")
Back to Journals » International Journal of General Medicine » Volume 15
Lower Plasma Albumin, Higher White Blood Cell Count and High-Sensitivity C-Reactive Protein are Associated with Femoral Artery Intima-Media Thickness Among Newly Diagnosed Patients with Type 2 Diabetes Mellitus
Authors Phi Thi Nguyen N, Luong Cong T, Tran TTH , Nhu Do B , Tien Nguyen S , Thanh Vu B, Ho Thi Nguyen L, Van Ngo M, Trung Dinh H , Duong Huy H , Xuan Vu N , Nguyen Trung K , Ngoc Vu D, The Pham N, Dinh Le T
Received 10 December 2021
Accepted for publication 22 February 2022
Published 8 March 2022 Volume 2022:15 Pages 2715—2725
DOI https://doi.org/10.2147/IJGM.S351342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Nga Phi Thi Nguyen,1,2,* Thuc Luong Cong,3,4,* Thi Thanh Hoa Tran,5 Binh Nhu Do,6 Son Tien Nguyen,1,2 Binh Thanh Vu,7,* Lan Ho Thi Nguyen,8 Manh Van Ngo,9 Hoa Trung Dinh,10 Hoang Duong Huy,11 Nghia Xuan Vu,12 Kien Nguyen Trung,13 Duong Ngoc Vu,14 Nghia The Pham,14 Tuan Dinh Le2,15,*
1Department of Endocrinology, Military Hospital 103, Hanoi, Vietnam; 2Department of Rheumatology and Endocrinology, Vietnam Military Medical University, Hanoi, Vietnam; 3Cardiovascular Center, Military Hospital 103, Hanoi, Vietnam; 4Department of Cardiology, Vietnam Military Medical University, Hanoi, Vietnam; 5Emergency Resuscitation Department, National Hospital of Endocrinology, Hanoi, Vietnam; 6Division of Military Science, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 7Department of Internal Medicine, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 8Department of General Internal Medicine, National Hospital of Endocrinology, Hanoi, Vietnam; 9Postgraduate Training Management Department, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 10Department of Requested Treatment, National Hospital of Endocrinology, Hanoi, Vietnam; 11Department of Neurology, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 12Department of Blood Transfusion, 108 Military Central Hospital, Hanoi, Vietnam; 13Department of Science Management, Thai Binh University of Medicine and Pharmacy, Thai Binh, Vietnam; 14Department of Imaging Diagnosis, Hanoi Medical University, Hanoi, Vietnam; 15Center of Emergency, Critical Care Medicine and Clinical Toxicology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Tuan Dinh Le, Center of Emergency, Critical Care Medicine and Clinical Toxicology, Military Hospital 103, Vietnam Military Medical University, 261 Phung Hung Street, Phuc La Ward, Ha Dong District, Hanoi, Vietnam, Tel +84 388166078, Email [email protected] Binh Thanh Vu, Department of Internal Medicine, Thai Binh University of Medicine and Pharmacy, 373 Ly Bon Street, Ky Ba Ward, Thai Binh, Vietnam, Tel +84 334588298, Email [email protected]
Introduction: Low albumin levels, high levels of high-sensitivity C-reactive protein (hs-CRP), and high white blood cell count were risk factors for changes in arterial intima-media thickness (IMT). Femoral artery IMT damages were one of the common peripheral artery type 2 diabetes. This study was conducted to determine the association between femoral artery IMT and plasma albumin, hs-CRP levels, and white blood cell count in newly diagnosed patients with type 2 diabetes mellitus (nT2D).
Materials and Methods: From January 2015 to May 2020, 306 patients with nT2D were recruited for this cross-sectional descriptive study at Vietnam’s National Endocrinology Hospital. We measured IMT by Doppler ultrasound.
Results: There was a statistically significant difference in albumin, hs-CRP levels, hs-CRP-to-albumin ratio, and white blood cell counts between three different IMT groups namely normal IMT, thick IMT, and atherosclerosis (p = 0.003, p = 0.001, p = 0.001 and p = 0.049, respectively). In the multivariate linear regression analysis, white blood cell count, and hs-CRP levels showed a significantly positive correlation to IMT (standardized B and p of 0.17, 0.015 and 0.163, 0.024, respectively), but albumin levels were a significantly negative correlation to IMT (standardized B = – 0.151, p = 0.029). The multivariate logistic regression analysis showed that albumin (OR = 0.79, 95% CI 0.65– 0.90, p = 0.018), hs-CRP (OR = 1.09, 95% CI 1.01– 1.18, p = 0.026), and white blood cell count (OR = 1.36, 95% CI 1.03– 1.81, p = 0.033) had correlation to atherosclerosis of femoral artery.
Conclusion: Reduced plasma albumin, elevated hs-CRP, and white blood cell count associated with IMT increased the odds for atherosclerosis of femoral artery among nT2D.
Keywords: plasma albumin, high-sensitivity C-reactive protein, white blood cell count, newly diagnosed type 2 diabetes mellitus, intima-media thickness, atherosclerotic plaque, femoral artery
Introduction
The number of diabetes has been rising rapidly in the world. As of 2019, 79% of adults with diabetes were living in low- and middle-income countries.1,2 Macro- and micro-vascular complications due to prediabetes or diabetes increase the burden on the healthcare system and society, also reduce the patient’s quality of life in these countries.3–6 Peripheral arterial disease is a major macrovascular complication of type 2 diabetes that can lead to limb amputation and enhance the risk of morbidity and mortality in diabetic patients.7–9
Common femoral arterial damages are one of the peripheral arterial diseases, with endothelium dysfunction, thick intima-media, and atherosclerosis.7 Recently, researchers have turned their focus on the potential role of the femoral arterial IMT in evaluating cardiovascular complications in diabetic patients.10–12 It is indisputable that cardiovascular risk factors (for example, age, duration of type 2 diabetes, smoking, hypertension, hyperglycemia, dyslipidemia, overweight, and obesity) in diabetic patients promote endothelium dysfunction and atherosclerosis of femoral arteries.7,11 Diabetes enhances the risk of inflammation via increases in hs-CRP, interleukin (such as interleukin-4,6,8,17), tumor necrosis factor-alpha, platelet adhesion and aggregation, and coagulation disorders, which contributes to developing endothelium dysfunction.7,13,14 Recent studies have demonstrated hypoalbuminemia and an increase in inflammatory factors such as hs-CRP and white blood cell count are the main factors for endothelium dysfunction and atherosclerosis in diabetic patients.15–18 Plasma albumin protects against endothelial dysfunction via immunomodulatory and antioxidant function.19 High-sensitive CRP and white blood cell count have contradictory pro-angiogenic, anti-angiogenic effects, and inhibit nitric oxide synthase determining tissue remodeling in the atherosclerotic plaque.20,21 Besides, the hs-CRP-to-albumin ratio is a new marker to predict inflammatory events, with increased hs-CRP-to-albumin ratio playing a role in the pathogenesis of coronary slow flow, coronary artery disease.22,23
Whilst there are many patients with clinically femoral arterial atherosclerosis, there are few studies on femoral arterial IMT among patients with type 2 diabetes mellitus. Vietnam is one of the developing countries, the number of nT2D and vascular complications has increased rapidly. Nevertheless, there is a lack of studies on the role of plasma albumin, hs-CRP levels, and white blood cell count in femoral artery lesions. This study was conducted to investigate the association between femoral arterial IMT and plasma albumin, hs-CRP, and white blood cell count in nT2D.
