Back to Journals » Journal of Asthma and Allergy » Volume 16
Lung Function and Asthma Clinical Control in N-ERD Patients, Three-Year Follow-Up in the Context of Real-World Evidence
Authors Pavón-Romero GF ![]() , Falfán-Valencia R
, Falfán-Valencia R ![]() , Gutiérrez-Quiroz KV
, Gutiérrez-Quiroz KV ![]() , De La O-Espinoza EA
, De La O-Espinoza EA ![]() , Serrano-Pérez NH, Ramírez-Jiménez F
, Serrano-Pérez NH, Ramírez-Jiménez F ![]() , Teran LM
, Teran LM
Received 11 May 2023
Accepted for publication 21 August 2023
Published 6 September 2023 Volume 2023:16 Pages 937—950
DOI https://doi.org/10.2147/JAA.S418802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Gandhi Fernando Pavón-Romero,1 Ramcés Falfán-Valencia,2 Katia Vanessa Gutiérrez-Quiroz,1 Estivaliz Arizel De La O-Espinoza,1 Nancy Haydée Serrano-Pérez,1 Fernando Ramírez-Jiménez,1 Luis M Teran1
1Department of Immunogenetics and Allergy, Instituto Nacional de Enfermedades Respiratorias, Mexico City, Mexico; 2Laboratory of Human Leukocyte Antigen, Instituto Nacional de Enfermedades Respiratorias, Mexico City, Mexico
Correspondence: Luis M Teran, Department of Immunogenetics and Allergy, Instituto Nacional de Enfermedades Respiratorias, Ismael Cosío Villegas, Tlalpan, Mexico City, 14080, Mexico, Tel +52 5557481700 exr. 5162, Email [email protected]
Purpose: To describe the lung function and clinical control of asthma in patients with N-ERD during three years of medical follow-up using GINA guidelines.
Methods: We evaluated 75 N-ERD and 68 asthma patients (AG). Clinical control, lung function, and asthma treatment were evaluated according to GINA-2014. We compared all variables at baseline and one, two, and three years after treatment.
Results: At baseline, the N-ERD group had better basal lung function (LF) than the AG group (p< 0.01), and the AG group used higher doses of inhaled corticosteroids than the N-ERD group (52.4% vs 30.5%, p=0.01) and short-term oral corticosteroid (OCS) use (52.4% vs 30.5%, p< 0.01). Instead, N-ERD patients needed more use of leukotriene receptor antagonists (LTRA) (29.3% vs 5.9%, p< 0.01). This group had better clinical control than the AG group (62.1% vs 34.1%, p< 0.01). During the medical follow-up, the LF of the N-ERD group remained at normal values; however, these parameters improved in AG from one year (p< 0.01). Likewise, there was a diminished use of high doses of ICS (52.4% vs 33%, p< 0.05) and short-term OCS (67.6% vs 20.6%, p< 0.01) in asthma patients. However, N-ERD patients still needed more use of LTRAs (p< 0.02) during the study. In this context, one-third of N-ERD patients had to use a combination of two drugs to maintain this control. From the second year on, clinical control of asthma was similar in both groups (p> 0.05).
Conclusion: According to GINA guidelines, only one-third of patients with N-ERD can gradually achieve adequate lung function and good asthma control with a high ICS dosage. Only a very small portion of patients will require the continued use of a second medication as an LTRA to keep their asthma under control.
Keywords: N-ERD, asthma, severe asthma, corticosteroids, GINA guidelines, asthma clinical control
Introduction
Nonsteroidal anti-inflammatory drug-exacerbated respiratory disease (N-ERD) is an entity characterized by hypersensitivity to nonsteroidal anti-inflammatory drugs (NSAIDs), nasal polyps, and asthma.1 It is considered an asthma phenotype with a very low frequency.2 The physiopathology is not yet clear,3 and the main hypothesis accepted is the blockage of the cyclooxygenase pathway by NSAIDs, increasing the synthesis of leukotrienes with subsequent induction of bronchospasm and nasal congestion after its intake.1,4
Inhaled corticosteroids (ICS) and leukotriene receptor antagonists (LTRA) are considered sufficient for asthma control in N-ERD patients, according to expert medical groups.5 Even this recommendation could be considered the “first-line” therapeutic before the use of aspirin desensitization or monoclonal antibodies (anti-IgE or anti-IL-5).6,7 Most studies that have evaluated lung function and clinical control have used a transversal design as part of the phenotyping of asthma8 or for some genetic-molecular studies.9,10 In the last years, few studies have evaluated these objectives from therapeutic (anti-leukotriene therapy, nebulized steroids, and aspirin desensitization) and surgical maneuvers on sinus outcomes in a second time with variable results.11–14 However, the use of standard therapy for asthma control in N-ERD long-time has not been sufficiently described, has only been described that the combination of ICS plus long-acting β2-agonists (LABA, ICS/LABA) and antileukotrienes diminishes bronchial symptoms during aspirin oral challenge in N-ERD patients.15
N-ERD has been considered a severe asthma phenotype for many years,16 requiring the use of multiple medicines or large doses for asthma control. In the present study, we described the use of first-line therapy in a Mexican cohort of N-ERD and asthma patients according to GINA-2014 guidelines17 in a real context life for three years (See Figure 1).
 |
Figure 1 GINA-2014 guidelines. Abbreviations: ICS, inhaled corticosteroids; OCS, oral corticosteroids; LTRA, leukotriene receptor antagonists; LABA, long-actingbeta2-agonist; SABA, short-actingbeta2-agonist; IgE, immunoglobulin E. |
Methods
Description of the Study
The present study is a descriptive analysis of the clinical-genetic cohort of patients with N-ERD in which information was obtained based on the clinical follow-up of patients with N-ERD and asthma attended in the Department of Immunogenetics and Allergy of the Instituto Nacional de Enfermedades Respiratorias (INER) “Ismael Cosío Villegas”. We evaluated 14 variables over three years in four time periods, which were put into a case report format (CRF, see Supplementary Figure 1). We enrolled patients during 2014–2015 (when patients started their medical follow-up) and subsequently, they continued their medical follow-up at 12 months-time 1 (t1), 2 years-time 2 (t2), and 3 years-time 3 (t3) (See Figure 2).
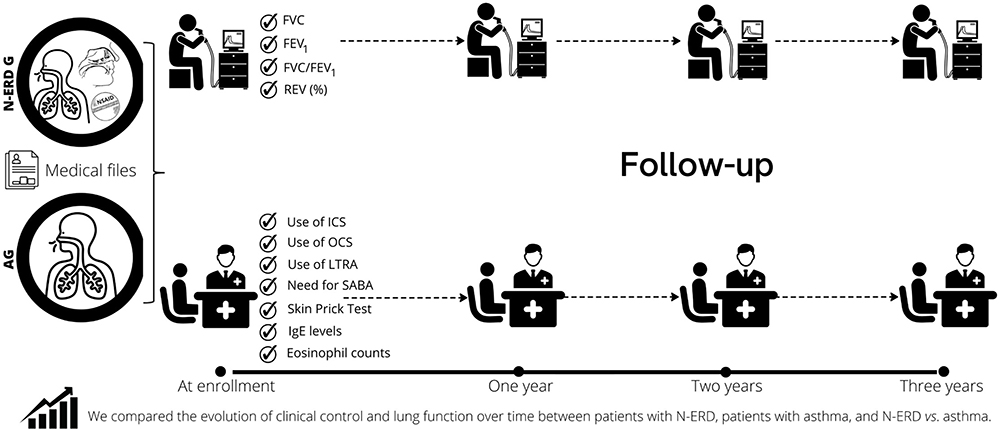 |
Figure 2 Design of the study. Abbreviations: N-ERD G, nonsteroidal anti-inflammatory drugs-exacerbated respiratory disease group; AG, asthma group; NSAID, non-steroidal anti-inflammatory drugs; FVC, forced vital capacity; FEV1, forced expiratory volume in the first second; REV, reversibility; OCS, oral corticosteroids; LTRA, leukotriene receptor antagonists; SABA, short-actingbeta2-agonist; IgE, immunoglobulin E. |
Patients
Only the information of the patients who completed three years of follow-up were selected. A patient with N-ERD was defined as a patient who met three basic conditions inherent to this disease (asthma, nasosinusal polyposis, and hypersensitivity to aspirin or NSAIDs). Asthma condition was established with the presence of suggestive symptoms: cough, dyspnea, wheezing, the sensation of chest tightness, and positive reversibility test >12% and 200mL concerning baseline Forced Expiratory Volume in the First Second (FEV1). The nasosinusal polyposis was established with the presence of nasosinusal polyposis or a history of polypectomy or nasalization. And hypersensitivity to ASA or NSAIDs was established with the nasal challenge with lysine-aspirin (reduction of baseline total nasal flow >40% for baseline after the nasal administration of lysine-aspirin) or the history of bronchospasm 30 minutes after the ingestion of ASA or NSAIDs and that had warranted hospitalization in the emergency room of the INER. The asthma patients should only present the criteria corresponding to asthma and have not had any related to N-ERD.
