")
Back to Journals » Drug Design, Development and Therapy » Volume 15
Lower Background Infusion of Oxycodone for Patient-Controlled Intravenous Analgesia, Combined with Ropivacaine Intercostal Nerve Block, in Patients Undergoing Thoracoscopic Lobectomy for Lung Cancer: A Randomized, Double-Blind, Controlled Clinical Trial
Authors Zhang Y , Yan W, Chen Y, Fan Z, Chen J
Received 24 April 2021
Accepted for publication 21 July 2021
Published 13 August 2021 Volume 2021:15 Pages 3535—3542
DOI https://doi.org/10.2147/DDDT.S316583
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Yunxiao Zhang,1 Wanpu Yan,2 Yanyun Chen,1 Zhiyi Fan,1 Jiheng Chen1
1Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Anesthesiology, Peking University Cancer Hospital & Institute, Beijing, People’s Republic of China; 2Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), The First Department of Thoracic Surgery, Peking University Cancer Hospital & Institute, Beijing, People’s Republic of China
Correspondence: Jiheng Chen
Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Anesthesiology, Peking University Cancer Hospital & Institute, 52 Fucheng Street, Haidian District, Beijing, 100142, People’s Republic of China
Tel +86 10 88196553
Fax +86 10 88122437
Email [email protected]
Purpose: To compare the efficacy of a lower dose background infusion of oxycodone for patient-controlled intravenous analgesia (PCIA) with the conventional dose, following intercostal nerve block, for the management of postoperative pain in patients undergoing thoracoscopic lobectomy for lung cancer.
Patients and Methods: This was a prospective, single-center, randomized, parallel-group, double-blind, controlled clinical trial. In total, 155 patients scheduled for elective radical lobectomy via video-assisted thoracoscopy were recruited from December 2018 to July 2019, of whom 140 were ultimately included in the study population. Patients were randomized to receive either oxycodone 0.25 mg/h (low-dose group, n=70) or oxycodone 0.5 mg/h (control group, n=70) as a background infusion for PCIA, following ropivacaine intercostal nerve block, for postoperative pain management. The primary endpoints were rest and dynamic visual analogue scale (VAS) scores within 72 h of the operation. The secondary endpoints were patient satisfaction scores, consumption of postoperative analgesics, times of patient-controlled analgesia (PCA), and adverse events.
Results: All 140 enrolled patients completed the study requirements and were included in the final analysis. The rest and dynamic VAS scores at 4 h, 24 h, 48 h, and 72 h postoperative were comparable between the low-dose group and the control group (P> 0.05). However, the low-dose group had statistically significantly higher patient satisfaction scores (P< 0.001) and lower postoperative analgesic consumption (P< 0.001) as well as lower incidence of nausea and vomiting (P< 0.05). The times of PCA was not statistically significantly different between the two groups, and no serious adverse events occurred in either group (P> 0.05).
Conclusion: A low-dose background infusion of oxycodone for postoperative PCIA can achieve a comparable analgesic effect to the conventional dose after thoracoscopic lobectomy for lung cancer. Furthermore, the low-dose regimen was associated with reduced consumption of oxycodone and increased patient satisfaction.
Keywords: oxycodone, postoperative analgesia, patient-controlled intravenous analgesia, radical resection of lung cancer
Introduction
Although thoracoscopic surgery is associated with less postoperative pain than thoracotomy, thoracoscopic patients still suffer from moderate to severe pain, largely owing to the intraoperative interaction of thoracoscopic devices with the ribs, which may lead to intercostal neuropathy or neuroma.1 Thoracoscopic cannulas can also cause postoperative pain, as they can result in compression or damage of the intercostal nerves when placed between the ribs. Furthermore, closed thoracic drainage tubes (CTDTs) are often a major cause of pain and discomfort in patients who have undergone thoracic surgery and are sometimes associated with a higher degree of pain than that caused by incisions, as the CTDT may result in strong stimulation of the pleura.2 Intercostal nerve injury frequently leads to neurological pain, whereas CTDT stimulation often leads to visceral pain, resulting in pain after thoracoscopic surgery that is both neurological and visceral.3
Oxycodone is an agonist of μ- and κ-opioid receptors that can neutralize both neurological4 and visceral pain5 and has been widely used for postoperative analgesia through patient-controlled intravenous analgesia (PCIA) with an apparent effect.6–8 At present, the routine background dose of oxycodone for PCIA, to ensure the continuity and effectiveness of the analgesic effect, is 0.5 mg/h to 1 mg/h.9 However, higher doses of oxycodone may lead to overdose and increase the incidence of adverse events such as dizziness, nausea, and vomiting.10 Time-scheduled decremental infusion of oxycodone for PCIA, and even no background infusion, have been reported;11–13 however, the optimal approach and dose of oxycodone for PCIA remain unclear. What’s more, intercostal nerve block has been widely used for thoracic patients as part of a multimodal analgesia approach in line with the trend of rapid rehabilitation, but the use of intercostal nerve block followed by postoperative oxycodone PCIA has not been widely studied.
