Back to Journals » Cancer Management and Research » Volume 13
Lymphadenectomy Around Inferior Mesenteric Artery in Low-Tie vs High-Tie Laparoscopic Anterior Resection: Short- and Long-Term Outcome of a Cohort of 614 Rectal Cancers
Authors Luo Y, Yu MH, Huang YZ, Jing R, Qin J, Qin SL, Shah JN ![]() , Zhong M
, Zhong M
Received 20 September 2020
Accepted for publication 10 December 2020
Published 14 May 2021 Volume 2021:13 Pages 3963—3971
DOI https://doi.org/10.2147/CMAR.S282986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Yang Luo,1,* Min-Hao Yu,1,* Yi-Zhou Huang,1 Ran Jing,1 Jun Qin,1 Shao-Lan Qin,1 Jay N Shah,1,2 Ming Zhong1
1Department of Gastrointestinal Surgery, Renji Hospital, Jiao Tong University School of Medicine, Shanghai, 200127, People’s Republic of China; 2Department of Surgery, Patan Hospital, Patan Academy of Health Sciences, Lalitpur, Kathmandu, 44700, Nepal
*These authors contributed equally to this work
Correspondence: Ming Zhong; Jay N Shah Email [email protected]; [email protected]
Background: Preservation of the left colic artery in low-tie (LT) of inferior mesenteric artery remains controversial compared to high-tie (HT) in the colon and rectal cancers, for lymph node dissection, anastomotic leakage, and oncological outcome. This cohort study aims to analyze short- and long-term outcomes of laparoscopic anterior resections in LT vs HT for rectal cancers.
Methods: We analyzed a cohort of laparoscopic AR for RC from 2013 to 2016 at Renji Hospital, Shanghai, China. Short- and long-term outcome in LT vs HT group were compared for clinico-demographic characteristics, operative-time, lymph node dissection, short-term 30-day outcome, and long-term 3- and 5-year overall survival as well as disease-free survival. The x2, t-test, and logistic regressions analysis were used and p< 0.05 was considered significant.
Results: The cohort consisted of 614 laparoscopic AR with LT (236) and HT (378). The clinicodemographic characteristics were comparable among the groups. The surgery took longer in LT. The yield of LND was similar. Leakage occurred in 12.21% (n=75). Leakage was fewer in LT than HT, 8.89% vs 14.28%, p=0.047. The postoperative severe complications were higher in HT. The 30-day mortality was nil. The long-term 3- and 5-year overall survival and disease-free survival were similar in LT and HT.
Conclusion: The LT with preservation of left colic artery had similar lymph node yield, but lower leakage and complications than HT in laparoscopic anterior resections for rectal cancers. The long-term 3- and 5-year overall and disease-free survival were similar in the two groups.
Keywords: anastomotic leakage, Clavien-Dindo complications, laparoscopic anterior resection, left colic artery, low-tie high-tie of the inferior mesenteric artery, rectal cancer
Plain Language Summary
Our findings in a cohort of 641 patients with rectal cancer who underwent laparoscopic anterior resection affirm that low-tie (LT) of the inferior mesenteric artery with preservation of left colic artery maintains the oncological principle for lymph node harvesting including at the root of the inferior mesenteric artery. The LT group had fewer anastomotic leakage compared to high-tie (HT), and comparable 3- and 5-year long-term outcomes of overall survival and disease-free survival.
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide and is of concern in China due to its steady increase in age-standardized incidence rates (ASIR) from 14.25 to 25.27 per 100,000 observed during 1990–2016, with an average annual percentage change of 2.34, and Shanghai at 2nd position with an ASIR of 32.30 after Hong Kong at 39.97.1
Total mesorectal excision (TME) is the gold standard for rectal cancer (RC),2 but the controversies continue for high-tie (HT) with ligation of the inferior mesenteric artery (IMA) at its root above the branching of left colic artery “LCA” vs low-tie (LT) with ligation of IMA below LCA. The HT is credited for ease of lymph node dissection (LND) around IMA for staging and oncological outcome plus tension-free anastomosis of the remaining colon.3,4 The compromise of blood supply leading to colon ischemia,5 hypoperfusion and anastomotic leakage (AL),6,7 damage to superior hypogastric plexus,8 and genitourinary defecatory functions9 are some concerns for the HT. The LT has shown a decrease in leakage with the comparable oncological outcome and 5-year long-term survival.8,10 Chinese studies advocate preoperative 3D CT reconstruction to recognize variations11 in the mesenteric artery and vein to preserve LCA and expertise in laparoscopic12 procedure.
In this large cohort of laparoscopic anterior resection for rectal cancer, we aim to analyze the feasibility, safety, and oncological outcome of low-tie vs high-tie.
Methods
This retrospective cohort study included patients with rectal cancer who underwent laparoscopic anterior resection from January 2013 to December 2016 at the Department of Gastrointestinal Surgery, Renji Hospital, Jiao Tong University School of Medicine, Shanghai, China. Patients with a metastatic disease requiring additional procedures (organ resection), documented ischemic/atherosclerosis vascular disease, open surgery, abdominoperineal resection, having diverting stomas, and Hartmann’s procedures were excluded. The data from this cohort of AR for RC were analyzed and compared between LT vs HT groups for clinicodemographic variables (age, gender, body mass index “BMI”, diabetes, hypertension, neoadjuvant therapy, American Society of Anesthesiologist ASA grade, tumor size and location in the upper or lower rectum, and carcinoembryonic antigen CEA values). The operative data analyzed included duration of surgery (time for IMA ligation and completion of TME), blood loss, blood transfusion, level of colorectal anastomosis from the anal verge, the yield of LND around IMA, and total LN, tumor margins, and histopathology findings. Post-operative 30-day short-term outcome included urinary retention, ileus, flatus, AL, surgical site infection (SSI), grade of complication as per Clavien-Dindo (CD) classification15, hospital stay, and mortality. The long-term outcome included 3- and 5-years overall survival (OS) and disease-free survival (DFS). Ethical approval was obtained by the Institute Research Ethics Committee of Renji Hospital. Patient consent was not required because it was already archived data in the hospital electronic database, and we anonymized it for personal identification during analysis in compliance with the Declaration of Helsinki.
