Back to Journals » Journal of Pain Research » Volume 19
Lumbar Sympathicolysis Attenuates Refractory Chemotherapy-Induced Peripheral Neuropathy in the Lower Extremities: A Prospective, Real-World Study
Authors Suo J ![]() , Zhang F, Fan B, Joshi KS, Ma D
, Zhang F, Fan B, Joshi KS, Ma D ![]() , Xie G
, Xie G
Received 28 August 2025
Accepted for publication 6 February 2026
Published 16 February 2026 Volume 2026:19 563861
DOI https://doi.org/10.2147/JPR.S563861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Michael Überall
Jiaojiao Suo,1,* Fang Zhang,2,* Bifa Fan,3 Kiran S Joshi,4 Daqing Ma,4,5 Guanglun Xie1
1Department of Pain Rehabilitation and Palliative Medicine, The Affiliated Cancer Hospital of Zhengzhou University and Henan Cancer Hospital, Zhengzhou, People’s Republic of China; 2Department of Anesthesiology, People’s Hospital of Henan University of Traditional Chinese Medicine, Zhengzhou, People’s Republic of China; 3Department of Pain Management, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 4Division of Anaesthetics, Pain Medicine and Intensive Care, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, Chelsea and Westminster Hospital, London, UK; 5Perioperative and Systems Medicine Laboratory and Department of Anesthesiology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guanglun Xie, Department of Pain Rehabilitation and Palliative Medicine, the Affiliated Cancer Hospital of Zhengzhou University and Henan Cancer Hospital, ZhengZhou, 450008, People’s Republic of China, Tel +8613939029792, Email [email protected] Daqing Ma, Division of Anaesthetics, Pain Medicine and Intensive Care, Department of Surgery and Cancer, Faculty of Medicine, Imperial College London, Chelsea and Westminster Hospital, London, SW109NH, UK, Email [email protected]
Purpose: Currently, there are limited effective treatment strategies available for refractory chemotherapy-induced peripheral neuropathy (CIPN). Lumbar sympathicolysis is a minimally invasive therapy and may offer an option for CIPN. This single-center, prospective, observational study aimed to evaluate the efficacy and safety of CT-guided lumbar sympathicolysis in alleviating multiple symptoms of refractory CIPN in the lower extremities.
Methods: This single-arm study conducted at Henan Cancer Hospital from September 2022 to July 2024,twenty-five patients with refractory CIPN in both lower extremities received CT-guided lumbar sympathicolysis. The effectiveness of the treatment for pain, numbness, cold sensation, and dyskinesia was evaluated using a Numerical Rating Scale (NRS) at day 3, one month, and three months following treatment. Treatment response was defined as an NRS score reduction of ≥ 30%. Changes in NRS scores over time were analyzed using generalized estimating equations. Any adverse effects related to the treatment were recorded.
Results: Postoperative NRS scores for pain, numbness, cold sensation, and dyskinesia at 3 days, 1 month, and 3 months were significantly lower than these assessed before the treatment. The pain improvement assessed with NRS scores was reported to be 61.1% at 3 days, 55.5% at 1 month, and 55.5% at 3 months by patients (n=18). The numbness improvement was 24.0% at day 3, 16.0% at 1 month, and 16.0% at 3 months (n=25). Cold sensation improvement (n=21) was 71.4%, 57.1%, and 52.4% at day 3, 1 month, and 3 months (n=21), respectively. The decreased dyskinesia sensation was reported by 50.0% at day 3 and 1 month, and 57.1% at 3 months (n=14). Overall, all symptoms were decreased by 68% at day 3, 64% at 1 month, and 60% at 3 months.
Conclusion: The CT-guided lumbar sympathicolysis may offer substantial symptom relief for CIPN in the lower extremities without clinically significant adverse effects. These preliminary findings warrant further validation in larger, controlled studies.
Keywords: chemotherapy-induced peripheral neuropathy, lumbar sympathicolysis, pain relief
Introduction
Chemotherapy-induced peripheral neuropathy (CIPN) is one of the most serious toxicity effects caused by chemotherapy agents such as taxanes, platinum compounds, vinca alkaloids, thalidomide, and bortezomib.1–3 CIPN presents with classic “glove and stocking” neuropathy dominated by sensory disturbances (ie, numbness, pins-and-needles sensation, pain or cold sensitivity), in addition to motor and autonomic dysfunction, especially in the lower limbs.4 CIPN is unpredictable, and previous studies showed that up to 30% of patients treated with high-risk chemotherapy drugs may experience symptoms lasting for six months or even longer.5 As chemotherapy doses accumulated, symptoms often worsen, requiring dose reductions or early termination of treatment. This not only severely affects patients’ quality of life but may also negatively impact overall survival.6–8 Although symptoms may gradually improve over time, a significant number of patients, particularly long-term cancer survivors, suffered from persistent or even permanent nerve damage.5,9,10 Pharmacological and non-pharmacological interventions for managing CIPN are limited and also lack strong evidence supporting their effectiveness.11 Commonly prescribed drugs included duloxetine, pregabalin, opioids, neurotrophic agents (such as B vitamins and methylcobalamin), and NSAIDs.12–14 Non-pharmacological treatments, such as acupuncture, physical therapy, and neurofeedback, also have been reported but their effectiveness in CIPN remains uncertain.15–17 Hence, the need for more effective CIPN treatments remains urgent.
