09.015
14. Yamamoto N, Inoue T, Kuki I, et al. A pediatric case of autoimmune glial fibrillary acidic protein astrocytopathy with unique brain imaging patterns and increased cytokines/chemokines. Brain Dev. 2022;44(10):753–758. doi:10.1016/j.braindev.2022.06.011
15. Iorio R, Damato V, Evoli A, et al. Clinical and immunological characteristics of the spectrum of GFAP autoimmunity: a case series of 22 patients. J Neurol Neurosurg Psychiatry. 2018;89(2):138–146. doi:10.1136/jnnp-2017-316583
16. Liu L, Fang B, Qiao Z, et al. Clinical manifestation, auxiliary examination features, and prognosis of GFAP autoimmunity: a Chinese cohort study. Brain Sci. 2022;12(12):1662. doi:10.3390/brainsci12121662
17. Flanagan EP, Hinson SR, Lennon VA, et al. Glial fibrillary acidic protein immunoglobulin G as biomarker of autoimmune astrocytopathy: analysis of 102 patients. Ann Neurol. 2017;81(2):298–309. doi:10.1002/ana.24881
18. Matsuki N, Fujiwara K, Tamahara S, et al. Prevalence of autoantibody in cerebrospinal fluids from dogs with various CNS diseases. J Vet Med Sci. 2004;66(3):295–297. doi:10.1292/jvms.66.295
19. Matsuki N, Takahashi M, Yaegashi M, Tamahara S, Ono K. Serial examinations of anti-GFAP autoantibodies in cerebrospinal fluids in canine necrotizing meningoencephalitis. J Vet Med Sci. 2009;71(1):99–100. doi:10.1292/jvms.71.99
20. Kimura A, Takekoshi A, Yoshikura N, Hayashi Y, Shimohata T. Clinical characteristics of autoimmune GFAP astrocytopathy. J Neuroimmunol. 2019;332:91–98. doi:10.1016/j.jneuroim.2019.04.004
21. Gravier-Dumonceau A, Ameli R, Rogemond V, et al. Glial fibrillary acidic protein autoimmunity: a French cohort study. Neurology. 2022;98(6):e653–e668. doi:10.1212/WNL.0000000000013087
22. Shan F, Long Y, Qiu W. Autoimmune glial fibrillary acidic protein astrocytopathy: a review of the literature. Front Immunol. 2018;9:2802. doi:10.3389/fimmu.2018.02802
23. Shu Y, Long Y, Chang Y, et al. Brain Immunohistopathology in a Patient with Autoimmune Glial Fibrillary Acidic Protein Astrocytopathy. Neuroimmunomodulation. 2018;25(1):1–6. doi:10.1159/000488879
24. Xiao J, Zhang SQ, Chen X, et al. Comparison of clinical and radiological characteristics in autoimmune GFAP astrocytopathy, MOGAD and AQP4-IgG(+) NMOSD mimicking intracranial infection as the initial manifestation. Mult Scler Relat Disord. 2022;66:104057. doi:10.1016/j.msard.2022.104057
25. Liao H, Chen Q, Zhang M, Chen W. MRI features and evolution of autoimmune glial fibrillary acidic protein astrocytopathy: a retrospective cross-sectional and longitudinal study. Mult Scler Relat Disord. 2022;58:103512. doi:10.1016/j.msard.2022.103512
26. Oger V, Bost C, Salah L, et al. Mild encephalitis/encephalopathy with reversible splenial lesion syndrome: an unusual presentation of anti-GFAP astrocytopathy. Eur J Paediatr Neurol. 2020;26:89–91. doi:10.1016/j.ejpn.2020.03.002
27. Tan C, Zhong M, Yao Z, Hong S, Jiang L, Jiang Y. Anti-GFAP antibody-associated hypertrophic pachymeningitis. Neuropediatrics. 2022;53(2):143–145. doi:10.1055/s-0042-1742718
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.