Data are from Renji Hospital. All laparoscopic surgeons are specialists with experience of more than 10 years of service at Renji. As per the hospital practice, a medial-to-lateral approach for laparoscopic dissection was used.13 In HT, the IMA was ligated at its origin within 1 cm from the aorta proximal to the branching of LCA. In LT, the IMA was skeletonized, and en-bloc LN dissection continued medially along with the IMA up to its root at the abdominal aortic (AA) plane and IMA was clipped distal to the branching of LCA to preserve the LCA,14 Figure 1A–B. The proximal colon was divided at 10 cm from the lesion. The distal rectal margin was maintained at 3 cm for tumors in the proximal rectum above the peritoneal reflection and 2 cm for tumors in the distal rectum below the peritoneal reflection. The specimen was removed via a small abdominal wall incision. The double staple technique was used for end-to-end colorectal anastomosis. An air leak test was performed to ensure the integrity of anastomosis, Figure 2A–D. The follow-up after discharge included clinical physical examination at 4–6 weeks and laboratory biochemical and radiological assessments every 3 months during the first 2-year, and thereafter every 6 months up to 5 years, as per our hospital protocol.
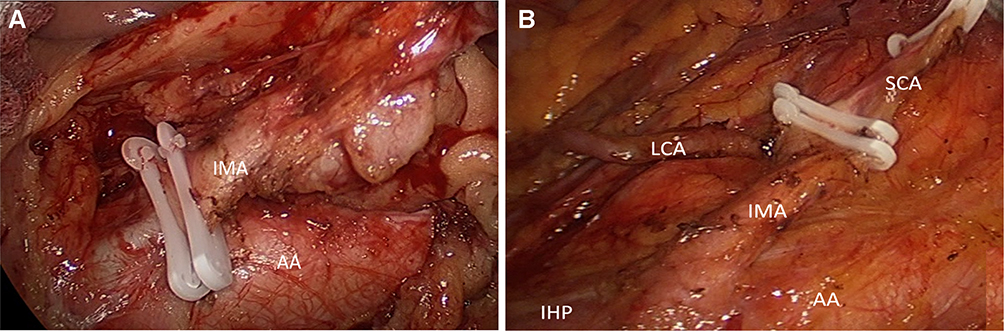 |
Figure 1 (A) High-tie, the IMA is ligated at its origin within 1 cm from the aorta, with dissection of the apical lymph nodes (LN); (B) Low-tie, the IMA and the proximal left colic artery (LCA) are skeletonized, LCA is preserved, the superior rectal artery (SRA) is ligated, LN dissection medially along the IMA root, including the abdominal aortic (AA) plane. |
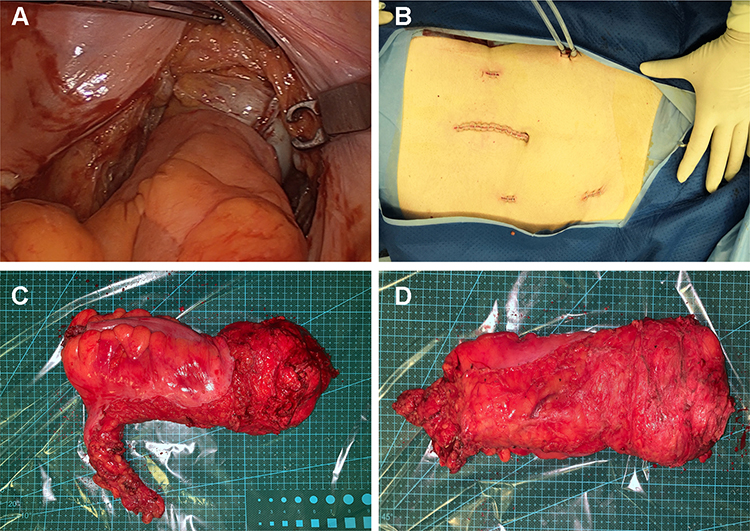 |
Figure 2 (A) Tension-free anastomosis after low-tie of IMA and preservation of LCA; (B) Completion of laparoscopic surgery for rectal cancer and skin closure of ports; (C-D) Retrieved specimen after low-tie and total mesorectal excision (TME) for rectal cancer. |
In this study, the short-term outcome was defined as complications (including bleeding, AL, colon ischemia, peritonitis, infection, urinary retention, ileus, or death) and their management (medical, radiological, surgical) within 30 postoperative days. The postoperative hospital stay was measured from the date of surgery to the date of discharge. Anastomotic leakage was analyzed as “leakage or no leakage” mentioned in the discharged diagnosis of the electronic database. In our hospital, the clinicians follow the diagnosis of leakage as defined by the International Study Group of rectal cancer.16 Follow-up information was obtained from medical records, outpatient clinic (and/or through phone interview) including recurrence of cancer, site of recurrence, and death until December 2019. Long-term outcome was defined as OS and DFS in 3 and 5 years.
We described the baseline characteristics, tumor characteristics, and oncologic treatments using descriptive statistics and compared these variables between high-tie and low-tie groups using the χ2 test for categorical variables and Wilcoxon Signed Rank Test for continuous variables. The categorical variables are expressed as frequency (%) and continuous variables as the median. Univariate and multivariate logistic regression was performed to identify the risk factors for anastomotic leakage (AL) in rectal tumor patients. We used univariable logistic regression for the association of level of ligation (high or low) with outcome in individual models including age ≥ 65 years, male, diabetes and/or hypertension, neoadjuvant treatment, and tumor location in the lower rectum. For long-term outcomes, Kaplan–Meier curves were plotted and patients with and without low-tie were compared using the Log rank test. Cox regression analyses were used to investigate the influence of low-tie on overall survival and disease-free survival. Missing values were disregarded and thus not imputed. Exposure and outcome variables were complete for all individuals. All baseline, tumor-related, and cancer treatment-related variables were complete for all individuals. We conducted the statistical analysis in SPSS 22.0 (IBM Corporation, 2013, New York, USA) and R project version 3.3.2 (Foundation for Statistical Computing, Vienna, Austria). We considered a two-tailed p-value of < 0.05 to be statistically significant.