Clinical Control of Asthma
The clinical control of asthma in patients with N-ERD and asthma was classified according to the GINA 2014 guidelines, considering the presence of asthma symptoms in the last four weeks, nocturnal awakening, activity limitation, and the use of rescue medication and their frequency by numbers of days of the week classifying it as controlled (1 day), partially controlled (2 days) and uncontrolled (>2 days) (See Supplementary Table 1). Subsequently, we joined asthma partially controlled and uncontrolled as non-control and well control as good clinical control.
Lung Function
Lung function was performed according to the guidelines established by the American Thoracic Society, using a Jaeger Care fusion spirometer (Leibnizstrasse, Germany), performing a minimum of three maneuvers until a quality grade A was achieved, selecting the best result in the FVC (Forced Vital Capacity) and FEV1 parameters concerning those predicted in the Mexican population proposed by Pérez-Padilla.18
Treatment
The treatment was chosen according to the GINA 2014 guidelines; based on the dose of inhaled steroids (low, medium, and high dose; See Supplementary Table 2) as well as the need for the use of leukotriene receptor antagonists. Similarly, the use of continuous oral steroids for six months based on prednisone or short-term use of systemic steroids was reported.
Statics
The statistical analysis considered the strategy of comparing the group of interest (N-ERD) vs the comparison group (Asthma-AG). The order of analysis consisted of comparing baseline (t0) vs t1, t0 vs t2, t0 vs t3, t1 vs t2, etc. Then we compared by sectional specific periods both intergroup and intragroup and logistic regression was developed. For quantitative clinical variables, nonparametric statistics were used Mann Whitney U and Wilcoxon test, expressing their results in medians and interquartile range. Qualitative variables were analyzed with chi-square. was developed Statistical analyses were performed with SPSS V.21 and Epi info v.5.07 software. For all analyses, a p-value <0.05 was considered significant.
Ethics
The present study was reviewed and approved by the Bioethics and Science Committee in Research, with protocol number B14-12, and the Institutional Review Board at Instituto Nacional de Enfermedades Respiratorias (INER), Ismael Cosío Villegas, which complies with the Declaration of Helsinki. The participants were invited to join the study and they then signed the informed consent letter and were provided with an assurance-of-personal-data document. Each participant was assigned an alphanumeric key with the purpose of assuring confidentiality.
Results
Comparison Between Groups
Baseline
Of 120 N-ERD and 160 asthma patients, only 143 completed the medical follow-up (75 N-ERD and 68 asthma patients) for three years. At enrollment, the two groups had a predominance of female patients compared to male patients, with mean age and BMI similar in the two groups. Regarding the age of asthma diagnosis, smoking antecedent and the smoking index did not show significant differences (p>0.05). Eosinophil counts were double in the N-ERD group than in the AG group (400 vs 200 cells, p=0.05), but the allergic sensitivity was similar in both groups (66.6% vs 69%, p>0.05) (See Table 1).
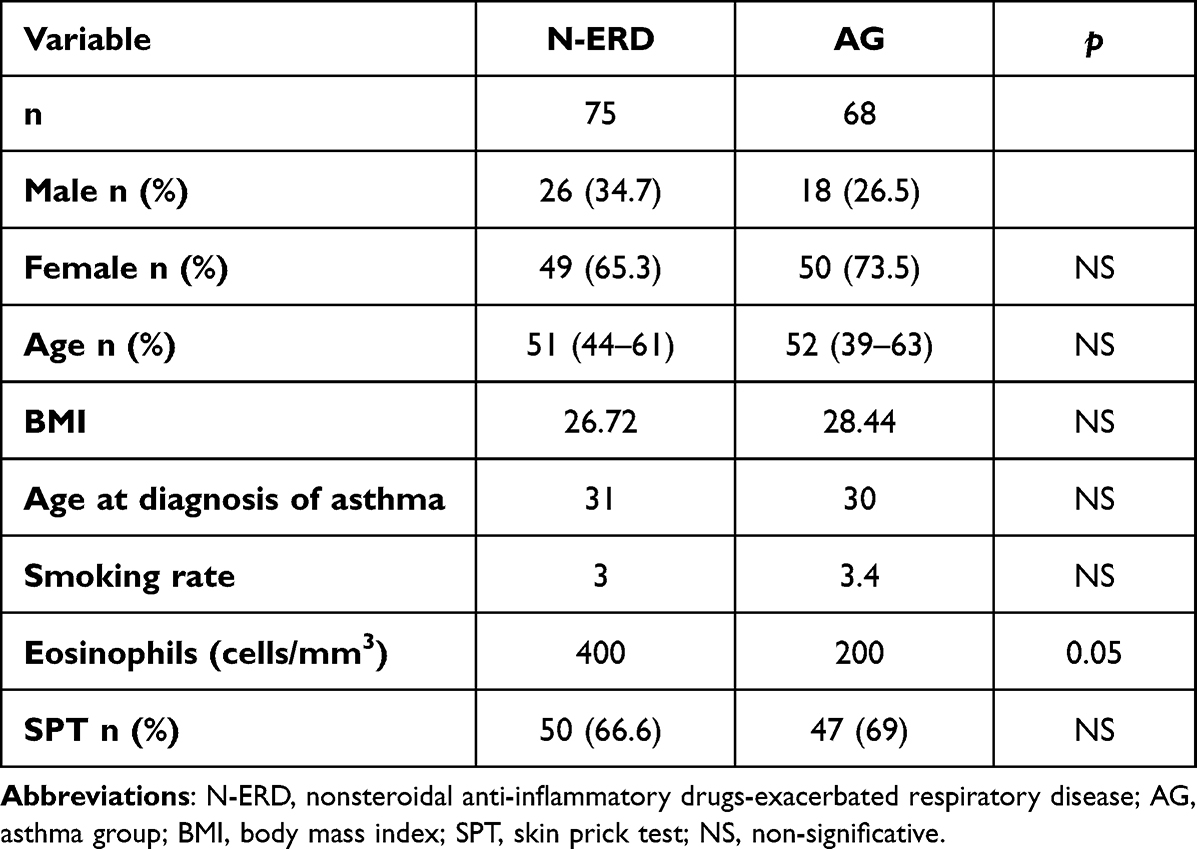 |
Table 1 Demographic Data |
Regarding lung function, the group of patients with N-ERD had a better percentage of FVC compared to AG (98% vs 69%, p<0.01), FEV1 (87% vs 50%, p<0.01), and FVC/FEV1 ratio (75% vs 66.6%, p<0.01). The frequency of lung obstruction was higher in AG than in N-ERD (60.2% vs 32% p<0.001). However, there was no difference in the reversibility test (p=0.41).
Patients with asthma had a higher proportion of high-dose ICS (52.4% vs 30.5%, p=0.01) and were prescribed a higher number of short-term OCS use (67.7% vs 42.6%, p=0.004) compared to patients with N-ERD; however, these patients received six times more LTRA (29.3% vs 5.9%, p<0.001; OR=6.6). In both groups, there was no statistically significant difference regarding the use of SABAs or the use of systemic steroids for asthma control (p>0.05). With this treatment description, patients with N-ERD had better clinical control than those with AG (62.1% vs 34.1%, p<0.01; OR=3.28) (See Table 2).