Lumbar sympathicolysis is the physical and chemical disruption of the corresponding segment of the lumbar sympathetic nerve to inhibit sympathetic conduction and thereby treat sympathetic-related pain, numbness, cold sensation, intermittent sensation, claudication, and other symptoms.18,19 Previous evidence showed that lumbar sympathicolysis alleviated symptoms such as pain and cold sensation in lower limb ischemic diseases (eg atherosclerotic occlusive disease, diabetic foot and thromboembolic vasculitis) by improving blood flow.20,21 However, its mechanism of action extends beyond vascular effects and can also be applied to the treatment of neuropathic pain. The sympathetic nervous system has been shown to participate in peripheral sensitization and the maintenance of chronic neuropathic pain.22 Although CIPN is primarily mediated by neurotoxic mechanisms, abnormal sympathetic activity may exacerbate symptoms such as persistent pain and vasomotor instability.23,24 Therefore, based on the established role of sympathetic modulation in neuropathic pain syndromes, the application of targeted lumbar sympathicolysis to CIPN remains unexplored. We hypothesized that lumbar sympathicolysis would alleviate refractory sensory and vasomotor symptoms in patients with CIPN by attenuating sympathetic overactivity and its downstream effects on neuroinflammation and peripheral microcirculation. To test this hypothesis, we conducted a single-arm, prospective study to evaluate, for the first time, the efficacy and safety of CT-guided lumbar sympathicolysis in patients with bilateral lower limb CIPN refractory to conventional pharmacological treatment.
Methods
Patient Recruitment
This prospective,single-center study adopted a single-arm, quasi-experimental design with repeated measures (pre- and post-intervention assessments) to evaluate CT-guided lumbar sympathicolysis for refractory CIPN under routine clinical conditions. This study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Biomedical Ethics Committee of Henan Cancer Hospital (No. 2022-KY-0077-002) and written informed consent was obtained from all participants. This study was conducted from September 2022 to July 2024. Patients with refractory CIPN were recruited at Henan Cancer Hospital. All patients underwent CT-guided lumbar sympathicolysis, with symptom scores evaluated preoperatively, as well as on the third day, at one month, and three months postoperatively.
Refractory CIPN was defined based on the following criteria were: 1) CIPN symptoms in the lower extremities; 2) symptoms persisting for over three months; 3) presence of pain, numbness, cold sensation, or motor dysfunction, with at least one symptom having an NRS score ≥ 4; and 4) lack of symptom improvement following treatment with duloxetine, pregabalin, neurotropin, or other neurotrophic agents.
Exclusion criteria included: 1) neurological symptoms due to primary tumor, metastasis, or non-chemotherapy-related causes (eg, diabetic peripheral neuropathy); 2) infection, coagulation disorders, or severe cardiac, pulmonary, or other comorbid conditions precluding surgery; 3) CT evidence of metastatic lymph nodes or abnormalities around the puncture site; 4) psychiatric disorders or cognitive impairment affecting compliance; 5) alcohol allergy.
Procedures
CT-guided lumbar sympathicolysis was performed bilaterally on the lumbar sympathetic ganglia. In the prone position, the puncture sites and paths were determined through CT images. The 15 cm, 20G radiofrequency cannula needles were inserted, with the tips positioned at the anterolateral third of the L2 vertebra and the upper third of the L3 vertebra, to minimize the risk of injury to the aorta or mesenteric artery. Following confirmation of needle placement, sensory and motor function assessments were conducted using radiofrequency electrodes (Figure 1a and b), and 1–2 mL of a mixture of 1% lidocaine and 10% iodinated contrast agent was injected. CT confirmed the appropriate spread of the contrast agent along the prevertebral fascial plane without abnormal diffusion.
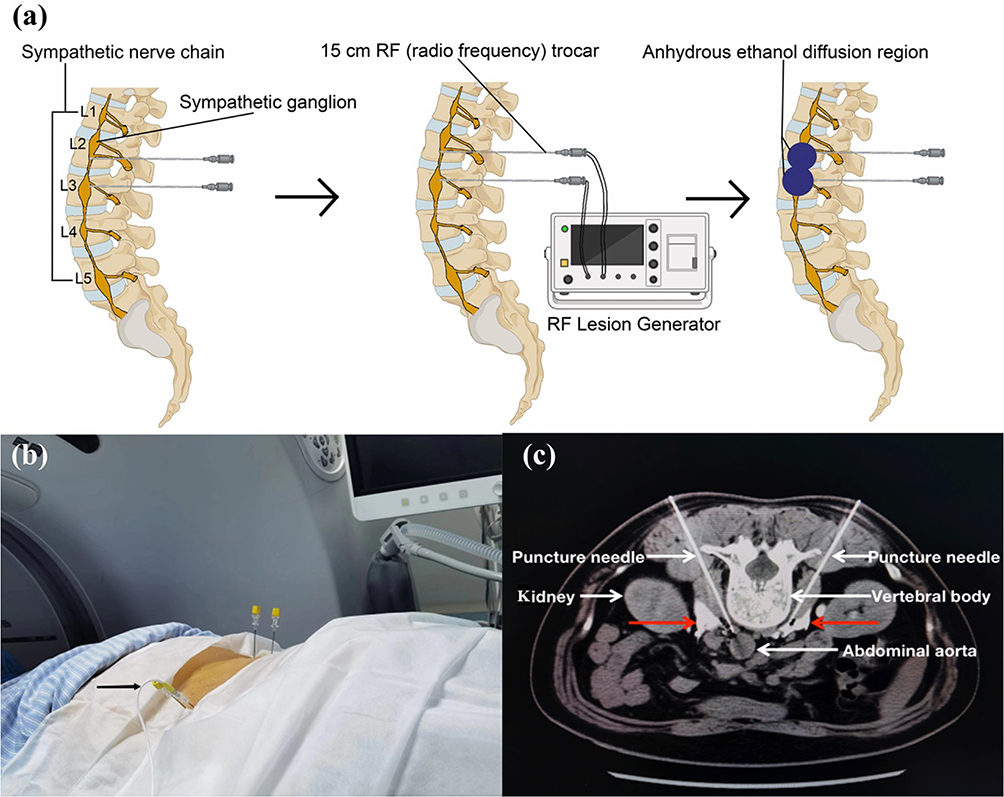 |
Figure 1 Schematic diagram of CT-guided lumbar sympathicolysis in patients with refractory chemotherapy-induced peripheral neuropathy in the lower extremities. (a) Schematic illustration of the procedure. (b) After four puncture needles were inserted into place under CT-guidance, radiofrequency electrodes (black arrow) were disposed of from the core of the puncture needles for sensory-motor testing and subsequent continuous operation with physical radiofrequency. (c) A CT scan in the case of both-sided lumbar sympathicolysis: intercavovertebral positioning of the puncture needle and distribution of the sympatholytic agent.Red arrows highlight the distribution area of the agent around the lumbar sympathetic chain. |
The radiofrequency ablation was performed for 6 minutes (75°C for 3 minutes, followed by 80°C for 3 minutes). Subsequently, 2–3 mL of a mixture of 90% anhydrous alcohol and 10% contrast agent was injected on each side, with the total dose per side being 6–9 mL (Figure 1c). Postoperative CT verified the appropriate distribution of the agent. Patients remained in a prone position for two hours post-procedure to minimize the risk of alcohol diffusion.