Results
Overall, a cohort of 614 (LT 236, HT 378) patients were included in the study. In the LT group, the LCA was preserved in all cases, and the division of LCA was not required due to tension at the colorectal anastomosis. In demographic characteristics, diabetes and/or hypertension in the LT group were more common compared to HT, 19.07 vs 12.69, p=0.032. Neoadjuvant treatment was performed in 47 (12.54%) patients, similar in both groups, 11.38% in HT and 14.41% LT, p=0.270. Tumor located in lower rectum was 238 (38.76%), more in LT (39.83%) than HT (32.76%), p=0.080, Table 1.
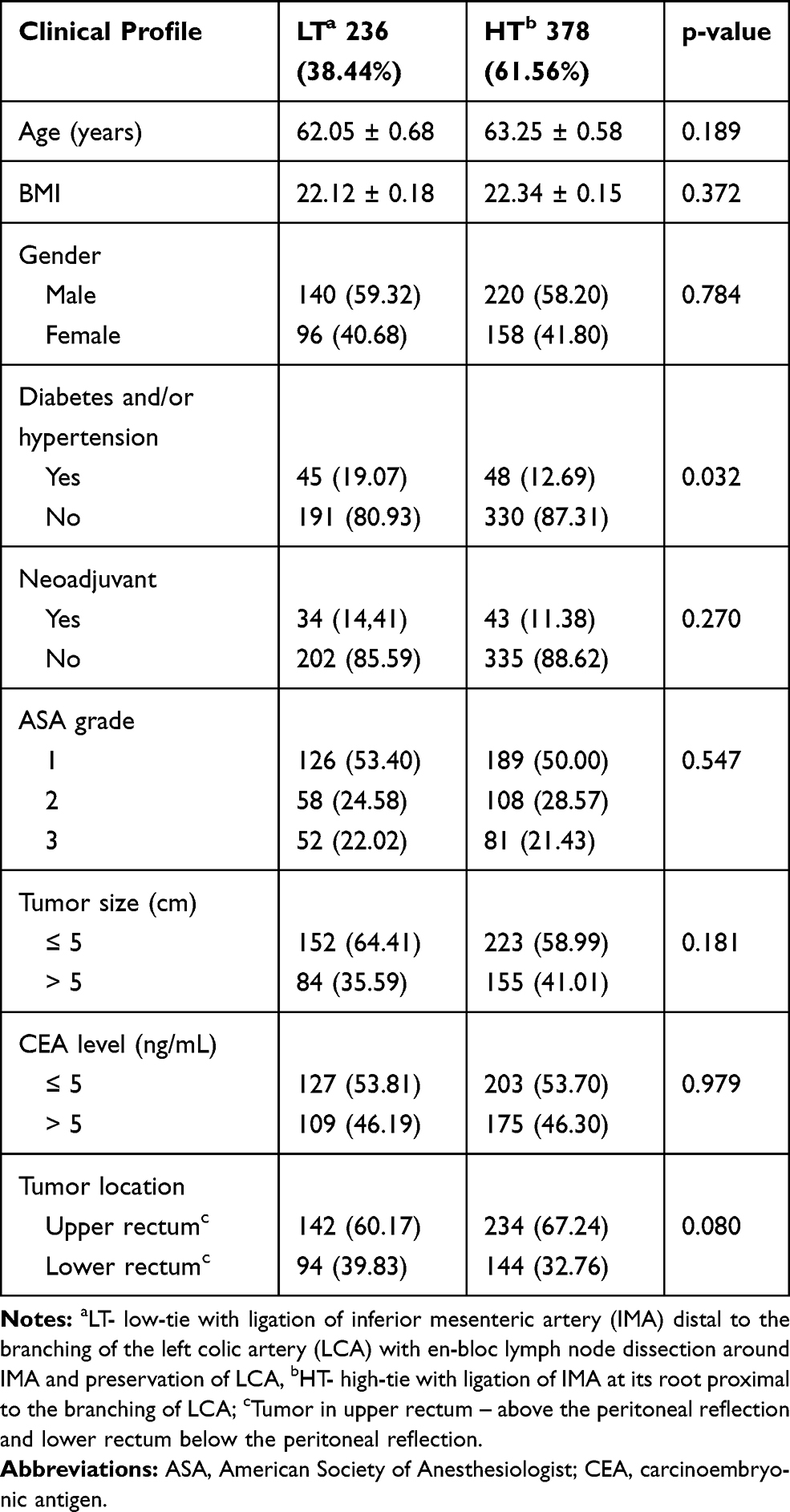 |
Table 1 Clinicodemographic Profile of Patients with Low-Tie vs High-Tie of the Inferior Mesenteric Artery in Laparoscopic Anterior Resection of Rectal Cancer, N=614 |
In perioperative parameters, the duration of surgery in LT (146.0 ± 2.46 min) was longer than in HT (138.6 ± 2.01 min), p=0.021. The time required for IMA tie in LT (41.46 ± 0.66 min) was longer than HT (32.69 ± 0.59 min), p=0.000. Blood loss, LND, level of anastomosis from the anal verge, and pathological margins were not significantly different in the two groups. Patients with positive IMA root nodes also had positive intermediate or perirectal lymph nodes, Table 2.
