")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Lung-Protective Effects of Lidocaine Infusion on Patients with Intermediate/ High Risk of Postoperative Pulmonary Complications: A Double-Blind Randomized Controlled Trial
Authors Wang X, Guo K, Zhao Y, Li T, Yang Y, Xu L, Liu S
Received 15 January 2022
Accepted for publication 26 March 2022
Published 8 April 2022 Volume 2022:16 Pages 1041—1053
DOI https://doi.org/10.2147/DDDT.S358609
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Xinghe Wang,1– 3,* Kedi Guo,1– 3,* Ye Zhao,4,* Tong Li,1– 3 Yuping Yang,1– 3 Lingfei Xu,1,3 Su Liu1– 3
1NMPA Key Laboratory for Research and Evaluation of Narcotic and Psychotropic Drugs, Xuzhou Medical University, Xuzhou, People’s Republic of China; 2Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China; 3Jiangsu Province Key Laboratory of Anesthesiology, Xuzhou Medical University, Xuzhou, People’s Republic of China; 4Department of Anesthesiology, Changzhou Maternal and Child Health Care Hospital, Changzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Su Liu, Department of Anesthesiology, The Affiliated Hospital of Xuzhou Medical University, 99 Huaihai West Road, Xuzhou, Jiangsu, 221000, People’s Republic of China, Tel +86 18118309692, Email [email protected]
Purpose: The non-local anesthetic effects of lidocaine have been widely reported, but there are still few studies on lung protection. We aimed to test the hypothesis that intravenous infusion of lidocaine exerts lung-protective effects in patients at intermediate/high risk of postoperative pulmonary complications (PPCs) on major abdominal surgery.
Patients and Methods: Patients ≥ 18 years, ASA II or III, with intermediate/high risk for PPCs, were included. Patients were randomly assigned into group lidocaine (received a bolus of lidocaine 1.5 mg kg− 1 before the induction of anesthesia, then followed by a continuous infusion of 2.0 mg kg− 1 h− 1 intraoperatively until the end of surgery) or group control (received 0.9% saline in place of lidocaine at the same time points). The incidence of PPCs within 7 postoperative days was measured, defined as a collapsed composite outcome of atelectasis, respiratory infection, pleural effusion, pneumonia, respiratory failure or acute respiratory distress syndrome (ARDS) developed within 7 postoperative days, or hospital discharge, whichever came sooner.
Results: Of 200 subjects screened, 195 patients were finally analyzed. Overall, 35.9% (70/195) patients sustained PPCs, which occurred fewer in group lidocaine 25.8% (25/97), compared with group control 45.9% (45/98) (relative risk: 0.56, 95% CI: 0.38 to 0.84; absolute risk reduction: − 20.1%; P = 0.003). Considering single PPCs episode, the most common PPC in both groups was atelectasis. The atelectasis incidence was 11.3% (11/97) in group lidocaine, much lower than that in group control 29.6% (29/98) (relative risk: 0.38, 95% CI: 0.20 to 0.72; absolute risk reduction: − 18.3%, P = 0.002). However, the incidences of any other PPCs episodes were similar between the two groups.
Conclusion: Intraoperative intravenous infusion lidocaine could decrease the incidence of PPCs in patients at intermediate/high risk of postoperative pulmonary complications undergoing major abdominal surgery.
Keywords: postoperative pulmonary complications, lidocaine, lung injury, pulmonary protection
Introduction
Postoperative pulmonary complications (PPCs) are one of the main causes of morbidity and mortality in patients undergoing surgery requiring anesthesia,1 especially within the first postoperative week.2 The incidence of PPCs in major surgery ranges from 11%-59%, which differ depending on the PPCs definitions and types of surgery.3 The reasons for PPCs are complex and the underlying mechanisms are unclear, which may include the prior health status of the patient and the effects of anesthesia and surgical trauma.4 The patient’s overall health has a strong influence on the development of complications. Surgery and anesthesia can induce inflammatory responses. A previous study found that inflammation plays a key role in the development of PPCs.5 In addition, respiratory depression caused by opioids, and postoperative pain-induced voluntary limitation of respiratory motion can also increase the risk of PPCs.6,7
Lidocaine, an amide-based local anesthetic and membrane stabilizer, is widely used in local nerve block and anti-arrhythmia. Recently, numerous studies have found that lidocaine also has anti-inflammatory effects.8–10 Intravenous administration lidocaine could attenuate lung injury induced by endotoxin, hyperoxia, and ischemia/reperfusion injury by inhibiting inflammatory cascade reaction.11–13 Several clinical studies showed that perioperative administration of lidocaine was significantly associated with attenuation of the surgery-induced release of pro-inflammatory cytokines, and decreased C-reactive protein levels.10,14 Besides, intravenous infusion of lidocaine can also exert analgesia and relieve postoperative pain, which can further reduce opioid consumption.15
Therefore, considering these non-local anesthetic effects of lidocaine are associated with PPCs risk factors, we hypothesized that intravenous infusion of lidocaine may alleviate lung injury, protect pulmonary function, reduce the incidence of PPCs and improve the prognosis in surgical patients.
Patients and Methods
Ethical approval for this study was provided by the Ethical Committee of the Affiliated Hospital of Xuzhou Medical University, Jiangsu, China (Chairperson Prof Tie Xu) on 1 January 2019 with protocol number XYFY2019-KL105-01. The trial was registered in the Chinese Clinical Trial Registry (ChiCTR1900021677). This report adheres to the CONSORT guidelines. The study was conducted according to the guidelines of the Declaration of Helsinki with Good Clinical Practice. All participants provided written informed consent before enrolment.
Participants
Patients aged ≥ 18 years, ASA classification II to III, with an intermediate-to-high risk for PPCs (defined by Assess Respiratory Risk in Surgical Patients in Catalonia score (ARISCAT)≥26; Low Risk<26, Intermediate Risk 26–44, High Risk≥45),16 and undergoing selective abdominal surgery under general anesthesia were eligible for inclusion. Exclusion criteria were: body mass index (BMI)>30 kg m−2, emergency surgery, preoperative ventilator use, Adams syndrome, severe heart block (II or III atrioventricular block, double-bundle branch block), severe sinoatrial node dysfunction, congestive heart failure, liver parenchyma damage (ALT or AST>2× normal value), Child-Pugh grade C cirrhosis, renal failure (SCr>177 µmol l−1), respiratory failure, epilepsy history, lidocaine allergy, steroid anti-inflammatory drug use 24 h before surgery, pregnancy, and refusal to provide written informed consent or to participate in testing. Rejection criteria included operation cancellation, voluntary patient dropout, short surgery duration (<2 hours), and/or serious perioperative adverse events.
Randomization and Masking
Patients were allocated randomly to group lidocaine or group control in a 1:1 ratio. Randomization was done with a web-based computer-generated block randomization procedure after stratified according to the type of surgery (laparoscopy or open) and surgery site (upper or lower abdomen). The allocation sequence was generated by one of the independent investigators, who provided the randomization assignments to the operating room pharmacy that assigned patients to the study groups and prepared all of the study medications. Intervention staff, patients, outcome assessors, and investigators involved in trial and data management were masked to group assignment.