Considering that oxycodone has a rapid onset (2 to 3 min), a strong analgesic effect, and a long acting time (3.5 to 4.0 h),14 we hypothesized that a lower background dose of oxycodone for PCIA, especially as part of a multimodal analgesia approach, may achieve a comparable analgesic effect to the conventional dose after thoracoscopic lobectomy for lung cancer with reduced consumption of oxycodone and improved patients’ experience. In this study, we assessed the efficacy and safety of a low-dose background infusion of oxycodone for PCIA, following ropivacaine intercostal nerve block, for postoperative pain management in patients who underwent thoracoscopic lobectomy for lung cancer.
Materials and Methods
This was a prospective, single-center, randomized, parallel-group, double-blind, controlled clinical trial. Participants were randomized into 1 of 2 groups at a ratio of 1:1. The study was approved by the Medical Ethics Committee of Peking University Cancer Hospital (approval no. 2016YJZ11) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants. The study was registered with the Chinese Clinical Trial Registry (http://www.chictr.org.cn) under the accession number ChiCTR1800016369.
Participants
In total, 155 patients with lung cancer who were scheduled for elective radical lobectomy via video-assisted thoracoscopy between December 1, 2018 and July 31, 2019 were recruited from the First Department of Thoracic Surgery, Peking University Cancer Hospital.
The main inclusion criteria was American Society of Anesthesiologists classification I or II. Exclusion criteria included (1) chronic pain; (2) long-term use of analgesics, sedatives, or antidepressants; (3) alcohol abuse; (4) use of sedatives, antiemetics, or antipruritics 24 h before surgery; (5) pregnant (6) or lactating; (7) scheduled to undergo a two-sided procedure; (8) reopening of the chest within 48 h of the operation; (9) and inability to score pain accurately.
Interventions
All patients received routine monitoring once they entered the operating room and the peripheral vein access was established. Patients then received total intravenous anesthesia. For induction of anesthesia, propofol 1 to 3 mg/kg, sulfentanyl 0.4 μg/kg, and rocuronium 0.6 mg/kg were administered. After endotracheal intubation, mechanical ventilation was conducted at a tidal volume of 8 mL/kg, respiratory rate of 12 to 14/min, and inspiration: expiration ratio of 1.0:1.5, with 60% oxygen at 1 L/min flow rate, positive end-expiratory pressure of 0 cm H2O, and end-tidal PCO2 of 30 to 40 mmHg (1 mmHg=0.133 kPa). For maintenance of anesthesia, an intravenous infusion of propofol 120 to 200 µg/kg/min and remifentanil 0.2 to 0.3 µg/kg/min was given with an intravenous injection of cisatracurium 0.2 mg/kg at a 30-min interval to maintain blood pressure and heart rate within <20% deviation from baseline and bispectral index at 40 to 60. During the operation, Ringer’s lactate solution and 6% hydroxyethyl starch (130/0.4) were infused intravenously at a ratio of 1:1 and at a total infusion speed of 8 to 12 mL/kg/h. At 30 min before the end of the operation, administration of the cisatracurium and remifentanil was stopped, and the patient was given an injection of oxycodone 0.05 mg/kg (batch number: BE123; Hamol, Nottingham, UK). Before the chest was closed, intercostal nerve block was performed on the operation segment (T2-T8) by the surgeon with 0.375% ropivacaine 2 mL for each point. At the end of the operation, When the patient begins to breathe autonomously, atropine 1 mg and neostigmine 2 mg were injected intravenously to antagonize the effect of residual muscle relaxants. The endotracheal tube was removed after satisfactory recovery of respiration.