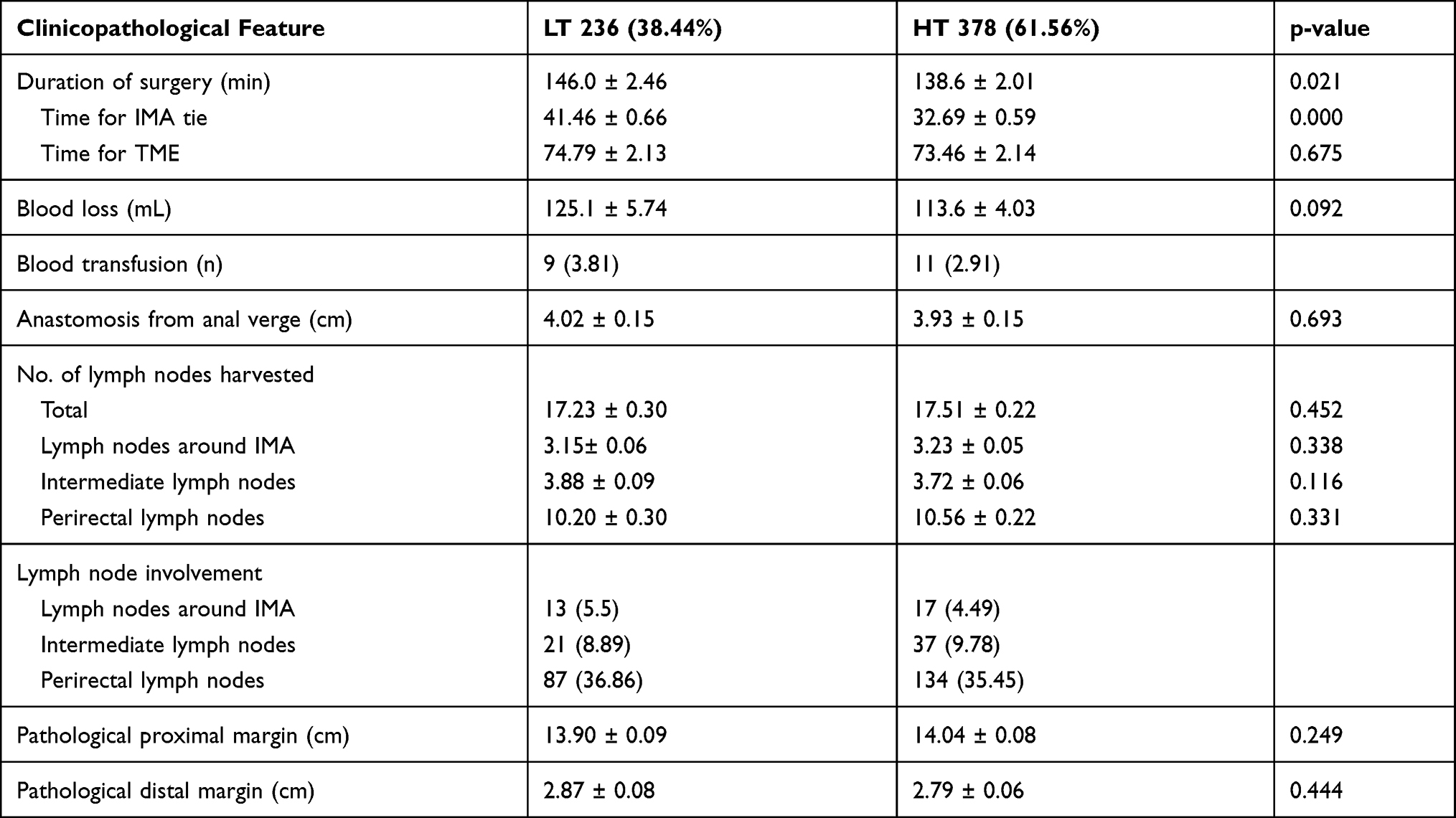 |
Table 2 Operative Findings of Rectal Cancer Patients with LT vs HT in Laparoscopic Anterior Resection of Rectal Cancer, N=614 |
In postoperative outcome, 207 (33.71%) patients had complications, 30.08% in LT vs 35.98% in HT, p=0.133. Postoperative severe complications (CD grade III–IV) were lower in LT than HT (7.98% vs 11.90%, p=0.120).
Anastomotic leaks were found in 75 (12.21%) patients, less in LT (8.89%) than HT (14.28%), p=0.047. Hazard ratio, uni- and multivariate analysis for factors associated with anastomotic leakage included male, elder age, diabetes and/or hypertension, neoadjuvant treatment, and lower rectum. As per our main focus, we estimated the effect of low-tie in anastomotic leakage and found that for tumors located in the lower rectum, there was fewer leakage in LT than HT (10.64% vs 20.83%), p=0.040. Patients with associated comorbidities of diabetes and/or hypertension, with neoadjuvant treatment, age ≥65 years, and male gender also had a lower leak in LT than HT, but the difference was not significant, p>0.05, Tables 3 and 4.
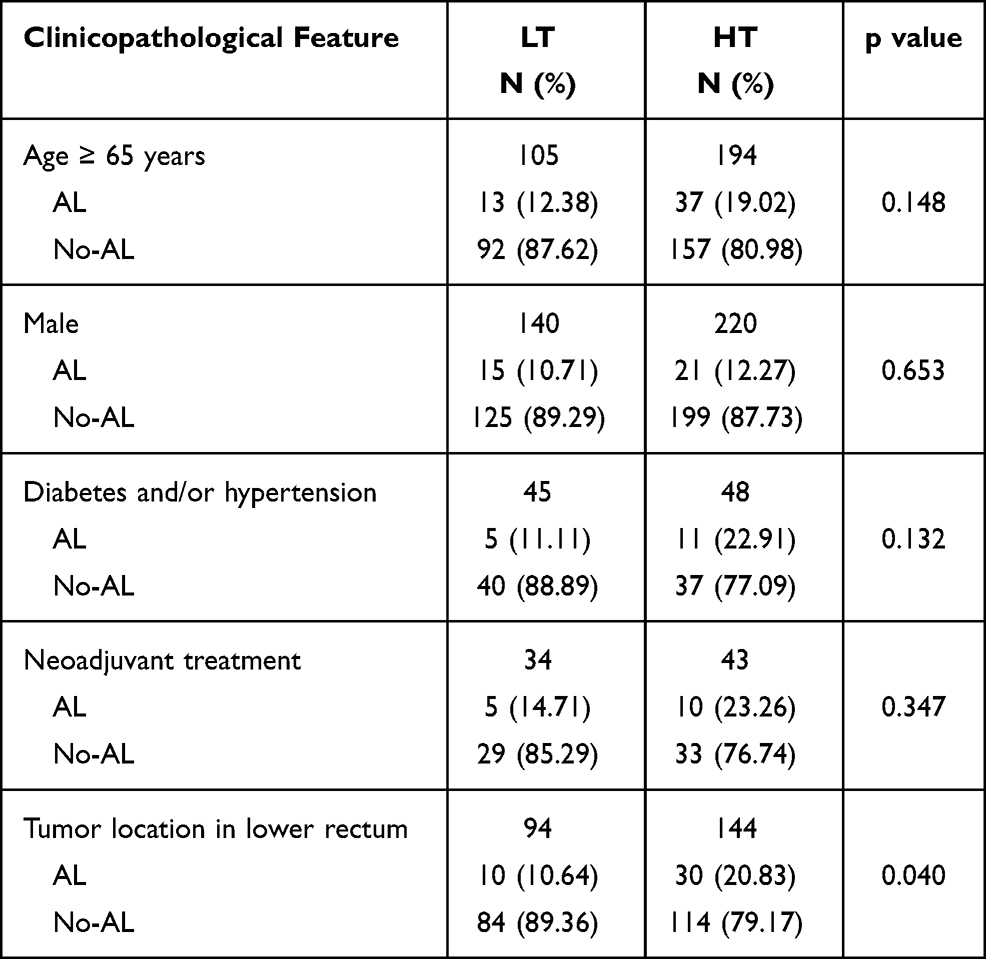 |
Table 3 Risk Factors for Anastomotic Leakage in Patients with LT vs HT in Laparoscopic Anterior Resection for Rectal Cancer, N=614 |
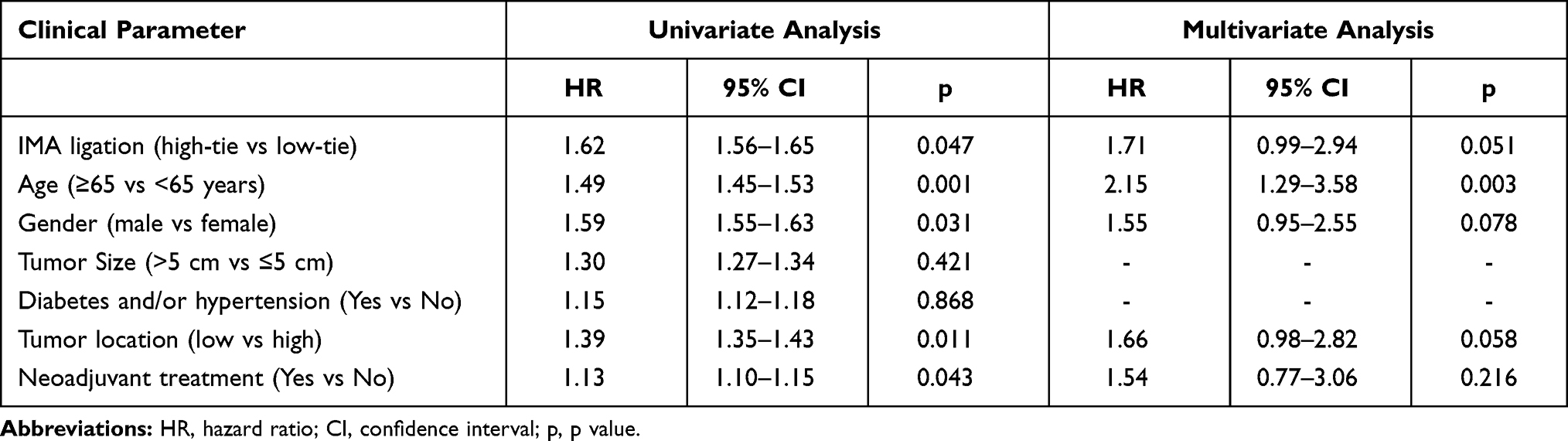 |