Materials and Methods
Study Population and Design
A cross-sectional descriptive study was conducted on 306 patients with nT2D in the National Endocrinology Hospital (Hanoi, Vietnam) from January 2015 to December 2020. All participants provided written informed consents. The diagnosis of type 2 diabetes mellitus was based on the American Diabetes Association guideline (2019)24 for the first time on examination day to minimize other treatment-related factors such as acarbose, miglitol, metformin, insulin therapy. Exclusion criteria included patients that suffered from severe chronic liver failure (cirrhosis or acute liver failure), heart failure (with a mid-range and reduced ejection fraction [EF] <50%), or kidney failure (with estimated glomerular filtration rate estimation [eGFR] <45 [mL/min]), hemodynamic diseases (aplastic anemia, moderate-to-severe anemia, and hemolytic anemia), systemic diseases (systemic lupus erythematosus, and peripheral arterial occlusive diseases), infections, and critical diabetic conditions (hyperosmolarity, diabetic ketoacidosis, and hypoglycemia), and who were undergoing anticoagulant treatment from the study (sintrom, aspirin, clopidogrel, and heparin).
The sample size (n) of 306 patients with nT2DM was calculated based on Cochran’s formula used for qualitative analysis in descriptive and analytical research as follows n = [Z2(1-α/2) x p(1 – p)]/∆2, where p = 0.228 is the rate of increased aortic-IMT in adult diabetes mellitus patients,25 Z2(1-α/2) = 1.96 is the value corresponding to α = 0.05 and ∆ is the desired deviation between the rate obtained from our study sample and p of 0.228 of the previous study population. In our study, ∆ = 0.05. In order to avoid potential loss of data, we decided to include 10% more patients in our study population.
Clinical and Biochemical Assessments
All patients were questioned about their comorbid conditions and medication consumption histories. Anthropometric measurements and clinical examination were collected, with drinking, smoking history, age, gender, height, weight, waist and hip circumference, waist-to-hip ratio (WHR), body mass index (BMI), pulses, systolic blood pressure (SBP), and diastolic blood pressure (DBP).
Blood samples were taken on the morning of clinical examination day after a fast of at least 8 hours. Blood lipid profiles (total cholesterol, high-density lipoprotein [HDL-C], and triglyceride), aspartate transferase (AST), alanine transferase (ALT), creatinine, electrolytes, albumin, and hs-CRP were measured by the enzyme colorimetric method (Beckman AU680, USA). Low-density lipoprotein (LDL-C) was calculated by Friedewald formula (all variables in mmol/L) as follow:

Chemiluminescent enzyme immunoassays for the measurement of C-peptide and insulin (COBAS E411, USA). HbA1c was measured by high-performance liquid chromatography (Adams A1C, Japan), Quantification of fasting glucagon-like peptide-1 (fGLP-1) levels by enzyme-linked immunosorbent assay (Human ELISA GLP-1 kits, IBL, Japan, #27784). We used the hexokinase methods (Beckman AU680, USA) to measure fasting plasma glucose (FPG) and two-hour postprandial glucose (2h-PPG) and enzymatic turbidimeter autoanalyzer (Beckman AU680, USA) to measure urine albumin levels in a 24-hour urine sample (24hUA). The white blood cell was counted using K-4500, Japan. Evaluation of eGFR by Cockcroft-Gault’s formula from serum creatinine (Scr) in adult males (15% less in females)26 as follow:

Bilateral Femoral Arteries Findings by Ultrasonography
Patients were guided to lay in the supine position with flexible lower extremities. Under the standardized protocol for ultrasound in Vietnam, experienced ultrasound practitioners investigated femoral arteries from the inguinal ligament position downwardly to common femoral arteries to the bifurcation of the femoral artery into the subsartorial artery and the deep femoral artery by Philip HD 11 XE Color Doppler apparatus using a linear transducer (frequency of 7.5 MHz). Colored Doppler and continuous Doppler modes were employed to investigate the morphology and functions of arteries. The position for evaluating IMT (mm) was at the distal walls of femoral arteries which were 2 cm from the bifurcation of the femoral artery into subsartorial artery and deep femoral artery.27 Following Pignoli’s method,28 the IMT measurements were performed at both femoral arteries and the highest IMT was reported as an IMT variable for each patient, and then classified into 3 categories, namely normal IMT (less than 1 mm), thick IMT (1 ≤ IMT < 1.5 mm), and atherosclerosis (IMT ≥ 1.5 mm).29,30
Ethical Statement
All participants provided written informed consents and agreed to join our study; and the protocol was approved by the Ethical Review Committee of Vietnam Military Medical University, Vietnam (Reference No 168/2014/IRB-VMMU). The study was also conducted using good clinical practice following the Declaration of Helsinki.
Statistical Analysis
Data were expressed as mean ± standard deviation or median (interquartile range, Q1-Q3). Differences between groups were examined with either Student’s t-test or Mann–Whitney test. Correlations between plasma albumin, hs-CRP levels, white blood cell count, and other variables were evaluated with Pearson’s and Spearman correlation analysis, respectively. The Chi-square test of association is used to discover if there is a relationship between two categorical variables. Kruskal–Wallis H-tests with Dunn’s pairwise post hoc tests were used to analyze the differences in plasma albumin, hs-CRP levels, white blood cell count between groups of IMT. Multivariate linear regression was employed to analyze the effects of plasma albumin, hs-CRP levels, white blood cell count, and other related factors and IMT. The VIF value < 10 was defined as no collinear for each variable in the multivariate regression. Multivariate logistic regression analysis was used to analyze the effects of related factors and abnormal IMT and atherosclerosis of the femoral artery. Due to the fact that age, BMI, blood pressure, FPG, lipid profiles, eGFR, urine protein, C-peptide, red blood cells, and potassium related to the development of abnormalities in IMT, we considered these variables as confounders and to be adjusted for multivariate regression analyses between plasma albumin, hs-CRP levels, white blood cell counts and IMT. A p-value <0.05 was defined as statistically significant. Data were analyzed with the SPSS version 26 (SPSS Inc, Chicago, IL).