Efficacy Evaluation
Baseline data including age, sex, symptom duration, tumor type, and chemotherapy cycles were recorded. Symptom severity (pain, numbness, cold sensation, dyskinesia) in the lower extremities was assessed using the Numerical Rating Scale (NRS), with 0 indicating no symptoms and 10 indicating the most intolerable symptoms imaginable.25 NRS scores were collected before and at day 3, 1 month, and 3 months after the treatment by unblinded clinicians or research nurses.
A reduction in NRS score of ≥ 30% from baseline was considered a clinically meaningful response, while a reduction of < 30% was deemed non-responsive. The improvement in sensation was expressed as a response rate, which was calculated as the proportion of responsive cases relative to the total number of cases for each symptom. Adverse events, such as bleeding, hypotension, diarrhea, or nerve damage, were identified, recorded, and graded for severity (Grades 1–5) in strict accordance with the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical Analysis
Data were analyzed using SPSS 26.0. Non-normally distributed data were expressed as median and interquartile range [M (P25, P75)]. Given the repeated-measures structure of longitudinal symptom assessments, comparisons of NRS scores across different time points were performed using generalized estimating equations with an exchangeable working correlation matrix. Categorical data were presented as [n (%)], and Fisher’s exact test was used to compare response rates across time points. A P value less than 0.05 was considered to be of statistical significance.
Results
Patient Characteristics
From September 2022 to July 2024, a total of 25 patients participated and completed the study (Table 1). The median age of the patients was 64 years with a higher proportion of female patients (60%). The median duration of CIPN symptoms was 6.0 months following the median 6 cycles of chemotherapy. The most commonly used chemotherapy agents were platinum (14/25) and taxanes (8/25). The symptoms were reported as numbness, affecting all patients (100%), followed by cold sensation (84%), pain (72%), and dyskinesia (56%).