Intervention
Patients in group lidocaine received a bolus of lidocaine 1.5 mg kg−1 (10 mg mL−1 in a 20-mL syringe) before the induction of anesthesia, then followed by a continuous infusion of 2.0 mg kg−1 h−1 (10 mg mL−1 in a 50-mL syringe) intraoperatively until the end of surgery. Patients in group control received 0.9% saline in place of lidocaine at the same time points.
Perioperative Management
Patients were given 2 mg of midazolam (i.v.) after entering the operating room. Standard intraoperative monitoring was applied, which included electrocardiography, capnography, pulse oximetry, and bispectral index (BIS) monitoring. In addition, a radial artery cannula was placed for monitoring arterial pressure and blood gas. Anesthesia was induced with lidocaine (1.5 mg kg−1) (or the same volume of 0.9% saline), propofol 1–2 mg kg−1, sufentanil 0.5 μg kg−1, and cisatracurium 0.2 mg kg−1. The lidocaine or 0.9% saline infusion was initiated after induction and dosed as described above. Anesthesia was maintained by remifentanil (0.1–0.3 μg kg−1 min−1) and propofol, combined with sevoflurane 1%. Maintain the BIS values between 40 and 60 by adjusting the dose of propofol. All patients accepted ultrasound-guided bilateral transverse abdominis plane block (0.25% ropivacaine 40 mL) after anesthesia induction. Mean arterial pressure was maintained within ± 20% of the baseline. Hypotension was treated with phenylephrine 40 µg, ephedrine 5mg, or a fluid bolus; episodes of hypertension were managed by increasing the propofol or remifentanil infusion rate. Lung protective ventilation was used during surgery (the combination of tidal volume 8 mL kg−1 predicted body weight or lower and PEEP 5 cm H2O or higher, with a recruitment manoeuvre, fraction of inspired oxygen 60%). Cisatracurium was injected intermittently according to requirements. Patients in both groups received i.v. acetaminophen 1 g at the beginning of the stitching. At the end of the surgical procedure, neuromuscular block was reversed and extubation was attempted in the operating theatre. Patients who did not meet extubation criteria were transferred to the post-anesthesia care unit (PACU).
Postoperative patient-controlled intravenous analgesia (PCA) was performed with drug formulations (sufentanil 2 μg kg−1, tropisetron 10 mg, 0.9% saline diluted to 100 mL) using a set lock time of 15 min, a background infusion dose to 2 mL h−1, and the PCA was set at 0.5 mL times−1. Patients were assessed for pain at PACU by nurses and every 15min thereafter (0 to 10 cm, Visual Analogue Scale (VAS) score, 0 indicates “no pain” and 10 indicates “most severe pain”; 1–3, mild pain; 4–6, moderate pain; 7–10, severe pain). Moderate pain was treated with hydromorphone 0.25mg, and severe pain with hydromorphone 0.5mg, to reduce pain scores to less than or equal to 3. Discharge to the surgical wards when Aldrete scores of greater than or equal to 8 out of 10 were achieved. Pain was managed on the first 2 postoperative days using the PCA device, which was discontinued at the discretion of the managing surgical service. Patients were transitioned to tramadol 50 mg tablets when able to resume oral intake. Pain was assessed and treated by surgical ward nurses per standard protocols, to maintain pain scores less than or equal to 3.
Endpoints
We initially used the CC-16 protein as the main outcome of this study, but considered that the relationship between CC-16 protein concentration and lung damage remains controversial.5,17 As a composite clinical indicator, PPCs can directly and comprehensively reflect the postoperative lung function of patients, which may better reflect the lung protection effect of intraoperative intravenous infusion lidocaine. Therefore, we changed CC-16 to a secondary outcome, and changed the primary outcome to the incidence of PPCs, defined as a collapsed composite outcome of atelectasis, respiratory infection, pleural effusion, pneumonia, respiratory failure or acute respiratory distress syndrome (ARDS) developed within 7 postoperative days (PODs), or hospital discharge, whichever came sooner. This was approved by the Ethics Committee and written informed consent was obtained from all patients. Assessors masked to group allocation assessed participants prospectively and daily until the seventh postoperative day. Participants were screened using standardized validated diagnostic criteria (Box 1).18,19 A PPC was diagnosed when one or more of these criteria were present at any time. Patients discharged before the end of follow-up without any PPCs were considered as without PPCs at 7 PODs.
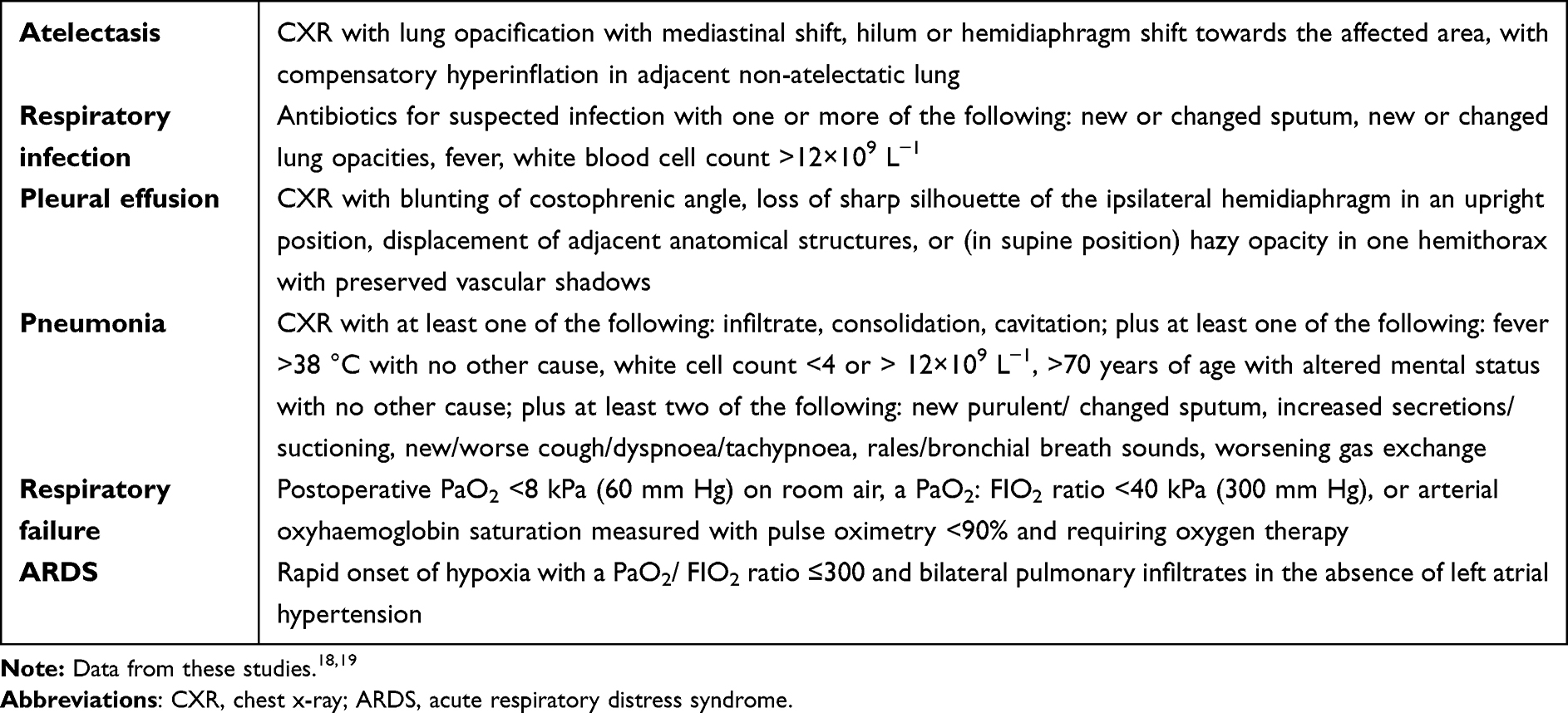 |
Box 1 Postoperative Pulmonary Complications Diagnostic Criteria |
The secondary outcomes included: (1) plasma concentration of CC-16, IL-6, and IL-10; (2) parameters reflecting pulmonary function and mechanics: oxygenation index (OI=PaO2/FiO2, respiratory index (RI=A-aDO2/PaO2), dynamic lung compliance (Cdyn=Vt/(Pmax-PEEP)) and driving pressure (ΔP); (3) hemodynamics (heart rate and mean arterial pressure); (4) postoperative total opioid consumption (in mg morphine equivalents (MEQ); (5) postoperative pain level (0 to 10 cm, Visual Analogue Scale (VAS) score, 0 indicates “no pain” and 10 indicates “most severe pain”); (6) gastrointestinal recovery; (7) The quality of recovery-40 score (QoR-40 score) at 24 h postoperatively; (8) length of hospital stay (defined as the time from the end of the surgery to discharge); (9) adverse events (death, arrhythmia, light-headedness, perioral numbness, and dizziness).