After extraction of the endotracheal tube, if the visual analog scale (VAS) score was ≥4, an intravenous injection of oxycodone 2 mg was repeatedly given, at 5-min intervals, until the VAS score reached ≤3; the dose of oxycodone used for titration was recorded. PCIA was then initiated using the AutoMed 3000 pain pump (Woo Young, Korea). The PCIA drug solution consisted of oxycodone hydrochloride 50 mg and tropisetron 20 mg/100 mL of saline. The PCIA pump was set as follows: precharge 2 mL, patient-controlled analgesia (PCA) 2 mL per time and lockout interval of 10 min; For the low-dose group, the background infusion rate was 0.5 mL/h (oxycodone 0.25 mg/h), whereas for the control group, the background infusion rate was 1.0 mL/h (oxycodone 0.5 mg/h).
Outcomes
The primary endpoints were rest and dynamic VAS scores, scored by nurse anesthetists blinded to group assignment at 4 h, 24 h, 48 h, and 72 h after the operation. Dynamic VAS was defined as VAS when coughing.
The secondary endpoints were patient satisfaction score, dose of analgesics consumed in PCIA, the times of PCA, the dose of remedial drugs (analgesic and antiemetic), and the incidence of adverse events within 72 h after the operation (also recorded by nurse anesthetists). Patient satisfaction scores for postoperative analgesia were as follows: 5, very satisfied; 4, satisfied; 3, not sure; 2, unsatisfied; 1, very unsatisfied.
Sample Size
The difference in VAS scores between the two groups was analyzed using Student’s t test. The difference in VAS scores and tolerance between the two groups was expected to be 20%, and the maximum tolerance was expected to be 30%. The statistical significance level was set at α bilateral = 0.05, the test efficiency was set at 0.8, and the minimum sample size was calculated to be 148 cases, with the potential of 5% dropout and loss to follow-up.
Randomization
Eligible patients were randomized to receive either a low-dose or a conventional-dose background infusion of oxycodone for postoperative PCIA. The allocation sequence was generated using a computer program by a staff member not otherwise involved in the trial. Concealment was performed using opaque envelopes that were opened upon the patient’s arrival in the operating room.
Blinding
This was a double-blind trial. The patients and the nurse anesthetists in charge of the postoperative follow-up were blinded to group assignment. The anesthesiologist and the surgeons were also blinded to group assignments. Data were recorded using a standardized study case report form and were later entered into a computerized database.
Statistics