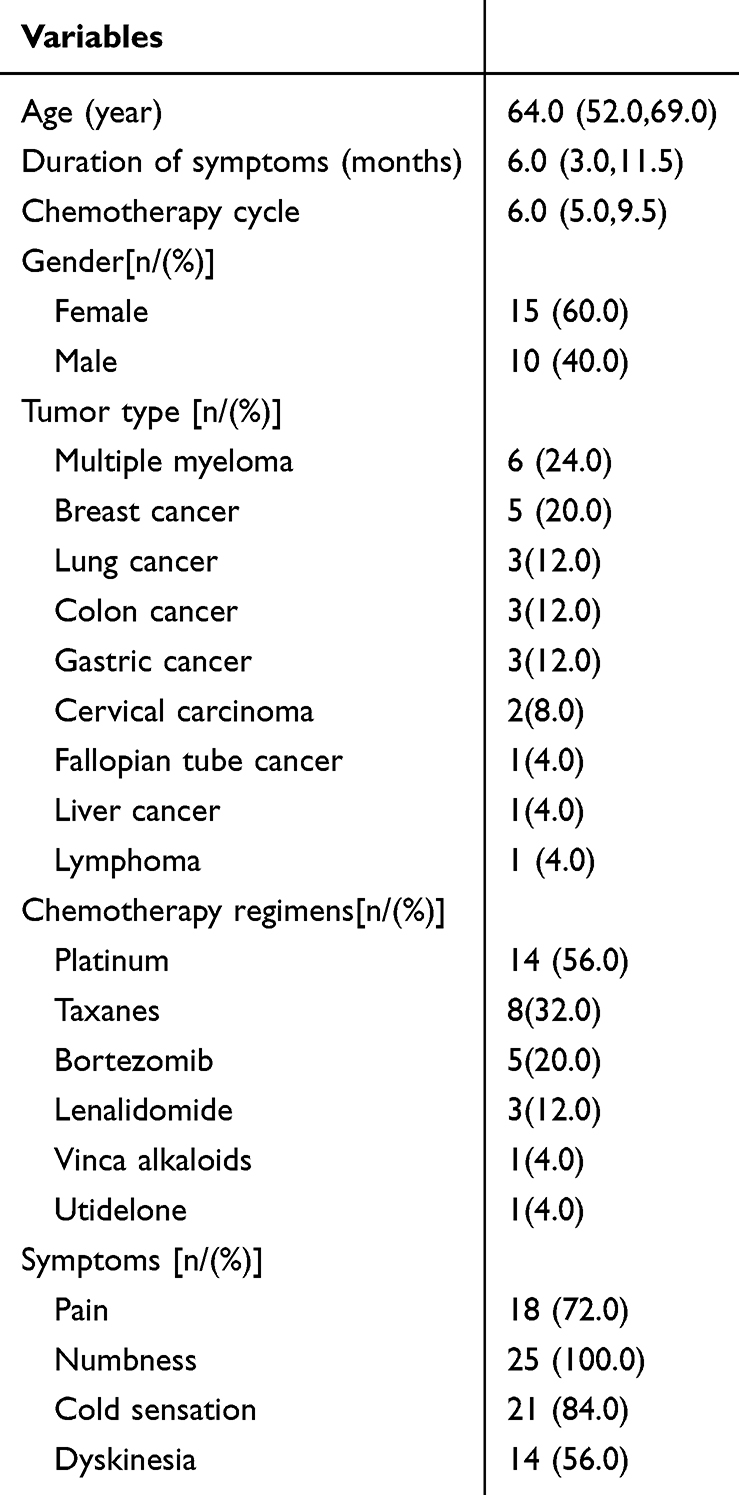 |
Table 1 Baseline Characteristics of the Patients Included in This Study |
Efficacy and Outcomes
Overall, the NRS scores for pain, numbness, cold sensation, and dyskinesia were significantly lower at 3 days, 1 month, and 3 months post-CIPN surgery compared to preoperative scores (P < 0.05) (Figure 2 and Table 2). Across the 25 patients, The improvement response rates were 68% at 3 days, 64% at 1 month, and 60% at 3 months post-operation (P < 0.05) (Figure 3 and Table 3).
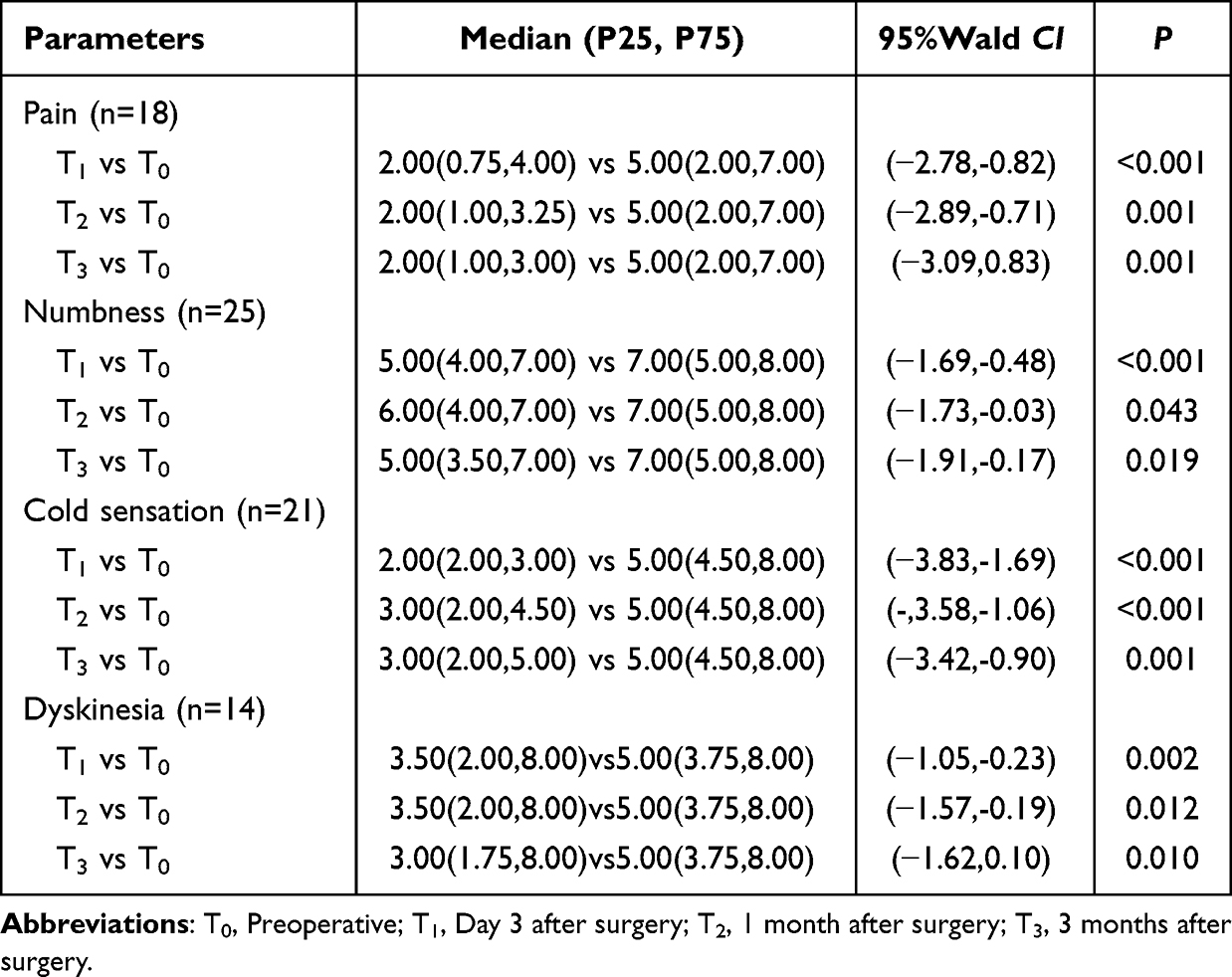 |
Table 2 Changes in NRS Scores Over Time Analyzed by Generalized Estimating Equation (GEE) |
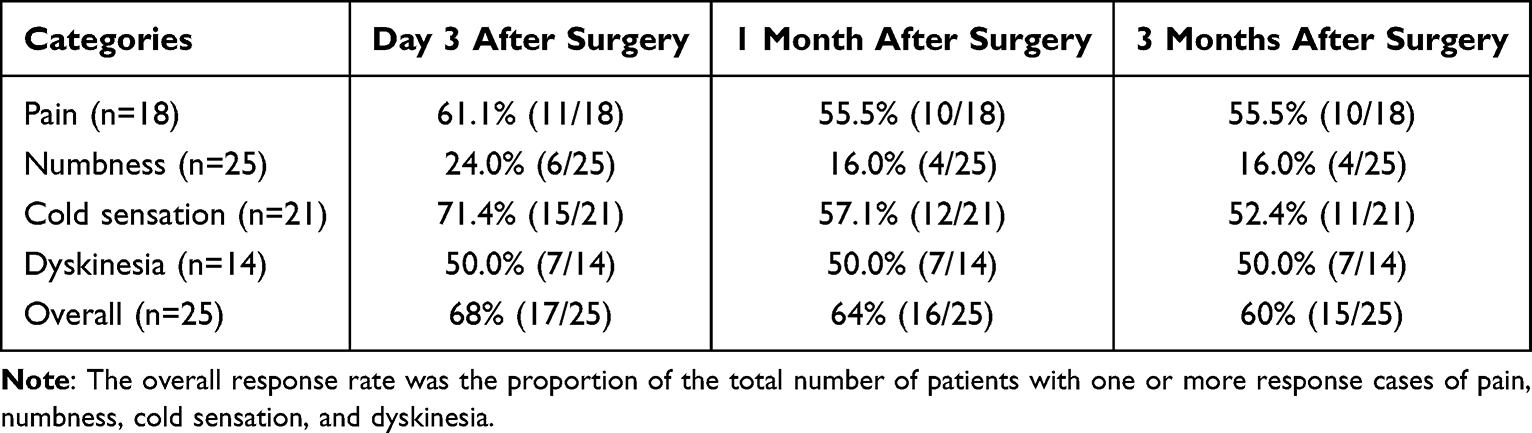 |
Table 3 Response Rates of Improvement in Pain, Numbness, Cold Sensation, Dyskinesia, and Overall (%) |
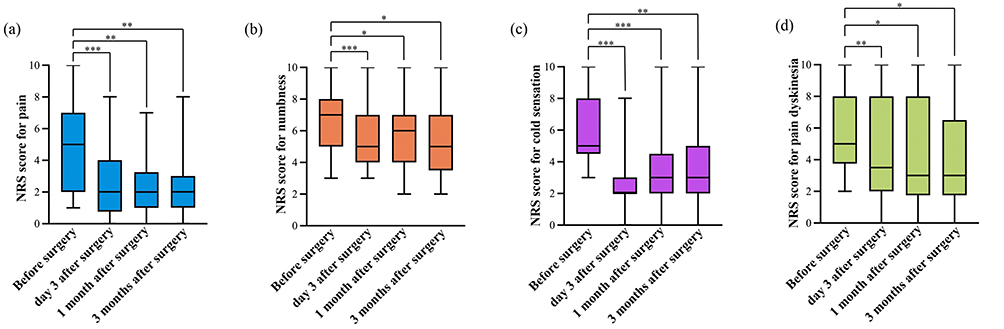 |
Figure 2 NRS scores at different moments for pain, numbness, cold sensation and dyskinesia analyzed by generalized estimating equation (GEE). (a) NRS scores for pain (n=18). (b) NRS scores for numbness (n=25). (c) NRS scores for cold sensation (n=21). (d) NRS scores for dyskinesia (n=14). Abbreviations: T0, preoperative; T1, Day 3 after surgery; T2, 1 month after surgery; T3, 3 months after surgery. Note: *P < 0.05, **P < 0.01, and ***P < 0.001. |
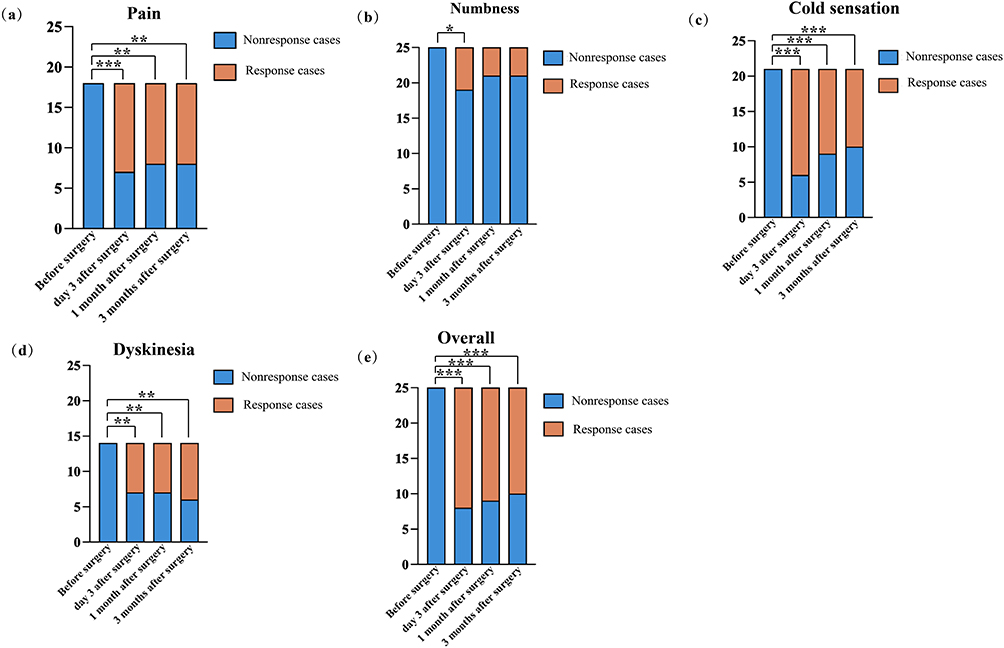 |
Figure 3 Distribution of response rates for pain, numbness, cold sensation, dyskinesia, and overall effectiveness analyzed by Fisher’s exact test. (a) Number of response cases for pain (n=18). (b) Number of response cases for numbness (n=25). (c) Number of response cases for cold sensation (n=21). (d) Number of response cases for dyskinesia (n=14). (e) Number of response cases for overall (the number of cases with at least one of the four response cases of pain, numbness, cold sensation and dyskinesia)(n=25). Abbreviations: T0, Preoperative; T1, Day 3 after surgery; T2, 1 month after surgery; T3, 3 months after surgery. Note: *P < 0.05, **P < 0.01, and ***P < 0.001. |