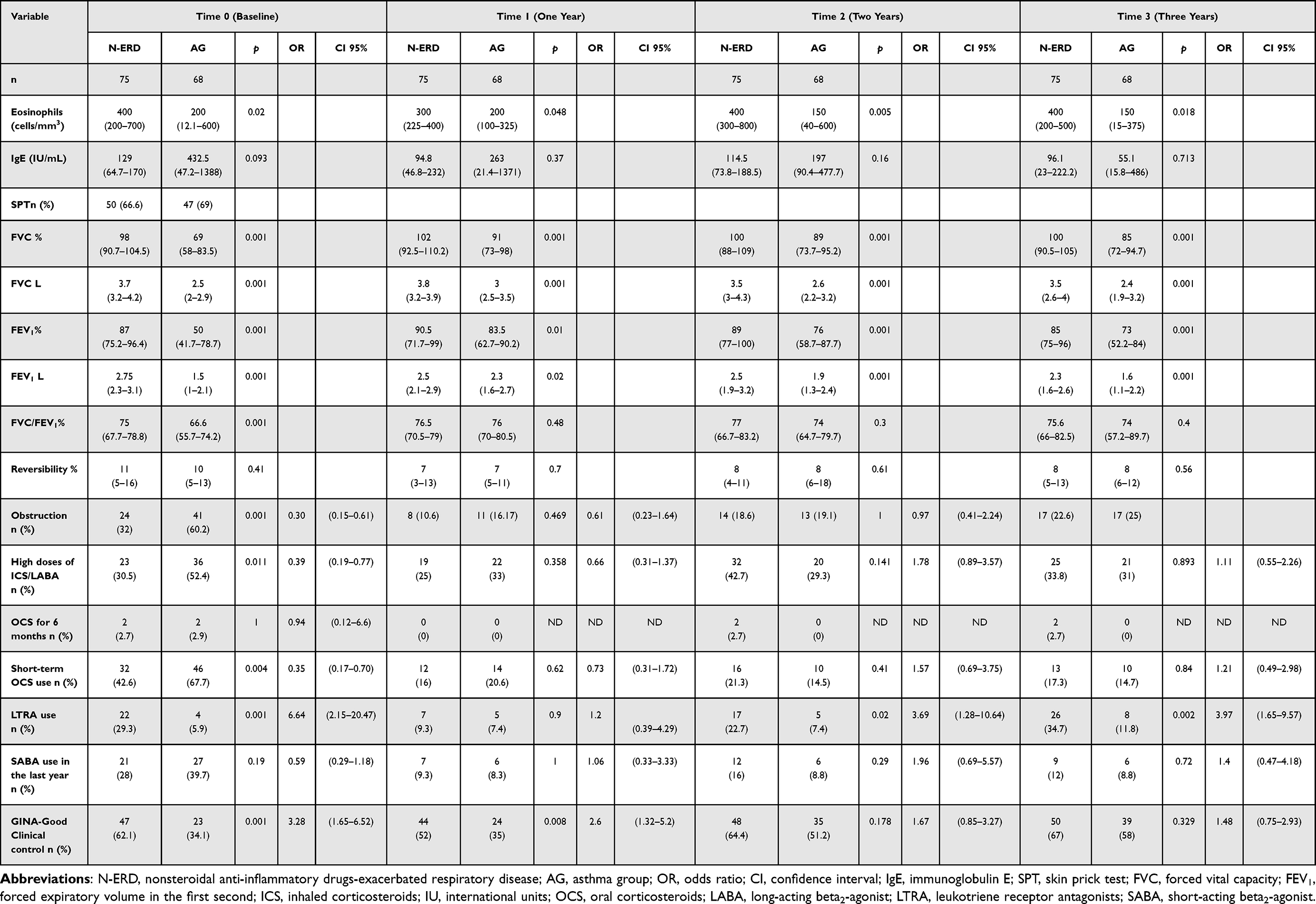 |
Table 2 Comparison Between the N-ERD Group and the AG |
Time 1 (One Year)
At 12 months after the initial measurements, the difference in the absolute eosinophil count was significantly higher in the group of N-ERD patients (300 vs 200 cells/mm3 p=0.04), even though IgE levels were higher in the AG; however, there was no statistical significance (p>0.05). The N-ERD patients had better FVC (102 vs 91%, p=0.001) and FEV1 (90.5% vs 83.5%, p=0.01), but we did not find a significant difference in the FVC/FEV1 ratio, lung obstruction, and reversibility test. There were no differences in the use of high doses of ICS, OCS, LTRA, or in the use of rescue medication with SABA (p>0.05). However, asthma clinical control continued to be better in the N-ERD group (52% vs 35%, p<0.01) (See Table 2).
Time 2 (Two Years)
Two years after starting follow-up, the total eosinophil count remained significantly higher in the group of patients with N-ERD (400 vs 150 cells/mm3, p=0.005), and IgE levels were very similar between both groups. Regarding the lung function reports, patients with N-ERD had better percentage values of FVC (100% vs 89%, p=0.001) and FEV1 (89% vs 76%, p=0.001), and no significant difference was identified in the other lung function parameters. Patients with N-ERD received 3.6 times more LTRA (22.7% vs 7.4% p=0.02; OR=3.6), but no significant difference was reported in the use of ICS at high doses, oral steroids, or SABA. At this time, we did not identify a significant difference in the clinical controls (See Table 2).
Time 3 (Three Years)
Three years after the start of follow-up, the eosinophil count remained statistically significant (400 vs 150 cells/mm3, p=0.01), unlike the IgE level. In contrast, the lung function of patients with N-ERD was better in both FVC (100% vs 85% p=0.001) and FEV1 (85% vs 73% p=0.001). FVC/FEV1, lung obstruction, and reversibility were not statistically significant. Regarding treatment, the use of LTRAs was higher (p=0.002) in patients with N-ERD. Similar to the other times, there was no significant difference in the use of high doses of ICS, oral steroids, or rescue medication in the last year of the study. According to the asthma clinical control, there was no statistical significance between both groups after three years of evaluation (p>0.05) (See Table 2).
Intragroup Analysis
IgE levels and eosinophil counts did not change substantially in the N-ERD group during the course of the study (p>0.05). Likewise, lung function remained within normal parameters (See Figure 3); although one-third of the patients had lung obstruction, it diminished at 1 year (32% vs 10.6%, p=0.002). Subsequently, the mean percentage of patients with obstruction was 17%, which did not represent a statistically significant variation. At baseline, approximately one-third of patients required high doses of ICS, LTRA, or OCS; this proportion decreased significantly at one year of evaluation (p<0.05). However, the frequency of use of these drugs increased again at 2 years and remained so until the end of the study (See Table 3). This strategy induced good clinical control according to GINA guidelines in approximately 70% of the patients (See Figure 4). Specifically, only 24 of 75 patients (32%) needed combination therapy (oral steroids plus LTRA) at least once (median of 8, 10.5%). However, only three patients required this therapeutic consecutively two times (3/75, 4%, See Figure 5). We developed a logistic regression, we just found that high doses of inhaled steroids contribute six-times to improve the clinical control of patients with N-ERD when the model was adjusted by gender. (See Table 4) However, when performing a multivariate analysis of lung function, no significant interactions were found.