Continuous data were expressed as mean ± standard deviation (SD) and compared using Student’s t test. Categorical data were compared using the χ2 test. Grading data were compared using the rank and balance test. Variance analysis of repeated measurement data was used for comparisons at different time points. Statistical analyses were performed using SPSS software (version 22.0, SPSS, Chicago, IL, USA). P<0.05 (2-sided) was considered statistically significant.
Results
Demographic Characteristics and Intraoperative Data
The study flowchart is shown in Figure 1. In total, 155 patients were scheduled for thoracoscopic lobectomy for lung cancer during the study period. Nine patients who declined to participate in the study were excluded. Therefore, 146 patients were randomized to either the low-dose group or the control group. Three patients in the low-dose group and 3 patients in the control group were unable to describe accurate pain scores and were excluded from the final analysis. The final analysis included 140 patients: 70 patients in the low-dose group and 70 patients in the control group. The two groups were comparable in terms of demographic variables, intraoperative data, and dose of oxycodone used for titration before PCIA (Table 1).
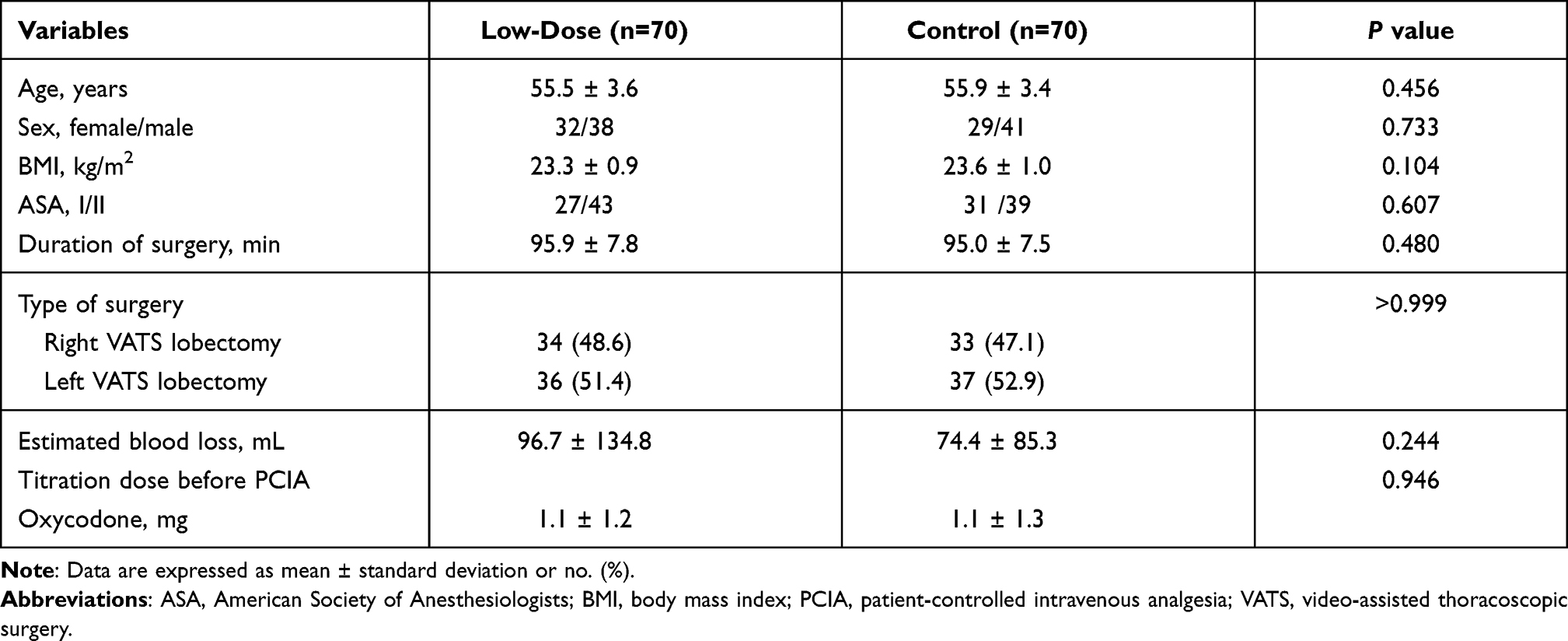 |
Table 1 Demographic Characteristics and Intraoperative Data |
 |
Figure 1 Study flowchart. |
Postoperative VAS Scores
To assess the efficacy of the two approaches, the rest and dynamic VAS scores were recorded at 4 h, 24 h, 48 h, and 72 h postoperative. There were no statistically significant differences in VAS scores between the two groups, indicating that, in combination with ropivacaine intercostal nerve block, a low-dose background infusion was as effective as a conventional-dose background infusion of oxycodone for PCIA (Figure 2).
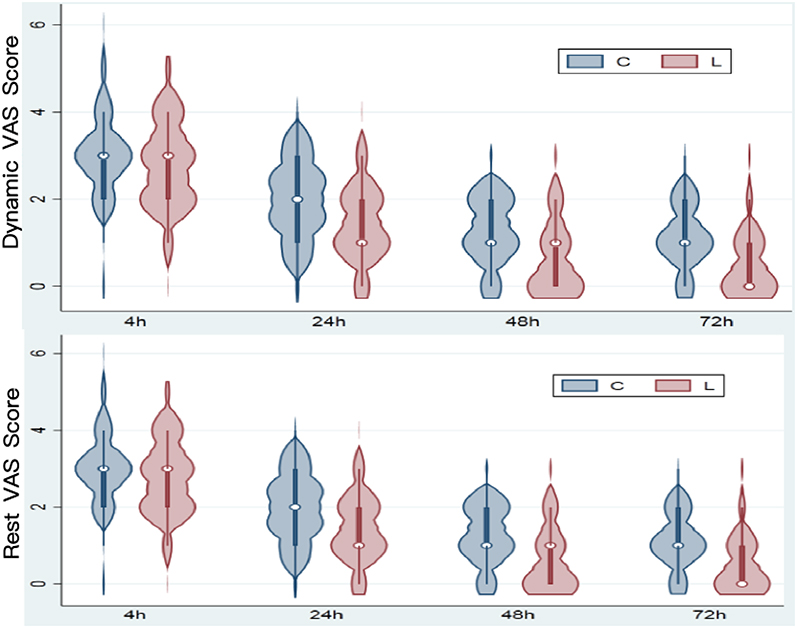 |
Figure 2 Postoperative rest and dynamic visual analog scale (VAS) scores for the two groups. There were no statistically significant differences in VAS scores between the two groups at 4 h, 24 h, 48 h, and 72 h postoperative (all P>0.05). Abbreviations: C, control; L, low dose. |
Dose of Analgesics Consumed Postoperatively
To assess analgesics consumed postoperatively between the two groups, the dose of analgesics consumed in PCIA, the dose of postoperative remedial analgesics, and the number of times of PCA were recorded. The dose of analgesics consumed in PCIA was not statistically significantly different between the two groups within the first 4 h after operation; however, at 24 h, 48 h, and 72 h postoperative, the dose of analgesics consumed was statistically significantly lower in the low-dose group than in the control group. When the VAS score ≥4 and the patients complained of pain even after the use of PCIA, the rescue analgesics (morphine) will be given. The dose of postoperative rescue analgesics, the total times of PCA, and the times of effective/invalid PCA were not statistically significantly different between the two groups (Table 2).