Results
Demographic and Biomedical Findings
Age, insulin, C-peptide levels, and platelet count at the time of diagnosing in women patients were higher than those in men. Male patients had higher waist circumference, WHR, femoral arterial IMT, FPG, triglyceride, creatinine, red blood cell count, hemoglobin, 24hUA, and eGFR than female patients. There was no significant difference in hip circumference, BMI, SBP, DBP, 2hr-PPG, HbA1c, fGLP-1, total cholesterol, HDL-C, LDL-C, AST, ALT, hs-CRP, potassium ion, and white blood cell count between male and female patients (Table 1).
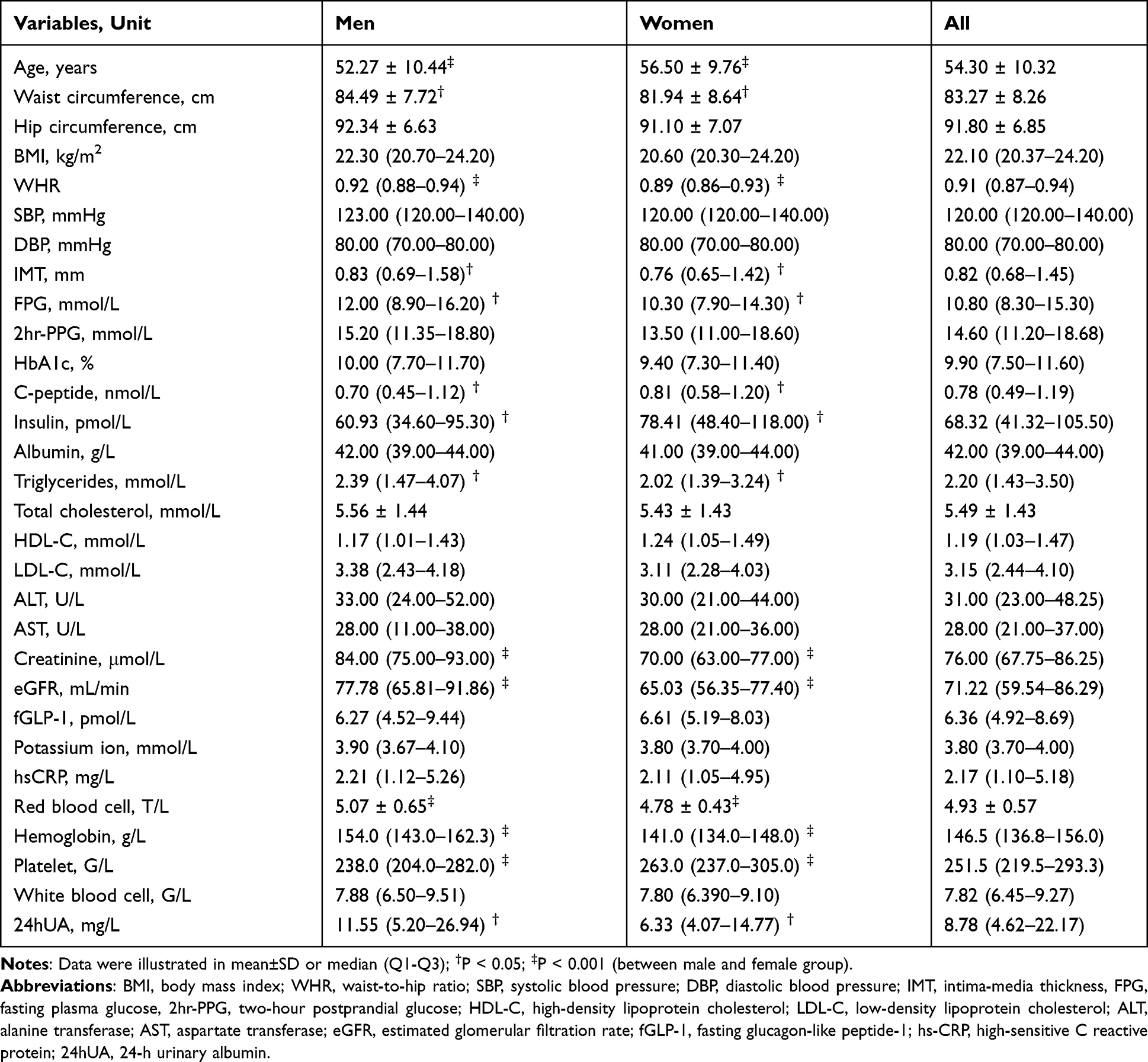 |
Table 1 The Demographic and Biomedical Characteristics of the Study Population |
A Kruskal–Wallis H-tests showed that there was a significant difference in albumin, hs-CRP levels, hs-CRP-to-albumin ratio, and white blood cell count between the different IMT groups (χ2(2) = 11.703, p = 0.003; χ2(2) = 13.511, p = 0.001; χ2(2) = 15.059, p = 0.001; and χ2(2) = 6.047, p = 0.049, respectively). Dunn’s pairwise tests were carried out for the three pairs of groups (normal, thick IMT and atherosclerosis). Mainly, there was strong evidence (p <0.01, adjusted using Bonferroni corrections) of a difference in albumin and hs-CRP levels between normal IMT and both thick IMT and atherosclerosis group in male patients and in overall (χ2(2) = 7.951, p = 0.019 and χ2(2) = 10.828; p = 0.004, respectively) (Table 2).