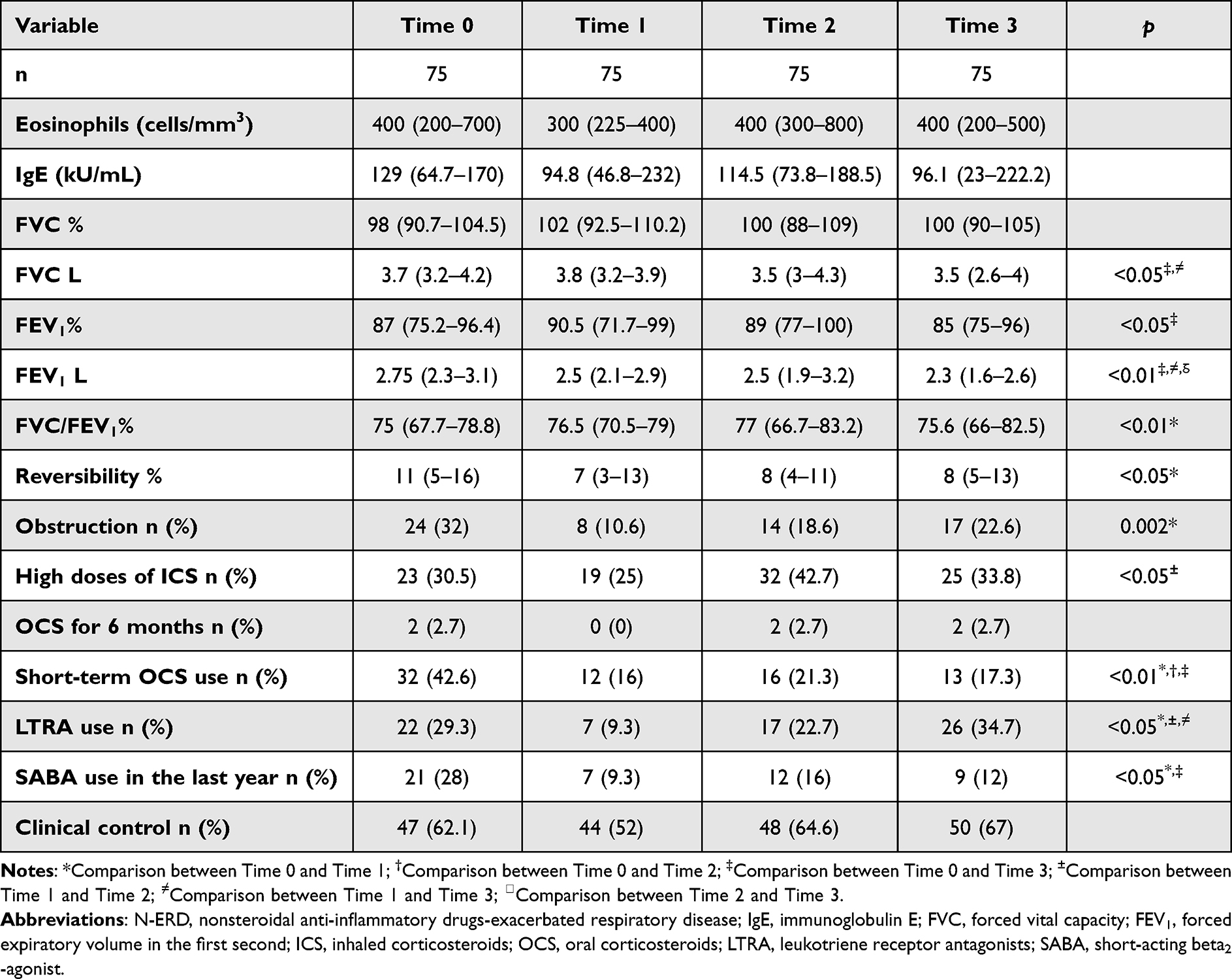 |
Table 3 Comparison Between the N-ERD Group |
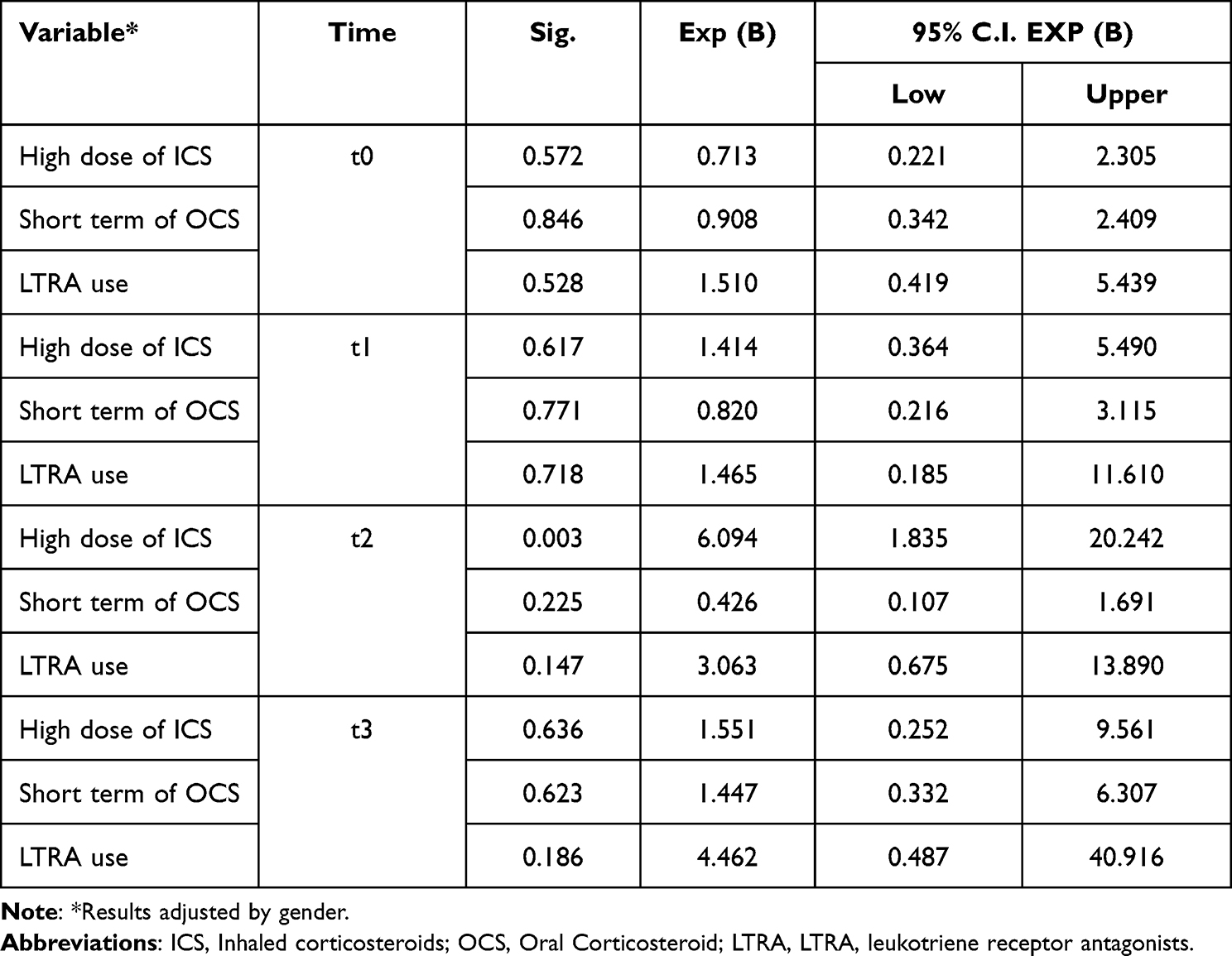 |
Table 4 Logistic Regression in N-ERD Group |
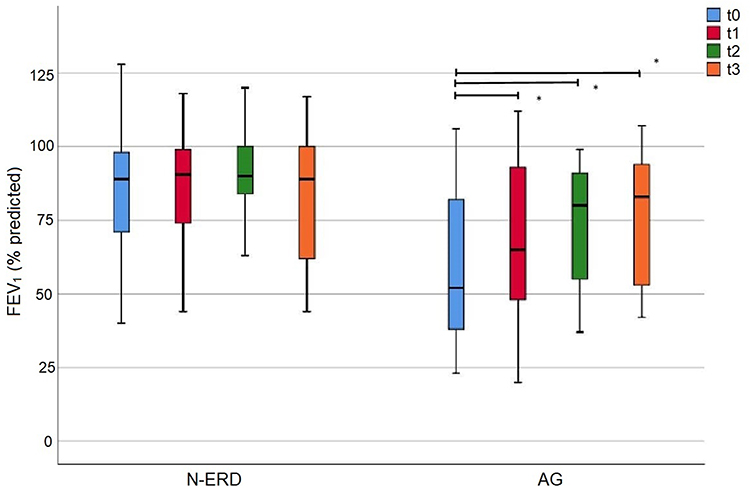 |
Figure 3 Forced Expiratory Volume in the First Second (FEV1) in N-ERD and Asthma groups. *Indicates p-value <0.05. Abbreviations: AG, Asthma group; N-ERD, Nonsteroidal anti-inflammatory drug-exacerbated respiratory disease. |
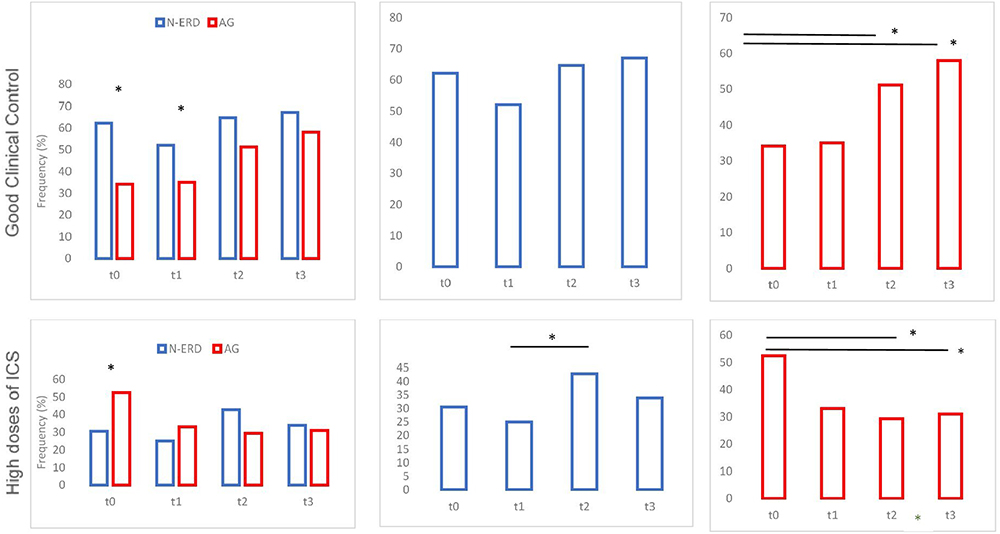 |
Figure 4 Frequency of good clinical control of asthma and high doses of inhaled corticosteroids in N-ERD and asthma groups. Basal time (t0), 12 months-time 1 (t1), 2 years-time 2 (t2), and 3 years-time 3 (t3). *Indicates p-value <0.05. Abbreviations: AG, Asthma group (RED); N-ERD, Nonsteroidal anti-inflammatory drug-exacerbated respiratory disease (BLUE). |
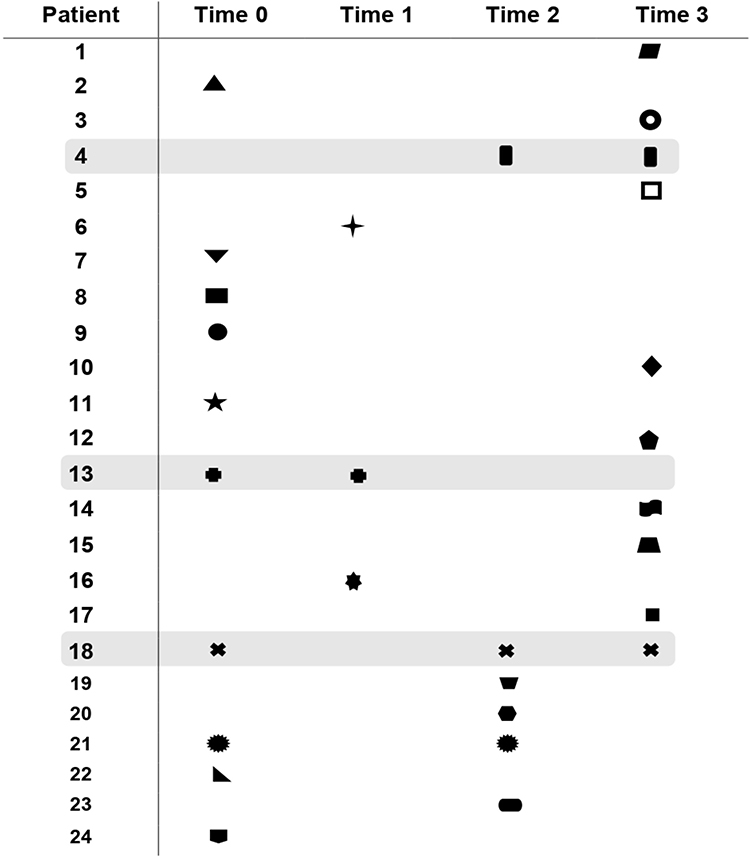 |
Figure 5 N-ERD patients in step 4 of the GINA 2014 guidelines. |
Regarding asthma patients, eosinophil counts and IgE levels decreased at the end of medical follow-up, although FVC and FEV1 increased considerably from 1 year (p<0.05), remaining without significant changes at subsequent evaluation times (Figure 3). In the case of lung obstruction, we identified a significant reduction in the frequency of patients with the condition at the same