Table 4 Hazard Ratio in for Anastomotic Leakage in Patients with LT vs HT in Laparoscopic Anterior Resection for Rectal Cancer, N=614 |
In short-term outcome, there was no death within 30 days in either group. Long-term outcomes in two groups were not significantly different, with 3-years OS (LT 81.78% vs HT 83.33%, p=0.658) and DFS (LT 78.38% vs HT 83.33%, p=0.143) and 5-years OS (LT 59.51% vs HT 61.46%, p=0.671) and DFS (LT 52.20% vs 53.52%, p=0.690), Table 5, Figure 3A–D.
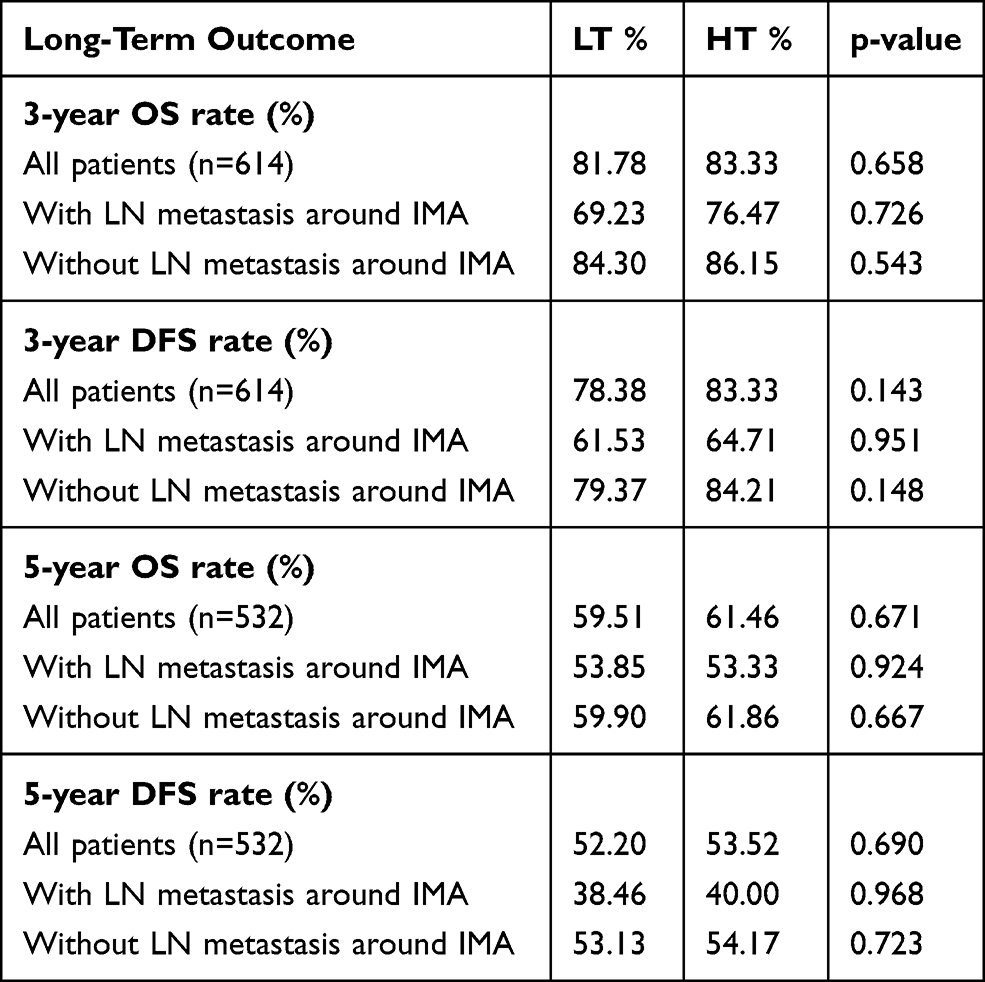 |
Table 5 Long-Term Results of Overall Survival (OS) and Disease-Free Survival (DFS) in Patients with LT vs HT Anterior Resection of Rectal Cancer, N=614 |
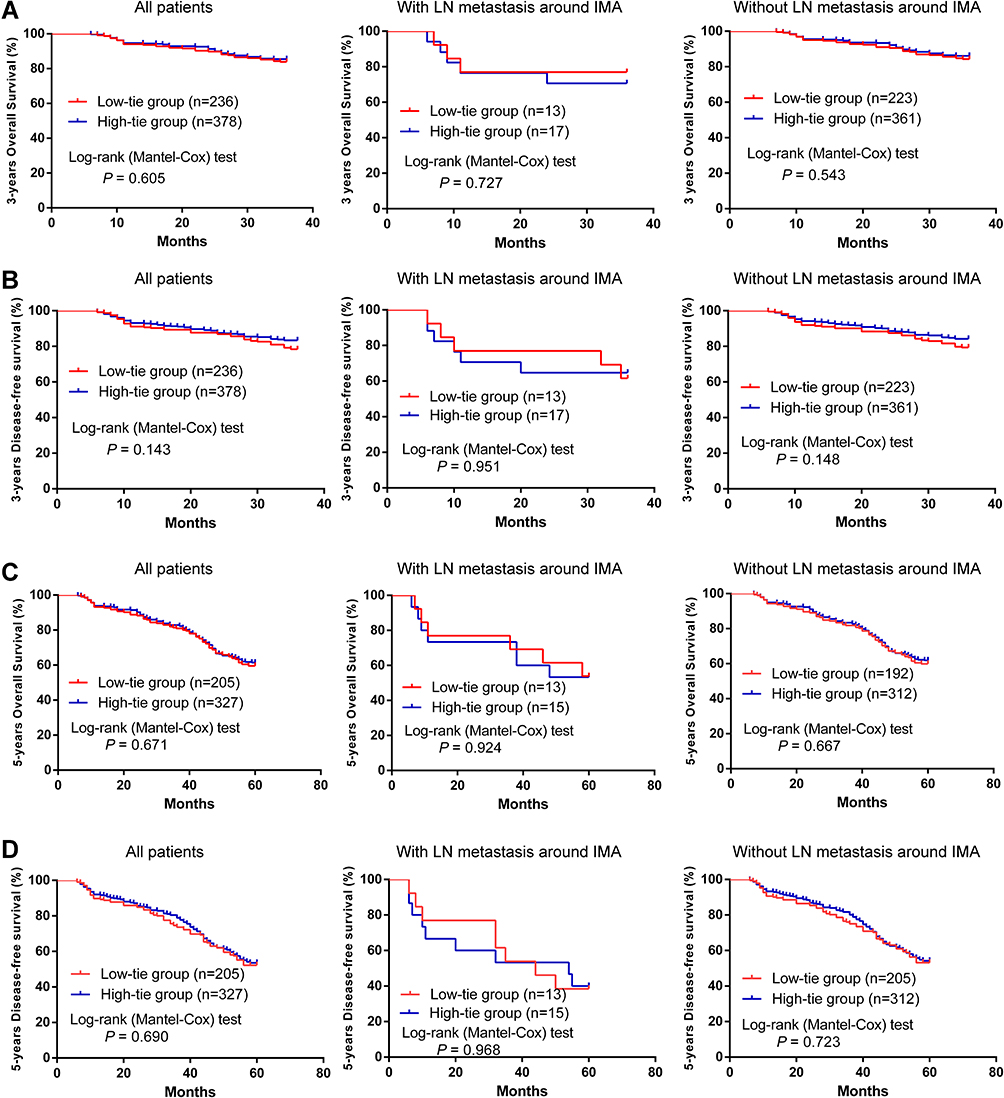 |
Figure 3 Long-term outcomes in the low-tie groups and high-tie groups. (A) 3-years OS with all patients, LN metastasis around IMA patients, and without LN metastasis around IMA patients; (B) 3-years DFS with all patients, LN metastasis around IMA patients, and without LN metastasis around IMA patients; (C) 5-years OS with all patients, LN metastasis around IMA patients, and without LN metastasis around IMA patients; (D) 5-years DFS with all patients, LN metastasis around IMA patients, and without LN metastasis around IMA patients. |
Discussion