The median NRS pain score was significantly decreased from 5.00 (2.00, 7.00) at baseline to 2.00 (0.75, 4.00) by the third day post-operation (P < 0.001). This reduction was maintained at 2.00 (1.00, 3.25) at 1 month (P = 0.001) and 2.00 (1.00, 3.00) at 3 months (P = 0.001), demonstrating stable and long-term pain control. Among the 18 patients reporting pain symptoms, there were 11 response cases at 3 days, 10 at 1 month, and 10 at 3 months post-operation, with all improvements being statistically significant (P < 0.05). The corresponding response rates were 61.1% at 3 days, 55.5% at 1 month, and 55.5% at 3 months (Table 2 and Table 3).
Although the median NRS score for numbness was decreased from 7.00 (5.00, 8.00) at baseline to 5.00 (4.00, 7.00) by the third day post-operation (P < 0.001), the magnitude of improvement was modest and did not reach the predefined threshold for clinical significance (≥30% reduction from baseline). At 1 month, the score was slightly increased to 6.00 (4.00, 7.00) (P = 0.043), before returning to 5.00 (3.50, 7.00) at 3 months (P = 0.019). Among the 25 patients with numbness, there were 6 response cases at 3 days post-operation (P < 0.05), but only 4 cases at both 1 month and 3 months, which were not statistically significant (P > 0.05). The response rates were 24.0% at 3 days, and 16.0% at both 1 and 3 months (Table 2 and Table 3).
A significant reduction in cold sensation was observed, with the median NRS score dropping from 5.00 (4.50, 8.00) at baseline to 2.00 (2.00, 3.00) on the third day post-operation (P < 0.001), followed by 3.00 (2.00, 4.50) at 1 month (P < 0.001) and 3.00 (2.00, 5.00) at 3 months (P = 0.001). Among the 21 patients with cold sensation, 15 response cases were noted at 3 days, 12 at 1 month, and 11 at 3 months, all of which were statistically significant (P < 0.05). Response rates for cold sensation relief were 71.4% at 3 days, 57.1% at 1 month, and 52.4% at 3 months (Table 2 and Table 3).