time (60.2% vs 16.1%, p=0.01). Additionally, we also observed a decrease in the usage of high doses of ICS (21%, p<0.05) and OCS (53% p<0.01) at the end of the study (See Table 5). Nonetheless, the need for high doses of ICS was similar to N-ERD patients (30%) at 3 years (See Figure 4), but not the use of LTRA (11%) or OCS (See Table 5). In the case of patients with asthma, only 11/68 (16.1%) were required to take two medications; however, they were distributed among the study times, and none were consecutively repeated (See Supplementary Figure 2). Unfortunately, no therapeutic variable associated with control improved the clinical control of patients with asthma in the logistic regression at any time (See Supplementary Table 3).
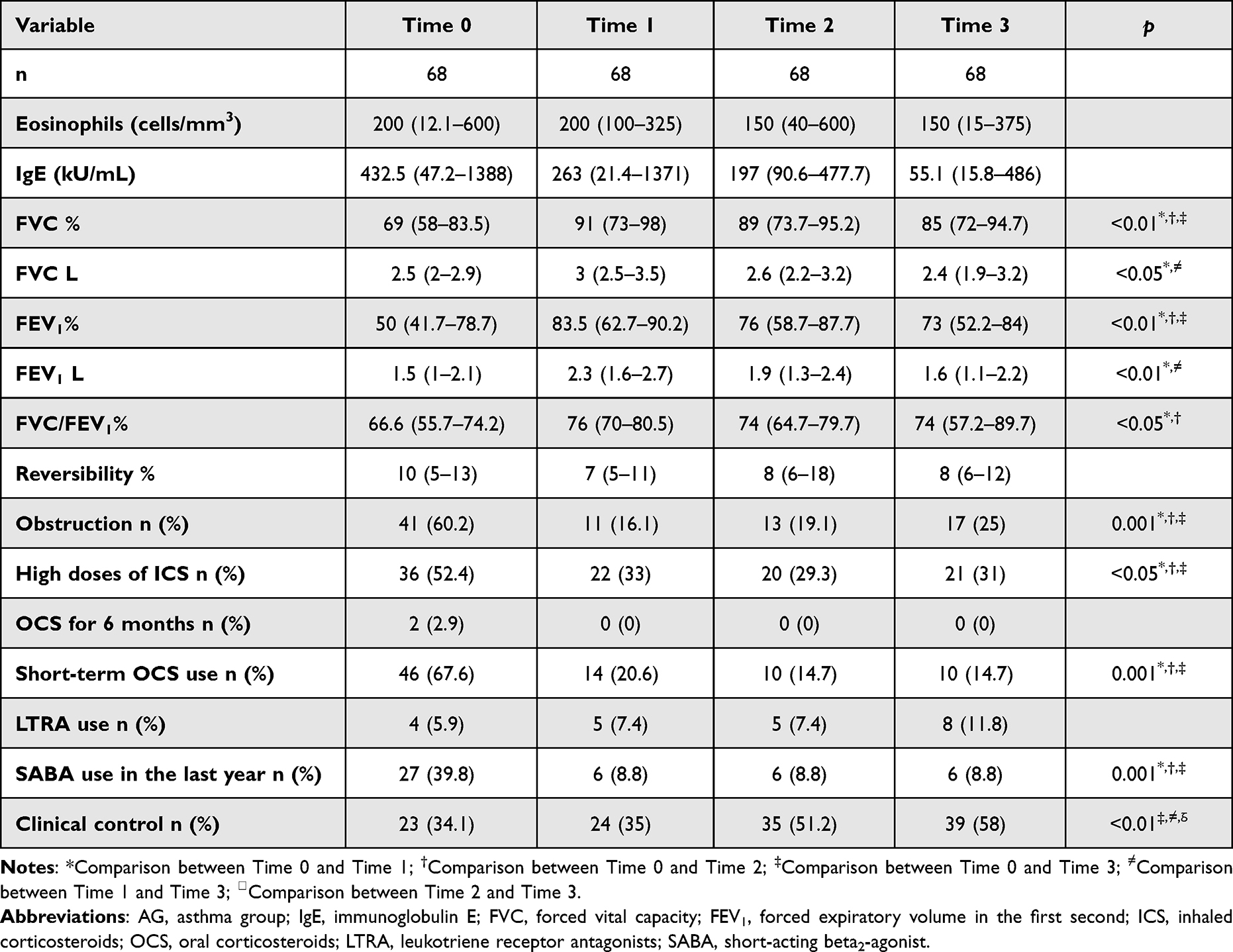 |
Table 5 Comparison Between the AG |
Discussion
In the present real-life study, we described asthma clinical control and lung function in Mexican patients with N-ERD over time according to the GINA-2014 guidelines. We demonstrated that N-ERD patients had better lung function and clinical control than asthma patients. However, N-ERD patients required higher doses of ICS and LTRA than AG patients. The asthma group also experienced improvements in these parameters during the medical follow-up with less frequent use or lower doses of these medications.