Data Collection
The day before the operation, the patient’s baseline characteristics were recorded. On the operation day, the patient’s heart rate and mean arterial blood pressures (MAP) were recorded at four timepoints: pre-induction (T0), 1 hour after ventilation (T1), 2 hours after ventilation (T2), and at the end of surgery (T3). Radial arterial blood samples were also collected at the four-time points and were analyzed using Roche Cobas B123 POC blood gas analyzer (Roche Group, Basel, Switzerland). Venous blood samples were collected from the peripheral venous line at T0-T3 time points and 24 hours after surgery (T4). These samples were centrifuged at 3000 rpm for 10 min at 4°C, and the supernatant was stored at –80°C for further test. The concentrations of IL-6, IL-10, and CC-16 in plasma were measured using sandwich enzyme-linked immunosorbent assay (ELISA) with commercially available kits (Wuhan Cloud-Clone Co., Ltd, Wuhan, China) according to the manufacturer’s instruction. Respiratory parameters (T1-T3), intraoperative medication, i.v. fluid, transfusion, urine output, and surgery time were also recorded. PACU nurses documented the level of pain (using VAS score), the total doses of analgesic drugs. The QoR-40 score at 24 hours postoperatively was assessed by follow-up staff. The staff also recorded postoperative pain level, opioid consumption, gastrointestinal recovery (include first defecation or bowel movements, time to first flatus, ileus (postoperative ileus were identified by the presence of two or more clinical indicators of gastrointestinal dysfunction, at least one for each of the two following criteria: (1) presence of vomiting or abdominal distension and (2) absence of flatus/stool or not tolerating oral diet.)), length of hospital stay. Possible lidocaine-related adverse events were noted. PPCs in the postoperative period were collected until day 7 or hospital discharge, whichever came first.
Sample Size
We originally planned to use CC-16 as the primary outcome measure. According to previous studies, postoperative plasma levels of CC–16 in patients undergoing abdominal surgery was 17.8 ng mL−1, the standard deviation was 9.4.5,20 Assuming that intravenous infusion of lidocaine can reduce CC-16 by 30%, 53 patients in each group can provide 80% power with a significance level of 0.05. We planned to recruit 62 patients in each group to compensate for 15% dropouts. Since we changed the primary outcome measure, we recalculated the sample size based on the new primary outcome measure. A new sample size calculation was based on a previous study that the incidence of PPCs for patients with intermediate to high risk of PPCs is about 48%.21 Therefore, assuming an expected clinical intergroup difference of 20% as the significance threshold and anticipating a 10% dropout rate, the estimated sample size of 200 patients provided 80% power with a significance level of 5% to detect a 20% reduction in PPCs incidence between groups. PASS 11.0 (NCSS, LLC, Kaysville, USA) was used for sample size calculation. All of the final statistical analysis was based on the new sample size.
Statistical Analysis
The measurement data used the Shapiro–Wilk test to determine the normality of the data distribution, and the Levene method was used to test the homogeneity of variance. Normally distributed continuous variables were presented as the mean ± standard deviation (mean ± SD) and were compared using Student’s t-test. Nonnormally distributed continuous data were reported as median (interquartile range, IQR) and compared using the Mann–Whitney U-test. Median differences and their 95% CIs were estimated using the Hodges–Lehmann estimator. Categorical data were reported as frequency (%) and were analyzed using the chi-squared test or Fisher’s exact test. We used Kaplan-Meier curves and hazard ratios (HRs) for time to first diagnosis of PPC. Serial parameters reflecting lung function, hemodynamic data, VAS score were analyzed using two-way repeated-measures ANOVA. The group-by-time interaction term was tested first. If significant, between-group differences at each time point were tested at α=0.05. If not significant, the treatment main effect was tested next. Otherwise, Bonferroni correction was applied at each time point. The criterion for rejection of the null hypothesis was a two-tailed P<0.05. All statistical analyses were performed using SPSS software (version 24.0; SPSS Inc., IBM, Chicago, IL, USA).
Results
Subject Characteristics
Figure 1 shows the flowchart of this study. In total, 200 subjects were enrolled and 100 were randomized to each study group from April 2019 to January 2020. Three subjects in group lidocaine and two subjects in group control were excluded because of the operation time<2 hours and voluntary withdrawal. As a result, 97 subjects in group lidocaine and 98 subjects in group control were analyzed. There were no study protocol violations. Complete data were available for the primary and secondary endpoints. The groups were comparable concerning age, gender, height, weight, BMI, ASA physical status, current smoking, ARISCAT score, the form of surgery, site of surgery, i.v. fluid, transfusion, urine output, surgery time, anesthesia time, and nasogastric tubes (Table 1).