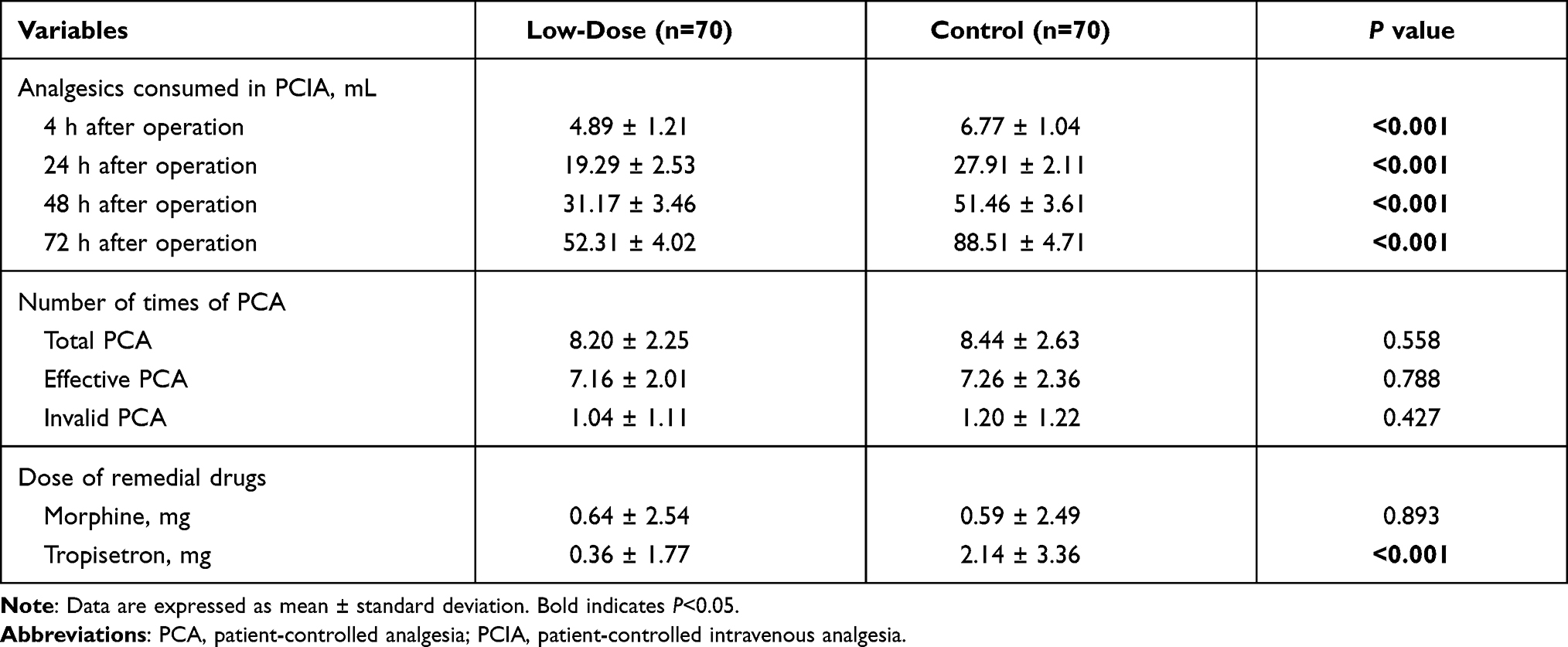 |
Table 2 Analgesics Consumed in PCIA, Times of PCA and Remedial Drugs Consumed Postoperatively |
Postoperative Nausea and Vomiting
The incidence of nausea was statistically significantly lower in the low-dose group at 5 to 24 h, 24 to 48 h, and 48 to 72 h postoperative. Similarly, the incidence of vomiting was statistically significantly lower in the low-dose group at 5 to 24 h and 24 to 48 h (Table 3).