Asthma with hypersensitivity to NSAIDs is considered a specific phenotype, where the intake of NSAIDs is a risk factor for developing an asthma attack.19 Traditionally, it was considered a difficult type of asthma to treat, requiring the use of high doses of corticosteroids and/or the addition of other therapeutics for its clinical control.20 However, genetic studies that evaluated approximately 100 patients with N-ERD demonstrated that the LFT and frequency of severe asthma were similar to those of asthma patients.21–23
In our study, we enrolled patients who met the three clinical criteria needed for N-ERD diagnosis and not just those with asthma who were hypersensitive to NSAIDs. The N-ERD patients had similar clinical characteristics to those reported in other published series. N-ERD is diagnosed at approximately 30 years old and more frequent in women, with elevated blood eosinophil counts and a relevant proportion of allergic sensitivity.24,25 Instead, the AG was integrated with patients with the most common phenotype, the allergic phenotype,20 who had clinical and demographic characteristics similar to those of the N-ERD group.
At the time of enrollment, the N-ERD group had better lung function than the AG group. Few studies have evaluated the LFT in adult asthma patients over time (~12 years), and these have shown that the global improvement in FVC and FEV1 is approximately 3%.26,27 This is in accordance with our results in the N-ERD group. These values differ from the reports of drug efficacy, which evaluated its outcomes in a short time (twelve weeks); these studies showed an increase in FEV1 >15% with the use of ICS/LABA.28,29 A similar change was identified in the AG from t0 to t1, and after this time, it did not change significantly. Specifically, in the context of N-ERD, most studies have evaluated the beneficial role of desensitization. For example, this therapy improved respiratory symptoms, reduced systemic steroid intake after one month, and even increased quality of life in patients after three years.30,31
Some studies considered that N-ERD is a phenotype with severe lung obstruction and a factor driving the severity of the disease.32,33 However, in our study, only one-third of the N-ERD patients had lung obstruction at baseline, which diminished to 10% after 12 months of supervised treatment. This proportion is lower than that in studies that evaluated fixed airway obstruction in asthma (~30%).34 In addition, many studies have shown that smoking is one of the major risk factors for fixed airway obstruction in adults with severe asthma.34,35 However, in our study, neither group had an important history of smoking.
In a similar context, some studies described an augmentation in the frequency of the clinical control of asthma patients, which can reach ~60% according to GINA guidelines after the installation of the treatment.36,37 It is probable that the maximum benefits of the LFT and clinical control in asthma patients would be after the intake of control drugs for the first time, and these changes were not more noticeable over time.
In the past, some groups considered N-ERD as a phenotype of severe asthma (two or more unplanned asthma visits, two or more oral corticosteroid prescriptions in the last 12 months, current use of three or more medicines, or chronic daily high doses of ICS).33 However, the concept of severe asthma has changed. Currently, GINA establishes severe asthma as the presence of symptoms that remain uncontrolled despite optimized treatment with high-dose ICS from step 4 or that require such treatment to prevent it from becoming uncontrolled.17
N-ERD guidelines report that N-ERD patients respond well to a typical, stepwise approach to asthma treatment based on clinical guidelines such as GINA. In most N-ERD patients, a combination of ICS and LABA is sufficient to control asthma.38 However, this premise is based on expert consensus, and few studies support this precept. This is one of the first studies that evaluated lung function and clinical control in N-ERD patients over time. Despite this, current findings indicate that patients with N-ERD continue to utilize a higher proportion of inhaled oral corticosteroids and LTRA than asthma patients. This is in the same sense as reported by the Korean series which showed that about half of the patients with N-ERD are classified as severe asthma with adequate lung function values according to the parameters established by GINA.39 Regarding lung function, it did not show significant changes at the end of our study in N-ERD patients. Instead, the Korean series identified a significant change at the end of follow-up (10 years), however, it should be considered that there is an expected decrease in lung function in asthma patients, which is approximately 38 mL/year.40 Nonetheless, in both series lung function was adequate according to GINA parameters.17 It is probable that only 10% of patients with N-ERD require at least some additional treatment (LTRA) in addition to ICS/LABA (step 5 of GINA-2022),17 being the true candidates to receive biologic therapy for asthma control, which would lead to better-planned management of this therapy, reducing the costs of these treatments and improving patient adherence.
The number of polypectomies is associated with a better outcome in N-ERD. Elina Jerschow et al showed that this surgery decreased aspirin sensitivity and urine/plasma eicosanoid levels in N-ERD patients.20,41 In this way, most of our N-ERD patients had a high frequency of polypectomy or nasalization at enrollment. Likewise, aspirin desensitization and therapy with monoclonal antibodies improve asthma symptoms;6,42 however, patients with these therapies were not included. There were other factors that we did not consider that could influence the results. For example, the intake of high doses of omega-3 in the diet increases the quality of life in N-ERD patients,43 an action that some patients were able to carry out.
On the other hand, asthma is a disease that reports poor adherence to treatment (30%), which is related to higher mortality, several annual exacerbations, and the use of rescue medication.44,45 The main factor associated with adequate adherence is that the patient is aware that they need treatment. However, it has been described that after an exacerbation, patients with asthma had better adherence than patients with mild disease.46,47 This could explain why the patients with N-ERD in our study could have better adherence to treatment and therefore better lung function since one of the criteria for diagnosing N-ERD is the presence of two documented asthmatic attacks secondary to intake of NSAIDs.1 Moreover, specialized medical attendance developed by allergists, pneumologists, and noise surgeons could help to improve therapeutic adherence. Unfortunately, we did not evaluate medication adherence in asthma because there was not a validated test translated into the Spanish language and adapted to Mexican at the time of enrollment. Additionally, we did not evaluate biomarkers related to N-ERD (LTE4, LTD4, and/or PGD2). These molecules may significantly change after the initial medical treatment is established. We did not analyze other well-being markers, such as quality of life tests (AQLQ or RQLQ), due to the time, it takes to fill them. According to GINA evidence, most individuals with N-ERD can achieve satisfactory asthma control, and this evaluation is equal to obtaining a score >21 on the asthma control test.48,49
The present article is not a study of clinical efficacy or noninferiority among different brands of drugs; instead, it is a description of the modification of the clinical control of the disease with a standard therapy approved and suggested by one of the main guidelines for this disease for its control under real circumstances. This kind of study complements the knowledge generated by clinical trials that are usually limited to small, homogeneous groups of patients in specialized, controlled settings, contributing to the creation of information on the efficacy, efficiency, and safety of a drug or therapy in patients with diverse characteristics in various contexts and not just the disease of interest.50,51
Limitations to this kind of study include a) selection bias (for example, therapies may be different prescribed depending on the patient and disease characteristics, for example, the severity of the disease and/or other patient characteristics), b) information bias (misclassification of data), c) recall bias (caused by selective recall of shocking events by patients/carers), and d) detection bias (where an event is more likely to be captured in a treatment group than another).52 In these contexts, both patients with N-ERD and asthma came from first-and second-level clinics with different dosage regimens. However, these studies have the advantage of better representing the population with which is dealt in everyday clinical practice.53
Conclusion
Most patients with N-ERD can achieve good control of their asthma and adequate lung function over time according to GINA guidelines. Only a third of patients need high dosages of ICS, and a small proportion requires using a second drug to maintain asthma control during the 3-year follow-up.