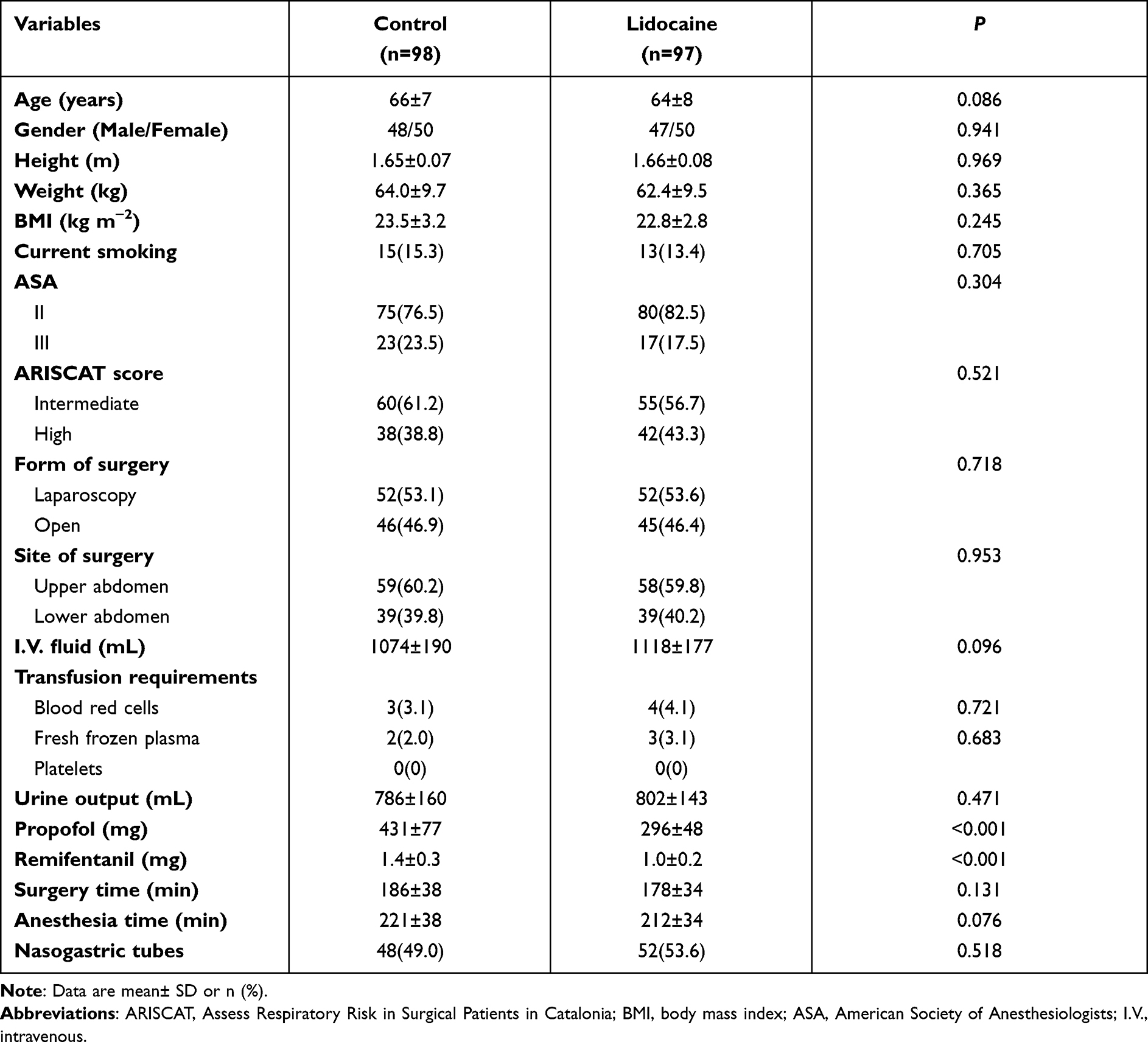 |
Table 1 Patients’ Characteristics, Type of Surgery and Intraoperative Variables |
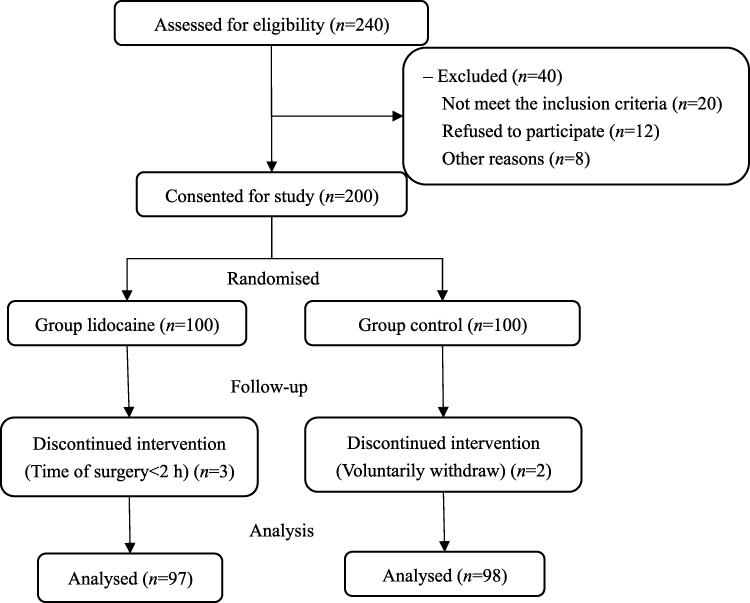 |
Figure 1 CONSORT flowchart diagram. |
Primary Outcome: Postoperative Pulmonary Complications
As presented in Table 2, there were 35.9% (70/195) patients who sustained PPCs. Twenty-five subjects in the group lidocaine (25/97; 25.8%) and forty-five subjects in the group control (45/98; 45.9%) were evaluated as developing PPCs within the first 7 postoperative days or until hospital discharge (relative risk:0.56, 95% CI: 0.38 to 0.84; absolute risk reduction: −20.1%, P=0.003). Considering single PPCs episode, the most common PPC in both groups was atelectasis. The atelectasis incidence was 11.3% (11/97) in group lidocaine, much lower than that in group control 29.6% (29/98) (relative risk: 0.38, 95% CI: 0.20 to 0.72; absolute risk reduction: −18.3%, P=0.002). However, the incidences of any other PPCs episodes were similar between the two groups. Kaplan-Meier cumulative survival rates were 71.2% in group lidocaine versus 51.0% in group control at 7 postoperative days (Hazard ratio: 0.40, 95% CI: 0.30 to 0.77, P=0.002, Figure 2).