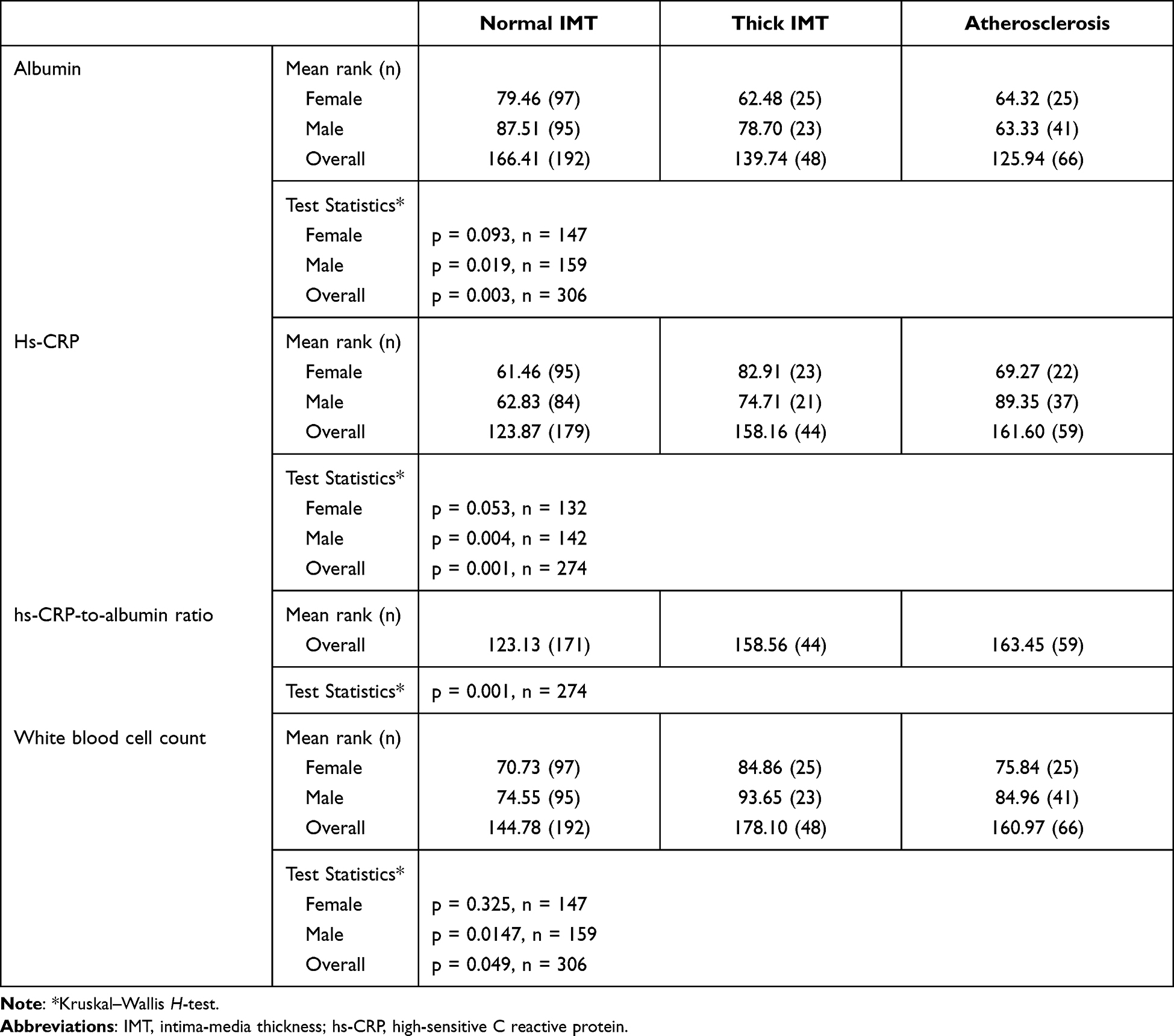 |
Table 2 The Relationship Between Plasma Albumin, Hs-CRP Levels, Hs-CRP-to-Albumin Ratio and White Blood Cell Count and Femoral Arterial Intima-Media Thickness Stratified by Gender and Overall |
In the univariate linear regression analysis, femoral arterial IMT significantly correlated to age, waist circumference, WHR, total cholesterol, SBP, DBP, fGLP-1, albumin, hs-CRP, eGFR, and 24hUA. After adjusting for other related factors (namely, waist circumference, WHR, fGLP-1), while age, SBP, hs-CRP, white blood cell count, and potassium ion showed a significantly positive correlation with IMT (Standardized B and p of 0.311, 0.000; 0.275, 0.002; 0.163, 0.024; 0.170, 0.015 and 0.131, 0.042, respectively), albumin levels showed a significant inverse correlation with IMT (standardized B = –0.151 and p = 0.029) (Table 3).
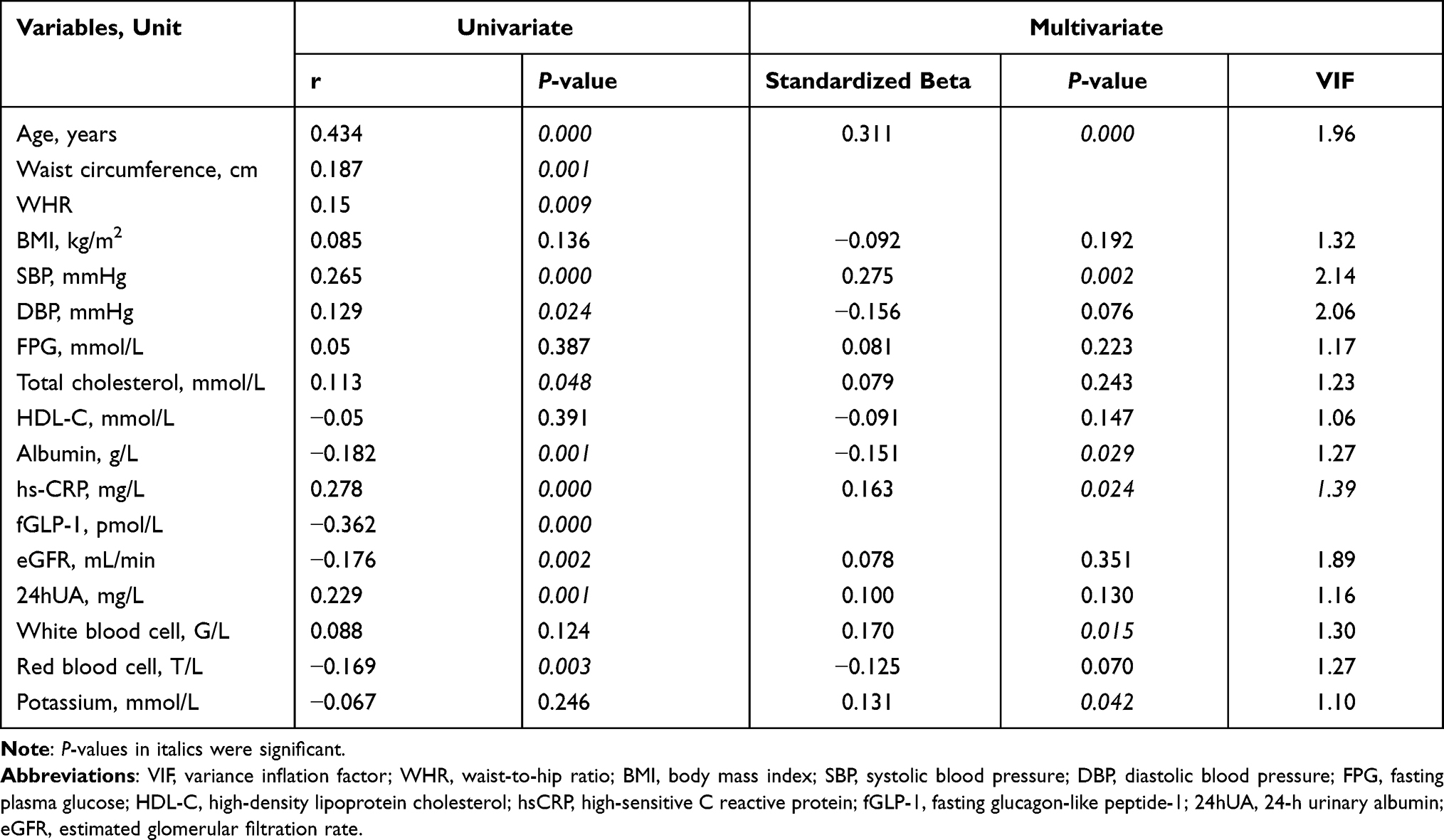 |
Table 3 Univariate and Multivariate Linear Regression Analysis: Standardized Beta Coefficients of Independent Variables and Femoral Intimal Media Thickness |
The multivariate logistic regression analysis showed that the following factors correlated to abnormal femoral arterial IMT (including in thick IMT and atherosclerosis) in nT2D: albumin (OR = 0.84, 95% CI 0.71–0.98, p = 0.028), hs-CRP (OR = 1.08, 95% CI 1.01–1.16, p = 0.036), white blood cell count (OR = 1.44, 95% CI 1.13–1.83, p = 0.003), SBP (OR = 1.07, 95% CI 1.02–1.13, p = 0.007), and DBP (OR = 0.92, 95% CI 0.85–0.99, p = 0.036). Albumin, hs-CRP and white blood cell count correlated to atherosclerosis (OR = 0.79, 95% CI 0.65–0.96, p = 0.018; OR = 1.09, 95% CI 1.01–1.18, p = 0.026; OR = 1.36, 95% CI 1.03–1.81, p = 0.033, respectively) (Table 4).