Disclosure
The authors report no conflicts of interest in this work.
References
1. White AA, Stevenson DD, Longo DL. Aspirin-exacerbated respiratory disease. N Engl J Med. 2018;379(11):1060–1070. doi:10.1056/nejmra1712125
2. Rajan JP, Wineinger NE, Stevenson DD, White AA. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: a meta-analysis of the literature. J Allergy Clin Immunol. 2015;135(3):676–681.e1. doi:10.1016/j.jaci.2014.08.020
3. Pavón-Romero GF, Ramírez-Jiménez F, Roldán-Alvarez MA, Terán LM, Falfán-Valencia R. Physiopathology and genetics in aspirin-exacerbated respiratory disease. Exp Lung Res. 2017;43(8):327–335. doi:10.1080/01902148.2017.1358776
4. Scott WC, Cahill KN, Milne GL, et al. Inflammatory heterogeneity in aspirin-exacerbated respiratory disease. J Allergy Clin Immunol. 2021;147(4):1318–1328.e5. doi:10.1016/j.jaci.2020.11.001
5. Kowalski ML, Agache I, Bavbek S, et al. Diagnosis and management of NSAID ‐Exacerbated Respiratory Disease (N‐ ERD)—a EAACI position paper. Allergy. 2019;74(1):28–39. doi:10.1111/all.13599
6. Li R, Luo F. Safety and efficacy of aspirin desensitization combined with long-term aspirin therapy in aspirin-exacerbated respiratory disease. J Investig Allergol Clin Immunol. 2020;30(5):327–333. doi:10.18176/jiaci.0433
7. Tuttle KL, Buchheit KM, Laidlaw TM, Cahill KN. A retrospective analysis of mepolizumab in subjects with aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2018;6(3):1045–1047. doi:10.1016/j.jaip.2018.01.038
8. Schatz M, Hsu JWY, Zeiger RS, et al. Phenotypes determined by cluster analysis in severe or difficult-to-treat asthma. J Allergy Clin Immunol. 2014;133(6):1549–1556. doi:10.1016/j.jaci.2013.10.006
9. Joppert W, Stillner CA, Cruz VO. Closure of splenic bed after splenectomy in cases of huge splenomegaly. Int Surg. 1979;64(3):61–62.
10. Shin S-W, Park J, Kim Y-J, et al. A highly sensitive and specific genetic marker to diagnose aspirin-exacerbated respiratory disease using a genome-wide association study. DNA Cell Biol. 2012;31(11):1604–1609. doi:10.1089/dna.2012.1688
11. Turpeinen H, Laulajainen-Hongisto A, Lyly A, et al. Lung function and side effects of Aspirin desensitization: a real world study. Eur Clin Respir J. 2021;8(1). doi:10.1080/20018525.2020.1869408
12. Makary CA, Holmes T, Unsal A, et al. Long-term role of zileuton in the treatment of chronic rhinosinusitis in aspirin exacerbated respiratory disease. Am J Otolaryngol. 2022;43(1):103227. doi:10.1016/j.amjoto.2021.103227
13. Talat R, Gengler I, Phillips KM, Caradonna DS, Gray ST, Sedaghat AR. Chronic rhinosinusitis outcomes of patients with aspirin-exacerbated respiratory disease treated with budesonide irrigations: a case series. Ann Otol Rhinol Laryngol. 2022;131(10):1130–1136. doi:10.1177/00034894211054948
14. Lal D, Golisch K, Chang YHA, Rank M. Baseline clinical characteristics predict follow-up clinic attendance in patients undergoing endoscopic sinus surgery for chronic rhinosinusitis: clinic attendance after ESS. Int Forum Allergy Rhinol. 2016;6(5):508–513. doi:10.1002/alr.21701
15. Ramírez-Jiménez F, Vázquez-Corona A, Sánchez-de la Vega Reynoso P, et al. Effect of LTRA in L-ASA challenge for aspirin-exacerbated respiratory disease diagnosis. J Allergy Clin Immunol Pract. 2021;9(4):1554–1561. doi:10.1016/j.jaip.2020.10.041
16. Jakiela B, Soja J, Sladek K, et al. Heterogeneity of lower airway inflammation in patients with NSAID-exacerbated respiratory disease. J Allergy Clin Immunol. 2021;147(4):1269–1280. doi:10.1016/j.jaci.2020.08.007
17. Global strategy for asthma management and prevention revised 2014; 2014. Available from: https://ginasthma.org/wp-content/uploads/2019/01/2014-GINA.pdf.
18. Torre-Bouscoulet L, Pérez-Padilla R. Ajuste de varias ecuaciones de referencia espirométrica a una muestra poblacional en México. Salud Publica Mex. 2006;48(6). doi:10.1590/s0036-36342006000600004
19. ENFUMOSA Study Group. The ENFUMOSA cross-sectional European multicentre study of the clinical phenotype of chronic severe asthma. Eur Respir J. 2003;22(3):470–477. doi:10.1183/09031936.03.00261903
20. Bochenek G, Szafraniec K, Kuschill-Dziurda J, Nizankowska-Mogilnicka E. Factors associated with asthma control in patients with aspirin-exacerbated respiratory disease. Respir Med. 2015;109(5):588–595. doi:10.1016/j.rmed.2015.02.015
21. Ban GY, Youn DY, Ye YM, Park HS. Increased expression of serine palmitoyl transferase and ORMDL3 polymorphism are associated with eosinophilic inflammation and airflow limitation in aspirin-exacerbated respiratory disease. PLoS One. 2020;15(10):e0240334. doi:10.1371/journal.pone.0240334
22. Park BL, Kim TH, Kim JH, et al. Genome-wide association study of aspirin-exacerbated respiratory disease in a Korean population. Hum Genet. 2013;132(3):313–321. doi:10.1007/s00439-012-1247-2
23. Pavón-Romero GF, Pérez-Rubio G, Ramírez-Jiménez F, et al. IL10 rs1800872 is associated with non-steroidal anti-inflammatory drugs exacerbated respiratory disease in Mexican-mestizo patients. Biomolecules. 2020;10(1):104. doi:10.3390/biom10010104
24. Kuruvilla ME, Lee FEH, Lee GB. Understanding asthma phenotypes, endotypes, and mechanisms of disease. Clin Rev Allergy Immunol. 2019;56(2):219–233. doi:10.1007/s12016-018-8712-1
25. Taniguchi M, Mitsui C, Hayashi H, et al. Aspirin-exacerbated respiratory disease (AERD): current understanding of AERD. Allergol Int. 2019;68(3):289–295. doi:10.1016/j.alit.2019.05.001
26. Vähätalo I, Ilmarinen P, Tuomisto LE, Niemelä O, Kankaanranta H. Inhaled corticosteroids and asthma control in adult-onset asthma: 12-year follow-up study. Respir Med. 2018;137:70–76. doi:10.1016/j.rmed.2018.02.025
27. Vähätalo I, Kankaanranta H, Tuomisto LE, Niemelä O, Lehtimäki L, Ilmarinen P. Long-term adherence to inhaled corticosteroids and asthma control in adult-onset asthma. ERJ Open Res. 2021;7(1):00715–02020. doi:10.1183/23120541.00715-2020
28. Hojo M, Iikura M, Hirashima J, Suzuki M, Sugiyama H. A comparison of long-term anti-inflammatory effect of two ICS/LABA combination inhalers; Fix-dosed maintenance therapy with budesonide/formoterol and salmeterol/fluticasone. Allergol Int. 2014;63(1):103–111. doi:10.2332/allergolint.13-oa-0590
29. Sher LD, Yiu G, Sakov A, Liu S, Caracta CF. Fluticasone propionate and fluticasone propionate/salmeterol multidose dry powder inhalers compared with placebo for persistent asthma. Allergy Asthma Proc. 2017;38(5):343–353. doi:10.2500/aap.2017.38.4069