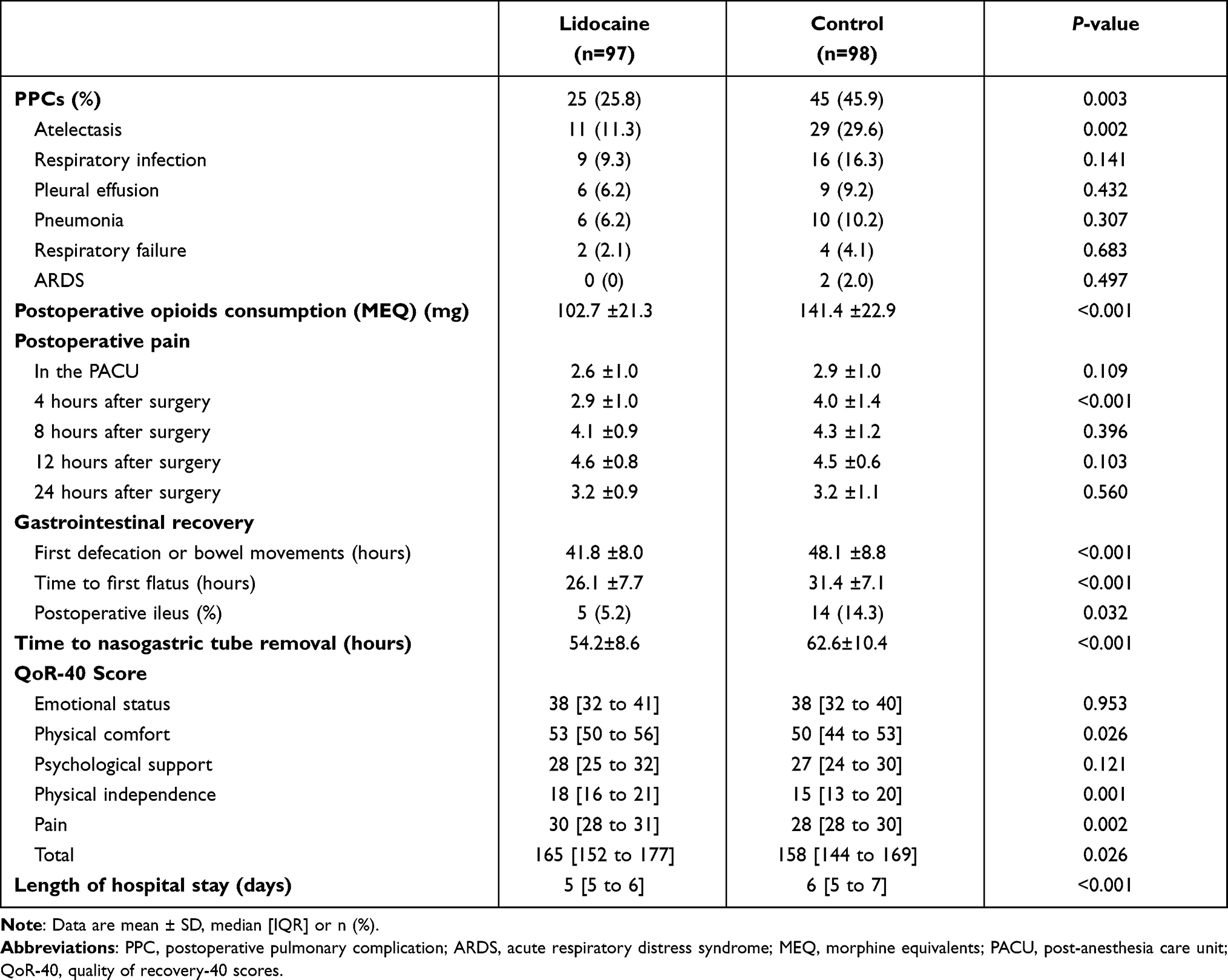 |
Table 2 Primary and Secondary Outcomes |
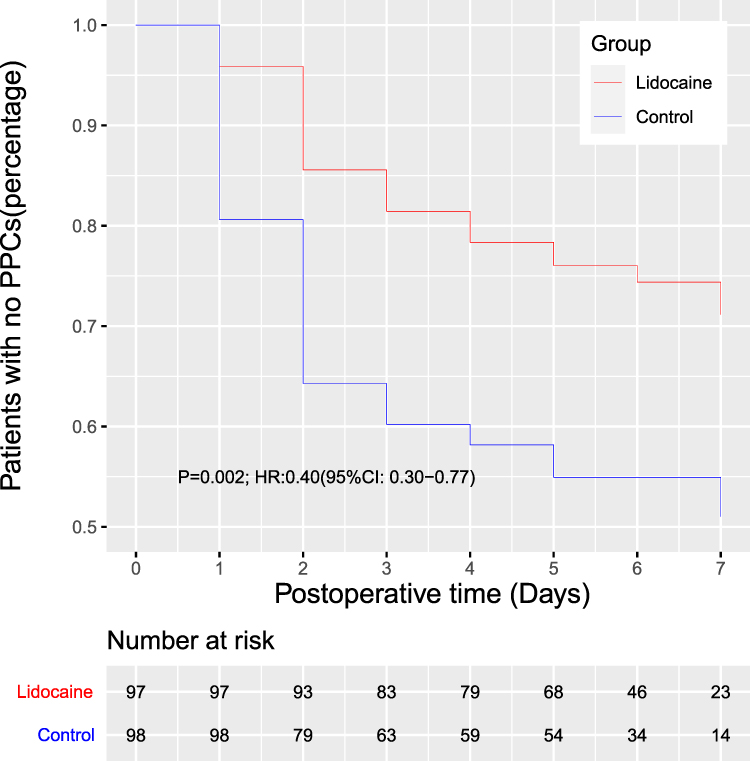 |
Figure 2 Patients with no PPCs at 7 postoperative days. No PPCs was defined as no PPCs occurred within 7 postoperative days or before discharge, whichever came sooner. |
Secondary Endpoints
Plasma Concentration of CC-16, IL-6, and IL-10 at T0-T4
Surgery and anesthesia can result in inflammatory responses. As shown in Figure 3, after anesthesia induction, the concentrations of IL-6, IL-10, and CC-16 were increased in both groups and reached peak levels at the end of surgery. However, lidocaine administration effectively inhibited the increase of IL-6 concentrations (T2, 31.8 (27.0 to 34.4) vs 34.9 (30.3 to 39.5) pg mL−1; T3, 95.4 (58.2 to 242.1) vs 122.4 (68.8 to 265.3) pg mL−1 respectively, Figure 3A). In addition, the concentration of IL-6 decreased more rapidly in group lidocaine compared with group control (T4, 78.4 (48.1 to 218.2) vs 118.3 (65.0 to 253.6) pg mL−1, Figure 3A). The concentration of IL-10 in each group shows no obvious differences at any time points (Figure 3B). Group lidocaine had a lower CC-16 concentration than group control at T4 (15.2 (11.3 to 20.4) vs 19.5 (13.7 to 23.9) ng mL−1, Figure 3C).