Our finding shows that the most feared complications in colorectal surgery, the leakage occurred in 75 (12.21%), and at a significantly lower rate in the LT group compared to HT, 8.89% vs 14.28%, p=0.047. Among the associated risk factors, only the level of “tumor in lower rectum” was significantly associated with leakage, occurring in 10 (10.64%) in LT compared to 30 (20.83%) in HT group, p=0.040. This could be due to better blood supply in the LT group by the preservation of LCA. Other studies have reported that male gender, elder age, diabetes and/or hypertension, neoadjuvant treatment, and tumor in the lower rectum were associated with anastomotic leakage.17–19 In our study, “diabetes and/or hypertension, neoadjuvant treatment, age ≥65 years, and male gender” had a higher percentage of leakage in HT than LT, but the difference was not statistically significant.
We found no significant difference in yield of lymph node between the two groups, both in terms of the number of nodes harvested around IMA (LT 3.15± 0.06 vs HT 3.23 ± 0.05, p=0.338) and total lymph nodes (LT 17.23 ± 0.30 vs HT 17.51 ± 0.22, p=0.452). For the past 100 years, it is still a controversial topic, and debate for the optimal level of IMA ligation has continued for better radical resection and oncological staging.20,21 Our results for this cohort of 614 rectal cancer suggest LT maintains the oncological principle of radicality with adequate LND around IMA in laparoscopic anterior resection.