The median NRS score for dyskinesia showed a notable improvement, decreasing from 5.00 (3.75, 8.00) at baseline to 3.50 (2.00, 8.00) on the third day post-operation (P = 0.002). This was followed by stable improvement at 1 month (3.50, P = 0.012) and a further reduction to 3.00 (1.75, 8.00) at 3 months (P = 0.010). Among the 14 patients experiencing dyskinesia, there were 7 response cases at both 3 days and 1 month, and 8 cases at 3 months, all statistically significant (P < 0.05). The response rates were 50.0% at both 3 days and 1 month, increasing to 57.1% at 3 months (Table 2 and Table 3).
There were three noteworthy cases: one involved a patient with hypertension who discontinued his medication following surgery, and the other two involved a patient with lymphedema who experienced significant reduction in edema of both lower extremities within three months. Additionally, there were two adverse effects, both of them had minor bleeding at the tip of the puncture needle. In each case, the blood loss was less than 5 mL and had no clinical impact. No other adverse effects were noted.
Discussion
In this single-center exploratory study, we found that lumbar sympathicolysis significantly alleviated symptoms associated with bilateral lower limb CIPN, without causing adverse effects such as lumbar plexus nerve injury, male ejaculatory dysfunction, or vascular embolism. Our study suggested that CT-guided lumbar sympathicolysis provided immediate and sustained relief for pain and cold sensation, and gradual improvement in dyskinesia in patients with bilateral lower limb CIPN unresponsive to drug therapy. The sustained response in pain and cold sensation may be due to the anti-inflammatory effects of local sympathectomy, which promotes vasodilation, increased blood flow, and the elimination of toxic chemotherapy byproducts.26 In contrast, the gradual improvement in dyskinesia may be related to the self-repair and regeneration of autonomic nerves and the alleviation of pain, numbness, and cold sensation, indirectly improving motor function.