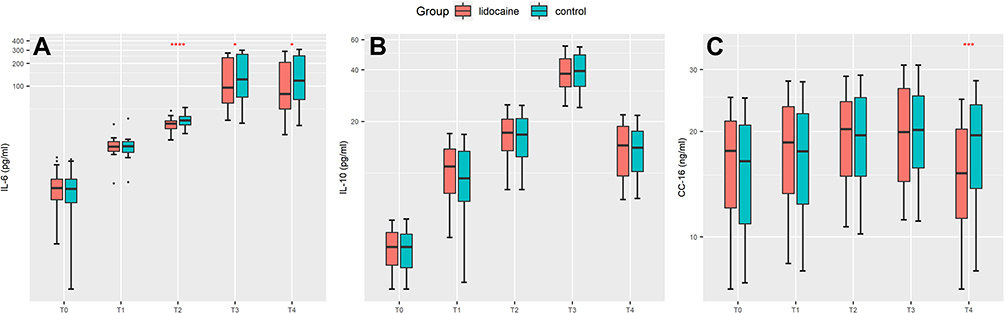 |
Figure 3 Concentrations of inflammatory factors at different time points. (A) Concentrations of IL-6; (B) concentrations of IL-10; (C) concentrations of CC-16. *P<0.05; ***P<0.02; ****P<0.001. IL-6, interleukin-6; IL-10, interleukin-10; CC-16, Clara cell protein-16; T0, pre-induction of anesthesia; T1, 1 hour after ventilation; T2, 2 hours after ventilation; T3, the end of surgery; T4, 24 hours after surgery. All of the y-axis were log2 transformed. |
Postoperative Total Opioid Consumption (MEQ)
The total postoperative opioid consumption in group lidocaine was less than that in group control (102.7±21.3 vs 141.4 ±22.9 mg, difference: −38.7, 95% CI: −44.9 to −32.4; P<0.001) (Table 2).
Postoperative Pain Level
The comparison of VSA scores between group lidocaine and group control at various time points only showed a difference at 4 hours postoperatively (2.9 ±1.0 vs 4.0 ±1.4, difference: −1.1, 95% CI: −1.5 to −0.8; P<0.001) (Table 2).
Gastrointestinal Recovery
The time of first defecation or bowel movements in group lidocaine was 6.3 hours (95% CI: 3.9 to 8.7) earlier than that in group control (P<0.001). And the time of first flatus was also shorter in group lidocaine (26.1 ±7.7 vs 31.4 ±7.1 hours, difference: −5.0, 95% CI: −7.3 to −3.2; P<0.001). In addition, the incidence of postoperative ileus was lower in group lidocaine, compared with group control (5.2% vs 14.3%, relative risk: 0.36, 95% CI: 0.14 to 0.96, absolute risk reduction: −9.1%, P=0.032). Consistent with these results, removal time of nasogastric tube was also earlier in the lidocaine group (54.2±8.6 vs 62.6±10.4 hours, difference: −8.4, 95% CI: −12.2 to −4.6; P<0.001) (Table 2).
Quality of Recovery
Compared with group control, the total QoR-40 score in group lidocaine was higher at 24 hours postoperatively (165 (152 to 177) vs 158 (144 to 169), difference:7, 95% CI:4 to 13; P=0.026). To be specific, the scores of physical comfort, physical independence, and pain domains in group lidocaine were higher than those in group control (53 (50 to 56) vs 50 (44 to 53), difference:3, 95% CI:2 to 5, P=0.026; 18 (16 to 21) vs 15 (13 to 20), difference:3, 95% CI:2 to 4, P=0.001; 30 (28 to 31) vs 28 (28 to 30), difference:2, 95% CI:1 to 4, P=0.002, respectively). However, there were no obvious differences in emotional status and psychological support domains (Table 2).
Length of Hospital Stay
The median length of hospital stay in group lidocaine was shorter than that in group control (5 (5 to 6) vs 6 (5 to 7), difference: −1, 95% CI: −1 to 0, P<0.001) (Table 2).
Parameters Reflecting Pulmonary Function and Mechanics and Hemodynamics
There was interaction of group and time on driving pressure (P=0.032). The simple effects of the group were analyzed. The driving pressure between the two groups was similar at each time point (Table 3). The interaction of group and time was not statistically significant on Cdyn (P=0.831), RI (P=0.130), PO2/FiO2 (P=0.422), heart rate (P=0.980), and MAP (P=0.485). The main effects of the group were analyzed. Cdyn, RI, and PO2/FiO2 were similar between the two groups. Compared with group control, the heart rate and MAP were not affected by infusion lidocaine (Table 3).
 |
Table 3 Secondary Outcomes: Intraoperative Variables Reflecting Lung Function and Hemodynamics |
Adverse Events
There were no significant lidocaine-related adverse events during the entire trial.
Discussion
In this prospective, double-blind, randomized controlled trial, we found that intravenous infusion of lidocaine could significantly reduce the incidence of PPCs within 7 days postoperatively in patients undergoing major abdomen surgical procedures, shortened lengths of hospital stays, and improved patient prognosis. Possible underlying mechanisms maybe include inhibiting inflammation, reducing opioid consumption, and promoting gastrointestinal motility. In the present study, the total incidence of PPCs seems higher (35.9%) than those in previous studies.22,23 It may be because the patients we included were at intermediate to high risk of PPCs (ARISCAT ≥ 26).
Risk factors for PPCs development are numerous, including systemic inflammatory response after surgery, side effects of opioids, postoperative inadequate analgesia, and changes of respiratory mechanics.4 All these entities are ameliorated by the administration of i.v. lidocaine.24
Intravenous administration of lidocaine showed analgesic effect, and reduced postoperative pain, especially in the early postoperative period.25,26 In our present study, i.v. lidocaine effectively reduced postoperative pain, although the VAS scores were significantly lower only at 4 hours postoperatively. This may be because the PCA we used had background infusion. The analgesia effect of i.v. lidocaine resulted in reducing opioid consumption. Previous studies showed that intraoperative i.v. lidocaine reduced morphine consumption in patients undergoing open radical prostatectomy and open gastrectomy.26,27 Similar results were found in the present study. The total opioid consumption was much lower in group lidocaine than that in group control, so the side effects induced by opioids, such as respiratory depression, were reduced.
In addition to analgesia, the anti-inflammatory effects of lidocaine have been extensively studied.8–10 The systemic inflammatory response is an important factor in PPCs. Lidocaine was reported to activate protein kinase C to reduce endotoxin-induced leukocyte adhesion and granulocyte-mediated phagocytosis through G-protein coupled signal pathways.28 The anti-inflammatory effect of lidocaine was also reflected in blocking neutrophil activation and inhibiting inflammatory cytokines and proteolytic enzyme release.11,29 In the present study, i.v. lidocaine significantly prevented IL-6 release during operation. Besides, the level of CC-16 in plasma was significantly lower in group lidocaine than in group control at 24 hours postoperatively. CC-16 protein, a homodimer protein synthesized and secreted by lung epithelial cells, is a specific biomarker of the damage of Clara cell and alveolar-capillary permeability. It can reflect early alveolar epithelial permeability changes induced by subclinical lung injury30,31 by leaking from damaged lung epithelial barrier to blood.32 These results suggested that i.v. lidocaine presents lung protective effects by inhibiting inflammation and protecting alveolar epithelial and alveolar-capillary barriers.
Interestingly, although the previous study33 found that intravenous lidocaine could improve the respiratory mechanics of patients undergoing thoracoscopic surgery during operation, however, in our present study, it was not improved by i.v. lidocaine. This may be due to the different types of surgery (abdominal surgery vs thoracic surgery). Thoracoscopic surgery maybe have a greater impact on respiratory mechanics than laparoscopic surgery. In addition, we stratified patients according to the type of surgery and adopted standard lung protection ventilation strategies. Although the anti-inflammatory effect of lidocaine had benefits on lung function, it was not enough to affect the intraoperative respiratory mechanics. So, the improvement of respiratory mechanics was not obvious.