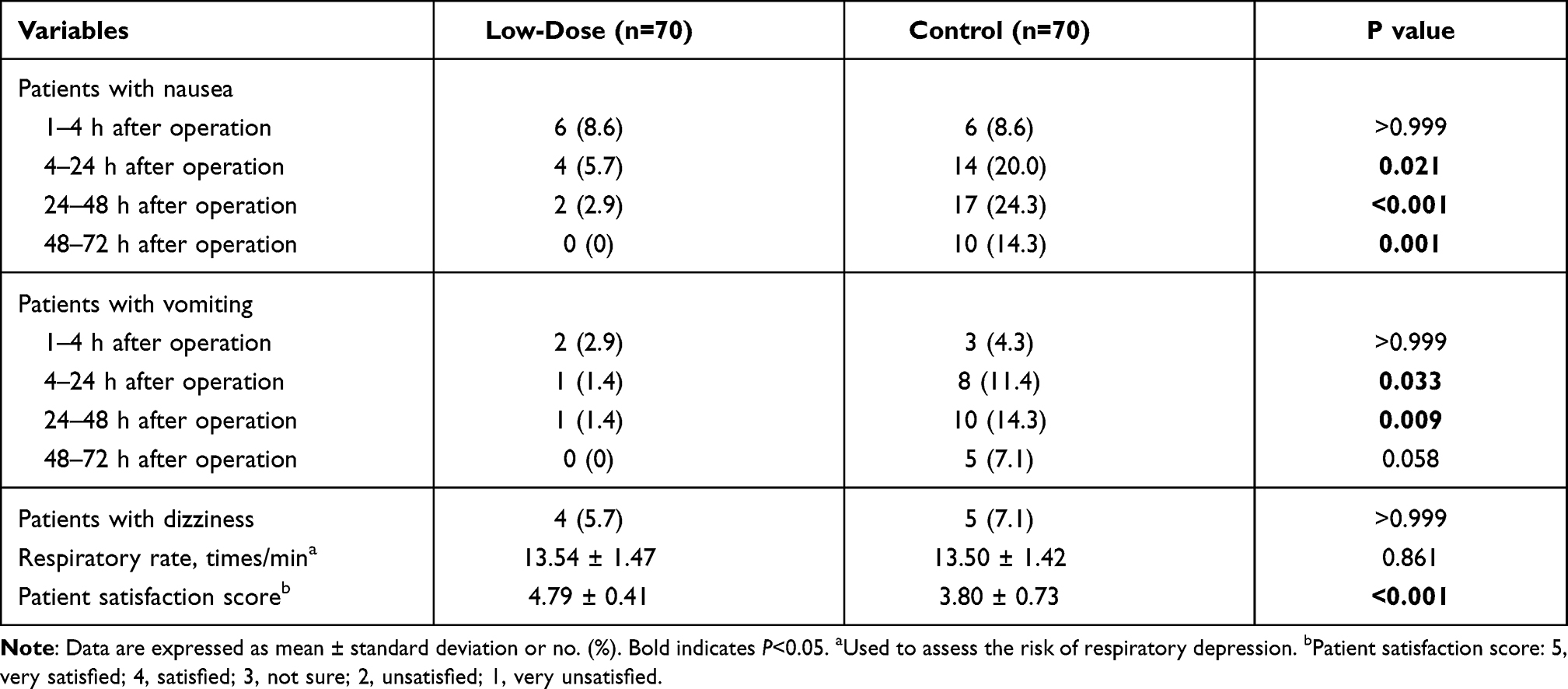 |
Table 3 Incidence of Adverse Events and Patient Satisfaction Scores |
Other Adverse Effects
No patients were admitted to the ICU after surgery. Incidence of postoperative dizziness and respiratory rate (used to assess the risk of respiratory depression) were not statistically significantly different between the two groups. No serious adverse events occurred in either group (Table 3).
Patient Satisfaction Scores
Patient satisfaction scores with the effect of postoperative analgesia were higher in the low-dose group than in the control group (Table 3).
Discussion
We compared the analgesic effects of a low-dose and a conventional-dose background infusion of oxycodone for PCIA in patients who underwent radical thoracoscopic lung cancer surgery. Ropivacaine intercostal nerve block was administered in all patients near the end of the operation. The analgesic effect was comparable between the two groups, whereas patient satisfaction scores were higher and PCIA consumption and postoperative nausea and vomiting were lower in the low-dose group.