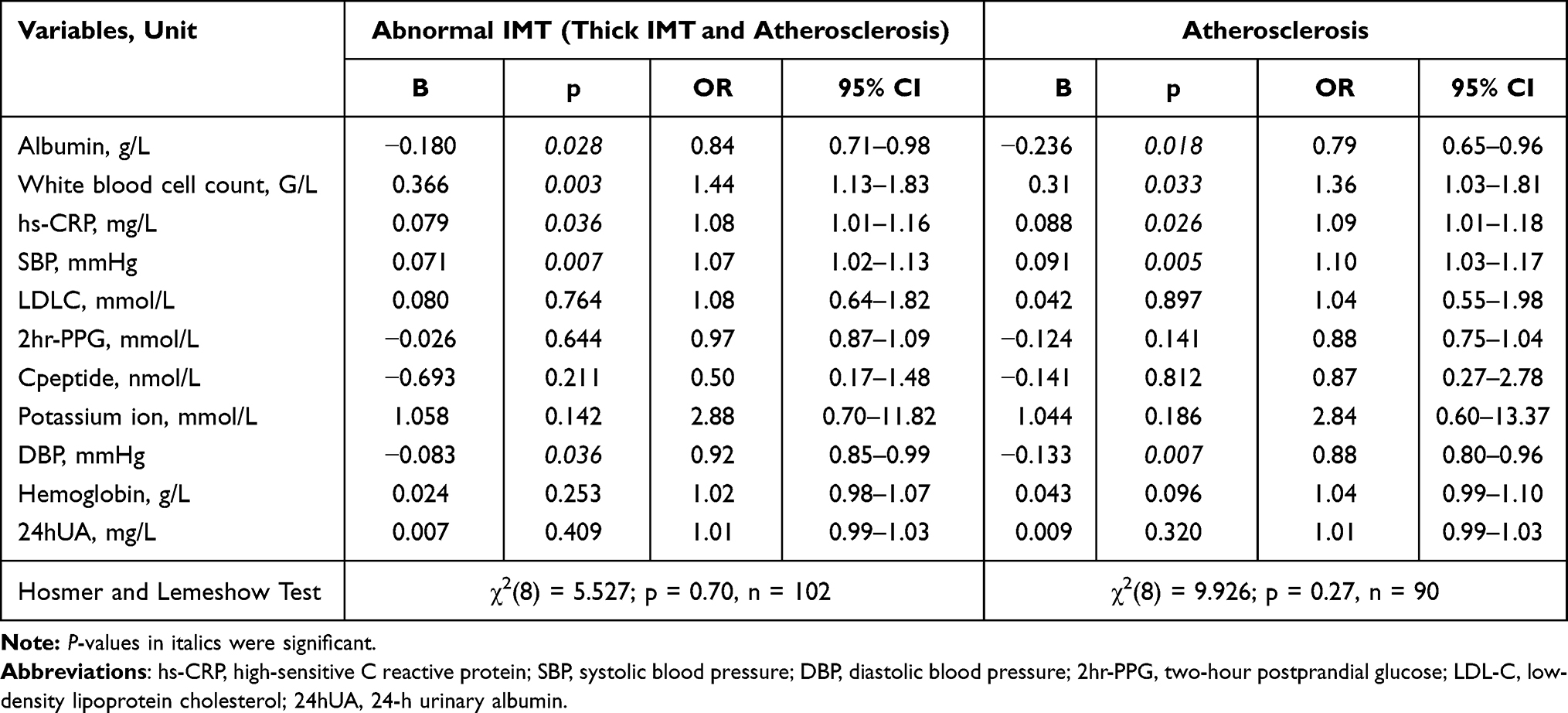 |
Table 4 The Multivariate Logistic Regression Analysis Associated Other Factors with Abnormal IMT and Atherosclerosis of Femoral Artery |
Discussion
The Relation Between Femoral Arterial IMT and Plasma Albumin Levels
This study showed that there was a significant difference in albumin levels among different femoral arterial IMT groups (i.e, normal IMT, thick IMT, and atherosclerosis). In the multivariate linear regression analysis, albumin levels showed an inverse correlation with IMT. The multivariate logistic regression analysis showed that albumin was correlated to thick IMT of the femoral artery in nT2D (OR = 0.84, p = 0.028).