PPC is a composite outcome measure, the rate of atelectasis in group lidocaine was significantly lower than that in group control. This is mainly because of the benefits of i.v. lidocaine (pain relief, reduced opioid consumption, anti-inflammatory effects) could promote deep breathing and coughing, which is of great significance for reducing postoperative atelectasis.4 In addition, a previous study showed that patients with a nasogastric tube had a higher risk of atelectasis.34 The rapid recovery of gastrointestinal function in group lidocaine allowed the nasogastric tube to be removed earlier, which may be another important reason for the decrease in the incidence of postoperative atelectasis. However, the incidence of other PPCs (Respiratory infection, Pleural effusion, Pneumonia, Respiratory failure, ARDS) decreased in group lidocaine, but the difference was not statistically significant. This may be due to our insufficient sample size. Because sample size calculation was based on the primary outcome measure (the incidence of PPCs). Since PPCs are a composite indicator, the incidence of single PPC is lower than that of PPCs, lower incidence means less difference between the two groups, so a larger sample size may be required to meet the same power and level of the test.
In this study, we observed that i.v. lidocaine had a promoting effect on gastrointestinal recovery. Previous study and meta-analyses showed that i.v. lidocaine could reduce the time to first bowel movement and the incidence of ileus.35,36 The main reasons may include reducing opioid consumption and inhibiting systemic inflammation. Inflammation plays a crucial role in sustaining postoperative ileus,37 lidocaine may mediate its beneficial effects on promoting gastrointestinal recovery by anti-inflammatory. The rapid recovery of gastrointestinal function allowed the nasogastric tube, which is closely related to atelectasis, to be removed earlier, and thus promote patients’ early recovery.
Taking together, i.v. lidocaine reduced the incidence of PPCs, promoted patients’ recovery, and shortened the length of hospital stay by inhibiting systemic inflammation, relief pain, reducing opioid consumption, and promoting gastrointestinal recovery.
There are some limitations in our research. First, we did not measure the blood concentration of lidocaine. This is because the dose we used is similar to others. Previous studies38–40 found that after a bolus of 1.5 mg kg−1 with 1.0–2.0 mg kg−1 h−1 continuous infusion of lidocaine, the average plasma concentration of lidocaine was 1.60–2.05 μg mL−1, which is far lower than the concentration of 5.0 μg mL−1 that produces toxic reactions41 and is therefore considered to be safe. Second, we did not continue i.v. lidocaine for a longer time after surgery, this is mainly because of concerns about the safety of patients after returning to the ward. Third, we only enrolled patients at an intermediate/high risk for PPCs undergoing major abdominal surgery, these findings cannot be generalized to more patients. Finally, long-term effects of i.v. lidocaine were not observed. Hence, further multi-center, large-sample randomized trials are needed to investigate the long-term impact of lidocaine infusion on surgery patients.
Conclusions
In summary, our results suggest that perioperative lidocaine administration can reduce the incidence of PPCs in patients with intermediate/high risk of PPCs under major abdominal surgery. In addition, i.v. lidocaine can also relieve early pain level (postoperative 4 hours), promote gastrointestinal recovery, improve the quality of recovery and shorten the length of hospital stay. These findings may provide a new strategy of lung protection for patients with intermediate/high risk of PPCs during the perioperative period.
Data Sharing Statement
The authors will share participant data, such as blood pressure, heart rate, and pain scores and so on. No other study-related documents will be available. Emails could be sent to the address below to obtain the shared data: [email protected]. The data will be accessible from the publication date.
Acknowledgments
Financial support and sponsorship: This work was supported by grants from the Qing Lan Project of Jiangsu Province; the Nature Science Foundation of Jiangsu Province (BK20161175); the “Six One” Project of Jiangsu Province (LGY2016039).
Disclosure
The authors report no conflicts of interest in this work.
References
1. de la Gala F, Pineiro P, Reyes A, et al. Postoperative pulmonary complications, pulmonary and systemic inflammatory responses after lung resection surgery with prolonged one-lung ventilation. Randomized controlled trial comparing intravenous and inhalational anaesthesia. Br J Anaesth. 2017;119(4):655–663. doi:10.1093/bja/aex230
2. Futier E, Constantin JM, Paugam-Burtz C, et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. N Engl J Med. 2013;369(5):428–437. doi:10.1056/NEJMoa1301082
3. O’Gara B, Talmor D. Perioperative lung protective ventilation. BMJ. 2018;362:k3030. doi:10.1136/bmj.k3030
4. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
5. Serpa Neto A, Campos PP, Hemmes SN, et al. Kinetics of plasma biomarkers of inflammation and lung injury in surgical patients with or without postoperative pulmonary complications. Eur J Anaesthesiol. 2017;34(4):229–238. doi:10.1097/EJA.0000000000000614
6. Shea RA, Brooks JA, Dayhoff NE, Keck J. Pain intensity and postoperative pulmonary complications among the elderly after abdominal surgery. Heart Lung. 2002;31(6):440–449. doi:10.1067/mhl.2002.129449
7. Warner DO, Weiskopf R. Preventing postoperative pulmonary complications: the role of the anesthesiologist. Anesthesiology. 2000;92(5):1467–1472. doi:10.1097/00000542-200005000-00037
8. Hollmann MW, Durieux ME. Local anesthetics and the inflammatory response: a new therapeutic indication? Anesthesiology. 2000;93(3):858–875. doi:10.1097/00000542-200009000-00038
9. Fischer LG, Bremer M, Coleman EJ, et al. Local anesthetics attenuate lysophosphatidic acid-induced priming in human neutrophils. Anesth Analg. 2001;92(4):1041–1047. doi:10.1097/00000539-200104000-00044
10. Kuo CP, Jao SW, Chen KM, et al. Comparison of the effects of thoracic epidural analgesia and i.v. infusion with lidocaine on cytokine response, postoperative pain and bowel function in patients undergoing colonic surgery. Br J Anaesth. 2006;97(5):640–646. doi:10.1093/bja/ael217
11. Chen LJ, Ding YB, Ma PL, et al. The protective effect of lidocaine on lipopolysaccharide-induced acute lung injury in rats through NF-kappaB and p38 MAPK signaling pathway and excessive inflammatory responses. Eur Rev Med Pharmacol Sci. 2018;22(7):2099–2108. doi:10.26355/eurrev_201804_14743