30. Berges-Gimeno MP, Simon RA, Stevenson DD. Early effects of aspirin desensitization treatment in asthmatic patients with aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol. 2003;90(3):338–341. doi:10.1016/s1081-1206(10)61803-0
31. Porpodis K, Papakosta D, Manika K, et al. Long-term prognosis of asthma is good—A 12-year follow-up study. Influence of treatment. J Asthma. 2009;46(6):625–631. doi:10.1080/02770900903029796
32. Hough KP, Curtiss ML, Blain TJ, et al. Airway Remodeling in Asthma. Front Med. 2020;7. doi:10.3389/fmed.2020.00191
33. Mascia K, Haselkorn T, Deniz YM, Miller DP, Bleecker ER, Borish L. Aspirin sensitivity and severity of asthma: evidence for irreversible airway obstruction in patients with severe or difficult-to-treat asthma. J Allergy Clin Immunol. 2005;116(5):970–975. doi:10.1016/j.jaci.2005.08.035
34. Yii ACA, Tan GL, Tan KL, Lapperre TS, Koh MS. Fixed airways obstruction among patients with severe asthma: findings from the Singapore general hospital-severe asthma phenotype study. BMC Pulm Med. 2014;14(1). doi:10.1186/1471-2466-14-19
35. Lee T, Lee YS, Bae YJ, et al. Smoking, longer disease duration and absence of rhinosinusitis are related to fixed airway obstruction in Koreans with severe asthma: findings from the COREA study. Respir Res. 2011;12(1). doi:10.1186/1465-9921-12-1
36. Boskabady MH, Rezaeitalab F, Rahimi N, Dehnavi D. Improvement in symptoms and pulmonary function of asthmatic patients due to their treatment according to the Global Strategy for Asthma Management (GINA). BMC Pulm Med. 2008;8(1). doi:10.1186/1471-2466-8-26
37. Lin J, Fu X, Jiang P, et al. INITIAL – an observational study of disease severity in newly diagnosed asthma patients and initial response following 12 weeks’ treatment. Sci Rep. 2019;9(1). doi:10.1038/s41598-018-36611-w
38. Stevens WW, Peters AT, Hirsch AG, et al. Clinical characteristics of patients with chronic rhinosinusitis with nasal polyps, asthma, and aspirin-exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2017;5(4):1061–1070.e3. doi:10.1016/j.jaip.2016.12.027
39. Lee Y, Kim C, Lee E, et al. Long‐term clinical outcomes of aspirin‐exacerbated respiratory disease: real‐world data from an adult asthma cohort. Clin Exp Allergy. 2023. doi:10.1111/cea.14362
40. Sears MR. Lung function decline in asthma. Eur Respir J. 2007;30(3):411–413. doi:10.1183/09031936.00080007
41. Jerschow E, Edin ML, Chi Y, et al. Sinus surgery is associated with a decrease in aspirin-induced reaction severity in patients with aspirin exacerbated respiratory disease. J Allergy Clin Immunol Pract. 2019;7(5):1580–1588. doi:10.1016/j.jaip.2018.12.014
42. Mullur J, Steger CM, Gakpo D, et al. Aspirin desensitization and biologics in aspirin-exacerbated respiratory disease. Ann Allergy Asthma Immunol. 2022;128(5):575–582. doi:10.1016/j.anai.2022.01.043
43. Schneider TR, Johns CB, Palumbo ML, Murphy KC, Cahill KN, Laidlaw TM. Dietary fatty acid modification for the treatment of aspirin-exacerbated respiratory disease: a prospective pilot trial. J Allergy Clin Immunol Pract. 2018;6(3):825–831. doi:10.1016/j.jaip.2017.10.011
44. Lindsay JT, Heaney LG. Non-adherence in difficult asthma and advances in detection. Expert Rev Respir Med. 2013;7(6):607–614. doi:10.1586/17476348.2013.842129
45. Schatz M, Zeiger RS, Yang SJ, et al. Change in asthma control over time: predictors and outcomes. J Allergy Clin Immunol Pract. 2014;2(1):59–64. doi:10.1016/j.jaip.2013.07.016
46. Baba K, Hattori T, Yagi T, et al. Adherence with long-term asthma management in patients who experienced hospitalized asthma exacerbation. Allergol Int. 2009;58(2):217–224. doi:10.2332/allergolint.08-oa-0012
47. Engelkes M, Janssens HM, de Jongste JC, Sturkenboom MCJM, Verhamme KMC. Medication adherence and the risk of severe asthma exacerbations: a systematic review. Eur Respir J. 2015;45(2):396–407. doi:10.1183/09031936.00075614
48. Akan A, Dibek Mısırlıoğlu E, Civelek E, Kocabaş CN. Determining the best tool comparable with global initiative for asthma criteria for assessing pediatric asthma control. Pediatr Allergy Immunol Pulmonol. 2021;34(3):89–96. doi:10.1089/ped.2020.1334
49. Alvarez-Gutiérrez FJ, Medina-Gallardo JF, Pérez-Navarro P, et al. Relación del test de control del asma (ACT) con la función pulmonar, niveles de óxido nítrico exhalado y grados de control según la Iniciativa Global para el Asma (GINA). Arch Bronconeumol. 2010;46(7):370–377. doi:10.1016/j.arbres.2010.04.003
50. Franklin JM, Liaw KL, Iyasu S, Critchlow CW, Dreyer NA. Real‐world evidence to support regulatory decision making: new or expanded medical product indications. Pharmacoepidemiol Drug Saf. 2021;30(6):685–693. doi:10.1002/pds.5222
51. Maissenhaelter BE, Woolmore AL, Schlag PM. Real-world evidence research based on big data: motivation-challenges-success factors. Onkologe. 2018;24(S2):91–98. doi:10.1007/s00761-018-0358-3
52. Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world clinical data for the practicing clinician. Adv Ther. 2018;35(11):1763–1774. doi:10.1007/s12325-018-0805-y
53. Harari S. Randomised controlled trials and real-life studies: two answers for one question. Eur Respir Rev. 2018;27(149):180080. doi:10.1183/16000617.0080-2018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Extracellular Traps: A Novel Therapeutic Target for Severe Asthma
Choi Y, Luu QQ, Park HS
Journal of Asthma and Allergy 2022, 15:803-810
Published Date: 14 June 2022
Management of Uncontrolled Asthma: A Framework for Novel and Legacy Biologic Treatments
Tan LD, Nguyen N, Alismail A, Castro M
Journal of Asthma and Allergy 2022, 15:875-883
Published Date: 29 June 2022
Utilization Patterns and Trends in the Use of Medications for Asthma in a Cohort of Colombian Patients
Machado-Duque ME, Gaviria-Mendoza A, Valladales-Restrepo LF, García-Nuncira C, Laucho-Contreras M, Machado-Alba JE
Journal of Asthma and Allergy 2022, 15:1347-1357
Published Date: 25 September 2022
Prevalence and Characterisation of Patients with Asthma According to Disease Severity in Portugal: Findings from the EPI-ASTHMA Pilot Study
João C, Jácome C, Brito D, Teixeira P, Quelhas-Santos J, Amorim L, Barbosa MJ, Bulhões C, Lopes F, Pardal M, Bernardo F, Fonseca JA, Correia de Sousa J
Journal of Asthma and Allergy 2022, 15:1441-1453
Published Date: 19 October 2022
Association Between Medication Adherence and Risk of COPD in Adult Asthma Patients: A Retrospective Cohort Study in Canada
Asamoah-Boaheng M, Farrell J, Bonsu KO, Oyet A, Midodzi WK
Clinical Epidemiology 2022, 14:1241-1254
Published Date: 27 October 2022