Previous study showed that a background infusion of oxycodone of 0.5–1 mg/h could achieve satisfactory postoperative analgesic effects in patients after surgery, but postoperative nausea and vomiting were observed.7,9,10 Other studies have reported that a low dose of oxycodone can achieve a good analgesic effect and is associated with fewer side effects.4,12 Therefore, in our trial, we set the background infusion dose of oxycodone in the control group at conventional 0.5 mg/h, and tried to investigate a background infusion dose of 0.25 mg/h, with the goals of achieving satisfactory analgesia and reducing side effects, following ropivacaine intercostal nerve block, for postoperative pain management.
All patients with a VAS score ≥4 after removal of the endotracheal tube received intravenous titration of oxycodone until VAS was ≤3. The titration levels of the two groups were not statistically significantly different, which indicates that the patients had comparable degrees of pain immediately after surgery and similar sensitivity to oxycodone. In the present study, consumption of analgesics was evaluated at 4 h, 24 h, 48 h, and 72 h postoperative, as the basic metabolism of anesthetic analgesics was expected to be complete by 4 h postoperative,15 the CTDT was most often removed at approximately 48 h (which would largely relieve related pain), and the postoperative analgesia for this type of operation regularly lasts 72 h.10 Rest and dynamic VAS scores were comparable between the two groups and were <3 at all selected time points, indicating that both approaches provide adequate analgesia for patients undergoing radical surgery for lung cancer via thoracoscopy.
Patient satisfaction scores in the low-dose group were statistically significantly higher than those in the control group, which may be due to the lower incidence of postoperative nausea and vomiting in the low-dose group. Studies have shown that postoperative analgesia with oxycodone is often accompanied by nausea, vomiting, dizziness, fatigue, and other complications, and the incidence of these increase with the dose of oxycodone and the duration of use.7,8,16 The precise mechanisms of oxycodone-induced nausea and vomiting are not known with certainty, although such side effects may be due to multiple opioid effects, such as enhanced vestibular sensitivity, direct effects on the chemoreceptor trigger zone, and delayed gastric emptying.17 In the present study, we have shown that a lower background dose of oxycodone for PCIA may decrease the incidence of postoperative nausea and vomiting and analgesia-related adverse events, owing to the substantial reduction in the amount of analgesics consumed postoperatively.
In line with the trend of rapid rehabilitation, intercostal nerve block has been widely used as part of a multimodal analgesia approach for thoracic patients.13 In the present study, ropivacaine was used for intercostal nerve block, the effect of which usually lasted approximately 10 h.18 Studies have shown that the primary pain caused by skin incision subsides within 1 h, whereas severe secondary pain can last until the early postoperative period.19 Previous studies have also found that the degree of postoperative pain is highest at 4 h after surgery and then declines thereafter.20,21 Therefore, in the first few hours after surgery, ropivacaine intercostal nerve block may contribute substantially to the satisfied analgesia of patients in both groups.
The limitations of this study include its small sample size. In addition, the study was performed at a single institution, which may limit the generalizability of our results.
In conclusion, a low-dose (0.25 mg/h) background infusion of oxycodone in PCIA, following ropivacaine intercostal nerve block, is safe and effective for postoperative pain management in patients undergoing thoracoscopic lobectomy for lung cancer, with comparable analgesic effect to the conventional dose, but reduced consumption of oxycodone and increased patient satisfaction.