In the present study, the overall postoperative early recovery in terms of ‘time to first flatus’ was better in LT. We also found that there were fewer complications of mild grade (CD I–II) and severe grade (CD III–IV) in LT than HT. However, the differences were statistically not significant. The dreaded short-term complication of leakage was significantly less in LT than in HT. However, we could analyze “leakage or no leakage” as per the discharge diagnosis in the electronic record, and could not further analyze the grading of the anastomotic leak as defined by the International Study Group of rectal cancer.16 However, in our hospital, the clinicians follow the diagnosis of leakage as per international norms. Studies have shown that patients with leakage have a poor perioperative recovery, requiring a longer period of antibiotics, drainage of collection, and reoperation and may cause local recurrence and diminished survival.22,23
Maintaining blood supply and ensuring a tension-free anastomosis reduces the incidence of AL.24 Preserving LCA in LT ensures adequate blood supply and oxygenation to the remaining colon. In contrast, the blood supply of the remaining distal colon in the case of HT solely depends on the middle colic and marginal arteries.25,26 The doppler flowmetry has shown IMA clamping results in a >50% reduction in blood flow27 to the anastomosis and development of proximal bowel necrosis or ischemia5,28 after HT of IMA.
Similar to our finding of reduced rate of AL in LT, other studies have also reported a reduced rate of leakage in LT.29 However, there are reports which did not demonstrate a statistical difference in leakage between LT and HT.30,31 This may be due to other related factors related to surgeons and/or patients which may have a role in leakage of the anastomosis.
Tension at anastomosis is an important factor for leakage. The HT has traditionally been thought to help preserve sufficient bowel length for tension-free anastomosis.4,32 However, reports show that preserving LCA and mobilization of splenic flexure provide adequate bowel length for tension-free anastomosis.29 In the present study, our results show that tension-free anastomosis is feasible in all cases in the LT group, without the need for re-do of anastomosis because of the in-adequate remaining length of the colon or undue tension for anastomotic reconstruction. And, significantly less leakage was observed in our cohort of patients with adequate length of the remaining colon for tension-free anastomosis was reflected in the LT group.
Historically, the HT of IMA in CRC has been credited for the ease of LND, including the LN at IMA root, to achieve accurate pathological staging and improvement in overall prognosis.32,33 The IMA root lymph nodes metastasis has been reported in 1.7 to 7.8% of cases.34,35 The development of laparoscopic technology and the feasibility of LND around IMA with preservation of LCA is a feasible and valid surgical treatment. In a randomized clinical trial of 324 RCs, the 5-year outcome of the LT group did not differ from the HT.36 Our study has reaffirmed the good oncological outcomes of LT with no significant differences between the number of harvested lymph nodes compared to HT (17.23 ± 0.30 vs 17.51 ± 0.22). Also, we found that the long-term 3- and 5-year survival (OS and DFS) of LT and HT were comparable.
Some of the limitations of the present study include those inherent to the retrospective data analysis. There may be a selection bias from the individual surgeon for techniques and we could not analyze the variables like metastasis, atherosclerosis, use of neoadjuvant therapy, transanal drainage tube, diverting stoma, circumferential resection margin, the severity of leak due to inconsistency in detail in the electronic database. However, clinicians at our hospital do practice as per international norms to define anastomotic leakage, the preoperative staging of the tumor and neoadjuvant therapy, etc. All these issues may be answered by a prospective study with detailed data-keeping, preferably a multi-institutional accumulation of data in Shanghai and at the national level. In the present study, our main aim was to analyze the feasibility, safety, and oncological outcome of low vs high ligation of the inferior mesenteric artery.
In conclusion, our findings of a retrospective analysis of a cohort of 641 patients with rectal cancer who underwent laparoscopic anterior resection affirm that low-tie (LT) of the inferior mesenteric artery with preservation of left colic artery maintains the oncological principle for lymph node dissection around and at the root of the inferior mesenteric artery, and had improved short-term outcome of less anastomotic leakage compared to high-tie (HT), possibly due to better preservation of blood supply. The 3- and 5-year long-term overall survival and disease-free survival did not differ significantly between the LT and HT groups. Thus, our findings provide evidence for safety and feasibility for low-tie laparoscopic anterior resection for rectal cancer, maintain the oncological principle of adequate lymph node dissection around the inferior mesenteric artery, had fewer leakage compared to high-tie with and comparable long-term overall and disease-free survival.
Funding
This work was supported by the grant from Shanghai Municipal Commission of science and technology (19411966200) and the National Natural Science Foundation of China (no. 81802308, 81873555).
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Zhang L, Cao F, Zhang G, et al. Trends in and predictions of colorectal cancer incidence and mortality in China from 1990 to 2025. Front Oncol. 2019;9:98.
2. Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery–the clue to pelvic recurrence? Br J Surg. 1982;69(10):613–616.
3. Kim CS, Kim S. Oncologic and anastomotic safety of low ligation of the inferior mesenteric artery with additional lymph node retrieval: a case-control study. Ann Coloproctol. 2019;35(4):167–173.
4. Bonnet S, Berger A, Hentati N, et al. High tie versus low tie vascular ligation of the inferior mesenteric artery in colorectal cancer surgery: impact on the gain in colon length and implications on the feasibility of anastomoses. Dis Colon Rectum. 2012;55(5):515–521.
5. Park MG, Hur H, Min BS, Lee KY, Kim NK. Colonic ischemia following surgery for sigmoid colon and rectal cancer: a study of 10 cases and a review of the literature. Int J Colorectal Dis. 2012;27(5):671–675.
6. Guo Y, Wang D, He L, et al. Marginal artery stump pressure in left colic artery-preserving rectal cancer surgery: a clinical trial. ANZ J Surg. 2017;87(7–8):576–581.
7. Son GM, Kim TU, Park B-S, et al. Colonic hypoperfusion following ligation of the inferior mesenteric artery in rectosigmoid colon cancer patients. Ann Surg Treat Res. 2019;97(2):74–82.
8. Fan Y-C, Ning F-L, Zhang C-D, Dai D-Q. Preservation versus non-preservation of left colic artery in sigmoid and rectal cancer surgery: a meta-analysis. Int J Surg. 2018;52:269–277.