While postoperative numbness were significantly improved immediately after treatment but long term effect was limited. This may be due to the non-regenerative nature of neurons and the inherent challenges in nerve repair per se.27 Despite this limitation, the procedure provided some benefit to patients with refractory CIPN, maintaining a consistent, albeit modest symptom relief.
Current approaches to CIPN management—including neuromodulation techniques such as transcutaneous electrical nerve stimulation (TENS) and spinal cord stimulation, acupuncture, and physical therapy—have demonstrated variable and often modest efficacy.15,28–30 For instance, a recent multicenter, placebo-controlled RCT of a wireless TENS device for chronic CIPN demonstrated preliminary efficacy primarily for painful symptoms (eg, burning/sharp pain and cramping), with between-group differences ranging from 1.21 to 1.37 points on a 0–10 NRS in predefined symptomatic subgroups. However, no significant effects were observed for numbness or tingling.28 In contrast, our exploratory study on CT-guided lumbar sympathicolysis demonstrated significant and sustained improvement not only in pain and cold sensation but also, to a degree, in dyskinetic symptoms. Notably, the intervention provided rapid and substantial symptom relief, with 60% of patients achieving a clinically meaningful response (≥30% NRS reduction) in at least one core symptom at three months. While direct efficacy comparisons cannot be drawn from different study designs, the magnitude, rapidity, and breadth of symptom relief observed with lumbar sympathicolysis—particularly targeting refractory, multimodal symptoms—suggest it may represent a more invasive yet potentially more targeted and effective interventional option for a specific subset of patients with severe, pharmacotherapy-resistant, lower-limb CIPN.
This study has limitations. First, the single-arm design without a control group limits causal inference. Second, no formal sample size calculation or power analysis was performed due to the exploratory nature of this first-in-kind study. Third, while a ≥30% NRS reduction defined treatment response, validated minimally important difference thresholds for numbness, cold sensation, and dyskinesia are lacking. Fourth,the small sample size and short-term follow-up warrant verification in larger, longer studies. Additionally, the reliance solely on subjective patient-reported outcomes (NRS scores) without complementary objective measures (eg, nerve conduction studies, quantitative sensory testing) limits the mechanistic insight and scientific robustness of our findings.
Conclusions
Preliminary findings suggest, CT-guided lumbar sympathicolysis may be a potentially effective and safe minimally invasive intervention for refractory lower extremity CIPN, providing significant and rapid relief for pain and cold sensation, along with gradual improvement in dyskinetic symptoms. Further clinical applications will require larger-scale and controlled trials for verification to confirm its long-term efficacy and safety.
Data Sharing Statement
The data used and analyzed during the current study are available from the corresponding author, Guanglun Xie, upon reasonable request.
Ethical Statement
The study was reviewed and approved by the Biomedical Ethics Committee of Henan Cancer Hospital (No. 2022-KY-0077-002). Written consent was obtained before participation.
Funding
This work was supported by the Science and Technology Research Project of Henan Province [grant number 242102521028].
Disclosure
Jiaojiao Suo and Fang Zhang are co-first authors for this study. The authors declare that they have no conflicts of interest for this work.
References
1. McCrary JM, Goldstein D, Boyle F. et al. Optimal clinical assessment strategies for chemotherapy-induced peripheral neuropathy (CIPN): a systematic review and Delphi survey. Support Care Cancer. 2017;25(11):3485–9. doi:10.1007/s00520-017-3772-y
2. Pachman DR, Barton DL, Watson JC, Loprinzi CL. Chemotherapy-induced peripheral neuropathy: prevention and treatment. Clin Pharmacol Ther. 2011;90(3):377–387. doi:10.1038/clpt.2011.115
3. Staff NP, Cavaletti G, Islam B, Lustberg M, Psimaras D, Tamburin S. Platinum-induced peripheral neurotoxicity: from pathogenesis to treatment. J Peripher Nerv Syst. 2019;24(Suppl 2):S26–s39. doi:10.1111/jns.12335
4. Cavaletti G, Alberti P, Argyriou AA, Lustberg M, Staff NP, Tamburin S. Chemotherapy-induced peripheral neurotoxicity: a multifaceted, still unsolved issue. J Peripher Nerv Syst. 2019;24 Suppl 2:S6-s12. doi:10.1111/jns.12337
5. Seretny M, Currie GL, Sena ES, et al. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy: a systematic review and meta-analysis. Pain. 2014;155(12):2461–2470. doi:10.1016/j.pain.2014.09.020
6. Hershman DL, Weimer LH, Wang A, et al. Association between patient reported outcomes and quantitative sensory tests for measuring long-term neurotoxicity in breast cancer survivors treated with adjuvant paclitaxel chemotherapy. Breast Cancer Res Treat. 2011;125(3):767–774. doi:10.1007/s10549-010-1278-0