Albumin is the most important plasma protein with many biological functions, including maintenance of colloidal osmotic pressure, binding of endo- and exo-genous substances, and antithrombotic effects.31 Serum albumin concentrations have also been proved to be inversely associated with various type 2 diabetes risk variables including age, BMI, and insulin resistance.32–34 Lower serum albumin levels are associated with an increased risk of cardiovascular diseases such as coronary heart disease, ischemic heart disease, cardiovascular mortality, and carotid atherosclerosis.15,35,36 The antioxidant and anti-inflammatory properties of albumin in the atherogenic process have been hypothesized as possible mechanisms for this inverse association.37,38
In this study, although there was no difference in albumin concentration between men and women, albumin concentration was statistically low in males with thickened IMT or atherogenesis of femoral artery, but no difference in females. Moreover, men’s IMT was significantly higher than that in women, so the proportion of men with IMT thickness or atherogenesis was higher than women. Besides, reduced plasma albumin is a risk factor for type 2 diabetes,39 and endothelial dysfunction.40 At the same time, men have more cardiovascular risk factors and a higher risk of peripheral artery disease than women due to harmful habits, namely smoking, drinking alcohol, metabolic disorders, hypertension, and hypercholesterolemia.41,42
The Relation Between Femoral Arterial IMT and Plasma Hs-CRP Levels
High-sensitive CRP, an acute phase of the inflammatory marker, might relate to an increased risk of cardiovascular diseases and incident metabolic syndrome.13,43,44 High-sensitive CRP could reduce nitric oxide (NO) bioavailability, which induces endothelial and cardiovascular dysfunctions.45,46 In our study, there was a significant difference in hs-CRP levels among different IMT groups. An increase in hs-CRP levels significantly correlated to thickened IMT of the femoral artery. Studies have shown that hs-CRP is associated with peripheral arterial disease in patients with type 2 diabetes. Serum hs-CRP seems to be associated with a low ankle-brachial pressure index (ABPI <0.9).47 High-sensitive CRP is also produced at the area of atherosclerotic plaques of lower limb arteries.48 Moreover, a positive association has been reported between hs-CRP levels and direct risk factors for atherosclerosis such as age, smoking, body mass, total cholesterol, lipoprotein a, fibrinogen and homocysteine.49 Secreted frizzled-related protein (SFRP-5) which appears to be an anti-inflammatory adipokine and a modulator of metabolic dysfunction contributes to preventing obesity, insulin resistance, cardiovascular disease, and diabetes mellitus.50,51 Other studies showed that the association between a low level of SFPR5 and an increase in hs-CRP are independent biomarkers for risk stratification in heart failure in patients with T2DM.52,53
This study showed that hs-CRP levels increased significantly in male patients with thickened femoral arterial IMT or atherosclerosis, similar to the data of albumin level. The ratio between hs-CRP and albumin was high in the thickened IMT and atherosclerosis compared with normal IMT. This correlation suggests that a decrease in albumin levels and an increase in hs-CRP play an important role in endothelial dysfunction and atherosclerosis. In patients with type 2 diabetes, serum hs-CRP/albumin ratio was significantly higher in complicated diabetic patients compared with the control group.7 Another study showed that the hs-CRP/albumin ratio is useful to evaluate prognosis and mortality in many diseases.54 Additionally, the hs-CRP-to-albumin ratio was associated with all-cause in-hospital mortality among patients older than 65 years55 and played a role in the pathogenesis of slow coronary flow.22
The Relation Between Femoral Arterial IMT and White Blood Cell Count
White blood cell count, a routinely available marker of inflammation, is associated with macro- and microvascular complications56 and is known to be involved in vascular damage and atherosclerosis,57,58 mediated the association between increased arterial stiffness and risk of type 2 diabetes mellitus.18 In our study, there was a significant difference in white blood cell count among different IMT groups, and the increase in white blood cell count significantly correlated with IMT and thickened femoral arterial IMT. However, there was no significant difference between men and women. Another study showed that impaired endothelium-dependent dilation was associated with increased numbers of neutrophils, eosinophils, and monocytes mediated by the decreased response to NO and myeloperoxidase-associated reductions in tetrahydrobiopterin and NO bioavailability.59 White blood cell, neutrophil, and eosinophil count are the independent predictors of increased cardiovascular risk in the adolescent population.60 White blood cell count is linked to carotid and femoral atherosclerosis.61
The present study showed that, in the univariate linear regression analysis, the femoral arterial IMT positively correlated to hs-CRP levels and white blood cell count, and negatively correlated to albumin levels. In the multivariate logistic regression analysis, these factors also correlated to abnormal femoral arterial IMT (including thick IMT and atherosclerosis) and atherosclerosis in nT2D. Inflammatory biomarkers such as higher concentrations of hs-CRP, higher white blood cell count and lower serum albumin levels are associated with weight gain, increasing body fat,62,63 and increased risk of cardiovascular disease.10,33 Specifically, high hs-CRP level and white blood cell count, and low serum albumin level are independent risk factors for endothelial dysfunction and cardiovascular disease.33 Since higher concentrations of hs-CRP, higher white blood cell count, and lower serum albumin levels could predict changes in arterial IMT and atherosclerosis.
This study has limitations. This study was just an observational and cross-sectional design since causality can not be confirmed. Moreover, we did not measure the thickness of the femoral artery wall, albumin levels, hs-CRP levels, and white blood cell count in the control group.
Conclusion
In conclusion, there was a significant difference in albumin, hs-CRP levels, hs-CRP-to-albumin ratio, and white blood cell count between the different femoral arterial IMT groups (namely normal IMT, thick IMT, and atherosclerosis) and these factors correlated to IMT of the femoral artery. Reduced plasma albumin, high hs-CRP, and elevated white blood cell count increased the odds for atherosclerosis of the femoral artery.
Abbreviations
hs-CRP, high-sensitivity C-reactive protein; IMT, intima-media thickness; nT2D, newly-diagnosed type 2 diabetes mellitus; WHR, waist-to-hip ratio; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; FPG, fasting plasma glucose; 2h-PPG, two-hour postprandial glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; fGLP-1, fasting glucagon-like peptide-1; AST, aspartate transferase; ALT, alanine transferase; 24hUA, 24-h urinary albumin; eGFR, estimated glomerular filtration rate; OR, odds ratio; CI, confidence interval; SD, standard deviation; VIF, variance inflation factor.
Acknowledgments
We thank all the staff in Outpatients Department of the Vietnam Endocrinology Hospital and Director Board of Military Hospital 103 for supporting the study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, or publication of this article.
Disclosure
The authors declared no conflicts of interest for this work and no potential conflicts of interest with respect to the research, authorship, or publication of this article.
References
1. Saeedi P, Petersohn I, Salpea P, et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res Clin Pract. 2019;157:107843. doi:10.1016/j.diabres.2019.107843