Data Sharing Statement
All the data in the manuscript are available upon reasonable request from the corresponding author.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vogt A, Stieger DS, Theurillat C, et al. Single-injection thoracic paravertebral block for postoperative pain treatment after thoracoscopic surgery. Br J Anaesth. 2005;95(6):816–821. doi:10.1093/bja/aei250
2. Guay J. The benefits of adding epidural analgesia to general anesthesia: a metaanalysis. J Anesth. 2006;20(4):335–340. doi:10.1007/s00540-006-0423-8
3. Bendixen M, Jørgensen OD, Kronborg C, et al. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. 2016;17(6):836–844. doi:10.1016/S1470-2045(16)00173-X
4. Lazzari M, Sabato AF, Caldarulo C, et al. Effectiveness and tolerability of low-dose oral oxycodone/naloxone added to anticonvulsant therapy for noncancer neuropathic pain: an observational analysis. Curr Med Res Opin. 2014;30(4):555–564. doi:10.1185/03007995.2013.866545
5. Staahl C, Dimcevski G, Andersen SD, et al. Differential effect of opioids in patients with chronic pancreatitis: an experimental pain study. Scand J Gastroenterol. 2007;42(3):383–390. doi:10.1080/00365520601014414
6. Xiang X, Yuan X, Lian Y, et al. Effect of oxycodone hydrochloride combined with flurbiprofen axetil for intravenous patient-controlled analgesia in lower abdominal patients: a randomized trial. Medicine (Baltimore). 2018;97(7):e9911. doi:10.1097/MD.0000000000009911
7. Park JH, Lee C, Shin Y, et al. Comparison of oxycodone and fentanyl for postoperative patient-controlled analgesia after laparoscopic gynecological surgery. Korean J Anesthesiol. 2015;68(2):153–158. doi:10.4097/kjae.2015.68.2.153
8. Hwang BY, Kwon JY, Kim E, et al. Oxycodone vs. fentanyl patient-controlled analgesia after laparoscopic cholecystectomy. Int J Med Sci. 2014;11(7):658–662. doi:10.7150/ijms.8331
9. Nie JJ, Sun S, Huang SQ. Effect of oxycodone patient-controlled intravenous analgesia after cesarean section: a randomized controlled study. J Pain Res. 2017;10:2649–2655. doi:10.2147/JPR.S142896
10. Olczak B, Kowalski G, Leppert W, et al. Analgesic efficacy, adverse effects, and safety of oxycodone administered as continuous intravenous infusion in patients after total hip arthroplasty. J Pain Res. 2017;10:1027–1032. doi:10.2147/JPR.S125449
11. Dang SJ, Li RL, Wang J, et al. Oxycodone vs sufentanil in patient-controlled intravenous analgesia after gynecological tumor operation: a Randomized Double-Blind Clinical Trial. J Pain Res. 2020;13:937–946. doi:10.2147/JPR.S236933
12. Kwon YS, Jang JS, Lee NR, et al. A comparison of oxycodone and alfentanil in intravenous patient-controlled analgesia with a time-scheduled decremental infusion after laparoscopic cholecystectomy. Pain Res Manag. 2016;2016:7868152. doi:10.1155/2016/7868152
13. Zhang B, Wang G, Liu X, et al. The opioid-sparing effect of perioperative dexmedetomidine combined with oxycodone infusion during open hepatectomy: a Randomized Controlled Trial. Front Pharmacol. 2017;8:940. doi:10.3389/fphar.2017.00940
14. Lenz H, Sandvik L, Qvigstad E, et al. A comparison of intravenous oxycodone and intravenous morphine in patient-controlled postoperative analgesia after laparoscopic hysterectomy. Anesth Analg. 2009;109(4):1279–1283. doi:10.1213/ane.0b013e3181b0f0bb
15. Hao GT, Zhou HY, Gao HZ, et al. Pharmacokinetics of oxycodone hydrochloride and three of its metabolites after intravenous administration in Chinese patients with pain. Pharmacol Rep. 2014;66(1):153–158. doi:10.1016/j.pharep.2013.08.012
16. Pedersen KV, Olesen AE, Drewes AM, et al. Morphine versus oxycodone analgesia after percutaneous kidney stone surgery: a randomised double blinded study. Urolithiasis. 2013;41(5):423–430. doi:10.1007/s00240-013-0587-2
17. Smith HS, Laufer A. Opioid induced nausea and vomiting. Eur J Pharmacol. 2014;722:67–78. doi:10.1016/j.ejphar.2013.09.074
18. Choi SW, Cho SJ, Moon HW, et al. Effect of intercostal nerve block and nephrostomy tract infiltration with ropivacaine on postoperative pain control after tubeless percutaneous nephrolithotomy: a Prospective, Randomized, and Case-controlled Trial. Urology. 2018;114:49–55. doi:10.1016/j.urology.2017.12.004
19. Kawamata M, Watanabe H, Nishikawa K, et al. Different mechanisms of development and maintenance of experimental incision-induced hyperalgesia in human skin. Anesthesiology. 2002;97(3):550–559. doi:10.1097/00000542-200209000-00006
20. Kim HS, Czuczman GJ, Nicholson WK, et al. Pain levels within 24 hours after UFE: a comparison of morphine and fentanyl patient-controlled analgesia. Cardiovasc Intervent Radiol. 2008;31(6):1100–1107. doi:10.1007/s00270-008-9430-5
21. Kim JJ, Ha MH, Jung SH, et al. The efficiency of IV PCA with remifentanil and ketorolac after laparoscopic-assisted vaginal hysterectomy. Korean J Anesthesiol. 2011;61(1):42–49. doi:10.4097/kjae.2011.61.1.42
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.