7. Cavaletti G, Frigeni B, Lanzani F, et al. Chemotherapy-induced peripheral neurotoxicity assessment: a critical revision of the currently available tools. Eur J Cancer. 2010;46(3):479–494. doi:10.1016/j.ejca.2009.12.008
8. Lyman GH. Impact of chemotherapy dose intensity on cancer patient outcomes. J Natl Compr Canc Netw. 2009;7(1):99–108. doi:10.6004/jnccn.2009.0009
9. Cavaletti G, Marmiroli P. Chemotherapy-induced peripheral neurotoxicity. Nat Rev Neurol. 2010;6(12):657–666. doi:10.1038/nrneurol.2010.160
10. Desforges AD, Hebert CM, Spence AL, et al. Treatment and diagnosis of chemotherapy-induced peripheral neuropathy: an update. Biomed Pharmacother. 2022;147:112671. doi:10.1016/j.biopha.2022.112671
11. Colvin LA. Chemotherapy-induced peripheral neuropathy: where are we now? Pain. 2019;160(Suppl 1):S1–s10. doi:10.1097/j.pain.0000000000001540
12. Loprinzi CL, Lacchetti C, Bleeker J, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. J Clin Oncol. 2020;38(28):3325–3348. doi:10.1200/jco.20.01399
13. Jordan B, Margulies A, Cardoso F, et al. Systemic anticancer therapy-induced peripheral and central neurotoxicity: ESMO-EONS-EANO clinical practice guidelines for diagnosis, prevention, treatment and follow-up. Ann Oncol. 2020;31(10):1306–1319. doi:10.1016/j.annonc.2020.07.003
14. Smith EM, Pang H, Cirrincione C, et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy: a randomized clinical trial. JAMA. 2013;309(13):1359–1367. doi:10.1001/jama.2013.2813
15. Friedemann T, Kark E, Cao N, et al. Acupuncture improves chemotherapy-induced neuropathy explored by neurophysiological and clinical outcomes - The randomized, controlled, cross-over ACUCIN trial. Phytomedicine. 2022;104:154294. doi:10.1016/j.phymed.2022.154294
16. Brayall P, Donlon E, Doyle L, Leiby R, Violette K. Physical therapy–based interventions improve balance, function, symptoms, and quality of life in patients with chemotherapy-induced peripheral neuropathy: a systematic review. Rehabil Oncol. 2018;36(3):161–166. doi:10.1097/01.Reo.0000000000000111
17. Prinsloo S, Novy D, Driver L, et al. Randomized controlled trial of neurofeedback on chemotherapy-induced peripheral neuropathy: a pilot study. Cancer. 2017;123(11):1989–1997. doi:10.1002/cncr.30649
18. Burbelko M, Wagner HJ, Gutberlet M, Grothoff M. [Image-guided pain therapy Sympathicolysis]. Radiologe. 2015;55(6):462–469. doi:10.1007/s00117-014-2802-8
19. Scheer F, Wiggermann P, Kamusella P, Wissgott C, Andresen R. CT-assisted sympathicolysis as an additional minimally invasive therapeutic option in primary focal plantar hyperhidrosis. Cardiovasc Intervent Radiol. 2014;37(6):1554–1558. doi:10.1007/s00270-013-0824-7
20. Abramov R. Lumbar sympathetic treatment in the management of lower limb pain. Curr Pain Headache Rep. 2014;18(4):403. doi:10.1007/s11916-014-0403-x
21. Bombor I, Wissgott C, Andresen R. Lumbar sympathicolysis in patients with severe peripheral artery disease: hemodynamics of the lower limbs determined by near-infrared spectroscopy, color coded duplex sonography, and temperature measurement. Clin Med Insights Cardiol. 2014;8(Suppl 2):29–36. doi:10.4137/cmc.S15233
22. Phuphanich ME, Convery QW, Nanda U, Pangarkar S. Sympathetic blocks for sympathetic pain. Phys Med Rehabil Clin North America. 2022;33(2):455–474. doi:10.1016/j.pmr.2022.02.002
23. Argyriou AA, Bruna J, Marmiroli P, Cavaletti G. Chemotherapy-induced peripheral neurotoxicity (CIPN): an update. Crit Rev Oncol Hematol. 2012;82(1):51–77. doi:10.1016/j.critrevonc.2011.04.012
24. Starobova H, Vetter I. Pathophysiology of chemotherapy-induced peripheral neuropathy. Front Mol Neurosci. 2017;10:174. doi:10.3389/fnmol.2017.00174
25. Bouhassira D, Attal N, Fermanian J, et al. Development and validation of the neuropathic pain symptom inventory. Pain. 2004;108(3):248–257. doi:10.1016/j.pain.2003.12.024
26. Krumova EK, Gussone C, Regeniter S, Westermann A, Zenz M, Maier C. Are sympathetic blocks useful for diagnostic purposes? Reg Anesth Pain Med. 2011;36(6):560–567. doi:10.1097/AAP.0b013e318229bbee
27. Staff NP, Grisold A, Grisold W, Windebank AJ. Chemotherapy‐induced peripheral neuropathy: a current review. Ann Neurol. 2017;81(6):772–781. doi:10.1002/ana.24951
28. Gewandter JS, Culakova E, Davis JN, et al. Wireless transcutaneous electrical nerve stimulation (TENS) for chronic chemotherapy-induced peripheral neuropathy (CIPN): a proof-of-concept randomized clinical trial. J Pain. 2024;25(5):104431. doi:10.1016/j.jpain.2023.11.014
29. Tamburin S, Park SB, Schenone A, et al. Rehabilitation, exercise, and related non-pharmacological interventions for chemotherapy-induced peripheral neurotoxicity: systematic review and evidence-based recommendations. Crit Rev Oncol Hematol. 2022;171:103575. doi:10.1016/j.critrevonc.2021.103575
30. Vu PD, McDonough KE, Dougherty PM, D’Souza RS, Javed S. Psychophysical and functional outcomes in chemotherapy-induced peripheral neuropathy after spinal cord stimulation: a narrative review and case series. Neuromodulation. 2024;27(8):1305–1320. doi:10.1016/j.neurom.2024.06.006
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.