12. Takao Y, Mikawa K, Nishina K, Maekawa N, Obara H. Lidocaine attenuates hyperoxic lung injury in rabbits. Acta Anaesthesiol Scand. 1996;40(3):318–325. doi:10.1111/j.1399-6576.1996.tb04439.x
13. Rancan L, Simon C, Marchal-Duval E, et al. Lidocaine administration controls MicroRNAs alterations observed after lung ischemia-reperfusion injury. Anesth Analg. 2016;123(6):1437–1447. doi:10.1213/ANE.0000000000001633
14. Sridhar P, Sistla SC, Ali SM, Karthikeyan VS, Badhe AS, Ananthanarayanan PH. Effect of intravenous lignocaine on perioperative stress response and post-surgical ileus in elective open abdominal surgeries: a double-blind randomized controlled trial. ANZ J Surg. 2015;85(6):425–429. doi:10.1111/ans.12783
15. Dunn LK, Durieux ME. Perioperative Use of Intravenous Lidocaine. Anesthesiology. 2017;126(4):729–737. doi:10.1097/ALN.0000000000001527
16. Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338–1350. doi:10.1097/ALN.0b013e3181fc6e0a
17. Celli BR, Anderson JA, Brook R, et al. Serum biomarkers and outcomes in patients with moderate COPD: a substudy of the randomised SUMMIT trial. BMJ Open Respir Res. 2019;6(1):e000431. doi:10.1136/bmjresp-2019-000431
18. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
19. Force ADT, Ranieri VM, Rubenfeld GD, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. doi:10.1001/jama.2012.5669
20. Wu CY, Cheng YJ, Hung MH, Lin IJ, Sun WZ, Chan KC. Association between early acute respiratory distress syndrome after living-donor liver transplantation and perioperative serum biomarkers: the role of club cell protein 16. Biomed Res Int. 2019;2019:8958069. doi:10.1155/2019/8958069
21. Ferrando C, Soro M, Unzueta C, et al. Individualised perioperative open-lung approach versus standard protective ventilation in abdominal surgery (iPROVE): a randomised controlled trial. Lancet Respir Med. 2018;6(3):193–203. doi:10.1016/S2213-2600(18)30024-9
22. Boden I, Skinner EH, Browning L, et al. Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: pragmatic, double blinded, multicentre randomised controlled trial. BMJ. 2018;360:j5916. doi:10.1136/bmj.j5916
23. Fernandez-Bustamante A, Frendl G, Sprung J, et al. Postoperative pulmonary complications, early mortality, and hospital stay following noncardiothoracic surgery: a multicenter study by the perioperative research network investigators. JAMA Surg. 2017;152(2):157–166. doi:10.1001/jamasurg.2016.4065
24. Koppert W, Weigand M, Neumann F, et al. Perioperative intravenous lidocaine has preventive effects on postoperative pain and morphine consumption after major abdominal surgery. Anesth Analg. 2004;98(4):1050–1055. doi:10.1213/01.ANE.0000104582.71710.EE
25. Staikou C, Avramidou A, Ayiomamitis GD, Vrakas S, Argyra E. Effects of intravenous versus epidural lidocaine infusion on pain intensity and bowel function after major large bowel surgery: a double-blind randomized controlled trial. J Gastrointest Surg. 2014;18(12):2155–2162. doi:10.1007/s11605-014-2659-1
26. Weinberg L, Rachbuch C, Ting S, et al. A randomised controlled trial of peri-operative lidocaine infusions for open radical prostatectomy. Anaesthesia. 2016;71(4):405–410. doi:10.1111/anae.13368
27. Kang JG, Kim MH, Kim EH, Lee SH. Intraoperative intravenous lidocaine reduces hospital length of stay following open gastrectomy for stomach cancer in men. J Clin Anesth. 2012;24(6):465–470. doi:10.1016/j.jclinane.2012.02.006
28. Lauretti GR. Mechanisms of analgesia of intravenous lidocaine. Rev Bras Anestesiol. 2008;58(3):280–286. doi:10.1590/S0034-70942008000300011
29. Sinclair R, Eriksson AS, Gretzer C, Cassuto J, Thomsen P. Inhibitory effects of amide local anaesthetics on stimulus-induced human leukocyte metabolic activation, LTB4 release and IL-1 secretion in vitro. Acta Anaesthesiol Scand. 1993;37(2):159–165. doi:10.1111/j.1399-6576.1993.tb03693.x
30. Celli BR, Owen CA. The club cell and its protein, CC16: time to shine. Lancet Respir Med. 2013;1(10):757–759. doi:10.1016/S2213-2600(13)70247-9
31. Kropski JA, Fremont RD, Calfee CS, Ware LB. Clara cell protein (CC16), a marker of lung epithelial injury, is decreased in plasma and pulmonary edema fluid from patients with acute lung injury. Chest. 2009;135(6):1440–1447. doi:10.1378/chest.08-2465
32. Broeckaert F, Bernard A. Clara cell secretory protein (CC16): characteristics and perspectives as lung peripheral biomarker. Clin Exp Allergy. 2000;30(4):469–475. doi:10.1046/j.1365-2222.2000.00760.x
33. Wang L, Sun J, Zhang X, Wang G. The effect of lidocaine on postoperative quality of recovery and lung protection of patients undergoing thoracoscopic radical resection of lung cancer. Drug Des Devel Ther. 2021;15:1485–1493. doi:10.2147/DDDT.S297642
34. Li C, Yang WH, Zhou J, et al. Risk factors for predicting postoperative complications after open infrarenal abdominal aortic aneurysm repair: results from a single vascular center in China. J Clin Anesth. 2013;25(5):371–378. doi:10.1016/j.jclinane.2013.01.013
35. Cooke C, Kennedy ED, Foo I, et al. Meta-analysis of the effect of perioperative intravenous lidocaine on return of gastrointestinal function after colorectal surgery. Tech Coloproctol. 2019;23(1):15–24. doi:10.1007/s10151-019-1927-1
36. Rollins KE, Javanmard-Emamghissi H, Scott MJ, Lobo DN. The impact of peri-operative intravenous lidocaine on postoperative outcome after elective colorectal surgery: a meta-analysis of randomised controlled trials. Eur J Anaesthesiol. 2020;37(8):659–670. doi:10.1097/EJA.0000000000001165
37. Seifarth C, Hering NA, Arndt M, et al. Increased proinflammatory cytokines in mesenteric fat in major surgery and Crohn’s disease. Surgery. 2021;169(6):1328–1332. doi:10.1016/j.surg.2020.11.039
38. Ho MLJ, Kerr SJ, Stevens J. Intravenous lidocaine infusions for 48 hours in open colorectal surgery: a prospective, randomized, double-blinded, placebo-controlled trial. Korean J Anesthesiol. 2018;71(1):57–65. doi:10.4097/kjae.2018.71.1.57
39. El-Tahan MR, Warda OM, Diab DG, Ramzy EA, Matter MK. A randomized study of the effects of perioperative i.v. lidocaine on hemodynamic and hormonal responses for cesarean section. J Anesth. 2009;23(2):215–221. doi:10.1007/s00540-009-0738-3
40. Sahmeddini MA, Khosravi MB, Farbood A. Comparison of perioperative systemic lidocaine or systemic ketamine in acute pain management of patients with opioid use disorder after orthopedic surgery. J Addict Med. 2019;13(3):220–226. doi:10.1097/ADM.0000000000000483
41. Beaussier M, Delbos A, Maurice-Szamburski A, Ecoffey C, Mercadal L. Perioperative use of intravenous lidocaine. Drugs. 2018;78(12):1229–1246. doi:10.1007/s40265-018-0955-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.