2. International Diabetes Federation. IDF Diabetes Atlas.
3. De visser CL, Bilo HJG, Groenier KH, De visser W, Jong Meyboom-de B. The influence of cardiovascular disease on quality of life in type 2 diabetics. Qual Life Res. 2002;11(3):249–261. doi:10.1023/a:1015287825660
4. Pinchevsky Y, Butkow N, Raal FJ, Chirwa T, Rothberg A. Demographic and clinical factors associated with development of type 2 diabetes: a review of the literature. Int J Gen Med. 2020;13:121–129. doi:10.2147/IJGM.S226010
5. Cai X, Zhang Y, Li M, et al. Association between prediabetes and risk of all cause mortality and cardiovascular disease: updated meta-analysis. BMJ. 2020;370:m2297. doi:10.1136/bmj.m2297
6. Cai X, Liu X, Sun L, et al. Prediabetes and the risk of heart failure: a meta-analysis. Diabetes Obes Metab. 2021;23(8):1746–1753. doi:10.1111/dom.14388
7. American Diabetes Association. Peripheral arterial disease in people with diabetes. Diabetes Care. 2003;26(12):3333–3341. doi:10.2337/diacare.26.12.3333
8. Wang Z, Chen Y, Lv S, et al. Predictive value of limb artery indices and endothelial functional tests for the degree of coronary artery stenosis in a diabetic population. Int J Gen Med. 2021;14:2343–2349. doi:10.2147/IJGM.S316297
9. Mufti Alsadiqi AI, Subki AH, Abushanab RH, et al. Peripheral artery disease risk factors in Jeddah, Saudi Arabia: a retrospective study. Int J Gen Med. 2019;12:49–54. doi:10.2147/IJGM.S176451
10. Temelkova-Kurktschiev T, Koehler C, Henkel E, Hanefeld M. Leukocyte count and fibrinogen are associated with carotid and femoral intima-media thickness in a risk population for diabetes. Cardiovasc Res. 2002;56(2):277–283. doi:10.1016/S0008-6363(02)00547-3
11. Jeremiás Z, Makó K, Bogdan A, Miu I, Șerdean A, Benedek T. Femoral intima-media thickness, risk factors, and markers of inflammation in cardiovascular disease. J Interdiscip Med. 2018;3(3):141–151. doi:10.2478/jim-2018-0032
12. Nativel M, Potier L, Alexandre L, et al. Lower extremity arterial disease in patients with diabetes: a contemporary narrative review. Cardiovasc Diabetol. 2018;17(1):138. doi:10.1186/s12933-018-0781-1
13. Dregan A, Charlton J, Chowienczyk P, Gulliford MC. Chronic inflammatory disorders and risk of type 2 diabetes mellitus, coronary heart disease, and stroke. Circulation. 2014;130(10):837–844. doi:10.1161/CIRCULATIONAHA.114.009990
14. Li X, Su T, Xiao H, et al. Association of the HDL-c Level with HsCRP, IL-6, U-NAG, RBP and Cys-C in Type 2 diabetes mellitus, hypertension, and chronic kidney disease: an epidemiological survey. Diabetes, Metab Syndr Obes Targets Ther. 2020;13:3645–3654. doi:10.2147/DMSO.S265735
15. Folsom AR, Ma J, Eckfeldt JH, et al. Low serum albumin☆Association with diabetes mellitus and other cardiovascular risk factors but not with prevalent cardiovascular disease or carotid artery intima-media thickness. Ann Epidemiol. 1995;5(3):186–191. doi:10.1016/1047-2797(94)00105-3
16. Vainas T, Stassen FRM, de Graaf R, et al. C-reactive protein in peripheral arterial disease: relation to severity of the disease and to future cardiovascular events. J Vasc Surg. 2005;42(2):243–251. doi:10.1016/j.jvs.2005.03.060
17. Bayrak M. Predictive value of C-Reactive Protein/Albumin ratio in patients with chronic complicated diabetes mellitus. Pakistan J Med Sci. 2019;35(6). doi:10.12669/pjms.35.6.618
18. Liu Y, Lai X, Guo W, et al. Total white blood cell count mediated the association between increased arterial stiffness and risk of type 2 diabetes mellitus in Chinese adults. Arterioscler Thromb Vasc Biol. 2020;40(4):1009–1015. doi:10.1161/ATVBAHA.119.313880
19. Garcia-Martinez R, Andreola F, Mehta G, et al. Immunomodulatory and antioxidant function of albumin stabilises the endothelium and improves survival in a rodent model of chronic liver failure. J Hepatol. 2015;62(4):799–806. doi:10.1016/j.jhep.2014.10.031
20. Badimon L, Peña E, Arderiu G, et al. C-Reactive protein in atherothrombosis and angiogenesis. Front Immunol. 2018;9. doi:10.3389/fimmu.2018.00430
21. Gimbrone MA, García-Cardeña G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. 2016;118(4):620–636. doi:10.1161/CIRCRESAHA.115.306301
22. Kayapinar O, Ozde C, Kaya A. Relationship between the reciprocal change in inflammation-related biomarkers (Fibrinogen-to-Albumin and hsCRP-to-Albumin Ratios) and the presence and severity of coronary slow flow. Clin Appl Thromb. 2019;25:107602961983538. doi:10.1177/1076029619835383
23. Nasr Ads M, Ibrahim Mohamed Ali AE-R, Abd El-Alem Ali El-Gendy AE-A, Samy Abd El-Samea M. Relationship between c- reactive protein/albumin ratio and coronary artery disease severity in patients with stable angina. Al-Azhar Med J. 2020;49(3):1339–1348. doi:10.21608/amj.2020.107129
24. American Diabetes Association. Standards of medical care in diabetes—2019 abridged for primary care providers. Clin Diabetes. 2019;37(1):11–34. doi:10.2337/cd18-0105
25. Koc AS, Sumbul HE. Increased aortic intima-media thickness may be used to detect macrovascular complications in adult type II diabetes mellitus patients. Cardiovasc Ultrasound. 2018;16(1):8. doi:10.1186/s12947-018-0127-x
26. Cockcroft DW, Gault H. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31–41. doi:10.1159/000180580
27. Le TD, Nguyen NPT, Nguyen ST, et al. The association between femoral artery intima-media thickness and serum glucagon-like peptide-1 levels among newly diagnosed patients with type 2 diabetes mellitus. Diabetes, Metab Syndr Obes Targets Ther. 2020;13:3561–3570. doi:10.2147/DMSO.S264876
28. Pignoli P, Tremoli E, Poli A, Oreste P, Paoletti R. Intimal plus medial thickness of the arterial wall: a direct measurement with ultrasound Imaging. Circulation. 1986;74(6):1399–1406. doi:10.1161/01.CIR.74.6.1399
29. Soneye M, Adekanmi A, Obajimi M, Aje A. Intima-media thickness of femoral arteries and carotids among an adult hypertensive Nigerian population: a case-control study to assess their use as surrogate markers of atherosclerosis. Ann Afr Med. 2019;18(3):158–166. doi:10.4103/aam.aam_57_18
30. Godoi E, Brandt CT, Lacerda HR, et al. Intima-media thickness in the carotid and femoral arteries for detection of arteriosclerosis in human immunodeficiency virus-positive individuals. Arq Bras Cardiol. 2017;108(1):3–11. doi:10.5935/abc.20160197
31. Zakarija M, Garcia A, McKenzie JM. 5 human albumin. Transfus Med Hemother. 2009;36(6):399–407. doi:10.1172/JCI112183
32. Kunutsor SK, Khan H, Laukkanen JA. Serum albumin concentration and incident type 2 diabetes risk: new findings from a population-based cohort study. Diabetologia. 2015;58(5):961–967. doi:10.1007/s00125-015-3520-0
33. Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease. JAMA. 1998;279(18):1477. doi:10.1001/jama.279.18.1477
34. Bae JC, Seo SH, Hur KY, et al. Association between serum albumin, insulin resistance, and incident diabetes in nondiabetic subjects. Endocrinol Metab. 2013;28(1):26. doi:10.3803/EnM.2013.28.1.26
35. Schalk BWM, Visser M, Bremmer MA, Penninx BWJH, Bouter LM, Deeg DJH. Change of serum albumin and risk of cardiovascular disease and all-cause mortality: longitudinal aging study Amsterdam. Am J Epidemiol. 2006;164(10):969–977. doi:10.1093/aje/kwj312
36. Djousse L, Rothman KJ, Cupples LA, Arnett DK, Ellison RC. Relation between serum albumin and carotid atherosclerosis The NHLBI Family Heart Study. Stroke. 2003;34(1):53–57. doi:10.1161/01.STR.0000048675.97975.84
37. Roche M, Rondeau P, Singh NR, Tarnus E, Bourdon E. The antioxidant properties of serum albumin. FEBS Lett. 2008;582(13):1783–1787. doi:10.1016/j.febslet.2008.04.057
38. Don BR, Kaysen G. Poor nutritional status and inflammation: serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
39. Chang DC, Xu X, Ferrante AW, Krakoff J. Reduced plasma albumin predicts type 2 diabetes and is associated with greater adipose tissue macrophage content and activation. Diabetol Metab Syndr. 2019;11(1):14. doi:10.1186/s13098-019-0409-y
40. Kremer H, Baron-Menguy C, Tesse A, et al. Human serum albumin improves endothelial dysfunction and survival during experimental endotoxemia: concentration-dependent properties*. Crit Care Med. 2011;39(6):1414–1422. doi:10.1097/CCM.0b013e318211ff6e
41. Joosten MM, Pai JK, Bertoia ML, et al. Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men. JAMA. 2012;308(16):1660. doi:10.1001/jama.2012.13415
42. Fowkes FGR, Aboyans V, Fowkes FJI, McDermott MM, Sampson UKA, Criqui MH. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol. 2017;14(3):156–170. doi:10.1038/nrcardio.2016.179
43. Hong G, Gao P, Chen Y, et al. High-Sensitivity C-reactive protein leads to increased incident metabolic syndrome in women but not in men: a five-year follow-up study in a Chinese population. Diabetes, Metab Syndr Obes Targets Ther. 2020;13:581–590. doi:10.2147/DMSO.S241774
44. Klisic A, Kavaric N, Kotur J, Ninic A. Serum soluble transferrin receptor levels are independently associated with homeostasis model assessment of insulin resistance in adolescent girls. Arch Med Sci. 2021. doi:10.5114/aoms/132757
45. Tsuda K. Associations between high-sensitivity C-reactive protein and membrane fluidity of red blood cells in hypertensive elderly men: an Electron Spin Resonance Study. Int J Hypertens. 2012;2012:1–5. doi:10.1155/2012/292803
46. García-álvarez A, Sitges M, Heras M, et al. Endothelial function and high-sensitivity C-reactive protein levels in patients with Chagas disease living in a nonendemic area. Rev Española Cardiol (English Ed. 2011;64(10):891–896. doi:10.1016/j.rec.2011.05.017
47. McDermott MM, Green D, Greenland P, et al. Relation of levels of hemostatic factors and inflammatory markers to the ankle brachial index. Am J Cardiol. 2003;92(2):194–199. doi:10.1016/S0002-9149(03)00537-X
48. Yasojima K, Schwab C, McGeer EG, McGeer PL. Generation of C-Reactive protein and complement components in atherosclerotic plaques. Am J Pathol. 2001;158(3):1039–1051. doi:10.1016/S0002-9440(10)64051-5
49. Ridker PM. High-sensitivity C-Reactive protein. Circulation. 2001;103(13):1813–1818. doi:10.1161/01.CIR.103.13.1813
50. Huang A, Huang Y. Role of Sfrps in cardiovascular disease. Ther Adv Chronic Dis. 2020;11:204062232090199. doi:10.1177/2040622320901990
51. Ma T, Huang X, Zheng H, et al. SFRP2 improves mitochondrial dynamics and mitochondrial biogenesis, oxidative stress, and apoptosis in diabetic cardiomyopathy. Oxid Med Cell Longev. 2021;2021:1–18. doi:10.1155/2021/9265016
52. Wu J, Zheng H, Liu X, et al. Prognostic value of secreted frizzled-related protein 5 in heart failure patients with and without type 2 diabetes mellitus. Circ Hear Fail. 2020;13(9):730–738. doi:10.1161/CIRCHEARTFAILURE.120.007054
53. Wu Y, Liu X, Zheng H, et al. Multiple roles of sFRP2 in cardiac development and cardiovascular disease. Int J Biol Sci. 2020;16(5):730–738. doi:10.7150/ijbs.40923
54. Haruki K, Shiba H, Shirai Y, et al. The C-reactive protein to albumin ratio predicts long-term outcomes in patients with pancreatic cancer after pancreatic resection. World J Surg. 2016;40(9):2254–2260. doi:10.1007/s00268-016-3491-4
55. Oh J, Kim SH, Park KN, et al. High-sensitivity C-reactive protein/albumin ratio as a predictor of in-Hospital mortality in older adults admitted to the emergency Department. Clin Exp Emerg Med. 2017;4(1):19–24. doi:10.15441/ceem.16.158
56. Tong PC, Lee K-F, So W-Y, et al. White blood cell count is associated with macro- and microvascular complications in Chinese patients with type 2 diabetes. Diabetes Care. 2004;27(1):216–222. doi:10.2337/diacare.27.1.216
57. Taleb S. Inflammation in atherosclerosis. Arch Cardiovasc Dis. 2016;109(12):708–715. doi:10.1016/j.acvd.2016.04.002
58. Li J, Flammer AJ, Reriani MK, et al. High leukocyte count is associated with peripheral vascular dysfunction in individuals with low cardiovascular risk. Circ J. 2013;77(3):780–785. doi:10.1253/circj.CJ-12-1131
59. Walker AE, Seibert SM, Donato AJ, Pierce GL, Seals DR. Vascular endothelial function is related to white blood cell count and myeloperoxidase among healthy middle-aged and older adults. Hypertension. 2010;55(2):363–369. doi:10.1161/HYPERTENSIONAHA.109.145870
60. Klisic A, Radoman Vujačić I, Vučković AN. Total leukocyte count, leukocyte subsets and their indexes in relation to cardiovascular risk in adolescent population. Eur Rev Med Pharmacol Sci. 2021;25(7):3038–3044. doi:10.26355/eurrev_202104_25557
61. Ortega E, Gilabert R, Nuñez I, et al. White blood cell count is associated with carotid and femoral atherosclerosis. Atherosclerosis. 2012;221(1):275–281. doi:10.1016/j.atherosclerosis.2011.12.038
62. Barzilay JI, Forsberg C, Heckbert SR, Cushman M, Newman AB. The association of markers of inflammation with weight change in older adults: the Cardiovascular Health Study. Int J Obes. 2006;30(9):1362–1367. doi:10.1038/sj.ijo.0803306
63. Basolo A, Ando T, Chang DC, et al. Reduced albumin concentration predicts weight gain and higher ad libitum energy intake in humans. Front Endocrinol (Lausanne). 2021;12. doi:10.3389/fendo.2021.642568
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.