9. Yang XF, Li GX, Luo GH, Zhong SZ, Ding ZH. New insights into autonomic nerve preservation in high ligation of the inferior mesenteric artery in laparoscopic surgery for colorectal cancer. Asian Pac J Cancer Prev. 2014;15(6):2533–2539.
10. Zeng J, Su G. High ligation of the inferior mesenteric artery during sigmoid colon and rectal cancer surgery increases the risk of anastomotic leakage: a meta-analysis. World J Surg Oncol. 2018;16(1):157.
11. Wang KX, Cheng ZQ, Liu Z, Wang XY, Bi DS. Vascular anatomy of inferior mesenteric artery in laparoscopic radical resection with the preservation of left colic artery for rectal cancer. World J Gastroenterol. 2018;24(32):3671–3676.
12. Zang W, Liu S, He H. Laparoscopic anterior resection of rectal cancer with lymph node dissection around the inferior mesenteric artery with preservation of the left colic artery (LAR-LND-PLCA). Ann Laparosc Endosc. 2016;1:6.
13. Liang JT, Shieh MJ, Chen CN, Cheng YM, Chang KJ, Wang SM. Prospective evaluation of laparoscopy-assisted colectomy versus laparotomy with resection for management of complex polyps of the sigmoid colon. World J Surg. 2002;26(3):377–383.
14. Yamamoto M, Okuda J, Tanaka K, Ishii M, Hamamoto H, Uchiyama K. Oncological impact of laparoscopic lymphadenectomy with preservation of the left colic artery for advanced sigmoid and rectosigmoid colon cancer. Dig Surg. 2014;31(6):452–458.
15. Dindo D, Demartines N, Clavien P-A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213.
16. Rahbari NN, Weitz J, Hohenberger W, et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: a proposal by the International Study Group of Rectal Cancer. Surgery. 2010;147(3):339–351.
17. Fukada M, Matsuhashi N, Takahashi T, et al. Risk and early predictive factors of anastomotic leakage in laparoscopic low anterior resection for rectal cancer. World J Surg Oncol. 2019;17(1):178.
18. Walker KG, Bell SW, Rickard MJFX, et al. Anastomotic leakage is predictive of diminished survival after potentially curative resection for colorectal cancer. Ann Surg. 2004;240(2):255–259.
19. Parthasarathy M, Greensmith M, Bowers D, Groot-Wassink T. Risk factors for anastomotic leakage after colorectal resection: a retrospective analysis of 17 518 patients. Colorectal Dis. 2017;19(3):288–298.
20. Cirocchi R, Trastulli S, Farinella E, et al. High tie versus low tie of the inferior mesenteric artery in colorectal cancer: a RCT is needed. Surg Oncol. 2012;21(3):e111–23.
21. Draginov A, Chesney TR, Quereshy HA, Chadi SA, Quereshy FA. Association of high ligation versus low ligation of the inferior mesenteric artery on anastomotic leak, postoperative complications, and mortality after minimally invasive surgery for distal sigmoid and rectal cancer. Surg Endosc. 2019.
22. Ramphal W, Boeding JRE, Gobardhan PD, et al. Oncologic outcome and recurrence rate following anastomotic leakage after curative resection for colorectal cancer. Surg Oncol. 2018;27(4):730–736.
23. Gessler B, Eriksson O, Angenete E. Diagnosis, treatment, and consequences of anastomotic leakage in colorectal surgery. 2017;32(4):549–556.
24. Girard E, Trilling B, Rabattu PY, et al. Level of inferior mesenteric artery ligation in low rectal cancer surgery: high tie preferred over low tie. Tech Coloproctol. 2019;23(3):267–271.
25. Seike K, Koda K, Saito N, et al. Laser Doppler assessment of the influence of division at the root of the inferior mesenteric artery on anastomotic blood flow in rectosigmoid cancer surgery. Int J Colorectal Dis. 2007;22(6):689–697.
26. Rutegård M, Hassmén N, Hemmingsson O, Haapamäki MM, Matthiessen P, Rutegård J. Anterior resection for rectal cancer and visceral blood flow: an explorative study. Scand J Surg. 2016;105(2):78–83.
27. Dworkin MJ, Allen-Mersh TG. Effect of inferior mesenteric artery ligation on blood flow in the marginal artery-dependent sigmoid colon. J Am Coll Surg. 1996;183(4):357–360.
28. Tsujinaka S, Kawamura YJ, Tan KY, et al. Proximal bowel necrosis after high ligation of the inferior mesenteric artery in colorectal surgery. Scand J Surg. 2012;101(1):21–25.
29. Buunen M, Lange MM, Ditzel M, Kleinrensink G, Lange JF. Level of arterial ligation in total mesorectal excision (TME): an anatomical study. Int J Colorectal Dis. 2009;24(11):1317–1320.
30. Fujii S, Ishibe A, Ota M, et al. Short-term and long-term results of a randomized study comparing high tie and low tie inferior mesenteric artery ligation in laparoscopic rectal anterior resection: sub-analysis of the HTLT (high tie vs. Low Tie) Study. Surg Endosc. 2019;33(4):1100–1110.
31. Matsuda K, Hotta T, Takifuji K, et al. Randomized clinical trial of defaecatory function after anterior resection for rectal cancer with high versus low ligation of the inferior mesenteric artery. BJS Br J Surg. 2015;102(5):501–508.
32. Hida J-I, Okuno K. High ligation of the inferior mesenteric artery in rectal cancer surgery. Surg Today. 2013;43(1):8–19.
33. Chin CC, Yeh CY, Tang R, Changchien CR, Huang WS, Wang JY. The oncologic benefit of high ligation of the inferior mesenteric artery in the surgical treatment of rectal or sigmoid colon cancer. Int J Colorectal Dis. 2008;23(8):783–788.
34. Kang J, Hur H, Min BS, Kim NK, Lee KY. Prognostic impact of inferior mesenteric artery lymph node metastasis in colorectal cancer. Ann Surg Oncol. 2011;18(3):704–710.
35. Huh JW, Kim YJ, Kim HR. Distribution of lymph node metastases is an independent predictor of survival for sigmoid colon and rectal cancer. Ann Surg. 2012;255(1):70–78.
36. Fujii S, Ishibe A, Ota M, et al. Randomized clinical trial of high versus low inferior mesenteric artery ligation during anterior resection for rectal cancer. BJS Open. 2018;2(4):195–202.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.